 Ursula Winterfeld1*
Ursula Winterfeld1* Kenneth Hodson2,3
Kenneth Hodson2,3 Maya Berlin4Benoît Marin5
Maya Berlin4Benoît Marin5 Michael Ceulemans6,7,8Corinna Weber-Schoendorfer9
Michael Ceulemans6,7,8Corinna Weber-Schoendorfer9 François R. Girardin10
François R. Girardin10 David Baud11Béatrice Schaad12,13Alice Panchaud14,15
David Baud11Béatrice Schaad12,13Alice Panchaud14,15- 1Swiss Teratogen Information Service and Clinical Pharmacology Service, Lausanne University Hospital, Lausanne, Switzerland
- 2UK Teratology Information Service, Newcastle uponTyne, United Kingdom
- 3Directorate of Women’s Services, Royal Victoria Infirmary, Newcastle uponTyne, United Kingdom
- 4Clinical Pharmacology and Toxicology Unit, Drug Consultation Center, Shamir Medical Center affiliated with Faculty of Medical & Health Science, Tel Aviv University, Tel Aviv, Israel
- 5Département de Santé Publique, Sorbonne Université, INSERM, Institut Pierre Louis d’Epidémiologie et de Santé Publique, AP-HP, Hôpital Trousseau, Centre de Référence sur les Agents Tératogènes (CRAT), Paris, France
- 6Department of Pharmaceutical and Pharmacological Sciences, Leuven, Belgium
- 7KU Leuven Child & Youth Institute, Leuven, Belgium
- 8IQ Health, Radboud University Medical Center, Nijmegen, Netherlands
- 9Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Pharmakovigilanzzentrum Embryonaltoxikologie, Institut für Klinische Pharmakologie und Toxikologie, Berlin, Germany
- 10Service of Clinical Pharmacology, Department of Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 11Materno-Fetal and Obstetrics Research Unit, Department “Woman-Mother-Child”, Lausanne University Hospital, Lausanne, Switzerland
- 12Communication Department, Lausanne University Hospital, Lausanne, Switzerland
- 13Institute of Humanities in Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 14Service of Pharmacy, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 15Institute of Primary Healthcare (BIHAM), University of Bern, Bern, Switzerland
Medication use during pregnancy is common, yet safety data remain limited, often leading to exaggerated risk perceptions and suboptimal care. Current communication practices are fragmented: product labeling and patient leaflets tend to emphasize potential harms, while specialized resources are underused. We explore the challenges of conveying accurate risk-benefit information and highlight the need for shared decision making. Integrated, evidence-based resources accessible to both healthcare providers and patients can reduce misinformation, improve adherence to essential treatments, and ultimately enhance maternal and child health. The Swiss MAMA-MEDS initiative illustrates how a unified knowledge base can align messaging, address health inequalities, and support patient-centered pregnancy care.
1 Introduction
In 1961, thalidomide as an unforeseen human teratogenic drug led to the exclusion of most women of childbearing potential and pregnant women from clinical trials (Gerbier and Panchaud, 2023). Consequently, our knowledge about drug safety in pregnancy is reliant on observational data collected post-marketing, with a significant time lag between a drug’s initial approval and the availability of essential pharmacokinetic and safety data specific to pregnancy (Gerbier and Panchaud, 2023). The result is highly restrictive drug labelling, often limited to “do not use during pregnancy” or “use with caution during pregnancy” recommendations. Extensive and supportive knowledge about a drug is rarely incorporated into product labelling, whereas study findings linking drugs to malformations are quickly included in package leaflets (Winterfeld et al., 2014; Crettenand et al., 2018). As patients frequently refer to the package leaflet, while healthcare providers (HCP) predominantly rely on the summary of product characteristics (SmPC), this perpetuates the misconception that all drugs are dangerous during pregnancy (Csajka et al., 2014; Sanz et al., 2001). The result is a widespread distortion of the safety information used by HCP to communicate with their patients.
2 Challenges in communicating medication risks during pregnancy
While many medications have not been shown to adversely affect fetal health, certain conditions such as systemic lupus erythematosus, diabetes, or inflammatory bowel disease necessitate careful management during pregnancy. Discontinuing medication may lead to maternal health decline, posing greater risks to the fetus than the potential hazards associated with the medication itself. Thus, optimal disease management during pregnancy is essential for the wellbeing of both mother and child. Medication use is highly prevalent with 27%–93% of women reporting using at least one drug during pregnancy with variations across countries (Mitchell et al., 2011; Lupattelli et al., 2014; Daw et al., 2011). These figures are expected to rise due to higher maternal age at first pregnancy (EUROSTAT, 2021), associated with an increased risk of pre-existing medical conditions and pregnancy complications, and frequent polypharmacy (Fridman et al., 2014; Anand et al., 2023).
The decision to use medication during pregnancy should consider safety data availability, treatment indication, maternal disease severity, and alternative options. In reality, risk perception by both women and HCP are crucial, with studies indicating overestimation of medication-induced malformation risk by both groups (Sanz et al., 2001; Ceulemans et al., 2019). Thus, even when a medication is not expected to adversely affect the health of the fetus, mothers might receive incorrect advice to discontinue essential treatments. This miscommunication poses a serious risk, potentially harming both the mother and child, and, in extreme cases, end in unjustified termination of pregnancy (Schirm et al., 2004; Saha et al., 2015; Einarson et al., 2001a; Polifka and Friedman, 2003; Einarson et al., 2001b). Moreover, regardless of the advice of the HCP, women may choose to discontinue essential medications due to safety concerns or uncertainty about potential adverse effects on the fetus (Watanabe et al., 2021). The overly cautious attitude towards the use of medication during pregnancy is a major issue in communicating medicine, particularly in the field of maternal health and obstetrics. Although the direct impact of communicating distorted information remains relatively unexplored, some evidence of pregnancy disruptive effects has been provided for chronic conditions, such as hypertension, lupus, psychiatric disorders, epilepsy, or inflammatory bowel disease, with observed increase of risk of relapse, hospital admission, and disability in case of avoidance of medication use (Einarson et al., 2001a; Cohen et al., 2004; Cohen et al., 2006; Alcantarilla et al., 2023; Benard-Laribiere et al., 2020; Edey et al., 2014; Leach et al., 2017; Hellwig et al., 2022).
3 Role and limitations of current information sources
Whilst there is still insufficient evidence regarding the safety of medicines during pregnancy, where evidence does exist, it should be communicated and factored into the risk assessment. Experts in this domain gather and disseminate this information through specialized up-to-date sources (Table 1). These resources provide comprehensive data, risk classification, therapeutic alternatives, and practical guidance for pregnancy follow-up. In addition to reference books, websites, such as UKTIS (www.uktis.org), Embryotox (in German) (Embryotox, 2018), and Le CRAT (in French) (CRAT, 2018; Elefant et al., 2014), serve as reliable online sources for HCP and are accessible for everyone free of charge. BUMPs (www.medicinesinpregnancy.org) and MotherToBaby (in English) are directed towards parents, addressing the need for accessible information. HCP, and sometimes patients, can also obtain information and individual risk assessments from Teratology Information Services (TIS) (Chambers, 2011). These centers of expertise provide free information and advice, prospectively collect high quality data on reported cases of exposure and outcomes, and pool these data at a network level (e.g., MotherToBaby, European Network of Teratology Information Services–ENTIS (European Network of Teratology Information, 2011)) to improve knowledge on drug safety during pregnancy (Lurie et al., 2021). Despite the availability of various resources, there is currently no specialized information source tailored to address the information needs of both HCP and patients simultaneously.
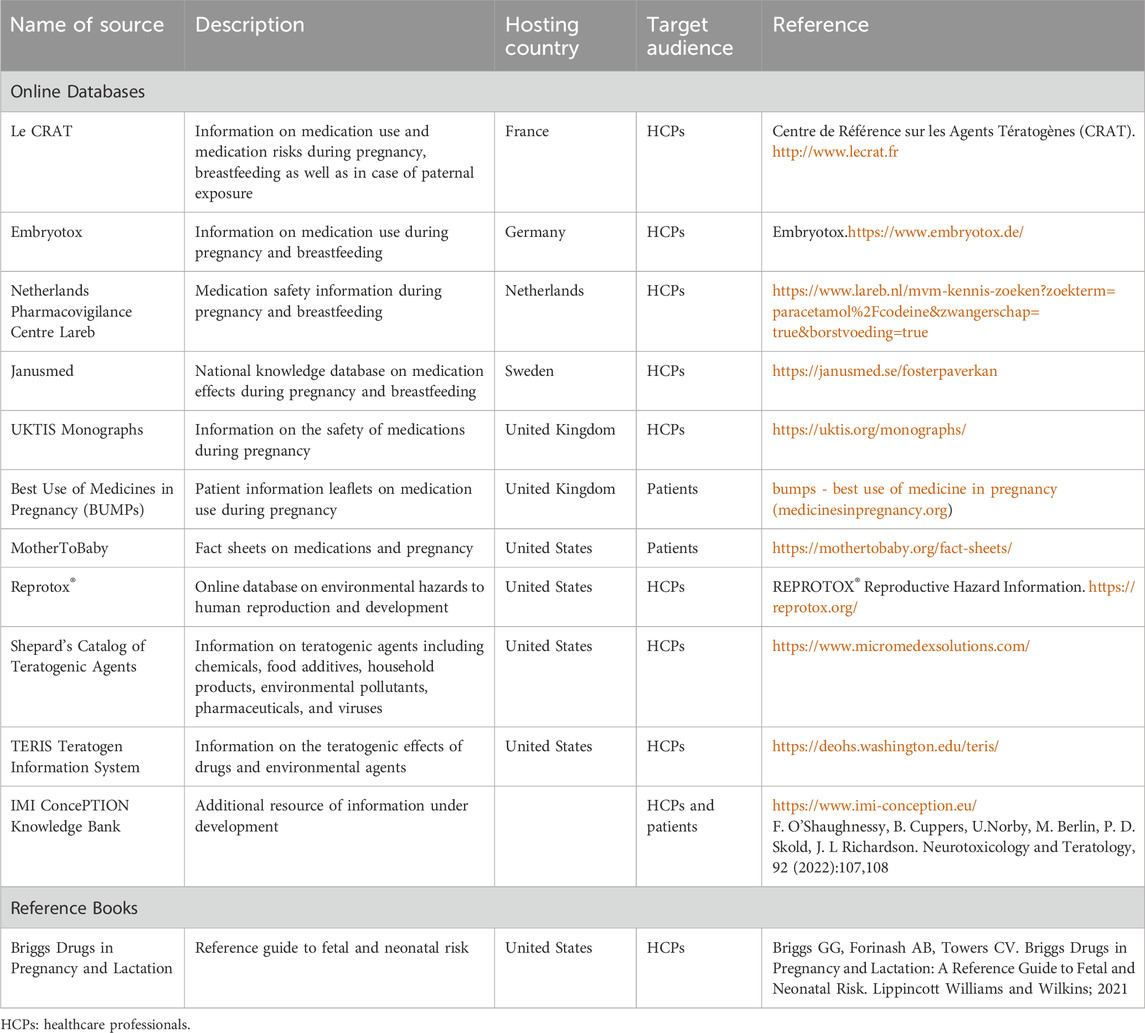
Table 1. Information sources for medication use during pregnancy.
4 Discussion
Although currently lacking, a single data source for HCPs and patients, would promote shared decision-making by encouraging information synergy. Shared decision-making is a collaborative process between patients and their HCP, aimed at reaching joint decisions and broad consensus about care based on evidence and informed personal preferences, health beliefs, and values (NICE, 2018; NICE, 2015). This involves ensuring that patients have a good understanding of the risks, benefits, and possible consequences of different options through discussion and information sharing (Stacey et al., 2024). While the benefits of shared-decision making are increasingly recognized, it is not yet routinely practiced in every setting, particularly within the specific field of medication use during pregnancy. A common information tool for patient and HCP aligns with key steps recommended in shared decision-making implementation frameworks (England, 2022). Providing access to evidence-based, language appropriate information for patients and HCPs empowers individuals to make informed decisions and promotes adherence to evidence-based treatment. A common data source serves as a decision support tool tailored to individuals with varying levels of health literacy, facilitating comprehension of available options and associated benefits, harms, consequences, and burdens. It also helps HCPs and patients to make high-value decisions, such as in pregnancy, where decisions about the use of medicines can have a significant impact on the health of both mother and child. Furthermore, a common data source can serve as a training tool for HCPs, specifically in the context of risk communication, facilitating meaningful shared decision-making conversations. Health informatics must also work to address health inequality that exists within most high-income countries. In the UK, for example, compared to white women, there was a more than three-fold increase in maternal mortality in women from black ethnic backgrounds, and mortality was almost doubled in women from Asian ethnic backgrounds. Furthermore, babies born to these women were more likely to be stillborn, or to die in the neonatal period (MBRRACE-UK, 2022). Communication failures including language barriers, and inadequate information or signposting are common themes cited by women from these communities (Khan et al., 2023). Due to socioeconomic factors, these women have more complex medical needs and so the need to deliver accessible information about medicine use and healthcare in general is imperative.
Addressing gaps in medication risk communication during pregnancy requires resources that are reliable, accessible, and tailored to both healthcare providers and patients. Such tools can strengthen shared decision making, promote informed choices, and improve maternal and child health outcomes. Initiatives like MAMA-MEDS in Switzerland illustrate how these approaches can be put into practice.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
UW: Conceptualization, Writing – original draft, Writing – review and editing. KH: Writing – review and editing. MB: Writing – review and editing. BM: Writing – review and editing. MC: Writing – review and editing. CW-S: Writing – review and editing. FG: Writing – review and editing. DB: Writing – review and editing. BS: Writing – review and editing. AP: Conceptualization, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The research activities of MC are supported by a Senior Postdoctoral Fellowship of the Research Foundation Flanders (FWO, 1246425N).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Correction Note
This article has been corrected with minor changes. These changes do not impact the scientific content of the article.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alcantarilla, L., López-Castro, M., Betriu, M., Torres, A., Garcia, C., Solé, E., et al. (2023). Risk factors for relapse or recurrence in women with bipolar disorder and recurrent major depressive disorder in the perinatal period: a systematic review. Arch. Womens Ment. Health 26 (6), 737–754. doi:10.1007/s00737-023-01370-9
Anand, A., Phillips, K., Subramanian, A., Lee, S. I., Wang, Z., McCowan, R., et al. (2023). Prevalence of polypharmacy in pregnancy: a systematic review. BMJ Open 13 (3), e067585. doi:10.1136/bmjopen-2022-067585
Benard-Laribiere, A., Pambrun, E., Sutter-Dallay, A. L., Gautier, S., Hurault-Delarue, C., Damase-Michel, C., et al. (2020). Impact of pregnancy on antidepressant treatment course: a population-based comparative cohort study in France. Arch. Womens Ment. Health 23 (5), 699–707. doi:10.1007/s00737-020-01033-z
Ceulemans, M., Lupattelli, A., Nordeng, H., Odalovic, M., Twigg, M., and Foulon, V. (2019). Women's beliefs about medicines and adherence to pharmacotherapy in pregnancy: opportunities for community pharmacists. Curr. Pharm. Des. 25(5): 469–482. doi:10.2174/1381612825666190321110420
Chambers, C. (2011). The role of teratology information services in screening for teratogenic exposures: challenges and opportunities. Am. J. Med. Genet. C Semin. Med. Genet. 157C (3), 195–200. doi:10.1002/ajmg.c.30303
Cohen, L. S., Nonacs, R. M., Bailey, J. W., Viguera, A. C., Reminick, A. M., Altshuler, L. L., et al. (2004). Relapse of depression during pregnancy following antidepressant discontinuation: a preliminary prospective study. Arch. Womens Ment. Health 7 (4), 217–221. doi:10.1007/s00737-004-0059-3
Cohen, L. S., Altshuler, L. L., Harlow, B. L., Nonacs, R., Newport, D. J., Viguera, A. C., et al. (2006). Relapse of major depression during pregnancy in women who maintain or discontinue antidepressant treatment. JAMA 295 (5), 499–507. doi:10.1001/jama.295.5.499
CRAT (2018). Centre de Référence sur les Agents Tératogènes (CRAT). Available online at: http://www.lecrat.fr.
Crettenand, M., Rossetti, A. O., Buclin, T., and Winterfeld, U. (2018). Use of antiepileptic drugs during breastfeeding: what do we tell the mother? Nervenarzt 89 (8), 913–921. doi:10.1007/s00115-018-0496-2
Csajka, C., Jaquet, A., Winterfeld, U., Meyer, Y., Einarson, A., and Panchaud, A. (2014). Risk perception by healthcare professionals related to drug use during pregnancy: a Swiss survey. Swiss Med. Wkly. 144, w13936. doi:10.4414/smw.2014.13936
Daw, J. R., Hanley, G. E., Greyson, D. L., and Morgan, S. G. (2011). Prescription drug use during pregnancy in developed countries: a systematic review. Pharmacoepidemiol Drug Saf. 20 (9), 895–902. doi:10.1002/pds.2184
Edey, S., Moran, N., and Nashef, L. (2014). SUDEP and epilepsy-related mortality in pregnancy. Epilepsia 55 (7), e72–e74. doi:10.1111/epi.12621
Einarson, A., Selby, P., and Koren, G. (2001a). Abrupt discontinuation of psychotropic drugs during pregnancy: fear of teratogenic risk and impact of counselling. J. Psychiatry Neurosci. 26 (1), 44–48.
Einarson, A., Selby, P., and Koren, G. (2001b). Discontinuing antidepressants and benzodiazepines upon becoming pregnant. Beware of the risks of abrupt discontinuation. Can. Fam. Physician 47, 489–490.
Elefant, E., Vauzelle, C., and Beghin, D. (2014). Centre de reference sur les agents teratogenes (CRAT): a pioneer center. Therapie 69 (1), 39–45. doi:10.2515/therapie/2014004
Embryotox (2018). Embryotox. Available online at: https://www.embryotox.de/.
england, N. (2022). Shared decision-making: Summary guide. Available online at: https://www.england.nhs.uk/publication/shared-decision-making-summary-guide/.
European network of teratology information (2011). European network of teratology information services (ENTIS). Available online at: https://www.entis-org.eu/.
EUROSTAT (2021). Women in the EU are having their first child later. Available online at: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20210224-1.
Fridman, M., Korst, L. M., Chow, J., Lawton, E., Mitchell, C., and Gregory, K. D. (2014). Trends in maternal morbidity before and during pregnancy in California. Am. J. Public Health 104 (Suppl. 1), S49–S57. doi:10.2105/AJPH.2013.301583
Gerbier, E., and Panchaud, A. (2023). Specialty grand challenge editorial innovative approaches for pharmacoepidemiologic research in pregnancy: shifting the paradigm of Thalidomide’s impact on pregnant women. Front. Drug Saf. Regul. 3, 1187070. doi:10.3389/fdsfr.2023.1187070
Hellwig, K., Tokic, M., Thiel, S., Esters, N., Spicher, C., Timmesfeld, N., et al. (2022). Multiple sclerosis disease activity and disability following discontinuation of natalizumab for pregnancy. JAMA Netw. Open 5 (1), e2144750. doi:10.1001/jamanetworkopen.2021.44750
Khan, Z., Vowles, Z., Fernandez Turienzo, C., Barry, Z., Brigante, L., Downe, S., et al. (2023). Targeted health and social care interventions for women and infants who are disproportionately impacted by health inequalities in high-income countries: a systematic review. Int. J. Equity Health 22 (1), 131. doi:10.1186/s12939-023-01948-w
Leach, J. P., Smith, P. E., Craig, J., Bagary, M., Cavanagh, D., Duncan, S., et al. (2017). Epilepsy and pregnancy: for healthy pregnancies and happy outcomes. Suggestions for service improvements from the multispecialty UK epilepsy mortality group. Seizure 50, 67–72. doi:10.1016/j.seizure.2017.05.004
Lupattelli, A., Spigset, O., Twigg, M. J., Zagorodnikova, K., Mårdby, A. C., Moretti, M. E., et al. (2014). Medication use in pregnancy: a cross-sectional, multinational web-based study. BMJ Open 4 (2), e004365. doi:10.1136/bmjopen-2013-004365
Lurie, Y., Bar, M., Levdov, I. A., Tkachenko, D., Bentur, Y., and Kurnik, D. (2021). Adherence with prescription drugs in pregnant and breastfeeding women consulting with the Israel poison information center teratology service. Clin. Toxicol. (Phila) 59 (6), 457–463. doi:10.1080/15563650.2020.1823405
MBRRACE-UK (2022). Saving lives, improving mothers’ care. Available online at: https://www.npeu.ox.ac.uk/assets/downloads/mbrrace-uk/reports/maternal-report-2022/MBRRACE-UK_Maternal_MAIN_Report_2022_UPDATE.pdf.
Mitchell, A. A., Gilboa, S. M., Werler, M. M., Kelley, K. E., Louik, C., Hernández-Díaz, S., et al. (2011). Medication use during pregnancy, with particular focus on prescription drugs: 1976-2008. Am. J. Obstet. Gynecol. 205 (1), 51 e1–51.e518. doi:10.1016/j.ajog.2011.02.029
NICE (2015). Shared decision making collaborative A consensus statement. Available online at: https://www.nice.org.uk/Media/Default/About/what-we-do/SDM-consensus-statement.pdf.
NICE (2018). N.I.f.H.a.C.E. Evidence review for effectiveness of approaches and activities to increase engagement in shared decision making and the barriers and facilitators to engagement: shared decision making: evidence review A. 2021. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK572433/.
Polifka, J. E., and Friedman, J. M. (2003). Developmental toxicity of ribavirin/IFalpha combination therapy: is the label more dangerous than the drugs? Birth Defects Res. A Clin. Mol. Teratol. 67 (1), 8–12. doi:10.1002/bdra.10020
Saha, M. R., Ryan, K., and Amir, L. H. (2015). Postpartum women's use of medicines and breastfeeding practices: a systematic review. Int. Breastfeed. J. 10, 28. doi:10.1186/s13006-015-0053-6
Sanz, E., Gomez-Lopez, T., and Martinez-Quintas, M. J. (2001). Perception of teratogenic risk of common medicines. Eur. J. Obstet. Gynecol. Reprod. Biol. 95 (1), 127–131. doi:10.1016/s0301-2115(00)00375-4
Schirm, E., Schwagermann, M. P., Tobi, H., and de Jong-van den Berg, L. T. W. (2004). Drug use during breastfeeding. A survey from the Netherlands. Eur. J. Clin. Nutr. 58(2): 386–390. doi:10.1038/sj.ejcn.1601799
Stacey, D., Bennett, C. L., Barry, M. J., Col, N. F., Eden, K. B., Holmes-Rovner, M., et al. (2024). Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst. Rev. 1, CD001431. doi:10.1002/14651858.CD001431.pub6
Watanabe, C., Nagahori, M., Fujii, T., Yokoyama, K., Yoshimura, N., Kobayashi, T., et al. (2021). Non-adherence to medications in pregnant ulcerative colitis patients contributes to disease flares and adverse pregnancy outcomes. Dig. Dis. Sci. 66 (2), 577–586. doi:10.1007/s10620-020-06221-6
Winterfeld, U., Gotta, V., Rothuizen, L. E., Panchaud, A., Rossetti, A. O., and Buclin, T. (2014). Antiepileptics in women of childbearing age and during pregnancy: comparison of specialized information with the current state of knowledge in Germany and Switzerland. Nervenarzt 85 (6), 738–746. doi:10.1007/s00115-014-4091-x
Keywords: medication, pregnancy, risk communication, shared decision making, pharmacovgilance
Citation: Winterfeld U, Hodson K, Berlin M, Marin B, Ceulemans M, Weber-Schoendorfer C, Girardin FR, Baud D, Schaad B and Panchaud A (2025) Communicating medication risks in pregnancy: Towards shared decision making. Front. Drug Saf. Regul. 5:1712216. doi: 10.3389/fdsfr.2025.1712216
Received: 24 September 2025; Accepted: 06 October 2025;
Published: 16 October 2025; Corrected: 22 October 2025.
Edited by:
Wolfgang Paulus, University of Ulm, GermanyReviewed by:
Herbert Juch, Medical University of Graz, AustriaCopyright © 2025 Winterfeld, Hodson, Berlin, Marin, Ceulemans, Weber-Schoendorfer, Girardin, Baud, Schaad and Panchaud. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ursula Winterfeld, dXJzdWxhLndpbnRlcmZlbGRAY2h1di5jaA==