Abstract
Objectives:
“No bed syndrome” has become a familiar phrase in Ghana. Yet, there is very little in medical texts or the peer reviewed literature about it. This review aimed to document what the phrase means in the Ghanaian context, how and why it occurs, and potential solutions.
Design:
A qualitative desk review using a thematic synthesis of grey and published literature, print and electronic media content covering the period January 2014 to February 2021. Text was coded line by line to identify themes and sub-themes related to the research questions. Analysis was manual and with Microsoft Excel to sort themes.
Setting:
Ghana.
Participants and Intervention:
Not applicable.
Results:
“No bed syndrome” describes the turning away by hospitals and clinics of people seeking walk in or referral emergency care with the stated reasons “no bed available” or “all beds are full”. There are reported cases of people dying while going round multiple hospitals seeking help and being repeatedly turned away because there is “no bed”. The situation appears to be most acute in the highly urbanized and densely populated Greater Accra region. It is driven by a complex of factors related to context, health system functions, values, and priorities. The solutions that have been tried are fragmented rather than well-coordinated whole system reform.
Discussions and recommendations:
The “no bed syndrome” describes the challenge of a poorly functioning emergency health care system rather than just the absence of a bed on which to place an emergency case. Many low and middle income countries have similar challenges with their emergency health care systems and this analysis from Ghana is potentially valuable in attracting global attention and thinking about emergency health systems capacity and reform in low and middle income countries. The solution to the “no bed syndrome” in Ghana requires reform of Ghana's emergency healthcare system that takes a whole system and integrated approach. All the components of the health system such as human resource, information systems, financing, equipment tools and supplies, management and leadership need to be examined and addressed together alongside health system values such as accountability, equity or fairness in the formulation, implementation, continuous monitoring and evaluation of policies and programs for system reform to expand and strengthen emergency healthcare system capacity and responsiveness. Despite the temptation to fall back on them as low hanging fruit, piecemeal and ad-hoc solutions cannot solve the problem.
Introduction
Responsiveness is one of the outcome goals of health systems. Responsiveness refers to the outcomes that can be achieved when institutions and institutional relationships in health systems are designed in such a way that they are aware of and respond appropriately to the universal and legitimate expectations of individuals. Responsiveness can be viewed from the angles of encouraging use of the system and safeguarding the right of users to safe and adequate care (1, 2). Responsiveness can also be viewed as a value within health systems (3).
Assured ready access and prompt attention for emergency medical, surgical and obstetric conditions is an important part of responsiveness within health systems. Emergency obstetric referral and care are a critical part of attaining the health-related Sustainable Development Goals (SDG) in Ghana as in much of Sub-Saharan Africa (4–6). Referral has been defined as “a process in which a health worker at one level of the healthcare system, having insufficient resources (drugs, equipment, skills) to manage a clinical condition, seeks the assistance of a better or differently resourced facility at the same or higher level to assist in, or take over the management of, the client's case” (7). Often patients presenting as emergencies have been referred. However, some also are brought in without a referral. Once a case is potentially life-threatening urgent attention should occur regardless of whether a person is brought to a clinic as an emergency with or without a referral.
Ghana developed a referral policy and guidelines in 2012 to help address some of the observed challenges in its referral systems. “The policy covers all types of referrals whether between different facilities or from one department of the same facility to another: and from primary through to tertiary care. It emphasizes the need to avoid delays in access to critical and emergency referral care, rights of referred patients to care and proper documentation of referrals. All public and private health facilities are expected to adhere to the policy and develop operational institutional guidelines to facilitate implementation” (8). Despite the comprehensive referral policy and guidelines Ghana's emergency referral system has been observed to be plagued by many shortcomings (9–12). These affect delivery of quality emergency services to patients, including pregnant women (13, 14). Several factors related to patients, health system and organizational challenges such as inadequate human and material resources, infrastructure, and context have been suggested to account in part at least for this problem. A recurring theme in the media and public discussions of the challenge of providing prompt and timely emergency care is a phenomenon referred to as the “no bed syndrome”. It is cited as contributing to Ghana's relatively high levels of maternal and neonatal mortality particularly in the Greater Accra Region (15, 16). In 2018, the death of a 70-year-old man after being turned away by multiple hospitals made media headlines and brought this issue which had already existed for a few years into acute public attention and triggered a parliamentary enquiry (17, 18).
What exactly is the phenomenon that is labelled as “no bed syndrome” in Ghana? Any resolution to the problem requires a clear understanding of the phenomenon, how and why it occurs and potential as well as actual solutions already tried. To inform ongoing policy discussions and the search for effective solutions a desk review was conducted with the review questions: “what does the term “no bed syndrome” refer to?”; “How and why does the “no bed syndrome” occur”; and “what interventions are in place or have been tried in Ghana to deal with the problem”? Reflecting the nature of the questions being asked the review team was multi-disciplinary with expertise in medical anthropology, clinical care, health policy and systems, communication, and media. The team also had a mix of early, mid-career and senior researchers and practitioners, reflecting the capacity building and use of evidence to inform policy and practice objectives of the project of which this work was a part.
Materials, subjects and methods
The study design was a qualitative desk review using a thematic synthesis approach. Thematic synthesis is an approach to qualitative synthesis that involves coding of text, development of descriptive themes and a synthesis of analytical themes out of these to answer specific questions (19). We reviewed grey and published literature including dissertations, presentations, policies, legislation, administrative reports, and press statements as well as electronic and print media reports covering the period January 2014 (just before the onset of the SDG) to February 2021.
Key words and phrases used in all the searches were: “no bed syndrome”, “no bed”, “emergency care” “access”, “Ghana”, “Sub-Saharan Africa”, “Low- and middle-income countries”. We searched Google, Google scholar and PubMed. For student dissertations we searched the websites of the two oldest universities in Ghana with well-established Schools of Public Health, the University of Ghana and the Kwame Nkrumah University of Science and Technology. We also searched the websites of the Ghana Health Service and the Ministry of Health. The electronic and print media search was done using the Dow Jones Factiva software in March 2021. In Factiva we searched electronic and print media content from six media houses, three public (Graphic Online, Ghanaian Times and the Ghana News Agency) and three private (Daily Guide Network, The Ghanaian Chronicle, and MyJoyonline); and from the Ghana web. We purposively selected these as the most widely used public and private media outlets in Ghana.
Though the phrase “no bed syndrome” has been in widespread use by the media, public, non-medical and medical professionals, legislators, and policy makers in Ghana for several years now our search in the international peer reviewed literature for that phrase alone was not productive for the period of our review. Even as at the time of writing this paper a repeat search on 2 April 2022 in PubMed for the phrase “no bed syndrome” yielded the results “Quoted Phrase not found: No bed syndrome”.
The Google search, grey literature, print and electronic media searches were the main sources of information for answering most of our study questions. This review therefore relies on information from the electronic and print media where the term “no bed syndrome” is used to understand what the terminology refers to and why it is of policy and implementation relevance.
The inclusion criteria were all scholarly articles, grey literature such as press statement, policy briefs and dialogues, media articles within the six newspapers, that contained the search words and within the Ghanaian context. Exclusion criteria were documents that did not write about the no bed syndrome, problems with bed availability in hospitals and clinics, emergency referral access and/or emergency obstetric referral and care in Ghana.
Where abstracts were available, they were first reviewed to decide if the full text merited review. Where there were no abstracts, the full text was reviewed.
The Factiva search yielded 70 print and electronic media records for the search term “no bed syndrome”. The Google search initially turned up 16,400 results which was unmanageable. The search was refined using the search term combination “no bed syndrome” AND “emergency care access” AND “Ghana”. This yielded 37 records all of which were reviewed. Eight records were not relevant to the study based on the exclusion and inclusion criteria and were excluded. The remaining twenty-nine (29) articles, in addition to the seventy (70) media reports were fully reviewed and inform our analysis.
The selected articles were read thoroughly looking for themes and sub-themes related to “no bed syndrome”, emergency care and referral including emergency obstetric referrals. The coding of themes and sub-themes was done manually and then further analysed with text sorting of themes and sub-themes in Microsoft Excel. All analysis was done by the same three team members and reviewed by the others. It was not relevant to appraise quality of studies given the information available on our study questions was mainly from journalistic articles and descriptive studies. Our study questions were moreover about understanding framing and concepts.
We used the enhancing transparency in reporting the synthesis of qualitative research (ENTREQ) guidelines (20) to inform our reporting of results.
Results
What is the “no bed syndrome”?
The Ghanaian phraseology “No bed syndrome” is consistently used to describe a situation in which patients presenting at hospitals and clinics as emergencies are turned away, or asked to move on to another facility without any preliminary examination or management with the reason “no bed available”. Such patients may have been referred from one facility to another as a medical, surgical or obstetric emergency, or been brought directly to a hospital outpatients or emergency room. They may also be brought from the community without a referral in what is perceived to be a medical, surgical or obstetric emergency situation (10, 15, 16, 21, 22).
“ “No bed syndrome” means patients who need emergency care, go through several facilities in Accra seeking medical attention but do not receive care on account of no bed, and eventually leads to the patient's death” (23).
Its occurrence including in emergency obstetric care is most mentioned in the Greater Accra Region (24).
“It is reported that the region is facing what they call “no bed syndrome”, where pregnant women who have referred are moved around from one facility to the other, being rejected on account of no bed. This situation results in the clients finally being attended to when the condition is very critical (15).
Beyond the commonly stated reason when emergency patients are turned away because there is literally no bed available to place the patient on, the phraseology appears to cover underlying other issues often not stated when the patient is turned away. They are issues associated with long standing health system challenges and deficiencies in the state of the emergency healthcare system and the impact on care and outcomes (4, 21, 25–29). The “no bed syndrome” is therefore not just about physical non availability of a hospital bed to place a patient on, even if that is one of the most visible manifestations of inadequate emergency care access and responsiveness it describes. It is rather a complex issue that involves the turning away of clients in urgent need of health care sometimes at multiple points of care which relates to multiple failures and inadequacies of the emergency health care and referral system capacity and functioning.
How and why does the “no bed syndrome” occur?
To understand how and why the “no bed syndrome” occurs is to take a closer look at Ghana's emergency health care system. Figure 1 summarizes the review findings as to how and why the “no bed syndrome” occurs. They can be clustered into three broad categories of factors related to context, health system functions or building blocks, health system values such as equity and responsiveness; and health system priorities such as resource allocation and distribution. Rather than any one factor, the combination of contextual challenges, malfunctioning in aspects of the health system needed to support effective emergency referral systems and care, values and priorities drives the “no bed syndrome” and the related potentially avoidable morbidity, mortality and poor emergency health system responsiveness.
Figure 1
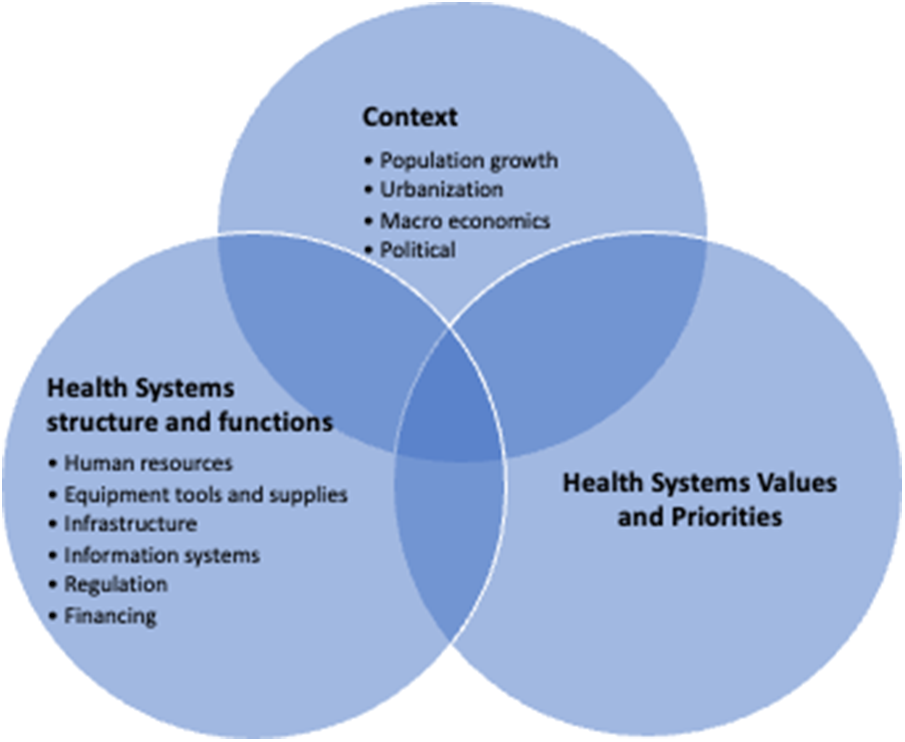
How and why does the “no bed syndrome” occur in Ghana?
Context
Contextual factors influencing the occurrence of the no bed syndrome are related to macro-economic, population, urbanization, and political factors. Ghana's population has grown rapidly in the decades since independence in 1957. Along with population growth has been urbanization (30) and an increasing dual burden of communicable and non-communicable diseases (31). Patients with complications of chronic non communicable conditions such as heart diseases, hypertension and diabetes sometimes have longer hospital stays, increasing bed occupancy rates in an already under-served system. The supply of human resource, infrastructure, equipment, tools, and supplies in the health system has not kept pace with these increases in demand and changes in disease burden. These interrelated factors combine to create a situation of overcrowding and congestion, especially in more densely populated urban areas. This is especially evident in public facilities, which are cheaper and therefore used by more people, with the number of patients outstripping bed and other resource capacities as both emergency and non-emergency cases compete for the limited resources available and have to be attended to in the same space and resource envelope (32). It hampers the ability to provide timely and responsive quality care (33). It also forces frontline health care providers, who in addition to the lack of resources to care for the patient may themselves be exhausted, stressed and frustrated (34), to adopt practices such as turning away clients with the explanation of “no-bed”, as part of coping behaviour.
On the macro-economic front, Ghana's economic growth for many years post-independence was slow, even stagnating or having some downturns in the seventies and eighties and has only picked up in recent years (35). This has limited the availability of government resources to expand capacity.
Political decisions to start and then abandon infrastructure projects related to changes in government emerged in our review as perceived contributors to the inadequate emergency care infrastructure that is one of the drivers of the “no bed syndrome” (24, 36–38). An illustrative example from periodic media reports on this theme is as below:
“The KATH maternity ward project was started in 1974 by the Kutu Acheampong regime but the project has been abandoned by successive governments, resulting in deaths of pregnant women and babies at the facility” (37).
Health system priorities and values
Inadequate prioritization and related underfunding and relative neglect of assuring well distributed and equipped emergency health services by successive governments contributes to the “no bed syndrome”. The Accra Sports Stadium disaster on May 9, 2001, prompted the establishment of a national ambulance service after the findings and recommendation of the official commission of enquiry (38) drew attention to the role the lack of first aid facilities and emergency transportation systems played in the high death toll. Unfortunately, the strengthening of emergency care services appears not to have been carried much beyond the establishment of the national ambulance service (39, 40). As well as the non-existence of a national ambulance services until the early 2000s (9) functional emergency departments were a challenge. Even where emergency departments were set up, they were sometimes below international standards1. Emergency departments were observed to be often left out in the architectural designs of public primary healthcare facilities (24).
Historical and continuing contemporary decisions and prioritization of where to locate facilities may also be contributing to the problem in the densely populated and highly urbanized Greater Accra region where the problem is most acute and visible. The majority of the major referral hospitals such as the Korle-Bu teaching hospital (KBTH), Greater Accra Regional Hospital, 37 Military hospital and the Police hospital, are located in the city centre. The periphery that used to be rural is increasingly almost as urbanised as the centre with health and other infrastructure and services struggling to keep pace with population growth. It is therefore underserved (10).
Health systems functions or building blocks
Interrelated to and working synergistically with the contextual factors are several health system functions or building blocks, related to financing, regulation, information systems and technology, human resources capacity, numbers and distribution, availability of equipment, tools, supplies, infrastructure, and emergency transportation.
Financing
Resource constraints and under funding of the health system generally and emergency care specifically are a longstanding problem (36, 41). Inadequate procurement of tools, equipment and supplies required for emergency health service provision appeared in several media reports on the “no bed syndrome” e.g.
“Government's refusal to increase bed numbers in numerous government hospitals has also propounded the issue of ‘no bed syndrome’ both in general medical emergencies and emergency obstetric care” (42).
These problems were also reported in the media as further compounded by the National Health Insurance Scheme (NHIS) chronic indebtedness to health care facilities for services rendered to clients (29). Provider financial constraints sometimes made it difficult for facilities to restock needed emergency care resources such as medicines and devices. Sometimes when frontline providers turned patients away because of “no bed” it was also because of the of the lack of these other essentials that enable care rather than just the absence of a bed to place the patient on (see footnote 1).
Regulation
Challenges related to various health regulatory bodies in the country such as the Health Facility Regulatory Authority (HeFRA) and Professional Councils such as the Medical and Dental Council (MDC) that are responsible for accreditation, monitoring and supervision towards assuring high quality standards emerged from the review as health system factors contributing to the “no bed syndrome” (see footnote 1). Sometimes the regulatory bodies, also under funded like the rest of the health sector, were unable to fully enforce the regulatory measures required by law. Health care facilities sometimes did not meet required standards or breached emergency referral protocols or process, citing reasons such as scarcity of both human and material resources. The reality of the scarcity of human and other resources sometimes created dilemmas for the regulatory authorities. Without some bending of rules and compromise in a resource constrained system the alternative might be no service at all.
Information systems and technology
Health Management information systems and information technology also emerged as important health system factors through their effect on poor documentation and coordination and communication of referrals between facilities and between emergency transportation and facilities. Inadequate incorporation of Information Technology (IT) innovations in emergency service was cited as contributing to the “no bed syndrome” (41). It appeared a normal practice in emergencies where patients needed to be referred for the attending health providers to call the receiving facility using their personal mobile phone or directing the call for help informally to a friend at the next referral level. This was because of the absence of well-structured systems, such as a call centre that could coordinate, support, and facilitate timely communications for referral in emergencies (8). Other times, patients were just referred to the next level of care without any prior communication with the receiving facility to confirm their ability and readiness to take the case (43).
Human resources for health
Inadequate health staff numbers, skills and distribution also contributed to the “no bed syndrome”. Emergency health care usually requires the efforts of skilled multi-professional teams with ready availability of staff such as anaesthetists, critical care physicians and nurses, surgeons, obstetricians, theatre nurses, and laboratory personnel among others. The very few skilled emergency and critical care staff tended to be concentrated in the teaching and bigger public hospitals located centrally, where they provided care as well as training to medical, nursing and other health care professionals (44) (See footnote 1). Frontline health workers in peripheral facilities multitasked as providers of both emergency and non-emergency care even though they might have little or no training skills and experience for emergency care, given the alterative was often “no care at all” (45). Emergency Medicine, surgery, nursing, and related specialty training opportunities for Ghanaian health professionals are limited (9). Training in emergency medicine and continuous professional development programmes in basic and advanced life support are only now emerging and the supply still needs to develop to meet the demand (9, 39, 46, 47).
Poor motivation and unprofessional attitudes were also reported as driving the “no bed syndrome” in the review (11). These appeared to be often driven by the context and systems. Practices such as poor adherence to emergency care guidelines, sending patients away without trying to triage or provide any kind of first aid were sometimes related to lacking the requisite skills and confidence to manage clients, feeling overwhelmed and worn-out from high workloads. Essential health staff absenting themselves from work, requests for upfront payment for emergency services and staff being disgruntled that they receive few incentives despite their heavy workloads were mentioned as contributors to the “no bed syndrome” (33, 44, 48, 52).
Inadequate monitoring and supervision of frontline providers by management staff were felt by some to be a factor fuelling what were seen as negative attitudes such as turning away emergencies (49). Facility managers on the other hand, sometimes struggled to know how to deal decisively and effectively with the given contextual challenges and somewhat narrow decision-making space. In the public sector human resource management including recruitment and salaries as well as budgets for capital investments such as infrastructure and major equipment are generally centralized. Facility managers are limited in what disciplinary action can be taken against staff indiscipline and may have limited say on priorities for infrastructure development or major equipment purchase. Management sometimes turned a blind eye to problems for fear they would lose critical staff for whom it was not clear where they would find a replacement (50).
Equipment, tools and supplies including emergency transport
Inadequate supplies of emergency drugs, tools, logistics (including beds), laboratories, equipment, infrastructure, and transport emerged frequently as a contributor to the “no bed syndrome”. This included challenges with maintenance of broken-down emergency diagnostic equipment, or procurement of sub-standard quality (33, 43, 44, 51–55). Limited bed availability to meet the increases in patient numbers often resulted in healthcare workers in densely populated urban areas with already overcrowded public sector emergency rooms providing emergency care to patients on floors, benches, and chairs improvised as beds or referring patients to other facilities even when the health professionals with needed expertise to provide care were present in the referring facility (57).
In terms of emergency transportation, though the establishment of a national ambulance service after the 2001 stadium disaster was a major gain, the service remains under-funded and under-equipped in relation to the needs in the country (9). To fill in the gaps, people continue to use other means of transport services such as taxis and private cars to get emergency cases to hospitals and clinics. Sometimes even when available ambulances are challenged by the availability of patient trolleys and other essential ambulance equipment as well as inadequate numbers of trained technicians needed to give first aid and keep patients stable until they got to the referral centre.
In the highly urbanized and densely populated Greater Accra region of Ghana where the “no bed syndrome” has been and remains most visible, there are a multiplicity of private hospitals and clinics. In theory they could help relieve some of the strain in the public sector. However, like the public sector they also appeared to be challenged by inadequately trained human resources, as well as a lack of equipment, tools, and infrastructure for emergency care. It also appeared that concerns about their public image and reputation under these circumstances generated an unwillingness to take risk and a tendency to quickly refer patients with life threatening conditions to the public sector.
What are the existing and potential solutions?
Our review identified several efforts to address directly or indirectly the “no bed syndrome” that have occurred over time in Ghana. Most of these efforts have been done in as fragmented single interventions and piecemeal approaches rather than based on a holistic assessment and a nationally coordinated and well synergized intervention. The efforts we identified from our review were mainly supply-side interventions, namely: administrative directives, health worker training, call centre and teleconsultation-based interventions, and donation of logistics, supplies and emergency transportation, new infrastructure, and software to monitor bed availability and referrals. Demand-side interventions such as rights-based approaches involving seeking legal redress appear to be uncommon (56).
Administrative directives
Following the highly publicized death of a 70-year-old man after being turned away from several hospitals, the Ministry of Health (MOH) and Ghana Health Service (GHS) issued a directive to all public hospitals not to turn away any emergency cases regardless of their bed state. Rather, health facilities should rather aim at stabilizing patients that arrive in their facilities as emergencies and after which arrange for proper transfer to a higher referral hospital for care as needed (44, 63, 65). Public sector health facilities tried to adhere. The challenges that confront the emergency healthcare system such as inadequate numbers, skills and distribution of staff, infrastructure, equipment, tools and supplies were not immediately addressed and it is not clear how effective this directive has been in terms of saving lives since there was no evaluation available.
Health worker training and deployment
In addition, in the wake of the “No Bed Syndrome”, the Ghana Health Service initiated training for medical doctors in basic life support and lifesaving skills under the continuous professional development programme of the Medical and Dental Council. We did not find any evaluation of impact.
One media report mentioned a Medical Outreach and re-deployment programme of doctors from the Korle Bu Teaching Hospital (KBTH) in the Greater Accra Region being deployed to some health facilities to help address the “no bed syndrome” (58).
Call centre and teleconsultation-based interventions
In the Greater Accra region, pilot research has been conducted to establish and evaluate a call centre to coordinate referring and receiving referral facilities and provide up to date information on bed availability. It was targeted at obstetric and new-born referrals but was used for referrals for almost all cases. In the pilot, facilities referring women would call the centre and be guided as to which facilities had the needed expertise and available space to receive the client. The national ambulance service was also alerted to assist with the transportation of emergencies (15). An assessment of the call centre functioning noted the initiative had to a large extent had helped to minimise the effect of “no bed syndrome” on pregnant women and other emergency cases. However, the problems of poor funding and inadequate staffing were among the problems confronting the call centre (59, 60).
In the Amansie West district a teleconsultation program has been piloted that provides decision making support to community health workers for advise on the treatment of their patients, as well as help to manage emergency cases that are beyond their capacity and avoid unnecessary referrals (61). Calls have been made for more or scaled-up versions of these kinds of interventions e.g., (48). Like the other interventions, evaluation of impact on the ultimate outcomes of morbidity and mortality of medical surgical and obstetric emergencies of the teleconsultation-based interventions is currently not available. None of them have been applied at scale across the country.
Some facilities in the country such as Komfo Anokye Teaching Hospital (KATH), Social Security National Insurance Trust Hospital and Legon Hospital resorted to the use of technology to assist them in monitoring and assessing bed availability and referrals. For example, Korle-bu teaching hospital was trialling a pilot project on using a software that allows departments to keep track of beds in the hospital.
Logistics, supplies, infrastructure and emergency transport provision
Governments, individuals, and corporate organisations have periodically donated beds, ambulances, mattresses etc., to different hospitals in various parts of the country (44, 62, 63). For example, the president of the country presented ten thousand hospital beds, under the infrastructure for Poverty Eradication Programme (IPEP), to be distributed to hospitals across the country (64). Sometimes new infrastructure has been commissioned (65). In addition, ambulances were also procured for the National Ambulance Service to increase their fleet numbers, as well as replace ambulances that had broken down. The recurrent costs of running and maintaining the emergency transport system appear to be a challenge, and we found reports of the emergency transportation services needing to demand for money for fuel for example, before patients were transported by ambulances (9).
Discussion
The “no bed syndrome” is popular phraseology used in Ghana to describe the turning away of emergency cases from public and private hospital and clinic outpatient's department (OPD) and emergency rooms with the stated reason “no bed available”. The syndrome is the manifestation of an inadequate emergency health care system. What is known as the “no bed syndrome” in Ghana is effectively a synonym for inadequate emergency health care access. The problem is especially acute in densely populated highly urbanized regions like Greater Accra, where the rapid growth in population from a combination of migration and natural increase has resulted in demand outstripping supply of emergency care infrastructure in a system that was already under-funded and under-capacitated.
Inadequate emergency health care access challenges similar to what we have found in this review are documented from other countries in Sub-Saharan Africa (SSA). For example, a review of key barriers to the provision of emergency and surgical care in Ghana, Kenya, Rwanda, Tanzania and Uganda showed none of the surveyed hospitals had enough infrastructure to follow minimum standards and practices that the World Health Organization considers essential for provision of emergency and surgical care (66).
A systematic review of barriers to access and utilization of Emergency Obstetric Care (EmOC) in SSA found that barriers included lack of emergency obstetric care services and supplies, shortage of trained staff, poor management of emergency obstetric care provision, cost of services, long waiting times, poor referral practices, and poor coordination among staff (67). There are moreover stark inequities in the distribution of the little available. A systematic review of the geographical distribution of EmOC in sub-Saharan Africa showed a concentration of EmOC facilities in capitals, central and urban areas. At least a third of women in the sub-region cannot reach their nearest EmOC facility within the recommended two-hour timeframe (68). Sierra Leone's referral system is described as weak and vulnerable, with 75% of the country having insufficient access to essential health care (69).
Beyond SSA, similar challenges are recorded in some other low-and-lower-middle income countries (LMIC), and in some cases even upper middle and high-income countries – albeit of lower severity than in the LMIC context. Issues that have been found underlying the “why” and “how” of these challenges are similar to some of those we have found in this review of the “no bed syndrome” in Ghana such as human resources including overstretched, stressed and demotivated health workers, information and communication gaps, and inadequate equipment, tools, supplies, and infrastructure (7, 33, 70–73).
These multiple factors work as a tightly linked system rather than individually. “No bed syndrome” is a system problem. Unfortunately, the efforts that have been made to address the problem in Ghana to date appear to be piecemeal rather than an integrated and well synergized systems reform approach. A systems approach needs to address context, political and health system priorities, and values such as equity in access alongside addressing deficiencies in core health system functions or building blocks simultaneously. Addressing deficiencies in core health system functions or building blocks such as information systems and human resources will include agreeing on and adequately equipping public and private hospital emergency rooms with a basic minimum package of modern emergency care equipment to adequately manage emergencies according to international standards. It also requires the development and adequate funding of emergency and critical care training programs for health workers as sub-specialty training options as well as periodic in-service training updates for all frontline staff and managers of emergency rooms and care facilities. Experiences from other settings shows that legislation that imposes sanctions for refusal to offer first aid care to patients with life-threatening conditions before referring them if a facility cannot cope can make a difference (74). However, legislation will be ineffectual if not accompanied by an addressing of the resource challenges that make care unavailable.
Difficult as it is in the resource constrained context of a lower middle-income country like Ghana, more efforts need to be made to ensure adequate numbers of well trained and highly skilled emergency care staff are well distributed across the health system. This will require not only higher enrolment numbers but also better retention strategies such as better working conditions including higher salaries as well as infrastructure, tools and equipment and accessible career development opportunities. This can help to spread workload and reduce provider stress and burnout. It can also reduce referrals to the few relatively better-staffed facilities (in terms of skills and numbers as well as resources including equipment, tools, and supplies), and therefore reduce the likelihood of overwhelming the ability of bigger hospitals to handle emergencies.
The terminology “no bed syndrome” may not be in use outside Ghana but the problem of inadequate emergency health care access is a shared problem across many countries in Sub-Saharan Africa (SSA) and in low- and middle-income countries beyond SSA. This review from Ghana is therefore potentially valuable not only in pointing the way forward for change in Ghana but in other LMIC in SSA and beyond. It can contribute to moving global attention to emergency health care systems capacity and reform in low and middle income countries as part of the global SDG 3 sub-goal of UHC.
Limitations of the study
This review was limited by the lack of research and peer reviewed publications on the specific terminology “no bed syndrome”. However, there was enough information from the grey and published literature and the wide media coverage of the issue in Ghana to provide clarity as to what “no bed syndrome” is and highlight its driving factors, and identify future research agendas that may solve the problem or encourage the monitoring and evaluation of the impact of solutions. Practically it was not possible to review the myriad of print and electronic media available in Ghana and the electronic and print media review focused only on the six high circulation media and the Ghana web. Though often the same story is carried by multiple media, it is possible we have missed some information.
Conclusions
In conclusion:
- (1)
The “no bed syndrome” is a synonym for inadequate emergency health care access and reflects a neglect of emergency and critical health care in the UHC agenda.
- (2)
Integrated systems reform rather piecemeal and fragmented solutions are needed to address the problems.
- (3)
Though this review has focused on Ghana where the neglect of emergency and critical care has now become a problem attracting continuous public, media and legislator attention and scrutiny to the extent that a new terminology has become part of the popular discourse, the underlying problems would appear to be of concern well beyond Ghana.
- (4)
It is time to put emergency medical and surgical as well as obstetric care high on the UHC policy, implementation and research agenda for sub-Saharan Africa.
- (5)
Practically this should include:
- a.
A systems approach that addresses the context, political and health system priorities, values such as equity in access alongside addressing deficiencies in core health system functions or building blocks simultaneously.
- b.
Addressing deficiencies in core health system functions will include agreeing on and adequately equipping public and private hospital emergency rooms with a basic minimum package of modern emergency care equipment to adequately manage emergencies according to international standards.
- c.
Development and adequate funding of emergency and critical care training programs for health workers as sub-specialty training options as well as periodic in-service training updates for all frontline staff and managers of emergency rooms and care facilities.
- d.
Legislation that imposes sanctions for refusal to offer first aid care to patients with life-threatening conditions accompanied by an addressing of the resource challenges that make care unavailable.
- e.
Ensuring adequate numbers of well trained and highly skilled emergency care staff are well distributed across the health system.
- a.
Statements
Author contributions
All authors participated in the conceptualization of the paper. LLY, KAA, JAA, LW and IAA: led the desk review, analysis and writing of the paper. All authors contributed to the article and approved the submitted version.
Funding
The work described here has been funded by IDRC Canada under the project “Catalysing leadership to improve health outcomes for women, adolescents and children in West Africa” Centre file # 108937.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1.^ Ghana College of Physicians and Surgeons. Faculty of Public Health. Public health membership program. Cohort 13, Faculty of Public Health. Health Policy Brief: No Bed Syndrome in GHANA. Ghana College of Physicians and Surgeons. (Unpublished).
References
1.
de Silva A . A framework for measuring responsiveness. GPE discussion paper series: No 32. EIP/GPE/EBD. Geneva: World Health Organization (2000).
2.
Mirzoev T Kane S . What is health systems responsiveness? Review of existing knowledge and proposed conceptual framework. BMJ Glob Health. (2017) 2:e000486. 10.1136/bmjgh-2017-000486
3.
Agyepong IA Kwamie A Frimpong E Defor S Ibrahim A Aryeetey GC et al Spanning maternal newborn and child health (MNCH) and health policy and systems (HPS) boundaries: conducive and limiting health system factors to improving MNCH outcomes in West Africa. Health Res Policy Syst. (2017) 15(Suppl 1):54. 10.1186/s12961-017-0212-x
4.
Ngmenenso S . An evaluation of maternal referrals in the Sissala East District. [master's thesis]. [Accra]: University of Ghana. (2009) http://ugspace.ug.edu.gh/handle/123456789/21694?show=full(Accessed May 1, 2022).
5.
Daniels AA Abuosi A . Improving emergency obstetric referral systems in low and middle income countries: a qualitative study in a tertiary health facility in Ghana. BMC Health Serv Res. (2020) 20:32. 10.1186/s12913-020-4886
6.
Ofosu B Ofori D Ntumy M Asah-Opoku K Boafor T . Assessing the functionality of an emergency obstetric referral system and continuum of care among public healthcare facilities in a low resource setting: an application of process mapping approach. BMC Health Serv Res. (2021) 21(1):402. 10.1186/s12913-021-06402-7
7.
Harahap NC Handayani PW Hidayanto AN . Barriers and technologies of maternal and neonatal referral systems in developing countries: a narrative review. Info Med Unlocked. (2019) 15:100184. 10.1016/j.imu.2019.100184
8.
Ministry of Health Ghana. Ministry of health referral policy and guidelines. Accra: Ministry of Health Ghana (2012). https://www.moh.gov.gh/wp-content/uploads/2016/03/Referral-Policy-Guidelines.pdf(Accessed April 29, 2022).
9.
Frimpong J Dinye R . Ambulance emergency services and healthcare provision in Ghana: a district level performance appraisal. Inter J Health Med Info. (2014) 3(1) https://www.icidr.org/ijhmi-vol3no1-april2014/Ambulance%20Emergency%20Services%20and%20Healthcare%20Provision%20in%20Ghana-A%20District%20Level%20Performance%20Appraisal.pdf (Accessed March 12, 2023).
10.
Haliq A . Referral process and service for expectant mothers and newborns at Shai-Osudoku District Hospital. [master's thesis]. [Accra]: University of Ghana. (2015) http://ugspace.ug.edu.gh/bitstream/handle/123456789/8099/ADAM%20HALIQ_REFERRAL%20PROCESSES%20AND%20SERVICES%20FOR%20EXPECTANT%20MOTHERS%20AND%20_2015.pdf?sequence=1(Accessed 3 May 2022)
11.
Ashinyo M. (2015). Sub District Maternal Referral Practices in Ho Municipality [master's thesis]. [Accra]: University of Ghana. https://ugspace.ug.edu.gh/handle/123456789/8267(Accessed May 1, 2022)
12.
Bailey P Koku Awoonor-Williams J Lebrun V Keyes E Chen M Aboagye P et al Referral patterns through the lens of health facility readiness to manage obstetric complications: national facility-based results from Ghana. Reprod Health. (2019) 16:19. 10.1186/s12978-019-0684-y
13.
Awoonor-Williams JK Bailey PE Yeji F Adongo AE Baffoe P Williams A et al Conducting an audit to improve the facilitation of emergency maternal and newborn referral in northern Ghana. Glob Public Health. (2015) 10(9):1118–33. 10.1080/17441692.2015.1027247
14.
Amoah P Phillips D . Strengthening the referral system through social capital: a qualitative inquiry in Ghana. Healthcare. (2017) 5(4):80. 10.3390/healthcare5040080
15.
Ghana Health Service. (2016). Family Health Division: Annual Report 2016https://www.ghanahealthservice.org/downloads/FHD_2016_ANNUAL_REPORT_Final_June%2019.2017%20nat%20final.pdf(Accessed February 28, 2017).
16.
Akosa AB . ‘No bed’ syndrome, a telling phenomenon of Ghana's health care. Daily Graphic Online. (2018). https://www.graphic.com.gh/features/opinion/no-bedsyndrome-a-telling-phenomenon-of-ghana-s-health-care.html (Accessed October 1, 2020).
17.
Adogla-Bessa D . Man, 70 dies after 7 hospitals rejected him over lack of beds. Citi Newsroom. (2018). https://citinewsroom.com/2018/06/man-70-dies-after-7-hospitals-rejected-him-over-lack-of-beds/ (Accessed December 10, 2020).
18.
TV3 News. Parliament probes how lack of hospital beds led to death of 70 year old man. (2018). https://3news.com/parliament-probes-how-lack-of-hospital-beds-caused-death-of-70-year-old-man/ (Accessed December 11, 2020).
19.
Thomas J Harden A . Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:45. 10.1186/1471-2288-8-45
20.
Tong A Fleming K McInnes E Oliver S Craig J . Enhancing transparency in reporting the synthesis of qualitative research (ENTREQ). BMC Med Res Methodol. (2012) 12:181. 10.1186/1471-2288-12-181
21.
Japiong KB . Preparedness of the Medical Corps of the Ghana Police Service towards emergency management and care: An assessment of the Emergency Unit of the Ghana Police Hospital, Accra. [master's thesis]. [Kumasi]: University of Ghana. (2014) https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.936.7036&rep=rep1&type=pdf (Accessed May 1, 2022).
22.
Daily Guide (Ghana). There Is No Bed. (2016) Accessed via Factiva: https://www.dowjones.com/professional/factiva/.
23.
My Joyonline. (2018). GMA: No bed syndrome is systemic. My Joyonline. https://www.myjoyonline.com/gma-no-bed-syndrome-is-systemic/(Accessed May 1, 2022).
24.
Vanotoo LA . (2019). Predictors of Intrapartum Stillbirths in Singletons in Six Public Hospitals in the Greater Accra Region, Ghana. [thesis]. [Accra]: University of Ghana. http://ugspace.ug.edu.gh/handle/123456789/35705(Accessed May 1, 2022).
25.
Rahman A Shaban A . (2018). Lack of beds forces Ghana's main hospital to reject critical referrals. Africanews EN. https://www.africanews.com/2018/07/11/lack-of-beds-forces-ghanas-main-hospital-to-reject-critical-referrals//(Accessed May 1, 2022).
26.
Tarlue M . Ridge hospital charges patients for toiletries. Daily Guide (Accra). (2015). https://www.modernghana.com/news/601011/ridge-hospital-charges-patients-for-toiletries.html (Accessed December 15, 2020).
27.
Ghana News Agency. Government urged to complete abandoned maternity blocks. (2015). https://www.ghanaweb.com/GhanaHomePage/NewsArchive/Government-urged-to-complete-abandoned-maternity-blocks-358162 (Accessed December 15, 2020).
28.
Modern Ghana. 37 Military hospital attends to more emergency cases. Curled from Ghana News Agency. (2015). https://www.modernghana.com/news/638010/37-military-hospital-attends-to-more-emergency-cases.html (Accessed December 15, 2020).
29.
Zoure S . 12 Babies die at Salaga Hospital. Daily Guide. (2015). https://www.ghanaweb.com/GhanaHomePage/NewsArchive/12-babies-die-at-Salaga-Hospital-380551#:~:text=Poor%20healthcare%20delivery%20at%20the,the%20death%20of%2012%20babies (Accessed December 18, 2020)
30.
Cobbinah PB Erdiaw-Kwasie MO . Urbanization in Ghana: insights and implications for urban governance. In E-planning and collaboration: concepts, methodologies, tools, and applications. Information Management Resources Association (2018). p. 256–78. 10.4018/978-1-5225-5646-6.ch012
31.
GBD Profile Ghana. https://www.healthdata.org/sites/default/files/files/country_profiles/GBD/ihme_gbd_country_report_ghana.pdf(Accessed April 22, 2022).
32.
Quao N Bonney J Forson P Oduro G . Overcrowding in a low resource emergency setting in West Africa: perceptions by health workers in the accident and emergency center, komfo anokye teaching hospital (kath) kumasi, Ghana. Prehosp Disaster Med. (2017) 32(S1):S33–4. 10.1017/S1049023X17001054
33.
Ayamgha B . Korlebu-Teaching hospital board inaugurated. Ministry of Health Public Relations Unit (Accra). (2018). https://gna.org.gh/2021/10/moh-inaugurates-governing-board-of-korle-bu-teaching-hospital/ (Accessed December 21, 2020).
34.
Aberese Ako M van Djik H Gerrits T Arhinful DK Agyepong IA . Your health our concern, our health whose concern?”: perceptions of injustice in organizational relationships and processes and frontline health worker motivation in Ghana. Health Policy Plan. (2014) 29(Supplement 2):ii15–28. 10.1093/heapol/czu068
35.
Agyepong IA . Universal health coverage: breakthrough or great white elephant. Lancet. (2018) 392(10160):2229–36. 10.1016/s0140-6736(18)32402-4
36.
Newton R . Who are we? Daily Guide (Accra). (2018). https://dailyguidenetwork.com/who-are-we/ (Accessed December 18, 2020).
37.
My Joyonline. (2019). Government signs 138.5 m contract to complete KATH maternity block. https://www.myjoyonline.com/government-signs-a¬1385m-contract-to-complete-kath-maternity-block/(Accessed May 1, 2022).
38.
Accra Sports Stadium Disaster Commission of Inquiry. (2001). Ernest Aryeetey, Centre for Policy Analysis (Accra, Ghana), E. V. Doku, Tom K. Kumekpor, Food and Energy Security Foundation (Ghana), J. E. J. M. van Landewijk. Final Report: Presented to His Excellency President John Agyekum Kufuor at State House, Accra, Ghana. Selected Economic Issues, Centre for Policy Analysis (Accra, Ghana). ISBN: 9080184128, 9789080184121
39.
Osei-Ampofo M Oduro G Oteng R Zakariah A Jacquet G Donkor P . The evolution and current state of emergency care in Ghana. Afr J Emerg Med. (2013) 3:52–8. 10.1016/j.afjem.2012.11.006
40.
Oduro GD . Improving emergency care in Ghana. Postgraduate Med J Ghana. (2015) 4(1):23–9. Available at: https://journal.gcps.edu.gh/index.php/pmjg/article/view/81
41.
Larbie S . Korle-Bu teaching hospital to expand its facilities next year. Ghana News Agency. (2019). https://newsghana.com.gh/korle-bu-teaching-hospital-to-expand-its-facilities-next-year/ (Accessed December 18, 2020).
42.
Ghana News Agency. Upgrade Tema general hospital to regional status'Dr Edusei Poku. (2018). https://www.thepublisheronline.com/upgrade-tema-general-hospital-to-regional-status/ (Accessed December 19, 2020).
43.
Okertchiri JA . Implement Emergency Guidelines GMA Tells MOH. Daily Guide. (2018). https://dailyguidenetwork.com/implement-emergency-guidelines-gma-tells-moh/ (Accessed December 16, 2020).
44.
Asante C . Assessment of the triage system at the emergency department of the Greater Accra regional hospital. [master's thesis]. [Accra]: University of Ghana (2019).
45.
Goodman DM Srofenyoh EK Ramaswamy R Bryce F Floyd L Olufolabi A et al Addressing the third delay: implementing a novel obstetric triage system in Ghana. BMJ Global Health. (2018) 3(2):e000623. 10.1136/bmjgh-2017-000623
46.
Ghana Business News. (2015). Ghana establishes first emergency medicine training programme in West Africa. https://www.ghanabusinessnews.com/2015/04/13/ghana-establishes-first-emergencymedicine-training-programme-in-west-africa/ (Accessed August 11, 2021).
47.
Klufio C Kwawukume EY Danso KA Sciarra J Johnson T . Ghana Postgraduate obstetrics/gynecology collaborative residency training program: success story and model for Africa. Am J Obstet Gynecol. (2003) 189(3):692–6. 10.1067/S0002-9378(03)00882-2
48.
Ghana News Agency. We need toll free lines to deal with “no-bed syndrome”- MP. (2018). http://www.businessghana.com/site/news/General/166803/We-need-toll-free-lines-to-deal-with-no-bed-syndrome-MP (Accessed December 16, 2020).
49.
Badu-Agyei B. MP Calls for specialized hospitals to address emergency healthcare. Accra: Ghana News Agency. (2018) https://ghheadlines.com/agency/ghana-business-news/20180620/80489613/mp-calls-for-specialized-hospitals-to-address-emergency-healthcare (Accessed December 10, 2020).
50.
Aberese-Ako M Agyepong IA van Dijk H . Leadership styles in two Ghanaian hospitals in a challenging environment. Health Policy Plan. (2018) 33:ii16–26. 10.1093/heapol/czy038
51.
Japiong KB Asiamah G Owusu-Dabo E Donkor P Stewart B Ebel BE et al Availability of resources for emergency care at a second-level hospital in Ghana: A mixed methods assessment. Afr J Emerg Med. (2016) 6(1):30–7. 10.1016/j.afjem.2015.06.006
52.
DeWulf A Otchi E Soghoian S . Identifying priorities for quality improvement at an emergency department in Ghana. BMC Emerg Med. (2017) 17:28. PMID: 28854879.
53.
Tenyah-Ayettey L . A-Plus saga: the inside story. Accra: Daily Guide. (2017) https://upghana.com/40694/a-plus-saga-the-inside-story (Accessed December 16, 2020).
54.
Daily Guide. Korle-Bu Receives Emergency Beds. (2018) https://dailyguidenetwork.com/korle-bu-receives-emergency-beds/ (Accessed December 16, 2020).
55.
Morhee RAS Sosoo F Morhee ESK . Human rights-based approach to reducing preventable maternal deaths in Ghana: a six-year review of media reports. Ghana J Devel Studies. (2019) 6(3). 10.4314/gjds.v16i3.7
56.
Okertchiri JA Odonkor JN . GHS Cracks whip on ‘No bed’ syndrome. Accra: Daily Guide. (2018). https://dailyguidenetwork.com/ghs-cracks-whip-on-no-bed-syndrome/ (Accessed December 21, 2020).
57.
Ngnenbe T Adu P . No bed syndrome: korle-bu deploys doctors to handle emergency cases. Accra: Graphic Online (2018). https://www.graphic.com.gh/news/general-news/no-bed-syndrome-korle-bu-deploys-doctors-to-handle-emergency-cases.html#:~:text=The%20Korle%20Bu%20Teaching%20Hospital,hit%20hospitals%20in%20the%20country%20 (Accessed December 13, 2020).
58.
Richardson S . Risk recognition: rationing emergency department care as a response to overcrowding. Prehosp Disaster Med. (2017) 32(Suppl. 1):s33–s34. 10.1017/S1049023X17001054
59.
Frimpong E Oduro-Mensah E Vanotoo L Agyepong IA . An exploratory case study of the organizational functioning of a decision-making and referral support call center for frontline providers of maternal and new born care in the greater Accra region of Ghana. Inter J Health Plan Manag. (2018) 33(4):e1112–23. 10.1002/hpm.2595
60.
Oduro-Mensah E Agyepong I Frimpong E Zweekhorst M Vanotoo L . Implementation of a referral and expert advice call center for maternal and newborn care in the resource constrained health system context of the greater Accra region of Ghana. BMC Pregnancy Childbirth. (2021) 21(1). 10.1186/s12884-020-03534-2
61.
The Novartis Foundation. Ghana Telemedicine. https://www.novartisfoundation.org/past-programs/digital-health/ghana-telemedicine (Accessed May 1, 2022).
62.
Arko C . MPs call for increased support for korle-bu teaching hospital. Amsterdam: Elsevier Ghana News Agency (2018). https://www.businessghana.com/site/news/General/168757/MPs-call-for-increased-support-for-Korle-Bu-teaching-Hospital (Accessed December 16, 2020)
63.
Ghana News Agency. Community three livestock farmers association to adopt tema manhean polyclinic. Amsterdam: Elsevier Ghana News Agency (2018). https://www.businessghana.com/site/news/General/170521/Community-Three-Livestock-farmers-Association-to-adopt-Tema-Manhean-Polyclinic (Accessed December 13, 2020).
64.
Graphic online. President presents 10,000 beds to MoH. Amsterdam: Elsevier Peace fmonline (2020). https://www.graphic.com.gh/news/health/president-presents-10-000-beds-for-distribution-to-hospitals.html (Accessed December 22, 2020).
65.
Ghana News Agency. New accident and emergency center commissioned at Korlebu. Amsterdam: Elsevier Ghana News Agency (2018). https://www.ghanaweb.com/GhanaHomePage/NewsArchive/Korle-Bu-s-new-Accident-and-Emergency-Centre-opens-on-Friday-669676 (Accessed December 13, 2020).
66.
Hsia RY Naboth A Mbembati NA Sarah Macfarlane S Margaret E Kruk ME . Access to emergency and surgical care in sub-saharan Africa: the infrastructure gap. Health Policy Plan. (2012) 27:234–44, Advance Access publication 26 March 2011. 10.1093/heapol/czr023
67.
Geleto A Chojenta C Musa A Loxton D . Barriers to access and utilization of emergency obstetric care at health facilities in sub-saharan Africa: a systematic review of literature. Syst Rev. (2018) 7(1):183. 10.1186/s13643-018-0842-2
68.
Banke-Thomas A Wright K Collins L . Assessing geographical distribution and accessibility of emergency obstetric care in sub-saharan Africa: a systematic review. J Glob Health. (2019) 9(1):010414. 10.7189/jogh.09.010414
69.
Ragazzoni L Caviglia M Rosi P Buson R Pini S Merlo F et al Designing, implementing, and managing a national emergency medical service in Sierra Leone prehosp. Disaster Med. (2021) 36(1):115–20. 10.1017/S1049023X20001442.Epub2020 Dec 1.
70.
Bailey P Keyes E Parker C Abdullah M Kebede H Freedman L . Using a GIS to model interventions to strengthen the emergency referral system for maternal and newborn health in Ethiopia. Inter J Gynecol Obstet. (2011) 115:300–9. 10.1016/j.ijgo.2011.09.004
71.
Gula P Karwan K . Increased burdens of emergency departments—organizational challenges. Prehosp Disaster Med. (2017) 32(Suppl. 1):s33–4. 10.1017/S1049023X17001078
72.
Pittalis C Brugha R Gajewski J. et al Surgical referral systems in low- and middle-income countries: a review of the evidence. PLoS One. (2019) 14(9). 10.1371/journal.pone.0223328
73.
Singh S Doyle P Campbell OM Mathew M Murthy GV . Referrals between Public Sector Health Institutions for Women with Obstetric High Risk, Complications, or Emergencies in India – A Systematic Review. PLoS One. (2016) 11(8):e0159793. 10.1371/journal.pone.0159793
74.
Zibulewsky J . The emergency medical treatment and active labor act (EMTALA): what it is and what it means for physicians. Proc (Bayl Univ Med Cent). (2001) 14(4):339–46. 10.1080/08998280.2001.11927785
Summary
Keywords
emergency medical services, health system, Ghana, no bed syndrome, health priorities
Citation
Yevoo LL, Amarteyfio KA, Ansah-Antwi JA, Wallace L, Menka E, Ofori-Ansah G, Nyampong I, Mayeden S and Agyepong IA (2023) The “No bed syndrome” in Ghana — what, how and why? A literature, electronic and print media review. Front. Health Serv. 3:1012014. doi: 10.3389/frhs.2023.1012014
Received
04 August 2022
Accepted
03 March 2023
Published
10 May 2023
Volume
3 - 2023
Edited by
Godfrey Mubyazi, National Institute of Medical Research, Tanzania
Reviewed by
Polina Anang, University of Manitoba, Canada Prince Peprah, University of New South Wales, Australia
Updates
Copyright
© 2023 Yevoo, Amarteyfio, Ansah-Antwi, Wallace, Menka, Ofori-Ansah, Nyampong, Mayeden and Agyepong.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
* Correspondence: Irene Akua Agyepong iagyepong@gcps.edu.gh
ORCID Linda Lucy Yevoo orcid.org/0000-0003-2309-2158 Kezia Amerley Amarteyfio orcid.org/0009-0005-0383-7927 Irene Akua Agyepong orcid.org/0000-0002-0193-5882
Specialty Section: This article was submitted to Health Policy and Management, a section of the journal Frontiers in Health Services
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.