 Sónia Martins1
Sónia Martins1 Lia Fernandes1,2,3*
Lia Fernandes1,2,3*- 1 Research and Education Unit on Aging, UNIFAI/ICBAS, University of Porto, Porto, Portugal
- 2 Clinical Neuroscience and Mental Health Department, Faculty of Medicine, University of Porto, Porto, Portugal
- 3 Psychiatry Service, S. João Hospital, Porto, Portugal
The present review aims to highlight this intricate syndrome, regarding diagnosis, pathophysiology, etiology, prevention, and management in elderly people. The diagnosis of delirium is based on clinical observations, cognitive assessment, physical, and neurological examination. Clinically, delirium occurs in hyperactive, hypoactive, or mixed forms, based on psychomotor behavior. As an acute confusional state, it is characterized by a rapid onset of symptoms, fluctuating course and an altered level of consciousness, global disturbance of cognition or perceptual abnormalities, and evidence of a physical cause. Although pathophysiological mechanisms of delirium remain unclear, current evidence suggests that disruption of neurotransmission, inflammation, or acute stress responses might all contribute to the development of this ailment. It usually occurs as a result of a complex interaction of multiple risk factors, such as cognitive impairment/dementia and current medical or surgical disorder. Despite all of the above, delirium is frequently under-recognized and often misdiagnosed by health professionals. In particular, this happens due to its fluctuating nature, its overlap with dementia and the scarcity of routine formal cognitive assessment in general hospitals. It is also associated with multiple adverse outcomes that have been well documented, such as increased hospital stay, function/cognitive decline, institutionalization and mortality. In this context, the early identification of delirium is essential. Timely and optimal management of people with delirium should be performed with identification of any possible underlying causes, dealing with a suitable care environment and improving education of health professionals. All these can be important factors, which contribute to a decrease in adverse outcomes associated with delirium.
Introduction
The word delirium is derived from the Latin term delirare, meaning to become “crazy or to rave” (Saxena and Lawley, 2009). It has been documented in medical literature for more than 2000 years, with a fairly consistent clinical description (Adamis et al., 2007). It was reported during the time of Hippocrates, who used the words phrenitis (frenzy) and lethargus (lethargy) to describe the hyperactive and hypoactive subtypes of delirium. As a medical term, delirium was first used by Celsus in the first century A. D. to describe mental disorders associated with fever or head trauma (Khan et al., 2009).
A variety of terms have been used in the literature to describe delirium, including “acute confusional state,” “acute brain syndrome,” “acute cerebral insufficiency,” and “toxic-metabolic encephalopathy” (Morandi et al., 2008). However, delirium is now the preferred term (Gill and Mayou, 2000) and it has been suggested that acute confusional state should be the only accepted synonym for this syndrome (Lipowski, 1992).
Delirium was standardized for the first time as a clinical entity in the Diagnostic and Statistical Manual of Mental Disorders, third edition/DSM-III (APA, 1980). The more recent version of this manual is now considered to be the gold standard for delirium diagnosis (CCSMH, 2006; NICE, 2010). Furthermore, this classification has been designed to be simple and sensitive enough to detect the presence of delirium in different settings, in particular among acutely ill and hospitalized elderly patients (Laurila et al., 2004).
According to the current DSM criteria (APA, 2000), delirium is characterized by the rapid onset of symptoms that tend to fluctuate even during the same day with an altered level of consciousness, global disturbance of cognition or perceptual abnormalities and evidence of a physical cause, substance intoxication/withdrawal, or multiple etiologies.
Delirium is a common and serious problem, mainly in hospitalized elderly patients (Saxena and Lawley, 2009). Its diagnosis is based on clinical history, key features observation, and physical and cognitive assessment (Fearing and Inouye, 2009; Fong et al., 2009a).
The etiology of delirium is usually multifactorial, resulting commonly from a combination of predisposing and precipitating factors (Rolfson, 2002; CCSMH, 2006). Its pathophysiological mechanisms remain poorly understood, with some evidence for the contribution of neurotransmission disruption, inflammation, or acute stress responses (Saxena and Lawley, 2009).
Delirium has also been associated with multiple adverse outcomes (Siddiqi et al., 2006; Cole et al., 2009). It is often poorly diagnosed, in particular due to its fluctuating nature, its overlap with dementia and lack of formal cognitive assessment in general hospitals (Cole, 2005; CCSMH, 2006; Inouye, 2006).
In the management of delirium, non-pharmacological interventions have been considered the first-line strategy (Fong et al., 2009a), which includes, initially, the identification of underlying causes, supportive care (with involvement of family), and manipulation of the environment. In spite of that, prevention strategies emerge as the most important and cost-effective approaches for delirium, contributing to the decrease in its frequency, and associated poor outcomes (Inouye, 2006; NICE, 2010), namely in patients with Alzheimer’s disease (Fick et al., 2002), given the evidence that delirium accelerates disease progression, even in cases where the etiology does not involve any cerebral structural insult.
Epidemiology
Delirium is a common and serious condition among the elderly, particularly in hospitalized patients, affecting up to 30% of this patient population (Saxena and Lawley, 2009). Most recent studies report a prevalence of delirium of 10–31% on admission and an incidence of 3–29% during hospitalization (Siddiqi et al., 2006).
This risk increases exponentially in intensive care units, with prevalence rates of up to 80% (Morandi and Jackson, 2011) and in palliative care units, where it is reported to be as high as 85% (Casarett and Inouye, 2001). Higher rates are also noted in surgical settings (Young and Inouye, 2007), with an incidence reported to range from 10 to 70% after surgery (Guenther and Radtke, 2011), especially in patients undergoing cardiothoracic surgery, emergency orthopedic procedures (repair of a hip fracture), vascular surgery, or cataract removal (Saxena and Lawley, 2009). Studies among elderly people presenting in emergency departments have reported prevalence rates of 5–30% (Lewis et al., 1995; Elie et al., 2000; Inouye, 2006).
In spite of long-term care, nursing home residents represent a vulnerable group, but only a few studies have been carried out (CCSMH, 2006). In a recent study (McCusker et al., 2011) the prevalence of delirium has been estimated between 3.4 and 33.3%. In the community, as expected, the prevalence is lower, ranging from 1 to 2% (Popeo, 2011).
Clinical Features
Based on DSM-IV-TR criteria, delirium is characterized by the rapid onset of symptoms (usually hours or days) and tends to fluctuate, with an altered level of consciousness, with an inability to focus, sustain or shift attention, and a change in cognition (such as memory impairment, disorientation, language disturbance) or development of a perceptual disturbance that is not better accounted for by dementia. Moreover, there is evidence from the history, physical examination, or laboratory findings that the disturbance is caused by the direct physiological consequences of a general medical condition, or substance intoxication/withdrawal, or due to multiple etiologies (APA, 2000).
This definition has the advantage of covering a broad clinical spectrum, but it also implies great complexity. The areas of neurological function identified are indeed wide and can hardly be attributed to the activity of discrete cerebral structures. Also controversial is the interpretation that the syndrome is caused by the ability of different etiological factors to impact on a final common pathway producing stereotyped clinical consequences (Caraceni and Grassi, 2011).
Sudden and acute onset and fluctuating course are the central features of delirium. Therefore, it is important to establish the patient’s level of baseline cognitive functioning and the course of cognitive change (Fearing and Inouye, 2009). Symptom fluctuation is unpredictable. They may be intermittent, and are often worse at night (Cole, 2004).
Consciousness as a brain function allows the awareness of oneself and of the environment (Fish, 1967) and is characterized by two main aspects: the level of consciousness and the content of consciousness (Plum and Posner, 1972). The level of consciousness reflects arousal and vigilance: being awake, asleep, or comatose. The content of consciousness, or part of it, is experienced by the subject as awareness of him or herself and of the environment when awake and normally alert. The content of consciousness and cognition can be examined only if at least a certain degree of wakefulness and alertness are preserved (Caraceni and Grassi, 2011).
Consciousness should also be considered as a continuum from full alertness and awareness to coma and its impairment appears as the primary change in acute organic disorders. In this sense, it places an important role in the detection of acute disturbances of brain function, as well as, in the assessment of its severity (Lishman, 1997).
In delirium, the disturbance of consciousness is one of the earliest manifestations, which often fluctuates, mainly in the evening when environmental stimulation is at its lowest (Burns et al., 2004). The level of consciousness may fluctuate between extremes in the same patient, or alternatively may present with more subtle signs, such as mild drowsiness, or an impaired level of attention (Saxena and Lawley, 2009). In fact, the patient may appear obviously drowsy, lethargic, or even semi-comatose in more advanced cases. The opposite extreme, hyper-vigilance, may also occur, especially in cases of alcohol or sedative drug withdrawal (less common in elderly people; Francis and Young, 2011).
Attention is the process that enables one to select relevant stimuli from the environment, to focus and sustain behavioral responses to such stimuli, and to switch mental activity toward new stimuli, reorienting the individual behavior, according to the relevance of the stimulus (Caraceni and Grassi, 2011). Attention is a different function from consciousness, but it is dependent on it. Thus, variable degrees of attention are possible with full consciousness, but complete attention and concentration are impossible with diminished consciousness. In fact, attention may be pathologically decreased in organic states, usually with lowering of consciousness (Oyebode, 2008).
In delirium, inattention occurs and it is also considered one of the important cardinal features (Cole, 2005). Usually these patients are easily distractible by irrelevant stimuli, or have difficulty keeping track of what was being said during the clinical interview. Moreover, most of the time, the questions must be repeated because the individual’s attention wanders (APA, 2000).
Typically there are global or multiple deficits in cognition, including memory impairment and disorientation. In fact, due to this inattentiveness, the registration of new information can be impaired, affecting memory, and orientation functions (Cole, 2004).
In the first case, the short-term memory is the most commonly affected (APA, 2000; Longo et al., 2011), but retrieval of stored information can also be disturbed (Saxena and Lawley, 2009). For instance, patients can have an inability to remember events in the hospital or difficulty in remembering instructions (Inouye, 2003).
Disorientation is usually common, first in reference to time and then to place (Burns et al., 2004). However, it may be considered not abnormal for an inpatient that has been seriously ill for a long time, without references of days or months.
The functions of thinking and speaking overlap and cannot be readily separated from each other, but they are clearly different. Both can be impaired in delirium (Oyebode, 2008).
Language difficulties and its impoverishment in delirium patients are probably more related to the disorder of arousal and attention levels, than a specific cause, or still they may reveal a thought process alteration. In severe cases of global impairment, frank confabulation can dominate, leaving little opportunity to assess language, memory, and thought content. Often language and speech, including reading, are less affected than writing, especially in mild or early stages. Few specific observations on language disturbances found in the course of delirium are available. In one study, misnaming has been commonly found, as frequent as observed in demented patients, but they differed in being more often of the types of word intrusion and unrelated misnaming (Wallesch and Hundsaltz, 1994). Word intrusion is in part explained by perseveration. The patient repeats a previously uttered word (therefore perseverating) rather than the expected word that he/she is unable to find or pronounce. Unrelated misnaming is the use of word that wildly differs in meaning from the intended word and therefore has no relationship with the word appropriate for the context, unlike paraphasia (Caraceni and Grassi, 2011).
Another clinical feature is disorganized thinking, manifested by incoherent speech and rambling or irrelevant conversation, or unclear or illogical flow of ideas (Inouye, 2006). The patient may be unable to make appropriate decisions, or execute simple tasks. Their judgment and insight may be poor and delusions can also occur in around 30% of the cases (Meagher et al., 2007), particularly of a paranoid or persecutory nature (Cole, 2004).
Perceptual disturbances have also been described in people with delirium. These may include illusions and misinterpretations, which arise from a false impression of an actual stimulus. For example, a patient may become agitated and fearful, believing that a shadow in a dark room is actually an attacker. The perceptual disturbance can also include hallucinations, where no object is actually present (Oyebode, 2008). Visual hallucinations are the most frequent, often occurring at night (Cole, 2004), and in some cases they can appear during the day as soon as the patient closes his eyes. The content of the hallucinations tends to be simple, at times just colors, lines, or shapes (Caraceni and Grassi, 2011). However, it can include, for instance, dangerous animals or bizarre images (Saxena and Lawley, 2009).
There are other clinical features commonly associated with delirium that are not included in the diagnostic criteria (Fearing and Inouye, 2009). One of them is sleep-wake cycle disturbance, characterized by an excessive daytime sleepiness with insomnia at night, fragmentation, and reduction of sleep or complete sleep-cycle reversal (Inouye, 2006).
Some studies have observed the potential role of these disturbances, in particular disordered circadian rhythm (Bachman and Rabins, 2006) and sleep fragmentation (Kim et al., 2005) as an important contributing factor to the sundowning syndrome. This phenomenon has been seen in patients with delirium and is characterized by worsening of disruptive behavior in the late afternoon or evening. This syndrome may also be due to fatigue and reduced sensory input toward the evening (Bachman and Rabins, 2006; Saxena and Lawley, 2009).
Disturbed psychomotor behavior is another clinical feature of delirium, with unusually increased or decreased motor activity. In the first case, patients may have restlessness or frequent sudden changes of position. On the other hand, the patient may also show sluggishness or lethargy, approaching stupor (APA, 2000).
In these patients, emotional disturbances, such as anxiety, fear, irritability, anger, depression, and euphoria, may also be seen. These symptoms are often influenced by factors, such as medical or surgical conditions, personality characteristics, premorbid psychiatric disorders, or recent life events (Cole, 2004).
According to some authors (Meagher et al., 2008) some caveats should be taken into account in the discussion of delirium classification and criteria currently used.
For instance, despite the tendency to make the criteria explicit according to the specificity of the symptoms of delirium, it must be remembered that certain clinical situations, hospitalization, or physical symptoms, such as pain or breathing difficulty, can give rise to pseudo-delirious symptoms, such as sleep disturbance (Caraceni and Grassi, 2011).
Moreover, a poor correlation has been shown between the different sets of diagnostic criteria (DSM-IV, ICD-10). In particular, a study (Laurila et al., 2003) reported different delirium prevalence rates in elderly people admitted to hospital or nursing homes, according to the criteria used (24.9% by DSM-IV and 10.1% by ICD-10). These results clearly indicate that too inclusive or too restrictive criteria can cause marked differences in estimated prevalence rates of delirium (Caraceni and Grassi, 2011).
Bearing this controversy in mind, some authors (Watt et al., 2012) go beyond this criticism of delirium in the DSM-IV criteria. These authors have questioned the notion of delirium as reflecting an “altered level of consciousness.” As an alternative, these authors have suggested that delirium reflects the collapse of cognitive operations (attention, working memory, and executive functions), in direct proportion to the severity of any confusional state, and given that these processes are basilar for every other cognitive process, their breakdown compromises the entire cognitive apparatus (Watt et al., 2012). These processes define a base for the cognitive pyramid and are functionally deeply interdigitating, and difficult to neatly separate (Watt and Pincus, 2004). This perspective is not present in the current DSM criteria.
Another limitation is related to the severity of delirium, which is inadequately represented in this classification, as the complete clinical spectrum ranges from very severe deliriums where patients are minimally conscious, to low-grade encephalopathic states in a broad continuum, frequently missed by clinicians (Watt et al., 2012).
So, according to these authors (Watt et al., 2012), delirium might belong to a broader category of diseases of consciousness. They have suggested the following as a rough heuristic, with disorders of consciousness ranging from the most severe to the least severe: Coma; Persistent Vegetative State; Stupor; Akinetic Mutism; Minimally Conscious State; Delirium/Confusional States (Watt and Pincus, 2004). Such taxonomy would provide a continuum, with “gray zones,” or transitional regions demarcating one disorder from the next. This approach would further allow for a continuum of severity in relation to delirium itself, which is currently disregarded in DSM-IV (Watt et al., 2012).
In spite of this, clinical evaluation according to the symptom phenomenology and the nosographic criteria appears as a reference standard for the diagnosis of delirium. In addition, the correct examination of delirious symptoms for epidemiological reasons, research, and clinical purposes is essential and has been reported by many authors (Casarett and Inouye, 2001; Breitbart et al., 2009).
Subsyndromal Delirium
Since the publication of well-established sets of diagnostic criteria, such as the DSM-IV, there has recently emerged a new concept known as subsyndromal delirium (Voyer et al., 2009).
This condition has been defined as the presence of one or more core diagnostic symptoms that do not meet the full criteria for delirium, and where progression to delirium does not occur. The core symptoms were: inattention, altered level of consciousness, disorientation, and perceptual disturbances (Levkoff et al., 1996; Cole et al., 2003).
From a clinical perspective, some authors have suggested an alternative term: “low-grade confusional state.” This emphasizes the need to rate the severity of confusional states – mild, moderate, severe – in opposition to the strict concept of DSM-IV (Watt et al., 2012). As suggested by Voyer et al. (2009), these criteria, when applied very literally, produce underestimation of delirium.
Subsyndromal delirium occurs in 21–76% of hospitalized elderly people (Cole et al., 2008). Prevalence rates of 30–50% have been reported in intensive care units (Ouimet et al., 2007). In long-term care elderly residents, with dementia, the occurrence was 48.4 or 50.3%, depending on the criteria used (Voyer et al., 2009). A recent cohort study has found that 68 of the 104 residents had incident subsyndromal delirium during 6 months of observation. The incidence rate was 5.2 per 100 person-weeks of follow-up (Cole et al., 2011).
The risk factors for subsyndromal delirium are similar to those for classical overt delirium: advanced age, dementia, and severe illness. Moreover, this condition has been associated with poor outcomes, such as a lower cognitive and functional level, increased length of acute care hospital stay, and decreased post-discharge survival at 12 months (Cole et al., 2003).
Thus, patients with subsyndromal delirium require identification and clinical attention in line with management of delirium in order to attain the best outcome (Levkoff et al., 1996).
Clinical Subtypes
Lipowski (1980) was the first author to suggest that delirium can occur in three clinical forms: hyperactive, hypoactive, and mixed, based on psychomotor behavior. This classification is not recognized by DSM-IV or ICD-10 (International Classification of Diseases; WHO, 1992) diagnostic criteria (Lindsay et al., 2002). However several studies have confirmed the existence of this clinical classification (Camus et al., 2000; de Rooij et al., 2005).
In the hyperactive subtype, there is increased psychomotor activity. Patients show features such as hyper-vigilance, restlessness, agitation, aggression, mood lability, and in some cases, hallucinations and delusions (Lipowski, 1980). Behaviors are frequently disruptive (e.g., shouting or resisting, pulling out the IV tubing) or potentially harmful (e.g., pulling out catheters). Because of this, this subtype is the most easily identified (Saxena and Lawley, 2009). Moreover, patients with this form are more likely to be medicated, in particular with benzodiazepines and neuroleptics (Caraceni and Grassi, 2011).
In contrast, the hypoactive form is characterized by decreased psychomotor activity, with the presence of lethargy and drowsiness, apathy, and confusion. Patients become withdrawn, answering slowly to questions and without spontaneity. Sometimes patients can also appear to be sedated (NICE, 2010). This is the most common subtype of delirium in elderly people (Meagher et al., 2011). In a recent study (Khurana et al., 2011) with hospitalized elderly delirious patients, a high prevalence of hypoactive delirium was found (65%), when compared to the other forms. However, due to the absence of disruptive and injurious behaviors, this subtype can be more difficult to recognize by clinicians (NICE, 2010; Mittal et al., 2011).
In mixed delirium, patients have symptoms of both the subtypes mentioned above (Liptzin and Levkoff, 1992). It has been reported to be the most common type.
Different patterns have been suggested for these three different forms of delirium. Dissimilar underlying pathogenetic pathways will determine different management, course, prognosis, and outcomes (Meagher et al., 2000; de Rooij et al., 2005; Fong et al., 2009a).
Unfortunately, the literature is inconsistent about which subtype has the worse prognosis. However, some authors have suggested there is evidence that the hypoactive form is associated with a relatively poorer prognosis (Yang et al., 2009) and in a recent longitudinal study (Meagher et al., 2011), the patients with this subtype have been significantly more likely to die within 1 month of study entry.
Diagnosis
Delirium is frequently under-recognized and often misdiagnosed by health professionals. Between a third and two-thirds of delirium cases go unrecognized (Siddiqi et al., 2006). A recent study (Han et al., 2009) in an emergency department concluded that the emergency physicians missed delirium in 76% of the cases.
This under-recognition has been associated with factors such as the fluctuating nature of delirium, its overlap with dementia and depression, the scarcity of formal cognitive assessment in general hospitals by routine, under-appreciation of its clinical consequences, and failure to consider the diagnostic importance (CCSMH, 2006; Inouye, 2006; Philpot, 2011). Non-detection of delirium has been also associated with the high prevalence of the hypoactive form of delirium (Armstrong et al., 1997). Four independent risk factors for the under-recognition of delirium by nurses have been identified: hypoactive delirium, advanced age, vision impairment, and dementia (Inouye et al., 2001).
A recent survey of trainee physicians in the UK revealed a lack of basic knowledge about the diagnosis and management of delirium, although they appeared to be aware of its high prevalence in hospitals as well as its potential clinical significance (David and MacLullich, 2009).
The diagnosis of delirium remains primarily clinical, without specific diagnostic tests (Young and Inouye, 2007). In this way, it is made on the basis of clinical history, behavioral observation of key features, and comprehensive physical and cognitive assessment (Fearing and Inouye, 2009; Fong et al., 2009a). In this context, understanding and considering its clinical features is crucial for a correct diagnosis (Inouye, 2006).
Taking into account the acute onset and fluctuating course of delirium, it is important to establish the patient’s level of baseline cognitive functioning and the course of cognitive change. In this way, the diagnosis is made more easily if there has been a prior assessment of cognitive abilities. In other instances it is necessary, in a clinical interview, to obtain information from the family members/caregivers and/or medical and nursing staff (Cole, 2005; Fearing and Inouye, 2009). Moreover, patients should be assessed more than once during the day, in order to detect a possible fluctuating path of symptoms.
Inattention is another central feature of delirium. The cognitive assessment should include not only global cognitive screening tools (e.g., Mini-Mental State Examination – MMSE; Folstein et al., 1975), but also a measurement of attention (Fearing and Inouye, 2009). There are quick screening instruments for inattention that are commonly used: Digit Span Test (Wechsler, 1997) and Trail Making Test A (Reitan, 1958). In this context, it is also important to note that changes in arousal can affect performance in attention tests as can other conditions, such as fatigue. Moreover, depending on the severity of delirium, cognitive tasks can be affected proportionally to attention demands required by the task (Oyebode, 2008).
The level of consciousness is another important aspect of this evaluation that has to be determined. The Glasgow Coma Scale (Teasdale and Jennett, 1974) has been classically used to quantify this level of consciousness.
According to the most recent international guidelines (NICE, 2010), all elderly people admitted to hospital or in long-term care units should be screened for risk factors of developing delirium and cognitive impairment, using a brief cognitive test (e.g., MMSE). If recent changes or fluctuations in cognitive function, perception, physical function, or in social behavior are identified in people at risk, a clinical assessment should be carried out based on the DSM-IV criteria or short Confusion Assessment Method – CAM (Inouye et al., 1990), CAM (algorithm) to confirm the diagnosis. This evaluation should also be carried out by a trained healthcare professional.
The CAM is a widely used delirium screening instrument, based on DSM-III-R criteria (APA, 1987). It can be readily used in routine clinical settings by non-psychiatric medical or nursing staff with some previous training (Wei et al., 2008). The short version includes a diagnostic algorithm, based on four cardinal features of delirium: (1) acute onset and fluctuating course; (2) inattention; (3) disorganized thinking; and (4) altered level of consciousness. A diagnosis of delirium according to the CAM requires the presence of features 1, 2, and either 3 or 4. In critical care or in the recovery room after surgery, in particular in patients who are not able to communicate verbally, CAM-ICU (Ely et al., 2001), an adaptation derived from CAM, should be used (Luetz et al., 2010; NICE, 2010). Recent review studies (Adamis et al., 2010; Wong et al., 2010) corroborated this recommendation, citing evidence to support the use of CAM as a diagnostic instrument. The use of the Delirium Rating Scale-R-98 – DRS-R-98 (Trzepacz et al., 2001) has also been suggested as a measure of delirium symptom severity in effective assessment. This scale includes three diagnostic items (onset, fluctuation of symptoms, physical disorder) and 13 severity items (sleep-wake cycle, perceptual disturbances/hallucinations, delusions, lability of affect, language, thought process abnormalities, motor agitation, motor retardation, orientation, attention, short-term memory, long-term memory, visuospatial ability). A high score is indicative of greater severity.
The identification of underlying causes is crucial in delirium diagnosis (Marcantonio, 2011). Because of that, physical and neurological examinations are extremely important, helping to rule out infectious, metabolic, endocrine, cardiovascular, and cerebrovascular diseases (Fong et al., 2009a).
The diagnostic approach should include the following tests: complete blood count, blood urea and creatinine levels, electrolytes, blood sugar, C-reactive protein, liver function, and thyroid function (Cole, 2004; Saxena and Lawley, 2009).
It is also important to identify medication and substance usage, namely alcohol or benzodiazepines use, which can contribute to this ailment (Inouye, 2006).
The physical examination should also include the evaluation of vital signs, with oxygen saturation. The general examination should focus on cardiac and pulmonary function. Beyond this, a neurological examination should incorporate the mental status, as well as focal findings (Marcantonio, 2011).
No laboratory test, brain imaging or other tests are more accurate than clinical assessment (Inouye, 2006). However, they can be useful to identify possible causes of delirium and correctable contributing factors. In some situations, brain imaging and electroencephalography (EEG) can be useful, when there is strong evidence of an intracranial cause, based on clinical assessment (e.g., change in mental status after a blow to the head) or if focal neurological signs or seizure activity is detected during physical examination (Hirano et al., 2006; Saxena and Lawley, 2009).
Differential Diagnosis
Delirium is frequently confused with dementia (Table 1). Globally, dementia is characterized by cognitive and functional impairment and usually follows a chronic deteriorating course, whereas delirium is characterized primarily by inattention and has an acute onset with a fluctuating course (Meagher et al., 2006). Also, an abnormal level of consciousness is highly suggestive of delirium, while in dementia attention and the level of consciousness tend to remain intact (Fearing and Inouye, 2009; Marcantonio, 2011), at least until late stages, or in the case of Dementia with Lewy Bodies (DLB; McKeith et al., 2005).
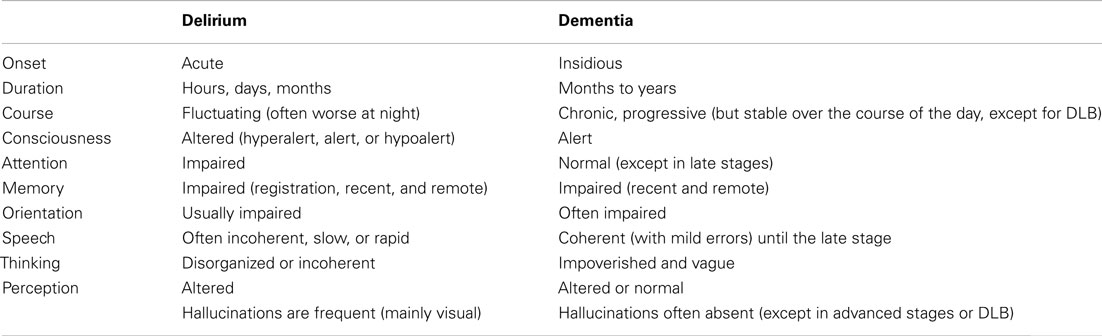
Table 1. Differential diagnoses of delirium and dementia.
Additionally, physical illness or drug toxicity can alone or together be present in delirium, whereas it is often absent in Alzheimer’s disease (Saxena and Lawley, 2009).
Although delirium and dementia are often separated clinically and methodologically, these conditions often occur together, with prevalence ranges from 22 to 89% in both hospital and community settings. These clinical situations are also probably highly interrelated, specifically because both share many pathophysiological features (Fick et al., 2002, 2009).
Delirium complicates 24–89% of inpatient stays for elderly patients with dementia (Sampson et al., 2009). Inversely, the available evidence strongly suggests that delirium increases the risk of new-onset dementia in the long-term, as much as sixfold at 3 year follow-up (MacLullich et al., 2009). Also, people with pre-existing dementia suffer from an acceleration of cognitive decline following an episode of delirium (Fong et al., 2009b).
However, distinguishing delirium and dementia becomes crucial because the diagnosis of delirium is urgent, as it can be the first indicator of a serious medical problem (Wahlund and Bjorlin, 1999), which can be treatable, and because it has been associated with poor outcomes (Siddiqi et al., 2006).
Differential diagnosis with DLB can also be difficult. In both clinical situations, there is a fluctuating course, altered level of consciousness, as well as visual hallucinations. However, this type of dementia has a longer duration (months or years) and parkinsonian symptoms are common (McKeith et al., 2005). Besides, visual hallucinations are more complex and persistent in DLB than in delirium (Cole, 2005).
Depression may also be mistaken for the hypoactive form of delirium, due to the presence of symptoms such as slowed thinking, decreased concentration, and memory impairment. However, the presentation of depression tends to be insidious, without fluctuations and the level of consciousness remains unaffected. Moreover, there is usually a history of previous episodes, and a predominance of mood symptoms (Cole, 2005; Saxena and Lawley, 2009).
Other less common situations should also be considered, such as mania and schizophrenia (Saxena and Lawley, 2009). In the first case, it can be confused with the hyperactive form of delirium, with reduced attention, agitation, and rapid fluctuations. However, in this situation there are usually previous episodes of euphoria/mania (Cole, 2005).
In the second case, disturbance of thought can be also present in both. However, in delirium, these alterations fluctuate and are often fragmentary and less complex. Thought insertion, very common in schizophrenia, is unusual in delirium. On the other hand, schizophrenic delusions are very systematized, bizarre, and not influenced by the environment, which contrasts with the poor systematization and environmental influence observed in delirium (Cole, 2005).
Perception is also affected in schizophrenia, with hallucinations. They are persistent, consistent, and usually auditory, as opposed to those occurring in delirium, which are predominantly visual (Saxena and Lawley, 2009).
Pathophysiology
The pathophysiological mechanisms of delirium remain unclear (Gofton, 2011). However, current evidence suggests that disruption of neurotransmission can contribute to the development of this disorder (Saxena and Lawley, 2009).
The neurotransmitter hypothesis suggests that cholinergic deficits and dopaminergic excess could be involved in the development of delirium (Trzepacz, 2000; Gaudreau and Gagnon, 2005). Indeed, the cholinergic system has an important role in cognition and attention (Hshieh et al., 2008), so its impact in the development of delirium is not surprising. Moreover, drugs with anticholinergic properties may precipitate delirium, in susceptible individuals (Trzepacz, 1996). There is also strong evidence supporting the importance of the role of cholinergic deficits in the development of this condition (Gofton, 2011).
Another important neurotransmitter that could be involved in delirium is dopamine, since delirium can be a common side effect of the dopaminergic drugs used in the treatment of Parkinson’s disease (Trzepacz and van der Mast, 2002). This neurotransmitter has been related to psychotic symptoms (Ramirez-Bermudez et al., 2008), which can reinforce the function of these symptoms in delirium, if not the whole syndrome (Hall et al., 2011). Furthermore, dopamine also has an important role in motor activity, as well as, cognitive functions, such as attention, thought, and perception (Trzepacz, 2000), which are affected in this clinical condition.
Inflammation or acute stress responses are less supported pathophysiological mechanisms (Fong et al., 2009a). The first has been inferred from basic and clinical research literature evidence, supporting the hypothesis that trauma and infection or surgery can lead to increased production of cytokines (Rudolph et al., 2008; Cerejeira et al., 2010). This mechanism may induce delirium in susceptible patients (Maclullich et al., 2008). Furthermore, a recent review concluded that this increase in cytokines plays a crucial role, specifically in the development of cognitive dysfunction, observed in delirium (van Munster et al., 2008; Simone and Tan, 2011).
On the other hand, a recent prospective study (Cerejeira et al., 2011) stated that elective hip-replacement surgery induced a reduction of plasma activity of cholinesterases (acetylcholinesterase – AChE and butyrylcholinesterases – BuChE) and found lower preoperative activity levels of plasma cholinesterases in subjects who developed delirium postoperatively.
Another hypothesis is related to cortisol, a hormone of the hypothalamic-pituitary-adrenal axis, which is part of the body’s major response to stressful or traumatic insults (Olsson, 1999). Aging and dementia have been connected with an increase and duration of cortisol response to stress (MacLullich et al., 2008). This could explain why high levels of this hormone associated with acute stress have been hypothesized to precipitate and/or sustain delirium (Trzepacz and van der Mast, 2002).
Some authors (Watt et al., 2012) have suggested a simple heuristic that all etiologies for delirium emerge due to the deleterious effect of insults on neural networks supporting large-scale and highly integrative global cognitive processes involved in attention, working memory, and executive functions, which depend on the functional integrity of cortical prefrontal and parietal networks, as well as specific subcortical structures, such as the basal ganglia, cerebellum, thalamic nuclei, and the reticular activating system.
According to these authors, “a true understanding of delirium cannot emerge through simply focusing on single molecules, however important those particular transmitter systems may be, but can only come from focusing on the large-scale networks that underlie organized behavior and thought” (Watt et al., 2012).
Risk Factors
The etiology of delirium is usually multifactorial. However, it can be caused by a single factor, such as alcohol withdrawal or substance abuse (Burns et al., 2004; Fearing and Inouye, 2009).
Research has identified several consistent risk factors for delirium, which are classified into two groups: predisposing and precipitating factors. The first one makes the elderly person more vulnerable to the development of delirium and the second comprises acute factors for triggering delirium (CCSMH, 2006). A combination of these predisposing and precipitating factors appears to be the rule rather than an exception in delirious elderly people (Inouye, 1999; Rolfson, 2002).
The most common predisposing factors are: advanced age, male gender, pre-existing dementia and depression, visual and hearing impairment, functional dependence, dehydration and malnutrition, polymedication (mainly psychoactive drugs), alcohol abuse and coexistence of multiple, and severe medical conditions (Saxena and Lawley, 2009).
Next to increasing age, dementia appears as the second most frequent risk factor for delirium (Burns et al., 2004; Cole, 2004; CCSMH, 2006; Inouye, 2006). According to Inouye (2006), the underlying vulnerability of the brain in patients with dementia may predispose them to the development of delirium, as a consequence of insults related to the acute medical disease, medication, as well as environmental factors.
According to Saxena and Lawley (2009), the most common precipitating factors are: intercurrent illnesses (e.g., infections), iatrogenic complications, metabolic derangements, primary neurological conditions (e.g., acute stroke), surgery, drugs (particularly benzodiazepines, narcotic analgesics, and drugs with anticholinergic effects (Han et al., 2001). Uncontrolled pain has also been associated with the development of delirium.
Environmental factors, such as admission to an ICU, use of physical restraints or bladder catheterization have also been implicated (Brauer et al., 2000; Rolfson, 2002; Cole, 2004; Fong et al., 2009a; Saxena and Lawley, 2009).
In this context, Inouye and Charpentier (1996) present a model to predict the development of delirium in elderly hospitalized patients, with a greater number of or more severe predisposing factors (use of physical restraints, malnutrition, more than three medications in the previous day, use of a bladder catheter, and any iatrogenic event), in association to few precipitating factors. This model has been considered an excellent framework for identification of various etiologies of delirium in old age (Rolfson, 2002).
More recently, the guidelines (NICE, 2010) recommend the identification, in elderly people admitted to hospital or in long-term care, of the following risk factors: age 65 years old or over, cognitive impairment (past or present), dementia or both, current hip fracture, and presence of a severe illness. This identification brings the opportunity to change the risk factors for the development of delirium.
Prognosis
Delirium in both medical and surgical elderly hospitalized patients has been associated with multiple adverse outcomes that have been well documented (NICE, 2010).
Overall, delirium has been associated with the increase of hospital stay (Cole and Primeau, 1993; Dubois et al., 2001; McCusker et al., 2003; Koster et al., 2011; van den Boogaard et al., 2011; Shi et al., 2012), cognitive decline (Inouye et al., 1998; McCusker et al., 2001; Jackson et al., 2004; Fong et al., 2009b; Witlox et al., 2010), functional decline (Inouye et al., 1998; Marcantonio et al., 2000; McCusker et al., 2001, 2002a), institutionalization (Cole and Primeau, 1993; Inouye et al., 1998; Witlox et al., 2010), and mortality (Cole and Primeau, 1993; Cole et al. 2008; Inouye et al., 1998; McCusker et al., 2002b; Witlox et al., 2010; Koster et al., 2011; Shi et al., 2012).
In intensive care units, delirium has been shown to be associated with prolonged duration of mechanical ventilation (van den Boogaard et al., 2011), longer stay in hospital, and in the ICU (Dubois et al., 2001; van den Boogaard et al., 2011) as well as mortality during hospitalization (van den Boogaard et al., 2011).
A systematic review (Siddiqi et al., 2006), with medical elderly in patients, concluded that this condition had been related to an increase of mortality (discharge/12 months), length of hospital stay, and institutionalization.
More recently, a meta-analysis (Witlox et al., 2010) confirms that delirium is associated with the increased risk of dementia, institutionalization, and mortality, independently of important confounder factors (age, gender, comorbidity, severity of illness, and baseline dementia).
Fong et al. (2009b) demonstrate that incident delirium accelerates the trajectory of cognitive decline in hospitalized elderly patients with Alzheimer’s disease.
Although traditionally viewing delirium as a transient and reversible condition, some studies have found evidence that a significant proportion of patients do not recover from delirium, presenting persistent symptoms at time of discharge, or beyond (Levkoff et al., 1992; Murray et al., 1993; McCusker et al., 2002b; Siddiqi et al., 2006; Cole et al., 2009). According to Cole et al. (2009), this situation, called persistent delirium, may contribute to the poor prognosis of delirium. These patients have worse outcomes (mortality, nursing home placement, function, and cognition), when compared with patients who have recovered from delirium (Cole et al., 2009; Cole 2010). In a recent systematic review (Dasgupta and Hillier, 2010) persistent delirium was associated with dementia, medical conditions, severity of delirium, hypoactive symptoms, and hypoxic illness.
Prevention
Due to the adverse outcomes and increased health care costs that accompany delirium, the interventions to prevent this condition become crucial for reducing its frequency and complications (Inouye, 2006). In fact, one-third of delirium episodes could be prevented (Inouye, 2006; Marcantonio, 2011). Beyond that, the most recent guidelines (NICE, 2010) have considered delirium prevention as a cost-effective strategy. These provide a quick reference guide for preventing delirium in elderly people at risk, based on a multicomponent and non-pharmacological intervention that addresses a number of modifiable risk factors. First of all, people at risk of developing delirium (advanced age, suffering from cognitive impairment/dementia, hip fracture, or severe illness) should be assessed within 24 h of admission. In this case, the following 10 precipitating factor groups should be taken into consideration: cognitive impairment and disorientation, dehydration, and constipation, hypoxia, immobility/limited mobility, infection, polymedication, pain, poor nutrition, sensory impairment, and sleep disturbance. Based on this assessment, a trained and multidisciplinary team should provide a multicomponent intervention, taking into account the needs of the person, as well as the clinical care setting.
The success of a multidisciplinary and multicomponent approach in prevention of delirium springs from the many causes in the origin of this condition (Inouye, 2006; Fearing and Inouye, 2009; Salawu et al., 2009).
One of the most important examples of this kind of intervention was the Hospital Elder Life Program – HELP (Inouye et al., 1999, 2006), which was widely implemented (Marcantonio, 2011).
This intervention was carried out by a skilled interdisciplinary team and trained volunteers with standardized protocols for a personalized management of six risk factors (cognitive impairment, sleep deprivation, immobility, visual and hearing impairment, and dehydration). The effectiveness of this intervention decreased the incidence of delirium in 40% of cases and resulted in significantly fewer days and episodes of delirium.
On the other hand, educational programs targeting health professionals have been used alone or as part of multicomponent interventions, which seems to be crucial for a more appropriate management of patients with delirium (CCSMH, 2006), from the primary care level.
In regard to this, Naughton et al. (2005) have studied the effectiveness of multifactorial intervention designed to reduce delirium and hospital stay in elderly patients, carried out among a group of physicians and nurses from an emergency department and an acute geriatric unit. This intervention was shown to contribute to a decrease in psychotropic medication prescription (benzodiazepine and antihistamine), delirium prevalence, and hospital stay.
In another study (Tabet et al., 2005), an educational program for medical and nursing staff on an acute medical ward also contributed to a reduction in delirium prevalence in an intervention group, compared with a control group. Staff members were also more likely to correctly recognize this clinical condition.
In this context, a recent review (Teodorczuk et al., 2010) concluded that the majority of educational interventions focused on delirium prevention and management were shown to be effective in various healthcare settings. Moreover, this study also recognized that these programs should be carried out by a Liaison Old Age Psychiatry team, in particular in a hospital setting. This has been shown to be effective, with an improvement in key outcomes (Slaets et al., 1997).
Management
Once delirium occurs, non-pharmacological interventions should be considered as the first-line of delirium management (Cole, 2004; Fong et al., 2009a; Aguirre, 2010). This approach should address all evident causes, providing supportive care and preventing complications and treating behavioral problems (Inouye, 2006).
As delirium is a medical emergency and requires urgent intervention, the management of this condition must focus initially on identification and monitoring of underlying causes (CCSMH, 2006; NICE, 2010).
Supportive care remains as another important non-pharmacological strategy (Young and Inouye, 2007). This includes close and continuing observation and care from nursing staff, which should include vital sign monitoring, protecting the patient’s airway, ensuring nutrition, correction and prevention of dehydration, attention to oral intake, prevention of aspiration, encouragement of mobility, and ensuring a good sleep pattern. In this context, it is also essential to support the patient’s daily care and encourage self-care (Meagher et al., 1996; Cole, 2005; BGS, 2006; Inouye, 2006; Young and Inouye, 2007; Fearing and Inouye, 2009). The use of physical restraint is always questionable, but may be necessary to control violent behavior or to prevent the removal of important devices, such as endotracheal tubes (Marcantonio, 2011). However, it should be avoided, because it has been associated with worsening agitation and injury, prolonged delirium, and increased complications (Inouye, 2006; Young and Inouye, 2007).
Another important factor for the effective management of delirium is the involvement of the family and caregivers by health professionals. They can help re-orientate, calm, assist, protect, and support older people. Furthermore, they can also facilitate effective communication (CCSMH, 2006; NICE, 2010; Marcantonio, 2011). Medical and nursing staff, as well as families, should know the importance of effective communication in these situations. This can include strategies such as frequent verbal reorientation, clear instructions, and eye contact (Fearing and Inouye, 2009).
Delirium can be a psychologically traumatic experience, not only for the patients, but also for their family or caregivers (Breitbart et al., 2002). In this way, providing support and information can help throughout this process, as well as encouraging people to share their experiences (Inouye, 2006).
The education of families and caregivers by health professionals about delirium, in particular about its symptoms (especially disinhibition, agitation, hallucinations, and delusions) becomes crucial (CCSMH, 2006). It is also important to explain the fluctuating course, explaining that the transitory phases of awareness do not necessarily mean a recovery, because symptoms can recur. The possible causes of delirium, a possible relation with Alzheimer’s disease or dementia, as well as treatment options should also be clearly explained. In fact, this specific intervention can be extremely important to the family, contributing not only to an improvement of their involvement in the management of delirium, but also to alleviate the profound sense of helplessness, incredulity, and anxiety that these members can feel during an episode of delirium (Gagnon et al., 2002).
Environmental manipulation is also recommended as an integral part of delirium management (NICE, 2010). It may include the following strategies: ensuring that there is a clock and a calendar in the room; giving the older person frequent verbal reminders of the time, day, and place; avoiding medical/nursing staff changes; transferring the patient to an isolated room, if possible; obtaining familiar possessions from home (e.g., family picture); avoiding sensory deprivation (e.g., windowless room) or sensory overload (e.g., too much noise); minimizing sensory impairment (including vision and hearing loss) by the use of corrective devices.
Pharmacological interventions in delirium should be considered only in the management of behavioral symptoms, but not for the basic treatment of this condition (Flaherty et al., 2011). They can be useful in situations of severe agitation, which interfere with medical procedures or when the patient puts himself or others, at risk and when non-pharmacological interventions fail (Inouye, 2006; NICE, 2010; Rathier and Baker, 2011).
In this context, the most recent guidelines (NICE, 2010) recommend the administration of haloperidol or olanzapine, only for a short period of time (for a maximum of 1 week or less), starting with low doses and titrating carefully, according to symptom severity.
In spite of this, the U.S. Food and Drug Administration has not yet approved any of these agents for the treatment of delirium (Flaherty et al., 2011).
With the use of antipsychotics one always has to take into consideration one of the most adverse effects of this high-potency medication: akathisia (motor restlessness), which can be confused with worsening of delirium (Marcantonio, 2011), or even being worse it in reality (Francis, 1992; Inouye et al., 2011). Recent evidence indicates that the use of antipsychotics is not safe in elderly patients, especially in those with dementia. Concerns include the development of adverse vascular events and death (Mittal et al., 2011).
On the other hand, the administration of antipsychotics should be avoided in Parkinson’s disease or DLB (NICE, 2010).
Benzodiazepines have also been recommended, but only in delirium due to alcohol and benzodiazepine withdrawal, or neuroleptic malignant syndrome (Lonergan et al., 2009).
The introduction of cholinesterase inhibitors for the treatment of dementia suggested their potential usefulness to improve symptoms of delirium (Caraceni and Grassi, 2011). However, there is no specific evidence from controlled trials that donepezil or rivastigmine are effective in the treatment of this medical condition (Overshott et al., 2008; Gamberini et al., 2009).
The plan of discharge from hospital should be handled carefully, involving the team of health professionals and the patient, as well as the family (Saxena and Lawley, 2009). In addition, as symptoms of delirium can persist (Cole, 2010), a close clinical follow-up after discharge is crucial, especially due to the poor outcomes associated with this situation (BGS, 2006; Inouye, 2006). This could help identify residual cognitive, social, or functional problems, modify risk factors and help to reduce the recurrence of an episode of delirium (Saxena and Lawley, 2009).
Conclusion
Delirium is a common neuropsychiatric syndrome, mainly in elderly hospitalized patients. Despite this, it is frequently under-recognized by health professionals, due to its fluctuating nature, its overlap with dementia and the scarcity of formal cognitive assessment in general hospitals by routine. Once manifested, delirium is associated with increased morbidity and mortality. For that reason, prevention based on risk factor identification, early recognition, as well as an effective management, particularly if based on non-pharmacological strategies, is essential, because of the prevalence and the adverse outcomes associated with this disorder.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The present work was supported by FCT (Foundation for Science and Technology) Ph.D. fellowships (SFRH/BD/63154/2009 – S. Martins).
References
Adamis, D., Sharma, N., Whelan, P. J., and Macdonald, A. J. (2010). Delirium scales: a review of current evidence. Aging Ment. Health 14, 543–555.
Adamis, D., Treloar, A., Martin, F. C., and Macdonald, A. J. (2007). A brief review of the history of delirium as a mental disorder. Hist. Psychiatry 18(72 Pt 4), 459–469.
Aguirre, E. (2010). Delirium and hospitalized older adults: a review of nonpharmacologic treatment. J. Contin. Educ. Nurs. 41, 151–152.
APA. (1980). Diagnostic and Statistical Manual of Mental Disorders DSM-III Third Edition. Washington, DC: American Psychiatric Association.
APA. (1987). Diagnostic and Statistical Manual of Mental Disorders DSM-III-TR Third Edition (Text Revision). Washington, DC: American Psychiatric Association.
APA. (2000). Diagnostic and Statistical Manual of Mental Disorders DSM- IV-TR Fourth Edition (Text Revision). Washington, DC: American Psychiatric Association.
Armstrong, S. C., Cozza, K. L., and Watanabe, K. S. (1997). The misdiagnosis of delirium. Psychosomatics 38, 433–439.
Bachman, D., and Rabins, P. (2006). “Sundowning” and other temporally associated agitation states in dementia patients. Annu. Rev. Med. 57, 499–511.
BGS. (2006). Clinical Guidelines for the Prevention, Diagnosis and Management of Delirium in Older People in Hospital. British Geriatric Society. Available at: http://www.bgs.org.uk/Publications/Clinical%20Guidelines/clinical_1-2_fulldelirium.htm
Brauer, C., Morrison, R. S., Silberzweig, S. B., and Siu, A. L. (2000). The cause of delirium in patients with hip fracture. Arch. Intern. Med. 160, 1856–1860.
Breitbart, W., Gibson, C., and Tremblay, A. (2002). The delirium experience: delirium recall and delirium-related distress in hospitalized patients with cancer, their spouses/caregivers, and their nurses. Psychosomatics 43, 183–194.
Breitbart, W., Lawlor, P., and Friedlander, M. (2009). “Delirium in the terminally ill,” in Handbook of Psychiatry in Palliative Medicine, eds H. M. Chohinov and W. Breitbart (New York: Oxford University Press), 81–100.
Burns, A., Gallagley, A., and Byrne, J. (2004). Delirium. J. Neurol. Neurosurg. Psychiatr. 75, 362–367.
Camus, V., Burtin, B., Simeone, I., Schwed, P., Gonthier, R., and Dubos, G. (2000). Factor analysis supports the evidence of existing hyperactive and hypoactive subtypes of delirium. Int. J. Geriatr. Psychiatry 15, 313–316.
Caraceni, A., and Grassi, L. (2011). Delirium. Acute Confusional States in Palliative Medicine, 2nd Edn. Oxford: Oxford University Press.
Casarett, D. J., and Inouye, S. K. (2001). Diagnosis and management of delirium near the end of life. Ann. Intern. Med. 135, 32–40.
CCSMH. (2006). National Guidelines for Seniors Mental Health – The Assessment and Treatment of Delirium. Toronto: Canadian Coalition for Seniors Mental Health.
Cerejeira, J., Batista, P., Nogueira, V., Firmino, H., Vaz-Serra, A., and Mukaetova-Ladinska, E. B. (2011). Low preoperative plasma cholinesterase activity as a risk marker of postoperative delirium in elderly patients. Age Ageing 40, 621–626.
Cerejeira, J., Firmino, H., Vaz-Serra, A., and Mukaetova-Ladinska, E. B. (2010). Theneuroinflammatoryhypothesis of delirium. Acta Neuropathol. 119, 737–754.
Cole, M., McCusker, J., Dendukuri, N., and Han, L. (2003). The prognostic significance of subsyndromal delirium in elderly medical inpatients. J. Am. Geriatr. Soc. 51, 754–760.
Cole, M. G. (2010). Persistent delirium in older hospital patients. Curr. Opin. Psychiatry 23, 250–254.
Cole, M. G., Ciampi, A., Belzile, E., and Zhong, L. (2009). Persistent delirium in older hospital patients: a systematic review of frequency and prognosis. Age Ageing 38, 19–26.
Cole, M. G., McCusker, J., Voyer, P., Monette, J., Champoux, N., Ciampi, A., Vu, M., and Belzile, E. (2011). Subsyndromal delirium in older long-term care residents: incidence, risk factors, and outcomes. J. Am. Geriatr. Soc. 59, 1829–1836.
Cole, M. G., and Primeau, F. J. (1993). Prognosis of delirium in elderly hospital patients. CMAJ 149, 41–46.
Cole, M. G., You, Y., McCusker, J., Ciampi, A., and Belzile, E. (2008). The 6 and 12 month outcomes of older medical inpatients who recover from delirium. Int. J. Geriatr. Psychiatry 23, 301–307.
Dasgupta, M., and Hillier, L. M. (2010). Factors associated with prolonged delirium: a systematic review. Int. Psychogeriatr. 22, 373–394.
David, D., and MacLullich, A. (2009). Understanding barriers to delirium care: a multicentre survey of knowledge and attitudes amongst UK junior doctors. Age Ageing 38, 559–563.
de Rooij, S. E., Schuurmans, M. J., van der Mast, R. C., and Levi, M. (2005). Clinical subtypes of delirium and their relevance for daily clinical practice: a systematic review. Int. J. Geriatr. Psychiatry 20, 609–615.
Dubois, M. J., Bergeron, N., Dumont, M., Dial, S., and Skrobik, Y. (2001). Delirium in an intensive care unit: a study of risk factors. Intensive Care Med. 27, 1297–1304.
Elie, M., Rousseau, F., Cole, M., Primeau, F., McCusker, J., and Bellavance, F. (2000). Prevalence and detection of delirium in elderly emergency department patients. CMAJ 163, 977–981.
Ely, E. W., Margolin, R., Francis, J., May, L., Truman, B., Dittus, R., Speroff, T., Gautam, S., Bernard, G. R., and Inouye, S. K. (2001). Evaluation of delirium in critically ill patients: validation of the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Crit. Care Med. 29, 1370–1379. doi:10.1016/j.ijnurstu.2011.11.016
Fick, D. M., Agostini, J. V., and Inouye, S. K. (2002). Delirium superimposed on dementia: a systematic review. J. Am. Geriatr. Soc. 50, 1723–1732.
Fick, D. M., Kolanowski, A., Beattie, E., and McCrow, J. (2009). Delirium in early-stage Alzheimer’s disease: enhancing cognitive reserve as a possible preventive measure. J. Gerontol. Nurs. 35, 30–38.
Flaherty, J. H., Gonzales, J. P., and Dong, B. (2011). Antipsychotics in the treatment of delirium in older hospitalized adults: a systematic review. J. Am. Geriatr. Soc. 59(Suppl. 2), S269–S276.
Folstein, M. F., Folstein, S. E., and McHugh, P. R. (1975). Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198.
Fong, T. G., Tulebaev, S. R., and Inouye, S. K. (2009a). Delirium in elderly adults: diagnosis, prevention and treatment. Nat. Rev. Neurol. 5, 210–220.
Fong, T. G., Jones, R. N., Shi, P., Marcantonio, E. R., Yap, L., Rudolph, J. L., Yang, F. M., Kiely, D. K., and Inouye, S. K. (2009b). Delirium accelerates cognitive decline in Alzheimer disease. Neurology 72, 1570–1575.
Francis, J., and Young, G. B. (2011). Diagnosis of Delirium and Confusional States, UptoDate Edition. Available at: www.uptodate.com
Gagnon, P., Charbonneau, C., Allard, P., Soulard, C., Dumont, S., and Fillion, L. (2002). Delirium in advanced cancer: a psychoeducational intervention for family caregivers. J. Palliat. Care 18, 253–261.
Gamberini, M., Bolliger, D., LuratiBuse, G. A., Burkhart, C. S., Grapow, M., Gagneux, A., Filipovic, M., Seeberger, M. D., Pargger, H., Siegemund, M., Carrel, T., Seiler, W. O., Berres, M., Strebel, S. P., Monsch, A. U., and Steiner, L. A. (2009). Rivastigmine for the prevention of postoperative delirium in elderly patients undergoing elective cardiac surgery-a randomized controlled trial. Crit. Care Med. 37, 1762–1768.
Gaudreau, J. D., and Gagnon, P. (2005). Psychotogenic drugs and delirium pathogenesis: the central role of the thalamus. Med. Hypotheses 64, 471–475.
Gill, D., and Mayou, R. (2000). “Delirium,” in The New Oxford Textbook of Psychiatry, eds M. G. Gelder, J. J. Jr. López-Ibor and N. C. Andreasen (Oxford: Oxford University Press), 382–387.
Guenther, U., and Radtke, F. M. (2011). Delirium in the postanaesthesia period. Curr. Opin. Anaesthesiol. 24, 670–675.
Hall, R. J., Shenkin, S. D., and Maclullich, A. M. (2011). A systematic literature review of cerebrospinal fluid biomarkers in delirium. Dement. Geriatr. Cogn. Disord. 32, 79–93.
Han, J. H., Zimmerman, E. E., Cutler, N., Schnelle, J., Morandi, A., Dittus, R. S., Storrow, A. B., and Ely, E. W. (2009). Delirium in older emergency department patients: recognition, risk factors, and psychomotor subtypes. Acad. Emerg. Med. 16, 193–200.
Han, L., McCusker, J., Cole, M., Abrahamowicz, M., Primeau, F., and Elie, M. (2001). Use of medications with anticholinergic effect predicts clinical severity of delirium symptoms in older medical inpatients. Arch. Intern. Med. 161, 1099–1105.
Hirano, L. A., Bogardus, S. T. Jr., Saluja, S., Leo-Summers, L., and Inouye, S. K. (2006). Clinical yield of computed tomography brain scans in older general medical patients. J. Am. Geriatr. Soc. 54, 587–592.
Hshieh, T. T., Fong, T. G., Marcantonio, E. R., and Inouye, S. K. (2008). Cholinergic deficiency hypothesis in delirium: a synthesis of current evidence. J. Gerontol. A Biol. Sci. Med. Sci. 63, 764–772.
Inouye, S. K. (1999). Predisposing and precipitating factors for delirium in hospitalized older patients. Dement. Geriatr. Cogn. Disord. 10, 393–400.
Inouye, S. K. (2003). The Confusion Assessment Method (CAM): Training Manual and Coding Guide. New Haven: Yale University School of Medicine.
Inouye, S. K., Baker, D. I., Fugal, P., and Bradley, E. H. (2006). Dissemination of the hospital elder life program: implementation, adaptation, and successes. J. Am. Geriatr. Soc. 54, 1492–1499.
Inouye, S. K., Bogardus, S. T. Jr., Charpentier, P. A., Leo-Summers, L., Acampora, D., Holford, T. R., and Cooney, L. M. Jr. (1999). A multicomponent intervention to prevent delirium in hospitalized older patients. N. Engl. J. Med. 340, 669–676.
Inouye, S. K., and Charpentier, P. A. (1996). Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA 275, 852–857.
Inouye, S. K., Fearing, M. A., and Marcantonio, R. A. (2011). “Delirium,” in Hazzard’s Geriatric Medicine and Gerontology, Chap. 53, eds J. B. Halter, J. G. Ouslader, M. E. Tinetti, S. Studenski, K. P. High and S. Asthana. Available at: http://accessmedicine.com/content.aspx?aid = 5119453
Inouye, S. K., Foreman, M. D., Mion, L. C., Katz, K. H., and Cooney, L. M. Jr. (2001). Nurses’ recognition of delirium and its symptoms: comparison of nurse and researcher ratings. Arch. Intern. Med. 161, 2467–2473.
Inouye, S. K., Rushing, J. T., Foreman, M. D., Palmer, R. M., and Pompei, P. (1998). Does delirium contribute to poor hospital outcomes? A three-site epidemiologic study. J. Gen. Intern. Med. 13, 234–242.
Inouye, S. K., van Dyck, C. H., Alessi, C. A., Balkin, S., Siegal, A. P., and Horwitz, R. I. (1990). Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 113, 941–948.
Jackson, J. C., Gordon, S. M., Hart, R. P., Hopkins, R. O., and Ely, E. W. (2004). The association between delirium and cognitive decline: a review of the empirical literature. Neuropsychol. Rev. 14, 87–98.
Khan, R. A., Kahn, D., and Bourgeois, J. A. (2009). Delirium: sifting through the confusion. Curr. Psychiatry Rep. 11, 226–234.
Khurana, V., Gambhir, I. S., and Kishore, D. (2011). Evaluation of delirium in elderly: a hospital-based study. Geriatr. Gerontol. Int. 11, 467–473.
Kim, P., Louis, C., Muralee, S., and Tampi, R. R. (2005). Sundowning in the elderly patient. Clin. Geriat. 13, 32–36.
Koster, S., Hensens, A. G., Schuurmans, M. J., and van der Palen, J. (2011). Consequences of delirium after cardiac operations. Ann. Thorac. Surg.
Laurila, J. V., Pitkala, K. H., Strandberg, T. E., and Tilvis, R. S. (2003). The impact of different diagnostic criteria on prevalence rates for delirium. Dement. Geriatr. Cogn. Disord. 16, 156–162.
Laurila, J. V., Pitkala, K. H., Strandberg, T. E., and Tilvis, R. S. (2004). Impact of different diagnostic criteria on prognosis of delirium: a prospective study. Dement. Geriatr. Cogn. Disord. 18, 240–244.
Levkoff, S. E., Evans, D. A., Liptzin, B., Leary, P. D., Lipsitz, L. A., Wetle, T. T., Reilly, C. H., Pilgrim, D. M., Scho, R. J., and Rowe, J. (1992). Delirium the occurrence and persistence of symptoms among elderly hospitalized patients. Arch. Intern. Med. 152, 334–340.
Levkoff, S. E., Liptzin, B., and Cleary, P. D. (1996). Subsyndromal delirium. Am. J. Geriatr. Psychiatry 4, 320–329.
Lewis, L. M., Miller, D. K., Morley, J. E., Nork, M. J., and Lasater, L. C. (1995). Unrecognized delirium in ED geriatric patients. Am. J. Emerg. Med. 13, 142–145.
Lindsay, J., Rockwood, K., and Macdonald, A. (2002). Delirium in Old Age. Oxford: Oxford University Express.
Liptzin, B., and Levkoff, S. E. (1992). An empirical study of delirium subtypes. Br. J. Psychiatry 161, 843–845.
Lishman, W. A. (1997). Organic Psychiatry: The Psychological Consequences of Cerebral Disorder, 3rd Edn. Oxford: Blackwell Scientific.
Lonergan, E., Luxenberg, J., and AreosaSastre, A. (2009). Benzodiazepines for delirium. Cochrane Database Syst. Rev. 4, CD006379.
Longo, D. L., Fauci, A. S., Kasper, D. L., Hauser, S. L., Jameson, J. L., and Loscalzo, J. (2011). Harrison’s Principles of Internal Medicine, 18th Edn. New York: McGraw-Hill Medical Publishing Division.
Luetz, A., Heymann, A., Radtke, F. M., Chenitir, C., Neuhaus, U., Nachtigall, I., von Dossow, V., Marz, S., Eggers, V., Heinz, A., Wernecke, K., and Spies, C. (2010). Different assessment tools for intensive care unit delirium: which score to use? Crit. Care Med. 38, 409–418.
MacLullich, A., Ferguson, K., Miller, T., de Rooij, S., and Cunningham, C. (2008). Unraveling the pathophysiology of delirium: a focus on the role of aberrant stress responses. J. Psychosom. Res. 65, 229–238.
MacLullich, A. M., Beaglehole, A., Hall, R. J., and Meagher, D. J. (2009). Delirium and long-term cognitive impairment. Int. Rev. Psychiatry 21, 30–42.
Maclullich, A. M., Ferguson, K. J., Miller, T., de Rooij, S. E., and Cunningham, C. (2008). Unravelling the pathophysiology of delirium: a focus on the role of aberrant stress responses. J. Psychosom. Res. 65, 229–238.
Marcantonio, E. R. (2011). In the clinic. Delirium. Ann. Intern. Med. 154, ITC6-1, ITC6-2, ITC6-3, ITC6-4, ITC6-5, ITC6-6, ITC6-7, ITC6-8, ITC6-9, ITC6-10, ITC16-11, ITC16-12, ITC16-13, ITC16-14, ITC16-15; quiz ITC16-16.
Marcantonio, E. R., Flacker, J. M., Michaels, M., and Resnick, N. M. (2000). Delirium is independently associated with poor functional recovery after hip fracture. J. Am. Geriatr. Soc. 48, 618–624.
McCusker, J., Cole, M., Dendukuri, N., Belzile, E., and Primeau, F. (2001). Delirium in older medical inpatients and subsequent cognitive and functional status: a prospective study. CMAJ 165, 575–583.
McCusker, J., Cole, M. G., Dendukuri, N., and Belzile, E. (2003). Does delirium increase hospital stay? J. Am. Geriatr. Soc. 51, 1539–1546.
McCusker, J., Cole, M. G., Voyer, P., Monette, J., Champoux, N., Ciampi, A., Vu, M., and Belzile, E. (2011). Prevalence and incidence of delirium in long-term care. Int. J. Geriatr. Psychiatry 26, 1152–1161.
McCusker, J., Kakuma, R., and Abrahamowicz, M. (2002a). Predictors of functional decline in hospitalized elderly patients: a systematic review. J. Gerontol. A Biol. Sci. Med. Sci. 57, M569–M577.
McCusker, J., Cole, M., Abrahamowicz, M., Primeau, F., and Belzile, E. (2002b). Delirium predicts 12-month mortality. Arch. Intern. Med. 162, 457–463.
McKeith, I. G., Dickson, D. W., Lowe, J., Emre, M., O’Brien, J. T., Feldman, H., Cummings, J., Duda, J. E., Lippa, C., Perry, E. K., Aarsland, D., Arai, H., Ballard, C. G., Boeve, B., Burn, D. J., Costa, D., Del Ser, T., Dubois, B., Galasko, D., Gauthier, S., Goetz, C. G., Gomez-Tortosa, E., Halliday, G., Hansen, L. A., Hardy, J., Iwatsubo, T., Kalaria, R. N., Kaufer, D., Kenny, R. A., Korczyn, A., Kosaka, K., Lee, V. M., Lees, A., Litvan, I., Londos, E., Lopez, O. L., Minoshima, S., Mizuno, Y., Molina, J. A., Mukaetova-Ladinska, E. B., Pasquier, F., Perry, R. H., Schulz, J. B., Trojanowski, J. Q., Yamada, M., Consortium on DLB. (2005). Diagnosis and management of dementia with Lewy bodies: third report of the DLB Consortium. Neurology 65, 1863–1872.
Meagher, D. J., Leonard, M., Donnelly, S., Conroy, M., Adamis, D., and Trzepacz, P. T. (2011). A longitudinal study of motor subtypes in delirium: relationship with other phenomenology, etiology, medication exposure and prognosis. J. Psychosom. Res. 71, 395–403.
Meagher, D. J., MacClulich, A. M., and Laurila, J. V. (2008). Defining delirium for the International Classification of Diseases, 11th Revision. J. Psychosom. Res. 65, 207–214.
Meagher, D. J., Moran, M., Raju, B., Gibbons, D., Donnelly, S., Saunders, J., and Trzepacz, P. T. (2007). Phenomenology of delirium. Assessment of 100 adult cases using standardized measures. Br. J. Psychiatry 190, 135–141.
Meagher, D. J., Norton, J. W., and Trzepacz, P. T. (2006). “Delirium in the elderly,” in Principles and Practice of Geriatric Psychiatry, eds M. E. Agronin and G. J. Maletta (Philadelphia: Lippincott Williams & Wilkins), 333–348.
Meagher, D. J., O’Hanlon, D., O’Mahony, E., and Casey, P. R. (1996). The use of environmental strategies and psychotropic medication in the management of delirium. Br. J. Psychiatry 168, 512–515.
Meagher, D. J., O’Hanlon, D., O’Mahony, E., Casey, P. R., and Trzepacz, P. T. (2000). Relationship between symptoms and motoric subtype of delirium. J. Neuropsychiatry Clin. Neurosci. 12, 51–56.
Mittal, V., Muralee, S., Williamson, D., McEnerney, N., Thomas, J., Cash, M., and Tampi, R. R. (2011). Review: delirium in the elderly: a comprehensive review. Am. J. Alzheimers Dis. Other Demen. 26, 97–109.
Morandi, A., and Jackson, J. C. (2011). Delirium in the intensive care unit: a review. Neurol. Clin. 29, 749–763.
Morandi, A., Pandharipande, P., Trabucchi, M., Rozzini, R., Mistraletti, G., Trompeo, A. C., Gregoretti, C., Gattinoni, L., Ranieri, M. V., Brochard, L., Annane, D., Putensen, C., Guenther, U., Fuentes, P., Tobar, E., Anzueto, A. R., Esteban, A., Skrobik, Y., Salluh, J. I., Soares, M., Granja, C., Stubhaug, A., de Rooij, S. E., and Ely, E. W. (2008). Understanding international differences in terminology for delirium and other types of acute brain dysfunction in critically ill patients. Intensive Care Med. 34, 1907–1915.
Murray, A. M., Levkoff, S. E., Wetle, T. T., Beckett, L., Cleary, P. D., Schor, J. D., Lipsitz, L. A., Rowe, J. W., and Evans, D. A. (1993). Acute delirium and functional decline in the hospitalized elderly patient. J. Gerontol. 48, M181–M186.
Naughton, B. J., Saltzman, S., Ramadan, F., Chadha, N., Priore, R., and Mylotte, J. M. (2005). A multifactorial intervention to reduce prevalence of delirium and shorten hospital length of stay. J. Am. Geriatr. Soc. 53, 18–23.
NICE. (2010). Delirium: Diagnosis, Prevention and Management. (Clinical Guideline 103). National Institute for Health and Clinical Excellence. Available at: www.nice.org.uk/CG103
Olsson, T. (1999). Activity in the hypothalamic-pituitary-adrenal axis and delirium. Dement. Geriatr. Cogn. Dis. 10, 345–349.
Ouimet, S., Riker, R., Bergeron, N., Cossette, M., Kavanagh, B., and Skrobik, Y. (2007). Subsyndromal delirium in the ICU: evidence for a disease spectrum. Intensive Care Med. 33, 1007–1013.
Overshott, R., Karim, S., and Burns, A. (2008). Cholinesterase inhibitors for delirium. Cochrane Database Syst. Rev. 1, CD005317.
Oyebode, F. (2008). Sims’ Symptoms in the Mind: An Introduction to Descriptive Psychopathology. 4th Edn. Philadelphia: Saunders Elsevier.
Ramirez-Bermudez, J., Ruiz-Chow, A., Perez-Neri, I., Soto-Hernandez, J., Flores-Hernandez, R., Nente, F., Montes, S., and Rios, C. (2008). Cerebrospinal fluid homovanillic acid is correlated to psychotic features in neurological patients with delirium. Gen. Hosp. Psychiatry 30, 337–343.
Rathier, M. O., and Baker, W. L. (2011). A review of recent clinical trials and guidelines on the prevention and management of delirium in hospitalized older patients. Hosp. Pract. (Minneap.) 39, 96–106.
Reitan, R. M. (1958). The validity of the Trail Making Test as an indicator of organic brain damage. Percept. Mot. Skills 8, 271–276.
Rolfson, D. (2002). “The causes of delirium,” in Delirium in Old Age, eds J. Lindsay, K. Rockwood and A. Macdonald (Oxford: Oxford University Express), 101–122.
Rudolph, J. L., Ramlawi, B., Kuchel, G. A., McElhaney, J. E., Xie, D., Sellke, F. W., Khabbaz, K., Levkoff, S. E., and Marcantonio, E. R. (2008). Chemokines are associated with delirium after cardiac surgery. J. Gerontol. A Biol. Sci. Med. Sci. 63, 184–189.
Salawu, F. K., Danburam, A., and Ogualili, P. (2009). Delirium: issues in diagnosis and management. Ann. Afr. Med. 8, 139–146.
Sampson, E. L., Blanchard, M. R., Jones, L., Tookman, A., and King, M. (2009). Dementia in the acute hospital: prospective cohort study of prevalence and mortality. Br. J. Psychiatry 195, 61–66.
Saxena, S., and Lawley, D. (2009). Delirium in the elderly: a clinical review. Postgrad. Med. J. 85, 405–413.
Shi, Q., Presutti, R., Selchen, D., and Saposnik, G. (2012). Delirium in acute stroke: a systematic review and meta-analysis. Stroke 43, 645–649.
Siddiqi, N., House, A. O., and Holmes, J. D. (2006). Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing 35, 350–364.
Simone, M. J., and Tan, Z. S. (2011). The role of inflammation in the pathogenesis of delirium and dementia in older adults: a review. CNS Neurosci. Ther. 17, 506–513.
Slaets, J. P., Kauffmann, R. H., Duivenvoorden, H. J., Pelemans, W., and Schudel, W. J. (1997). A randomized trial of geriatric liaison intervention in elderly medical inpatients. Psychosom. Med. 59, 585–591.
Tabet, N., Hudson, S., Sweeney, V., Sauer, J., Bryant, C., Macdonald, A., and Howard, R. (2005). An educational intervention can prevent delirium on acute medical wards. Age Ageing 34, 152–156.
Teasdale, G., and Jennett, B. (1974). Assessment of coma and impaired consciousness. A practical scale. Lancet 2, 81–84.
Teodorczuk, A., Welfare, M., Corbett, S., and Mukaetova-Ladinska, E. (2010). Developing effective educational approaches for Liaison Old Age Psychiatry teams: a literature review of the learning needs of hospital staff in relation to managing the confused older patient. Int. Psychogeriatr. 22, 874–885.
Trzepacz, P. (2000). Is there a final common neural pathway in delirium? Focus on acetylcholine and dopamine. Semin. Clin. Neuropsychiatry 5, 132–148.
Trzepacz, P. T. (1996). Anticholinergic model for delirium. Semin. Clin. Neuropsychiatry 1, 294–303.
Trzepacz, P. T., Mittal, D., Torres, R., Kanary, K., Norton, J., and Jimerson, N. (2001). Validation of the Delirium Rating Scale-revised-98: comparison with the delirium rating scale and the cognitive test for delirium. J. Neuropsychiatry Clin. Neurosci. 13, 229–242.
Trzepacz, P. T., and van der Mast, R. (2002). The Neuropathophysiology of Delirium. Oxford: Oxford University Press.
van den Boogaard, M., Schoonhoven, L., van der Hoeven, J. G., van Achterberg, T., and Pickkers, P. (2011). Incidence and short-term consequences of delirium in critically ill patients: a prospective observational cohort study. Int. J. Nurs. Stud. doi: 10.1016/j.ijnurstu.2011.11.016
van Munster, B. C., Korevaar, J. C., Zwinderman, A. H., Levi, M., Wiersinga, W. J., and De Rooij, S. E. (2008). Time-course of cytokines during delirium in elderly patients with hip fractures. J. Am. Geriatr. Soc. 56, 1704–1709.
Voyer, P., Richard, S., Doucet, L., and Carmichael, P. H. (2009). Detecting delirium and subsyndromal delirium using different diagnostic criteria among demented long-term care residents. J. Am. Med. Dir. Assoc. 10, 181–188.
Wahlund, L., and Bjorlin, G. A. (1999). Delirium in clinical practice: experiences from a specialized delirium ward. Dement. Geriatr. Cogn. Disord. 10, 389–392.
Wallesch, W. R., and Hundsaltz, A. (1994). Language function in delirium: a comparison of single word processing in acute confusional state and probable Alzheimer’s disease. Brain Lang. 46, 592–606.
Watt, D. F., Koziol, K., and Budding, D. (2012). “Delirium and confusional states,” in Disorders in Neuropsychiatry, eds C. A. Noggle and R. S. Dean (New York: Springer Publishing Company).
Watt, D. F., and Pincus, D. I. (2004). “Neural substrates of consciousness: implications for clinical psychiatry,” in Textbook of Biological Psychiatry, ed. J. Panksepp (New York: John Wiley & Sons, Inc.).
Wechsler, D. (1997). Weschsler Adult Intelligence Scale-III. San Antonio, TX: The Psychological Corporation.
Wei, L. A., Fearing, M. A., Sternberg, E. J., and Inouye, S. K. (2008). The Confusion Assessment Method: a systematic review of current usage. J. Am. Geriatr. Soc. 56, 823–830.
WHO. (1992). The ICD-10 Classification of Mental and Behavioural Disorders Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization.
Witlox, J., Eurelings, L. S., de Jonghe, J. F., Kalisvaart, K. J., Eikelenboom, P., and van Gool, W. A. (2010). Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA 304, 443–451.
Wong, C. L., Holroyd-Leduc, J., Simel, D. L., and Straus, S. E. (2010). Does this patient have delirium? Value of bedside instruments. JAMA 304, 779–786.
Yang, F. M., Marcantonio, E. R., Inouye, S. K., Kiely, D. K., Rudolph, J. L., Fearing, M. A., and Jones, R. N. (2009). Phenomenological subtypes of delirium in older persons: patterns, prevalence, and prognosis. Psychosomatics 50, 248–254.
Keywords: delirium, aged, diagnosis, etiology, prevention and control
Citation: Martins S and Fernandes L (2012) Delirium in elderly people: a review. Front. Neur. 3:101. doi: 10.3389/fneur.2012.00101
Received: 07 February 2012; Paper pending published: 28 February 2012;
Accepted: 01 June 2012; Published online: 19 June 2012.
Edited by:
João Massano, University of Porto, PortugalReviewed by:
Douglas Watt, Quincy Medical Center, USAElizabeta Blagoja Mukaetova-Ladinska, Newcastle University, UK
Anne Corbett, Alzheimer’s Society, UK
Copyright: © 2012 Martins and Fernandes. This is an open-access article distributed under the terms of the Creative Commons Attribution Non Commercial License, which permits non-commercial use, distribution, and reproduction in other forums, provided the original authors and source are credited.
*Correspondence: Lia Fernandes, Faculty of Medicine, University of Porto, Al. Hern᭩ Monteiro, 4200-319 Porto, Portugal. e-mail:bGlhLmZlcm5hbmRlc0BtYWlsLnRlbGVwYWMucHQ=