 Heber Isac Arbildo-Vega1,2
Heber Isac Arbildo-Vega1,2 Fredy Hugo Cruzado-Oliva3
Fredy Hugo Cruzado-Oliva3 Hernán Vásquez-Rodrigo1,4
Hernán Vásquez-Rodrigo1,4 Franz Tito Coronel-Zubiate5*Luis Felipe Alarco-La Rosa3Luisfelipe Carlos Alarco-Jurado6Stefanny Lisset Zarate-Chavarry6
Franz Tito Coronel-Zubiate5*Luis Felipe Alarco-La Rosa3Luisfelipe Carlos Alarco-Jurado6Stefanny Lisset Zarate-Chavarry6
- 1Faculty of Dentistry, Dentistry School, Universidad San Martín de Porres, Chiclayo, Peru
- 2Faculty of Human Medicine, Human Medicine School, Universidad San Martín de Porres, Chiclayo, Peru
- 3Faculty of Stomatology, Stomatology School, Universidad Nacional de Trujillo, Trujillo, Peru
- 4Department of Dentistry, Dentistry School, Universidad Norbert Wiener, Lima, Peru
- 5Faculty of Health Sciences, Stomatology School, Universidad Nacional Toribio Rodríguez de Mendoza de Amazonas, Chachapoyas, Peru
- 6Faculty of Human Medicine, Stomatology School, Universidad Privada Antenor Orrego, Trujillo, Peru
Background: The choice of restorative material in pediatric dentistry is clinically relevant for ensuring long-term tooth preservation and reducing recurrent caries. This systematic review and meta-analysis compared the clinical effectiveness of ion-releasing restorations (IRR) and composite resin (CR) in children's dental treatments.
Methods: Randomized clinical trials with ≥1-year follow-up were identified through comprehensive searches in PubMed, Cochrane Library, Scielo, Scopus, Web of Science, and Google Scholar up to January 2024. Studies reporting clinical outcomes of IRR vs. CR were analyzed. Risk of bias was assessed using RoB2.0, and evidence certainty with GRADE.
Results: Of 1,109 records screened, nine trials were included. Pooled analyzes showed no statistically significant differences between IRR and CR regarding secondary caries, marginal adaptation, or restoration survival (p > 0.05). Both materials demonstrated satisfactory longevity and clinical behavior.
Conclusions: Within the limitations of available evidence, ion-releasing and composite restorations provide comparable clinical performance in pediatric dentistry. The findings support the use of IRR as a reliable alternative for child patients, offering bioactive benefits while maintaining similar restorative success to composites.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024524163, PROSPERO CRD42024524163.
1 Introduction
Dentistry always seeks to improve the quality of restorative interventions to ensure long-lasting results with essential attributes such as durability, aesthetics and biocompatibility (1). The durability and resistance of restorations are essential to cope with chewing forces and variations in the oral environment (2), especially in contexts where dental caries remains a widespread health problem (3). Aesthetics are crucial, as patients value the appearance of restorations (4), and biocompatibility with surrounding tissues also influences the choice of material (5).
In recent years, there have been significant advances in composite resin (CR) formulations to address clinical challenges. Bulk placement techniques, new filler formulations, and simplified adhesion protocols have facilitated their application (6–8). However, clinical problems such as sensitivity of the technique, polymerization shrinkage, and lack of antibacterial properties still persist (9–11). Furthermore, the main reasons for its failure continue to be secondary caries and bulk fractures (6, 7, 12).
For this reason, intelligent and alternative restorative materials have been developed (13–15). Ion-releasing restorative (IRR) materials, such as glass ionomer cement (GIC), are known for their fluoride-releasing properties, which contribute to preventing caries and maintaining biocompatibility (16–18). However, marginal adaptation and resistance un-der load are important aspects to consider (19, 20). The CRs are a popular choice for es-thetic restorations, offering a wide range of shades and good marginal adaptation (21–23). Although they are sensitive to moisture and may experience wear, they provide excellent aesthetics and durability in appropriate situations (24, 25).
The choice between IRR and CR depends on specific clinical needs, prioritizing caries prevention and biocompatibility with IRR (26, 27), while for CR aesthetics and durability are prioritized (1). Other factors such as costs and ease of application also influence the decision of the most appropriate restorative material for each case (28).
Therefore, the purpose of this systematic review and meta-analysis is to compare the clinical effectiveness of IRRs vs. CRs in pediatric dental restorations. We hypothesized that ion-releasing restorations would demonstrate comparable or superior clinical performance to composite restorations in pediatric dental treatments.
2 Materials and methods
2.1 Protocol and registration
The present review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) (29) and registered in the Prospective Registry of Systematic Reviews (PROSPERO) (30). The registry is publicly available under CRD number 42024524163.
2.2 Definitions of interventions
• Ion-Releasing Restorations (IRR): IRR were defined as restorative materials capable of releasing therapeutic ions, primarily fluoride, and included conventional glass ionomer cements (GIC), resin-modified GIC (RMGIC), high-viscosity GIC, glass hybrids, compomers (polyacid-modified composites), and giomers. Materials were included only if their ion-releasing capacity was stated by the manufacturer or verified in the study protocol.
• Composite Resins (CR): CRs referred to light-cured resin-based materials with no inherent ion-releasing properties, used as control or comparison arms in eligible studies.
2.3 Focused question and PICO framework
The focused question was formulated using the PICO format (population, intervention, comparison and outcomes), as detailed below:
- Population: Children who received dental restorations.
- Intervention: Restoration with IRRs, which includes all GIC derivatives (RMGIC, HV-GIC, conventional and glass hybrid), polyacid-modified composites (compomer), giomer, and any material declared by the manufacturer to have the ability to release ions.
- Comparison: Restoration with CR.
- Outcomes: Retention, marginal adaptation, marginal discoloration, marginal or tooth integrity, secondary caries, color or translucency, surface texture or luster, surface staining, wear, anatomic form, post-operative sensitivity, periodontal tissue, integrity of contact point, occlusion.
Focused question (PICO): Is there a difference in the clinical effectiveness of ion-releasing restorations com-pared to resin composite in pediatric dental restorations?
2.4 Information sources and search strategy
For the present systematic review, a systematic search was carried out in five electronic databases (PubMed, Cochrane Library, Scopus, Web of Science, and Scielo). Gray literature was also consulted through Google Scholar, OpenGrey, and Proquest. Addition-ally, the reference lists of included studies were reviewed; all until January 2024; combining keywords and subject titles according to the thesaurus of each data-base: “ion-releasing”, “bioactive resin composite”, “glass ionomer cement”, “high viscosity glass ionomer”, “resin modified glass ionomer”, “glass hybrid”, “polyacid-modified composite”, “compomer”, “resin composite”, “composite resin”, “randomized clinical trial” and “clinical trial”. The search strategies for each of the databases are found in Table 1.

Table 1. Search and selection of studies.
Additionally, further relevant literature was included after a hand search of the reference lists of the final articles.
2.5 Study selection
The search in the electronic database was carried out by two authors (HA and FCO) independently, and the final inclusion decision was made according to the following criteria: Randomized clinical trials (RCTs), with a follow-up time greater than or equal to 1 year, without time and language limits, report the clinical effectiveness of the IRR and CR in pediatric dental restorations (I, II and V Class) using the World Dental Federation (FDI) or the United States Public Health Service Criteria (USPHS) as evaluation criteria. Articles that were prospective studies, unpublished studies, and reported in more than one publication with different follow-up periods were excluded.
2.6 Data extraction
A predefined table was used to extract data from each eligible study, including: author(s), year of publication, study design, country where the study was conducted, number of patients, proportion of male and female patients, age mean and age range, follow-up time, evaluation criteria, study groups, number of patients and teeth restored per study group, type of cavity (according to Black), tooth type, Retention, marginal adaptation, marginal discoloration, marginal or tooth integrity, secondary caries, color or translucency, surface texture or luster, surface staining, wear, anatomic form, post-operative sensitivity, periodontal tissue, integrity of contact point and occlusion. From each eligible study, two investigators (FCZ and LAR) independently extracted information, and all disagreements were resolved by discussion with a third reviewer (LAJ).
2.7 Risk of bias (RoB) assessment
The RoB of the included studies was independently assessed by two calibrated authors (FCO and SZ) (k = 0.98) using the Cochrane Group's RoB 2.0 tool (31) and all disagreements were resolved by discussion with a third reviewer (HA). According to this tool, clinical trials are evaluated in 5 domains: randomization process, deviations from planned interventions, missing outcome data, outcome measurement, and selection of the results report; to later be classified as: high risk of bias, bias with some concerns, or low risk of bias.
2.8 Statistical analysis and certainty of evidence (GRADE)
Data from each study were entered and analyzed in RevMan 5.3 (Cochrane Group, UK); using measures such as mean, standard deviation, and frequency in a random effects model with a 95% confidence interval. Additionally, a GRADE analysis was performed using the guideline development tool (GRADEPro GDT) (McMaster University and Evidence Prime Inc., Canada).
3 Results
3.1 Selection of studies
The electronic and manual search strategies yielded a total of 1,109 articles, excluding 347 duplicates (Figure 1) and 751 were excluded during title screening, leaving 17 potentially eligible for abstract screening, but 11 articles were excluded and 3 added from other reviews, resulting in 9 RCTs for full-text article screening, and they met the eligibility criteria for qualitative and quantitative synthesis (meta-analysis). The reasons for the exclusion of the studies are found in Table 2.
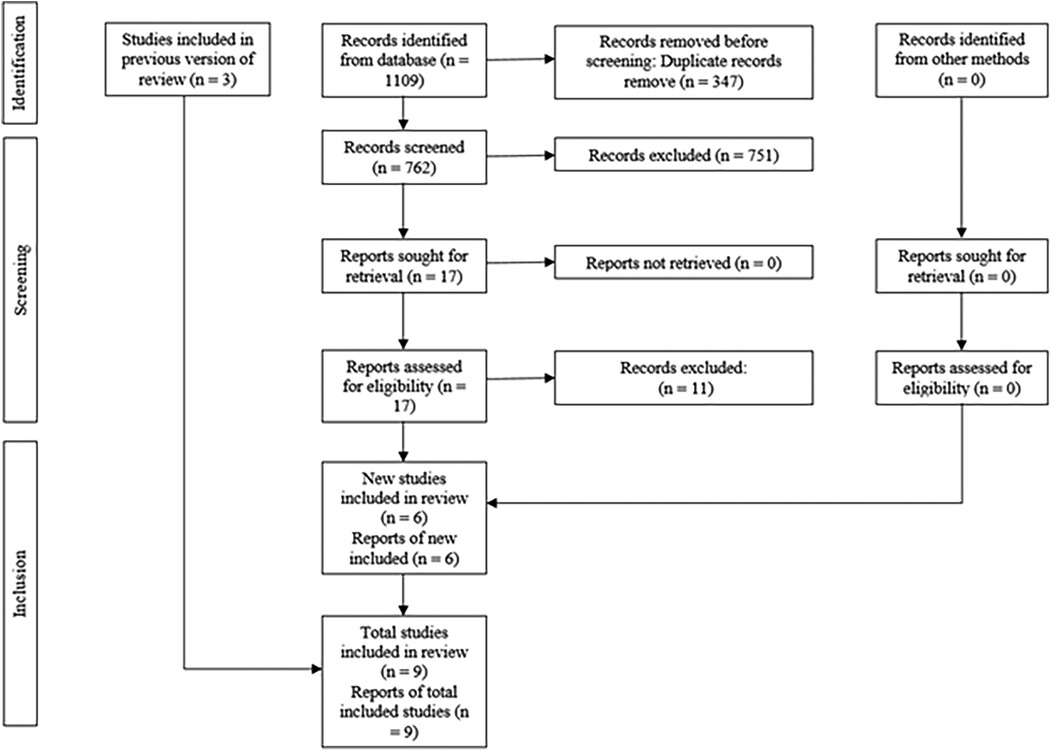
Figure 1. PRISMA diagram showing the process of inclusion and exclusion of studies.
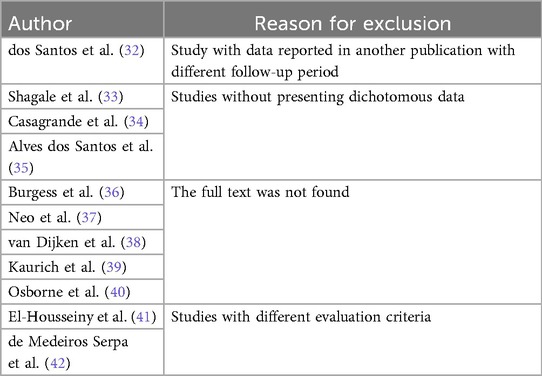
Table 2. Reason for exclusion of studies.
3.2 Characteristics of included studies
In total, 9 RCTs (43–51) were included, of which only two (45, 47) were parallel. All studies reported that the total number of patients ranged from 26 to 180 and the number of teeth treated ranged from 16 to 176. Six studies (43, 45, 46, 48–50) reported that the mean age of patients ranged from 5.08 to 8 years, and all studies reported a range of 4–11 years in all patients with a follow-up time of between 1 year and 2 years (Table 3).
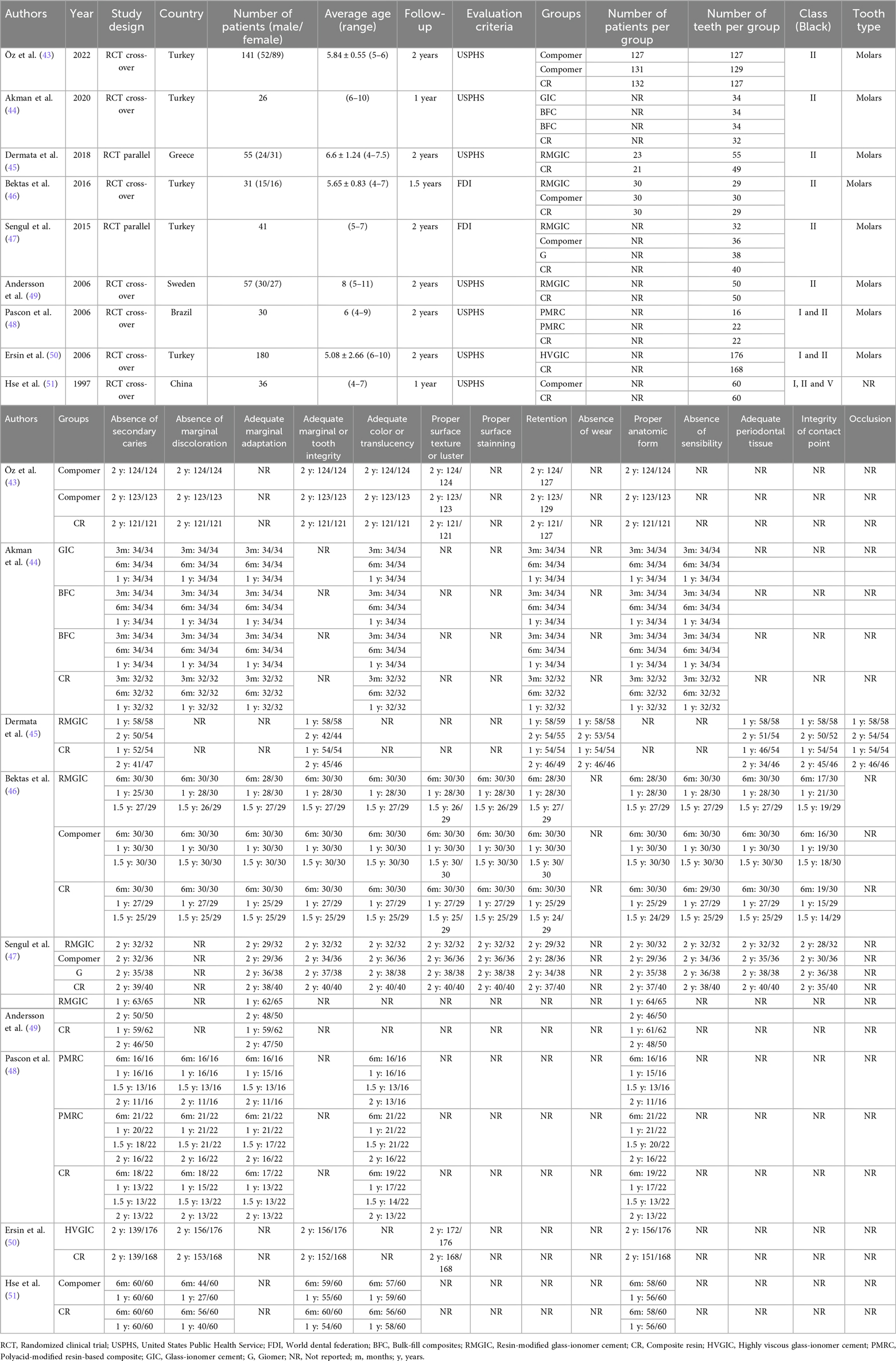
Table 3. Characteristics of included studies.
The countries where the studies were carried out were: Turkey (43, 44, 46, 47, 50), Greece (45), Sweden (49), Brazil (48) and China (51). Two studies (46, 47) mentioned that the evaluation criteria used for the analysis of the teeth was the FDI criteria. Five studies (43, 46–48, 51) reported the use of polyacid-modified resin-based composite (PMRC) or compomer, one study (47) used giomer, one study (44) reported the used bulk-fill composite, one study (44) used glass ionomer cement (GIC), one study (50) used high viscosity glass ionomer cement (HVGIC) and four studies (45–47, 49) used resin-modified glass ionomer cement (RMGIC) (Table 3).
A total of nine studies (43–51) evaluated the presence or absence of secondary caries. Marginal discoloration was reported in six studies (43, 44, 46, 48, 50, 51), marginal adaptation in five (44, 46–49), and marginal or tooth integrity in six (43, 45–47, 50, 51). Additionally, six studies (43, 44, 46–48, 51) evaluated color or translucency, four (43, 46, 47, 50) surface texture or luster, and two (46, 47) surface staining. Retention was reported in five studies (43–47), wear in one (45), and anatomical form in eight (43, 44, 46–51). Three studies (44, 46, 47) evaluated sensitivity, three (45–47) periodontal tissue conditions, three (45–47) contact point integrity, and one (45) occlusion (Table 3).
3.3 Risk of bias analysis of studies
All studies had a low risk of bias (Figure 2).
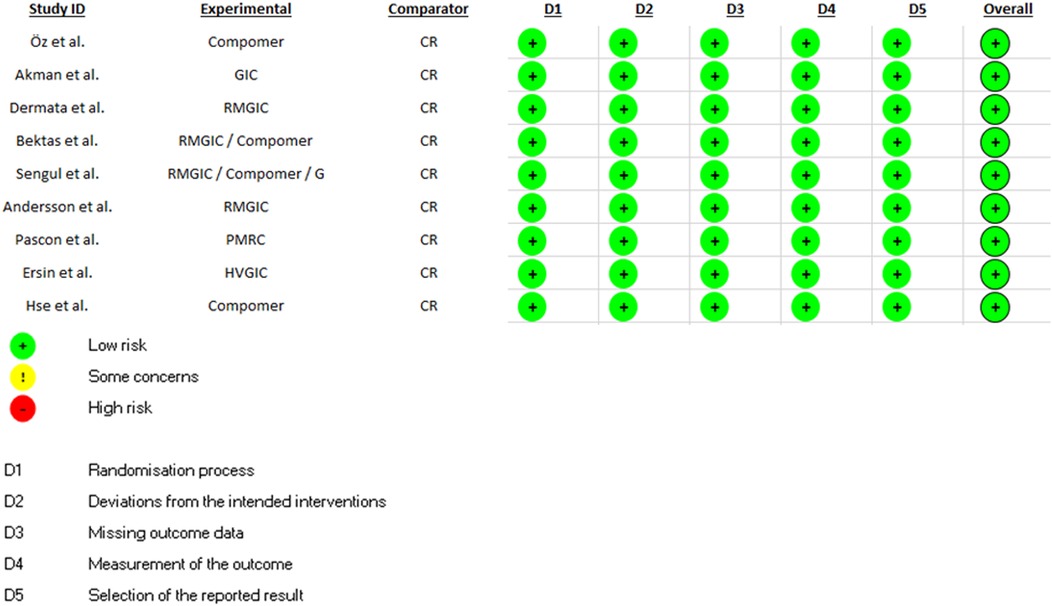
Figure 2. Risk of bias analysis of included studies.
3.4 Synthesis of results (meta-analysis)
The clinical effectiveness of IRR in comparison to CR in terms of absence of secondary caries, absence of marginal discoloration, adequate marginal adaptation, adequate marginal or tooth integrity, adequate color or translucency, proper surface texture or luster, proper surface staining, retention, proper anatomic form, absence of sensibility, adequate periodontal tissue and integrity of contact point was determined in nine (43–51), six (43, 44, 46, 48, 50, 51), five (44, 46–49), six (43, 45–47, 50, 51), six (43, 44, 46–48, 51), four (43, 46, 47, 50), two (46, 47), five (43–47), eight (43, 44, 46–51), three (44, 46, 47), three (45–47) and three (45–47) studies; which show that there was no statistically significant difference for all these clinical parameters (Supplementary Appendix A, Figures A1 – A12).
Across all meta-analyses, ion-releasing restorations (IRR) demonstrated comparable clinical outcomes to composite resins (CR). No statistically significant differences were found for the evaluated parameters (p > 0.05). Representative pooled effect sizes included: absence of secondary caries (RR = 1.01.95%CI0.99–1.03, p = 0.42); marginal discoloration (RR = 1.00.95%CI0.93–1.08, p = 0.97); marginal adaptation (RR = 1.02.95%CI0.96–1.08, p = 0.48); and retention (RR = 1.02,95%CI0.98–1.07, p = 0.32). These consistent risk ratios close to 1.0 indicate a clinical equivalence between IRR and CR across short- and medium-term follow-up periods. The complete set of estimates is shown in Table 4 and detailed forest plots are available in supplementary Appendix A.
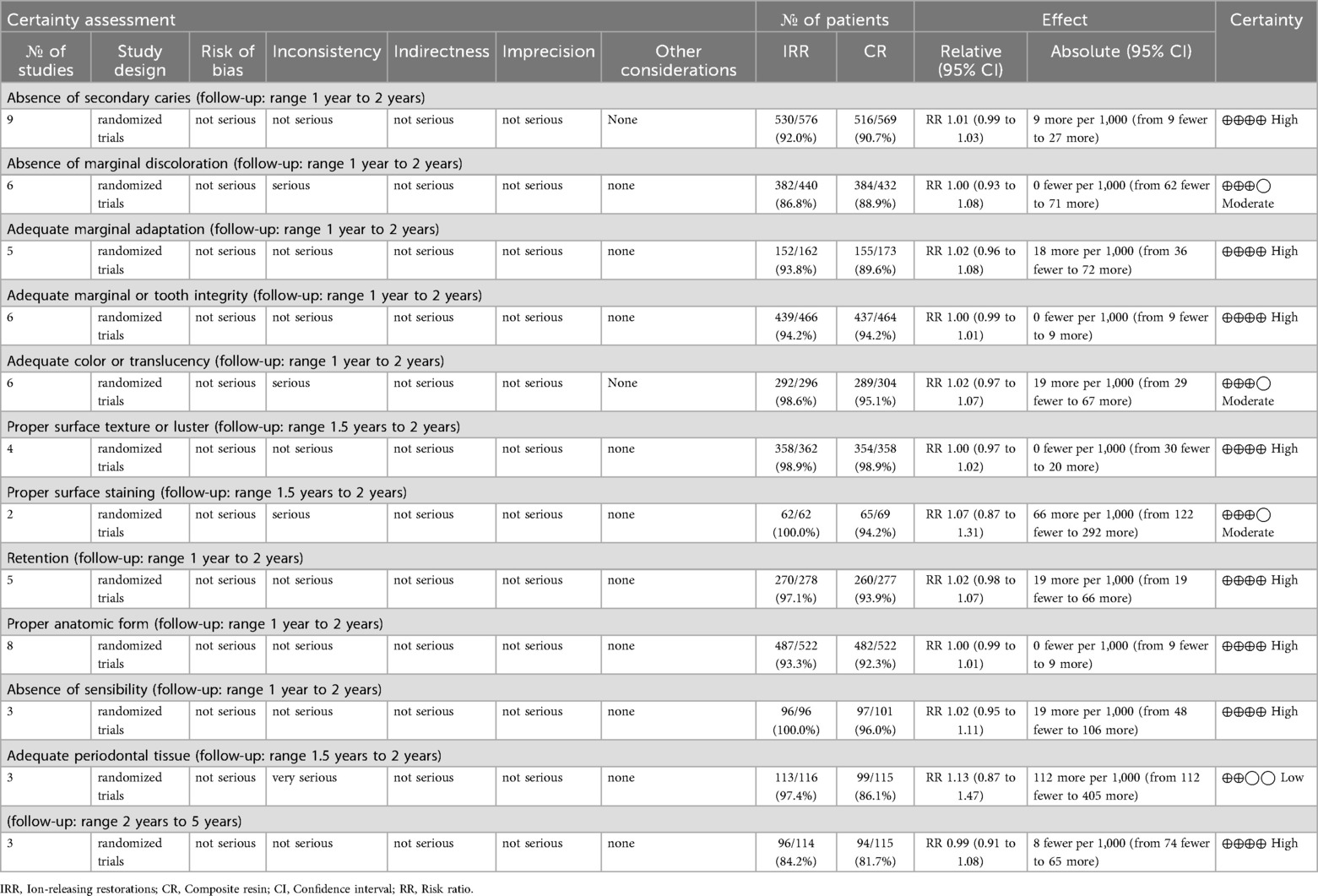
Table 4. GRADE analysis of included studies.
3.5 GRADE analysis
When evaluating the included studies, it was observed that there is high certainty in the absence of secondary caries, adequate marginal adaptation, adequate marginal or tooth integrity, proper surface texture or luster, retention, proper anatomic form, absence of sensibility and integrity of contact point; there is moderate certainty in the absence of marginal discoloration, adequate color or translucency and proper surface staining; and the is low certainty in the adequate periodontal tissue (Table 4). The GRADE summary confirmed that none of the clinical outcomes showed statistically significant differences between IRR and CR (all p > 0.05), supporting the equivalence observed in the pooled effect sizes.
3.6 Sensitivity and publication bias analysis
Sensitivity analyzes were conducted by sequentially omitting each included study (leave-one-out analysis) and re-running the meta-analyses. The pooled effect sizes remained stable across all primary outcomes, confirming the robustness of the findings.
Publication bias was evaluated using funnel plots and Egger's regression test (Supplementary Appendix A, Figures A1–A12). No statistically significant bias was detected in any of the assessed outcomes (all p-values >0.05), indicating that small-study effects are unlikely to have influenced the results. Mild asymmetry was visually observed for color/translucency, surface staining, and post-operative sensitivity; However, the corresponding Egger's tests remained non-significant.
4 Discussion
Nine RCTs, mostly conducted in Europe, were included in this meta-analysis. These studies used FDI and modified USPHS criteria to evaluate 12 clinical parameters, and all had a low risk of bias, reinforcing the validity of our findings. No statistically significant differences were found between IRR and CR restorations in any clinical outcome, indicating comparable efficacy. These results align with previous meta-analyses that reported no significant differences between the two materials (6).
The GRADE assessment showed high certainty for 8 outcomes, moderate for 3, and low for 1 (periodontal tissue status), supporting strong confidence in the main findings. These results are in line with recent studies in pediatric restorative dentistry. For instance, Dermata et al. (45) and a 2024 Egyptian RCT (52) reported no differences in failure rate or clinical performance between RMGIC and CR over 2–3 years.
Other reviews also confirmed this equivalence. Krishnakumar et al. reported satisfactory performance of HVGIC, and Albelasy et al. found no significant differences in secondary caries or marginal adaptation between IRR and CR (6, 53). Similar conclusions were reached for color, adaptation, and anatomical shape (53, 54).
Although some studies, such as Dias et al. (54), suggest isolated benefits of IRR in reducing secondary caries, our meta-analysis did not detect such differences—likely due to variations in study populations or follow-up periods. Overall, most recent evidence agrees on the clinical similarity of both materials in terms of retention, staining, and marginal adaptation.
Several factors may explain the observed equivalence. Strict protocols for isolation and technique in the included RCTs likely minimized marginal leakage in both groups. As Albelasy et al. (6) noted, secondary caries development depends on a multifactorial context—oral hygiene, diet, caries risk—beyond just the material. Thus, in well-controlled pediatric settings, the added benefits of ion release may not yield measurable differences.
Additionally, the performance gap between materials may have narrowed due to recent improvements in adhesive systems and “bioactive” CRs with fluoride or antimicrobial agents. This could explain the modest, non-significant differences in color or gloss (moderate certainty).
Sample sizes and follow-up durations (mostly 1–3 years) may have limited the detection of small differences. However, the GRADE analysis provides high certainty in the absence of meaningful disparities, indicating future research is unlikely to change these conclusions.
Furthermore, replacing part of the resin matrix with ion-releasing components in newer materials may balance performance features. For example, Bodur et al. (55) reported no clear superiority among four IRRs, although Fuji II LC showed a slight advantage in retention.
Sensitivity analysis confirmed that no individual study unduly influenced pooled results. Egger's tests for outcomes A1–A12 showed no evidence of publication bias (Supplementary Appendix A, Figures A1–A12), increasing confidence in the findings. Although some funnel plots showed visual asymmetry, small-study effects were not statistically supported.
In summary, this meta-analysis provides robust evidence for the equivalence of IRR and CR in pediatric restorations. Certainty was high for most functional and mechanical outcomes (secondary caries, marginal adaptation and integrity, retention, anatomical shape, sensitivity, contact point). Moderate certainty for color-related parameters suggests possible context-dependent differences. Periodontal health changes should be interpreted with caution due to low certainty.
The overall homogeneity of the results and low risk of bias across studies support evidence-based clinical decisions. Therefore, the selection between IRR and CR can be guided by practical considerations—cost, technical sensitivity, operator preference—without compromising clinical effectiveness.
4.1 Limitations
This study has several limitations that should be acknowledged. First, despite including only randomized clinical trials (RCTs), the heterogeneity in methodologies, sample sizes, and outcome assessment tools across the studies reduces the comparability and generalizability of the results. Second, the moderate to high risk of bias in several domains of the included trials may influence the reliability of the pooled estimates. Third, the follow-up periods varied significantly, and long-term outcomes were not consistently reported, limiting our ability to draw conclusions about durability. Lastly, publication bias could not be entirely ruled out due to the small number of studies per outcome.
5 Conclusions
The results of the present review indicate that there are no significant differences when restoring children's teeth using CR or IRR. According to the GRADE assessment, the certainty of evidence was high for key clinical parameters such as secondary caries, retention, marginal adaptation and integrity, anatomical shape, sensitivity, and contact point. This supports strong confidence in the equivalence of both materials in these outcomes.
However, moderate certainty was found for aesthetic parameters like color, gloss, and surface staining, suggesting that minor differences might be observed in certain contexts. Low certainty was observed for periodontal tissue outcomes, indicating that further research is needed in this area.
Notably, some outcomes exhibited considerable heterogeneity between studies, particularly those related to esthetic and periodontal parameters, which may reflect differences in assessment criteria, follow-up duration, or operator technique.
While the overall findings suggest that both materials are clinically comparable for most restorative purposes in pediatric dentistry, recommendations should be made considering the varying strength of evidence across outcomes, along with clinical context and individual patient needs.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
HA-V: Conceptualization, Formal analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing. FC-O: Investigation, Methodology, Writing – original draft. HV-R: Project administration, Validation, Writing – original draft. FC-Z: Resources, Validation, Visualization, Writing – review & editing. LA-L: Funding acquisition, Validation, Writing – original draft. LA-J: Validation, Writing – original draft. SZ-C: Data curation, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdmed.2025.1651696/full#supplementary-material
The meta-analyses of the data extracted from the included studies is presented. The data involved the following 12 clinical parameters: absence of secondary caries, absence of marginal discoloration, adequate marginal adaptation, adequate marginal or tooth integrity, adequate color or translucency, proper surface texture or luster, proper surface staining, retention, proper anatomic form, absence of sensibility, adequate periodontal tissue and integrity of contact point. The results are presented as forest plots; where: CR, composite resin; IRR, Ion-releasing restorative; CI, confidence interval; df, degrees of freedom; M-H, Mantel-Haenszel; I2,Higgins I2 test; Chi2, Chi square test. Additionally, funnel plots and results of Egger's tests are included to assess publication bias. A leave-one-out sensitivity analysis under random-effects DerSimonian-Laird model is also presented, evaluating the influence of each individual study on overall effect estimate.
All Egger's test p-values are reported below each funnel plot (Supplementary Figures A1–A12), and the p-values for each excluded study are shown in the final column of the sensitivity analyses.
References
1. Dobrzański LA, Dobrzański LB, Dobrzańska-Danikiewicz AD, Dobrzańska J. The concept of sustainable development of modern dentistry. Processes. (2020) 8:1605. doi: 10.3390/pr8121605
2. Yadav S, Gangwar S. A critical evaluation of tribological interaction for restorative materials in dentistry. Int J Polym Mater Polym Biomater. (2019) 68:1005–19. doi: 10.1080/00914037.2018.1525544
3. Demarco FF, Cenci MS, Montagner AF, de Lima VP, Correa MB, Moraes RR, et al. Longevity of composite restorations is definitely not only about materials. Dent Mater. (2023) 39:1–12. doi: 10.1016/j.dental.2022.11.009
4. Kaur G, Kaushal R, Prabhakar D. Esthetic restorations and smile designing: a review. Int J Health Sci (Qassim). (2021) 5:10–22. doi: 10.53730/ijhs.v5nS1.5273
5. Hatton PV, Mulligan S, Martin N. The safety and biocompatibility of direct aesthetic restorative materials. Br Dent J. (2022) 232:611–4. doi: 10.1038/s41415-022-4198-6
6. Albelasy EH, Hamama HH, Chew HP, Montaser M, Mahmoud SH. Secondary caries and marginal adaptation of Ion-releasing versus resin composite restorations: a systematic review and meta-analysis of randomized clinical trials. Sci Rep. (2022) 12:19244. doi: 10.1038/s41598-022-19622-6
7. van Dijken JWV, Pallesen U. A randomized 10-year prospective follow-up of class II nanohybrid and conventional hybrid resin composite restorations. J Adhes Dent. (2014) 16:585–92. doi: 10.3290/j.jad.a33202
8. van Dijken JW, Pallesen U. Randomized 3-year clinical evaluation of class I and II posterior resin restorations placed with a bulk-fill resin composite and a one-step self-etching adhesive. J Adhes Dent. (2015) 17:81–8. doi: 10.3290/j.jad.a33502
9. Barata JS, Casagrande L, Pitoni CM, De Araujo FB, Garcia-Godoy F, Groismann S. Influence of gaps in adhesive restorations in the development of secondary caries lesions: an in situ evaluation. Am J Dent. (2012) 25:244–8. 23082391
10. da Rosa Rodolpho PA, Cenci MS, Donassollo TA, Loguércio AD, Demarco FF. A clinical evaluation of posterior composite restorations: 17-year findings. J Dent. (2006) 34:427–35. doi: 10.1016/j.jdent.2005.09.006
11. Krämer N, Kunzelmann K-H, García-Godoy F, Häberlein I, Meier B, Frankenberger R. Determination of caries risk at resin composite margins. Am J Dent. (2007) 20:59–64. 17380810.
12. Opdam NJM, van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, et al. Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res. (2014) 93:943–9. doi: 10.1177/0022034514544217
13. Pinto NS, Jorge GR, Vasconcelos J, Probst LF, De-Carli AD, Freire A. Clinical efficacy of bioactive restorative materials in controlling secondary caries: a systematic review and network meta-analysis. BMC Oral Health. (2023) 23:394. doi: 10.1186/s12903-023-03110-y
14. McCabe JF, Yan Z, Al Naimi OT, Mahmoud G, Rolland SL. Smart materials in dentistry. Aust Dent J. (2011) 56:3–10. doi: 10.1111/j.1834-7819.2010.01291.x
15. van Dijken JWV. Three-year performance of a calcium-, fluoride-, and hydroxyl-ions-releasing resin composite. Acta Odontol Scand. (2002) 60:155–9. doi: 10.1080/000163502753740179
16. Makanjuola J, Deb S. Chemically activated glass-ionomer cements as bioactive materials in dentistry: a review. Prosthesis. (2023) 5:327–45. doi: 10.3390/prosthesis5010024
17. Park EY, Kang S. Current aspects and prospects of glass ionomer cements for clinical dentistry. Yeungnam Univ J Med. (2020) 37:169–78. doi: 10.12701/yujm.2020.00374
18. Saridena USNG, Sanka GSSJ, Alla RK, Ramaraju AV, Mc SS, Mantena SR. An overview of advances in glass ionomer cements. Int J Dent Mat. (2022) 4:89–94. doi: 10.37983/IJDM.2022.4403
19. Kim H-J. Comparative evaluation of bond strength and microleakage of three Ion-releasing restorative materials at various PH levels. Appl Sci. (2022) 12:6796. doi: 10.3390/app12136796
20. Sauro S, Makeeva I, Faus-Matoses V, Foschi F, Giovarruscio M, Maciel Pires P, et al. Effects of ions-releasing restorative materials on the dentine bonding longevity of modern universal adhesives after load-cycle and prolonged artificial Saliva aging. Materials (Basel). (2019) 12:722. doi: 10.3390/ma12050722
21. Aminoroaya A, Neisiany RE, Khorasani SN, Panahi P, Das O, Madry H, et al. A review of dental composites: challenges, chemistry aspects, filler influences, and future insights. Compos B Eng. (2021) 216:108852. doi: 10.1016/j.compositesb.2021.108852
22. Aminoroaya A, Esmaeely Neisiany R, Nouri Khorasani S, Panahi P, Das O, Ramakrishna S. A review of dental composites: methods of characterizations. ACS Biomater Sci Eng. (2020) 6:3713–44. doi: 10.1021/acsbiomaterials.0c00051
23. Cho K, Rajan G, Farrar P, Prentice L, Prusty BG. Dental resin composites: a review on materials to product realizations. Compos B Eng. (2022) 230:109495. doi: 10.1016/j.compositesb.2021.109495
24. Thalacker C. Dental adhesion with resin composites: a review and clinical tips for best practice. Br Dent J. (2022) 232:615–9. doi: 10.1038/s41415-022-4144-7
25. Kumar SR, Patnaik A, Bhat IK. Factors influencing mechanical and wear performance of dental composite: a review. Mat Werk. (2020) 51:96–108. doi: 10.1002/mawe.201900029
26. Simila HO, Boccaccini AR. Sol-Gel bioactive glass containing biomaterials for restorative dentistry: a review. Dent Mater. (2022) 38:725–47. doi: 10.1016/j.dental.2022.02.011
27. Shearer A, Montazerian M, Sly JJ, Hill RG, Mauro JC. Trends and perspectives on the commercialization of bioactive glasses. Acta Biomater. (2023) 160:14–31. doi: 10.1016/j.actbio.2023.02.020
28. Rokaya D, Srimaneepong V, Sapkota J, Qin J, Siraleartmukul K, Siriwongrungson V. Polymeric materials and films in dentistry: an overview. J Adv Res. (2018) 14:25–34. doi: 10.1016/j.jare.2018.05.001
29. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. Br Med J. (2015) 349:g7647. doi: 10.1136/bmj.g7647
30. Booth A, Clarke M, Ghersi D, Moher D, Petticrew M, Stewart L. An international registry of systematic-review protocols. Lancet. (2011) 377:108–9. doi: 10.1016/S0140-6736(10)60903-8
31. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
32. dos Santos MPA, Passos M, Luiz RR, Maia LC. A randomized trial of resin-based restorations in class I and class II beveled preparations in primary molars: 24-month results. J Am Dent Assoc. (2009) 140:156–66. doi: 10.14219/jada.archive.2009.0129
33. Shagale AM, Aby H, Prabhakar A, Bm D, Reddy GS. Clinical performance of equia forte: a glass hybrid GIC versus tetric N ceram; a bulk fill composite in class II carious primary molars: a 12 month split mouth clinical trial. Int J Appl Dent Sci. (2020) 6:435–40. doi: 10.22271/oral.2020.v6.i4g.1098
34. Casagrande L, Dalpian DM, Ardenghi TM, Zanatta FB, Balbinot CEA, García-Godoy F, et al. Randomized clinical trial of adhesive restorations in primary molars. 18-month results. Am J Dent. (2013) 26:351–5. 24640441
35. Alves dos Santos MP, Luiz RR, Maia LC. Randomised trial of resin-based restorations in class I and class II beveled preparations in primary molars: 48-month results. J Dent. (2010) 38:451–9. doi: 10.1016/j.jdent.2010.02.004
36. Burgess JO, Gallo JR, Ripps AH, Walker RS, Ireland EJ. Clinical evaluation of four class 5 restorative materials: 3-year recall. Am J Dent. (2004) 17:147–50. 15301207
37. Neo J, Chew CL. Direct tooth-colored materials for noncarious lesions: a 3-year clinical report. Quintessence Int. (1996) 27:183–8.9063232
38. van Dijken JW. 3-Year Clinical evaluation of a compomer, a resin-modified glass ionomer and a resin composite in class III restorations. Am J Dent. (1996) 9:195–8. 9545903
39. Kaurich M, Kawakami K, Perez P, Munn T, Hasse AL, Garrett NR. A clinical comparison of a glass ionomer cement and a microfilled composite resin in restoring root caries: two-year results. Gen Dent. (1991) 39:346–9. 1839833
40. Osborne JW, Berry TG. 3-year clinical evaluation of glass ionomer cements as class III restorations. Am J Dent. (1990) 3:40–3. 2150170
41. El-Housseiny AA, Alamoudi NM, Nouri S, Felemban O. A randomized controlled clinical trial of glass carbomer restorations in class II cavities in primary molars: 12-month results. Quintessence Int. (2019) 50:522–32. doi: 10.3290/j.qi.a42573
42. de Medeiros Serpa EB, Clementino MA, Granville-Garcia AF, Rosenblatt A. The effect of atraumatic restorative treatment on adhesive restorations for dental caries in deciduous molars. J Indian Soc Pedod Prev Dent. (2017) 35:167–73. doi: 10.4103/JISPPD.JISPPD_98_16
43. Öz E, Kirzioğlu Z. A randomised clinical trial evaluating the clinical performance of compomer and composite materials in class II primary molar restorations: 24 months results. JDMT. (2022) 11:1–10. doi: 10.22038/jdmt.2022.62404.1500
44. Akman H, Tosun G. Clinical evaluation of bulk-fill resins and glass ionomer restorative materials: a 1-year follow-up randomized clinical trial in children. Niger J Clin Pract. (2020) 23:489–97. doi: 10.4103/njcp.njcp_519_19
45. Dermata A, Papageorgiou SN, Fragkou S, Kotsanos N. Comparison of resin modified glass ionomer cement and composite resin in class II primary molar restorations: a 2-year parallel randomised clinical trial. Eur Arch Paediatr Dent. (2018) 19:393–401. doi: 10.1007/s40368-018-0371-7
46. Bektas Donmez S, Uysal S, Dolgun A, Turgut MD. Clinical performance of aesthetic restorative materials in primary teeth according to the FDI criteria. Eur J Paediatr Dent. (2016) 17:202–12. 27759409
47. Sengul F, Gurbuz T. Clinical evaluation of restorative materials in primary teeth class II lesions. J Clin Pediatr Dent. (2015) 39:315–21. doi: 10.17796/1053-4628-39.4.315
48. Pascon FM, Kantovitz KR, Caldo-Teixeira AS, Borges AFS, Silva TN, Puppin-Rontani RM, et al. Clinical evaluation of composite and compomer restorations in primary teeth: 24-month results. J Dent. (2006) 34:381–8. doi: 10.1016/j.jdent.2005.08.003
49. Andersson-Wenckert I, Sunnegårdh-Grönberg K. Flowable resin composite as a class II restorative in primary molars: a two-year clinical evaluation. Acta Odontol Scand. (2006) 64:334–40. doi: 10.1080/00016350600788245
50. Ersin NK, Candan U, Aykut A, Onçağ O, Eronat C, Kose T. A clinical evaluation of resin-based composite and glass ionomer cement restorations placed in primary teeth using the ART approach: results at 24 months. J Am Dent Assoc. (2006) 137:1529–36. doi: 10.14219/jada.archive.2006.0087
51. Hse KM, Wei SH. Clinical evaluation of compomer in primary teeth: 1-year results. J Am Dent Assoc. (1997) 128:1088–96. doi: 10.14219/jada.archive.1997.0366
52. Ahmed B, Wafaie RA, Hamama HH, Mahmoud SH. 3-Year Randomized clinical trial to evaluate the performance of posterior composite restorations lined with Ion-releasing materials. Sci Rep. (2024) 14:4942. doi: 10.1038/s41598-024-55329-6
53. Krishnakumar K, Kalaskar R, Kalaskar A, Bhadule S, Joshi S. Clinical effectiveness of high-viscosity glass ionomer cement and composite resin as a restorative material in primary teeth: a systematic review of clinical trials. Int J Clin Pediatr Dent. (2024) 17:221–8. doi: 10.5005/jp-journals-10005-2757
54. Dias AGA, Magno MB, Delbem ACB, Cunha RF, Maia LC, Pessan JP. Clinical performance of glass ionomer cement and composite resin in class II restorations in primary teeth: a systematic review and meta-analysis. J Dent. (2018) 73:1–13. doi: 10.1016/j.jdent.2018.04.004
Keywords: ion-releasing restoration, composite resin, glass ionomer cement, children, pediatric dentistry, systematic review, meta-analysis, dental materials
Citation: Arbildo-Vega HI, Cruzado-Oliva FH, Vásquez-Rodrigo H, Coronel-Zubiate FT, Alarco-La Rosa LF, Alarco-Jurado LC and Zarate-Chavarry SL (2025) Clinical effectiveness of ion-releasing restorations compared to composite restorations in pediatric dental treatments: a systematic review and meta-analysis. Front. Dent. Med. 6:1651696. doi: 10.3389/fdmed.2025.1651696
Received: 22 June 2025; Accepted: 11 November 2025;
Published: 25 November 2025.
Edited by:
Kitty Jieyi Chen, Sun Yat-sen University, ChinaReviewed by:
Angelo Aliberti, University of Naples Federico II, ItalyDr. Malayka Shah, Karnavati School of Dentistry, India
Aya Saad, Delta University for science and technology, Egypt
Copyright: © 2025 Arbildo-Vega, Cruzado-Oliva, Vásquez-Rodrigo, Coronel-Zubiate, Alarco-La Rosa, Alarco-Jurado and Zarate-Chavarry. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Franz Tito Coronel-Zubiate, ZnJhbnouY29yb25lbEB1bnRybS5lZHUucGU=