 Rasmus Kragh Jakobsen
Rasmus Kragh Jakobsen Ingeborg Farver-Vestergaard1,2
Ingeborg Farver-Vestergaard1,2 Anders Løkke
Anders Løkke- 1Department of Medicine, Lillebaelt Hospital, Vejle, Denmark
- 2Department of Regional Health Research, University of Southern Denmark, Odense, Denmark
Introduction: Smoking cessation remains among the most effective interventions for improving outcomes in patients with chronic obstructive pulmonary disease (COPD). Quitting smoking slows disease progression, reduces morbidity, improves quality of life and increases life expectancy. However, a substantial proportion of patients with COPD continue to smoke, and generic cessation strategies often fall short in this population. While most cessation research targets “healthy” smokers, individuals with COPD face additional challenges – including higher nicotine dependence and psychological comorbidities – that complicate quit attempts.
Methods: This mini-review summarises randomised controlled trials (RCTs) investigating smoking cessation interventions in COPD.
Results: Our study reveals wide variability in the intensity, duration and components of interventions, with only a minority achieving long-term abstinence. Notably, two high-performing studies stand out for their comprehensive, long-term and individualised approaches. These findings suggest that success in smoking cessation for patients with COPD relies not only on the right intervention components but also on the construction, durability and sustained support.
Conclusion: To support and sustain smoking cessation among patients with COPD, multicomponent, high-intensity and long-duration interventions tailored to individual needs appear to be required, with an emphasis on ongoing support and frequent follow-up.
1 Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide, and smoking is its most significant modifiable risk factor (1–3). It is well-established that smoking cessation is among the most effective existing interventions to halt disease progression, reduce symptom burden, improve quality of life and prolong survival (2–5). Despite this, smoking prevalence remains high among patients with COPD (6). This raises a vital question: Why are existing cessation interventions not effective in this high-risk population?
Traditional smoking cessation strategies – centered on counseling, pharmacotherapy (i.e., varenicline, buproprione, cytisine) and nicotine replacement therapy (NRT) – are generally developed and tested in otherwise healthy smokers (7, 8). While some of these interventions have been extended to patients with COPD (4, 9), this population often presents with more severe nicotine dependence, psychological distress and lower self-efficacy (10, 11). These factors may render standard cessation strategies insufficient and suggest the need for targeted approaches.
To illustrate, one may liken smoking cessation interventions to vehicles helping the patients ascend a steep incline. While most vehicles have the necessary components – wheels (NRT), engine (pharmacotherapy) and steering (behavioural support) – only some are built with the structural integrity and endurance required to complete the journey. To better understand what enables longterm cessation among smokers with COPD, we conducted a mini-review of randomised controlled trials (RCTs) evaluating smoking cessation interventions in this population.
2 Methods
We performed a mini-review to map the characteristics and effectiveness of RCTs targeting smoking cessation in patients with COPD. Following the Joanna Briggs Institute guidelines (12), our protocol was registered with the Open Science Framework (https://osf.io/md9ab).
Using a comprehensive block search strategy combining terms for COPD, smoking cessation interventions and cessation outcomes, we searched the databases of Medline, Embase and CINAHL from their inception to November 2024, combining the following search terms:
Block 1: (chronic obstructive lung disease OR COPD OR Chronic Obstructive Pulmonary Dis* OR Chronic Obstructive Air* Dis* OR COAD OR Airflow Obstruction?, Chronic OR Chronic Air* Obstruction? OR chronic obstructive bronchopulmonary Dis* OR chronic obstructive lung Dis* OR chronic obstructive respiratory Dis* OR chronic pulmonary obstructive dis* OR lung chronic obstructive Dis* OR lung dis*, chronic obstructive OR obstructive chronic lung Dis* OR obstructive chronic pulmonary Dis* OR obstructive lung Dis*, chronic OR pulmonary Dis*, chronic obstructive OR Asthma-Chronic Obstructive Pulmonary Disease Overlap Syndrome OR acute exacerbations of chronic bronchitis OR AECB OR Bronchitis, Chronic OR Chronic Bronchitis OR Pulmonary Emphysema).
AND
Block 2: (counseling OR e-counseling OR motivational interviewing OR nicotine replacement therapy OR varenicline OR amfebutamone OR Directive Counsel?ing OR Counsel?ing, Directive OR Prescriptive Counsel?ing OR Counsel?ing, Prescriptive OR Motivational Interview* OR Interview*, Motivational OR Distance Counsel?ing OR Counsel?ing, Distance OR E-Counsel?ing OR Ecounsel?ing OR E-Therap* OR ETherap* OR Online Counsel?ing OR remote Counsel?ing OR tele Counsel?ing OR Nicotine Replacement Therap* OR Therap*, Nicotine Replacement OR vareniclin? OR Chantix OR Champix OR vareniclin? tartrat? OR tyrvaya OR buprop* OR Amfebutamon? OR zyban OR Wellbutrin OR Quomen OR Zyntabac OR aplenzin OR budep* OR buxon OR elontril OR forfivo OR odranal OR quomem OR wellbatrin OR wellbutrin).
AND
Block 3: (smoking cessation OR Cessation?, Smoking OR Smoking Cessation? OR Giving Up Smoking OR Smoking?, Giving Up OR Up Smoking, Giving OR Quit* Smoking OR Smoking, Quitting OR * Smoking OR Smoking, Stopping OR abstination, smoking OR abstinence from nicotine OR abstinence from smoking OR abstinence from tobacco OR dehabituation, smoking OR nicotine abstin* OR nicotine cessation OR nicotine withdrawal OR smoking abstinence OR smoking dehabituation OR tobacco-use cessation).
The full search protocol as well as a PRISMA flowchart can be found in the Supplementary Material. Additional studies were identified through forward citation searches and comparison with prior systematic reviews (4, 13). We included studies published in English or Nordic languages that evaluated behavioural and/or pharmacologic cessation interventions in adults with a confirmed diagnosis of COPD. References were excluded if they were duplicates, protocols, reviews, conference abstracts and session posters, studies on animals or cells and mixed interventions other than smoking cessation. Studies were also excluded if they were not placebo-controlled RCT's or if the study focus was for another chronic disease and the COPD specific data could not be separated but included studies on patients with mixed morbidities (COPD and co-morbidities).
3 Results
We identified 15 placebo-controlled RCTs (5, 14–27) that investigated smoking cessation in patients with COPD, involving a total of 11.432 participants (Table 1). The studies were generally similar in terms of participant demographics (age, sex, number of pack-years) and disease severity [represented all GOLD grades (2) with an overweight of grade I and II].
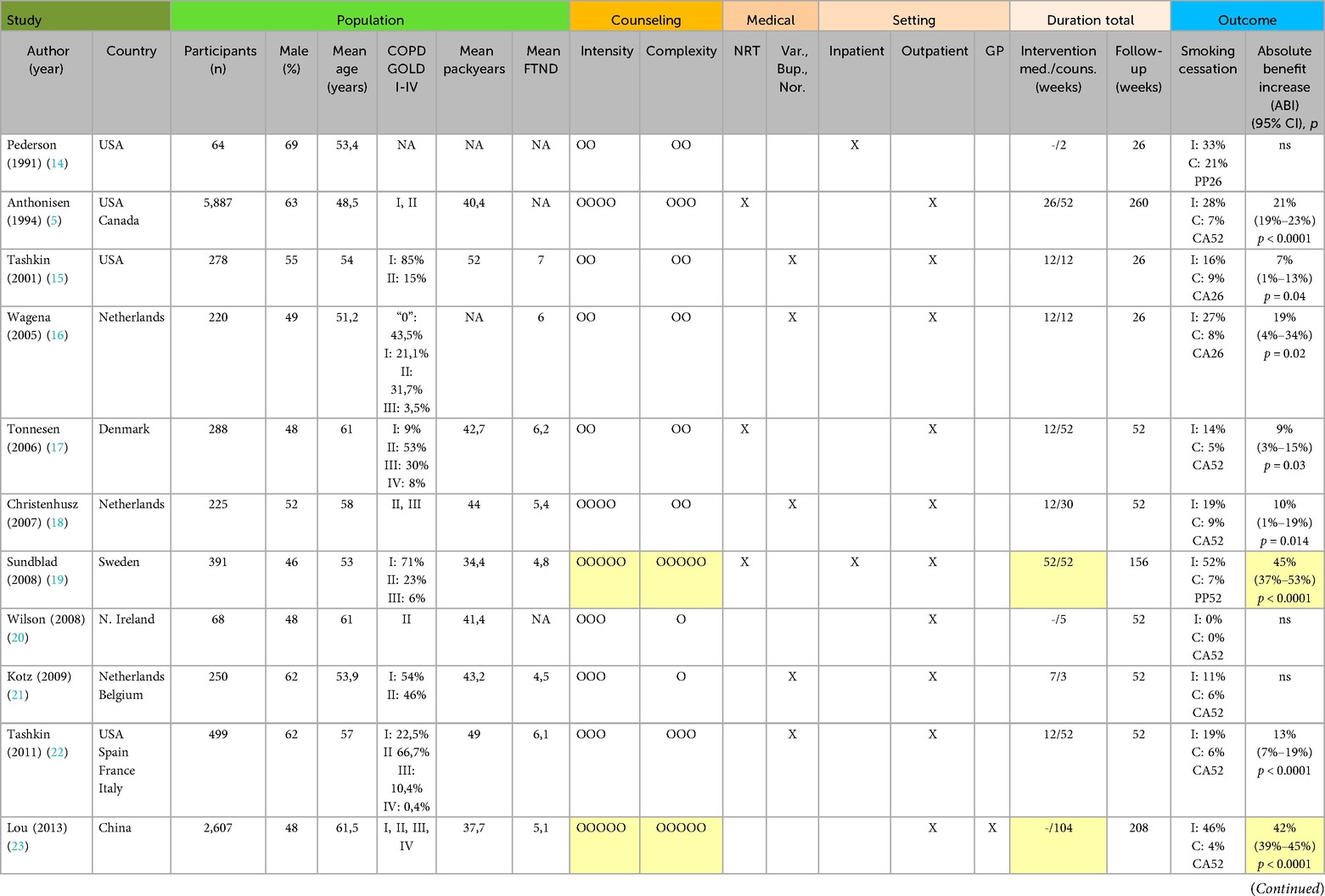
Table 1. Characteristics of the included studies.
All studies used counseling, six studies used pharmacotherapy in combination with counseling, three studies used NRT in combination with counseling, and one study combined all three components. Most medicine interventions lasted 12 weeks, though NRT-protocols extended up to 52 weeks. The specifics of the intervention delivery varied widely across studies (Figure 1):
• Duration ranged from 2 weeks to 2 years
• Intensity varied from brief advice (<60 min) to 11-day inpatient programs
• Number of sessions ranged from 4 to 26
• Healthcare professionals delivering the interventions included doctors, nurses, psychologists and/or trained counselors
• All studies used an outpatient setting except one study with an inpatient setting, and two studies combined the outpatient setting with either hospitalisation or visits by general practitioners. None used a community setting
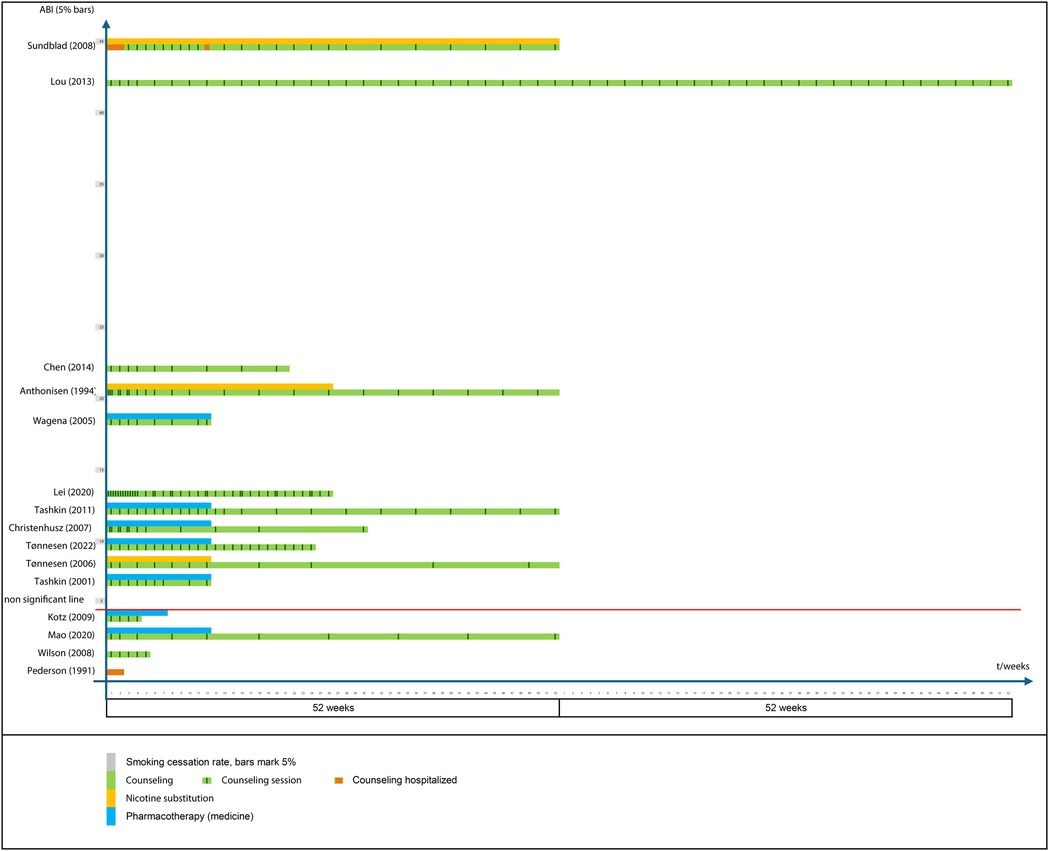
Figure 1. Interventions, time and smoking cessation success compared. 15 RCT's from 1991 to 2022. (1) axis is time in weeks, (2) axis is absolute benefit increases (ABI). Studies are arranged in order within 5% intervals of smoking cessation rates (grey bars). The red “non significant line” is added to mark the 4 studies where no statistically significant difference was seen between the intervention and control group (ie. ABI = 0%). Intervention types are counseling (green), nicotine replacement therapy (orange) and pharmacotherapy (blue). For studies reporting both NRT and medicines only the highest ABI is shown. To illustrate counseling intensity vertical lines marks each contact point whether individual or group sessions, phone call or text messages. Red vertical lines signifies hospitalised counseling.
Four studies followed the participants long-term (≥3 years) while the remaining studies followed participants for 12 months or less. Reported continuous abstinence (CA) rates ranged from 0% to 53%, with absolute benefit increases (ABI) of 0%–45% over control groups (Figure 1). Thirteen studies showed modest ABI (0%–22%) while two studies reported markedly higher ABIs of 42% and 45% (19, 23). These two studies also offered the most intensive, multicomponent and long-duration interventions. Hence, the study by Sundblad et al. (19) delivered an intervention that included bringing the patients (in groups of 4–10) to the hospital for smoking cessation during an 11 day stay. The stay included NRT, physical exercise and 1-hour daily meetings with a trained cessation nurse (individual counseling) and in addition a structured educational program on nicotine, health effects, dietary education, physical training, lung function testing delivered by a doctor, physiotherapist, dietitian, laboratory technician, psychologist, occupational therapist, and nurse. At home the intervention continued for 2–3 months with weekly telephone calls of 5–30 min (nurse). Then a second hospitalization for 2–4 days with spouses invited that included group discussions on how to sustain abstinence and avoid relapse. Then 10 months at home with first bi-weekly and later monthly telephone contacts. The study by Lou et al. (23) tested an intervention that included training more than 100 general practitioners in behavioural interventions for quitting to enable them to better supervise and advice the patients. The patients received individual counselling both in the general practice and during home visits by the general practitioners once per week for the first month and then at least once a month for the remainder of the intervention. Additionally, the patients were asked to participate in monthly group discussions and share the experience of quitting as well as participate in bi-monthly education by a multidisciplinary group of experts including respiratory, rehabilitation, nutrition, sports, and psychology specialists who joined the group meetings. The treatment lasted two years.
It should be noted that a Cochrane review (4) on smoking cessation for people with COPD recommends caution in the interpretation of the results of the Sundblad et al. (19) because of risk of bias due to lack of “blinding of participants and personnel”, “blinding of outcome assessment”, “incomplete outcome data” and “other bias”. However, “blinding of participants and personnel” is not possible for behavioral interventions nor for the “blinding of outcome assessment” when abstinence is self-reported. The review did find a low risk of bias due to “random sequence generation”, “allocation concealment” and “selective reporting” for Sundblad et al. and the Lou et al. (23) study was found to have an unclear risk of bias since four components of the risk of bias was unclear. The risk of selective reporting was assessed as low.
Overall, 12 of the 15 studies we found are included in the Cochrane review and almost all show either high or unclear risk of bias with the same four components as Sundblad et al. as well as low risk of bias for the same three components. This suggests an overall comparable methodological quality and a risk of bias that is at least part due to studying behavioral interventions.
4 Discussion
It is already well-established that a combination of behavioural and pharmacotherapeutic interventions are superior to single-component approaches in COPD (13). However, despite the consistent inclusion of counseling, pharmacotherapy and/or NRT across studies in the present review, there was substantial heterogeneity in how these components were implemented. No single combination of components appeared to consistently lead to successful, sustained outcomes, suggesting that effectiveness may depend more on how interventions are delivered than on what they contain.
4.1 What sets the top performers apart?
Two studies – conducted by Sundblad et al. and Lou et al. – demonstrated superior outcomes with ABIs exceeding 40% [45% (37%–53%, p < 0.0001) and 42% (39%–45%, p < 0.0001) respectively]. Though methodologically and contextually distinct, they shared a number of features:
• High intensity behavioural support
• Multidisciplinary involvement
• Long intervention duration (≥1 year)
• Frequent follow-up and patient engagement
• Broad educational and psychosocial support
Lou et al. used monthly home visits and group sessions with multidisciplinary input over two years. Sundblad et al. conducted an 11-day inpatient program followed by structured outpatient follow-up, including family involvement. While the generalisability and methodological rigor of these studies warrant further scrutiny (e.g., potential biases and use of point prevalence), their success point towards the value of long-term, individualised and intensive intervention frameworks.
None of the other 13 studies used as comprehensive or intensive interventions but within this group we may notice a similar trend: The four studies with the longest counseling duration (52 weeks) display a trend of higher outcome ABI corresponding with the level of intensity of the counseling from the highest and to the lowest (Anthonisen et al.; Tashkin et al.; Tønnesen et al.; Mao et al.) And conversely, we also notice how the three studies using the briefest counseling interventions (Pederson et al., Wilson et al. and Kotz et al.) exhibit the lowest outcome ABI.
Two studies seem to contradict the trend at a first glance (Figure 1). The study by Lei et al. displays relatively low outcome ABI compared to the very high number of counseling contacts. However, most of these contacts were text-messages which may not have as strong an effect as face-to-face or telephone contacts. The Chen et al. study display a high outcome ABI compared to the relatively short duration and low intensity, however, it should be noted that the outcome was measured after 26 weeks not 52 weeks like fx Anthonisen et al. and since the quit-rates tend to fall over time the ABI is falsely high in comparison. Similarly, the outcome ABI's reported by Wagena et al., Lei et al., Christenhusz et al., Tønnesen et al. (2022), Tashkin et al. (2001) would be expected to be lower at 52 weeks.
As pointed out in a recent scoping review of smoking cessation interventions in COPD (28), well-controlled clinical trials and rigorous, large-scale observational studies with long-term follow-up are needed to determine the optimal pharmacotherapy and the most cost-effective modalities of comprehensive smoking cessation interventions.
4.2 The role of structure and support
Returning to the “vehicle” metaphor, all interventions included in the present review were constructed with the necessary parts, but only a few were built to endure the challenging terrain of COPD-related smoking addiction. Hence, effective cessation in this population may require early-phase intensity to overcome withdrawal, ongoing support to prevent relapse, family and community involvement for sustained motivation, and tailored behavioural strategies responding to psychological burden and needs. Short-term interventions may capture initial abstinence but fail to support long-term cessation. The declining quit rates in studies with longer follow-up suggest that prolonged abstinence may be overestimated in brief interventions.
Intensive, long-term contact may provide psychological benefits beyond smoking cessation specifically. Due to severe addiction, most patients need several attempts to succeed with sustained smoking abstinence (29), and patients may feel “seen” and supported in this long and winding process when clinicians are personalising support strategies. Such an approach has the power to challenge common fatalistic attitudes that quitting is of no use once the disease, has developed (30) and to support the patients in converting unhelpful shame and guilt about smoking into helpful actions (i.e., attempts to quit) (31). Moreover, these interventions may signal how crucial cessation is, which can counter-act the therapeutic nihilism that is oftentimes associated with advanced COPD (32). A recent study by Zimmermann et al. (33) shows that patients with COPD, irrespective of age, sex, health literacy and burden of disease, welcome information about their illness and how to manage it – also when it comes to behavioural adaptation that require their own effort.
4.3 Financial considerations and reimbursement plan
Comprehensive interventions are undoubtedly more resource-intensive. However, their cost-effectiveness must be viewed in the context of the immense societal burden of COPD, including hospitalisations, disability and premature withdrawal from the workforce, which was recently pointed out as an immense problem across countries by the World Health Organisation (WHO) and the European Respiratory Society (ERS) (34). Of the two resource-intensive studies highlighted here only Sundblad et al. considers societal cost and show how their smoking intervention program, despite being extensive and expensive, would be cost-effective within a few years in the Swedish society. More specifically they calculate the cost at the time to render one smoke-free person at the 3-year follow-up to approximately 13.400 US$ and compare this to the estimated yearly societal cost of 790 US$, 4.100 US$ and 10.332 US$ for a person with mild, moderate and severe COPD respectively. In other words, halting progression makes economic sense to society not to mention the health and quality of life benefits to the patients.
Notably, inpatient rehabilitation is routinely used in other addiction disorders (34), and smokers with COPD, facing a comparably lethal and costly addiction, are rarely offered similar treatment intensity. Addressing this disparity will require structural changes, including cross-sector reimbursement models that reduce fragmentation and support patients along their cessation journey.
Initiatives like the London Tobacco Alliance's toolkit for pharmacotherapy commissioning pathways (35) as well as professional training resources developed by the National Centre for Smoking Cesssation and Training (NCSCT) in the UK (36), illustrate promising approaches to integration of care at the system-level.
4.4 Limitations
Several limitations should be acknowledged. First, the included studies varied significantly in methodological quality, definitions of abstinence (e.g., point prevalence vs. continuous), and length of follow-up, which complicates direct comparisons and generalizability. Second, publication bias cannot be ruled out, as interventions are more likely to be reported if successful. Third, patient characteristics such as socioeconomic status, comorbidities and health literacy were not systematically accounted for, yet these may significantly influence cessation outcomes.
5 Conclusion
It seems like we already know the important components of smoking cessation: counseling, NRT and pharmacotherapy. But the question is why don't they work better for patients with COPD? Existing studies varies widely in their specific delivery features, and evidence from two standout studies suggests that higher long-term quit rates are achievable through a combination of longer duration, higher intensity and individualised support. COPD-specific cessation strategies must move beyond standard protocols and towards tailored interventions that reflect the unique challenges of this population.
There is cause for cautious optimism. With strategic refinement and investment, cessation programs can be optimised to help more patients with COPD overcome addiction, improve their quality of life, and reduce the broader public health burden. Future research should systematically explore the relative contributions of intervention duration, complexity and support structure in achieving lasting abstinence in this particular patient group.
Author contributions
RKJ: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. IF-V: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing. AL: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
This is a short text to acknowledge the contributions of specific colleagues, institutions, or agencies that aided the efforts of the authors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2025.1659295/full#supplementary-material
References
1. WHO. Chronic obstructive pulmonary disease (COPD) (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (Accessed January 2025).
2. Agustí A, Celli BR, Criner GJ, Halpin D, Anzueto A, Barnes P, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Arch Bronconeumol. (2023) 59(4):232–48. doi: 10.1016/j.arbres.2023.02.009
3. Løkke A, Lange P, Scharling H, Fabricius P, Vestbo J. Developing COPD: a 25 year follow up study of the general population. Thorax. (2006) 61(11):935–9. doi: 10.1136/thx.2006.062802
4. van Eerd EA, van der Meer RM, van Schayck OC, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. (2016) 2016(8):Cd010744. doi: 10.1002/14651858.CD010744.pub2
5. Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The lung health study. JAMA. (1994) 272(19):1497–505. doi: 10.1001/jama.1994.03520190043033
6. Trofor AC. Smoking Cessation in Patients with Chronic Obstructive Pulmonary Disease. In: Tobacco Cessation Guidelines for High Risk Populations. TOB.g Project, Tobacco Cessation Guidelines for High Risk Groups (TOB.g)> (2017). http://tob-g.eu/wp-content/uploads/TOB-G-BOOK-DIGITAL-VERSION.pdf (Accessed September 04, 2025).
7. Stead LF, Koilpillai P, Fanshawe TR, Lancaster T. Combined pharmacotherapy and behavioural interventions for smoking cessation. Cochrane Database Syst Rev. (2016) 3(3):Cd008286. doi: 10.1002/14651858.CD008286.pub3
8. Hartmann-Boyce J, Livingstone-Banks J, Ordóñez-Mena JM, Fanshawe TR, Lindson N, Freeman SC, et al. Behavioural interventions for smoking cessation: an overview and network meta-analysis. Cochrane Database Syst Rev. (2021) 1(1):Cd013229. doi: 10.1002/14651858.CD013229.pub2
9. Tønnesen P. Smoking cessation and COPD. Eur Respir Rev. (2013) 22(127):37–43. doi: 10.1183/09059180.00007212
10. van Eerd EA, van Rossem CR, Spigt MG, Wesseling G, van Schayck OC, Kotz D. Do we need tailored smoking cessation interventions for smokers with COPD? A comparative study of smokers with and without COPD regarding factors associated with tobacco smoking. Respiration. (2015) 90(3):211–9. doi: 10.1159/000398816
11. Jiménez-Ruiz CA, Andreas S, Lewis KE, Tonnesen P, van Schayck CP, Hajek P, et al. Statement on smoking cessation in COPD and other pulmonary diseases and in smokers with comorbidities who find it difficult to quit. Eur Respir J. (2015) 46(1):61–79. doi: 10.1183/09031936.00092614
12. Peters MDJ, GC , McInerney P, Munn Z, Tricco AC, Khalil H. Scoping Reviews: JBI (2020). Available online at: https://synthesismanual.jbi.global (Accessed September 04, 2025).
13. Wei X, Guo K, Shang X, Wang S, Yang C, Li J, et al. Effects of different interventions on smoking cessation in chronic obstructive pulmonary disease patients: a systematic review and network meta-analysis. Int J Nurs Stud. (2022) 136:104362. doi: 10.1016/j.ijnurstu.2022.104362
14. Pederson LL, Wanklin JM, Lefcoe NM. The effects of counseling on smoking cessation among patients hospitalized with chronic obstructive pulmonary disease: a randomized clinical trial. Int J Addict. (1991) 26(1):107EP–19. doi: 10.3109/10826089109056242
15. Tashkin D, Kanner R, Bailey W, Buist S, Anderson P, Nides M, et al. Smoking cessation in patients with chronic obstructive pulmonary disease: a double-blind, placebo-controlled, randomised trial. Lancet. (2001) 357(9268):1571EP–5. doi: 10.1016/S0140-6736(00)04724-3
16. Wagena EJ, Knipschild PG, Huibers MJH, Wouters EFM, Van Schayck CP. Efficacy of bupropion and nortriptyline for smoking cessation among people at risk for or with chronic obstructive pulmonary disease. Arch Intern Med. (2005) 165(19):2286EP–92. doi: 10.1001/archinte.165.19.2286
17. Tonnesen P, Mikkelsen K, Bremann L. Nurse-conducted smoking cessation in patients with COPD using nicotine sublingual tablets and behavioral support. Chest. (2006) 130(2):334EP–42. doi: 10.1378/chest.130.2.334
18. Christenhusz L, Pieterse M, Seydel E, van der Palen J. Prospective determinants of smoking cessation in COPD patients within a high intensity or a brief counseling intervention. Patient Educ Couns. (2007) 66(2):162–6. doi: 10.1016/j.pec.2006.11.006
19. Sundblad BM, Larsson K, Nathell L. High rate of smoking abstinence in COPD patients: smoking cessation by hospitalization. Nicotine Tob Res. (2008) 10(5):883EP–90. doi: 10.1080/14622200802023890
20. Wilson JS, Fitzsimons D, Bradbury I, Elborn JS. Does additional support by nurses enhance the effect of a brief smoking cessation intervention in people with moderate to severe chronic obstructive pulmonary disease? A randomised controlled trial. Int J Nurs Stud. (2008) 45(4):508–17. doi: 10.1016/j.ijnurstu.2006.10.001
21. Kotz D, Wesseling G, Huibers MJH, Van Schayck OCP. Efficacy of confronting smokers with airflow limitation for smoking cessation. Eur Respir J. (2009) 33(4):754EP–62. doi: 10.1183/09031936.00116308
22. Tashkin DP, Rennard S, Hays JT, Ma W, Lawrence D, Lee TC. Effects of varenicline on smoking cessation in patients with mild to moderate COPD: a randomized controlled trial. Chest. (2011) 139(3):591EP–9. doi: 10.1378/chest.10-0865
23. Lou P, Zhu Y, Chen P, Zhang P, Yu J, Zhang N, et al. Supporting smoking cessation in chronic obstructive pulmonary disease with behavioral intervention: a randomized controlled trial. BMC Fam Pract. (2013) 14:91. doi: 10.1186/1471-2296-14-91
24. Chen J, Chen Y, Chen P, Liu Z, Luo H, Cai S. Effectiveness of individual counseling for smoking cessation in smokers with chronic obstructive pulmonary disease and asymptomatic smokers. Exp Ther Med. (2014) 7(3):716–20. doi: 10.3892/etm.2013.1463
25. Lei S, Li M, Duan W, Peng C, Chen P, Wu S. The long-term outcomes of tobacco control strategies based on the cognitive intervention for smoking cessation in COPD patients. Respir Med. (2020) 172:106155. doi: 10.1016/j.rmed.2020.106155
26. Le Mao R, Tromeur C, Paleiron N, Sanchez O, Gagnadoux F, Jouneau S, et al. Effect of early initiation of varenicline on smoking cessation in COPD patients admitted for exacerbation: the save randomized clinical trial. COPD. (2020) 17(1):7EP–14. doi: 10.1080/15412555.2019.1703928
27. Tønnesen P, Lawrence D, Tonstad S. Medication-assisted quit rates in participants with smoking-related diseases in EAGLES: post hoc analyses of a double-blind, randomized, placebo-controlled clinical trial. Tob Induc Dis. (2022) 20:46. doi: 10.18332/tid/146567
28. Feng L, Lv X, Wang Y, Chu S, Dai Z, Jing H, et al. Developments in smoking cessation interventions for patients with chronic obstructive pulmonary disease in the past 5 years: a scoping review. Expert Rev Respir Med. (2022) 16(7):749–64. doi: 10.1080/17476348.2022.2108797
29. Chaiton M, Diemert L, Cohen JE, Bondy SJ, Selby P, Philipneri A, et al. Estimating the number of quit attempts it takes to quit smoking successfully in a longitudinal cohort of smokers. BMJ Open. (2016) 6(6):e011045. doi: 10.1136/bmjopen-2016-011045
30. Bragadottir GH, Halldorsdottir BS, Ingadottir TS, Jonsdottir H. Patients and families realising their future with chronic obstructive pulmonary disease—a qualitative study. J Clin Nurs. (2018) 27(1-2):57–64. doi: 10.1111/jocn.13843
31. Arne M, Emtner M, Janson S, Wilde-Larsson B. COPD Patients’ perspectives at the time of diagnosis: a qualitative study. Prim Care Respir J. (2007) 16(4):215–21. doi: 10.3132/pcrj.2007.00033
32. Halpin DMG, Celli BR, Criner GJ, Frith P, López Varela MV, Salvi S, et al. It is time for the world to take COPD seriously: a statement from the GOLD board of directors. Eur Respir J. (2019) 54(1):1900914. doi: 10.1183/13993003.00914-2019
33. Zimmermann M, von Plessen CM, Kroppen D, Stanzel SB, Berger M, Wollsching-Strobel M, et al. Knowledge of and attitudes towards standard care in patients with COPD. Int J Chron Obstruct Pulmon Dis. (2025) 20:1287–97. doi: 10.2147/COPD.S489395
34. Report No.: WHO/EURO:2025-12340-52112-79990 (PDF). Chronic respiratory diseases and health equity by 2050: a spotlight on chronic obstructive pulmonary disease and asthma in the WHO European Region. Copenhagen: WHO Regional Office for Europe (2025).
35. Varenicline and Cytisine Toolkit for London: London Tobacco Alliance [Toolkit to support local commissioning pathways for provision of Varenicline and Cytisine] (2025). Available online at: https://www.londontobaccoalliance.org.uk/resources/varenicline-cytisine-toolkit/ (Accessed September 04, 2025).
36. NCSCT online training and assessment programme: National Centre for Smoking Cesssation and Training [Training modules for health and social care professionals] (2025). Available online at: https://elearning.ncsct.co.uk/england (Accessed September 04, 2025).
Keywords: chronic obstructive pulmonary disease, tobacco smoking, smoking cessation, pharmacological interventions, behavioural counseling, long-lasting abstinence, mini review
Citation: Jakobsen RK, Farver-Vestergaard I and Løkke A (2025) The uphill journey of smoking cessation in chronic obstructive pulmonary disease: why a well-built vehicle matters. Front. Health Serv. 5:1659295. doi: 10.3389/frhs.2025.1659295
Received: 3 July 2025; Accepted: 26 August 2025;
Published: 10 September 2025.
Edited by:
Ciska Hoving, Maastricht University, NetherlandsReviewed by:
Dong Liang, The First Affiliated Hospital of Shandong First Medical University, ChinaCopyright: © 2025 Jakobsen, Farver-Vestergaard and Løkke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rasmus Kragh Jakobsen, cmFzbXVzQGpha29ic2Vucy5kaw==
†Present Address: Rasmus Kragh Jakobsen,Department of Emergency Medicine, Hopital Unit West, Viborg, Denmark