 José García Ulerio1,2*†
José García Ulerio1,2*† Mouhanad Al Khatib3
Mouhanad Al Khatib3 Bassma Aammar1,2†
Bassma Aammar1,2† Luca Ragazzoni1,4†
Luca Ragazzoni1,4† Francesco Barone-Adesi1,2†
Francesco Barone-Adesi1,2† Marta Caviglia1,2
Marta Caviglia1,2- 1CRIMEDIM—Center for Research and Training in Disaster Medicine, Humanitarian Aid and Global Health, Università del Piemonte Orientale, Novara, Italy
- 2Department of Translational Medicine, Università del Piemonte Orientale, Novara, Italy
- 3Faculté de Santé, Université de Toulouse, Toulouse, France
- 4Department for Sustainable Development and Ecological Transition, Università del Piemonte Orientale, Vercelli, Italy
Background: Disaster medicine (DM) education has increasingly turned to simulation technologies to address the limitations of traditional training methods. Tools such as virtual reality, mobile applications, and e-learning platforms offer immersive and repeatable learning environments. However, the rapid growth of these tools has outpaced efforts to synthesize how they are being applied, what learning goals they target, and how outcomes are reported.
Objective: This scoping review aimed to map the current evidence on how simulation technologies are used in DM education and training, with a focus on the educational objectives addressed and the types of tools and metrics reported.
Methods: Following the PRISMA-ScR guidelines, a comprehensive search of four databases (PubMed, Scopus, Web of Science, and IEEE Xplore) identified original studies published between 2000 and 2024. Thirty-two studies met the inclusion criteria. Data were charted on the type of technology, training topic, learning group, and evaluation methods.
Results: Mass casualty triage was the most frequently addressed topic. Virtual reality, mobile application, and serious games were the most common modalities. Most studies reported improvements in knowledge, triage accuracy, or learner confidence. However, evaluation strategies varied widely, with most relying on short-term knowledge tests or self-reported confidence. Few studies addressed the realism of the training environments or the integration of digital tools into broader instructions frameworks.
Conclusion: Technology-enhanced DM education shows promise, particularly for immersive triage training. However, inconsistent evaluation practices and limited curricular integration highlight the need for more rigorous, outcome-aligned research to support effective use of simulation technology in this field.
1 Introduction
As the frequency and complexity of disasters continue to increase worldwide (1), the need for competency-based training in disaster response has become more urgent. Educational programs have shown promise in improving disaster readiness (2). However, traditional methods such as lectures and live drills often face logistical and financial constraints, making it difficult to expose learners to realistic scenarios in a safe way (3). This has contributed to growing interest in innovation in educational delivery, particularly through the use of emerging technologies (4).
In recent years, simulation technologies have increasingly been integrated into Disaster Medicine (DM) training to overcome the limitations of traditional methods and expand access to immersive learning experiences. Digital tools such as virtual reality (VR), mobile apps, e-learning platforms, and mixed-reality simulations are increasingly adopted to enhance not only knowledge acquisition, but also practical skills and decision-making under pressure. These technologies have also been explored in multiple domains of disaster management including preparedness, training, and real-time simulation. They offer repeatable exposure to complex scenarios, ease the logistical burden of live drills, provide real-time feedback on learner performance, are generally well received by users in terms of engagement and perceived preparedness (5, 6). Reviews suggest these applications may improve learner immersion, self-efficacy, and preparedness in disaster training.
While the adoption of these tools has been accelerated by broader trends in digital health and simulation, questions remain about how effectively they are being designed, integrated, and aligned with specific learning objectives (7). Furthermore, the growing operational use of simulation technologies in disaster response highlights the need to ensure that training environments mirror the complexity of the real-world systems they intend to prepare learners for.
Despite the growing application of new technologies in DM education, the current body of literature remains fragmented and uneven. Much of the existing research appears to focus on specific tools, with relatively few studies offering broader or comparative perspectives (5).
In addition, there appears to be limited synthesis on how various technologies are applied hacross different educational objectives and on the tools used to evaluate these outcomes. Questions remain about the consistency and rigor of outcome measurement across different modalities and training contexts.
Building on these observations and given the increasing reliance on digital tools in DM training, there is a clear need to map how these simulation technologies are currently being used and evaluated. Thus, we performed a scoping review to understand not only which technologies are being adopted, but also what educational goals they aim to achieve and how their effectiveness is being measured.
2 Methods
2.1 Approach
A scoping review methodology was chosen and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, exclusively with its extension for scoping reviews (PRISMA-ScR) (8), as it allows for the comprehensive mapping of the broad, interdisciplinary body of research on disaster medicine education and training that integrates new technologies for educational purposes. Supplementary Table 1 presents the corresponding PRISMA-ScR Checklist.
Through this approach, we aim to address the following research questions:
• RQ1: What is the current evidence of the utilization of simulation technologies in disaster medicine education and training?
• RQ2: What tools and metrics were used to measure effectiveness of these trainings?
2.2 Eligibility criteria
To ensure a comprehensive review, we included all original studies that reported on technological innovations in DM education. Eligible study designs encompassed experimental, quasi-experimental, mixed-methods, and feasibility studies. The training programs targeted healthcare professionals including physicians, nurses, paramedics, and students or residents, and aimed to develop disaster-related knowledge and skills. Interventions had to incorporate technology-based educational methods, including but not limited to mixed reality, simulation platforms, mobile applications, e-learning tools, gamified systems, smart devices, sensor-based tools, or any communication and information technologies (ICTs). Only peer-reviewed articles published in English from the year 2000 onward were included, with no geographical restrictions.
2.3 Information sources and search strategy
We conducted a comprehensive literature search across four electronic databases: PubMed, Scopus, Web of Science, and IEEE Xplore. The search was conducted in July 2024. It covered publications from January 1, 2000, to the date of the final search.
The search strategy combined terms related to DM and emergency preparedness (e.g., disaster, mass casualty, emergency medicine) with terms related to education and training (e.g., education, training, simulation) and simulation technology (e.g., virtual reality, mobile app, e-learning, ICT, smart, gamification). Boolean operators (AND, OR) and truncation were applied to maximize sensitivity. Supplementary Table 2 presents the implemented search string.
2.4 Selection process and data collection
Following the above eligibility criteria, titles and abstracts were first scanned independently by two reviewers (JGU, MAK), with the support of the software CADIMA (9), to select articles for in-depth analysis if both reviewers agreed upon. This web-based software platform streamlines the screening and data extraction process. After the initial screening process, reviewers assessed the full-text eligibility for inclusion. During the full-text screening phase, studies were selected only if there was an agreement among the reviewers, and a third researcher (BA) acted as arbitrator when there was no consensus. Subsequently, a comprehensive data extraction sheets was created to extract relevant information for thematic analysis. The primary author (JGU) extracted information about each included study, including the first author, publication year, country, study design, the number and type of participants, and details about the intervention. This information encompassed the type of simulation technology used, the comparator, and the training content. Additionally, results regarding the impact of the training and the methods employed to measure this impact, such as metrics and tools, were also collected.
2.5 Data synthesis and analysis
Data from the included studies was collated and tabulated to provide a comprehensive overview of the use of simulation technology in DM education and training. A semi-quantitative analysis using descriptive statistics was conducted to summarize the key characteristics of the studies. After identifying the overall trends, a qualitative synthesis was performed to gain deeper insights into the main topic, as well as the most commonly used tools and metrics.
3 Results
3.1 Search
The search retrieved a total of 1,917 articles from the four databases. After removal of duplicated (n = 598), the titles and abstracts of 1,319 records were screened for eligibility. Of these, 161 articles were selected for full-text review by the authors, resulting in 32 studies that finally met the established inclusion and exclusion criteria to be included in this scoping review. This literature search process is presented in the PRISMA flow-chart (Figure 1).
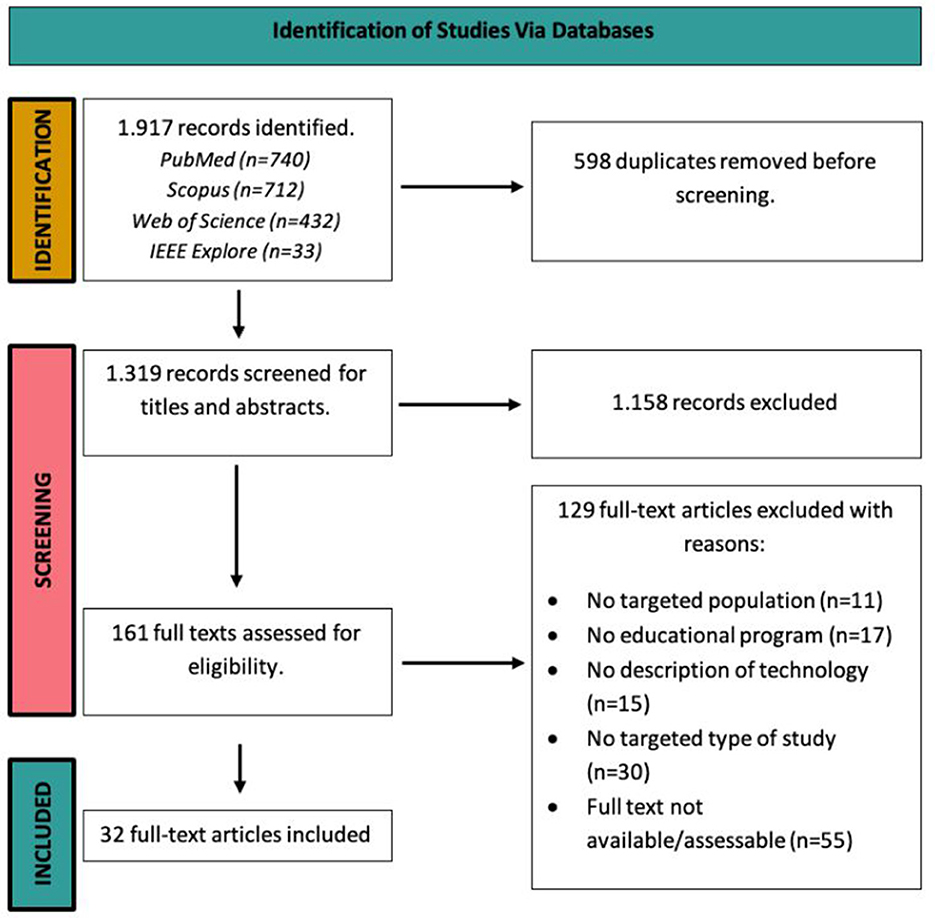
Figure 1. PRISMA flow diagram.
3.2 Study characteristics
Publications date from 2000 to 2024. 16 records were conducted in North America, particularly the United States, while the other half of studies are from East Asia and Europe. Over half of the studies adopted quasi-experimental designs (n = 17) (10–26), others utilized randomized controlled trial design (n = 12) (27–37), feasibility or pilot designs (n = 2) (38, 39) and qualitative methods (n = 1) (40). A comprehensive summary of the extracted data is provided in Table 1.
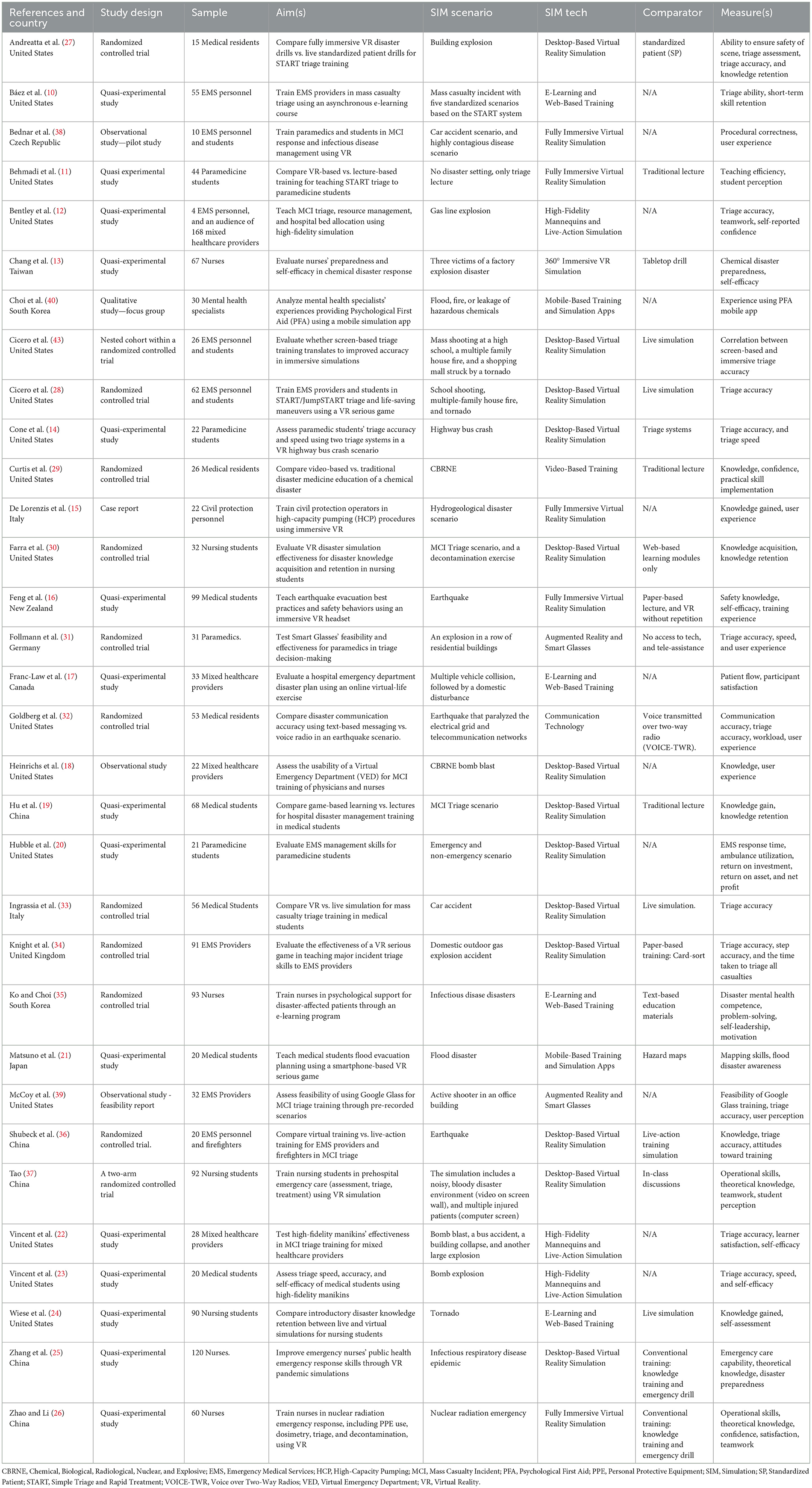
Table 1. Included studies.
Eight studies targeted an audience composed in first place by Emergency Medical Services (EMS) professionals. Following, five studies (16, 21, 22, 33, 41) delivered to undergraduate medical students, four studies to professional nurses (13, 25, 26, 35), three (11, 14, 20) to undergraduate paramedicine students, and other three studies to undergraduate nursing students. One study (40) on mental health specialists, another on professional paramedics, and one last study (15) on civil protection operators. The number of participants per study ranges from 4 to 120. The total number of participants was 1.464 among all studies, professional nurses being the most frequents (n = 340), followed by EMS personnel (n = 300), and medical students (n = 263).
Regarding the content, fifteen training courses aimed to the carrying out of execution of patient triage during MCIs, followed by four studies (13, 18, 26, 29) on decontamination in Chemical, Biological, Radiological, Nuclear, and high yield Explosives (CBRNE) disaster scenarios, and another four (24, 30, 37, 41) on general concepts of disaster management. Two studies (16, 21) on flood and earthquake evacuations, two studies on outbreak/pandemic preparedness (25, 38), and two other studies (35, 40) on mental health support in disasters. Lastly, the studies on hospital disaster preparedness (17), civil protection rescuing procedures (42), and in EMS executive management (20), were the least represented.
Technology-based trainings were primarily delivered using various forms of virtual reality (VR) simulation; from thirteen articles using desktop-based simulation (14, 18, 20, 25, 27, 28, 30, 33, 34, 36, 37, 41, 43), to five studies (11, 15, 16, 26, 38) utilizing fully immersive simulation methods. Successively, e-learning platforms were reported in four articles (10, 17, 24, 35), followed by high-fidelity mannequins (12, 22, 23), augmented reality (31, 39), mobile-based technology (21, 40), 360° immersive simulation (13), video-based trainings (29), and text-based mobile messaging (32). The relationship between technology used and topics taught can be appreciated in Figure 2.
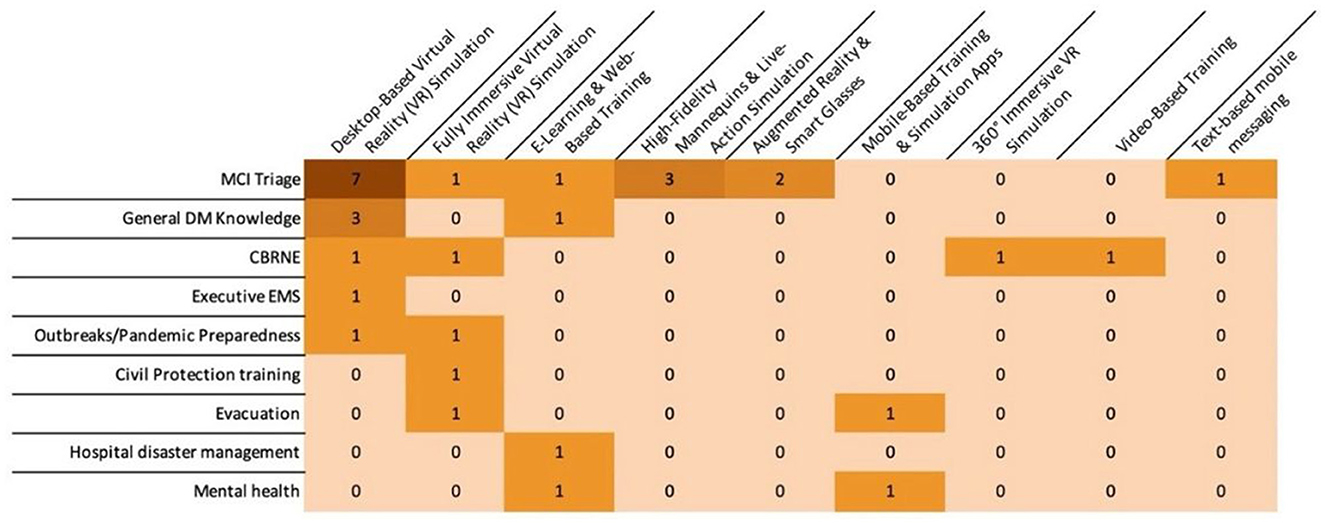
Figure 2. Common topics targeted by simulation technologies in included articles.
Examples of desktop-based simulations range from simple disaster footage projected on screen walls and trainees' individual screen-based multi-patient scenario (30), to the VR system CAVE, which is a full-immersion virtual environment enclosed by walls, floor, and ceiling, creating a realistic replica of a disaster using sophisticated three-dimensional computer-based imaging (27), the serious game “60 Seconds to Survival” (44), a tabletop virtual system (14), the online virtual simulation “Second Life” (45), simulation model of a regional EMS system that replicates the course of action after a 911 call (20), and the XVR training software (33). In these, extended reality (XR) accessories such as joysticks were utilized, and victims were simulated by avatars, sometimes replicating standardized patients. Head-mounted displays and tracking sensors were used by fully immersive simulations, exposing participants to the sensorial challenges of close-to-real disaster scenarios, to train and evaluate their behavior during exercises.
Notably, in all but one of the included studies, participants actively engaged with the technology themselves. In contrast, McCoy et al. (39) assessed the feasibility of a disaster course delivered via tele-simulation. In their study, an instructor used smart glasses to stream a live, interactive MCI scenario while acting as a paramedic evaluating victims and verbalizing key clinical information to remote learners.
Twenty-one studies had a least two training groups, four of which compared a type of virtual reality simulation (fully immersive, 360° immersive, augmented reality, and desktop-based) with traditional lecture sessions (11, 29, 35, 41), and other 11 studies with conventional live training methods (13, 16, 24–27, 33, 34, 36, 43, 44). The remaining five studies implemented a variety of other digital technologies; for instance, e-learning platform were used in two studies comparting with text-based traditional education and live simulation (24, 35). One study used video-based footage to compare CBNRE training performance against traditional lecture (29). Another study compared a text-based messaging mobile application with traditional voice over two-way radio during disaster simulation (32). One study used a mobile-based simulation app comparing with paper-based hazard maps to teach flood evacuation steps (21). Lastly, one study didn't introduce a comparator, rather confronted the performance of both groups on CBNRE disaster scenarios (18).
The remaining 11 articles had only one group that undertook either one or more tech interventions (10, 12, 14, 15, 17, 20, 22, 23, 38–40). Among these, two were feasibility studies of fully immersive and augmented reality (38, 39), and one compared two triage systems using the same desktop-based VR simulation method (SALT vs. SMART) (14).
Finally, it is worth noticing that the included articles revealed a research trend over the last 20 year, accentuated on the study of mass casualty triage, which can be appreciated in Figure 3.
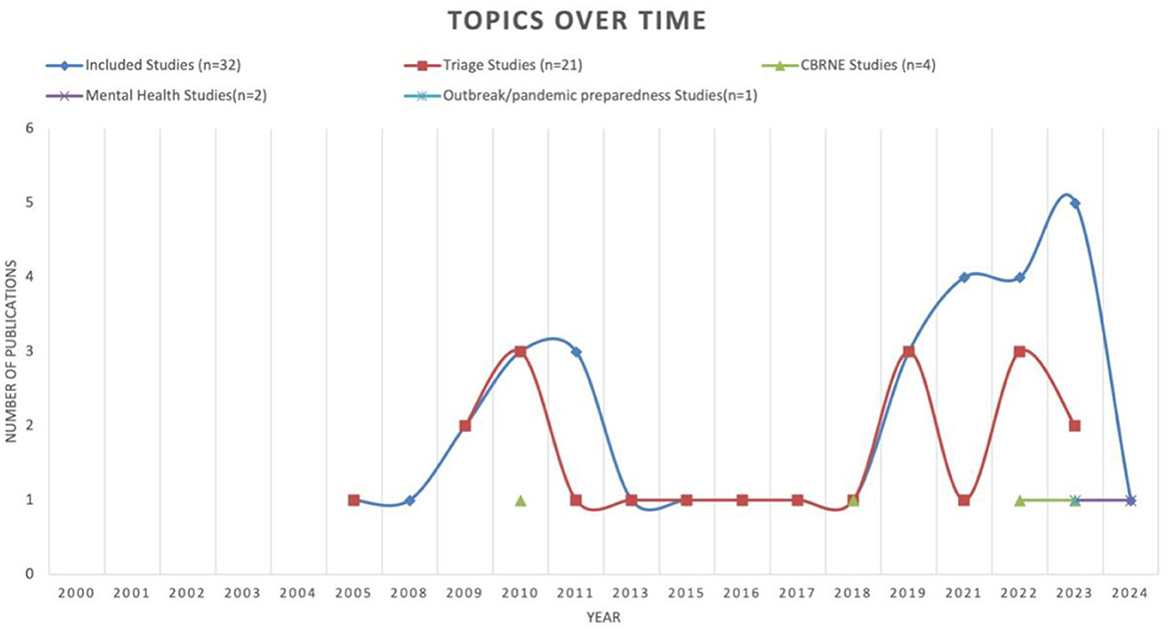
Figure 3. Most studied topics with integration of simulation technologies over time.
3.3 Mass casualty triage
The majority of the studies taught triage, either alone (10–12, 14, 22, 23, 27, 31–34, 36, 39, 43, 44) or in combination with other related content (13, 17, 18, 26, 29, 30, 41). Assessed as triage accuracy and time to triage, alongside with knowledge acquired, treatment/intervention accuracy, and performance correctness, these studies investigated the use of technology-enhanced educational strategies to train healthcare professionals and students in triage protocols under disaster conditions. Table 2 provides an insightful overview of this thematic cluster.
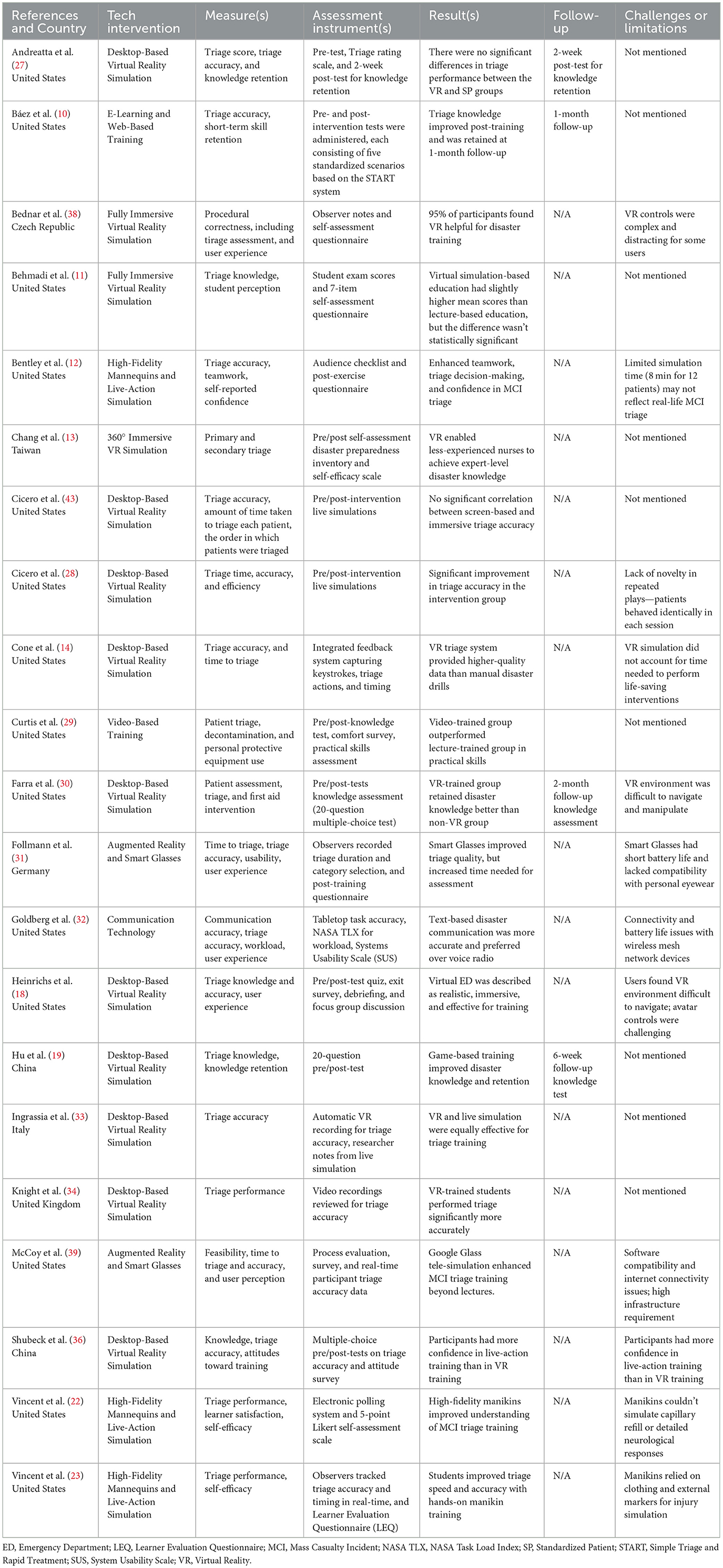
Table 2. Technology-based approaches to mass casualty triage trainings.
Desktop-based virtual reality was the most commonly used single tech to teach triage for MCIs (14, 18, 27, 30, 33, 34, 36, 41, 43, 44). These platforms immersed learners in virtual MCI scenarios where they were required to perform patient assessments, prioritize interventions, and allocate resources. Notably, some VR environments were found to offer better data capture and time-stamped data on triage actions, enhancing the granularity of performance assessment (14), although challenges such as user navigation difficulties (30) and low scenario novelty (44) were also reported.
Fully immersive VR and 360° VR simulations provided a more sensorial engaging experience, used to replicate high-pressure disaster environments. Studies using these methods (11, 13, 38) reported strong user engagement and perceived training value. However, technical barriers such as complex controls, hardware discomfort, and high costs were consistently mentioned. Augmented reality and smart-glasses-based interventions offered in two studies (31, 39) real-time overlays of clinical information or tele-simulation perspectives. These innovations were found to improve decision accuracy and broaden remote training possibilities, yet were limited by battery life, technical compatibility with eyewear, and the need for stable connectivity infrastructure.
E-learning modules (10, 17) and video-based trainings (29) provided more accessible formats for large-scale deployment. These studies showed consistent post-intervention improvements in knowledge and practical application, with Báez et al. reporting skill retention at one-month follow-up (10). Curtis et al. found video-based learners performed better in personal protective equipment (PPE) use and decontamination tasks than those taught via lecture (29). However, these methods lacked the experiential dimension of immersive platforms.
High-fidelity mannequins and live-actions simulations, featured in three studies (12, 22, 23), continued to play a valuable role in the hands-on skills development. While learners reported increased confidence and improved teamwork skills, high-fidelity mannequins were occasionally limited in replicating physiological responses.
Lastly, only one study (32) explored a different approach to disaster communication through text-based messaging mobile application against voice over radio, reaching improved information accuracy during hospital response to an MCI simulation.
In all these virtual environments, a variety of MCI scenarios were simulated, from urban area explosions (12, 13, 22, 23, 27, 31, 34), CBRNE events (18, 26, 29, 30), natural hazards such as earthquakes, floods and tornados (32, 36, 43, 44), mass shootings (39, 43, 44), car crashes (14, 33), and other non-specified MCIs scenarios (10, 11, 30, 41).
Measurements tools and metrics varied across studies. Most used scores, checklists, or pre/post-knowledge tests, while some conducted surveys with Likert scales. One study (18) implemented debriefing and focus group discussion to record participants experiences. Only three articles conducted follow-up assessment within their methods, completing post-test within 2 weeks, 1 month, and 2 months (10, 27, 30).
Comparative studies revealed mixed findings, highlighting either no improvement or no change in improvement in comparison to traditional methods (11, 27, 31, 33, 36, 43). For instance, while Knight et al. and Cicero et al. supported VR's superiority over traditional card-sort or lecture-based training (34, 44), others such as Shubeck et al. found participants preferred live-action training due to its perceived realism and greater emotional engagement (36). Moreover, Follman et al. highlighted a trade-off between quality and efficiency, noting that improvements in triage accuracy with augmented reality technology came at the cost of longer assessment times (31).
4 Discussion
4.1 Summary and key trends
This scoping review synthesized 32 original studies published between 2000 and 2024 that examined the use of technological tools in DM education and training. In doing so, it addressed the primary research question by mapping current evidence on how simulation technologies have been utilized to enhance knowledge acquisition, technical skills development, decision-making, and learners' engagement in disaster settings. The review also provided insights into the secondary research question by analyzing the outcome measures and evaluation strategies used to assess training impact, revealing substantial variability and lack of standardization across studies.
Mass casualty triage was the most prominent topic in the included studies and the over where digital training approaches were most actively developed. Over two-thirds of the included studies addressed triage either as the primary learning objective or as a key element of broader disaster preparedness curricula.
The reviewed studies employed a range of digital modalities to simulate mass casualty incidents and evaluate learners' ability to assess, prioritize, and manage multiple victims. These simulations commonly focused on structured protocols such as START or SALT, and measured outcomes like triage accuracy, speed, and decision-making under pressure.
4.2 Effectiveness and evaluation challenges
Although most studies reported positive short-term outcomes such as improved knowledge or triage accuracy, relatively few demonstrated statistically significant advantages of technology-enhanced methods over traditional pedagogical approaches such as lectures, tabletop exercises, or live-action simulations. Several studies, particularly those comparing VR with traditional simulations, found no significant differences in performance outcomes (27, 33, 43). Moreover, some participants expressed a preference for live-action scenarios, citing higher perceived realism and emotional engagement (36).
Despite the growing interest in simulation technology for DM education, our review found that the evaluation of training effectiveness remains inconsistent and largely unstandardized. Outcome measures across the included studies varied widely, with most relying on short-term knowledge quizzes, self-reported confidence, or simplified checklists. This pattern reflects what Cook et al. (7) described as a recurring challenge in digital learning environments, where the complexity of technologies often outpaces the development of appropriate evaluation frameworks, making it difficult to assess effectiveness beyond superficial metrics (42). In our review, none of the included studies employed structured tools, and only a few used validated instruments or follow-up assessments (30, 41). Several factors may explain this gap, including the lack of disaster-specific evaluation frameworks (46), and practical constraints that favor the use of simple, low-resource assessment methods over validated, behavior-based instruments (47).
At the same time, the increased reliance on simulation-based training is not unique to disaster medicine. Virtual reality and other immersive technologies are being increasingly adopted across health professions education, showing promising results in areas such as cardiopulmonary resuscitation and emergency care training. As highlighted by Trevi et al., simulation is emerging as both an effective and cost-effective modality in broader clinical education contexts (48). This further underscores the urgency of developing robust, transferable evaluation strategies that can be adapted across disciplines and scenarios, including but not limited to disaster response training.
These findings are consistent with those of Voicescu et al. (49), who reported a widespread mismatch between the educational objectives of disaster management programs and the strategies used to evaluate their outcomes. While many programs aimed to develop applied competencies these were often measured using basic tools that capture only surface-level cognitive gains. Our review reinforces this observation in the context of technology-enhanced training: although many interventions sought to build operational triage capabilities or situational awareness through immersive or interactive modalities, their impact was typically assessed using low-resolution, knowledge-based instruments.
4.3 Simulation fidelity and integration
Previous research indicated that simulation fidelity—the extent to which and educational environment replicates real-world conditions—plays an important role in shaping learning outcomes (50). Across several studies in our review, participants reported that immersive VR and high-fidelity simulation environments improved their engagement, emotional involvement, and ability to make rapid triage decisions under pressure (13, 16, 38). These tools commonly provided real-time feedback, sensory immersion, and dynamic scenarios that stimulated the cognitive and emotional challenges of mass causality incidents, supporting faster decision-making and triage. In contrast, desktop-bases simulation and e-learning modules, while useful for foundational knowledge, were often perceived as less realistic and less helpful in preparing learners for the stress and ambiguity of mass casualty incidents (30, 43).
This difference in learner perception aligns with the broader simulation literature, which emphasize that emotional, physical, and conceptual fidelity are essential to effective experiential learning, particularly in high-stakes, team-based scenarios like disaster response. Zechner et al. (51) echoes this in their mixed reality prototype study, demonstrating that the incorporation of realistic environmental cues—such as visual distraction and situational variability—along with adaptive scenario challenges, improved participants' sense of preparedness by more closely replacing the dynamic and unpredictable nature of real–world MCIs. Chang et al. (52) similarly found that tactile feedback from a capillary refill simulator resulted in more accurate diagnostic judgments compared to video–only instruction.
Furthermore, Weinstein et al. (53) concluded that effective MCI simulation must balance high physical conceptual, end emotional fidelity. This assertion is also reflected in our review, suggesting that hybrid and multi-modal formats hold promise, even if they were only explored in a few studies (25, 31).
These converging findings suggest that the effectiveness of technology-enhanced disaster education appears to depend less on the type of technology used and more on how well it is integrated into a coherent, immersive, and learner centered training ecosystem. Rather than novelty or format alone, realism, interactivity, and scenario flexibility appear to be the key drivers of meaningful learning. As digital tools become increasingly accessible and sophisticated, the next challenge may lie in ensuring their use is aligned with clear educational goals and embedded in structured, outcome-based training programs.
4.4 Future research and practice
This review identified triage as both a central of current educational efforts and a key area for future research. Its prominence in literature and operational relevance makes it an ideal testbed for intervention studies.
Notably, no study in this review addressed the use of Artificial Intelligence (AI), Machine learning, or adaptive learning systems is DM education, despite being included in the search strategy. Further research could investigate how AI-enable platforms might support dynamic scenario generation, personalized feedback, or real-time assessment in high-pressure training environments.
To move the field forward, educators and training developers are encouraged not only to adopt emerging technologies, but to integrate them onto pedagogically sound curricula that emphasize realism., feedback, and behavioral assessment. Building on this review, our forthcoming experimental study will examine the use of a mobile application to teach triage principles to medical students using tabletop simulation design.
5 Strengths and limitations
This scoping review offers a comprehensive and timely synthesis of the literature on technology-enhanced DM education, with a specific focus on training content, modality, and outcome evaluation. The inclusion of a wide range of technologies supports a holistic understanding of the field's interdisciplinary landscape. The review also identified triage as a pedagogical priority, setting the stage for targeted intervention studies.
However, several limitations should be acknowledged. As a scoping review, this study did not include a formal appraisal of methodological quality or risk of bias in the included studies. The findings therefore reflect the breadth and distribution of available evidence rather than the strength of individual outcomes. The review was limited to English-language, peer-reviewed literature, potentially excluding relevant studies published in other languages or found in gray literature. Finally, given the rapid pace of technological innovation, it is possible that recently developed tools or training approaches may not be represented in the published literature.
6 Conclusion
This scoping review synthesized the literature on the use of technology in DM education, with mass causality triage emerging as the most frequently addressed topic. While various digital tools have shown promise in enhancing knowledge and decision making, their effectiveness remain inconsistent, and evaluation methods are often limited to short-term or self-reported outcomes.
The review highlights the importance of simulation fidelity, pedagogical integration, alignment between training goals and assessment strategies. These insights inform a future research agenda focused on evidence-based tools. As technology continues to evolve, its role in disaster preparedness must be shaped by both innovation and instructional rigor.
Author contributions
JG: Data curation, Writing – original draft, Conceptualization, Methodology, Investigation, Visualization, Software, Writing – review & editing, Resources, Formal analysis. MA: Software, Writing – review & editing, Methodology, Data curation. BA: Methodology, Data curation, Writing – review & editing, Visualization. LR: Writing – review & editing, Supervision. FB-A: Writing – review & editing, Supervision, Formal analysis. MC: Supervision, Methodology, Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
This manuscript is the outcome of a study conducted within the international PhD Global Health Humanitarian Aid and Disaster Medicine program offered by the Universitá del Piemonte Orientale (UPO).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/femer.2025.1636285/full#supplementary-material
References
1. UNDRR UNOFDRR. GAR Special Report 2024 | UNDRR 2024. (2024). Available online at: https://www.undrr.org/gar/gar2024-special-report (Accessed April 22, 2025).
2. Lin C-H, Tzeng W-C, Chiang L-C, Lu M-C, Lee M-S, Chiang S-L. Effectiveness of a structured disaster management training program on nurses' disaster readiness for response to emergencies and disasters: a randomized controlled trial. J Nurs Manag. (2024) 2024:5551894. doi: 10.1155/2024/5551894
3. Madanian S, Norris T, Parry D. Disaster eHealth: scoping review. J Med Internet Res. (2020) 22:e18310. doi: 10.2196/18310
4. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE Guide No 82. Med Teach. (2013) 35:e1511–1530. doi: 10.3109/0142159X.2013.818632
5. Kao C-L, Chien L-C, Wang M-C, Tang J-S, Huang P-C, Chuang C-C, et al. The development of new remote technologies in disaster medicine education: A scoping review. Front Public Health. (2023) 11:1029558. doi: 10.3389/fpubh.2023.1029558
6. Gout L, Hart A, Houze-Cerfon C-H, Sarin R, Ciottone GR, Bounes V. Creating a novel disaster medicine virtual reality training environment. Prehosp Disaster Med. (2020) 35:225–8. doi: 10.1017/S1049023X20000230
7. Cook DA, Beckman TJ, Thomas KG, Thompson WG. Measuring motivational characteristics of courses: applying Keller's instructional materials motivation survey to a web-based course. Acad Med. (2009) 84:1505–9. doi: 10.1097/ACM.0b013e3181baf56d
8. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
9. Kohl C, McIntosh EJ, Unger S, Haddaway NR, Kecke S, Schiemann J, et al. Online tools supporting the conduct and reporting of systematic reviews and systematic maps: a case study on CADIMA and review of existing tools. Environm Evid. (2018) 7:8. doi: 10.1186/s13750-018-0115-5
10. Báez AA, Sztajnkrycer MD, Smester P, Giraldez E, Vargas LE. Effectiveness of a simple internet-based disaster triage educational tool directed toward Latin-American EMS providers. Prehospital Emergency Care. (2005) 9:227–30. doi: 10.1080/10903120590924555
11. Behmadi S, Asadi F, Okhovati M, Ershad Sarabi R. Virtual reality-based medical education versus lecture-based method in teaching start triage lessons in emergency medical students: Virtual reality in medical education. J Adv Med Educ Prof. (2022) 10:48–53. doi: 10.30476/JAMP.2021.89269.1370
12. Bentley S, Iavicoli L, Boehm L, Agriantonis G, Dilos B, LaMonica J, et al. A simulated mass casualty incident triage exercise: SimWars. MedEdPORTAL. (2023) 15:10823. doi: 10.15766/mep_2374-8265.10823
13. Chang C-W, Lin C-W, Huang C-Y, Hsu C-W, Sung H-Y, Cheng S-F. Effectiveness of the virtual reality chemical disaster training program in emergency nurses: a quasi experimental study. Nurse Educ Today. (2022) 119:105613. doi: 10.1016/j.nedt.2022.105613
14. Cone DC, Serra J. Kurland L. Comparison of the SALT and Smart triage systems using a virtual reality simulator with paramedic students. Eur J Emerg Med. (2011) 18:314–21. doi: 10.1097/MEJ.0b013e328345d6fd
15. De Lorenzis F, Pratticò F, Lamberti F. HCP–VR: training first responders through a virtual reality application for hydrogeological risk management. In: Proceedings of the 17th International Joint Conference on Computer Vision, Imaging and Computer Graphics Theory and Applications. Setúbal: SCITEPRESS - Science and Technology Publications (2022). p. 273–80.
16. Feng Z, González VA, Mutch C, Amor R, Cabrera-Guerrero G. Exploring spiral narratives with immediate feedback in immersive virtual reality serious games for earthquake emergency training. Multimed Tools Appl. (2023) 82:125–47. doi: 10.1007/s11042-022-13306-z
17. Franc-Law JM, Bullard M, Corte FD. Simulation of a hospital disaster plan: a virtual, live exercise. Prehosp Disaster Med. (2008) 23:346–53. doi: 10.1017/S1049023X00005999
18. Heinrichs WL, Youngblood P, Harter P, Kusumoto L, Dev P. Training healthcare personnel for mass- casualty incidents in a virtual emergency department: VED II 2010. Prehosp Disaster Med. 25:424–32. doi: 10.1017/S1049023X00008505
19. Hu H, Lai X, Yan L. Training nurses in an international emergency medical team using a serious role-playing game: a retrospective comparative analysis. BMC Med Educ. (2024) 24:432. doi: 10.1186/s12909-024-05442-x
20. Hubble MW, Richards ME, Wilfong D. Teaching emergency medical services management skills using a computer simulation exercise. Simulation in healthcare. J Soc Simul Healthc. (2011) 6:25–33. doi: 10.1097/SIH.0b013e3182043506
21. Matsuno Y, Fukanuma F, Tsuruoka S. Development of flood disaster prevention simulation smartphone application using gamification. In:Kotsireas IS, Nagurney A, Pardalos PM, Tsokas A, , editors. Dynamics of Disasters. Cham: Springer International Publishing (2021). p. 147–59.
22. Vincent DS, Berg BW, Ikegami K. Mass-casualty triage training for international healthcare workers in the Asia-Pacific region using manikin-based simulations. Prehosp Disaster Med. (2009) 24:206–13. doi: 10.1017/S1049023X00006828
23. Vincent DS, Burgess L, Berg BW, Connolly KK. Teaching mass casualty triage skills using iterative multimanikin simulations. Prehosp Emerg Care. (2009) 13:241–6. doi: 10.1080/10903120802706088
24. Wiese LK, Love T, Goodman R. Responding to a simulated disaster in the virtual or live classroom: is there a difference in BSN student learning? Nurse Educ Pract. (2021) 55:103170. doi: 10.1016/j.nepr.2021.103170
25. Zhang D, Liao H, Jia Y, Yang W, He P, Wang D, et al. Effect of virtual reality simulation training on the response capability of public health emergency reserve nurses in China: a quasiexperimental study. BMJ Open. (2021) 11:e048611. doi: 10.1136/bmjopen-2021-048611
26. Zhao X, Li X. Comparison of standard training to virtual reality training in nuclear radiation emergency medical rescue education. Disaster Med Public Health Prep. (2023) 17:e197. doi: 10.1017/dmp.2022.65
27. Andreatta PB, Maslowski E, Petty S, Shim W, Marsh M, Hall T, et al. Virtual reality triage training provides a viable solution for disaster-preparedness. Acad Emerg Med. (2010) 17:870–6. doi: 10.1111/j.1553-2712.2010.00728.x
28. Cicero MX, Whitfill T, Overly F, Baird J, Walsh B, Yarzebski J, et al. Pediatric disaster triage: multiple simulation curriculum improves prehospital care providers' assessment skills. Prehosp Emerg Care. (2017) 21:201–8. doi: 10.1080/10903127.2016.1235239
29. Curtis HA, Trang K, Chason KW, Biddinger PD. Video-based learning vs traditional lecture for instructing emergency medicine residents in disaster medicine principles of mass triage, decontamination, and personal protective equipment. Prehosp Disaster Med. (2018) 33:7–12. doi: 10.1017/S1049023X1700718X
30. Farra S, Miller E, Timm N, Schafer J. Improved training for disasters using 3-D virtual reality simulation. West J Nurs Res. (2013) 35:655–71. doi: 10.1177/0193945912471735
31. Follmann A, Ohligs M, Hochhausen N, Beckers SK, Rossaint R, Czaplik M. Technical support by smart glasses during a mass casualty incident: a randomized controlled simulation trial on technically assisted triage and telemedical app use in disaster medicine. J Med Internet Res. (2019) 21:e11939. doi: 10.2196/11939
32. Goldberg BS, Hall JE, Pham PK, Cho CS. Text messages by wireless mesh network vs voice by two-way radio in disaster simulations: a crossover randomized-controlled trial. Am J Emerg Med. (2021) 48:148–55. doi: 10.1016/j.ajem.2021.04.004
33. Ingrassia PL, Ragazzoni L, Carenzo L, Colombo D, Gallardo AR. Virtual reality and live simulation: a comparison between two simulation tools for assessing mass casualty triage skills. Eur J Emerg Med. (2015) 22:121–7. doi: 10.1097/MEJ.0000000000000132
34. Knight JF, Carley S, Tregunna B, Jarvis S, Smithies R, De Freitas S, et al. Serious gaming technology in major incident triage training: a pragmatic controlled trial. Resuscitation. (2010) 81:1175–9. doi: 10.1016/j.resuscitation.2010.03.042
35. Ko E, Choi Y-J. Efficacy of a virtual nursing simulation-based education to provide psychological support for patients affected by infectious disease disasters: a randomized controlled trial. BMC Nurs. (2024) 23:230. doi: 10.1186/s12912-024-01901-4
36. Shubeck KT, Craig SD, Hu X. Live-action mass-casualty training and virtual world training: a comparison. Proc Human Fact Ergon Soc Ann Meet. (2016) 60:2103–7. doi: 10.1177/1541931213601476
37. Tao H. Computer-based simulative training system—a new approach to teaching pre-hospital trauma care. J Med College PLA. (2011) 26:335–44. doi: 10.1016/S1000-1948(12)60029-X
38. Bednar M, Dufek P, Lochmannova A, Simon M, Bures M. Use of virtual reality for education and training of emergency rescue system for crisis situations. In: The 15th International Conference on Education Technology and Computers. Barcelona Spain: ACM (2023). p. 142–7.
39. McCoy E, Alrabah R, Weichmann W, Langdorf M, Ricks C, Chakravarthy B, et al. Feasibility of telesimulation and google glass for mass casualty triage education and training. WestJEM. (2019) 20:512–9. doi: 10.5811/westjem.2019.3.40805
40. Choi Y-J, Jung H-S, Choi E-J, Ko E. Disaster healthcare workers' experience of using the psychological first aid mobile app during disaster simulation training. Disaster Med Public Health Prep. (2023) 17:e55. doi: 10.1017/dmp.2021.308
41. Hu H, Liu Z, Li H. Teaching disaster medicine with a novel game-based computer application: a case study at Sichuan University. Disaster Med Public Health Prep. (2022) 16:548–54. doi: 10.1017/dmp.2020.309
42. Cook DA, Ellaway RH. Evaluating technology-enhanced learning: a comprehensive framework. Med Teach. (2015) 37:961–70. doi: 10.3109/0142159X.2015.1009024
43. Cicero MX, Whitfill T, Walsh B, Diaz MCG, Arteaga GM, Scherzer DJ, et al. Correlation between paramedic disaster triage accuracy in screen-based simulations and immersive simulations. Prehospital Emergency Care. (2019) 23:83–9. doi: 10.1080/10903127.2018.1475530
44. Cicero, Md MX, Whitfill, Mph T, Munjal, Md K, et al. 60 seconds to survival: a pilot study of a disaster triage video game for prehospital providers. Am J Disaster Med. (2017) 12:75–83. doi: 10.5055/ajdm.2017.0263
45. Cohen D, Sevdalis N, Taylor D, Kerr K, Heys M, Willett K, et al. Emergency preparedness in the 21st century: training and preparation modules in virtual environments. Resuscitation. (2013) 84:78–84. doi: 10.1016/j.resuscitation.2012.05.014
46. Bahattab AAS, Zain O, Linty M, Amat Camacho N, Von Schreeb J, Hubloue I, et al. Development and evaluation of scenario-based e-simulation for humanitarian health training: a mixed-methods action research study. BMJ Open. (2024) 14:e079681. doi: 10.1136/bmjopen-2023-079681
47. Hartono P, Adiyanto B, Nur RF, Ancilla C, Rahma AZ. Developing an effective team-based emergency training program for medical students. IJAR. (2024) 6:1–13. doi: 10.20473/ijar.V6I12024.1-13
48. Trevi R, Chiappinotto S, Palese A, Galazzi A. Virtual reality for cardiopulmonary resuscitation healthcare professionals training: a systematic review. J Med Syst. (2024) 48:50. doi: 10.1007/s10916-024-02063-1
49. Voicescu GT, Lamine H, Loson, t i AE, Lupan-Muresan EM, Luka S, Ulerio JG, et al. Monitoring and evaluation in disaster management courses: a scoping review. BMC Med Educ. (2025) 25:188. doi: 10.1186/s12909-025-06659-0
50. Carey JM, Rossler K. The How When Why of High Fidelity Simulation. Treasure Island (FL): StatPearls Publishing. (2025).
51. Zechner O, García Guirao D, Schrom-Feiertag H, Regal G, Uhl JC, Gyllencreutz L, et al. NextGen training for medical first responders: advancing mass-casualty incident preparedness through mixed reality technology. MTI. (2023) 7:113. doi: 10.3390/mti7120113
52. Chang TP, Santillanes G, Claudius I, Pham PK, Koved J, Cheyne J, et al. Use of a novel, portable, LED-based capillary refill time simulator within a disaster triage context. Prehosp Disaster Med. (2017) 32:451–6. doi: 10.1017/S1049023X17006343
Keywords: disaster medicine education, simulation technology, virtual reality, mass casualty incidents, mass casualty triage
Citation: García Ulerio J, Al Khatib M, Aammar B, Ragazzoni L, Barone-Adesi F and Caviglia M (2025) Simulation technology use in disaster medicine education and training: a scoping review. Front. Disaster Emerg. Med. 3:1636285. doi: 10.3389/femer.2025.1636285
Received: 27 May 2025; Accepted: 01 July 2025;
Published: 06 August 2025.
Edited by:
Fadi Issa, Harvard Medical School, United StatesReviewed by:
Csaba Dioszeghy, Surrey and Sussex Healthcare NHS Trust, United KingdomGuglielmo Imbriaco, AUSL di Bologna, Italy
Copyright © 2025 García Ulerio, Al Khatib, Aammar, Ragazzoni, Barone-Adesi and Caviglia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José García Ulerio, am9zZS5nYXJjaWF1bGVyaW9AdW5pdXBvLml0
†ORCID: José García Ulerio orcid.org/0009-0002-7559-5347
Bassma Aammar orcid.org/0009-0009-8067-6046
Luca Ragazzoni orcid.org/0000-0002-2528-4375
Francesco Barone-Adesi orcid.org/0000-0003-1550-436X