 Camilla Anker-Hansen1*
Camilla Anker-Hansen1* Liv Berit Olsen1
Liv Berit Olsen1 Vigdis Abrahamsen Grøndahl1
Vigdis Abrahamsen Grøndahl1 Ann-Chatrin Linqvist Leonardsen1Ann Karin Helgesen1Carina Bååth1,2Liv Halvorsrud3Gea Restad1
Ann-Chatrin Linqvist Leonardsen1Ann Karin Helgesen1Carina Bååth1,2Liv Halvorsrud3Gea Restad1 Brendan McCormack4
Brendan McCormack4 Ingrid Femdal1
Ingrid Femdal1
- 1Department of Nursing, Health and Bioengineering, Faculty of Health, Welfare and Organization, Østfold University College, Halden, Norway
- 2Faculty of Health, Science and Technology, Karlstad University, Karlstad, Sweden
- 3Faculty of Health Science, Oslo Metropolitan University, Oslo, Norway
- 4Susan Wakil School of Nursing and Midwifery, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia
Background: Implementing a person-centered approach in nursing homes can significantly improve patient satisfaction and care quality while also enhancing job satisfaction among healthcare staff. Leaders play a pivotal role in establishing and nurturing a culture that supports person-centered practices. While there is some empirical evidence, a more comprehensive understanding of how leaders effectively foster and sustain person-centered practices in nursing homes is needed.
Aim: To investigate the role of leaders in fostering person-centeredness within nursing homes.
Methods: The study is based on the PRISMA reporting guidelines. Comprehensive searches were performed in CINAHL and PubMed, with article screening and selection facilitated by Rayyan software. A convergent integrated approach from the Joanna Briggs Institute (JBI) was used to synthesize findings from both qualitative and quantitative studies.
Results: The review included ten studies, comprising six qualitative and four quantitative studies. The results indicate that leadership in nursing homes that fosters person-centeredness involves creating and communicating a shared vision, empowering staff, and ensuring systematic and consistent approaches. Additionally, leaders must embody person-centered values through role modeling.
Conclusions: This systematic review highlights the critical role of leadership in fostering and sustaining person-centered practices in nursing homes. Leaders carry a substantial burden of responsibility. The results suggest that a shift towards a more integrated leadership approach, incorporating both distributed and person-centered leadership models, could promote a more sustainable and supportive environment for both leaders and staff, ultimately enhancing the quality of care. These insights provide valuable guidance for nursing home leaders and policymakers aiming to strengthen person-centered practice.
1 Introduction
In nursing homes, a significant majority of residents are frail and vulnerable and cope with multiple health conditions (1). For this study, the term “nursing home” refers to residential care facilities that provide long-term care for individuals who are unable to live independently due to physical or cognitive limitations. These facilities offer a range of services, including assistance with activities of daily living, medical care, and rehabilitation. In some countries, such facilities may be referred to by other terms, such as “care homes,” “residential care facilities,” or “assisted living,” depending on the context and specific services provided.
Despite continuous efforts to improve care quality in nursing homes, a concerning number of residents still face poor care experiences (2). Rosemond et al. (3) suggest that adopting a person-centered approach, which emphasizes residents' relationships, life histories, abilities, and preferences, can be a transformative step in nursing home care. Person-centeredness is often hailed as the “gold standard” of care (4) and has become a cornerstone of healthcare, aiming for high-quality service (5, 6). Person-centeredness can be defined as follows:
“An approach to practice established through the formation and fostering of healthful relationships between all care providers, care receivers, and others significant to them in their lives. It is underpinned by values of respect for persons (personhood), individual right to self-determination, mutual respect, and understanding. It is enabled by cultures of empowerment that foster continuous approaches to practice development.” (5, p. 3)
We have chosen to adopt McCormack and McCance's (5) definition of person-centeredness, as it is recognized as a well-established mid-range theory with a solid empirical foundation (5). This definition is widely applied in academic research and practical implementations of person-centered practice (7–9), making it particularly relevant to our study.
The emphasis on person-centeredness represents a shift towards inclusivity and equality in the professional-patient relationship, aiming to address each person's unique needs. McCormack and Skatvedt (10) outlined four fundamental principles of person-centered practice: treating each person as a unique individual, respecting their rights, establishing mutual trust and understanding, and nurturing collaborative relationships. Person-centered practice encompasses the intricate nature of nursing and the broader healthcare context, emphasizing the significance of all individuals within the healthcare environment. Person-centered practice shifts from the dominant practice focus on “doing” to one of “being”, emphasizing the role of individuals working in healthcare and the significance of relationships with others (11). Person-centered care (PCC) is widely acknowledged as essential for ensuring both the quality of care and quality of life in long-term care settings (12). Research indicates that PCC leads to improved patient outcomes, more efficient resource utilization, reduced costs, and heightened satisfaction among both patients and staff (13). However, person-centered interactions can be challenging as nursing home routines sometimes take precedence over individual needs (8).
Leadership in nursing homes plays a crucial role in shaping staff interactions, the work environment, and the quality of resident care (14–16). Nursing home leaders also play a vital role in ensuring residents receive PCC (15). Over time, various leadership styles have emerged, including distributed, transactional, laissez-faire, transformational, and situational (16). While relational and transformative leadership styles have been identified as the most effective in nursing homes (14), research indicates that passive-avoidant leadership remains the most prevalent (17). Often considered a subtype of laissez-faire leadership, passive-avoidant leadership is marked by disengagement from both tasks and personnel, neglect of staff needs, and inaction in the face of emerging issues. It is frequently described as an absence of active or effective leadership (18) and has been linked to reduced satisfaction with leadership, increased incidence of workplace bullying, and higher levels of absenteeism (19). This leadership style may contribute to a disengaged work culture in which staff feel unsupported, ultimately compromising the delivery of PCC and negatively affecting the well-being of both residents and employees. Given the complex and relational demands of nursing home environments, these outcomes underscore the urgent need to adopt leadership models that are proactive, engaged, and aligned with person-centered values.
In recent years, there has been a growing interest in leadership approaches grounded in person-centered values (20, 21). One such approach is person-centered leadership, described by Eide and Cardiff (22) as “leadership supporting, creating, and securing person-centered values and practices” (p. 96). While closely aligned with the values underpinning the Person-Centered Practice Framework (5), person-centered leadership is not formally included in the framework but offers a complementary perspective on how leadership can foster a person-centered culture in healthcare organizations.
Much of the existing research has focused on associations between specific leadership styles and care outcomes. However, recent studies have underscored the need to consider both leadership behaviors and styles when evaluating the quality of care in nursing homes (23, 24), highlighting the importance of leadership approaches that are collaborative, value-driven, and relational in nature.
One such approach is distributed leadership, which has gained increasing relevance in healthcare settings, particularly where complex care processes require shared and relational leadership practices. Unlike traditional models centered on a single leader, distributed leadership involves the collective enactment of leadership tasks across multiple actors. Leadership is understood not as the responsibility of one person, but as a set of behaviors and interactions embedded within everyday relationships (25, 26). By enabling joint responsibility and shared decision-making, distributed leadership supports core person-centered principles such as empowerment, cooperation, and mutual respect. Evidence from a systematic review indicates that distributed leadership can enhance organizational performance (27), suggesting that this model may also contribute to the development of person-centered cultures in nursing homes.
The management of nursing homes requires systems and processes for planning, implementing, evaluating, and adjusting healthcare delivery in line with national laws and guidelines (28, 29). While these systems demand efficiency and compliance, leaders must also foster principles of compassion, individual attention, and relationship-building. Leadership, particularly when supported through facilitation, plays a vital role in strengthening team collaboration and refining person-centered strategies (20). More broadly, leaders carry both the opportunity and responsibility to shape, nurture, and sustain the cultural ethos of their organizations (30, 31).
However, transitioning to a person-centered approach in nursing homes represents a complex and far-reaching organizational shift (3). Despite growing interest in leadership approaches aligned with person-centered values, there remains limited guidance on how to educate and support leaders in this transformation (21). To date, no systematic review has examined the nuanced leadership dynamics that underpin the facilitation of person-centered practice in nursing homes.
2 Methods
This systematic review was conducted to investigate the role of leaders in fostering person-centeredness in nursing homes. The review specifically addressed the following research question:
What are the underlying leadership dynamics that facilitate person-centered practice in nursing homes?
Leaders are defined as individuals holding formal leadership roles in nursing homes, such as nursing home managers and head nurses.
The Joanna Briggs Institute (JBI) Manual for Evidence Synthesis guided the conduct and synthesis of this review (32). The a priori protocol was registered in PROSPERO, with the registration number CRD42022366678.
2.1 Search strategy
Systematic searches were conducted in the databases CINAHL and PubMed. A specialist librarian was consulted during the development of the search strategy and carried out the searches to ensure rigor. Keywords and MeSH terms were used in various combinations with Boolean operators. The search included terms related to:
• Leadership (e.g., leader*, situational leadership, attitude of health personnel, staff attitude)
• Person-centred care (e.g., person-cent* care, personhood, individualized care, patient-centered care, personalized care, person-directed care planning, person-centred practice framework)
• Care settings (e.g., nursing home*, long-term care, residential facilities, homes for the aged, municipal home*, assisted living)
• Implementation and organizational context (e.g., implementation, culture change, quality improvement, organizational change, innovation, experience*, perspective*, framework)
Full details of the search terms and search strings for each database are provided in Supplementary Material S1.
The study adheres to the PRISMA guidelines for systematic review (33). The inclusion and exclusion criteria are presented in Table 1.
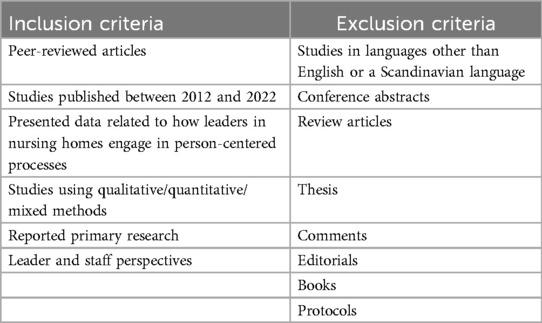
Table 1. Inclusion/exclusion criteria.
The year 2012 was selected as the starting point for the review because healthcare systems have undergone substantial changes over recent decades (34). Studies across diverse healthcare systems with different financial systems are included in this review, as the focus is on leadership dynamics that facilitate the adoption and maintenance of person-centered practice, independent of health policy structures or cultural contexts. We did not restrict inclusion to studies using a specific theoretical framework (e.g., McCormack and McCance's Person-centred Practice Framework). However, studies were only included if they explicitly referred to person-centeredness. Figure 1 presents the PRISMA flow diagram of the study selection process.
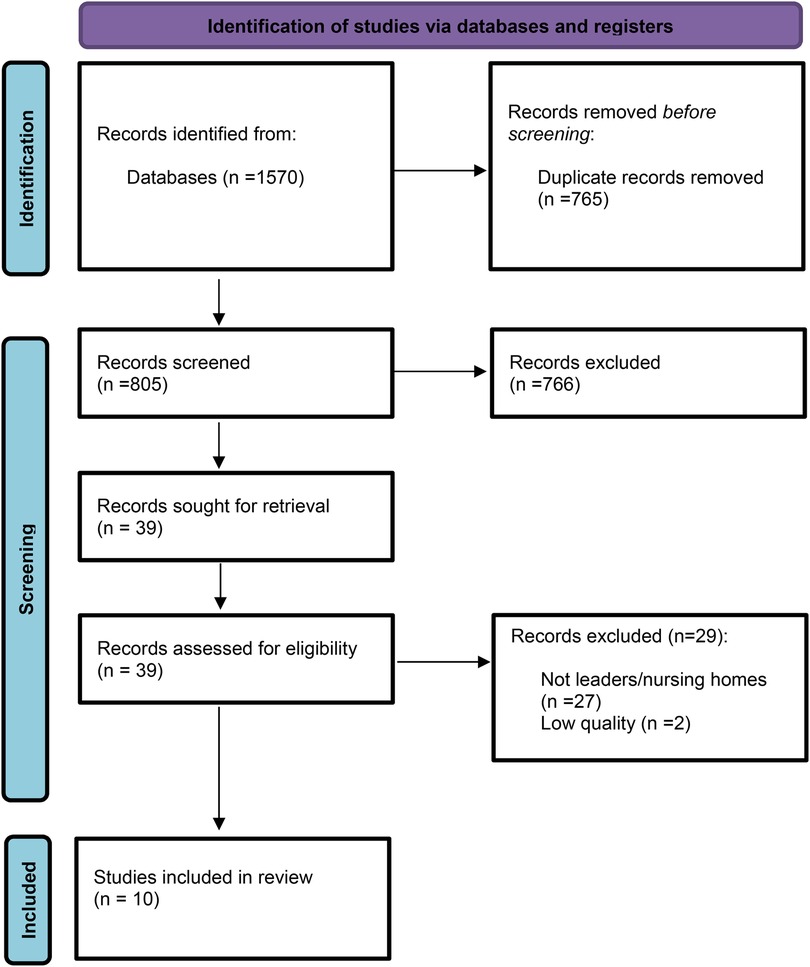
Figure 1. PRISMA 2020 flow diagram for new systematic reviews (33).
2.2 Quality assessment of the studies
The quality of the included articles was assessed by two authors (ACLL and CB) using the appropriate JBI Critical Appraisal Tool based on the study design: (i) JBI Critical Appraisal Checklist for Qualitative Research or (ii) JBI Critical Appraisal Checklist for analytical cross-sectional studies. Each author conducted assessments independently and then compared their results. Minor disagreements arose but were resolved through discussion until consensus was achieved. No established parameters exist for weighting qualitative studies (35). In this review, all criteria were deemed of equal importance. A study was classified as high quality if it achieved a score above 70%, moderate quality if it scored between 50% and 70%, and low quality if it scored below 50%, as outlined by Dijkshoorn et al. (36). Only high and moderate-quality studies were included in the final synthesis. Two studies were excluded due to insufficient quality.
2.3 Data extraction
The JBI QARI data extraction form for interpretive and critical research (32) served as our tool for data extraction, as outlined in Table 3. Data extraction was conducted for both qualitative and quantitative studies (32, 37). From qualitative studies, we extracted the authors' interpreted findings, such as thematic categories or subthemes, along with supporting interpretations and illustrations. For quantitative studies, we followed the approach described by Lizarondo et al. (37), in which narrative descriptions of results reported by the study authors are extracted and, where appropriate, rephrased or condensed to ensure clarity and relevance to the review objective. This allowed us to integrate quantitative data with qualitative findings by transforming them into textual representations, a process known as qualitization (37). Data extraction was initially conducted by the first author (CAH) and subsequently reviewed by co-authors LBO and IF to ensure accuracy and consistency. No disagreements arose that required further resolution.
2.4 Data synthesis
JBI's convergent integrated synthesis approach (32, 37) was used to synthesize data from the included primary studies. The synthesis process is summarized in Table 2, which provides a schematic overview of how the JBI convergent integrated approach was applied. The table outlines the steps from compiling primary data to generating synthesized findings.
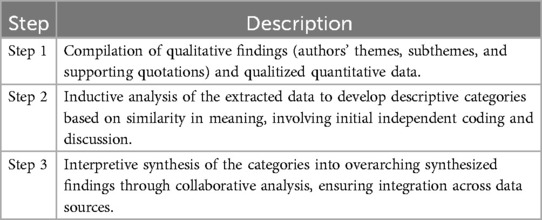
Table 2. Schematic overview of the synthesis process using JBI's convergent integrated approach (37).
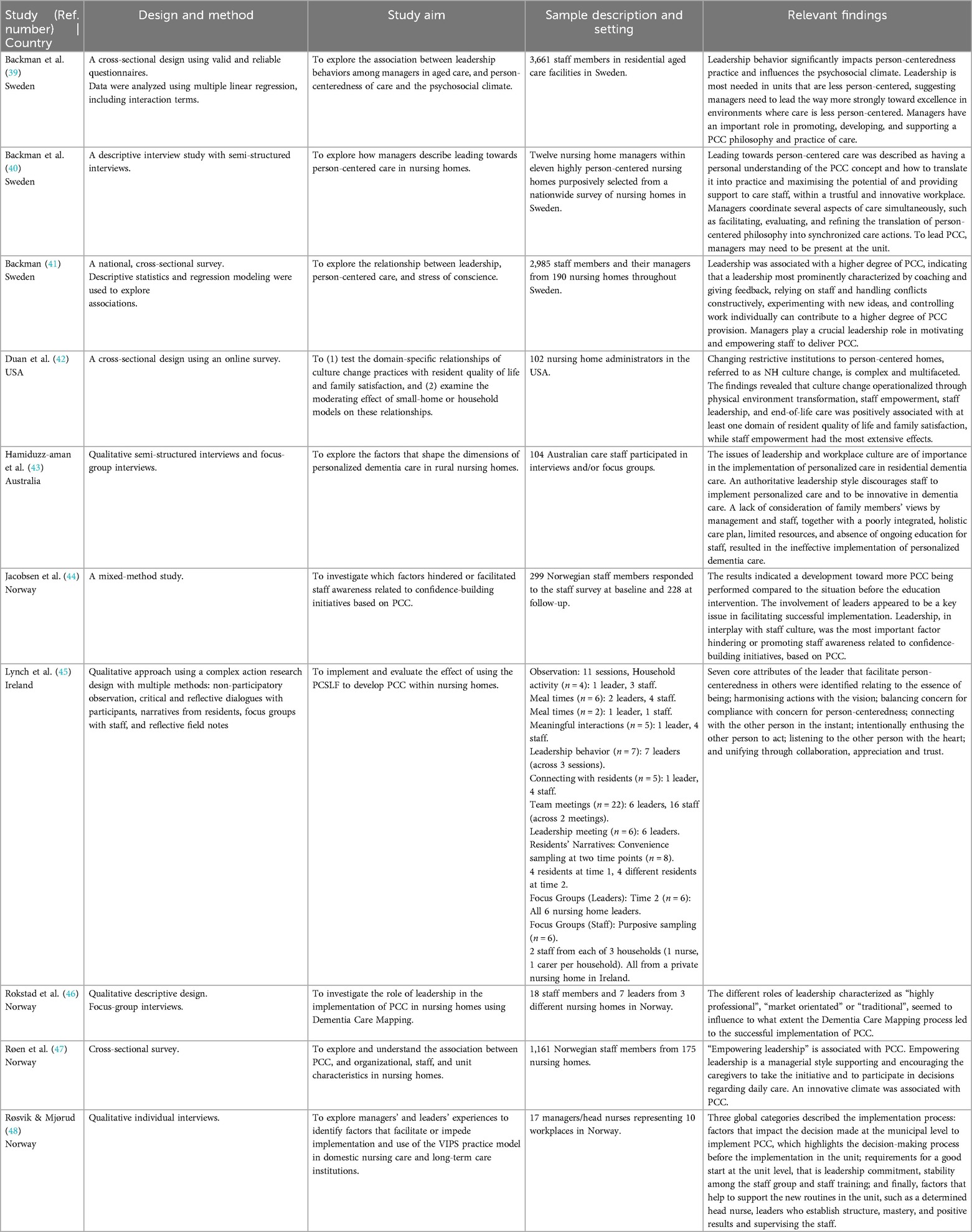
Table 3. JBI QARI data extraction form for interpretive and critical research.
Thematic categories were developed through an inductive analysis of the extracted data, which included authors' interpretive themes, subthemes, and supporting quotations from qualitative studies, as well as qualitized narrative findings from quantitative studies. During the process, findings were grouped based on similarity in meaning, with attention to recurring concepts, language, and underlying assumptions about leadership and person-centeredness. Contrasting perspectives were also explored to ensure a nuanced interpretation. Initial coding and categorization were performed independently by three reviewers (CAH, IF, LBO), followed by collaborative discussion to refine and consolidate categories.
Subsequently, one researcher (CAH) led the synthesis process by analyzing the descriptive categories for overarching patterns and integrating them into synthesized findings. This interpretive synthesis was carried out in ongoing dialogue with the co-authors (IF and LBO), ensuring that the final themes were grounded in the evidence and represented both convergence and variation across included studies.
3 Results
3.1 Study selection
The search yielded 1,570 potentially relevant papers. The papers were imported into EndNote software and subsequently transferred to Rayyan (38) for deduplication. Five members of the review author team independently screened the studies by title and abstract (CAH, LBO, LH, AKH, IF). For a paper to be considered relevant, it needed to include the terms “management” and “nursing home,” or their synonyms, in the text, in addition to adhering to the inclusion and exclusion criteria. The reviewers then divided into two groups and compared their results, identifying 39 articles. In the following screening phase, the five review authors independently assessed the full text of the 38 articles for final inclusion. Any discrepancies in selection during the review process were resolved through discussion.
The final sample comprised ten studies: six qualitative and four quantitative (Figure 1). Four of the studies were conducted in Norway, three in Sweden, one in Australia, one in Ireland, and one in the USA. Perspectives from both formal leaders (nursing home managers and head nurses) and non-managerial staff (e.g., registered nurses, enrolled nurses, and nursing assistants) were represented. The quality assessment of the included studies is presented in Table 4.
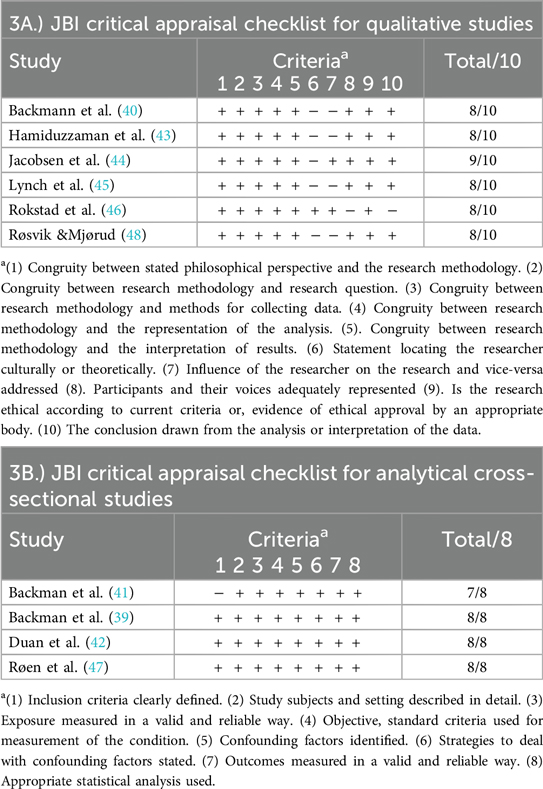
Table 4. Result of the quality assessment of the included studies.
3.2 Result of data synthesis
The data synthesis led to three synthesized findings: (i) Visionary leadership and empowerment; (ii) Consistent and systematic approach for person-centered outcomes; and (iii) Leadership through role modeling. These findings were arrived at through the use of the JBI's convergent integrated synthesis approach, as described earlier (32). Table 5 presents the results of the data synthesis following the convergent integrated approach (37), in which findings from included studies were grouped into thematic categories and further integrated into three overarching synthesized findings. The structure aims to illustrate how multiple qualitative findings were converged through interpretive analysis into higher-order syntheses, supported by excerpts from the primary studies.
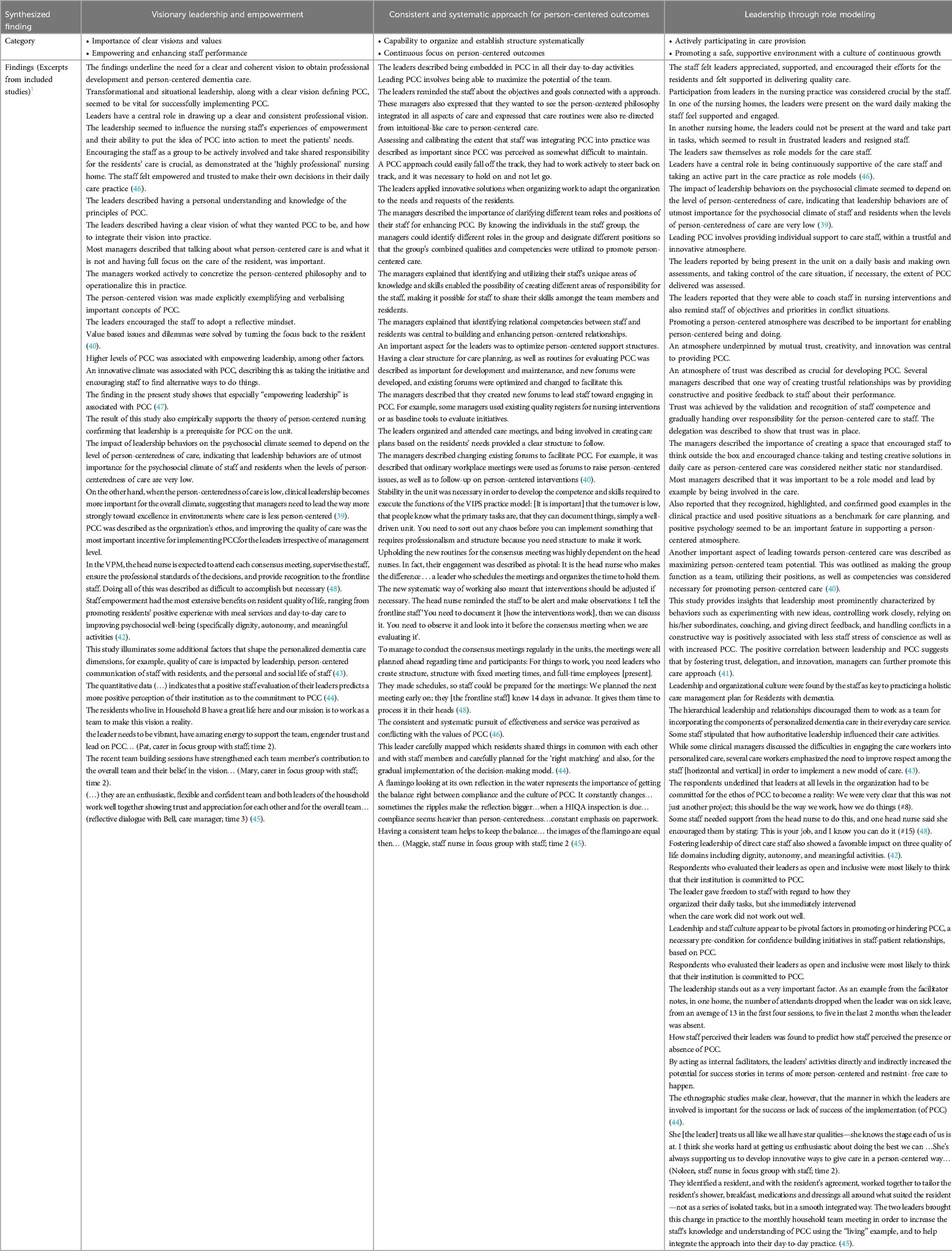
Table 5. Results
3.3 Visionary leadership and empowerment
The results in this synthesized finding highlight how the leaders had clear and shared visions for person-centered practice through the following categories: (i) Importance of clear visions and values, and (ii) Empowering and enhancing staff performance.
3.3.1 Importance of clear visions and values
Several of the reviewed papers identified the need for a clear, coherent vision in fostering professional development, establishment, and delivery of a person-centered practice (39, 40, 45–47). Leadership did not encompass a passive role; the leaders were at the forefront, actively shaping and defining visions and values into the professional practices of their teams. From the statement, “the managers in this study described having a personal understanding and knowledge of the principles of PCC, and also a clear vision of what they wanted it to be’ (40, p. 175), it is evident that leaders had a deep connection with the principles of PCC. For them, the vision of PCC was not just a mere policy tick-box but resonated with their beliefs and understanding about care. Further, several staff members had high expectations of their leaders in terms of supporting the staff team, as illustrated by the following quote:
“The leader needs to be vibrant, have amazing energy to support the team, engender trust and lead on person-centered care…” Carer (45).
3.3.2 Empowering and enhancing staff performance
Findings in this category focused on how leadership facilitated empowerment, autonomy, and the enhancement of staff performance within the realm of person-centered practice. Four studies highlighted the critical role of leader-facilitated staff empowerment, viewed from various perspectives (42, 45–47). Duan et al. (42) discovered that empowering staff significantly improved the quality of life for residents, with positive impacts observed in meal services, daily care, and psychosocial well-being aspects like dignity, autonomy, and engaging activities. Similar findings were reported by Røen et al. (47) and Rokstad et al. (46), both noting a positive correlation between PCC and empowered staff. Rokstad et al. (46) further observed how leadership seemed to influence staff's sense of empowerment and their ability to implement PCC effectively:
“The staff felt empowered and trusted to make their own decisions in their daily care practice.” Leader. (46, p. 23).
Elevated levels of PCC were associated with empowering leadership, among other factors. An innovative climate, typified by initiative and the encouragement of alternative methods and approaches, was also linked to PCC (47). Lynch et al. (45) found that the leaders empowered staff performance by encouraging innovative, individualized approaches, aligning with each team member's development level.
3.4 Consistent and systematic approach for person-centered outcomes
In this synthesized finding, the importance of having a systematic approach and a structured plan in the workplace to achieve person-centered goals is highlighted. In addition, the importance of maintaining focus on the goal was emphasized. The synthesized finding is reflected in the subcategories (i) Capability to organize and establish structure systematically, and (ii) Continuous focus on person-centered outcomes.
3.4.1 Capability to organize and establish structure systematically
Four of the articles emphasized the importance of having a systematic approach to person-centered practice (40, 44, 46, 48). Leaders strategically utilized both new and existing forums to promote person-centeredness. Whether through ordinary workplace meetings or specially created platforms, the agenda often revolved around person-centered issues and interventions. This involved planning meetings, scheduling various activities, and reminding the staff of objectives and goals connected with a person-centered approach (40, 48). Furthermore, a consistent and stable team in the department was underscored as a crucial component in achieving systematic organization and structure (45, 48).
The way of organizing and being systematic in the approach to achieving a person-centered practice also manifested itself in other ways, such as identifying different qualities among the staff so that staff and residents were matched based on the chemistry they had with each other (44), or seeing themselves as a team where the aim was to bring out the best in each other as quoted by this leader:
“I talk a lot about that we are like a football team, everyone cannot be Ibrahimović… but I think it's so important… “I think like this, we must have positions, as we are a team, sometimes you do more of this and less of that, but that does not mean that we are doing a poorer result, maybe better, as the result will be better when we position ourselves.” (40, p.178).
Thus, the capability to organize and establish structure systematically was not just about administrative processes or maintaining consistency within staff. The focus also lay in understanding how to best utilize the unique strengths and dynamics of each staff member to achieve the overarching goal of person-centered practice.
3.4.2 Continuous focus on person-centered outcomes
Within this category, the need for having a continuous focus on person-centeredness became evident (40, 46, 48). Establishing person-centered practice was not a one-time event; rather, it required sustained dedication and vigilance. As one leader articulated:
“We have to keep the idea of person-centeredness warm all the time” (46, p. 21).
Encouraging staff to observe, reflect, and share their thoughts seemed to be emphasized as valuable in the process of enhancing person-centered outcomes. In maintaining focus on person-centered practice, several elements were involved. One of the elements was to keep the awareness high about the concept, and to see and recognize the residents' needs:
“If you lived here, what would be most important for you? - What do you think is most important for the persons living here?” Leader (40., p.176).
Røsvik and Mjørud (48) on their side pointed out the importance of observing and documenting how the interventions worked, in order to evaluate together in staff meetings.
3.5 Leadership through role modeling
A recurring topic was the importance of the leaders leading by example. The importance of role modeling was emphasized both by the leaders and by the employees. The synthesized findings are divided into the following categories: (i) Actively participating in care provision, and (ii) Promoting a safe and supportive environment with a culture of continuous growth.
3.5.1 Actively participating in daily routine
When leaders were visibly present and validated the staff's approach to resident care, staff satisfaction and their motivation to provide personalized care were notably enhanced. The role of a leader extended beyond just oversight; they acted as both a support mechanism for the staff and as an integral part of residents' day-to-day care (40, 44–46, 48). As one leader detailed:
“I am out on the wards, I'm visible on a daily basis, and I follow up by asking questions: How is it going? How are we doing? What can we do here? How can we think concerning this…?” (40, p. 177).
Rokstad et al. (46) documented varying perspectives on this theme. In one nursing home, leaders and staff concurred on the importance of leaders' involvement in daily care. The care staff felt both inspired and supported to deliver quality care, and the leaders conveyed appreciation for their dedication and skills. In contrast, another nursing home saw a disconnect when leaders couldn't be present, resulting in disheartened leaders and a resigned staff. Both groups found this scenario challenging, with one leader commenting:
“I cannot be present on the ward on a daily basis, so I have to lead the care practice through others. I find this frustrating.” (46, p. 21).
Another study found that staff in one nursing home faced challenges with a leader who did not engage in daily activities, describing their leader as “distant” and “lacking involvement in staff and residents’ matters.” (44).
This category also shines a light on leaders as role models in a person-centered practice. Their involvement in nursing was viewed as more than just practical assistance; it symbolized leading by example (40, 43, 46):
“Most managers described that it was important to be a role model and lead by example by being involved in the care.” (40).
The active involvement of leaders in caregiving underscored how a person-centered approach was as much about hands-on participation as about guiding principles.
3.5.2 Promoting a safe, supportive environment with a culture of continuous growth
Several studies highlight the significance of not only adopting a person-centered approach for residents but also treating staff according to the principles of person-centeredness (40, 41, 43, 44, 46, 48). Moreover, it seemed like when employees perceived their leaders as open and inclusive, they were more inclined to believe that the institution genuinely valued person-centeredness (44).
Another key element identified was the commitment of leaders to embed the ethos of person-centeredness deeply within the organizational culture (42, 44, 48). The leaders in Røsvik and Mjørud's study (48) emphasized that leaders, regardless of their management level, should prioritize PCC as the main framework for addressing value-based issues and ensuring person-centered solutions for residents:
“The respondents underlined that leaders at all levels in the organization had to be committed for the ethos of person-centered care to become a reality: We were very clear that this was not just another project: this should be the way we work, how we do things.” (48).
Rokstad et al. (46) also emphasized the inherent responsibility of leaders to provide continuous support to care staff. This finding is echoed in Lynch et al. (45), where a nurse described how her leader demonstrated support:
She treats us all like we all have star qualities—she knows the stage each of us is at. I think she works hard at getting us enthusiastic about doing the best we can … (45).
Further findings from Backman et al. (39) illustrated the impact of leadership behaviors, especially in shaping the psychosocial climate for both staff and residents, with this influence being even more pronounced when PCC was inadequate.
4 Discussion
The findings from this study highlight several key dynamics underlying effective person-centered leadership in nursing homes, particularly the importance of visionary leadership and empowerment, a consistent and systematic approach, and the importance of modeling person-centered values and behaviors. This discussion aims to interpret the key findings of the study and situate them within the broader context of relevant existing literature.
4.1 Visionary leadership and empowerment
The findings underscore the necessity for nursing home leaders to possess a cohesive vision and set of values aligned with person-centered principles, ensuring these visions transcend superficial policies and resonate with leaders' core beliefs (39, 40, 45–48). These findings align with previous research indicating that leaders who deeply understand and embody person-centered principles are better positioned to implement them effectively in practice (30). Earlier studies also support the importance of a shared vision as an essential feature of leadership behavior. Martin et al. (49) found that vision provides orientation and meaning for leaders and their teams, helping them focus their energies and engage in the transformation of practice. A 2022 systematic overview of reviews by Feldthusen et al. (50) describes numerous prerequisites for facilitating person-centered practices in healthcare, including the formation of a vision.
The correlation between empowered staff and person-centeredness underscores the significance of effective leadership in fostering staff empowerment through support, autonomy, and opportunities for agency (45–47). Prior research (51) corroborates these findings, suggesting that empowering staff improves outcomes for nursing home residents and enhances staff motivation and job satisfaction. Additionally, Ta'an et al. (52) found that highly empowered nurses displayed higher performance than less empowered nurses in hospitals. Conversely, Feldthusen et al. (50) found that a lack of influence over policies, procedures, and practices contributed to feelings of disempowerment among healthcare professionals. These factors, coupled with rising workloads and insufficient support, adversely impacted their psychological well-being and their ability to deliver PCC (50).
4.2 Consistent and systematic approach for person-centered outcomes
The findings indicate that fostering person-centered practices requires systematic approaches and structured planning from leaders (40, 48). For instance, one nursing home in the study implemented systematic review meetings to evaluate care plans and PCC practices, which were deemed crucial for developing and maintaining person-centered practice (40). This finding aligns with international literature, where previous research supports the necessity of a systematic approach and regular evaluation to sustain high-quality person-centered practice (11, 53). These findings suggest that nursing home leaders should prioritize the development of structured care planning and evaluation routines to ensure consistent and high-quality PCC.
A stable workforce was identified as critical for achieving systematic organization and structure, ensuring a well-coordinated department, and promoting expertise development among staff (48). Stable staffing allows for continuity of care, which is essential for building trust and understanding between residents and caregivers. When staff members are familiar with the residents and their specific needs, they can provide more personalized and effective care (5). However, research by Moore et al. (54) suggests that consistent leadership may be even more critical. Consistent leadership provides direction, stability, and a clear vision, which are vital for sustaining person-centered practices (22). These findings underscore the importance of maintaining a stable workforce and ensuring continuity in leadership roles to effectively implement and maintain person-centered practice.
4.3 Leadership through role modeling
A recurring theme was the profound impact of leaders actively modeling person-centered behaviors (40, 43, 45, 46). By serving as visible role models, the leaders reinforced the importance of person-centered values and inspired staff to adopt similar practices. Numerous studies have underscored the leader's role as a model for expected behaviors (49, 54–57). However, what sets this context apart is that leaders also serve as role models in their execution of daily patient care, as evidenced in the study by Rokstad et al. (46), where staff regarded leader participation in nursing practice as crucial. While leader involvement in daily care can enhance understanding and presence, several challenges may emerge. Challenges such as role confusion, time pressure, insufficient clinical competence, and inadequate resource allocation can impede effective leadership and optimal care. Of particular concern is the potential lack of clinical competence among leaders. Although many leaders possess healthcare backgrounds (58), their clinical skills may not be as current as those of staff who work with patients daily. Moreover, Kirchhoff and Karlsson (59) found that first-line nurse managers frequently face role conflict or feel 'squeezed' by the competing demands of their responsibilities as registered nurses and leaders. This dual pressure can result in significant stress, emotional exhaustion, and an inclination to resign from their leadership roles.
A key finding was that the majority of the included studies emphasized the importance of adopting a person-centered approach not only for residents but also for treating staff according to the principles of person-centeredness (40, 41, 43, 44, 46, 48). Such findings illustrate the paradigm shift from the traditionally PCC, which primarily focuses on the patient as the sole important person in the relationship, to person-centered practice, which encompasses all individuals in the relationship, including healthcare professionals (7). Buetow (60) refers to this shift as viewing patients and healthcare personnel as “moral equals,” indicating that to provide effective PCC, healthcare professionals must also feel that their personhood is respected and recognized.
Backman et al. (39) discovered that the influence of leadership behaviors on the psychosocial climate was contingent on the degree of PCC, suggesting that leadership behaviors are critically important for the psychosocial well-being of staff and residents. Furthermore, Jacobsen et al. (44) found that staff perceptions of their leaders were indicators of the presence or absence of PCC in the nursing home. These findings align with research by Seljemo et al. (23) and Zonneveld et al. (24), who emphasize that the significance of leadership behaviors, rather than just leadership styles, is crucial in nursing home care.
4.4 Rethinking leadership expectations in nursing homes
The data from all included studies underscore the extensive and multifaceted expectations placed on leaders in nursing homes (39–48). Beyond ensuring the implementation of person-centered practices, leaders are tasked with a wide range of responsibilities, including administrative tasks, role modeling, and direct involvement in care activities (40, 43–46, 48). Persistent challenges in nursing home leadership, such as understaffing, financial constraints, limited resources for staff development, and blurred work-life boundaries, further exacerbate expectations (58, 61, 62). Such demands mirror the traditional “heroic” model of leadership, where leaders are expected to manage and resolve all organizational issues independently (63). This model raises questions about its feasibility and sustainability in the context of modern nursing homes.
There is an apparent contradiction between the expectations placed on leaders and the principles of person-centered practice, which advocate for shared responsibility and collaborative approaches (5). A disconnection between expectations and the support provided to leaders can lead to burnout and reduced effectiveness in leaders (59, 62) and diminish their ability to foster a person-centered culture. This issue highlights the need to rethink traditional leadership models in nursing homes.
4.5 Shifting towards integrated leadership models
The findings of this review point to the potential benefits of shifting towards a more integrated leadership model that aligns with person-centered values. In particular, distributed leadership may offer a valuable contribution by supporting a more balanced distribution of responsibilities and tasks across different organizational levels (64). In this model, administrative duties may be delegated to specialized personnel, while clinical leadership is exercised by experienced nurses closer to care delivery. By embedding distributed leadership within broader person-centered strategies, nursing homes may cultivate cultures where leadership is enacted through relationships rather than imposed hierarchically. This can enhance staff engagement and competence (62, 65) and support the sustainable implementation of person-centered practices. Moreover, person-centered leadership plays a crucial role in nurturing such practices by emphasizing staff empowerment, fostering teamwork, and aligning leadership actions with the core values of PCC (22). According to McCormack and McCance (11), the goal of person-centered processes is to create a “healthful culture”, an environment that promotes both staff well-being and quality of care. Emerging research on healthful leadership further reinforces its role in establishing supportive and sustainable workplaces (66).
By integrating the principles of person-centered and distributed leadership, healthcare organizations can enhance the well-being of both staff and leaders, ultimately improving care outcomes (11, 22, 64). Further support for this integrated approach comes from recent work by Cable, McCance, and McCormack (67), who explored how person-centered nursing leadership can be cultivated through transformative professional development. They emphasize that becoming a person-centered leader is a process of knowing, being, and becoming, an internal journey that fosters authenticity and relational depth in leadership.
Taken together, these insights suggest that developing integrated leadership models may be key to the sustained success of person-centered practices in nursing homes.
5 Conclusion
This systematic review has identified the underlying leadership dynamics facilitating person-centered practice in nursing homes. The analysis revealed three key themes: visionary leadership and empowerment, a consistent and systematic approach to achieving person-centered outcomes, and leadership through role modeling. The findings collectively indicate that substantial responsibility lies with leaders to effectively implement and sustain person-centered practice, in addition to fulfilling their broader managerial duties and obligations. These findings suggest a potential benefit of exploring a more integrated leadership model that draws on distributed and person-centered leadership models. Such a model could lead to a more sustainable and supportive environment for both leaders and staff, ultimately improving the quality of care. This synthesis of existing research provides valuable insights for nursing home leaders and policymakers striving to enhance PCC and highlights the importance of supporting leaders in their efforts to create and sustain person-centered environments.
5.1 Strengths and limitations
The strength of the study lies in summarizing knowledge in an area with limited existing evidence. Furthermore, the study is conducted systematically and rigorously, adhering to a recognized framework for systematic reviews. The included studies were critically appraised by multiple reviewers to enhance objectivity and reduce bias.
However, some limitations are evident in this review. The most notable is the imbalance in the distribution of findings among the included articles. Some articles contribute numerous findings, while others provide less. To ensure transparency, the details of which findings are extracted from each article are presented in the results section (see Table 5).
Of the ten included studies, seven were conducted in Norway and Sweden. This raised questions about our search terms and whether different words or concepts might be used in other countries. We extensively used various MeSH terms and examined search terms from comparable studies. Additionally, a specialized librarian conducted the searches. Despite these efforts, we acknowledge the possibility of overlooked factors. Furthermore, the review included only two databases, CINAHL and PubMed. While these databases are highly comprehensive within the scope of nursing and health services research, the use of additional databases might have yielded a small number of additional studies, and this is acknowledged as a limitation.
In our searches, we have not differentiated between professional and administrative leadership, and there might be differences in how closely these various levels work with the staff. There are also different ways of organizing nursing homes in various countries, which have not been considered in this study.
In addition to the limitations already discussed, we acknowledge potential methodological and theoretical constraints in this review. Methodologically, the search was limited to two databases (CINAHL and PubMed), which may have excluded relevant studies indexed elsewhere. Furthermore, while our inclusion criteria focused on studies that involved formal nursing home leaders, the variation in how leadership roles are defined and reported across countries and studies may have introduced some ambiguity.
Variability in study designs, populations, and outcome measures has made drawing definitive conclusions challenging, but such diversity also provides a comprehensive overview of the existing evidence and highlights areas where further research is needed.
5.2 Implications of the results for practice, policy, and future research
The findings of this review highlight the need for leadership approaches in nursing homes that are actively aligned with person-centered values and enacted through everyday leadership behaviors. In practice, this calls for leaders who can articulate and embed a clear vision for care, empower staff, and lead by example through consistent engagement in care provision. Establishing such leadership requires not only structural support but also the cultivation of reflective practice, where leaders routinely assess and adapt their approaches based on feedback, values, and situational demands.
From a policy perspective, these findings point to the importance of leadership development programs that prioritize relational and values-based competencies alongside organizational skills. Policies aimed at improving care quality in nursing homes should therefore support leadership models that encourage reflection, staff involvement, and shared responsibility.
Future research should explore how leadership practices can be systematically developed and sustained over time to promote person-centered practice in nursing home settings. Longitudinal studies may help clarify how specific leadership behaviors support the creation of person-centered cultures, enhance staff well-being, and improve person-centered outcomes for residents.
Author contributions
CA-H: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. LO: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Formal analysis. VG: Conceptualization, Writing – review & editing, Writing – original draft. A-CL: Conceptualization, Writing – review & editing, Writing – original draft. AH: Conceptualization, Investigation, Writing – review & editing, Writing – original draft. CB: Conceptualization, Writing – review & editing, Writing – original draft. LH: Conceptualization, Investigation, Writing – review & editing, Writing – original draft. GR: Writing – review & editing, Writing – original draft. BM: Validation, Writing – review & editing, Writing – original draft, Conceptualization. IF: Conceptualization, Investigation, Writing – original draft, Writing – review & editing, Formal analysis.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors wish to thank Trine Kristin Tingelholm Karlsen, librarian at Østfold University College, for her help with conducting the searches in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. This article has benefited from the proofreading and language refinement services provided by OpenAI's ChatGPT-3.5.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2025.1535414/full#supplementary-material
Footnote
1. ^The findings are presented article by article, and the reference is positioned after the final excerpt from each article.
References
1. Strand V, Vollrath ME, Skirbekk H. Dementia. In: Rørtveit G, editor. Folkehelserapporten. Oslo: Folkehelseinstituttet (2021). Available online at: https://www.fhi.no/he/folkehelserapporten/ikke-smittsomme/demens/?term= (Accessed June 03, 2025).
2. Myhre J, Saga S, Malmedal W, Ostaszkiewicz J, Nakrem S. Elder abuse and neglect: an overlooked patient safety issue. A focus group study of nursing home leaders’ perceptions of elder abuse and neglect. BMC Health Serv Res. (2020) 20:199. doi: 10.1186/s12913-020-5047-4
3. Rosemond CA, Hanson LC, Ennett ST, Schenck AP, Weiner BJ. Implementing person-centered care in nursing homes. Health Care Manag Rev. (2012) 37(3):257–66. doi: 10.1097/HMR.0b013e318235ed17
4. Yang Y, Li H, Xiao LD, Zhang W, Xia M, Feng H. Resident and staff perspectives of person-centered climate in nursing homes: a cross-sectional study. BMC Geriatr. (2019) 19:292. doi: 10.1186/s12877-019-1313-x
5. McCormack B, McCance T. Person-centred Practice in Nursing and Health Care: Theory and Practice. 2nd ed. Oxford: Wiley Blackwell (2017).
6. World Health Organization. Framework on Integrated People-centred health Services. Geneva: WHO (2015). Available online at: http://www.who.int/servicedeliverysafety/areas/people-centered-care/framework/en/ (Accessed Jun 3, 2025).
7. Anker-Hansen C. On Making the Invisible Visible: A Qualitative Study of Care Partners of Older People with Mental Health Problems and Home Care Services [dissertation]. Horten: Faculty of Health and Social Sciences, University of South-Eastern Norway (2020. Report No.: 57.
8. Helgesen AK, Fagerli LB, Grøndahl VA. Healthcare staff’s experiences of implementing one-to-one contact in nursing homes. Nurs Ethics. (2019) 26(1–9):505–13. doi: 10.1177/0969733019857775
9. Slater P, McCance T, McCormack B. The development and testing of the person-centred practice inventory-staff (PCPI-S). Int J Qual Health Care. (2017) 29(4):1–7. doi: 10.1093/intqhc/mzx066
10. McCormack B, Skatvedt A. Older people and their care partners’ experiences of living with mental health needs: a focus on collaboration and cooperation. J Clin Nurs. (2017) 26(1–2):103–14. doi: 10.1111/jocn.13381
11. McCance T, McCormack B. The person-centered practice framework. In: McCormack B, McCance T, Bulley C, Brown D, McMillan A, Martin S, editors. Fundamentals of Person-centered healthcare Practice. 1st ed. Oxford: Wiley Blackwell (2021). p. 23–32.
12. Dys S, Tunalilar O, Hasworth S, Winfree J, White DL. Person-centered care practices in nursing homes: staff perceptions and the organizational environment. Geriatr Nurs. (2022) 43:188–96. doi: 10.1016/j.gerinurse.2021.11.018
13. Gluyas H. Patient-centered care: improving healthcare outcomes. Nurs Stand. (2015) 30(4):50–7. doi: 10.7748/ns.30.4.50.e10186
14. Jeon YH, Simpson JM, Li Z, Cunich MM, Thomas TH, Chenoweth L, et al. Cluster randomized controlled trial of an aged care specific leadership and management program to improve work environment, staff turnover, and care quality. J Am Med Dir Assoc. (2015) 16(7):629.e19–e28. doi: 10.1016/j.jamda.2015.04.005
15. Moenke L, Handley M, Goodman C. The influence of care home managers’ leadership on the delivery of person-centered care for people living with dementia: a systematic review. J Nurs Manag. (2023) 2023:9872272. doi: 10.1155/2023/9872272
16. Specchia ML, Cozzolino MR, Carini E, Di Pilla A, Galletti C, Ricciardi W, et al. Leadership styles and nurses’ job satisfaction: results of a systematic review. Int J Environ Res Public Health. (2021) 18(4):1552. doi: 10.3390/ijerph18041552
17. Poels J, Verschueren M, Milisen K, Vlaeyen E. Leadership styles and leadership outcomes in nursing homes: a cross-sectional analysis. BMC Health Serv Res. (2020) 20:1009. doi: 10.1186/s12913-020-05854-7
19. Laguia A, Navas-Jiménez MC, Schettini R, Rodríguez-Batalla F, Guillén D, Moriano JA. Effects of secure base leadership vs. Avoidant Leadership on Job Performance. Businesses. (2024) 4(3):438–52. doi: 10.3390/businesses4030027
20. Cardiff S, McCormack B, McCance T. Person-centered leadership: a relational approach to leadership derived through action research. J Clin Nurs. (2018) 27:3056–69. doi: 10.1111/jocn.14492
21. Lood Q, Carlström E, Klinga C, Barenfeld E. A collaborative endeavour to integrate leadership and person-centered ethics: a focus group study on experiences from developing and realising an educational programme to support the transition towards person-centered care. BMC Health Serv Res. (2024) 24:395. doi: 10.1186/s12913-024-10793-8
22. Eide T, Cardiff S. Leadership research—a person-centered agenda. In: McCormack B, van Dulmen S, Eide H, Skovdahl K, Eide T, editors. Person-centered Healthcare Research. 1st ed. Oxford: Wiley-Blackwell (2017). p. 95–115.
23. Seljemo C, Viksveen P, Ree E. The role of transformational leadership, job demands and job resources for patient safety culture in Norwegian nursing homes: a cross-sectional study. BMC Health Serv Res. (2020) 20:799. doi: 10.1186/s12913-020-05671-y
24. Zonneveld N, Pittens C, Minkman M. Appropriate leadership in nursing home care: a narrative review. Leadersh Health Serv. (2021) 34(1):16–36. doi: 10.1108/LHS-04-2020-0012
25. Bennett N, Wise C, Woods PA, Harvey JA. Distributed Leadership. Nottingham: National College of School Leadership (2003).
26. Gronn P. Distributed leadership as a unit of analysis. Leadersh Q. (2002) 13(4):423–51. doi: 10.1016/S1048-9843(02)00120-0
27. Jambo D, Hongde L. The effect of principal’s distributed leadership practice on students’ academic achievement: a systematic review of the literature. Int J High Educ. (2020) 9(1):189–98. doi: 10.5430/ijhe.v9n1p189
28. European Union Agency for Fundamental Rights. Standards on residential care. Available online at: https://fra.europa.eu/en/content/standards-residential-care (Accessed Jun 3, 2025).
29. Act on municipal health and care services, etc. (Health and Care Services Act)—Chapter 3. Municipalities’ responsibility for health and care services. Lovdata. Available online at: https://lovdata.no/dokument/NL/lov/2011-06-24-30 (Accessed Jun 3, 2025).
30. Anker-Hansen C, Skovdahl K-I, McCormack B, Tønnessen S. Collaboration between home care staff, leaders, and care partners of older people with mental health problems: a focus on personhood. Scand J Caring Sci. (2019) 34(1):128–38. doi: 10.1111/scs.12714
31. Dickson C, Peelo-Kilroe L. Being person-centered in community and ambulatory services. In: McCormack B, McCance T, Bulley C, Brown D, McMillan A, Martin S, editors. Fundamentals of Person-centered care: Principles & Practice for Healthcare Students.1st ed. Oxford: Wiley-Blackwell (2021). p. 189–97.
32. Aromataris E, Munn Z. JBI Manual for Evidence Synthesis. JBI. (2020). doi: 10.46658/JBIMES-20-01
33. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 Explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. Br Med J. (2021) 372:n160. doi: 10.1136/bmj.n160
34. Barry S, Dalton R, Eustace-Cook J. Understanding change in complex health systems: a review of the literature on change management in health and social care 2007–2017. Organisation Development and Design Services. (2018). p. 1–44. Available online at: https://www.hse.ie/changeguide (Accessed June 03, 2025).
35. Hannes K. Critical appraisal of qualitative research. In: Noyes J, Booth A, Hannes K, Harden A, Harris J, Lewin S, Lockwood C, editors. Supplementary Guidance for Inclusion of Qualitative Research in Cochrane Systematic Reviews of Interventions. Cochrane Collaboration Qualitative Methods Group (2011). p. 1–14. Available online at: http://cqrmg.cochrane.org/supplemental-handbook-guidance (Accessed June 03, 2025).
36. Dijkshoorn ABC, van Stralen HE, Sloots M, Schagen SB, Visser-Meily JMA, Schepers VPM. Prevalence of cognitive impairment and change in patients with breast cancer: a systematic review of longitudinal studies. Psychooncology. (2021) 30(5):635–48. doi: 10.1002/pon.5623
37. Lizarondo L, Stern C, Salmond S, Carrier J, Cooper K, Godfrey C, et al. Methods for data extraction and data transformation in convergent integrated mixed methods systematic reviews. JBI Evid Synth. (2025) 23(3):429–40. doi: 10.11124/JBIES-24-00331
38. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan — a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
39. Backman A, Sjögren K, Lindkvist M, Lövheim H, Edvardsson D. Towards person-centeredness in aged care—exploring the impact of leadership. J Nurs Manag. (2016) 24(6):766–74. doi: 10.1111/jonm.12380
40. Backman A, Ahnlund P, Sjögren K, Lövheim H, McGilton KS, Edvardsson D. Embodying person-centered being and doing: leading towards person-centered care in nursing homes as narrated by managers. J Clin Nurs. (2020) 29(1–2):172–83. doi: 10.1111/jocn.15075
41. Backman A, Sjögren K, Lövheim H, Lindkvist M, Edvardsson D. The influence of nursing home managers’ leadership on person-centered care and stress of conscience: a cross-sectional study. BMC Nurs. (2021) 20:200. doi: 10.1186/s12912-021-00718-9
42. Duan Y, Mueller CA, Yu F, Talley KM, Shippee TP. The relationships of nursing home culture change practices with resident quality of life and family satisfaction: toward a more nuanced understanding. Res Aging. (2022) 44(2):174–85. doi: 10.1177/01640275211012652
43. Hamiduzzaman M, Kuot A, Greenhill J, Strivens E, Isaac V. Towards personalized care: factors associated with the quality of life of residents with dementia in Australian rural aged care homes. PLoS One. (2020) 15(5):e0233450. doi: 10.1371/journal.pone.0233450
44. Jacobsen FF, Mekki TE, Førland O, Folkestad B, Kirkevold Ø, Skår R, et al. A mixed method study of an education intervention to reduce use of restraint and implement person-centered dementia care in nursing homes. BMC Nurs. (2017) 16:55. doi: 10.1186/s12912-017-0244-0
45. Lynch BM, McCance T, McCormack B, Brown D. The development of the person-centered situational leadership framework: revealing the being of person-centeredness in nursing homes. J Clin Nurs. (2018) 27(3–4):427–40. doi: 10.1111/jocn.13949
46. Rokstad AMM, Vatne S, Engedal K, Selbæk G. The role of leadership in the implementation of person-centered care using dementia care mapping: a study in three nursing homes. J Nurs Manag. (2015) 23(1):15–26. doi: 10.1111/jonm.12072
47. Røen I, Kirkevold Ø, Testad I, Selbæk G, Engedal K, Bergh S. Person-centered care in Norwegian nursing homes and its relation to organizational factors and staff characteristics: a cross-sectional survey. Int Psychogeriatr. (2018) 30(9):1279–90. doi: 10.1017/S1041610217002708
48. Røsvik J, Mjørud M. We must have a new VIPS meeting soon!” barriers and facilitators for implementing the VIPS practice model in primary health care. Dementia (London). (2021) 20(8):2649–67. doi: 10.1177/14713012211007409
49. Martin J, McCormack B, Fitzsimons D, Spirig R. The importance of inspiring a shared vision. Int Pract Dev J. (2014) 4(2):4. doi: 10.19043/ipdj.42.004
50. Feldthusen C, Forsgren E, Wallström S, Andersson V, Löfqvist N, Sawatzky R. Centeredness in health care: a systematic overview of reviews. Health Expect. (2022) 25:885–901. doi: 10.1111/hex.13461
51. Gottlieb LN, Gottlieb B, Bitzas V. Creating empowering conditions for nurses with workplace autonomy and agency: how healthcare leaders could be guided by strengths-based nursing and healthcare leadership (SBNH-L). J Healthc Leadersh. (2021) 13:169–81. doi: 10.2147/JHL.S221141
52. Ta’an WF, Alhurani J, Alhalal E, Al-Dwaikat TN, Al-Faouri I. Nursing empowerment: how job performance is affected by a structurally empowered work environment. J Nurs Adm. (2020) 50(12):635–41. doi: 10.1097/NNA.0000000000000951
53. Santana MJ, Manalili K, Jolley RJ, Zelinsky S, Lu M. How to practice person-centered care: a conceptual framework. Health Expect. (2018) 21(2):429–40. doi: 10.1111/hex.12640
54. Moore L, Britten N, Lydahl D, Naldemirci Ö, Elam M, Wolf A. Barriers and facilitators to the implementation of person-centered care in different healthcare contexts. Scand J Caring Sci. (2017) 31(4):662–73. doi: 10.1111/scs.12376
55. Bahlman-van Ooijen W, van Belle E, Bank A, de Man-Van Ginkel J, Huisman-de Waal G, Heinen M. Nursing leadership to facilitate patient participation in fundamental care: an ethnographic qualitative study. J Adv Nurs. (2023) 79(3):1044–55. doi: 10.1111/jan.15329
57. Conroy T. Factors influencing the delivery of the fundamentals of care: perceptions of nurses, nursing leaders and healthcare consumers. J Clin Nurs. (2018) 27(11–12):2373–86. doi: 10.1111/jocn.14183
58. Aagestad C. Førstelinjeledere i døgnkontinuerlige tjenester. Norsk sykepleieforbund. (2022). p. 1–58. Available online at: https://www.agendakaupang.no/wpcontent/uploads/2022/10/Rapport_NSF_Forstelinjeledere-i-dognkontinuerlige-tjenester_Agenda-Kaupang.pdf (Accessed June 03, 2025).
59. Kirchhoff JW, Karlsson JC. Alternative careers at the first level of management: first-line nurse managers’ responses to role conflict. Leadersh Health Serv. (2019) 32(3):405–18. doi: 10.1108/LHS-11-2017-0067
60. Buetow S. Person-centered Health Care: Balancing the Welfare of Clinicians and Patients. New York, NY: Routledge (2016).
61. Magerøy MR, Macrae C, Braut GS, Wiig S. Managing patient safety and staff safety in nursing homes: exploring how leaders of nursing homes negotiate their dual responsibilities: a case study. Front Health Serv. (2024) 4:1275743. doi: 10.3389/frhs.2023.1275743
62. Ree E, Johannessen T, Wiig S. How do contextual factors influence quality and safety work in the Norwegian home care and nursing home settings? A qualitative study about managers’ experiences. BMJ Open. (2019) 9:e025197. doi: 10.1136/bmjopen-2018-025197
63. Bolman LG, Deal TE. Nytt perspektiv på organisasjon og ledelse: strukturer, HR, politikk og symboler. 6th ed Oslo: Gyldendal (2018).
64. Lindsay C. Distributed leadership in nursing and healthcare: theory, evidence, and development. Soc Policy Adm. (2023) 57(1):104–6. doi: 10.1111/spol.12847
65. Sammut R, Briffa B, Curtis EA. Distributed leadership and nurses’ job satisfaction: a survey. Int J Health Care Qual Assur. (2021) 34(1):37–51. doi: 10.1108/LHS-07-2020-0052
66. Dickson CAW, Merrell J, McIlfatrick S, Westcott L, Gleeson N, McCormack B. Leadership practices that enable healthful cultures in clinical practice: a realist evaluation. J Clin Nurs. (2024) 33:982–97. doi: 10.1111/jocn.16951
Keywords: attitudes, empowerment, leadership, management, nursing homes, older people, person-centered, role modeling
Citation: Anker-Hansen C, Olsen LB, Grøndahl VA, Leonardsen A-CL, Helgesen AK, Bååth C, Halvorsrud L, Restad G, McCormack B and Femdal I (2025) The interplay of leadership dynamics and person-centred practice in nursing homes: a mixed methods systematic review. Front. Health Serv. 5:1535414. doi: 10.3389/frhs.2025.1535414
Received: 27 November 2024; Accepted: 23 June 2025;
Published: 14 July 2025.
Edited by:
Vaibhav Tyagi, The University of Sydney, AustraliaReviewed by:
Busra Bildik, Karabük University, TürkiyeKelly Marriott-Statham, University of Canberra, Australia
Copyright: © 2025 Anker-Hansen, Olsen, Grøndahl, Leonardsen, Helgesen, Bååth, Halvorsrud, Restad, McCormack and Femdal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camilla Anker-Hansen, Y2FAaGlvZi5ubw==