 Aleksandra Pogoda-Wesołowska1*
Aleksandra Pogoda-Wesołowska1* Adam Stępień1
Adam Stępień1 Marcin Wnuk2
Marcin Wnuk2 Monika Marona2
Monika Marona2 Elżbieta Tokarz-Kupczyk3Karolina Piasecka-Stryczyńska3
Elżbieta Tokarz-Kupczyk3Karolina Piasecka-Stryczyńska3 Konrad Rejdak4
Konrad Rejdak4 Anna Jamroz-Wiśniewska4
Anna Jamroz-Wiśniewska4 Monika Adamczyk-Sowa5Katarzyna Kubicka-Bączyk5
Monika Adamczyk-Sowa5Katarzyna Kubicka-Bączyk5 Iwona Kurkowska-Jastrzębska6Katarzyna Kurowska6Przemysław Puz7Alina Kułakowska8
Iwona Kurkowska-Jastrzębska6Katarzyna Kurowska6Przemysław Puz7Alina Kułakowska8 Monika Chorąży8
Monika Chorąży8 Waldemar Brola9Halina Bartosik-Psujek10
Waldemar Brola9Halina Bartosik-Psujek10- 1Department of Neurology, Military Institute of Medicine, Warsaw, Poland
- 2Department of Neurology, Jagiellonian University Medical College, University Hospital in Krakow, Kraków, Poland
- 3Department of Neurology, Poznan University of Medical Sciences, Poznan, Poland
- 4Department of Neurology, Medical University of Lublin, Lublin, Poland
- 5Department of Neurology, Faculty of Medical Sciences in Zabrze, Medical University of Silesia in Katowice, Katowice, Poland
- 6Department of Neurology, Institute of Psychiatry and Neurology, Warsaw, Poland
- 7Department of Neurology, Upper Silesian Medical Centre of the Silesian Medical University in Katowice, Katowice, Poland
- 8Department of Neurology, Medical University of Bialystok, Białystok, Poland
- 9Department of Neurology, Jan Kochanowski University, Kielce, Poland
- 10Department of Neurology, Institute of Medical Sciences, University of Rzeszow, Rzeszów, Poland
Introduction: Cladribine tablets (CladT) are a high-efficacy disease-modifying therapy recommended for the treatment of relapsing–remitting multiple sclerosis (RRMS) particularly in early disease. This study is aimed to evaluate the long-term efficacy of CladT in population of Polish RRMS patients, with more advanced disease.
Methods: This retrospective observational study included patients with RRMS who started CladT treatment between December 2019 and November 2023. Collected data included prior treatments, annualized relapse rate (ARR), magnetic resonance imaging (MRI) activity, Expanded Disability Status Scale (EDSS) score, no evidence of disease activity (NEDA-3), lymphocyte counts, and safety outcomes were collected.
Results: Of the 230 patients (8.3% treatment-naïve, mean disease duration 9.2 years), follow-up data were available up to year 1 for 222 patients, year 2 for 154 patients, year 3 for 87 patients and year 4 for 31 patients. The ARR decreased from 1.42 at baseline to 0.26, 0.22, and 0.36 in years 1, 2, and 3, respectively. The proportion of relapse-free patients increased from 13.9% at baseline to 76.8% in year 1, 82% in year 2 and 75.4% in year 3 with no relapses reported in year 4. The proportion of patients with active MRI lesions declined from 90.4% at baseline to 36.3% in year 1, 25.2% in year 2, 45.9% in year 3 and 8.3% in year 4. Stable or improved EDSS was observed in 85.9% of patients in year 1, 80.8% in year 2, 73.7% in year 3 and 88.9% in year 4. NEDA-3 status was achieved in 47.4% of patients in year 1, 51.0% in year 2, 40.4% in year 3 and 71.4% in year 4. Adverse events were reported in 16.7% of patients in years 1–2 and in 6.3% of patients in year 3.
Discussion: The results indicate that CladT is effective and safe in Polish patients with RRMS, characterized by high disease activity, delayed treatment initiation, and multiple number of prior therapies.
1 Introduction
Multiple sclerosis (MS) is a chronic neurodegenerative disorder of the central nervous system that progressively leads to neurological deficits (1). It is characterized by recurrent episodes of inflammatory demyelination in the brain and spinal cord (2, 3).
Cladribine is a synthetic purine nucleoside analogue that induces transient lymphocyte apoptosis and depletion (4). Cladribine tablets (CladT) 10 mg (3.5 mg/kg cumulative dose over 2 years), approved in the European Union in 2017 and in the United States in 2019 for the treatment of adult patients with highly active relapsing forms of MS, have now gained marketing authorization in over 80 countries (5–8). As of the end of June 2024, approximately 101,132 patients have received CladT, with 251,900 patient-years of exposure since its approval (9).
CladT is a highly effective disease-modifying therapy (DMT) that acts as an immune reconstitution therapy. Unlike most other high-efficacy DMTs that act via continuous immunosuppression, CladT is administered orally in 2 short treatment courses over 2 years (8–10 days annually) (10–12). While offering an advantage of only a few treatment days per year (8 to 10), it offers a sustained therapeutic effect that may persist for up to 4 years, with no need for further treatment during that period (10, 12–14).
CladT is effective in relapsing–remitting MS (RRMS), reducing relapse rates, MRI activity, and disability progression (15–17). In patients with a first clinical demyelinating event, it was shown to reduce the risk of conversion to clinically definite MS and has a favorable safety profile (14, 18). Early initiation - especially in treatment-naïve patients or those with limited prior DMT exposure is associated with better outcomes (12, 13, 19, 20). Therefore, CladT is recommended for patients with active RRMS, including those with one relapse and MRI activity within the past year (21–23).
At the time of data collection, in Poland, under the national drug program, CladT could be offered to MS patients in whom other DMTs had been ineffective, as defined by at least 1 clinical relapse in the previous 12 months and at least 1 new gadolinium-enhancing (Gd+) lesion or at least 2 new T2 lesions. In treatment-naïve patients, CladT might be prescribed to those with at least 2 clinical relapses in the previous 12 months and an Expanded Disability Status Scale (EDSS) score between 0 and 4.5, or to those with at least 2 relapses requiring steroid treatment and at least 1 new Gd + lesion or at least 2 new T2 lesions (24). Consequently, all treatment-naïve patients in our cohort had highly active disease and many exhibited rapidly evolving severe MS.
The profile of MS patients treated with CladT in Poland differs markedly from populations commonly described in previous studies, which often focus on individuals in earlier stages of the disease. Consequently, there is a need for real world evidence (RWE) data to evaluate the clinical efficacy of CladT in patients with more advanced MS. Furthermore, the long-term effectiveness of CladT, particularly in previously treated patients, remains underexplored. This study was designed to address these gaps by assessing the long-term efficacy of CladT in a population of Polish RRMS patients with advanced disease and extensive prior treatment history.
2 Materials and methods
2.1 Study design
This retrospective observational study was conducted at 10 MS clinical centers in Poland and involved a cohort of all patients with RRMS who started treatment with CladT between December 2019 and November 2023.
One treatment course consisted of 2 cycles. All diagnoses were made according to the McDonald criteria (2017 update) (25). The study was approved by the Ethics Committee of the Polish Military Medical Chamber (approval number 235/22).
2.2 Data collection
The following data were collected: demographic characteristics; disease duration; number of previous MS therapies; the last DMT used before starting CladT treatment and the reason for switching; number of relapses in the past 12 months before CladT initiation and at 12, 24, 30, 36, 42, and 48 months after starting treatment; EDSS scores before CladT initiation and at 12, 24, 30, 36, 42, and 48 months; lymphocyte count before CladT initiation and at 2, 6, 12, 14, 18, 30, 36, 42, and 48 months; MRI assessments in the past 12 months before CladT initiation and at 12, 24, 36, and 48 months; adverse events (AEs); history of COVID-19 infection and SARS-CoV-2 vaccination; and discontinuation of CladT treatment or change to another DMT within the first 2 years of treatment and in the third and fourth years of treatment.
The differences in the number of patients evaluated for various parameters at the same time point stem from instances where certain parameters could not be assessed for specific patients due to data unavailability. As a result, the analyses for those parameters at that time point may include differing patient populations.
2.3 Definitions
Active MRI lesions were defined as Gd + lesions or as new or enlarging T2 lesions. No evidence of disease activity (NEDA-3) was defined as no relapses, no disability progression, and no active MRI lesions. The denominator for percentage calculations in a given year includes the total number of patients who achieved NEDA-3 and those who did not, provided that at least one of the three component parameters (number of relapses, MRI activity, or EDSS assessment) was available and indicated failure to meet the NEDA-3 criteria.
According to previous reports (26), changes in EDSS scores were classified as improvement or worsening as follows: for patients with a baseline EDSS score of 0, a change of at least 1.5 points; for patients with a baseline EDSS score of 0.5 to 4.5, a change of at least 1 point; and for patients with a baseline EDSS score of 5 or higher, a change of at least 0.5 points. EDSS changes that did not meet the criteria for improvement or worsening were classified as stable EDSS.
The degrees of lymphopenia were defined as follows: grade I (<1.0–0.8 × 109/L); grade II (<0.8–0.5 × 109/L); grade III (<0.5–0.2 × 109/L); and grade IV (<0.2 × 109/L) (27). The incidence of lymphopenia was assessed in patients whose lymphocyte counts were measured 2 months after the first treatment cycle or later, considering the lowest lymphocyte count recorded for each patient.
2.4 Statistical analysis
Descriptive data were presented as means and standard deviations (SDs) or medians and interquartile ranges (IQRs). The annualized relapse rate (ARR) with 95% confidence intervals (CIs) was calculated using a negative binomial regression model for the 12 months before CladT initiation and for the first, second, third-, and fourth years following treatment initiation. To compare ARR and EDSS results in years 1, 2, 3, and 4 of CladT treatment with the results before treatment initiation, the Wilcoxon test was used. A p-value of less than 0.05 was considered significant. Analyses were conducted using IBM SPSS Statistics (version 24.0.0.1) and the R (version 4.3.3) software.
3 Results
3.1 Patient characteristics
Overall, 230 patients were included in the study, and follow-up data were available 1 for 222 patients at year, 2 for 154 patients at year 2, for 87 patients at year 3, and for 31 patients at year 4 (Figure 1) with median follow-up 24 months. Women constituted 77.8% of patients. The mean age of patients was 37.7 years (SD, 10.7 years). Until 2023, the mean disease duration was 9.2 years (SD, 5.9 years). The mean time between diagnosis and treatment initiation was 1.4 years (SD, 3.8 years), between treatment initiation and switching to CladT – 6.1 years (SD, 4.5 years), and between diagnosis and switching to CladT – 7.5 years (SD, 5.9 years). Only 8.3% of patients were treatment-naïve and most of them (11/19) had rapidly evolving severe disease. Before switching to CladT, most patients (69.2%) received 1 or 2 other DMTs, and the remaining 22.6% of patients received 3 or more DMTs. The most frequent DMTs were dimethyl fumarate (44.1%), fingolimod (14.7%), and teriflunomide (10.9%). In most cases (87.2%), the reason for switching to CladT was the inefficacy of previous therapy. Most patients (60.0%) received the full treatment of 4 cycles, and 1 patient received 6 cycles. The remaining patients were in earlier stages of treatment (Figure 1; Table 1).
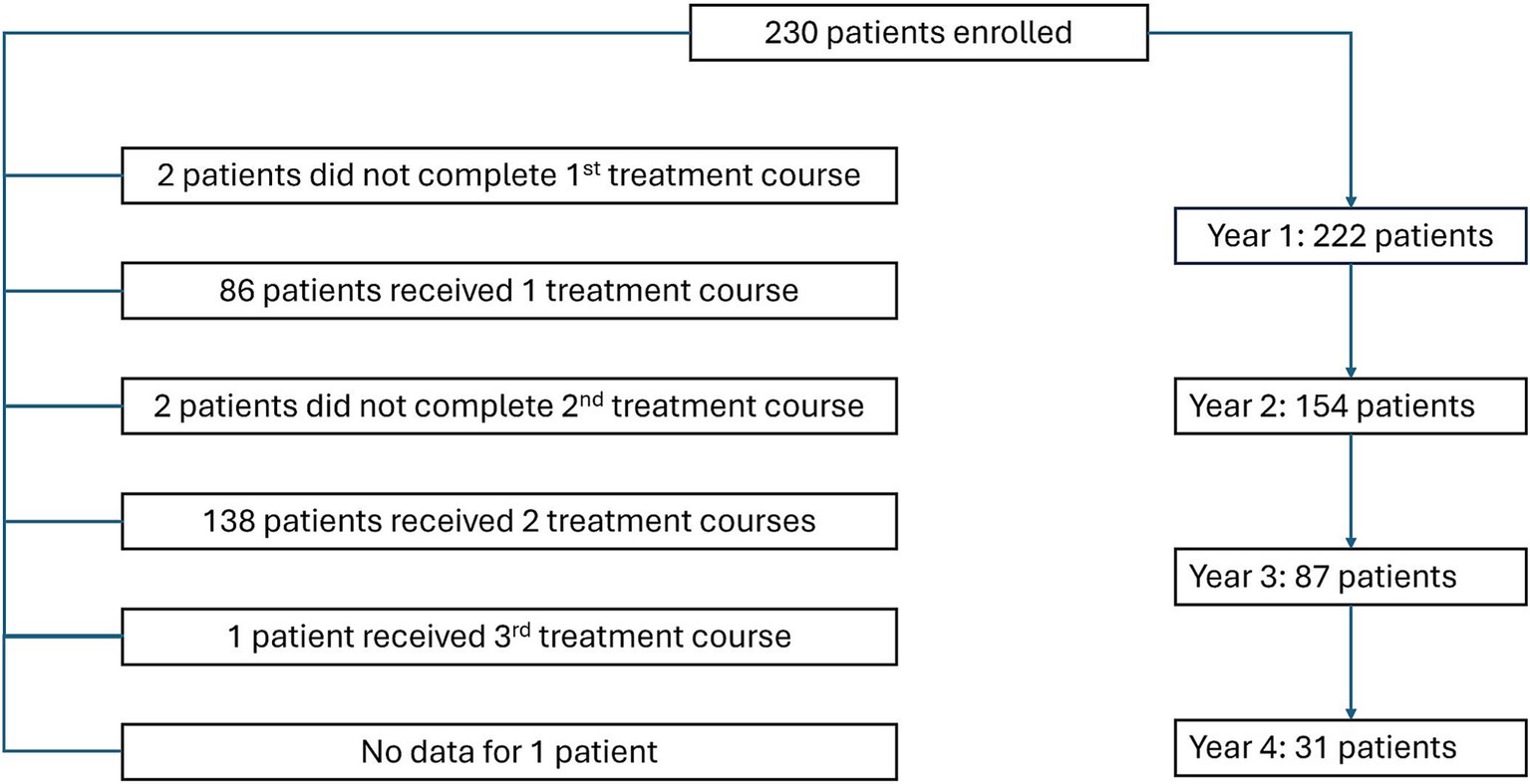
Figure 1. Flow diagram showing disposition of patients enrolled in the study.
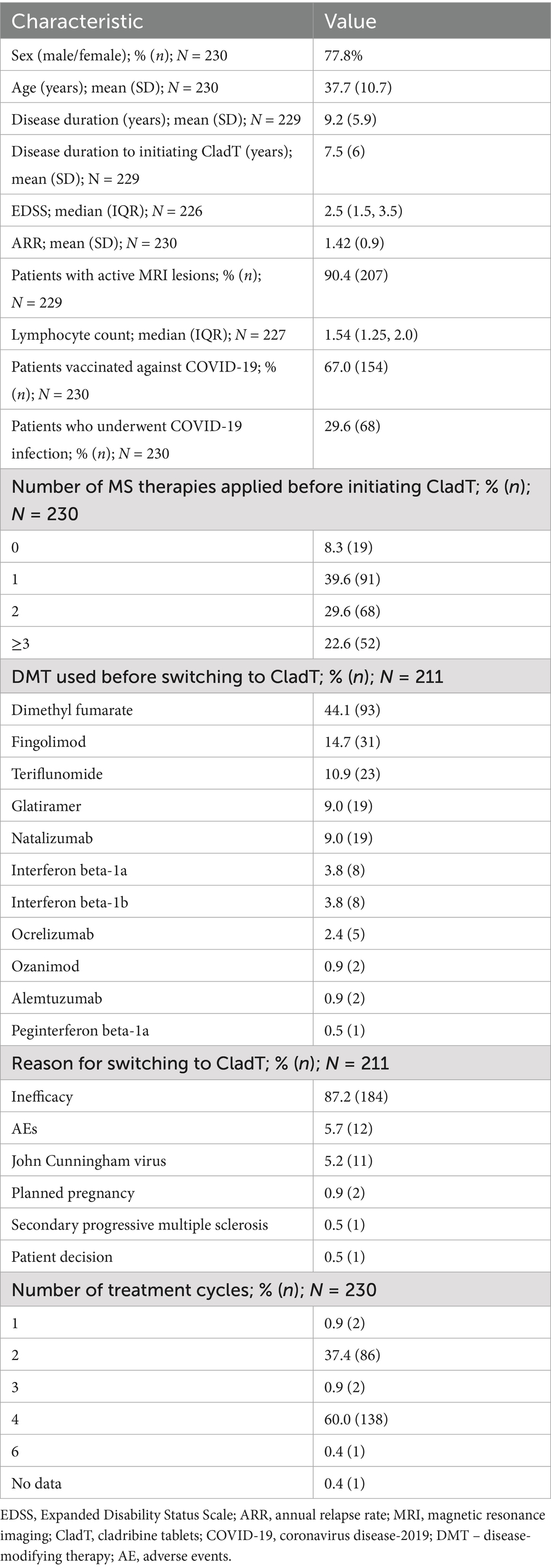
Table 1. Baseline characteristics of patients.
3.2 Treatment efficacy
During CladT treatment, the ARR decreased from 1.42 (95% CI: 1.28–1.58) at baseline to 0.26 (95% CI: 0.2–0.35) in year 1 (p < 0.001), 0.22 (95% CI: 0.15–0.32) in year 2 (p < 0.001), and 0.36 (95% CI: 0.24–0.55) in year 3 (p < 0.001; Figure 2A). The proportion of relapse-free patients increased from 13.9% at baseline to 76.8% in year 1, 82% in year 2, and 75.4% in year 3 (Figure 2B). There were no relapses in year 4. The proportion of patients with active MRI lesions decreased from 90.4% at baseline to 36.3% in year 1 and 25.2% in year 2, increased slightly to 45.9% in year 3, and decreased to 8.3% in year 4 (Figure 2C). Compared with baseline, the median EDSS score did not change in year 1 (2.5 [IQR, 1.5–4.0], p = 0.73) and year 2 (3 [IQR, 1.5–4.0], p = 0.25), but changed significantly in year 3 (3.0 [IQR, 2.0–4.0], p < 0.01). Stable or improved EDSS scores were observed in 85.9% of patients in year 1, 80.8% of patients in year 2, 73.7% of patients in year 3, and 88.9% of patients in year 4 (Figure 2D). NEDA-3 was achieved in 47.4% of patients in year 1, 51.0% of patients in year 2, 40.4% of patients in year 3, and 71.4% of patients in year 4 (Figure 2E).
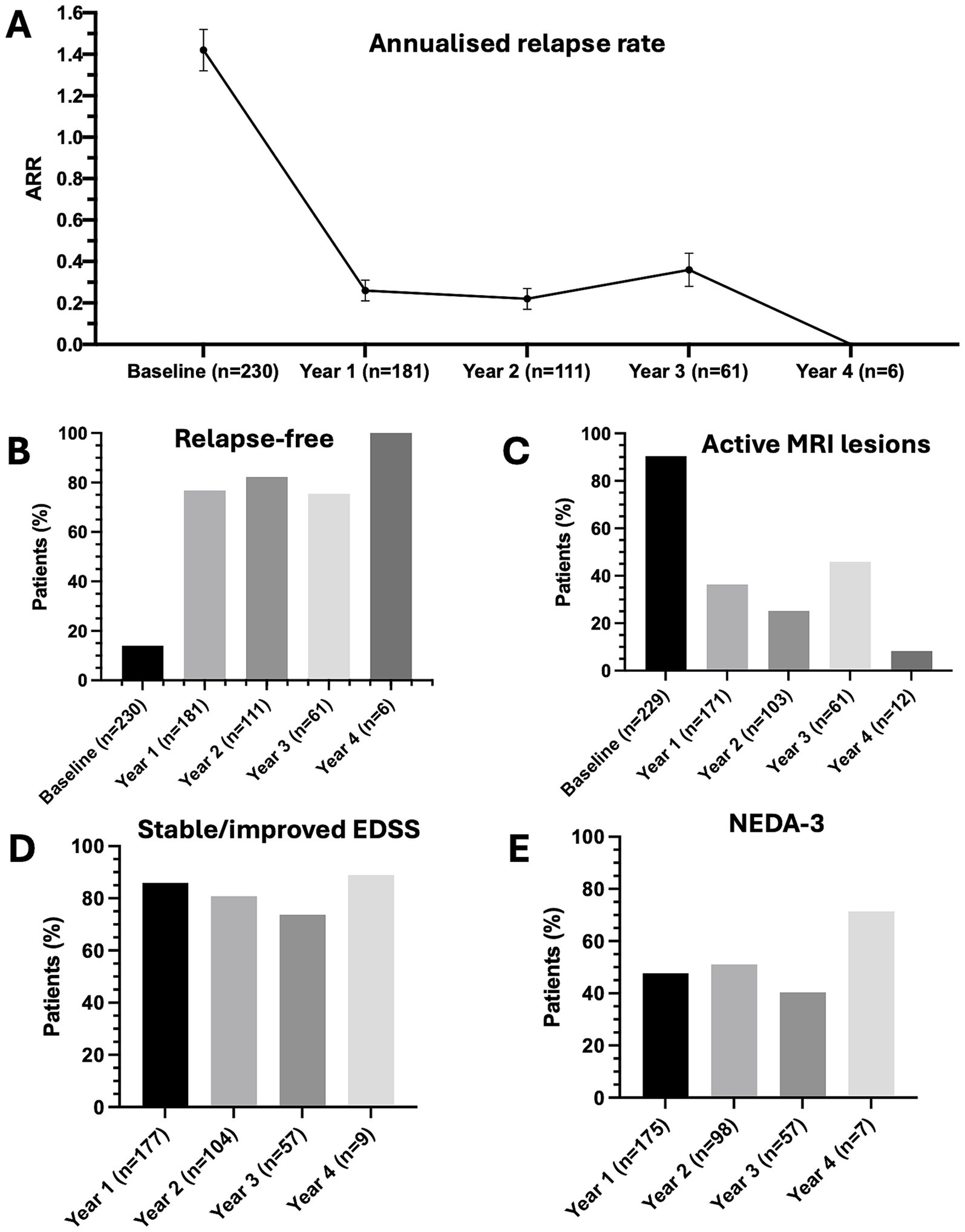
Figure 2. Efficacy outcomes after treatment with cladribine tablets. (A) Annualized relapse rate — point estimates are means and error bars are 95% confidence intervals. (B) Rate of relapse-free patients. (C) Rate of patients with active MRI lesions. (D) Rate of patients with stable/improved EDSS. (E) Percentage of patients with NEDA-3.
3.3 Safety
The median lymphocyte count decreased from 1.54 at baseline to 0.87 at month 2 and 0.71 in month 14. It subsequently started to increase and reached the baseline level by month 42 (Supplementary Figure 1).
Lymphocyte counts were within the reference range for 15.6% of patients, while 19.3% had grade 1 lymphopenia, 43.6% had grade 2 lymphopenia, 20.6% had grade 3 lymphopenia, and 0.9% had grade 4 lymphopenia. In years 1 and 2, lymphopenia occurred in 29.7% of patients. Grade 3 and 4 lymphopenia was reported only through month 18. The rates of lymphopenia during the study are presented in Supplementary Figure 2. Overall, AEs occurred in 37 patients (16.7%) in years 1 and 2 and in 4 patients (6.3%) in year 3. There were no AEs in year 4. Fatigue, herpes zoster infection, headache, and urinary tract infections were observed in 8.1% of patients each. Elevated liver enzymes, herpes simplex infection, and nausea were recorded in 5.4% of patients. There were also single cases of unspecified infections and COVID-19, eyeball pain, recurrent herpes simplex infection, drowsiness, skin rash, and dizziness.
Overall, 77.4% of patients completed or continued CladT treatment without switching to another therapy or starting another treatment during follow-up. The remaining 14.3% of patients discontinued treatment with CladT and/or switched to another DMT, while no data were available for 8.3% of patients (Table 2). Eleven patients (5%) discontinued treatment during years 1 and 2, 22% (17 of 79 patients) during year 3, and another 14% (5 of 36) during year 4. The reasons for discontinuation in years 1 and 2 were inefficacy (45.5%, 5 patients), patient decision (18.2%, 2 patients), and in 36.4% of cases (4 patients), the reason was unknown. In 30 patients, CladT was switched to another DMT, including ocrelizumab (50%), natalizumab (6.7%), fingolimod (3.3%), or mitoxantrone (3.3%). No data on subsequent treatment were available for 36.7% of cases. Among the 30 patients who switched from cladribine to another DMT, reasons for treatment discontinuation were documented only within the first 2 years of follow-up. Within this period, the reported reasons included lack of efficacy in 4 patients (13.3%), lymphopenia in 1 patient (3.3%), and a diagnosis of primary progressive multiple sclerosis in 1 patient (3.3%). In 5 cases (16.7%), no specific reason for discontinuation was recorded. In the remaining 19 patients (63.3%), cladribine treatment was not discontinued during the first 2 years, and therefore no data on the reasons for discontinuation were available for these individuals.
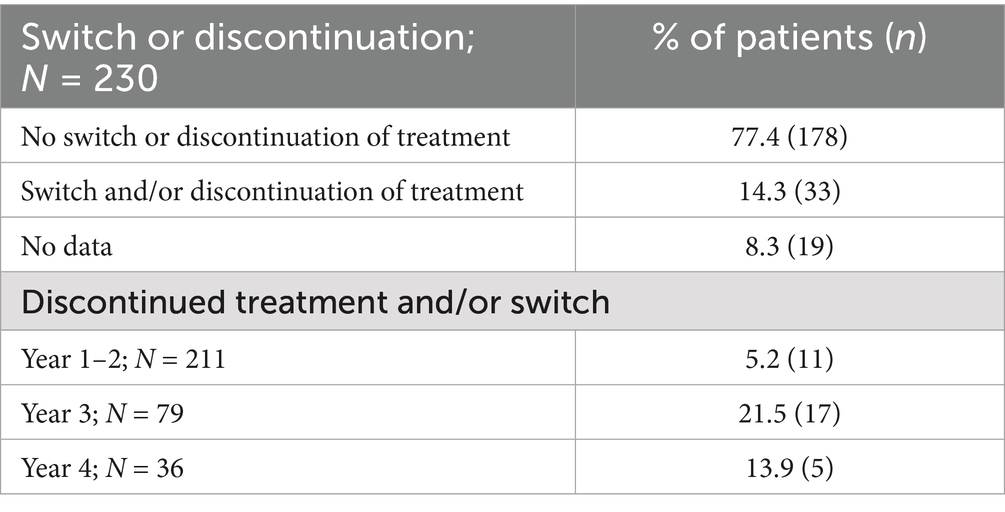
Table 2. Patient compliance with cladribine tablets treatment.
4 Discussion
RWE data is important for understanding the effectiveness and safety of medications, as they better reflect clinical practice than clinical trials. This study presents long-term data on the efficacy and safety of CladT treatment in Polish patients with MS.
Due to reimbursement rules in Poland, the use of CladT in patients with early-stage disease was very limited. Although these criteria have evolved over time, they remained conservative at the time of data collection, restricting access to CladT treatment primarily to patients with highly active and advanced disease, for whom the potential treatment benefits are relatively limited. Consequently, CladT treatment was initiated much later in Poland compared to standard care. As a result, our study population was suboptimal for evaluating CladT treatment efficacy compared to most available studies. Recruited patients were characterized by relatively long disease duration, a prolonged interval before CladT initiation, a high baseline ARR, and a very low proportion of treatment-naïve individuals, with over 50% of patients having received 2 or more other therapies prior starting CladT. Highly effective treatments, including fingolimod, natalizumab, ocrelizumab, ozanimod, and alemtuzumab, were previously used in 28% of patients, with most switching to CladT due to inefficacy of previous therapy. Several authors reported better treatment outcomes in treatment-naïve patients and those switching from first-line therapies compared to those switching from second-line therapies (12, 13, 20, 28–30). Treatment-naïve patients with 2 relapses in the previous 12 months, as well as those with 1 relapse and 1 or 2 poor prognostic factors (such as age >40 years, male sex, smoking, relapse severity and high lesion load) were suggested as good candidates for CladT treatment in contrast to patients who had experienced more than 2 relapses within the last 12 months (21). Despite the suboptimal characteristics of our sample, CladT treatment proved to be highly effective: 2 years after treatment onset, 51.0% of patients achieved NEDA-3, 82% were free from relapses, 80.8% remained free from EDSS progression, and 74.8% had no disease activity on MRI. These results are consistent with other studies demonstrating the clinical efficacy of CladT (11, 13, 15, 19, 20, 23, 29, 31, 32).
In presented study, 77.4% of patients completed or continued CladT treatment without switching to another therapy during the follow-up period, which is in line with the CLASSIC-MS study (33). A total of 11 patients (5%) discontinued treatment in year 1 or 2, with 45.5% of these cases attributed to treatment inefficacy. Additionally, 22 patients switched to another treatment in years 3 and 4. The discontinuation and switching to other treatments can be explained by the different types of responses to CladT treatment demonstrated by our patients, as previously described. According to recommendations, patients showing greater disease activity after treatment initiation in year 1, as well as those with substantial activity in years 3 or 4, should be switched to an alternative therapy. However, patients showing moderate disease activity or stable disease in year 1, followed by moderate activity in year 2 or minor activity in years 3 or 4 should receive additional CladT courses rather than be switched to another therapy (34–36). Importantly, some of our patients started their treatment in 2019 and 2020, when clinical management during longer follow-up and responses to treatment had not yet been established. Current recommendations state that the full cumulative dose of CladT should be administered even if disease activity occurs between the first and second courses (36, 37). Furthermore, treatment efficacy should be assessed only after 2 full cladribine courses, typically no earlier than 14 months after treatment initiation (21). The reappearance of disease activity in year 3, as observed in our study, has also been reported by other authors (13, 38, 39). This response pattern may be characteristic of mid-term responders, according to the classification proposed by German experts (34, 35). In such cases, it is recommended to continue yearly follow-ups and either administer additional CladT courses (in cases of minor activity without safety concerns) or switch to another DMT (if significant disease activity is present) (34, 35).
To our knowledge, the presented analysis was the first RWE study in Poland and represented a continuation of our research, which was published in 2023 (40). As mentioned in the introduction, at the time of data collection in Poland, according to the drug program, CladT could be offered to MS patients who had failed other DMTs due to inefficacy or previously untreated patients with had highly active disease or even rapidly evolving severe form of the disease. As a result, the profile of MS patients treated with CladT in Poland differed significantly from the populations most described in the literature, which often focuses on patients in earlier stages of the disease. In our analysis patients were older, with a longer disease duration and mostly previously treated. Moreover, this study was characterized by longer follow-up period.
Similarly to our results, in the study conducted by Magalashvili et al., among 128 patients with highly active MS that received CladT treatment, clinical outcomes were assessed in 61 patients at year 3 and in 35 patients at year 4 (32). At treatment initiation, the mean age was 39.6 years, disease duration was 12.7 years, EDSS was 3.7, and the ARR was 1.6. In addition, in study by Liza et al. the patients included in the study were an older population with a higher disability rate (11). However, the study also included patients with secondary progressive MS (SPMS), and the follow-up time was shorter (2 years). Furthermore, results from the study by Santos et al. showed that mean disease duration at CladT initiation was 8.9 and most patients (86.1%) were not treatment-naïve (31). However, 88.5% patients were diagnosed with RRMS and 11.5% with SPMS.
In contrast, in the study of Pfeuffer et al. (12), patients had lower disease activity and a shorter disease duration. The follow-up period was also shorter than in our study. Moreover, among the patients included in the study by Zanetta et al. (13), half of the patients were treatment-naïve. Like our findings, the previously untreated group was characterized by higher disease activity, but the follow-up time was limited to only 25 months. In turn, in the study by Petracca et al. (20), untreated patients (29.3%) were significantly younger and had a shorter disease duration compared to those switching from other therapies (32.86 vs. 35.7 years, p = 0.02 and 1.54 vs. 8.74 years p < 0.0001, respectively) as in our study. However, treatment-naïve patients and previously treated patients did not differ for ARR, presence of active lesions, or EDSS at baseline. Additionally, observation period in that study was only 22 months.
There is a paucity of studies evaluating the long-term efficacy of CladT. Studies with follow-up of beyond 36 months have reported a decline in the proportion of NEDA-3 patients, relapse-free patients, and patients with stable EDSS score between years 2 and 5 (26, 38, 39, 41). Additionally, a recent meta-analysis of CladT efficacy showed consistently better outcomes in studies with less than 24 months of follow-up than in studies with longer follow-up (42). These findings suggest that some patients may need additional CladT courses beyond the standard 2 courses given in years 1 and 2, supporting the recommendations proposed by German experts (34, 35). Further long-term studies are needed to clarify this issue.
Overall, CladT was well tolerated and demonstrated a favorable safety profile, consistent with previous reports (13, 15, 23). As in earlier studies, more patients reported AEs in years 1 and 2 than in year 3 (12, 13). The most common AEs were headache, fatigue, infections, nausea, and elevated liver enzymes, in line with previous data (13, 19, 29, 31, 43, 44). No additional AEs, including serious AEs, were reported in our cohort. These findings support the favorable safety profile of CladT in a population characterized by older age, longer disease duration, and more extensive prior treatment than in most other studies.
Lymphopenia is an expected effect of CladT treatment due to its mechanism of action (44). The initial decrease in lymphocyte counts after each CladT course, followed by gradual recovery, represents a typical pattern of lymphocyte kinetics after CladT exposure (12, 13, 20, 45, 46). Consistent with other reports, peaks of lymphopenia appearing in months 2 and 14 were observed (12, 13). In our cohort, 20.6% of patients experienced grade 3 lymphopenia, which is in line with other studies (12, 15, 19, 47), although some authors reported lower rates (13, 20, 48). Grade 4 lymphopenia was rare and transient, with an observed rate of 0.9%, confirming earlier findings (12, 13, 15, 19, 20, 47, 48). Additionally, as observed in other studies, a higher rate of grade 3 and 4 lymphopenia in year 2 compared to year 1 was observed (45). It has been reported that lymphopenia was more common in previously treated patients than in treatment-naïve individuals (12, 13, 48), with a higher number of previous therapies being a predictor of grade 3 lymphopenia (13). Despite the high proportion of first- and second-line switchers in our population, our data suggested a safety profile comparable to that reported by other studies.
The main limitation of our study was the small number of patients over the long follow-up period. As the population of Polish patients treated with CladT increases over time, future studies should provide more insights into the long-term efficacy of CladT treatment in Polish patients with RRMS.
In conclusion, our results suggested that CladT was effective and safe in the Polish population of RRMS patients characterized by high disease activity, late treatment initiation, and multiple previous therapies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the 116 Polish Military Medical Chamber (approval number 235/22). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin because it was retrospective observational study.
Author contributions
AP-W: Data curation, Investigation, Resources, Visualization, Writing – review & editing. AS: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing. MW: Data curation, Writing – review & editing. MM: Data curation, Writing – review & editing. ET-K: Data curation, Writing – review & editing. KP-S: Data curation, Writing – review & editing. KR: Data curation, Writing – review & editing. AJ-W: Data curation, Writing – review & editing. MA-S: Data curation, Writing – review & editing. KK-B: Data curation, Writing – review & editing. IK-J: Data curation, Writing – review & editing. KK: Data curation, Writing – review & editing. PP: Data curation, Investigation, Resources, Writing – review & editing. AK: Conceptualization, Methodology, Supervision, Writing – review & editing. MC: Investigation, Resources, Writing – review & editing. WB: Data curation, Writing – review & editing. HB-P: Data curation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research and medical writing were financially supported by Merck Sp. z o.o., Warsaw, Poland, an affiliate of Merck KGaA, Darmstadt, Germany (CrossRef Funder ID: 10.13039/100009945), who also reviewed the manuscript content during its development and submission.
Acknowledgments
The authors would like to thank Iwona Kołodziejczyk and Michał Piotrowski, PhD, of Proper Medical Writing Sp. z o. o. for their support in preparation of this manuscript (including text editing and graphical data presentation).
Conflict of interest
AP-W has participated in workshops and conferences and has provided articles and lectures for Novartis, Roche, Bristol Myers Squibb, Biogen, and Merck. AS in relation to the content of this publication, has served as a lecturer and an expert at advisory boards for Allergan, Amgen, Bayer, Novartis, Biogen, Merck, Polpharma, Roche, Teva, and Eli Lilly. MW has received lecture fees and sponsored participation in conferences from Bayer, Biogen, Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. He has also received consultation fees from Amgen, Biogen, Merck, Novartis, and Roche, and grants from the National Centre for Research and Development (no. SZPITALE-JEDNOIMIENNE/18/2020) and Medical Research Agency (no. 2020/ABM/01/00006)”. MM received compensation for preparing training sessions, workshops, and financial support related to participation in scientific conferences from Biogen, Roche, Novartis, and Merck. ET-K has delivered lectures sponsored by pharmaceutical companies during workshops, conferences, and Round Table meetings. She has cooperated with Biogen Poland, Roche Polska, Novartis Poland, Bristol Myers Squibb, Merck, and Janssen-Cilag Polska in this capacity. She also participated in the ECTRIMS conference sponsored by Merck and the XXV Congress of the Polish Neurological Society sponsored by Bristol Myers Squibb. KR has received speaking honoraria and travel expenses for participation in scientific meetings and has participated in advisory boards in the past years with Bayer, Biogen, Merck Healthcare KGaA (Darmstadt, Germany), Novartis, Roche, Sanofi-Genzyme, and Teva Pharmaceutical. AJ-W has received honoraria for lectures and has taken part in conferences organized by the following pharmaceutical companies: Bayer, Biogen, BMS, Merck, Novartis, Roche, Sandoz, and Teva. MA-S has received compensation for speaking and consulting services from Biogen, Bayer, Novartis, Roche, Merck, Teva, Sanofi-Genzyme, and BMS. None of the consulting agreements are relevant to the submitted work. KK-B has received compensation for preparing training sessions and workshops, as well as financial support for participation in scientific conferences, from Biogen, Roche, Novartis, and Merck. IK-J has received speaker honoraria from a company for lectures, though these were not directly connected to the above publication. AK has received compensation for speaking and consulting services from Biogen, Bayer, Novartis, Roche, Merck, Teva, and Sanofi-Genzyme. WB discloses involvement in scientific advisory boards for Biogen, Roche, Novartis, and Merck. He also receives honoraria for lecturing from Biogen, Merck, Novartis, Sanofi Genzyme, and Roche. HB-P has received advisory board and/or speaker honoraria from Biogen, BMS, Novartis, Merck, and Roche, as well as support for congress participation from Novartis.
The authors declare that this study received funding from Merck Sp.z.o.o., Warsaw, Poland, an affiliate of Merck KgaA, Darmstadt, Germany. The funder had the following involvement in the study: statistical analysis and medical writing.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1626317/full#supplementary-material
References
1. Haki, M, Al-Biati, HA, Al-Tameemi, ZS, Ali, IS, and Al-Hussaniy, HA. Review of multiple sclerosis: epidemiology, etiology, pathophysiology, and treatment. Medicine. (2024) 103:e37297. doi: 10.1097/md.0000000000037297
2. Kalinowska-Łyszczarz, A, Guo, Y, and Lucchinetti, CF. Update on pathology of central nervous system inflammatory demyelinating diseases. Neurol Neurochir Pol. (2022) 56:201–9. doi: 10.5603/PJNNS.a2022.0046
3. Reich, DS, Lucchinetti, CF, and Calabresi, PA. Multiple Sclerosis. N Engl J Med. (2018) 378:169–80. doi: 10.1056/NEJMra1401483
4. Karussis, D. Multiple Sclerosis In: SR Quah, editor. International encyclopedia of public health. Second ed. Oxford: Academic Press (2017). 145–79.
5. Moccia, M, Lanzillo, R, Petruzzo, M, Nozzolillo, A, De Angelis, M, Carotenuto, A, et al. Single-center 8-years clinical follow-up of Cladribine-treated patients from phase 2 and 3 trials. Front Neurol. (2020) 11:489. doi: 10.3389/fneur.2020.00489
6. Oreja-Guevara, C, Brownlee, W, Celius, EG, Centonze, D, Giovannoni, G, Hodgkinson, S, et al. Expert opinion on the long-term use of Cladribine tablets for multiple sclerosis: systematic literature review of real-world evidence. Mult Scler Relat Disord. (2023) 69:104459. doi: 10.1016/j.msard.2022.104459
7. Rammohan, K, Coyle, PK, Sylvester, E, Galazka, A, Dangond, F, Grosso, M, et al. The development of Cladribine tablets for the treatment of multiple sclerosis: a comprehensive review. Drugs. (2020) 80:1901–28. doi: 10.1007/s40265-020-01422-9
8. Merck Europe B.V. Mavenclad (summary of product characteristics). Amsterdam, Netherlands: Merck Europe B.V. (2020).
9. Hillert, J, Butzkueven, H, Magyari, M, Wergeland, S, Moore, N, Soilu-Hänninen, M, et al. Harmonized data quality indicators maintain data quality in long-term safety studies using multiple sclerosis registries/data sources: experience from the clarion study. Clin Epidemiol. (2024) 16:717–32. doi: 10.2147/clep.S480525
10. Ciron, J, Bourre, B, Castelnovo, G, Guennoc, AM, De Sèze, J, Ben-Amor, AF, et al. Holistic, long-term Management of People with relapsing multiple sclerosis with Cladribine tablets: expert opinion from France. Neurol Ther. (2024) 13:503–18. doi: 10.1007/s40120-024-00589-7
11. Lizak, N, Hodgkinson, S, Butler, E, Lechner-Scott, J, Slee, M, McCombe, PA, et al. Real-world effectiveness of cladribine for Australian patients with multiple sclerosis: an Msbase registry substudy. Mult Scler. (2021) 27:465–74. doi: 10.1177/1352458520921087
12. Pfeuffer, S, Rolfes, L, Hackert, J, Kleinschnitz, K, Ruck, T, Wiendl, H, et al. Effectiveness and safety of Cladribine in Ms: real-world experience from two tertiary Centres. Mult Scler. (2022) 28:257–68. doi: 10.1177/13524585211012227
13. Zanetta, C, Rocca, MA, Meani, A, Martinelli, V, Ferrè, L, Moiola, L, et al. Effectiveness and safety profile of Cladribine in an Italian real-life cohort of relapsing-remitting multiple sclerosis patients: a monocentric longitudinal observational study. J Neurol. (2023) 270:3553–64. doi: 10.1007/s00415-023-11700-7
14. Leist, T, Cook, S, Comi, G, Montalban, X, Giovannoni, G, Nolting, A, et al. Long-term safety data from the Cladribine tablets clinical development program in multiple sclerosis. Mult Scler Relat Disord. (2020) 46:102572. doi: 10.1016/j.msard.2020.102572
15. Giovannoni, G, Comi, G, Cook, S, Rammohan, K, Rieckmann, P, Soelberg Sørensen, P, et al. A placebo-controlled trial of Oral Cladribine for relapsing multiple sclerosis. N Engl J Med. (2010) 362:416–26. doi: 10.1056/NEJMoa0902533
16. Comi, G, Cook, SD, Giovannoni, G, Rammohan, K, Rieckmann, P, Sørensen, PS, et al. Mri outcomes with Cladribine tablets for multiple sclerosis in the Clarity study. J Neurol. (2013) 260:1136–46. doi: 10.1007/s00415-012-6775-0
17. Jacobs, BM, Ammoscato, F, Giovannoni, G, Baker, D, and Schmierer, K. Cladribine: mechanisms and mysteries in multiple sclerosis. J Neurol Neurosurg Psychiatry. (2018) 89:1266–71. doi: 10.1136/jnnp-2017-317411
18. Clavelou, P, Castelnovo, G, Pourcher, V, De Sèze, J, Vermersch, P, Ben-Amor, AF, et al. Expert narrative review of the safety of Cladribine tablets for the Management of Relapsing Multiple Sclerosis. Neurol Ther. (2023) 12:1457–76. doi: 10.1007/s40120-023-00496-3
19. Rauma, I, Viitala, M, Kuusisto, H, Atula, S, Sipilä, JOT, Ryytty, M, et al. Finnish multiple sclerosis patients treated with Cladribine tablets: a Nationwide registry study. Mult Scler Relat Disord. (2022) 61:103755. doi: 10.1016/j.msard.2022.103755
20. Petracca, M, Ruggieri, S, Barbuti, E, Ianniello, A, Fantozzi, R, Maniscalco, GT, et al. Predictors of Cladribine effectiveness and safety in multiple sclerosis: a real-world, multicenter, 2-year follow-up study. Neurol Ther. (2022) 11:1193–208. doi: 10.1007/s40120-022-00364-6
21. Meca-Lallana, V, García Domínguez, JM, López Ruiz, R, Martín-Martínez, J, Arés Luque, A, Hernández Pérez, MA, et al. Expert-agreed practical recommendations on the use of Cladribine. Neurol Ther. (2022) 11:1475–88. doi: 10.1007/s40120-022-00394-0
22. Deleu, D, Garcia Canibano, B, Elalamy, O, Sayed Abdelmoneim, M, and Boshra, A. Practical guidance on the use of Cladribine tablets in the management or relapsing multiple sclerosis: expert opinion from Qatar. Degener Neurol Neuromuscul Dis. (2023) 13:81–8. doi: 10.2147/dnnd.S433459
23. Sørensen, PS, Centonze, D, Giovannoni, G, Montalban, X, Selchen, D, Vermersch, P, et al. Expert opinion on the use of Cladribine tablets in clinical practice. Ther Adv Neurol Disord. (2020) 13:1756286420935019. doi: 10.1177/1756286420935019
24. Polish Drug Programme Appendix B.29. Treatment of patients with multiple sclerosis (Icd-10: G35). (2023). Available online at: https://www.gov.pl/web/zdrowie/obwieszczenie-ministra-zdrowia-z-dnia-11-grudnia-2023-r-w-sprawie-wykazu-refundowanych-lekow-srodkow-spozywczych-specjalnego-przeznaczenia-zywieniowego-oraz-wyrobow-medycznych
25. Thompson, AJ, Banwell, BL, Barkhof, F, Carroll, WM, Coetzee, T, Comi, G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the Mcdonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/s1474-4422(17)30470-2
26. Giovannoni, G, Comi, G, Rammohan, K, Rieckmann, P, Dangond, F, Keller, B, et al. Long-term disease stability assessed by the expanded disability status scale in patients treated with Cladribine tablets 3.5 mg/kg for relapsing multiple sclerosis: an exploratory post hoc analysis of the Clarity and Clarity extension studies. Adv Ther. (2021) 38:4975–85. doi: 10.1007/s12325-021-01865-w
27. U.S. Department of Health and Human Services. (2017). Common terminology criteria for adverse events (Ctcae) version 5.0. Available online at: https://ctep.cancer.gov/Protocoldevelopment/Electronic_Applications/Docs/Ctcae_V5_Quick_Reference_5x7.Pdf. (Accessed November 12, 2024).
28. Vermersch, P, Galazka, A, Dangond, F, Damian, D, Wong, SL, Jack, D, et al. The effect of Cladribine tablets in people with more active multiple sclerosis: a plain language summary. Neurodegener Dis Manag. (2022) 12:285–93. doi: 10.2217/nmt-2022-0009
29. Al-Hashel, J, Ahmed, SF, AlMojel, M, and Alroughani, R. A prospective observational longitudinal study with a two-year follow-up of multiple sclerosis patients on Cladribine. Clin Neurol Neurosurg. (2023) 232:107885. doi: 10.1016/j.clineuro.2023.107885
30. Alonso, R, Casas, M, Lazaro, L, Fernandez Liguori, N, Pita, C, Cohen, L, et al. Achieving no evidence of disease Activity-3 in highly active multiple sclerosis patients treated with Cladribine and monoclonal antibodies. Mult Scler J Exp Transl Clin. (2023) 9:20552173231154712. doi: 10.1177/20552173231154712
31. Santos, M, Sequeira, J, Abreu, P, Guerreiro, R, Santos, M, Ferreira, J, et al. Safety and effectiveness of Cladribine in multiple sclerosis: real-world clinical experience from 5 tertiary hospitals in Portugal. Clin Neuropharmacol. (2023) 46:105–11. doi: 10.1097/wnf.0000000000000552
32. Magalashvili, D, Mandel, M, Dreyer-Alster, S, Didikin, M, Harari, G, Flechter, S, et al. Cladribine treatment for highly active multiple sclerosis: real-world clinical outcomes for years 3 and 4. J Neuroimmunol. (2022) 372:577966. doi: 10.1016/j.jneuroim.2022.577966
33. Giovannoni, G, Boyko, A, Correale, J, Edan, G, Freedman, MS, Montalban, X, et al. Long-term follow-up of patients with relapsing multiple sclerosis from the Clarity/Clarity extension cohort of Classic-Ms: an Ambispective study. Mult Scler. (2023) 29:719–30. doi: 10.1177/13524585231161494
34. Meuth, SG, Bayas, A, Kallmann, B, Kleinschnitz, C, Linker, R, Rieckmann, P, et al. Long-term Management of Multiple Sclerosis Patients Treated with Cladribine tablets: an expert opinion. Expert Opin Pharmacother. (2020) 21:1965–9. doi: 10.1080/14656566.2020.1792885
35. Meuth, SG, Bayas, A, Kallmann, B, Linker, R, Rieckmann, P, Wattjes, MP, et al. Long-term Management of Multiple Sclerosis Patients Treated with Cladribine tablets beyond year 4. Expert Opin Pharmacother. (2022) 23:1503–10. doi: 10.1080/14656566.2022.2106783
36. Kułakowska, A, Mirowska-Guzel, D, Adamczyk-Sowa, M, Bartosik-Psujek, H, Brola, W, Kalinowska, A, et al. Recommendation of polish clinical experts on the strategy of treatment with cladribine tablets depending on the patient’s characteristic. MS Rep. (2022) 11:5–10.
37. Pandit, L. No evidence of disease activity (Neda) in multiple sclerosis - shifting the goal posts. Ann Indian Acad Neurol. (2019) 22:261–3. doi: 10.4103/aian.AIAN_159_19
38. Giovannoni, G, Singer, BA, Issard, D, Jack, D, and Vermersch, P. Durability of no evidence of disease Activity-3 (Neda-3) in patients receiving Cladribine tablets: the Clarity extension study. Mult Scler. (2022) 28:1219–28. doi: 10.1177/13524585211049392
39. Patti, F, Visconti, A, Capacchione, A, Roy, S, and Trojano, M. Long-term effectiveness in patients previously treated with cladribine tablets: a real-world analysis of the Italian multiple sclerosis registry (clarinet-Ms). Ther Adv Neurol Disord. (2020) 13:1756286420922685. doi: 10.1177/1756286420922685
40. Stępień, A, Pogoda-Wesołowska, A, Tokarz-Kupczyk, E, Słowik, A, Puz, P, Adamczyk-Sowa, M, et al. Cladribine tablets for highly active relapsing-remitting multiple sclerosis in Poland: a real-world, multi-Centre, retrospective, cohort study during the COVID-19 pandemic. Neurol Neurochir Pol. (2023) 57:371–8. doi: 10.5603/PJNNS.a2023.0050
41. Giovannoni, G, and Mathews, J. Cladribine tablets for relapsing-remitting multiple sclerosis: a clinician's review. Neurol Ther. (2022) 11:571–95. doi: 10.1007/s40120-022-00339-7
42. Nabizadeh, F, Mohamadi, M, Rahmani, S, Rajabi, R, Afrashteh, F, Najdaghi, S, et al. Safety and efficacy of Cladribine in multiple sclerosis: a systematic review and Meta-analysis. Neurol Sci. (2023) 44:3045–57. doi: 10.1007/s10072-023-06794-w
43. Aerts, S, Khan, H, Severijns, D, Popescu, V, Peeters, LM, and Van Wijmeersch, B. Safety and effectiveness of Cladribine tablets for multiple sclerosis: results from a single-center real-world cohort. Mult Scler Relat Disord. (2023) 75:104735. doi: 10.1016/j.msard.2023.104735
44. Cook, S, Leist, T, Comi, G, Montalban, X, Giovannoni, G, Nolting, A, et al. Safety of Cladribine tablets in the treatment of patients with multiple sclerosis: an integrated analysis. Mult Scler Relat Disord. (2019) 29:157–67. doi: 10.1016/j.msard.2018.11.021
45. Giovannoni, G, Coyle, PK, Vermersch, P, Walker, B, Aldridge, J, Nolting, A, et al. Integrated lymphopenia analysis in younger and older patients with multiple sclerosis treated with Cladribine tablets. Front Immunol. (2021) 12:763433. doi: 10.3389/fimmu.2021.763433
46. Möhn, N, Skripuletz, T, Sühs, KW, Menck, S, Voß, E, and Stangel, M. Therapy with Cladribine is efficient and safe in patients previously treated with Natalizumab. Ther Adv Neurol Disord. (2019) 12:1756286419887596. doi: 10.1177/1756286419887596
47. Brochet, B, Solari, A, Lechner-Scott, J, Piehl, F, Langdon, D, Hupperts, R, et al. Improvements in quality of life over 2 years with Cladribine tablets in people with relapsing multiple sclerosis: the clarify-Ms study. Mult Scler. (2023) 29:1808–18. doi: 10.1177/13524585231205962
48. Brochet, B, Hupperts, R, Langdon, D, Solari, A, Piehl, F, Lechner-Scott, J, et al. Treatment satisfaction, safety, and tolerability of Cladribine tablets in patients with highly active relapsing multiple sclerosis: clarify-Ms study 6-month interim analysis. Mult Scler Relat Disord. (2022) 57:103385. doi: 10.1016/j.msard.2021.103385
Keywords: cladribine, relapsing-remitting multiple sclerosis, safety, efficacy, real world evidence
Citation: Pogoda-Wesołowska A, Stępień A, Wnuk M, Marona M, Tokarz-Kupczyk E, Piasecka-Stryczyńska K, Rejdak K, Jamroz-Wiśniewska A, Adamczyk-Sowa M, Kubicka-Bączyk K, Kurkowska-Jastrzębska I, Kurowska K, Puz P, Kułakowska A, Chorąży M, Brola W and Bartosik-Psujek H (2025) Cladribine tablets as therapy for advanced relapsing-remitting multiple sclerosis: a 4-year follow-up real-world, multi-center, retrospective, cohort study. Front. Neurol. 16:1626317. doi: 10.3389/fneur.2025.1626317
Edited by:
Marcello Moccia, University of Naples Federico II, ItalyReviewed by:
Xue Ma, The First Affiliated Hospital of Xi’an Jiaotong University, ChinaPatrick Vermersch, Université de Lille, France
Copyright © 2025 Pogoda-Wesołowska, Stępień, Wnuk, Marona, Tokarz-Kupczyk, Piasecka-Stryczyńska, Rejdak, Jamroz-Wiśniewska, Adamczyk-Sowa, Kubicka-Bączyk, Kurkowska-Jastrzębska, Kurowska, Puz, Kułakowska, Chorąży, Brola and Bartosik-Psujek. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aleksandra Pogoda-Wesołowska, YXBvZ29kYS13ZXNvbG93c2thQHdpbS5taWwucGw=