
 Andres M. Salazar2
Andres M. Salazar2
- 1 Vietnam Head Injury Study, Henry M. Jackson Foundation, National Naval Medical Center, Bethesda, MD, USA
- 2 Cognitive Neuroscience Section, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, MD, USA
- 3 Department of Radiology, Johns Hopkins University, Baltimore, MD, USA
- 4 Traumatic Brain Injury Research Laboratory, Kessler Foundation, West Orange, NJ, USA
The study of those who have sustained traumatic brain injuries (TBI) during military conflicts has greatly facilitated research in the fields of neuropsychology, neurosurgery, psychiatry, neurology, and neuroimaging. The Vietnam Head Injury Study (VHIS) is a prospective, long-term follow-up study of a cohort of 1,221 Vietnam veterans with mostly penetrating brain injuries, which has stretched over more than 40 years. The scope of this study, both in terms of the types of injury and fields of examination, has been extremely broad. It has been instrumental in extending the field of TBI research and in exposing pressing medical and social issues that affect those who suffer such injuries. This review summarizes the history of conflict-related TBI research and the VHIS to date, as well as the vast range of important findings the VHIS has established.
The Recent History of Combat-Related TBI Research
Traumatic brain injury (TBI) is the principal cause of death and disability in those under 35 in the USA. Each year TBI leads to approximately 55,000 deaths, as well as 50,000 cases of associated physical, cognitive, behavioral, and social deficits (Kraus and McArthur, 1996). TBI remains extremely prevalent in combat situations, with nearly two-thirds of injured US soldiers sent from Iraq to Walter Reed Army Medical Center sustaining TBI (Warden, 2006). As recently as 2009, it was quoted that “Head injury has always been, and remains, an unpopular subject with British neurologists, presumably because they tend to see it as a surgical rather than a medical disorder.” (van Gijn, 2009). Fortunately this has not been the case for all neurologists. Much of what is known about TBI (e.g., the clinical course, cognitive changes, incidence of post-traumatic epilepsy, PTE) is in fact as a result of neurological studies in military populations. The First World War was the first conflict that led to a major move forward in the study of TBI because of the sheer quantity of casualties, the extent of trench warfare (and so vulnerability to head injuries), the unprecedented use of artillery, and a change to small, low velocity ammunition, which tended to create focal injuries. In addition, advances in the field of neurosurgery meant penetrating head wounds were no longer inevitably fatal. Gordon Holmes, a London neurologist described several groups of First World War veterans, including 23 cases of occipital lesions (Lepore, 1994). This led to what became the standard illustration of the cortical map of the retina (Holmes and Lister, 1916). Henry Head, another English neurologist, had conducted pioneering work into the somatosensory system prior to the First World War, and he expanded this work with George Riddoch by testing reflex activities of isolated portions of the spine subjected to gunshot wounds (Holmes, 1941). Across the channel, brain injury rehabilitation units in Frankfurt and Cologne were responsible for major innovations in neuropsychological assessments and rehabilitation techniques (Boake and Diller, 2005).
During the Second World War, the Russian psychologist Aleksandr Luria examined psychological dysfunctions in patients with brain lesions, and his work gave impetus to the emerging field of neuropsychology. Luria’s early work with Zazetsky (Luria, 1972), an ex-soldier who tried to make sense of his “shattered world” predated interest by others in the personal experience of those with TBI. Hans-Lukas Teuber and Morris Bender focused on visual deficits (Bender and Teuber, 1948) and long-term outcome from TBI (Teuber, 1975). Teuber was the first to report on the role of preinjury intelligence in cognition post-TBI (Weinstein and Teuber, 1957), and he also introduced was that of double dissociation of function, which has since become essential to functional localization (Lackner, 2009). Suzanne Corkin started assessing Second World War veterans while working for Teuber. She subsequently commented on the long-term prognosis of TBI, and developed the concept of exacerbated decline in intelligence post-TBI (Corkin et al., 1984, 1989). Her work with conflict-associated TBI was continued by Newcombe and Marshall in Second World War veterans, and later, in Korean War veterans. They focused on language difficulties post-TBI (Newcombe et al., 1971), long-term outcome, and rehabilitation (Newcombe et al., 1980). Their research helped develop a new classification for acquired alexias and lead to the conceptualization of the dual routes of visual processing that Ungerleiter and Mishkin later formalized in their theory (Mishkin, 1972). The neuropsychiatrist, Lishman (1992), was another early proponent of TBI research, and was amongst the first who examined social behavior changes following TBI.
History of the Vietnam Head Injury Study
Set Up and Phase 1
The Vietnam Head Injury Study (VHIS) was set up by William F. Caveness, a neurologist and retired Naval Reserve captain who had served in the Korean War, who was chief of the Laboratory of Experimental Neurology at the National Institute of Neurological and Communicative Disorders and Stroke from 1965. He designed the VHIS registry, which gathered information on 1,221 Vietnam veterans who sustained a TBI between 1967 and 1970 (Caveness et al., 1979). Of the 58,000 US combat fatalities in the Vietnam War, about 40% were due to head and neck wounds. The Vietnam conflict was the first that involved large scale helicopter evacuations and early treatment by neurosurgical teams close to the battlefield, so that most patients received definitive treatment with hours of their injuries, allowing a much higher rate of survival than in previous conflicts (Carey et al., 1982; Rish et al., 1983). In addition, the low velocity penetrating fragment wounds typically sustained resulted in relatively focal defects, and so these subjects provided a particularly large and informative group for study. It should be noted, therefore, that the data from this cohort addresses issues predominantly affecting those with penetrating TBI. This may contrast with closed injuries, which are considerably commoner in the civilian population and especially in mild cases lack some of the frequent, significant sequelae of penetrating TBI, such as impaired consciousness. Caveness requested that field neurosurgeons complete registry forms on those they anticipated would survive, detailing wound characteristics and neurological status immediately post-injury. Although he received around 2,000 registry forms, addresses could only be found for 1,221. Phase 1 (PH1) of the VHIS was a retrospective review of those subjects’ military and veterans affairs (VA) medical records from the 5-years post-injury (e.g., Caveness et al., 1979; Weiss et al., 1983, 1986). Patients were excluded if they had a spinal cord injury or if insufficient medical records were available. Caveness set up the VHIS to primarily study the causes of PTE but unfortunately died before the beginning of Phase 2 (PH2; e.g., Caveness et al., 1979; Rish et al., 1979, 1980, 1981; Mohr et al., 1980). The team of investigators that inherited the VHIS subsequently expanded the scope of the study well beyond his original focus.
Phase 2 – 15 Years on
Phase 2 evaluated 520 head-injured subjects from the original registry who responded to mailings, as well as 85 uninjured Vietnam veteran control subjects, matched by age. Of those who did not come to PH2, some had died, some declined, and some did not respond; 92% had penetrating head injuries (e.g., Grafman et al., 1986a, 1988, 1992; Salazar et al., 1987). Analysis of subjects who did and did not participate in PH2 showed no significant differences in terms of demographics or lesion type (Jonas et al., 1987). Subjects attended Walter Reed Army Medical Center, Washington, DC, USA for a 1-week evaluation, which consisted of neuropsychological, neurological, language, and brain imaging assessments. Specific subgroups and individual patients have returned more often for selected studies between each phase following PH2.
Phase 3 – 35 Years Post-TBI
Of the 520 head-injured subjects assessed at PH2, 484 were still alive, and 182 attended Phase 3 (PH3). Additionally, 17 head-injured subjects identified in PH1 that did not attend PH2 were assessed. Of the original 80 control subjects recruited in PH2, 32 attended and a further 23 were recruited. Subjects were assessed at the National Naval Medical Center, Bethesda, MD, USA, with a broad battery of neuropsychological, neurological, psychiatric, and imaging assessments. Brain lesions were identified by CT scan, and the data were reconstructed with a 3-mm overlapping slice thickness and a 1-mm interval. MRI scans were not used as a large number of the subjects had retained metal in their brains. Lesions were processed using “analysis of brain lesions” software (ABLe; Makale et al., 2002; Solomon et al., 2007). Within ABLe, the lesions were drawn manually in native space on each 1 mm thick slice by Vanessa Raymont (a psychiatrist with clinical experience of reading CT scans), and reviewed by Jordan Grafman, enabling a consensus decision to be reached regarding the limits of each lesion. Normalized lesion volume was calculated, and the percentage of brain lobes and regions involved determined. This methodology is explained further in our earlier paper (Raymont et al., 2008). However, this meant that the assessment of these lesions was to some extent dependent on subjective measurements.
Phase 4 – 40+ Years Later
Subjects from PH3 were invited to attend for Phase 4 (PH4) of the VHIS, approximately 40–45 years post-injury. PH4 is currently in progress at the National Institute of Neurological Disorders and Stroke in Bethesda, MD, USA, and contains a core set of tasks that are similar to those previously administered in PH2 and PH3, so longitudinal assessments can be completed. In addition, further molecular genetic studies are planned that examine the role of genetic polymorphisms in recovery of function from TBI and in predicting various kinds of outcomes. Experimental cognitive neuroscience studies in PH4 will expand upon previous work in social neuroscience, examining the brain areas associated with certain forms of economic decision-making, human belief systems and moral thinking, social status, and aggression. In addition, PH4 will examine the role of caregiver personality in outcome after combat-related TBI. We hope that these studies contribute to the emerging fields of social neuroscience and behavioral genetics, and lead to improved management and outcome of the patient with a TBI. Although there was no evidence of Alzheimer’s disease (AD) in this cohort at PH3, given the evidence of links between AD and TBI (Lindsay et al., 2002), Ann McKee, a neuropathologist from Boston University has also agreed to conduct autopsies on the brains of all VHIS subjects who consent. This will provide yet another dimension to the study by examining the causes and effects of long-term pathological changes following TBI, including the development of abnormal Tau deposits.
The advantages of studying this population have included their uniformity of age, gender, and education at time of injury, as well as the availability of preinjury intelligence data, making this a unique population for longitudinal assessment.
Selected Findings from the VHIS
One great advantage of the VHIS is that it has allowed the collection of a vast amount of data from a large cohort, which can subsequently be used to help answer basic neuropsychological questions (e.g., Rueckert and Grafman, 1996, 1998; Dimitrov et al., 1999; Lee et al., 1999). Over 80 papers have been published using VHIS data to date, and many more are expected. Here we describe some selected findings from each phase in order to give the reader a sense of the breadth and depth of our findings.
Neurosurgical Findings
A number of clinical questions regarding acute neurosurgical management were addressed at PH1, and are reviewed elsewhere (Grafman and Salazar, 1999). These include the use of improved protocols for evacuation and triage of large numbers of casualties, aggressive procedures for definitive surgical debridement close to the front, the issues of dural closure, retained metal and bone fragments, incidence and management of brain abscesses, use of antibiotics and anticonvulsants, and the timing of cranioplasty, among others. For example, it was reported that 491 cranioplasties were performed in 1,030 subjects from the registry, with a morbidity rate of 5.5% and a mortality rate was 0.2%, largely associated with surgical outcome (Rish et al., 1979). From these findings it was suggested that cranioplasty after penetrating TBI should be deferred for a minimum of 1 year, to control morbidity. Skull defects or cranioplasty were not found to predict tendency to post-traumatic seizures. In summary, the neurosurgical experience of the Vietnam War marked a turning point in the approach to emergency evacuation and management of severe TBI.
Research at PH2 further investigated the associations of traumatic unconsciousness post-TBI. Surprisingly, only 15% of the 342 subjects who survived severe penetrating TBI had prolonged loss of consciousness. Over half had no or only momentary unconsciousness after injury, and some even remained in battle and received citations for bravery. Over 40% had good recollection of injury events and were also alert at first examination, sometimes in spite of large lesions, further illustrating the largely focal nature of these wounds. The areas most associated with traumatic unconsciousness post-TBI in this cohort included the posterior limb of the left internal capsule, left basal forebrain, midbrain, and hypothalamus (Salazar et al., 1986).
Epilepsy
Previous studies of World War Two (Walker and Jablon, 1961) and Korean War veterans (Weiss and Caveness, 1972) had confirmed the association between post-traumatic seizures and penetrating TBI. At PH2, of the 421 veterans who had sustained a TBI, 53% had a history of PTE, which had started within a year of TBI in the majority of cases (Salazar et al., 1985). About one-half of the group were still experiencing seizures 15 years after injury. The relative risk of developing PTE dropped from about 580 times higher than the general age-matched population in the first year, to 25 times higher after 10 years, and the frequency of seizures in the first year predicted subsequent severity of seizures. Anticonvulsant therapy with phenytoin in the first year after injury did not prevent later seizures. Patients with focal neurological signs or large lesions had an increased risk of developing PTE. PTE was also associated with the presence of hematoma or retained metal fragments (Weiss et al., 1986). Only five affected brain areas significantly predicted seizure occurrence: right vertex gray matter, left convexity cortex, left temporal gray matter, right frontal white matter, and right corona radiate. Lesions in the left hippocampus correlated with increased seizure frequency, whereas insula and splenium lesions correlated with lower seizure frequency. Lesions of the posterior callosum and caudate nucleus were associated with less persistent seizures. From these data, the authors were able to develop a predictive formula (incorporating data from previous, shorter term studies of risk factors for seizures, all of which suggested that the time between injury and onset of PTE is independent of injury characteristics) for the time between injury and first seizure (Figure 1).
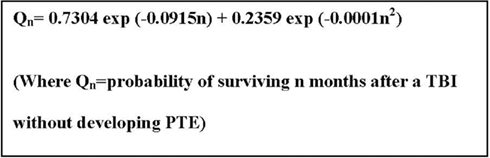
Figure 1. Predictive formula for the risk of developing PTE.
At PH3, the prevalence of seizures in the 199 TBI veterans who attended was 43.7%, similar to that 20 years earlier (Raymont et al., 2010). Remarkably 12.6% reported initial onset of PTE more than 14 years post-injury. These subjects were not different from earlier onset PTE subjects in any of the clinical measures examined. Within this cohort, the most common seizure type last experienced was complex partial seizures (31.0%), with increasing frequency post-injury. Eighty-eight percentage of subjects with PTE were receiving anticonvulsants. Left parietal lobe lesions and retained ferric metal fragments were associated with PTE and total brain volume loss predicted seizure frequency, although it should be emphasized that there is not substantial evidence in the general literature for lesion location being predictive of PTE.
Motor Disorders
Motor impairments following TBI are a common problem, which are very limiting to patient functioning. Within the first few months following a unilateral brain lesion affecting the motor cortex, therapeutic efforts are aimed primarily at the restoration of motor function on the hemiplegic side. Following on from the localization work conducted at the time of World War One, research carried out at PH1 reported that parietal wounds were particularly associated with hemiparesis, and that regardless of the features of the hemiparesis initially, the severity of the final syndrome was greatest in the hand and arm and least in the face (Mohr et al., 1980). At PH2, 90 subjects were found to have hemiparesis (Schwab et al., 1993), and in 32% of these subjects this prevented them from working. The relationship of preinjury left-hand dominance to post-injury distal motor skills was examined at PH2 (Grafman et al., 1985a). No persistent deficits were seen on distal motor tasks in left-handed adults who suffered a penetrating TBI, compatible with the previously reported relative sparing of persistent neuropsychological deficits in left-handed subjects following brain damage. In addition, other results indicated similar long-term functional outcome in right and left hemisphere-damaged subjects, despite more severe contralateral functional motor deficits following lesions of the left hemisphere. These results demonstrated that unilateral TBI involving the motor areas of either hemisphere has detrimental effects on ipsilateral upper extremity motor function, suggesting that the left hemisphere has greater neuronal representation for bilateral motor processes (Smutok et al., 1989).
Fatigue
Fatigue is a common and disabling symptom following TBI, and studies have suggested that the ventromedial prefrontal cortex (vmPFC) could play a significant role in fatigue pathophysiology. At PH3 it was found that individuals with vmPFC lesions were significantly more fatigued than individuals with dorsolateral prefrontal cortex (dlPFC) lesions, individuals with non-frontal lesions, or healthy controls (Pardini et al., 2010). The larger the lesion volume, the higher the fatigue score. This demonstrated that the vmPFC plays a critical role in penetrating brain injury-related fatigue, and possibly provides a rationale to link fatigue to different vmPFC functions, such as effort and reward perception. In contrast, also at PH3, insomnia was found to be associated with left dorsomedial PFC lesions, presumably due to a disruption of the brain systems sustaining the sleep control mechanisms that are associated with brain stem and other midline structures (Koenigs et al., 2010).
Neuropsychological Associations
One vital issue that was examined at PH2 was the link between preinjury intelligence (as measured by the Armed Forces Qualification Test, AFQT-7A, 1960; DoD) and lesion characteristics, as well as preservation of cognitive function long-term post-TBI. Grafman et al. (1986a, 1988) reported that post-injury overall intelligence was most predicted by preinjury intelligence, followed by size of lesion, with some controls and a few TBI subjects showing an increase in AFQT score from preinjury to PH2 (Figure 2), probably secondary to maturation of the educational abilities tested in the AFQT. Lesion location was least important in predicting overall intelligence 15 years post-injury. For subtest scores of intelligence, lesion location assumed much greater predictive value. Specifically, left temporal and occipital lesions impaired performance on subtests assessing vocabulary and object-function matching ability.
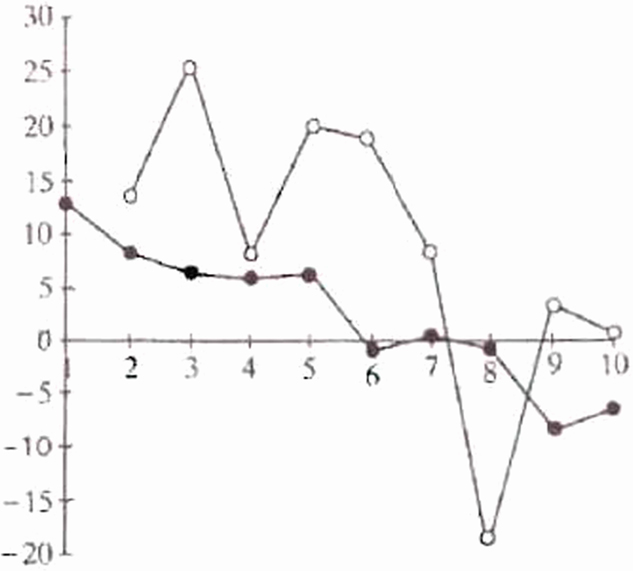
Figure 2. Pre- and PH2 Armed Forces Qualification Test (AFQT) scores in head injured subject (filled circles, r = −0.32) and controls (open circles, r = −0.44). Plot of pre- to PH2 AFQT differences (D-AFQT) by preinjury AFQT deciles.
Both cognitive change and return to work at PH2 were significantly related to total brain volume loss, third ventricle width, and septum caudate distance (Groswasser et al., 2002), with volume loss and third ventricle width being the most predictive. This suggests that quantity of brain disruption post-TBI influences long-term recovery of day-to-day functioning.
The same issues were revisited at PH3, via examination of past and current performance on the AFQT and current performance on the Wechsler Adult Intelligence Scale (WAIS-III). Raymont et al. (2008) reported that those with TBI showed a greater degree of overall cognitive decline overall during the years following injury compared with controls, which became increasingly significant later in life. Preinjury intelligence was the most consistent predictor of cognitive outcome and while laterality of lesion was not a factor, there were some predictable associations between atrophy and specific regions of tissue loss and long-term cognitive functioning (see Figure 3, which represents the change in intelligence seen in subjects with TBI only).
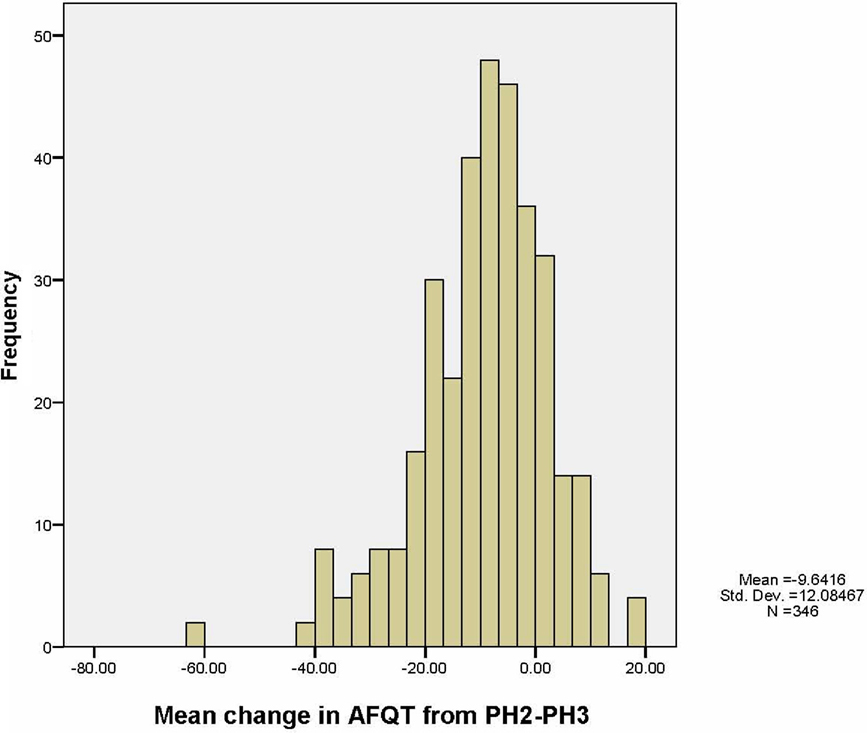
Figure 3. Mean change in AFQT scores from Phase 2 to Phase 3 in subjects with TBI.
The VHIS has thus produced some important contributions in terms of theories of neuroplasticity following TBI (Romero et al., 2002). Recent research has emphasized that this takes place via both local restitution, as well as reorganization and compensatory reassignment; processes which may vary at different points in the lifespan. The VHIS has been important in terms of highlighting how these changes may alter with aging, and how they may be impacted by a variety of factors, such as genetic make up (Raymont and Grafman, 2006).
Phase 2 included a review of the long-term outcome of post-TBI aphasia. At PH2, it was reported that aphasia occurred in 244 of the 1,030 patients with TBI, correlating with cause of injury and initial loss of consciousness. The aphasia disappeared within 10 years in 34% of cases. Sensorimotor aphasia usually changed to motor aphasia; motor aphasia disappeared; and sensory aphasia persisted. These improvements continued years after any accompanying hemiparesis stabilized, and were not related to wound site, depth, or whether the wound was caused by gunshot or fragment (Mohr et al., 1980). Chronic non-fluent aphasics demonstrated syntactic processing deficits in all language modalities, with greater posterior extension of their lesions in Wernicke’s area, with some involvement of the underlying white matter and basal ganglia in the left hemisphere (Ludlow et al., 1986). This paper also highlighted that that deeper lesions involving the white matter may be the key factor associated with lack of recovery and persistence of language deficits. One PH2 case study also reflected on the localization of calculation knowledge (Grafman et al., 1989). Despite an almost totally destroyed left hemisphere and a severe linguistic disorder, the subject retained the ability to read and write single and two-place digits, perform simple addition and subtraction, accurately judge magnitudes and quantities, and recognize arithmetic operational symbols. This supported the hypothesis of right hemisphere participation in selected aspects of number processing.
Besides more descriptive findings, detailed experiments on the functions of suppression of context-inappropriate meanings during lexical ambiguity resolution were conducted in PH3. Those with prefrontal lesions were found to have significantly lower accuracy rates for context-inappropriate conditions, suggesting a loss of the control aspects of inhibitory processes in lexical ambiguity resolution following prefrontal cortex damage (Frattali et al., 2007).
Memory Disorders
At PH2, deficits in semantic memory, verbal episodic memory, and visual episodic memory were found to be associated with lesion location, in a manner roughly consistent with the existing neuropsychological literature (Salazar et al., 1986). The advantage of being able to examine isolated brain lesions was vital in enabling the VHIS to identify possible site-specific sources of memory impairment. One case study demonstrated that the fornix cerebri has a role in the maintenance of information accessibility to both encoding and recall during post-working memory processing, as well as in the organization of verbal information (Grafman et al., 1985b). Another explored the basis of facial recognition memory, finding that impairment on tests of face memory was most associated with bilateral lesions and with unilateral lesions of the temporal lobe (Grafman et al., 1986b).
Schooler et al. (2008) used a specific modeling technique; mixture modeling (Muthén and Muthén, 1998–2004), to classify VHIS lesion groups and explore associations with subtypes of memory performance. One striking finding was that marked short term memory deficits were found in all classes of individuals with TBI, regardless of lesion location, and any concomitant effects of depressive symptomatology and substance dependence.
Theories of posterior parietal lobe involvement in memory have evolved over the years. However, definitive neuropsychological evidence supporting the superior parietal lobe’s purported role in working memory has been lacking. At PH3, subjects with superior parietal lesions were compared to those with no damage in this region and with control subjects with no history of TBI. Superior parietal damage was associated with deficits on tests involving the manipulation and rearrangement of information in working memory, but not on working memory tests requiring only rehearsal and retrieval processes, nor on tests of long-term memory. These results indicated that the superior parietal cortex is critically important for the manipulation of information in working memory (Koenigs et al., 2009a).
Reasoning, Decision-Making, Mood, and Social Behavioral Planning
The large number of subjects with circumscribed frontal lobe lesions in the VHIS enabled both PH2 and PH3 to investigate altered performance on standardized tests of higher cognition. One study of patients with lesions in the prefrontal cortex utilizing the Tower of Hanoi task (Goel and Grafman, 1995) suggested that both subjects with frontal lesions and controls use the same general strategy to solve problems, and that patients’ difficulties have little to do with planning deficits (as is generally assumed in the neuropsychology literature). Patient performance was rather explained in terms of an inability to see or resolve a goal–subgoal conflict, which is compatible with several other accounts of frontal lobe dysfunction. In a study of subjects with frontal lobe damage, their performance on the Tower of London task suggested impairment in execution-related processes (Carlin et al., 2000). Such analyses of data collected as part of the VHIS led to further conclusions on the regional contribution of planning and representations, which ultimately lead to novel theories of how the brain represents knowledge and responds to complex events (Goel and Grafman, 2000; Goel et al., 2001; Rattermann et al., 2001; Wood and Grafman, 2003; Wood et al., 2003).
Reasoning
While the role of left prefrontal cortex in reasoning tasks has long been recognized, the role of right prefrontal cortex remains unclear. One study undertaken at PH2 (Goel et al., 2007) found that the right prefrontal cortex plays an essential role in resolving indeterminate relations with no belief-bias cues, a fact that was later confirmed by a fMRI study in healthy control subjects (Goel et al., 2009). In addition, studies of decision-making and social behavior at PH2 provided new insight into these deficits, and helped define appropriate modes of assessing such difficulties in subjects with frontal lesions.
Many VHIS subjects had been previously dishonorably discharged from the military, when personality changes seen after frontal lobe injuries were less recognized. Thus, the VHIS was vital in establishing improvements in the assessment of those with frontal lobe syndrome. It was found that there may be subgroups of patients with specific social deficits even within groups whose lesion encompasses a larger region, e.g., vmPFC lesions (Sanfey et al., 2003; Goel et al., 2004; Mah et al., 2004, 2005). Administration of the Everyday Problem Solving Inventory (EPSI) suggested that some patients with prefrontal lobe lesions may have impaired social judgment that can be directly revealed only through the use of such relatively novel neuropsychological tests (Dimitrov et al., 1996).
Mood disorders
As well as examining the impact of TBI on executive functioning, the VHIS reported on effects in terms of mood and other psychological disorders. At PH2, subjects with TBI were compared with controls in terms of anxiety and aggressive symptoms, to explore the hypotheses regarding the regulation of anxiety by frontal cortical mechanisms (Grafman et al., 1986c). Results indicated that patients with right orbitofrontal lesions were prone to abnormally increased anxiety and depressive symptoms, whereas patients with left dorsofrontal lesions were prone to abnormally increased anger and hostility. These data suggested that mood symptoms are subject to influence by locality of brain damage. These theories were expanded during PH3, when the correlates of depressive disorder were studied in greater detail, in particular whether damage to either the vmPFC or dlPFC is related to the pathogenesis of depression. Bilateral vmPFC lesions were associated with low levels of depression, whereas bilateral dorsal PFC lesions (involving dorsomedial and dorsolateral areas in both hemispheres) were associated with substantially higher levels of depression. These findings suggested both the vmPFC and dorsal PFC are critical to depression, with vmPFC damage offering some resistance to depression, and dorsal PFC damage conferring vulnerability (Koenigs et al., 2008).
Post-traumatic stress disorder (PTSD) was specifically assessed at PH3, in particular the causal contribution of specific brain areas to PTSD symptoms. There was a substantially reduced occurrence of PTSD among those individuals with damage to one of two regions of the brain: the vmPFC and an anterior temporal area (that included the amygdala; Figure 4). The decreased prevalence of PTSD following vmPFC or amygdala damage appeared to be related to an overall reduction of symptom intensity or number, rather than a complete abolishment of all symptoms, suggesting that treatments aimed at selectively inhibiting vmPFC and/or amygdala function could be used to treat PTSD (Koenigs et al., 2009b).
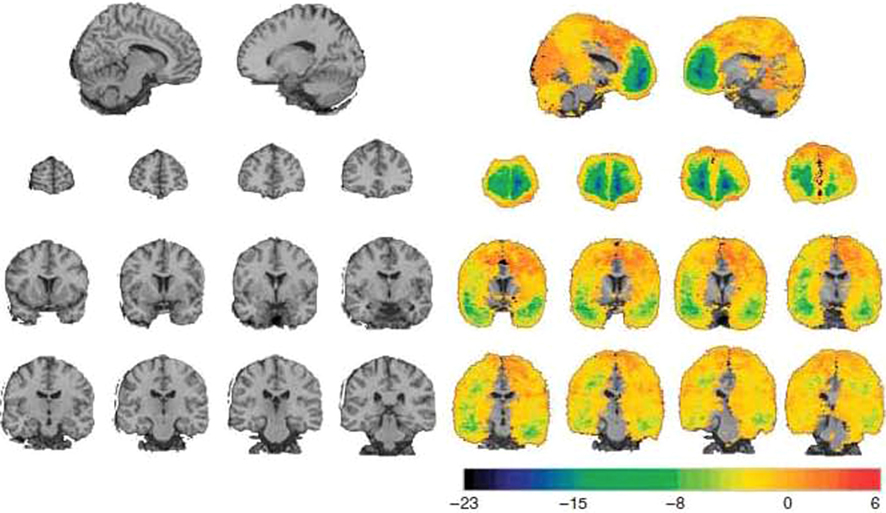
Figure 4. Lesion difference analysis. A healthy adult brain is shown on the left. The lesion difference analysis for the corresponding slices is shown on the right. The color of each voxel indicates the difference between the number of veterans with damage to that voxel that developed PTSD and did not develop PTSD. The colors blue and green indicate the most negative values – areas where damage was relatively infrequently associated with PTSD. Top row, sagittal views of negative value clusters in prefrontal cortex. The left hemisphere (x = −10) is on the left and the right hemisphere (x = 16) is on the right. Second row, coronal views of negative value clusters in bilateral prefrontal cortex. Slices are arranged with the anterior most slice on the left (y = 66, y = 56, y = 36, respectively). In each coronal slice, the right hemisphere is on the reader’s left (radiological convention). Third row, coronal views of negative value clusters in bilateral anterior temporal lobe (y = 14, y = 8, y = 2, y = −4, respectively). Fourth row, coronal views of posterior temporal lobe (y = −10, y = −16, y = −22, y = −28, respectively).
Personality
Phase 2 investigators sought to establish more concrete evidence for the postulated associations between interictal personality traits and complex partial epilepsy (Swanson et al., 1995). An association between interictal psychopathology and complex partial, partial generalized, and generalized seizures was found, but there were no significant between group differences.
Social cognition
In 1999, PH2 reported a single VHIS case very similar to the famous nineteenth-century patient Phineas Gage (Dimitrov et al., 1999). Phineas Gage’s case was described by his physician (Harlow, 1848, 1868), after he sustained a discrete but severe prefrontal cortex lesion during a railroad accident. Not only did Gage regain full consciousness and survive the incident, but he also demonstrated intact speech, learning, memory, and intelligence. However, his personality was profoundly changed, and he lost his “sense of responsibility” and respect for social conventions (Dimitrov et al., 1999). The subject described at PH2 was a 50-year-old male patient with a right frontal ventromedial lesion who showed preserved general cognitive, abstract thinking, and problem-solving abilities, in contrast to gross impairment in his social competence, social decision-making, and social conduct. He also demonstrated diminished sensitivity to socially relevant stimuli and situational nuances, impairment in sexual behavior, lost sense of responsibility, and disinhibition. This was cited as evidence for the regulation of emotion and social conduct by the vmPFC.
It is well reported that those with frontal lobe lesions may present with aggressive behavior. At PH2 family observations and self-reports were collected using scales and questionnaires that assessed a range of aggressive attitudes and behavior (Grafman et al., 1996). Patients with vmPFC lesions consistently demonstrated aggression scores significantly higher than controls and patients with lesions in other brain areas. However, the presence of aggressive and violent behavior was not associated with lesion size or history of seizures. The genotyping that was carried out as part of PH3 demonstrated an association between prefrontal cortex lesions and MAO-A in modulating aggression (Pardini et al., in press).
Results from a wealth of imaging and lesion studies have highlighted the involvement of the PFC in social cognition. Accumulating evidence demonstrates that representations within the lateral PFC enable people to coordinate their thoughts and actions with their intentions to support goal-directed social behavior. Despite the importance of this region in guiding social interactions, remarkably little is known about the functional organization and forms of social inference processed by the lateral PFC. Evidence from PH2 introduced a framework for understanding the inferential architecture of the PFC; “structured event complex theory” (Barbey et al., 2009). Data from both PH2 and PH3 have subsequently added to the evidence that regions of the PFC that are critical for both implicit and explicit social cognitive, as well as moral judgment processing. It seems there is considerable overlap between regions utilized when individuals engage in social cognition or assess moral appropriateness of behaviors, underscoring the similarity between social cognitive and moral judgment processes. The structured event complex theory emphasizes the dynamic flexibility in neural circuits involved in both implicit and explicit processing, and the likelihood that neural regions thought to uniquely underlie both processes in fact heavily interact (Forbes and Grafman, 2010).
Emotional intelligence (EI) has been referred to a set of competencies that are essential features of human social behavior (Krueger et al., 2009). At PH3 two components of this were assessed; (1) Strategic EI – the competency to understand emotional information and to apply it to management of yourself and others and, (2) Experiential EI – the competency to perceive emotional information and to integrate it into thinking. It was found that vmPFC damage diminishes strategic EI and dlPFC damage diminished experiential EI in subjects with frontal lobe damage.
An aspect of normal social cognition development is the development of stereotypical attitudes. At PH2, subjects with PFC lesions and controls were administered the Implicit Association Task (IAT) that measured the degree of association between male and female names and their stereotypical attributes of strength and weakness. Patients with dlPFC lesions and controls showed a strong association, whereas patients with vmPFC lesions had a significantly lower association, between the stereotypical attributes of men and women and their concepts of gender. This finding provided support for the hypothesis that patients with vmPFC lesions have a deficit in automatically accessing certain aspects of overlearned associated social knowledge (Milne and Grafman, 2001). At PH3, clinical observations of patients with ventral frontal and anterior temporal lesions revealed marked abnormalities in social attitudes. Gozzi et al. (2009) used the IAT to determine the differential effects of the vmPFC, ventrolateral prefrontal (vlPFC), and superior anterior temporal lobe (aTL) cortical lesions on attitudes. It was found that larger lesions in either the vmPFC or the superior aTL were associated with increased stereotypical attitudes, whereas larger lesions in the vlPFC were associated with decreased stereotypical attitudes.
Functional Outcome
In PH2, the relationship between neurological, neuropsychological, and social interaction impairments to work status was examined (e.g., Schwab et al., 1993; Salazar et al., 1995). Only 56% of the subjects with TBI were working at PH2, compared to 82% of the uninjured controls. Seven impairments correlated with work status; PTE, paresis, visual field loss, verbal memory loss, visual memory loss, psychological problems, and violent behavior. These disabilities had a cumulative and surprisingly equipotent affect upon the likelihood of work, suggesting that patients find it harder to compensate for increasing amounts of disabilities, whatever the disability. The authors suggested that a simple summed score of the number of these seven disabilities can yield a residual “disability score” which may prove to be a practical tool for assessing the likelihood of return to work post-TBI (Figures 5 and 6).
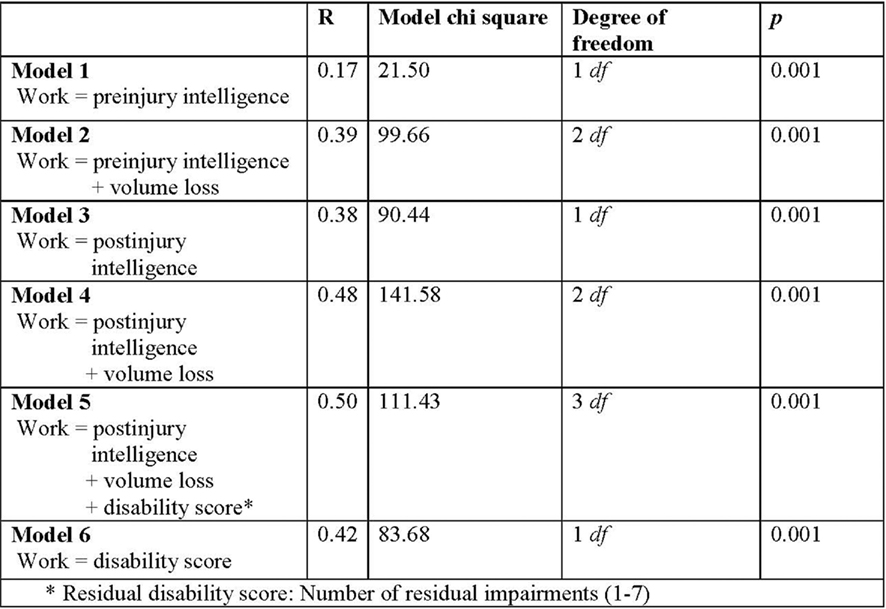
Figure 5. Logistic regression analysis outcomes for predictive factors of variation in work status.
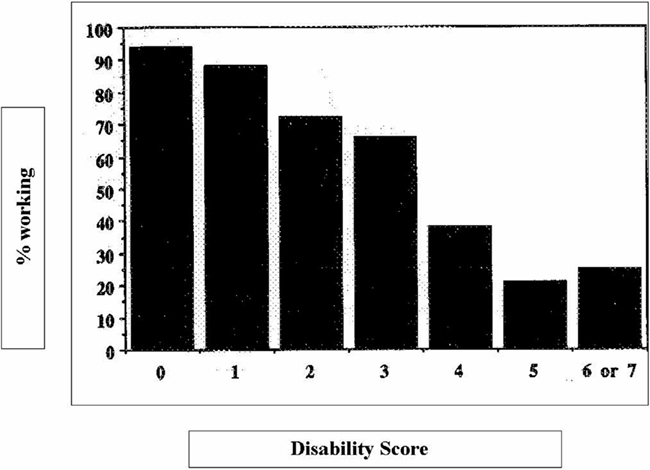
Figure 6. Vietnam Head Injury Study, percent working by disability score. The disability score represents the number of disabilities present (1–7).
Additionally, 82% had used VA educational benefits to return to school (Kraft et al., 1993), and 64% had achieved associate or bachelor’s degrees. Return to work was strongly related to level of educational achievement, particularly among the most severely disabled. Though only 56% of the TBI group were employed at PH2, the occupational distribution of those who were working differed little from uninjured controls, or the male labor force (Kraft et al., 1993). Thus severity of injury appears to affect educational achievement and return to work, but not the occupational distribution of those who do manage to return, implying some level of plasticity may occur which can overcome loss or brain tissue, but may still be restrained by other psychological or social factors.
Genetics
It has been established that that recovery of function after brain damage results from complex interactions between both environmental effects and genetic factors (Lindsay et al., 2002). In recent years, there has also been increasing evidence of links of between-specific genotypes and risk for accelerated cognitive decline or dementia following TBI. Any associations found between genetic information and outcome following TBI may also aid the acute triage of brain-injured patients as well as help to target future treatments.
One of the major advances at PH3 was the assessment of a large number of the genetic markers and their relation to various outcome measures. Raymont et al. (2008) reported the links with cognition. All subjects were both healthy and physically fit before their injury, yet preinjury intelligence was found to be significantly predicted by the following genotypes; GRIN2C rs689730, GAD2 rs2839670, and DBH444. It was suggested that the presence of all of these markers could account for 15.5% of the variability in preinjury intelligence. However, only GRIN2A rs968301 was found to be able to predict current intelligence and change in intelligence from preinjury to PH3. Experimental animal studies have revealed impaired plasticity following TBI, even in the absence of significant anatomical damage (Giza et al., 2006), evidenced by examining N-methyl-D-aspartate (NMDA). NMDA consists of a number of subunits, including the GRIN glutamate receptor, which seems to be specifically involved in the pathophysiology of CHI, including acting as a marker of neuronal death (Parton et al., 2005). There was a trend for dominant homozygotes to have a greater level of decline in intelligence from PH2 to PH3.
Neurotrophins such as brain-derived neurotrophic factor (BDNF) have an impact on neuronal function and synaptic plasticity in the brain (Varon et al., 1991). Recent evidence has shown functional differences between the proteins coded for by the val66 and met66 BDNF alleles in healthy subjects and patients with neurological or psychiatric disorders (Krueger et al., 2011). PH3 reported a functional relationship between the BDNF val66met genotype and recovery of executive function in subjects with frontal lobe lesions. Individuals carrying one or two copies of the BDNF met allele performed significantly better on cognitive tests measuring executive functions of the frontal cortex compared with individuals carrying the val/val homozygotes, suggesting that the val66met BDNF polymorphism may act differently in the injured and healthy brain.
Overall Significance and Consequences of the VHIS
The US military population offers a number of advantages for the study of the effects of TBI; its size, relative uniformity, the fact that all subjects are initially healthy, and the potential for long-term follow-up. Additionally, preinjury intelligence and aptitude testing is available on most military recruits, and the VA medical system allows them to be tracked over a long follow-up period. Given this, and the timing of its initiation coinciding with greater survival from conflict-related TBI, means the VHIS has been and continues to be instrumental in gathering long-term data about subjects with TBI. Results from the VHIS have suggested that penetrating TBI carries a high risk of long-term sequelae, such as PTE and cognitive impairment, which may occur decades after injury, so has provided solid evidence that such patients may require long-term medical follow up. It should be emphasized, however, that these results may not always be generalizable to closed TBI, and therefore the type of injuries seen in the civilian population. Our findings are probably compatible with focal lesions secondary to a variety of causes (e.g., stroke, tumor, etc.), but closed TBI may have additional white matter shearing and pathology that is more extensive than that seen in penetrating TBI. Penetrating TBI also crosses traditional vascular boundaries and does not generally respect different neuronal susceptibilities to disease, so does have a unique signature or profile of impairments in any individual patient, but by interpreting our results by lesion site, we have tried to make our results generalizable by location. However, the ability to maintain a longitudinal assessment of a large sample of subjects from preinjury, through acute injury and many years of follow up is fraught with difficulties. The VHIS has only been able to review the long-term clinical, neuropsychological, and genetic characteristics in a subset of the original cohort, and we may well have seen differing results if we had been able to examine the entire sample throughout the length of the study.
Besides a core clinical evaluation, each phase of the VHIS has tried to address emerging issues within cognitive neuroscience, neurology, and psychiatry. For instance, the need for an accurate assessment of the brain lesions in PH3 lead to the development of the ABLe software program (Makale et al., 2002; Solomon et al., 2007), which characterizes lesions in terms of volume and intersection with Brodmann areas and allows for correlations between subjects with overlapping lesions and behavioral deficit.
In addition, PH2 of the VHIS led directly to the establishment of the Defense and Veterans Head Injury Program (DVHIP). Such TBI units and programs at major Military and VA Hospitals continue to operate to this day, now as Defense and Veterans Brain Injury Centers (DVBIC). Until the creation of the DVHIP, there had been no national systematic program providing TBI-specific care and rehabilitation within the VA (Salazar et al., 2000). The DVHIP was created initially as an interagency clinical program oriented to treatment, rehabilitation, and care management. It was formed by collaboration between the Department of Defense, the Department of Veteran Affairs, the Brain Injury Association (BIA), and the International Brain Injury Association (IBIA). The principal goals of the program now are to ensure that military and veteran TBI patients receive standardized TBI-specific evaluation, treatment, and follow-up, while at the same time helping to define optimal acute and chronic care for victims of TBI nationwide, as well as conducting rehabilitation and clinical treatment trials. The DVHIP also included a simple, updated Head and Spinal Combat Injury Registry form similar to that used by in the original VHIS registry, which is now used within the military and VA via the DVBIC. This has been approved by the Joint Committee of Military Neurosurgeons of the American Association of Neurological Surgeons (AANS) and Congress of Neurological Surgeons (CNS) for deployment in time of war. Thus not only has the VHIS been vital in its contribution to our understanding of TBI and neuropsychology, it has helped produce a system that will facilitate the early identification of future injured soldiers and their long-term management – a worthy legacy for Dr. Caveness and the many victims of TBI studied in the last 40 years. The unique breadth and length of follow up of this cohort makes the future prospects for information to be collected from PH4 very exciting, and the VHIS has provided a model for subsequent longitudinal studies of TBI (Tables 1 and 2). Given the increasing numbers of both civilian patients and military casualties suffering TBI, which will certainly require care in the future, expanding such research seems long overdue.
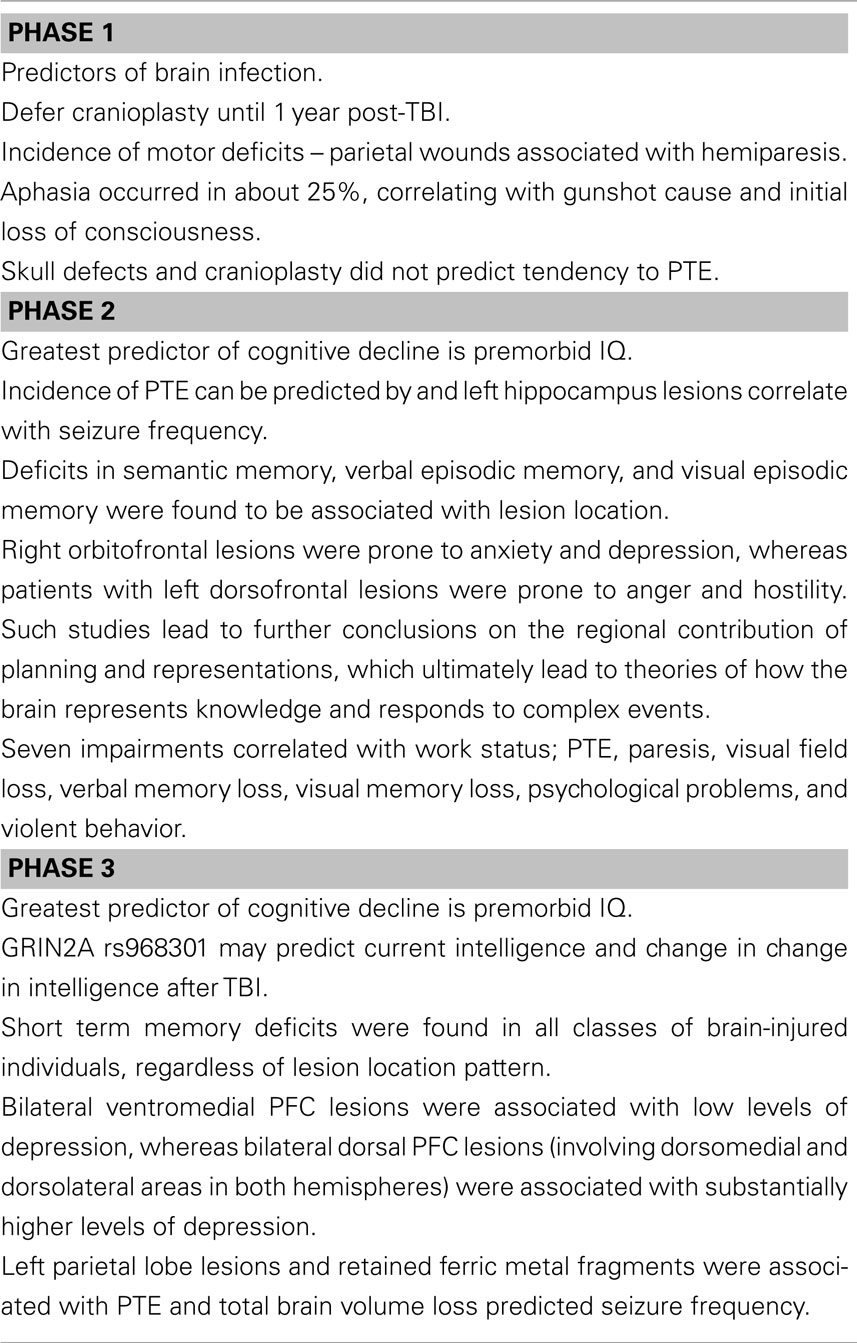
Table 1. Five key findings of the VHIS.
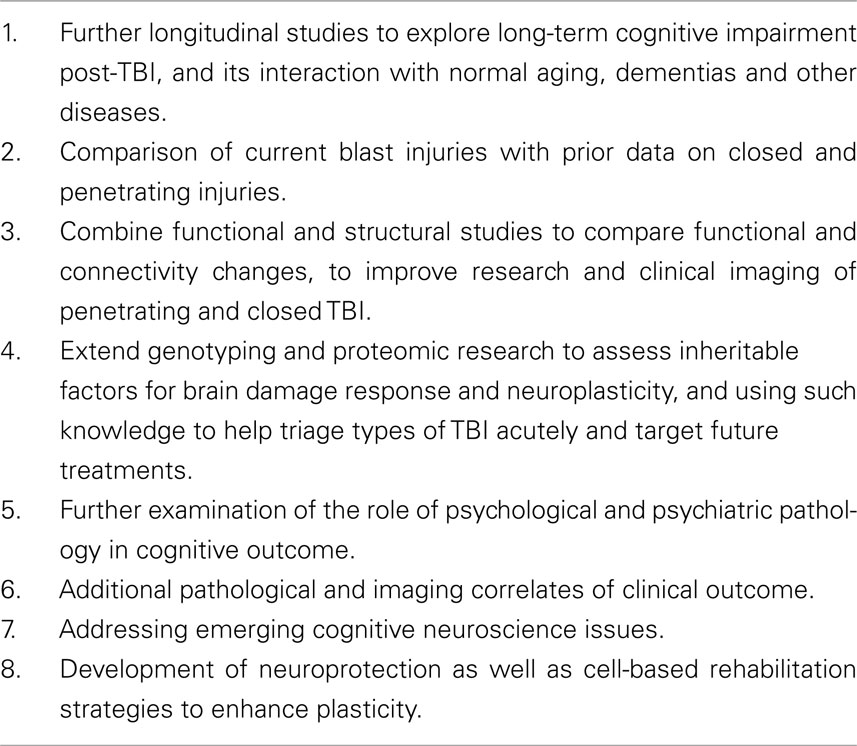
Table 2. Possible future goals for studies of military TBI patients.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to our research participants whose dedicated, selfless, long-term commitment to the Vietnam Head Injury Study enabled us to carry out our research and change the way the United States military diagnoses and treats traumatic brain injury. We also thank all of the associated principal investigators and collaborators who have helped insure the success of our research program. In particular we want to single out Herbert Brown, Max Hoyt, Karen Schwab, and William F. Caveness for their efforts in helping establish and sustain the Vietnam Head Injury Study. Finally, one of us (Jordan Grafman) benefited from the wise consul of Freda Newcombe, Charles G. Matthews, Herbert Weingartner, and Alwyn Lishman in the early stages of the Vietnam Head Injury Study.
References
Barbey, A. K., Krueger, F., and Grafman, J. (2009). An evolutionarily adaptive neural architecture for social reasoning. Trends Neurosci. 32, 603–610.
Bender, M. B., and Teuber, H. L. (1948). Spatial organization of visual perception following injury to the brain. Arch. Neurol. Psychiatry 59, 39–62.
Boake, C., and Diller, L. (2005). “History of rehabilitation for traumatic brain injury,” in Rehabilitation for Traumatic Brain Injury, eds W. M. High, A. M. Sander, M. A. Struchen and K. A. Hart (Oxford: Oxford University Press), 3–13.
Carey, M. E., Sacco, W., and Merkler, J. (1982). An analysis of fatal and non-fatal head wounds incurred during combat in Vietnam by U.S. forces. Acta Chir. Scand. Suppl. 508, 351–356.
Carlin, D., Bonerba, J., Phipps, M., Alexander, G., Shapiro, M., and Grafman, J. (2000). Planning impairments in frontal lobe dementia and frontal lobe lesion patients. Neuropsychologia 38, 655–665.
Caveness, W. F., Meirowsky, A. M., Rish, B. L., Mohr, J. P., Kistler, J. P., Dillon, D., and Weiss, G. H. (1979). The nature of posttraumatic epilepsy. J. Neurosurg. 50, 545–553.
Corkin, S., Rosen, T. J., Sullivan, E. V., and Clegg, R. A. (1989). Penetrating head injury in young adulthood exacerbates cognitive decline in later years. J. Neurosci. 9, 3876–3883.
Corkin, S., Sullivan, E. V., and Carr, F. A. (1984). Prognostic factors for life expectancy after penetrating head injury. Arch. Neurol. 41, 975–977.
Dimitrov, M., Grafman, J., and Hollnagel, C. (1996). The effects of frontal lobe damage on everyday problem solving. Cortex 32, 357–366.
Dimitrov, M., Phipps, M., Zahnl, T. P., and Grafman, J. (1999). A thoroughly modern gage. Neurocase 5, 345–354.
Forbes, C. E., and Grafman, J. (2010). The role of the human prefrontal cortex in social cognition and moral judgment. Annu. Rev. Neurosci. 33, 299–324.
Frattali, C., Hanna, R., McGinty, A. S., Gerber, L., Wesley, R., Grafman, J., and Coelho, C. (2007). Effect of prefrontal cortex damage on resolving lexical ambiguity in text. Brain Lang. 102, 99–113.
Giza, C. C., Maria, N. S., and Hovda, D. A. (2006). N-methyl-D-aspartate receptor subunit changes after traumatic brain injury to the developing brain. J. Neurotrauma 23, 950–961.
Goel, V., and Grafman, J. (1995). Are the frontal lobes implicated in “planning” functions? Re-interpreting data from the tower of Hanoi. Neuropsychologia 33, 623–642.
Goel, V., and Grafman, J. (2000). Role of the right prefrontal cortex in Ill-structured planning. Cogn. Neuropsychol. 17, 415–436.
Goel, V., Pullara, S. D., and Grafman, J. (2001). A computational model of frontal lobe dysfunction: working memory and the tower of Hanoi task. Cogn. Sci. 25, 287–313.
Goel, V., Shuren, J., Sheesley, L., and Grafman, J. (2004). Asymmetrical involvement of frontal lobes in social reasoning. Brain 127, 783–790.
Goel, V., Stollstorff, M., Nakic, M., Knutson, K., and Grafman, J. (2009). A Role for right ventromedial prefrontal cortex in reasoning about indeterminate relations. Neuropsychologia 47, 2790–2797.
Goel, V., Tierney, M., Sheesley, L., Bartolo, A., Vartanian, O., and Grafman, J. (2007). Hemispheric specialization in human prefrontal cortex for resolving certain and uncertain inferences. Cereb. Cortex 17, 2245–2250.
Gozzi, M., Raymont, V., Solomon, J., Koenigs, M., and Grafman, J. (2009). Dissociable effects of prefrontal and anterior temporal cortical lesions on stereotypical gender attitudes. Neurology 74, 749–754.
Grafman, J., Jonas, B., and Salazar, A. (1992). Epilepsy following penetrating head injury to the frontal lobes. Effects on cognition. Adv. Neurol. 57, 369–378.
Grafman, J., Jonas, B. S., Martin, A., Salazar, A. M., Weingartner, H., Ludlow, C., Smutok, M. A., and Vance, S. C. (1988). Intellectual function following penetrating head injury in Vietnam veterans. Brain 111(Pt 1), 169–184.
Grafman, J., Kampen, D., Rosenberg, J., Salazar, A., and Boller, F. (1989). Calculation abilities in a patient with a virtual left hemispherectomy. Behav. Neurol. 2, 183–194.
Grafman, J., and Salazar, A. (1999). The William Fields Caveness Vietnam head injury study: past and future. Brain Inj. Source 3, 12–14.
Grafman, J., Salazar, A., Weingartner, H., Vance, S., and Amin, D. (1986a). The relationship of brain-tissue loss volume and lesion location to cognitive deficit. J. Neurosci. 6, 301–307.
Grafman, J., Salazar, A. M., Weingartner, H., and Amin, D. (1986b). Face memory and discrimination: a preliminary analysis of the persistent effects of penetrating brain wounds. Int. J. Neurosci. 29, 125–139.
Grafman, J., Vance, S. C., Weingartner, H., Salazar, A. M., and Amin, D. (1986c). The effects of lateralized frontal lesions on mood regulation. Brain 109(Pt 6), 1127–1148.
Grafman, J., Smutok, M., Sweeney, J., Vance, S. C., Salazar, A. M., and Weingartner, H. (1985a). Effects of left-hand preference on postinjury measures of distal motor ability. Percept. Mot. Skills 61, 615–624.
Grafman, J., Salazar, A. M., Weingartner, H., Vance, S. C., and Ludlow, C. (1985b). Isolated impairment of memory following a penetrating lesion of the fornix. Arch. Neurol. 42, 1162–1168.
Grafman, J., Schwab, K., Warden, D., Pridgen, A., Brown, H. R., and Salazar, A. M. (1996). Frontal lobe injuries, violence, and aggression: a report of the Vietnam head injury study. Neurology 46, 1231–1238.
Groswasser, Z., Reider-Groswasser, I. I., Schwab, K., Ommaya, A. K., Pridgen, A., Brown, H. R., Cole, R., and Salazar, A. M. (2002). Quantitative imaging in late TBI. Part II: cognition and work after closed and penetrating head injury: a report of the Vietnam head injury study. Brain Inj. 16, 681–690.
Harlow, J. M. (1868). Recovery After Severe Injury to the Head. Boston: Massachusetts Medical Society
Holmes, G., and Lister, W. T. (1916). Disturbances of vision from cerebral lesions, with special reference to the cortical representation of the macula. Brain 39, 34.
Jonas, B. S., Schwab, K., and Salazar, A. M. (1987). “Factors influencing participation in a multi-stage study of head injury: potential biases in the Vietnam head injury study,” in Proceedings of the Section on Survey Research Methods of the Association for Statistical Analysis.
Koenigs, M., Barbey, A., Postle, B. R., and Grafman, J. (2009a). Superior parietal cortex is critical for the manipulation of information in working memory. J. Neurosci. 29, 14980–14986.
Koenigs, M., Huey, E. D., Raymont, V., Cheon, B., Solomon, J., Wassermann, E. M., and Grafman, J. (2009b). Focal brain damage protects against post-traumatic stress disorder in combat veterans. Proc. Natl. Acad. Sci. U.S.A. 106, 22486–22491.
Koenigs, M., Holliday, J., Solomon, J., and Grafman, J. (2010). Left dorsomedial frontal brain damage is associated with insomnia. J. Neurosci. 30, 16041–16043.
Koenigs, M., Huey, E. D., Calamia, M., Raymont, V., Tranel, D., and Grafman, J. (2008). Distinct regions of prefrontal cortex mediate resistance and vulnerability to depression. Nat. Neurosci. 11, 232–237.
Kraft, J. F., Schwab, K. A., Salazar, A. M., and Brown, H. R. (1993). Occupational and educational achievements of head injured Vietnam veterans at 15-year follow-up. Arch. Phys. Med. Rehabil. 74, 596–601.
Kraus, J. F., and McArthur, D. L. (1996). Epidemiologic aspects of brain injury. Neurol. Clin. 14, 435–450.
Krueger, F., Barbey, A. K., McCabe, K., Strenziok, M., Zamboni, G., Solomon, J., Raymont, V., and Grafman, J. (2009). The neural bases of key competencies of emotional intelligence. Proc. Natl. Acad. Sci. U.S.A. 106, 22486–22491.
Krueger, F., Pardini, M., Huey, E. D., Raymont, V., Solomon, J., Lipsky, R. H., Hodgkinson, C. A., Goldman, D., and Grafman, J. (2011). The role of the Met66 brain-derived neurotrophic factor allele in the recovery of executive functioning after combat-related traumatic brain injury. J. Neurosci. 31, 598–606.
Lee, S. S., Wild, K., Hollnagel, C., and Grafman, J. (1999). Selective visual attention in patients with frontal lobe lesions or Parkinson’s disease. Neuropsychologia 37, 595–604.
Lepore, F. E. (1994). Harvey Cushing, Gordon Holmes, and the neurological lessons of World War I. Arch. Neurol. 51, 711–722.
Lindsay, J., Laurin, D., Verreault, R., Hebert, R., Helliwell, B., Hill, G. B., and McDowell, I. (2002). Risk factors for Alzheimer’s disease: a prospective analysis from the Canadian study of health and aging. Am. J. Epidemiol. 156, 445–453.
Ludlow, C. L., Rosenberg, J., Fair, C., Buck, D., Schesselman, S., and Salazar, A. (1986). Brain lesions associated with nonfluent aphasia fifteen years following penetrating head injury. Brain 109(Pt 1), 55–80.
Luria, A. R. (1972). The Man with a Shattered World: The History of a Brain Wound. New York: Basic Books
Mah, L., Arnold, M. C., and Grafman, J. (2004). Lesions of prefrontal cortex impair social perception. Am. J. Psychiatry 161, 1247–1255.
Mah, L. W. Y., Arnold, M. C., and Grafman, J. (2005). Deficits in social knowledge following lesions of ventromedial prefrontal cortex. J. Neuropsychiatry Clin. Neurosci. 17, 66–74.
Makale, M., Solomon, J., Patronas, N. J., Danek, A., Butman, J. A., and Grafman, J. (2002). Quantification of brain lesions using interactive automated software. Behav. Res. Methods Instrum. Comput. 34, 6–18.
Milne, E., and Grafman, J. (2001). Ventromedial prefrontal cortex lesions in humans eliminate implicit gender stereotyping. J. Neurosci. 21, 1–6.
Mishkin, M. (1972). “Cortical visual areas and their interactions,” in Brain and Human Behavior, eds G. Karczmar and J. C. Eccles (Berlin: Springer), 178–208.
Mohr, J. P., Weiss, G. H., Caveness, W. F., Dillon, J. D., Kistler, J. P., Meirowsky, A. M., and Rish, B. L. (1980). Language and motor disorders after penetrating head injury in Vietnam. Neurology 30, 1273–1279.
Muthén, L. K., and Muthén, B. O. (1998–2004). Mplus User’s Guide, 3rd Edn. Los Angeles: Muthén & Muthén.
Newcombe, F., Brooks, N., and Baddeley, A. (1980). Rehabilitation after brain damage: an overview. Int. Rehabil. Med. 2, 133–137.
Newcombe, F., Oldfield, R. C., Ratcliff, G. G., and Wingfield, A. (1971). Recognition and naming of object-drawings by men with focal brain wounds. J. Neurol. Neurosurg. Psychiatr. 34, 329–340.
Pardini, M., Krueger, F., Hodgkinson, C., Raymont, V., Ferrier, C., Goldman, D., Strenziok, M., Guida, S., and Grafman, J. (in press). Prefrontal cortex lesions and MAO-A modulate aggression in penetrating traumatic brain injury.
Pardini, M., Krueger, F., Raymont, V., and Grafman, J. (2010). Ventromedial prefrontal cortex modulates fatigue after penetrating traumatic brain injury. Neurology 74, 749–754.
Parton, A., Coulthard, E., and Husain, M. (2005). Neuropharmacological modulation of cognitive deficits after brain damage. Curr. Opin. Neurol. 18, 675–680.
Rattermann, M. J., Spector, L., Grafman, J., Levin, H., and Howard, H. (2001). Partial and total-order planning: evidence from normal and prefrontally damaged populations. Cogn. Sci. 25, 941–975.
Raymont, V., and Grafman, J. (2006). Cognitive neural plasticity during learning and recovery from brain damage. Prog. Brain Res. 157, 199–206.
Raymont, V., Greathouse, A., Reding, K., Lipsky, R., Salazar, A., and Grafman, J. (2008). Demographic, structural and genetic predictors of late cognitive decline after penetrating head injury. Brain 131(Pt 2), 543–558.
Raymont, V., Salazar, A. M., Lipsky, R., Goldman, D., Tasick, G., and Grafman, J. (2010). Correlates of posttraumatic epilepsy 35 years following combat brain injury. Neurology 75, 224–229.
Rish, B. L., Caveness, W. F., Dillon, J. D., Kistler, J. P., Mohr, J. P., and Weiss, G. H. (1981). Analysis of brain abscess after penetrating craniocerebral injuries in Vietnam. Neurosurgery 9, 535–541.
Rish, B. L., Dillon, J. D., Caveness, W. F., Mohr, J. P., Kistler, J. P., and Weiss, G. H. (1980). Evolution of craniotomy as a debridement technique for penetrating craniocerebral injuries. J. Neurosurg. 53, 772–775.
Rish, B. L., Dillon, J. D., Meirowsky, A. M., Caveness, W. F., Mohr, J. P., Kistler, J. P., and Weiss, G. H. (1979). Cranioplasty: a review of 1030 cases of penetrating head injury. Neurosurgery 4, 381–385.
Rish, B. L., Dillon, J. D., and Weiss, G. H. (1983). Mortality following penetrating craniocerebral injuries. An analysis of the deaths in the Vietnam head injury registry population. J. Neurosurg. 59, 775–780.
Romero, S. G., Manly, C. F., and Grafman, J. (2002). Investigating cognitive neuroplasticity in single cases: Lessons learned from applying functional neuroimaging techniques to the traditional neuropsychological case study framework. Neurocase 8, 355–368.
Rueckert, L., and Grafman, J. (1996). Sustained attention deficits in patients with right frontal lesions. Neuropsychologia 34, 953–963.
Rueckert, L., and Grafman, J. (1998). Sustained attention deficits in patients with lesions of posterior cortex. Neuropsychologia 36, 653–660.
Salazar, A., Grafman, J., Jabbari, B., Vance, S. C., and Amin, D. (1987). “Epilepsy and cognitive loss after penetrating head injury,” in Advances in Epileptology, eds P. Wolf, W. Dam, M. Janz and F. Dreifuss (New York: Raven Press), 627–631.
Salazar, A. M., Grafman, J., Vance, S. C., Weingartner, H., Dillon, J. D., and Ludlow, C. (1986). Consciousness and amnesia following penetrating head injury. Neurology 36, 178–187.
Salazar, A. M., Jabbari, B., Vance, S. C., Grafman, J., Amin, D., and Dillon, J. D. (1985). Epilepsy after penetrating head injury. I. Clinical correlates: a report of the Vietnam head injury study. Neurology 35, 1406–1414.
Salazar, A. M., Schwab, K., and Grafman, J. H. (1995). Penetrating injuries in the Vietnam war. Traumatic unconsciousness, epilepsy, and psychosocial outcome. Neurosurg. Clin. N. Am. 6, 715–726.
Salazar, A. M., Zitnay, G. A., Warden, D. L., and Schwab, K. A. (2000). Defense and Veterans Head Injury Program: background and overview. J. Head Trauma Rehabil. 15, 1081–1091.
Sanfey, A. G., Hastie, R., Colvin, M. K., and Grafman, J. (2003). Phineas Gauged: decision-making and the human prefrontal cortex. Neuropsychologia 41, 1218–1229.
Schooler, C., Caplan, L. J., Revell, A. J., Salazar, A. M., and Grafman, J. (2008). Brain lesion and memory functioning: short-term memory deficit is independent of lesion location. Psychon. Bull. Rev. 15, 521–527.
Schwab, K., Grafman, J., Salazar, A. M., and Kraft, J. (1993). Residual impairments and work status 15 years after penetrating head injury: report from the Vietnam head injury study. Neurology 43, 95–103.
Smutok, M. A., Grafman, J., Salazar, A. M., Sweeney, J. K., Jonas, B. S., and DiRocco, P. J. (1989). Effects of unilateral brain damage on contralateral and ipsilateral upper extremity function in hemiplegia. Phys. Ther. 69, 195–203.
Solomon, J., Raymont, V., Braun, A., Butman, J. A., and Grafman, J. (2007). User-friendly software for the analysis of brain lesions (ABLe). Comput. Methods Programs Biomed. 86, 245–254.
Swanson, S. J., Rao, S. M., Grafman, J., Salazar, A. M., and Kraft, J. (1995). The relationship between seizure subtype and interictal personality. Results from the Vietnam head injury study. Brain 118(Pt 1), 91–103.
Teuber, H. L. (1975). Recovery of function after brain injury in man. Ciba Found. Symp. 34, 159–190.
van Gijn, J. (2009). From the archives. Cerebral involvement in head injury. A study based on the examination of two hundred cases. By W. Ritchie Russell, MD. 1932; 55: 549–603. Brain 132, 565–567.
Varon, S., Hagg, T., and Manthorpe, M. (1991). Nerve growth factor in CNS repair and regeneration. Adv. Exp. Med. Biol. 296, 267–276.
Warden, D. J. (2006). Military TBI during the Iraq and Afghanistan wars. Head Trauma Rehabil. 21, 398–402.
Weinstein, S., and Teuber, H. L. (1957). The role of pre-injury education and intelligence level in intellectual loss after brain injury. J. Comp. Physiol. Psychol. 50, 535–539.
Weiss, G. H., and Caveness, W. F. (1972). Prognostic factors in the persistence of posttraumatic epilepsy. J. Neurosurg. 37, 164–169.
Weiss, G. H., Feeney, D. M., Caveness, W. F., Dillon, D., Kistler, J. P., Mohr, J. P., and Rish, B. L. (1983). Prognostic factors for the occurrence of posttraumatic epilepsy. Arch. Neurol. 40, 7–10.
Weiss, G. H., Salazar, A. M., Vance, S. C., Grafman, J., and Jabbari, B. (1986). Predicting posttraumatic epilepsy in penetrating head injury. Arch. Neurol. 43, 771–773.
Walker, A. E., and Jablon, S. (1961). A Follow up Study of Head Wounds in World War II. Washington, DC: Veterans Administration
Wood, J. N., and Grafman, J. (2003). Human prefrontal cortex: processing and representational perspectives. Nat. Rev. Neurosci. 4, 139–147.
Keywords: brain imaging, brain injury, brain lesion, neuropsychology
Citation: Raymont V, Salazar AM, Krueger F and Grafman J (2011) “Studying injured minds” – the Vietnam head injury study and 40 years of brain injury research. Front. Neur. 2:15. doi:10.3389/fneur.2011.00015
Received: 06 December 2010; Accepted: 03 March 2011;
Published online: 28 March 2011.
Edited by:
Ibolja Cernak, Johns Hopkins University, USAReviewed by:
Jeffrey J. Bazarian, University of Rochester, USAVassilis E. Koliatsos, Johns Hopkins University School of Medicine, USA
Harvey S. Levin, Baylor College of Medicine, USA
Copyright: © 2011 Raymont, Salazar, Krueger and Grafman. This is an open-access article subject to an exclusive license agreement between the authors and Frontiers Media SA, which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
*Correspondence: Jordan Grafman, Traumatic Brain Injury Research Laboratory, Kessler Foundation, 1199 Pleasant Valley Road, West Orange, NJ 07052, USA e-mail: jgrafman@ kesslerfoundation.org