 Victória dos Santos Chemelo1Yago Gecy de Sousa Né1Deborah Ribeiro Frazão1Renata Duarte de Souza-Rodrigues1
Victória dos Santos Chemelo1Yago Gecy de Sousa Né1Deborah Ribeiro Frazão1Renata Duarte de Souza-Rodrigues1 Nathalia Carolina Fernandes Fagundes2
Nathalia Carolina Fernandes Fagundes2 Marcela Baraúna Magno3Cláudia Maria Tavares da Silva3
Marcela Baraúna Magno3Cláudia Maria Tavares da Silva3 Lucianne Cople Maia3
Lucianne Cople Maia3 Rafael Rodrigues Lima1*
Rafael Rodrigues Lima1*- 1Laboratory of Functional and Structural Biology, Institute of Biological Sciences, Federal University of Pará, Belém-Pará, Brazil
- 2Faculty of Medicine and Dentistry, University of Alberta, Edmonton, AB, Canada
- 3Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
This systematic review and meta-analysis aimed to investigate a possible association between stress and bruxism in humans. This study was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines under the code CRD42020188862, and the searches were performed on the following databases: PubMed, Scopus, Web of Science, Cochrane, LILACS, OpenGrey, and Google Scholar. This systematic review evaluated observational studies in adult humans with and without stress to verify the association between bruxism and the presence of stress. The risk of bias was evaluated through the Joanna Briggs Institute Critical Appraisal Tools for Analytical Cross-Sectional Studies. In quantitative analysis, the Odds Ratio (OR) and their 95% confidence interval (CI) were calculated through a fixed-effect model. Furthermore, a summary of the overall strength of evidence was presented using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE). A total of 1,458 studies were identified, and six were included in this systematic review. Two studies included were classified with a low risk of bias, and the others were classified with a moderate risk of bias. In three articles, a meta-analysis was performed and showed an association between these two factors (OR 2.07 [1.51, 2.83], p < 0.00001, I2 = 45%). Besides that, a low certainty of the evidence was detected among this association. Stressed individuals show a higher chance of presenting bruxism when compared to healthy individuals. Despite the low heterogeneity found in the quantitative analysis among the articles reporting an association between stress and bruxism, further studies with similar methods are necessary to understand this relationship better.
Introduction
Stress can be defined as “a condition or feeling experienced when a person perceives that the demands placed on them exceed the resources the individual has available” (1). Bad, excessive, or prolonged stress reactions may exceed the organism's natural adaptive capacity and permanently affect stress responses (2). The impact of stress on physiological and psychological processes is determined by characteristics of the stress stimulus (3), being able to trigger changes in several functions in the organism, including repercussions on the stomatognathic apparatus (4).
Bruxism is a repetitive muscular activity of the jaw characterized by grinding or clenching the teeth and bracing or thrusting of the mandible, is mainly regulated centrally, and may involve more than dental contact (5). Currently, bruxism has a distinction between sleep bruxism and awake bruxism. Sleep bruxism is a sleep-related movement disorder characterized as rhythmic or non-rhythmic of masticatory muscle activity (5, 6). In contrast, awake bruxism is a non-functional behavior during wakefulness characterized by repetitive or sustained tooth contact and/or by bracing or thrusting of the mandible (5, 6). However, both forms are associated with different personal behaviors as potential clinical consequences (5).
The factors associated with the development of bruxism are bad habits, such as smoking, high alcohol, and coffee consumption (7); sleep apnea syndrome, anxiety disorder, depression, respiratory diseases (8–10). Recent studies show that emotional changes may be associated with bruxism. However, few studies investigate these isolated manifestations (11).
This systematic review study was developed to gather evidence in the literature to answer the question: “Is there evidence in the literature that points to a possible association between stress and bruxism in humans?”
Materials and Methods
Protocol and Registration
This systematic review was registered at PROSPERO under the registration number CRD42020188862 and performed according to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) checklist (12) (Supplementary Table 1).
Eligibility Criteria and Search Strategy
The PECO strategy was followed in this systematic review. Observational studies in humans (P), with stress (E), and without stress (C) that verified the association between bruxism (O), were included. Also, opinion articles, case reports, descriptive studies, review articles, technical articles, guides, animal studies, and in vitro studies were excluded. No restriction about the diagnostic tool to assess the stress and age of the participants was applied. The null hypothesis of this review was: “There is no association between stress and bruxism.”
Searches were conducted in the following electronic databases, without language or year restriction until June 2020: PubMed, Scopus, Web of Science, The Cochrane Library, LILACS. The gray literature was searched through OpenGrey and Google Scholar. The search strategy was prepared to be held in PubMed and contained a combination of controlled pre-defined MeSh and free terms related to stress and bruxism. This strategy was adapted according to the syntax rules of each database. Boolean operators (OR, AND) were used to combine searches (Supplementary Table 2).
After searches, all relevant citations were saved in a bibliographic reference manager (EndNote, x9 version, Thomson Reuters). Duplicated results were considered only once. The titles and abstracts that did not adhere to the established eligibility criteria were excluded. The resulting articles were evaluated and judged by their full text.
Additional citations were sought from the analysis of the reference list of all articles previously selected. The selection process was conducted by two examiners (VC and YN) and checked by a third examiner (RL), in cases of disagreements.
Data Extraction and Studies Selection
Data extraction was carried by two examiners (VC and YN), independently. A third reviewer was consulted in case of disagreement.
It was took into consideration information related to the author, local and year of publication, study design, sample source and sample sizes, age of participants, stress and bruxism evaluation method, statistical analysis, and main results (Table 1).
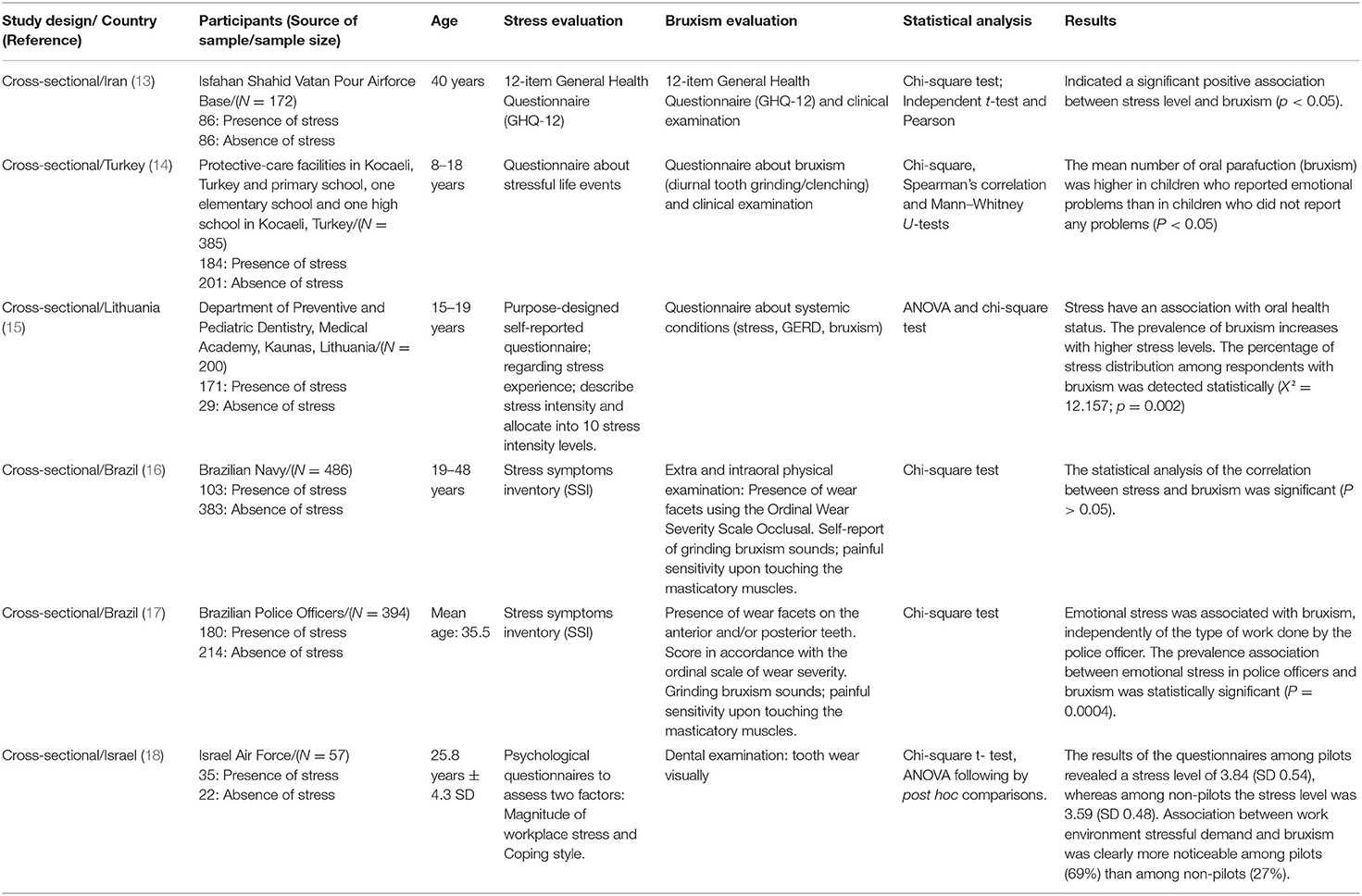
Table 1. Summary of characteristics and results of the included studies.
In case of the absence of relevant information for data extraction or risk of bias evaluation, we attempted to contact the authors by email. A weekly email was sent to the authors for up to five consecutive weeks.
Quality Assessment Analysis and Risk of Bias
The studies' quality and risk of bias were assessed through the Joanna Briggs Institute Critical Appraisal Tools for Analytical Cross-Sectional Studies (19). The tool consists of eight questions whose answers could be “yes,” “no,” “unclear,” and “not applicated.” The risk of bias was scored as Low when the study reached over 70% of the “yes” score, Moderate when the study reached from 50 to 69% of the “yes” score and High when the study reached up to 49% of “yes” score. Studies characterized as a “high risk of bias” were excluded (20, 21). The guidelines of evaluation criteria are described in Supplementary Table 3.
Quantitative Synthesis (Meta-Analysis)
The quantitative synthesis to evaluate the relationship between stress and bruxism was assessed using Review Manager software v. 5.3. Number of Bruxism (events) and the total number of individuals in case (stressed) and control (none stressed) groups were included to calculate the Odds Ratio (OR) with a 95% confidence interval (CI). A fixed-effect model was used (22), and heterogeneity significance was evaluated using the I2 index. Thresholds for the interpretation of the I2 statistic were considered as suggested by Cochrane handbook (www.training.cochrane.org/handbook): 0–40%: might not be important, 30–60%: may represent moderate heterogeneity, 50–90%: may represent substantial heterogeneity, 75– 100%: considerable heterogeneity. A sensitivity analysis was performed to evaluate the influence of risk of bias in effect significance. During this phase, studies with some type of risk of bias were excluded from meta-analysis and changes in the overall significance were evaluated.
Assessment of the Certainty of the Evidence
The certainty of the evidence (certainty in the estimates of effect) was determined for the outcome using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (23). Whereby observational studies start as low certainty in the body of evidence and could decreases to very low quality, if serious or very serious issues, related to the risk of bias, inconsistency, indirectness, imprecision, and publication bias, are present. Publication bias was evaluated through visual analysis of the funnel plot. Besides, the quality of the evidence can be upgraded if the magnitude of the effect is large or very large or if the effect of all plausible confounding factors would reduce the effect or suggest a spurious effect. The dose-response was not applied in the type of studies included in the present systematic review and as judged in a way to not uninfluenced in the final certainty of evidence. In this way, the quality of the evidence can vary from very low to high.
Results
Study Selection and Characteristics
1,458 articles were identified from all databases, and 548 duplicate citations were excluded. Titles and abstracts of 910 articles were verified following the entry criteria. 15 articles were selected for full-text appraisal, resulting in the exclusion of 895 articles. Six were included in this systematic review, and 3 of them were included in quantitative synthesis (meta-analysis). The articles excluded after reading in full and reasons for exclusions are shown in Supplementary Table 4.
Results of Individual Studies
Among the six articles included, all of them were cross-sectional studies. An association between the stress and bruxism was reported in all six articles (13–18). In the case of the absence of relevant information for data extraction and risk of bias, the authors were contacted by email, were made to provide the lack of information (13). These studies were performed in Iran (13), Turkey (14), Lithuania (15), Brazil (16, 17), and Israel (18).
According to the study, the stress evaluation was performed through validated and not validated questionnaires, assessing life events and stress scale. The parameters used to evaluate bruxism by the selected studies were clinical features and/or questionnaires. The data extraction about the articles is in Table 1.
Three studies performed a clinical evaluation regarding bruxism evaluation, considering tooth wear, teeth clenching, and grinding as diagnostic parameters. A 6-point scale was considered for final diagnosis (13, 16–18). Four studies applied validated questionnaires to evaluate bruxism (13–15).
Six articles were considered for quality assessment, and their summary selection is shown in Figure 1.
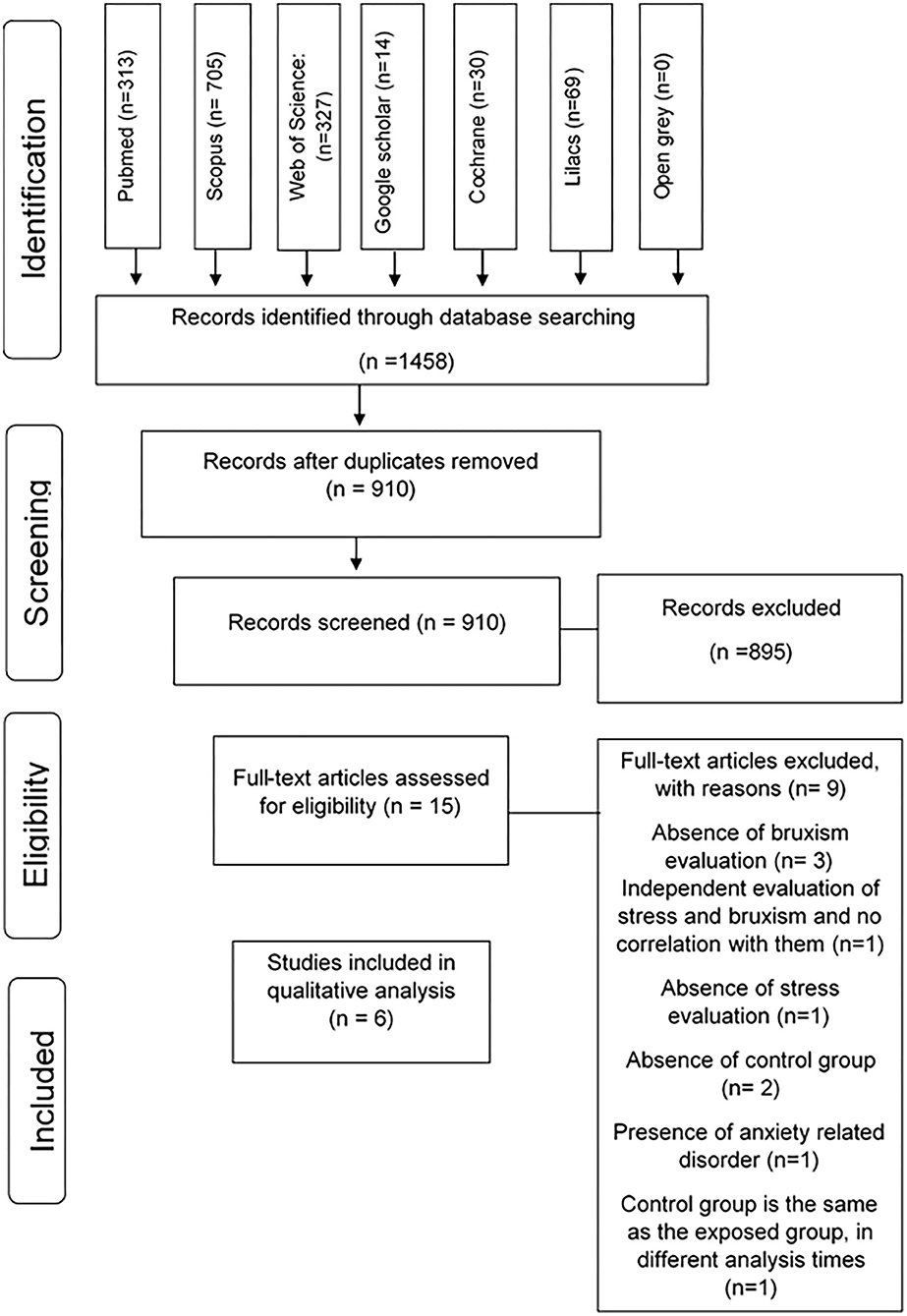
Figure 1. Flow diagram of databases searched according to PRISMA guidelines (Preferred Reporting Items for Systematic Review and Meta-Analysis).
Qualitative Assessment and Risk of Bias
All of the studies evaluated subsamples using cross-sectional methods (13–18). The quality of measurements described in the articles is shown in Table 2. None of the studies evaluated had a high risk of bias. However, some studies reduced the methodological quality due to issues reported in the assessment criteria such as inclusion criteria, subjects of study, exposure measure, outcomes measure, and statistical analysis.
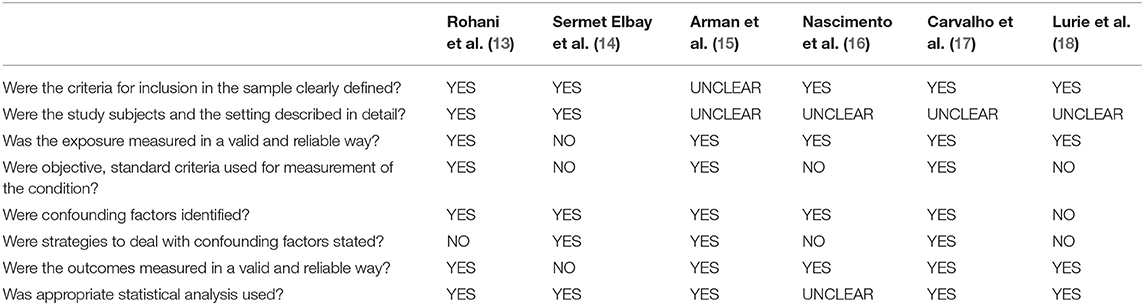
Table 2. Quality assessment and risk of bias according to Critical Appraisal Tool (Joanna Briggs Institute, 2017).
Two studies included were classified with low risk of bias (15, 17) and the others were classified with a moderate risk of bias (13, 14, 16, 18) (Table 2). In addition, some methodological problems were detected, more specifically: the lack of clarity in inclusion criteria (15); the presence of confounding factors such as smoking habits or other oral dysfunction (13–17); and the lack of clarity regarding stress evaluation (14, 16, 18).
Meta-Analysis and Certainty of the Evidence
Three studies were included in the meta-analysis (14, 15, 17). Three studies were not included in the meta-analysis due to a lack of data in the control group (13, 16, 18) (Figure 2).
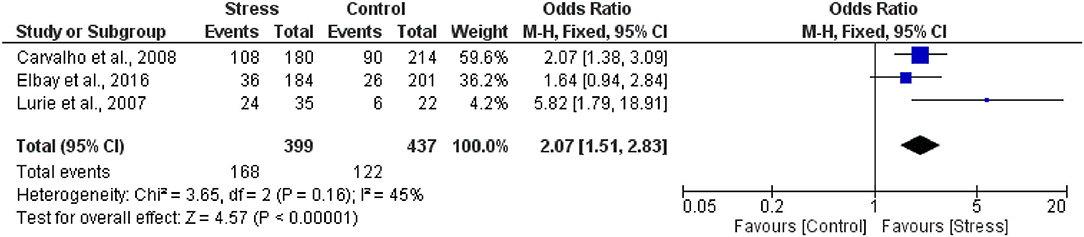
Figure 2. Forest plot of association between stress and bruxism.
The overall heterogeneity was I2 = 45% (p = 0.16) (moderate heterogeneity). The total individuals that in the case group (n = 399), 42.1% (n = 168), presented bruxism, while 27.9% (n = 122) of the total of individuals in the control group (n = 437) presented bruxism. Stress and bruxism are positively related once stressed people presented a 97% higher chance to present bruxism (OR 2.07 [1.51, 2.83], p < 0.00001), with low certainty of evidence (Table 3).
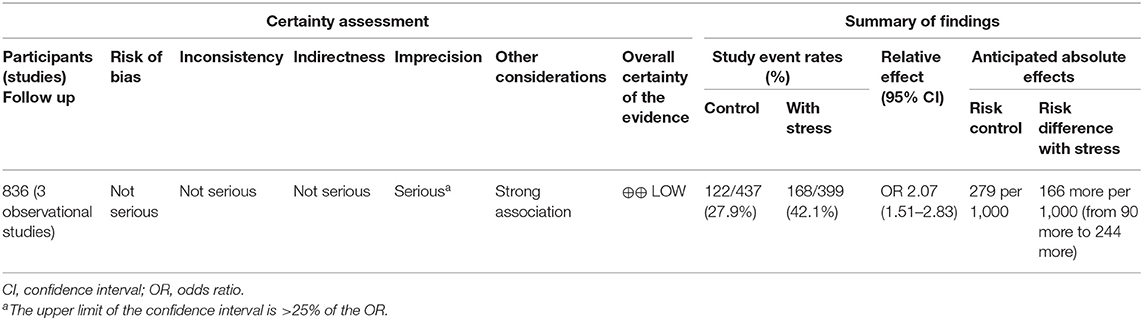
Table 3. The certainty of evidence: association between stress and bruxism.
The sensitivity analysis showed that the exclusion of studies with some type of risk of bias did not influenced in overall significance. Besides serious problems in “imprecision” the overall results presented strong association, so, the certainty of evidence was classified as low.
Discussion
In this systematic review, we gather evidence of the association between stress and bruxism, confirmed in the quantitative analysis. However, this association proved to have a low heterogeneity and a low certainty of evidence due to the elected studies' experimental design.
In this review, six of the chosen studies showed a comparable association of bruxism in patients with stress. The evaluation parameters of stress are related to validated or non-validated questionnaires to determine stress levels. Among these validated questionnaires, the oldest is the Perceived Stress Scale (24), 12-item General Health Questionnaire (25), and the most recent is the Stress Symptoms Inventory (SSI) (26) and non-validated questionnaires about stress events/experience (14, 15, 18). The Perceived Stress Scale (24) consists of one of the most cited instruments in the literature for stress assessment. It is known that stress diagnosis is a subjective criterion correlated to the answer of questionnaires with pre-established scores and scales.
Although the selected studies deal with different types of stress. Two studies assessed emotional stress (16, 17); two studies evaluated psychological stress (13, 18) and two studies evaluated stress in life events or experience (14, 15). Stress is manifested through physiological functions, performance, behavior, and subjective symptoms (27). In these cases, the stress has been associated with several altered cognitive function findings, such as poor processing speed, defective executive functioning, and memory deficits (28). Emotional stress has also been associated with risk factors for cardiovascular dysfunction (3), immune system functions (29), endocrine system (30) and in the stomatognathic system (31).
Another kind of stress evaluated by the included studies was psychosocial stress. This type of stress is induced by situations of social threat, including social evaluation, social exclusion, and achievement situations claiming goal-directed performance (32). Stressful life events could induce a series of psychological changes (27). Psychological and psychosomatic symptoms are related to stress in occupational exposure, anxiety, and depression, financial problems, and periodic headaches, and oral dysfunctions (33).
Bruxism functions as a kind of perpetual motion machine, as intensifying symptoms resulting from an organism's abnormal functioning increase a feeling of being stressed, and in consequence, lead to an increased muscle tone and teeth grinding (34). It is generally accepted that stressful situations and mental diseases conduct to the development of occlusal parafunction and temporomandibular disorders without being the only cause (35). Several studies reported that bruxism, one of the most common parafunctional habits, has psychosocial, emotional, and psychological as a risk factor triggering bruxism.
Bruxism is a repetitive masticatory muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible. That is specified as either sleep bruxism or awake bruxism, depending on its circadian phenotype (36). The etiology of bruxism is multifactorial. The anatomy, morphology, and dental occlusion are linked to bruxism (36). Early diagnosis of bruxism is of great importance both for its treatment and for its prevention. The diagnosis must focus on identifying the signs and symptoms reported by the patient or the dentist during a clinical examination (37).
In the present study, the selected articles evaluated bruxism without distinction of types, such as awake or sleep bruxism. This is because the selected articles had their publication year before the new classification on bruxism that advocates this subdivision (5). Therefore, the selected articles encompass a more generalized concept. Three studies evaluated bruxism with clinical examination, teeth clenching and grinding sounds, muscle pain, and tooth wear, the most common evidence of bruxism (16–18). Two studies assessed this condition using clinical examination and validated questionnaires (13, 14). The last one was evaluated with a questionnaire about systemic conditions, including bruxism (15).
The leading cause of bruxism has not been determined but is held to involve multiple factors (38). The risk factors are smoking (39), gastroesophageal reflux disease (40), sleep apnea syndrome (41), genetic and behavior (37), anxiety (42), alcohol excesses (43), depression (44). This systematic review shows that, despite other causal factors, the various types of stress may modulate bruxism.
Considering the problems due to the lack of data in the control group, three studies were excluded from the meta-analysis (13, 16, 17). Furthermore, a meta-analysis was performed. The data of meta-analyses revealed that stressed adults presented 2.07 more chances to present bruxism. Also, a low heterogeneity (I2 = 45%, p = 0.16) was observed in this evidence. In addition to problems with lack of data, failures were detected in the existence of confounding factors resulting from unpaired sample characteristics such as smoking, systemic diseases, types of works.
The level of evidence evaluation through GRADE assessment showed a low level in our analysis. This low certainty of evidence found in this systematic review is related to cross-sectional studies evaluated since the methodologies inconsistencies present discrepancies in sample size, use of non-validated analysis tools, and the available data.
As the strengths of this review, we pointed out the inclusion of observational studies regardless of the age or stress evaluation methods adopted by the studies. This review describes the results and the quality of the current evidence on the topic, suggesting an association between bruxism and stress and highlighting the future direction for future research. Despite the low level of certainty observed in GRADE, it is essential to note that, in the quantitative data, the selected studies suggest that patients with stress are very likely to present bruxism. These results must be questionable due to the substantial heterogeneity detected and the inconsistency of the evidence. Therefore, the results suggest that more studies are needed to establish a high certainty of evidence related to stress and bruxism.
Conclusion
This systematic review suggests a significant association between bruxism in patients stressed, especially in emotional disorders and occupational exposures. Our meta-analysis shows low heterogeneity between the studies due to a low level of evidence, which resulted in limitations of the bruxism evaluation parameters and lack of methodological criteria. Therefore, more studies with representative samples and other clinical assessments on stress and bruxism are necessary to establish this possible association.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
VC, CS, LM, and RL: study concept and design. VC, YN, DF, and MM: analysis and interpretation of data. VC, RS-R, and NF: preparation of the manuscript. LM and RL: critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brazil (CAPES)—Finance Code 001 and PROPESP-UFPA.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank the Federal University of Pará, Federal University of Rio de Janeiro, and the University of Alberta for technical and scientific support.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2020.590779/full#supplementary-material
References
1. American Institute of Stress. What is Stress? (2016). Available online at: http://www.stress.org/what-isstress (accessed July 12, 2020).
2. Chrousos GP. Stress and disorders of the stress system. Nat. Rev. Endocrinol. (2009) 5:374. doi: 10.1038/nrendo.2009.106
3. Crestani CC. Emotional stress and cardiovascular complications in animal models: a review of the influence of stress type. Front. Physiol. (2016) 7:251. doi: 10.3389/fphys.2016.00251
4. Saczuk K, Lapinska B, Wilmont P, Pawlak L, Lukomska-Szymanska M. Relationship between sleep bruxism, perceived stress, and coping strategies. Int. J. Environ. Res. Public Health. (2019) 16:3193. doi: 10.3390/ijerph16173193
5. Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, Glaros AG, Kato T, et al. International consensus on the assessment of bruxism: report of a work in progress. J. Oral Rehabil. (2018) 45:837–44. doi: 10.1111/joor.12663
6. Reissmann DR, John MT, Aigner A, Schön G, Sierwald I, Schiffman EL. Interaction between awake and sleep bruxism is associated with increased presence of painful temporomandibular disorder. J. Oral Facial Pain Headache. (2017) 31:299–305. doi: 10.11607/ofph.1885
8. Cruz Fierro N, Martínez Fierro M, Cerda Flores RM, Gómez-Govea MA, Delgado-Enciso I, Martínez-De-Villarreal LE, et al. The phenotype, psychotype and genotype of bruxism. Biomed. Rep. (2018) 8:264–8. doi: 10.3892/br.2018.1041
9. Castroflorio T, Bargellini A, Rossini G, Cugliari G, Rainoldi A, Deregibus A. Risk factors related to sleep bruxism in children: a systematic literature review. Arch. Oral Biol. (2015) 60:1618–24. doi: 10.1016/j.archoralbio.2015.08.014
10. Soares-Silva L, Tavares-Silva C, Fonseca-Gonçalves A, Maia LC. Presence of oral habits and their association with the trait of anxiety in pediatric patients with possible sleep bruxism. J. Indian Soc. Pedod. Prev. Dent. (2019) 37:245–50. doi: 10.4103/JISPPD.JISPPD_272_18
11. Yap AU, Chua AP. Sleep bruxism: current knowledge and contemporary management. J. Conserv. Dent. (2016) 19:383–9. doi: 10.4103/0972-0707.190007
12. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. (2015) 4:1. doi: 10.1186/2046-4053-4-1
13. Rohani B, Neshati A, Najafi S, Amini K, Shirani MJ. Comparing the psychological stress and health of masticatory system in military pilots to non-pilot officers. J. Mil. Med. (2018) 20:290–8.
14. Sermet Elbay Ü, Demirturk Kocasarac H, Elbay M, Kaya C, Ugurluel C, Baydemir C. Temporomandibular disorders and oral parafunction in children living with their parents and children living in institutional protective care: a comparative study. Int. Dent. J. (2017) 67:20–8. doi: 10.1111/idj.12253
15. Arman K, Petruninaite A, Grigalauskiene R, Slabšinskiene E. Stress experience and effect on self-perceived oral health status among high school students. Stomatologija. (2016) 18:75–9.
16. Nascimento AM, Pires AA, de Gouvêa CVD, Andrade F, dos Santos PH. Bruxism association with emotional stress: transversal study. Rev. Bras. Odontol. (2010) 66:160.
17. Carvalho AL, Cury AA, Garcia RC. Prevalence of bruxism and emotional stress and the association between them in Brazilian police officers. Braz. Oral Res. (2008) 22:31–35. doi: 10.1590/S1806-83242008000100006
18. Lurie O, Zadik Y, Einy S, Tarrasch R, Raviv G, Goldstein L. Bruxism in military pilots and non-pilots: tooth wear and psychological stress. Aviat. Space Environ. Med. (2007) 78:137–9.
19. Moola S, Munn Z, Tufanaru C, Aromataris E, Sears K, Sfetcu R, et al. Systematic reviews of etiology and risk. In: Aromataris E, Munn Z, editors. Joanna Briggs Institute Reviewer's Manual. Adelaide, SA: The Joanna Briggs Institute. (2017). Available online at: https://reviewersmanual.joannabriggs.org/ (accessed July 25, 2020).
20. Sampaio MS, Vieira WDA, Bernardino ÍDM, Herval ÁM, Flores-Mir C, Paranhos LR. Chronic obstructive pulmonary disease as a risk factor for suicide: a systematic review and meta-analysis. Respir. Med. (2019) 151:11–18. doi: 10.1016/j.rmed.2019.03.018
21. Polmann H, Melo G, Conti Réus J, Domingos FL, de Souza BDM, Padilha AC, et al. Prevalence of dentofacial injuries among combat sports practitioners: a systematic review and meta-analysis. Dent. Traumatol. (2020) 6:124–40. doi: 10.1111/edt.12508
22. Borenstein M. Common Mistakes in Meta-Analysis and How to Avoid Them. Englewood, NJ: Biostat, Incorporated. (2019), p. 388.
23. Ryan R, Hill S. How to GRADE the Quality of the Evidence. London: Cochrane Consumers and Communication Group. (2016). Available online at: http://cccrg.cochrane.org/author-resources (accessed June 27, 2020).
24. Cohen S, Lamarch T, Mermelstein R. A global measure of perceived stress. J. Health Soc. Behav. (1983) 24:385–96. doi: 10.2307/2136404
25. Graetz B. Multidimensional properties of the general health questionnaire. Soc. Psychiatry Psychiatr. Epidemiol. (1991) 26:132–8. doi: 10.1007/BF00782952
26. Lipp MEN, Guevara AJH. Empiric validation of stress symptoms inventory (SSI). Estud Psicol. (1994) 11:43–9.
27. Leppänen RA, Olkinuora MA. Psychological stress experienced by health care personnel. Scand. J. Work Environ. Health. (1987) 13:1–8. doi: 10.5271/sjweh.2086
28. Agorastos A, Pervanidou P, Chrousos GP, Baker DG. Developmental trajectories of early life stress and trauma: a narrative review on neurobiological aspects beyond stress system dysregulation. Front. Psychiatry. (2019) 10:118. doi: 10.3389/fpsyt.2019.00118
29. Vitlic A, Lord JM, Phillips AC. Stress, ageing and their influence on functional, cellular and molecular aspects of the immune system. Age. (2014) 36:9631. doi: 10.1007/s11357-014-9631-6
30. Charmandari E, Tsigos C, Chrousos G. Endocrinology of the stress response. Annu. Rev. Physiol. (2005) 67:259–84. doi: 10.1146/annurev.physiol.67.040403.120816
31. Chen YJ, Huang F, Zhang M, Shang HY. Psychological stress alters ultrastructure and energy metabolism of masticatory muscle in rats. Biomed. Res. Int. (2010) 2010:1–9. doi: 10.1155/2010/302693
32. Pruessner JC, Dedovic K, Pruessner M, Lord C, Buss C, Collins L. et al. Stress regulation in the central nervous system: evidence from structural and functional neuroimaging studies in human populations - 2008 Curt Richter Award Winner. Psychoneuroendocrinology. (2010) 35:179–91. doi: 10.1016/j.psyneuen.2009.02.016
33. Yang L, Zhao Y, Wang Y, Liu L, Zhang X, Li B, et al. The effects of psychological stress on depression. Curr. Neuropharmacol. (2015) 13:494–504. doi: 10.2174/1570159X1304150831150507
34. American Academy of Sleep Medicine (AASM). International Classification of Sleep Disorders: Diagnostic and Coding Manual (2005). p. 51–5.
35. Wieckiewicz M, Paradowska-Stolarz A, Wieckiewicz W. Psychosocial aspects of bruxism: the most paramount factor influencing teeth grinding. Biomed. Res. Int. (2014) 2014:469187. doi: 10.1155/2014/469187
36. Lobbezoo F, Ahlberg J, Glaros AG, Katos T, Koyano K, Lavigne GJ, et al. Bruxism defined and graded: an international consensus. J. Oral. Rehabil. (2013) 40:2–4. doi: 10.1111/joor.12011
37. Yamaguchi T, Abe S, Rompré PH, Manzini C, Lavigne GJ. Comparison of ambulatory and polysomnographic recording of jaw muscle activity during sleep in normal subjects. J. Oral. Rehabil. (2012) 39:2–10. doi: 10.1111/j.1365-2842.2011.02232.x
38. Balanta-Melo J, Toro-Ibacache V, Kupczik K, Buvinic S. Mandibular bone loss after masticatory muscles intervention with botulinum toxin: an approach from basic research to clinical findings. Toxins. (2019) 11:84. doi: 10.3390/toxins11020084
39. Rintakoski K, Ahlberg J, Hublin C, Lobbezoo F, Rose RJ, Murtomaa H, et al. Tobacco use and reported bruxism in young adults: a nationwide Finnish twin cohort study. Nicotine Tob. Res. (2010) 12:679–83. doi: 10.1093/ntr/ntq066
40. Machado NA, Fonseca RB, Branco CA, Barbosa GA, Fernandes Neto AJ, Soares CJ. Dental wear caused by association between bruxism and gastroesophageal reflux disease: a rehabilitation report. J. Appl. Oral Sci. (2007) 15:327–33. doi: 10.1590/S1678-77572007000400016
41. Martynowicz H, Gac P, Brzecka A, Poreba R, Wojakowska A, Mazur G, et al. The relationship between sleep bruxism and obstructive sleep apnea based on polysomnographic findings. J. Clin. Med. (2019) 8:1653. doi: 10.3390/jcm8101653
42. Ahlberg J, Lobbezoo F, Ahlberg K, Manfredini D, Hublin C, Sinisalo J, et al. Self-reported bruxism mirrors anxiety and stress in adults. Med. Oral Patol. Oral Cir. Bucal. (2013) 18:e7–11. doi: 10.4317/medoral.18232
43. Rintakoski K, Kaprio J. Legal psychoactive substances as risk factors for sleep-related bruxism: a nationwide Finnish Twin Cohort study. Alcohol. Alcohol. (2013) 48:487–94. doi: 10.1093/alcalc/agt016
Keywords: stress, bruxism, systematic review, meta-analysis, association
Citation: Chemelo VdS, Né YGdS, Frazão DR, Souza-Rodrigues RDd, Fagundes NCF, Magno MB, Silva CMTd, Maia LC and Lima RR (2020) Is There Association Between Stress and Bruxism? A Systematic Review and Meta-Analysis. Front. Neurol. 11:590779. doi: 10.3389/fneur.2020.590779
Received: 03 August 2020; Accepted: 07 September 2020;
Published: 07 December 2020.
Edited by:
Massimiliano Valeriani, Bambino Gesù Children Hospital (IRCCS), ItalyReviewed by:
Luiz Renato Paranhos, Federal University of Uberlandia, BrazilAli Sazci, Kocaeli University, Turkey
Copyright © 2020 Chemelo, Né, Frazão, Souza-Rodrigues, Fagundes, Magno, Silva, Maia and Lima. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rafael Rodrigues Lima, cmFmYWxpbWFAdWZwYS5icg==