 R. Cobos-Campos1,2*
R. Cobos-Campos1,2* S. Villullas3
S. Villullas3 S. García de Andoin1I. Pérez1,4C. Bermúdez-Ampudia1
S. García de Andoin1I. Pérez1,4C. Bermúdez-Ampudia1 E. López de Abechuco3
E. López de Abechuco3
- 1Primary Care, Epidemiology and Public Health Group, Bioaraba Health Research Institute, Vitoria-Gasteiz, Spain
- 2Research Network on Chronicity, Primary Care, Prevention and Health Promotion, Spain
- 3Associated Clinical Group, Bioaraba Health Research Institute, Vitoria-Gasteiz, Spain
- 4Osakidetza Basque Health Service, Vitoria-Gasteiz, Spain
Depression is one of the most prevalent psychiatric illnesses worldwide (1). The National Survey on Drug Use and Health revealed an unprecedented need for and use of mental health care resources. It is estimated that 5% of the world's adult population (1) suffers from depression with a prevalence of 4% among men and 6% among women (2). In Spain, 5.3% of the population over 15 years of age reported having depression in 2020, with a notable gender disparity: 7.2% of women compared to 3.2% of men (3–5).
The COVID-19 pandemic has had a profound impact on the mental health of the population. In 2020, approximately 21 million adults experienced a major depressive episode, and one in five Americans reported some form of mental illness during the pandemic period (6).
Moreover, according to a recent World Health Organization (WHO) report, both depression and anxiety increased by more than 25% in the first year of the pandemic (3, 7), especially in the 16–24 age group (2.7%). This rise has been driven, in part, by the context of social isolation experienced (4). Notably, the increase has also been more pronounced among women (0.6%) and in rural areas (0.7%) (4).
Depression is a common mental illness that can affect anyone. It is characterized by low mood or loss of interest in activities over extended periods (8). In addition, mental disorders contribute to 4.32% (9) of the global burden of disease, ranking them as the world's leading cause of disability and significantly contributing to workplace absenteeism (9–11).
Mental disorders often lead to a higher incidence of physical impairment (1) and greater likelihood of premature death compared to general population's expected age-related death rates (11). In addition, people with depression, regardless of age, are at increased risk of certain physical diseases (cardiovascular disease, stroke, diabetes, pain and Alzheimer's disease). The underlying reasons remain unclear. It may be attributed to reduced access to proper medical care, but there may also be physiological changes that impact on physical health (increased inflammation levels, changes in heart rate control and blood circulation, abnormalities in stress hormones production, metabolic changes…) (12).
Mental illnesses contribute significantly to morbidity, mortality and reduced quality of life worldwide (13, 14). Depression and anxiety, two common mental illnesses, were ranked respectively as the second and seventh leading causes of disability worldwide.
This complex relationship between mental and physical health highlights the need for developing strategies addressing both dimensions. In this regard, primary care is essential to tackle this growing public health concern.
Generally, primary care physicians treat mental symptoms as part of something, part of a larger, more general problem. The nature of primary care, is integrative. The more pronounced the physical symptomatology, regardless of whether the symptoms have a physical explanation or not, the greater the likelihood that a primary care patient has a mental health diagnosis (15). In other words, mental symptoms and disorders are concentrated precisely in those patients who visit their primary care physician for other reasons, such as physical illnesses or, at the very least, biomedical problems. Conversely, patients with psychological distress experience increased physical symptomatology (15).
The World Health Organisation (WHO) has published a new policy paper focusing on how countries can make mental health care more accessible and less stigmatizing through primary health care (16). The paper, entitled “Scaling up mental health services within the primary care approach: lessons from the WHO European Region”. Between one third and one half of all people presenting to primary care services do so because of mental health complaints, making primary care a crucial point for building trust in health systems. However, traditionally in many countries, in family health team models, if detected mental disorders, people may be immediately referred to specialist mental health services, where they often face long waiting times. These long delays can cause conditions to worsen, and the use of specialist services can also carry stigma, further discouraging people from seeking the help they need (16).
WHO refers primary care as the setting of choice to firstly address mental health problems. The accessibility and integrated approach of primary care make this first level of healthcare ideal to respond to the majority of mental health care needs, even in developed countries (17, 18).
Twenty five percent of individuals attending a health center have a diagnosable mental health condition, being depression the most predominant disorder. In fact, depression is the third most common cause for primary care consultation (17, 18). Therefore, it is necessary to implement collaborative strategies among different health care professionals, reinforcing the role of primary care in mental health care, and only referring to specialized services those patients requiring more intensive follow up (17–20). The risk of self-injury, the potential to harm others, or the presence of psychotic symptoms are critical factors when deciding the need for specialized psychiatric care. Geographical factors and available infrastructure also play a key role in assessing needs, since general practitioners are reluctant to refer a patient to specialized care if long journeys to hospital, often by public transport, are required. Moreover, insufficient cooperation between the primary care physician and patient is another important issue determining referrals to specialized care (21).
Collaborative care models are multicomponent interventions based on teamwork in order to redesign care delivery. Increased accessibility to psychological interventions by integrating clinical psychologists into the primary care team reduces medicalization of mild and/or moderate mental pathologies (20, 21).
The care manager is a key figure in collaborative care models. This role is assigned to primary care nurses, who, in close collaboration with primary care physician, are responsible not only for monitoring clinical progress and treatment adherence, but also for providing emotional and self-management support (17, 18, 22). This is a novel approach in our healthcare system, and implies profound changes in the way depression has traditionally been managed. Physicians have to relinquish responsibilities and nurse care managers have to assume new ones. Moreover, an additional challenge lies in establishing smooth and effective coordination among healthcare providers (17, 18). Such programs have demonstrated to be successful in previous experiences (17, 18); however, the approach needs to be bottom-up, involving front-line professionals in both, the development and implementation phases.
In spite of the high evidence of the need to implement these type of integrative programs, it is necessary to identify and to understand the factors and barriers, which make it difficult. Among them, we can mention the knowledge and skills of health care providers, the motivation for the change, the efficacy of health care centers to manage mental health disorders, the budget assigned to the mental health management and the credibility and confidence in the integrative models (23).
On the other hand, mental illness also has a huge economic impact. This impact has been estimated to reach up to 16.3 trillion dollars between 2011 and 2030 worldwide (24). In Spain, depression alone accounts a total cost of 6 billion euros. In particular, 67% of this amount is derived from productivity losses due to premature death and sick leave. It is therefore a major public health concern, but also a significant social and economic challenge (24).
The increase in depression diagnoses has been accompanied by a rise in the prescription of pharmacological treatment. Between 2015 and 2021, there has been an average increase of 15.1 DHD (defined daily doses per 1,000 inhabitants per day) (dayamong OECD countries (25). In Spain, this increase was even more pronounced, reaching up to 19.6 DHD (17). Figure 1 shows the upward trend in the number of DHDs in Spain over the years (26).
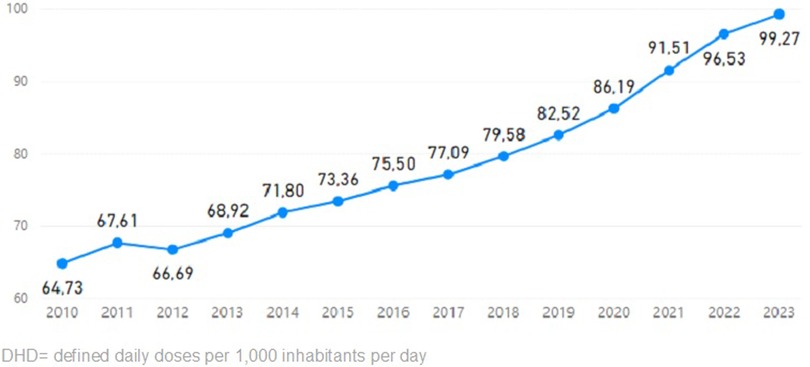
Figure 1. Variation of DHD of antidepressants in Spain over the years. Source: Spanish agency for medicine and health products.
Nevertheless, recent studies suggest that an integrated strategy combining pharmacotherapy with psychological support is more effective than each treatment separately (27). The combined approach shows enhanced efficacy [Risk Ratio (RR) vs. psychotherapy RR = 1.25; 95% CI 1.09–1.43; vs. drugs RR = 1.27; 95% CI 1.12–1.43], compared to psychotherapy or pharmacotherapy individually (26). In fact, when treating depression, apart from pharmacotherapy and psychotherapy, stress management, social and community support, stigma and discrimination, and concomitant comorbidity treatments (28) should also be addressed.
In general, antidepressants, either alone or in a combined approach, should be started at a subtherapeutic dose, in order to assess patient tolerability, and then, gradually increased to a minimally effective dose. Moreover, it is important to highlight that antidepressants can cause side effects such as hyponatremia [OR = 3.160 (95%CI 1.911–5.225)] (29), as well as an increased risk of suicide [OR = 1.66 (1.37–2.02)] (30). Therefore, clinicians should ensure that these drugs are only prescribed to patients with a clear indication. Particular caution should be taken when prescribing antidepressants to patients with an increased underlying risk of seizures (30). In these cases, patients should be referred to mental health professionals.
Mental illness is one of the greatest challenges facing the healthcare system. Given its prevalence, on the rise after the COVID-19 pandemic, this problem is remarkably concerning among adolescents, since one in seven young people aged 10–19 years suffers from some mental disorder (19). Due to the enormous impact on health, and on personal, family, social and economic consequences, depression is a major social health issue that must be addressed by all the society, extending beyond the healthcare sector alone.
As mentioned above, the World Health Organisation (WHO) has long advocated for the integration of mental health services into primary care and community settings to address the large gap in mental health treatment (13). Commissioners and providers of mental health services for people with depression should ensure the effective delivery of treatments. This should build on the key functions of a catchment area-based community mental health service and be provided in the context of a coordinated primary and secondary care mental health service. It is necessary to support the integrated delivery of services across primary and secondary care, to ensure individuals do not fall into gaps in service provision (31, 32).
Integration of mental health services is seen as a feasible strategy to reach a large proportion of the population, reduce mental health stigma and address both mental and physical health outcomes (20).
Multiple studies suggest that integrated primary care-based programs are effective in improving mental health outcomes and quality of life in low- and middle-income countries (21, 33).
Despite their effectiveness, integrated programs have not yet been widely adopted, implemented and scaled up (34). First, there is a need to better understand what core program components and implementation strategies work. Second, the lack of experimental evidence needs to be addressed through pragmatic implementation-effectiveness trials in routine primary care and community settings.
Author contributions
RC-C: Writing – original draft, Writing – review & editing. SV: Writing – original draft, Writing – review & editing. SG: Writing – original draft, Writing – review & editing. IP: Writing – original draft, Writing – review & editing. CB-A: Writing – original draft, Writing – review & editing. EL: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liu J, Liu Y, Ma W, Tong Y, Zheng J. Temporal and spatial trend analysis of all-cause depression burden based on global burden of disease (GBD) 2019 study. Sci Rep. (2024) 14(1):12346. doi: 10.1038/s41598-024-62381-9
2. WHO. (2024). Depressive disorder (depression). Available online at: https://www.who.int/news-room/fact-sheets/detail/depression#:∼:text=Women%20are%20more%20likely%20to,world%20have%20depression%20(1) (Accessed January 15, 2025).
3. Ministerio de Sanidad e Instituto Nacional de Estadística. (2022). Encuesta Europea de Salud en España 2020. Available online at: https://www.sanidad.gob.es/estadEstudios/estadisticas/EncuestaEuropea/EncuestaEuropea2020/EESE2020_inf_evol_princip_result.pdf (Accessed January 15, 2025).
4. Fuster-Casanovas A, Miró-Catalina Q, Vidal-Alaball J, Escalé-Besa A, Carrión C. Ehealth in the management of depressive episodes in Catalonia’s primary care from 2017 to 2022: retrospective observational study. JMIR Ment Health. (2024) 11:e52816. doi: 10.2196/52816
5. Denche-Zamorano Á, Ajenjo-Gomez D, Pereira-Payo D, Galán-Arroyo C, Vega-Muñoz A, Contreras-Barraza N, et al. Physical activity frequency and depression in the Spanish population. Int J Environ Res Public Health. (2022) 19(22):14704. doi: 10.3390/ijerph192214704
6. Trexler JE, Turi E, Poghosyan L. The role of nurse practitioners. JNP. (2023) 19(4):104579. doi: 10.1016/j.nurpra.2023.104579
7. World Mental Health Report. Transforming Mental Health For All. Geneva: World Health Organization (2022).
8. Bains N, Abdijadid S. Major depressive disorder. [Updated 2023 Apr 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing (2024). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK559078/
9. Piao J, Huang Y, Han C, Li Y, Xu Y, Liu Y, et al. Alarming changes in the global burden of mental disorders in children and adolescents from 1990 to 2019: a systematic analysis for the global burden of disease study. Eur Child Adolesc Psychiatry. (2022) 31(11):1827–45. doi: 10.1007/s00787-022-02040-4
10. Wang PS, Aguilar-Gaxiola S, Alonso J, Angermeyer MC, Borges G, Bromet EJ, et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO world mental health surveys. Lancet. (2007) 370(9590):841–50. doi: 10.1016/S0140-6736(07)61414-7
11. Cunningham R, Sarfati D, Peterson D, Stanley J, Collings S. Premature mortality in adults using New Zealand psychiatric services. N Z Med J. (2014) 127(1394):31–41. Available online at: https://pubmed.ncbi.nlm.nih.gov/24929569/24929569
12. NIMH Information Resource Center. Las enfermedades crónicas y la salud mental: Cómo reconocer y tratar la depresión. Available online at: https://www.nimh.nih.gov/health/publications/espanol/las-enfermedades-cronicas-y-la-salud-mental-como-reconocer-y-tratar-la-depresion (Accessed September 17, 2024)
13. Plan de acción integral sobre salud mental 2013-2030 [Comprehensive mental health action plan 2013-2030]. Ginebra: Organización Mundial de la Salud (2022). Licencia: CC BY-NC-SA 3.0 IGO
14. Susser E, Patel V. Psychiatric epidemiology and global mental health: joining forces. Int J Epidemiol. (2014) 43(2):287–93. doi: 10.1093/ije/dyu053
15. Kroenke K, Spitzer RL, Williams JB, Linzer M, Hahn SR, et al. Physical symptoms in primary care. Predictors of psychiatric disorders and functional impairment. Arch Fam Med. (1994) 3:774–9. doi: 10.1001/archfami.3.9.774
16. WHO research suggests. Available online at: https://www.who.int/europe/news/item/23-04-2025-scale-up-mental-health-care-within-primary-health-care–who-research-suggests (Accessed October 20, 2025)
17. García-Herrera Pérez Bryan JM, Nogueras Morillas V, Muñoz Cobos F, Morales Asencio JM. Guía de Práctica Clínica Para el Tratamiento de la Depresión en Atención Primaria. Málaga: Distrito Sanitario Málaga-UGC Salud Mental Hospital Regional Universitario “Carlos Haya” (2011). Available online at: https://consaludmental.org/publicaciones/GPCdepresionatencionprimaria.pdf (Accessed October 1, 2024)
18. Aragonès E, López-Cortacans G, Cardoner N, Tomé-Pires C, Porta-Casteràs D, Palao D, et al. Barriers, facilitators, and proposals for improvement in the implementation of a collaborative care program for depression: a qualitative study of primary care physicians and nurses. BMC Health Serv Res. (2022) 446. doi: 10.1186/s12913-022-07872-z
19. WHO. La salud mental de los adolescents. Available online at: https://www.who.int/es/news-room/fact-sheets/detail/adolescent-mental-health- (Accessed June 30, 2025)
20. Thornicroft G, Ahuja S, Barber S, Chisholm D, Collins PY, Docrat S, et al. Integrated care for people with long-term mental and physical health conditions in low-income and middle-income countries. Lancet Psychiatr. (2019) 6(2):174–86. doi: 10.1016/S2215-0366(18)30298-0
21. An Ginneken N, Chin WY, Lim YC, Ussif A, Singh R, Shahmalak U, et al. Primary-level worker interventions for the care of people living with mental disorders and distress in low- and middle-income countries (review). Cochrane Database Syst Rev. (2021) 8(8). doi: 10.1002/14651858.CD009149.pub3
22. Martín JC, Garriga A, Egea C, Díaz G, Campillo-Cascales MJ, et al. Intervención psicológica escalonada con trastornos mentales comunes en atención Primaria. An Psicol. (2014) 34(1):30–40. doi: 10.6018/analesps.34.1.281491
23. Mukala Mayoyo E, Chenge F, Sow A, Criel B, Michielsen J, et al. Health system facilitators and barriers to the integration of mental health services into primary care in the democratic Republic of the Congo: a multimethod study. BMC Prim Care. (2024) 25:214. doi: 10.1186/s12875-024-02460-y
24. Galán-Arroyo C, Pereira-Payo D, Rojo-Ramos J, Hernández-Mocholí MA, Merellano-Navarro E, Pérez-Gómez J, et al. Increased odds for depression and antidepressant use in the inactive Spanish population. Int J Environ Res Public Health. (2022) 19(5):2829. doi: 10.3390/ijerph19052829
25. OECD Data Explorer. (2024). Pharmaceutical Market. Available online at: https://stats.oecd.org/Index.aspx?DataSetCode=HEALTH_PHMC (Accessed July 3, 2025).
26. Agencia Española de Medicamentos y Productos Sanitarios (2004). Interpretación de datos de consumo. Available online at: https://app.powerbi.com/view?r=eyJrIjoiNWRkYjFmY2MtYjZjNy00N2Y3LWI0MzItODk0NGM4NNmMwIiwidCI6IjJkM2I1MGUwLTZlZjQtNGViYy05MjQ2LTdkMWNiYjc3MDg5YyIsImMiOjh9 (Accessed July 4, 2025).
27. Ng CW, How CH, Ng YP. Managing depression in primary care. Singapore Med J. (2017) 58(8):459–66. doi: 10.11622/smedj.2017080
28. Cuijpers P, Noma H, Karyotaki E, Vinkers CH, Cipriani A, Furukawa TA. A network meta-analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry. (2020) 19(1):92–107. doi: 10.1002/wps.20701
29. Gheysens T, Van Den Eede F, De Picker L. The risk of antidepressant-induced hyponatremia: a meta-analysis of antidepressant classes and compounds. Eur Psychiatry. (2024) 67(1):e20. doi: 10.1192/j.eurpsy.2024.11
30. Yang W, Jia YH, Jiang HY, Li AJ. Antidepressant use and the risk of seizure: a meta-analysis of observational studies. Eur J Clin Pharmacol. (2024) 80(2):175–83. doi: 10.1007/s00228-023-03597-y
31. National Institute for Health and Care Excellence. Depression in adults: treatment and management. NICE guideline, reference number:NG222. Published: 29 June 2022. Available online at: https://www.nice.org.uk/guidance/ng222 (Accessed October 16, 2025).
32. Kennedy SH, Lam RW, McIntyre RS, Tourjman SV, Bhat V, Blier P, et al. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Pharmacological treatments. Can J Psychiatry. (2016) 61(9):540–60. doi: 10.1177/0706743716659417
33. Habtamu K, Birhane R, Demissie M, Fekadu A. Interventions to improve the detection of depression in primary healthcare: systematic review. Syst Rev. (2023) 12(1):25. doi: 10.1186/s13643-023-02177-6
Keywords: primary care, depression, COVID-19 disease, burnout professional, health care economics and organizations
Citation: Cobos-Campos R., Villullas S., García de Andoin S., Pérez I., Bermúdez-Ampudia C. and López de Abechuco E. (2025) Approach to the increase of depression and its treatment. Role of primary care. An opinion article. Front. Health Serv. 5:1715754. doi: 10.3389/frhs.2025.1715754
Received: 29 September 2025; Accepted: 27 October 2025;
Published: 10 November 2025.
Edited by:
Chiachen Cheng, Northern Ontario School of Medicine University, CanadaReviewed by:
Ben Stride-Darnley, NOSM University - Thunder Bay Campus, CanadaCopyright: © 2025 Cobos-Campos, Villullas, García de Andoin, Pérez, Bermúdez-Ampudia and López de Abechuco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: R. Cobos-Campos, cmFxdWVsLmNvYm9zY2FtcG9zQGJpby1hcmFiYS5ldXM=