 Sarah Kassir
Sarah Kassir Yannick Béjot
Yannick Béjot- Université Bourgogne Europe, CHU Dijon Bourgogne, Service de Neurologie, Dijon Stroke Registry, Dijon, France
Preexisting cognitive impairment is a significant but often overlooked factor in the management and outcome of stroke patients. Patients with prior cognitive impairment suffering a stroke have less access to stroke units, and less administration of acute revascularization therapies, as a possible consequence of limited research on the benefits of these treatments in this specific population, with most data coming from observational studies. Prestroke cognitive impairment is associated with a greater clinical severity at onset, increased complications, and poorer survival and functional outcome, with a reduced access to rehabilitation services, and a greater need for institutionalization. Patients with preexisting cognitive impairment have more prevalent comorbidities and frailty, which contribute to their increased vulnerability to adverse health outcomes. Further research is needed to better understand how these factors may influence clinical outcomes and decision-making in stroke care in patients with neurocognitive disorders. More inclusive clinical trials and standardized assessment strategies to guide optimal care for this vulnerable population are required. This will be crucial in adapting healthcare systems to meet the needs of a growing and aging population.
1 Introduction
Neurocognitive disorders are strong contributors of frailty in elderly people. The risk of developing major cognitive impairment, also referred as dementia, increases with age (1), similar to the incidence of stroke that is 100 folds greater in people over 80 years than in young adults (2). In a context of ongoing aging and growing population, the proportion of patients suffering acute stroke who have preexisting cognitive impairment is rising. While numerous studies focused on post-stroke dementia, less attention has been paid to preexisting cognitive disorders in patients with stroke. This article aimed to depict the burden of prestroke cognitive impairment, its consequences on acute management and patients’ outcome, and relationship with other comorbidities and frailty.
2 Prevalence of preexisting cognitive impairment in patients with acute stroke
Only a few studies have evaluated the prevalence of preexisting cognitive impairment in patients with acute stroke. Prior dementia was estimated to range between 9 and 14% according to a meta-analysis (3). In Oxford Vascular Study (OXVASC), the prevalence of prestroke dementia increased with clinical severity of the cerebrovascular event, ranging from 5% in transient ischemic attack to 21% in severe major stroke (4). Mild cognitive impairment (MCI) before stroke has been even less investigated. A population-based study reported a prevalence of preexisting MCI of 14%, alongside with a similar proportion of patients with prior dementia (5). Not surprisingly, patients with prestroke cognitive impairment are older than their non-cognitively impaired counterparts (5, 6). Several methodological limitations can explain this lack of data in the literature. Above all, the assessment of cognitive disorders prior to stroke is challenging. This assessment can be conducted using standardized questionnaires, such as the IQCODE (Informant Questionnaire on COgnitive Decline in the Elderly) that has been shown to have a good accuracy for identifying preexisting dementia in patients with stroke (7), but their use remains limited especially when considering population-based settings. To address this limitation, retrospective epidemiological surveys are alternatives frequently used in observational studies. Finally, study setting (hospital- versus population-based recruitment of patients) and demographic characteristics of population strongly influence estimates of preexisting cognitive impairment and account for variations between studies.
Given the high prevalence of cognitive impairment in stroke patients, it has been hypothesized that it may conversely represent a risk factor for acute stroke. A meta-analysis reported 10 out of 12 studies corroborating this hypothesis with a global relative risk of 1.15 (8). However, a publication bias was not excluded. Moreover, establishing causality remains difficult as chronic vascular lesions contribute to vascular dementia, which may finally represent a clinical manifestation of an underlying neurovascular condition.
3 Acute stroke management in patients with preexisting cognitive impairment
Stroke units were progressively implemented over the last decades to improve acute management of stroke patients, and a meta-analysis of available literature suggested that admission to such organized inpatient care was associated with reduced mortality and disability as compared with general wards (9). Of note, the apparent benefits were independent of age, sex, stroke type, and clinical severity. However, no subgroup analysis according to preexisting comorbidities, including prior-to-stroke cognitive impairment, was performed, thus leaving uncertainty about the relevance of this type of care for patients with major neurocognitive disorders.
Several studies pointed out that patients with dementia were less likely to be admitted to (10–12) or have a shorter stay in (13) a stroke unit. In addition, they received a poorer quality of care with reduced access to various diagnostic procedures (11, 14, 15), swallowing assessment (11, 13), interdisciplinary functional evaluation (13), or invasive treatments such as endotracheal intubation (16). Treatment differences were also seen in revascularization decisions in patients with acute ischemic stroke, as studies reported that intravenous thrombolysis (10, 11, 17), and mechanical thrombectomy (10, 18) were less commonly administered to patients with preexisting dementia. The influence of prestroke MCI is less documented, a population-based study reported a similar administration of intravenous thrombolysis but lower use of mechanical thrombectomy in patients with prior MCI compared with those with normal cognition (5). Although evidence regarding sex disparities in access to diagnostic procedures and stroke care remains inconsistent in the general stroke population (14, 19–21), data specifically addressing sex differences among patients with prestroke cognitive impairment are limited. Most studies have treated sex as a confounding variable rather than performing dedicated subgroup analyses (14, 21, 22). Therefore, additional research is required to clarify this issue. Furthermore, disparities in stroke care for cognitively impaired patients appear to be a global phenomenon, with consistent reports from North America, Europe, and Asia. Notably, patients with MCI have also been shown to experience disparities in acute stroke care, including a lower rate of intravenous thrombolysis administration (22).
Several reasons could account for the lower administration of acute revascularization therapies including a greater clinical severity at onset (23), delays in treatment times (11, 17), or reluctance of clinicians with regard to the use of such therapies in severely cognitively-impaired patients. Another contributing factor is the scarcity of high-quality evidence on the effect of acute revascularization therapy in patients suffering ischemic stroke and who have preexisting neurocognitive disorders. Hence, most randomized clinical trials excluded individuals with prior disability (24). Consequently, current evidence on the efficacy and safety of intravenous thrombolysis and mechanical thrombectomy in patients with prestroke dementia exclusively come from observational studies. Although these studies suggested no loss of treatment benefit, an increased risk of symptomatic intracerebral hemorrhage was highlighted (25), and results should be interpretated with caution due to obvious selection bias inherent to such methodological approach. Efforts to enroll patients with premorbid neurocognitive disorders in future randomized clinical trials are urgently needed.
Finally, while treatment disparities have been mainly documented in ischemic stroke (for thrombolysis and thrombectomy), observational data suggest that similar patterns of reduced diagnostic and rehabilitative care also affect hemorrhagic stroke patients with pre-existing cognitive impairment.
4 Post-stroke outcome in patients with preexisting cognitive impairment
Several observational studies demonstrated that preexisting dementia was associated with a poorer early (5, 6, 26–29) and long-term (10, 28, 30) survival after stroke. Albeit some diverging conclusions (31), the association was found to be independent of confounding factors including age, sex, and stroke type in most studies. To account for this result it has been observed that patients admitted for a stroke and who have preexisting dementia could be at greater risk of acute medical complications including pneumonia, urinary tract infections, and gastrointestinal bleeding (6, 11, 26, 27). In addition, preexisting cognitive impairment was also associated with post-stroke delirium, thus contributing to a greater risk of in-hospital death (32, 33).
Among other hypotheses, it was assumed that the poorer prognosis after stroke in patients with preexisting cognitive impairment might be related to a greater clinical severity at onset. A population-based study demonstrated that patients with preexisting dementia, and to a lesser extent those with MCI, had more severe ischemic stroke, as measured at admission with the National Institute of Health Stroke Scale (NIHSS) score, than their not cognitively-impaired counterparts (23). Interestingly, the association was still observed after adjustment for well-established confounding factors, and was not mediated by preexisting structural visible brain damages on conventional imaging including old vascular lesion, brain atrophy, and leukoaraiosis (34), thus suggesting an impaired brain ischemic tolerance in patients with prior neurocognitive disorders that may involve processes at a cellular or neuronal network scale yet to be elucidated. However, in this study, the excess in case-fatality in patients with MCI or dementia persisted after adjustment on clinical severity (5), which indicated that a more complex interplay between preexisting cognitive impairment and outcome after stroke. Notably, a gradual effect was observed, whereby the association between dementia and either initial stroke severity or mortality was more pronounced than that observed for MCI, thus suggesting that the severity of cognitive impairment may influence post-stroke outcomes (5, 23). Conversely, whether the underlying cause of cognitive impairment may have an impact on post-stroke outcomes has been only poorly investigated. A study concluded that stroke patients with Alzheimer’s disease or mixed dementia had higher post-stroke mortality compared to those with vascular dementia (30). Furthermore, these outcomes may be also shaped by stroke recurrence, which depends on adequate vascular risk factor control and appropriate treatment. A twofold increase in recurrence risk has been reported among patients with prestroke cognitive impairment. This finding should be interpreted in the context of the well-established association between prestroke cognitive status and the development of post-stroke dementia (29, 35).
Stroke-related disability has a great impact on patients with neurocognitive impairment. Hence, several studies showed that patients with acute stroke and prior dementia had a reduced likelihood of returning to a prior living arrangement with a high risk of institutionalization (11, 36–38), thus highlighting consequences in terms of anticipating current and future needs of dedicated facilities. In a multicenter study conducted in England, patients with prestroke neurocognitive disorders received significantly fewer rehabilitation services, particularly physiotherapy (39). A qualitative assessment of clinical parameters influencing medical decisions about rehabilitation highlighted preexisting neurocognitive disorders as a major contributor of decision-making (40). Multiple barriers may contribute to the reluctance of clinicians to transfer patients with cognitive impairment to rehabilitation including inability to understand and participate in exercises, and behavior disturbances that could hinder the effectiveness of care programs. Therefore, some medical decisions may result from a subjective judgment, with clinicians anticipating a low chance of recovery in patients with preexisting cognitive impairment, in the absence of adapted evidence-based guidelines. Indeed, there are conflicting results in the literature regarding the benefit of rehabilitation after stroke in patient with preexisting cognitive impairment. Although some studies suggested that cognitive impairment negatively affect the effectiveness of rehabilitation, other works concluded to similar functional improvement, especially regarding ambulation, in cognitively normal and impaired patients (41, 42). Further research is needed to better define and evaluate cognitive-adapted rehabilitation programs that accommodate patients’ impairment.
5 Impact of other comorbidities on post-stroke outcome
Factors associated with poor prognosis following stroke remain a subject of ongoing research, underscoring the need to better understand and optimize care trajectories, particularly in patients experiencing ischemic stroke (43, 44). From a general point of view, comorbidities or dependency prior to stroke have been shown to be associated with a poorer survival (45, 46), and worse functional outcomes after rehabilitation (47). She et al. studied the impact of 16 chronic diseases, grouped together by categories (e.g., cardiopulmonary, hepatogastrointestinal, metabolic-renal, depression), all of which negatively affected functional and cognitive outcomes after a stroke (48). In most studies focusing on this topic, comorbidities were assessed by scores, the most frequently used being the Charlson Comorbidity Index, which was shown to positively correlate with an increased risk of death, particularly with conditions like cancer, renal, or liver disease. Notably, this index identifies dementia as a comorbidity alongside a list of other diseases, with results interpreted as a cumulative effect of each comorbidity, without considering potential interactions between them. Further works are needed to examine specifically the impact of comorbidities on management and outcome of stroke patients with preexisting neurocognitive disorders.
Another consideration is the complex interrelationship between cognitive impairment, frailty, and stroke. Frailty is a well-established risk factor for dementia (49, 50), and patients with neurocognitive disorders are at greater risk of having frailty than their non-cognitively impaired counterparts (51). On the other hand, there is growing evidence supporting a negative impact of frailty on post-stroke outcome. Hence, similarly to neurocognitive disorders, frailty seems to be associated with higher mortality, length of hospital stay, and disability after stroke (52–57). In a prospective study, frail patients had a higher in-hospital mortality, with a greater prevalence of deep venous thrombosis, and frailty emerged as best predictor of death at 12 months after ischemic stroke treated with acute revascularization therapy (56). In terms of recovery, functional improvement was shown to be largely reduced in frail versus robust patients (54). The risk of institutionalization after stroke was also greater in patients with frailty (58). To date, the mechanisms underlying these pejorative correlations remain unclearly explained. In secondary analysis of a cohort study, heterogeneity in trajectories after stroke was identified among frailer patients, and interactions with various variables including comorbidities and poor self-reported health were suggested (59). Additional research will help to clarify the individual contribution of frailty on post-stroke outcome in cognitively impaired patients.
6 Discussion
Based on relevant studies on this topic, the main ones of which are summarized in Table 1, this narrative review highlights the growing recognition of preexisting cognitive impairment as a major determinant of stroke trajectories.
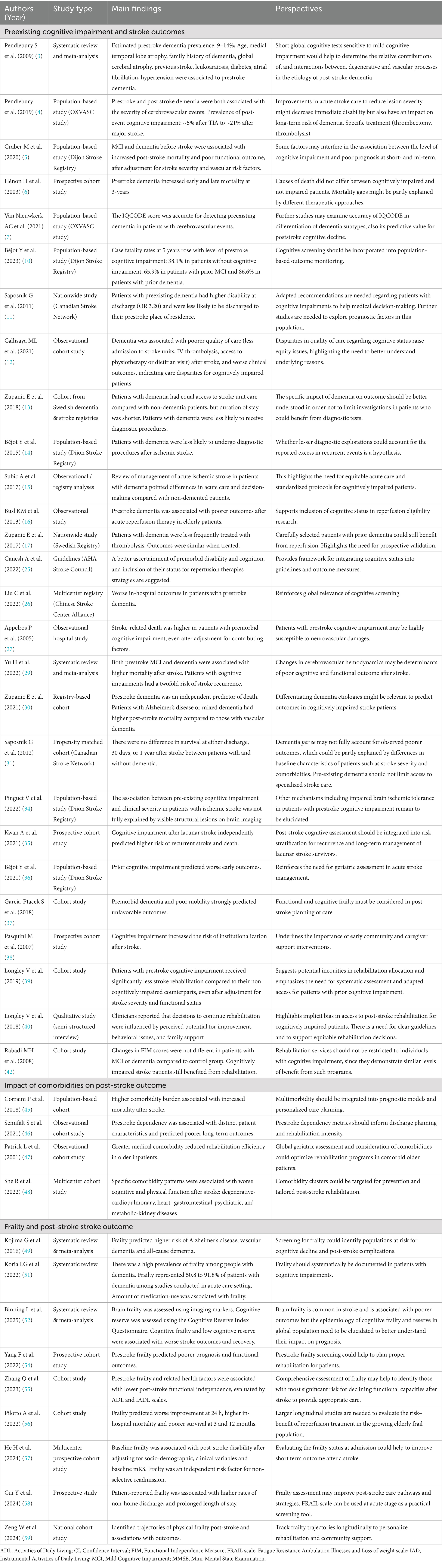
Table 1. Summary table of selected relevant studies on prestroke cognitive impairment, frailty, and post-stroke outcomes, and research perspectives.
Current literature pointed out a poorer outcome after stroke in patients with preexisting cognitive impairment, with data suggesting differential clinical management as a contributing factor. Given their complex health status, these patients are particularly vulnerable to early complications after stroke. In a context of growing and aging population, it is critical to further investigate the impact of comorbidities and frailty on post-stroke outcome, especially in patients with neurocognitive disorders, so as to better guide clinicians for treatment decisions, and help policy-makers to better anticipating resources allocation.
A statement from the American Heart Association/American Stroke Association recently pointed out the need for a better ascertainment and measurement of premorbid disability and cognitive impairment in the setting of acute stroke, thus requiring harmonized and validated strategies (25). These strategies include the use of clinical tools such as standardized scores in a more systematic way. There remain challenges in assessing profile of patients that would benefit the most from each strategy of care from the acute stage to post-stroke rehabilitation and follow-up. At the global level, evidence indicates disparities in the prevalence of cognitive disorders across ethnic group (60) and in stroke risk between low- and high-income countries (61, 62), thus emphasizing the importance of ethnically and socioeconomically inclusive research.
Author contributions
SK: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. YB: Conceptualization, Investigation, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
YB reports personal fees from BMS, Pfizer, Medtronic, Amgen, Servier, NovoNordisk, Novartis, Argenx, outside the submitted work.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor MZ declared a past collaboration with the author YB.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GBD 2016 Dementia Collaborators. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990-2016: a systematic analysis for the global burden of disease Study 2016. Lancet Neurol. (2019) 18:88–106. doi: 10.1016/S1474-4422(18)30403-4
2. Béjot, Y, Bailly, H, Durier, J, and Giroud, M. Epidemiology of stroke in Europe and trends for the 21st century. Presse Med. (2016) 45:e391–8. doi: 10.1016/j.lpm.2016.10.003
3. Pendlebury, ST, and Rothwell, PM. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. (2009) 8:1006–18. doi: 10.1016/S1474-4422(09)70236-4
4. Pendlebury, ST, and Rothwell, PM Oxford Vascular Study. Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: analysis of the population-based Oxford Vascular Study. Lancet Neurol. (2019) 18:248–58. doi: 10.1016/S1474-4422(18)30442-3
5. Graber, M, Garnier, L, Mohr, S, Delpont, B, Blanc-Labarre, C, Vergely, C, et al. Influence of pre-existing mild cognitive impairment and dementia on post-stroke mortality. The Dijon stroke registry. Neuroepidemiology. (2020) 54:490–7. doi: 10.1159/000497614
6. Hénon, H, Durieu, I, Lebert, F, Pasquier, F, and Leys, D. Influence of prestroke dementia on early and delayed mortality in stroke patients. J Neurol. (2003) 250:10–6. doi: 10.1007/s00415-003-0917-3
7. van Nieuwkerk, AC, Pendlebury, ST, Rothwell, PM, and Oxford Vascular Study,. Accuracy of the informant questionnaire on cognitive decline in the elderly for detecting preexisting dementia in transient ischemic attack and stroke: a population-based study. Stroke. (2021) 52:1283–90. doi: 10.1161/STROKEAHA.120.031961
8. Rostamian, S, Mahinrad, S, Stijnen, T, Sabayan, B, and de Craen, AJM. Cognitive impairment and risk of stroke: a systematic review and meta-analysis of prospective cohort studies. Stroke. (2014) 45:1342–8. doi: 10.1161/STROKEAHA.114.004658
9. Langhorne, P, and Ramachandra, S. Organised inpatient (stroke unit) care for stroke: network meta-analysis. Cochrane Database Syst Rev. (2020) 4:CD000197. doi: 10.1002/14651858.CD000197.pub4
10. Béjot, Y, Pinguet, V, and Duloquin, G. Long-term survival of ischemic stroke patients according to prior cognitive status: Dijon stroke registry. Neuroepidemiology. (2023) 57:345–54. doi: 10.1159/000533389
11. Saposnik, G, Cote, R, Rochon, PA, Mamdani, M, Liu, Y, Raptis, S, et al. Care and outcomes in patients with ischemic stroke with and without preexisting dementia. Neurology. (2011) 77:1664–73. doi: 10.1212/WNL.0b013e31823648f1
12. Callisaya, ML, Purvis, T, Lawler, K, Brodtmann, A, Cadilhac, DA, and Kilkenny, MF. Dementia is associated with poorer quality of care and outcomes after stroke: an observational Study. J Gerontol A Biol Sci Med Sci. (2021) 76:851–8. doi: 10.1093/gerona/glaa139
13. Zupanic, E, Kåreholt, I, Norrving, B, Secnik, J, von Euler, M, Winblad, B, et al. Acute stroke care in dementia: a cohort study from the Swedish dementia and stroke registries. J Alzheimer’s Dis. (2018) 66:185–94. doi: 10.3233/JAD-180653
14. Béjot, Y, Jacquin, A, Troisgros, O, Rouaud, O, Aboa-Eboulé, C, Hervieu, M, et al. Diagnostic procedures in ischaemic stroke patients with dementia. a population-based study. Int J Stroke Off J Int Stroke Soc. (2015) 10:95–8. doi: 10.1111/j.1747-4949.2012.00948.x
15. Subic, A, Cermakova, P, Norrving, B, Winblad, B, von Euler, M, Kramberger, MG, et al. Management of acute ischaemic stroke in patients with dementia. J Intern Med. (2017) 281:348–64. doi: 10.1111/joim.12588
16. Busl, KM, Nogueira, RG, Yoo, AJ, Hirsch, JA, Schwamm, LH, and Rost, NS. Prestroke dementia is associated with poor outcomes after reperfusion therapy among elderly stroke patients. J Stroke Cerebrovasc Dis. (2013) 22:718–24. doi: 10.1016/j.jstrokecerebrovasdis.2011.11.005
17. Zupanic, E, von Euler, M, Kåreholt, I, Contreras Escamez, B, Fastbom, J, Norrving, B, et al. Thrombolysis in acute ischemic stroke in patients with dementia: a Swedish registry study. Neurology. (2017) 89:1860–8. doi: 10.1212/WNL.0000000000004598
18. El-Ghanem, M, Abdulrazeq, H, Brasiliense, L, Abbad, H, Aguilar-Salinas, P, Al-Mufti, F, et al. Outcomes of mechanical Thrombectomy in patients with neurological disorders: a National Inpatient Sample Database Analysis. Cureus. (2024) 16:e54063. doi: 10.7759/cureus.54063
19. Medlin, F, Strambo, D, Lambrou, D, Caso, V, and Michel, P. Service delivery in acute ischemic stroke patients: does sex matter? Eur J Neurol. (2024) 31:e16287. doi: 10.1111/ene.16287
20. Di Carlo, A, Lamassa, M, Baldereschi, M, Pracucci, G, Basile, AM, Wolfe, CDA, et al. Sex differences in the clinical presentation, resource use, and 3-month outcome of acute stroke in Europe: data from a multicenter multinational hospital-based registry. Stroke. (2003) 34:1114–9. doi: 10.1161/01.STR.0000068410.07397.D7
21. Levine, DA, Galecki, AT, Morgenstern, LB, Zahuranec, DB, Langa, KM, Kabeto, MU, et al. Preexisting mild cognitive impairment, dementia, and receipt of treatments for acute ischemic stroke. Stroke. (2021) 52:2134–42. doi: 10.1161/STROKEAHA.120.032258
22. Levine, DA, Galecki, A, Kabeto, M, Nallamothu, BK, Zahuranec, DB, Morgenstern, LB, et al. Mild cognitive impairment and receipt of procedures for acute ischemic stroke in older adults. J Stroke Cerebrovasc Dis. (2020) 29:105083. doi: 10.1016/j.jstrokecerebrovasdis.2020.105083
23. Béjot, Y, Duloquin, G, Crespy, V, Durier, J, Garnier, L, Graber, M, et al. Influence of preexisting cognitive impairment on clinical severity of ischemic stroke: the Dijon stroke registry. Stroke. (2020) 51:1667–73. doi: 10.1161/STROKEAHA.119.028845
24. Béjot, Y. Age gap between stroke patients included in randomized clinical trials of acute revascularization therapy and those in population-based studies. A review Neuroepidemiology. (2023) 57:65–77. doi: 10.1159/000529552
25. Ganesh, A, Fraser, JF, Gordon Perue, GL, Amin-Hanjani, S, Leslie-Mazwi, TM, Greenberg, SM, et al. Endovascular treatment and thrombolysis for acute ischemic stroke in patients with premorbid disability or dementia: a scientific statement from the American Heart Association/American Stroke Association. Stroke. (2022) 53:e204–17. doi: 10.1161/STR.0000000000000406
26. Liu, C, Gu, H-Q, Yang, X, Wang, C-J, Meng, X, Yang, K-X, et al. Pre-stroke dementia and in-hospital outcomes in the Chinese stroke center Alliance. Ann Transl Med. (2022) 10:1050. doi: 10.21037/atm-22-723
27. Appelros, P, and Viitanen, M. What causes increased stroke mortality in patients with prestroke dementia? Cerebrovasc Dis. (2005) 19:323–7. doi: 10.1159/000084690
28. Koton, S, Tanne, D, Green, MS, and Bornstein, NM. Mortality and predictors of death 1 month and 3 years after first-ever ischemic stroke: data from the first national acute stroke Israeli survey (NASIS 2004). Neuroepidemiology. (2010) 34:90–6. doi: 10.1159/000264826
29. Yu, H, Ding, S, Wei, W, Guo, F, Li, Z, Yuan, Q, et al. Impact of pre-stroke dementia or mild cognitive impairment on stroke outcome: a systematic review and Meta-analysis. Dement Geriatr Cogn Disord. (2022) 51:101–9. doi: 10.1159/000522302
30. Zupanic, E, von Euler, M, Winblad, B, Xu, H, Secnik, J, Kramberger, MG, et al. Mortality after ischemic stroke in patients with Alzheimer’s disease dementia and other dementia disorders. J Alzheimer’s Dis. (2021) 81:1253–61. doi: 10.3233/JAD-201459
31. Saposnik, G, Kapral, MK, Cote, R, Rochon, PA, Wang, J, Raptis, S, et al. Is pre-existing dementia an independent predictor of outcome after stroke? A propensity score-matched analysis. J Neurol. (2012) 259:2366–75. doi: 10.1007/s00415-012-6508-4
32. Oldenbeuving, AW, de Kort, PLM, Jansen, BPW, Roks, G, and Kappelle, LJ. Delirium in acute stroke: a review. Int J Stroke. (2007) 2:270–5. doi: 10.1111/j.1747-4949.2007.00163.x
33. Shi, Q, Presutti, R, Selchen, D, and Saposnik, G. Delirium in acute stroke: a systematic review and meta-analysis. Stroke. (2012) 43:645–9. doi: 10.1161/STROKEAHA.111.643726
34. Pinguet, V, Duloquin, G, Thibault, T, Devilliers, H, Comby, P-O, Crespy, V, et al. Pre-existing brain damage and association between severity and prior cognitive impairment in ischemic stroke patients. J Neuroradiol J Neuroradiol. (2022) S0150-9861:00097–9. doi: 10.1016/j.neurad.2022.03.001
35. Kwan, A, Wei, J, Dowling, NM, Power, MC, and Nadareishvili, Z SPS3 Study Group. Cognitive impairment after lacunar stroke and the risk of recurrent stroke and death. Cerebrovasc Dis. (2021) 50:383–9. doi: 10.1159/000514261
36. Béjot, Y, Duloquin, G, Graber, M, Garnier, L, Mohr, S, and Giroud, M. Current characteristics and early functional outcome of older stroke patients: a population-based study (Dijon stroke registry). Age Ageing. (2021) 50:898–905. doi: 10.1093/ageing/afaa192
37. Garcia-Ptacek, S, Contreras Escamez, B, Zupanic, E, Religa, D, Von Koch, L, Johnell, K, et al. Prestroke mobility and dementia as predictors of stroke outcomes in patients over 65 years of age: a cohort Study from the Swedish dementia and stroke registries. J Am Med Dir Assoc. (2018) 19:154–61. doi: 10.1016/j.jamda.2017.08.014
38. Pasquini, M, Leys, D, Rousseaux, M, Pasquier, F, and Hénon, H. Influence of cognitive impairment on the institutionalisation rate 3 years after a stroke. J Neurol Neurosurg Psychiatry. (2007) 78:56–9. doi: 10.1136/jnnp.2006.102533
39. Longley, V, Peters, S, Swarbrick, C, Rhodes, S, and Bowen, A. Does pre-existing cognitive impairment impact on amount of stroke rehabilitation received? An observational cohort study. Clin Rehabil. (2019) 33:1492–502. doi: 10.1177/0269215519843984
40. Longley, V, Peters, S, Swarbrick, C, and Bowen, A. What influences decisions about ongoing stroke rehabilitation for patients with pre-existing dementia or cognitive impairment: a qualitative study? Clin Rehabil. (2018) 32:1133–44. doi: 10.1177/0269215518766406
41. Paker, N, Buğdaycı, D, Tekdöş, D, Kaya, B, and Dere, C. Impact of cognitive impairment on functional outcome in stroke. Stroke Res Treat. (2010) 2010:652612. doi: 10.4061/2010/652612
42. Rabadi, MH, Rabadi, FM, Edelstein, L, and Peterson, M. Cognitively impaired stroke patients do benefit from admission to an acute rehabilitation unit. Arch Phys Med Rehabil. (2008) 89:441–8. doi: 10.1016/j.apmr.2007.11.014
43. Zeinhom, MG, Khalil, MFE, Kamel, IFM, Kohail, AM, Ahmed, SR, Elbassiouny, A, et al. Predictors of the unfavorable outcomes in acute ischemic stroke patients treated with alteplase, a multi-center randomized trial. Sci Rep. (2024) 14:5960. doi: 10.1038/s41598-024-56067-5
44. Zeinhom, MG, Khalil, MFE, Elmesallami, AG, Zedan, TS, Hassaneen, KDH, Refat, HM, et al. Predictors of post-Alteplase long-term unfavorable outcome in atrial fibrillation patients presented with embolic stroke in the Middle East and North Africa regions: a multi-center, longitudinal study. Neurol Ther. (2025). doi: 10.1007/s40120-025-00814-x
45. Corraini, P, Szépligeti, SK, Henderson, VW, Ording, AG, Horváth-Puhó, E, and Sørensen, HT. Comorbidity and the increased mortality after hospitalization for stroke: a population-based cohort study. J Thromb Haemost. (2018) 16:242–52. doi: 10.1111/jth.13908
46. Sennfält, S, Pihlsgård, M, Norrving, B, Ullberg, T, and Petersson, J. Ischemic stroke patients with prestroke dependency: characteristics and long-term prognosis. Acta Neurol Scand. (2021) 143:78–88. doi: 10.1111/ane.13328
47. Patrick, L, Knoefel, F, Gaskowski, P, and Rexroth, D. Medical comorbidity and rehabilitation efficiency in geriatric inpatients. J Am Geriatr Soc. (2001) 49:1471–7. doi: 10.1046/j.1532-5415.2001.4911239.x
48. She, R, Yan, Z, Hao, Y, Zhang, Z, Du, Y, Liang, Y, et al. Comorbidity in patients with first-ever ischemic stroke: disease patterns and their associations with cognitive and physical function. Front Aging Neurosci. (2022) 14:887032. doi: 10.3389/fnagi.2022.887032
49. Kojima, G, Taniguchi, Y, and Iliffe, S. Frailty as a predictor of Alzheimer disease, vascular dementia, and all dementia among community-dwelling older people: a systematic review and meta-analysis. J Am Med Dir Assoc. (2016) 17:881–8. doi: 10.1016/j.jamda.2016.05.013
50. Searle, SD, and Rockwood, K. Frailty and the risk of cognitive impairment. Alzheimer’s Res Ther. (2015) 7:54. doi: 10.1186/s13195-015-0140-3
51. Koria, LG, Sawan, MJ, Redston, MR, and Gnjidic, D. The prevalence of frailty among older adults living with dementia: a systematic review. J Am Med Dir Assoc. (2022) 23:1807–14. doi: 10.1016/j.jamda.2022.01.084
52. Binning, L, Basquill, C, Tvrda, L, and Quinn, T. Epidemiology and outcomes associated with cognitive frailty and reserve in a stroke population: systematic review and meta-analysis. Cerebrovasc Dis Basel Switz. (2025) 54:536–47. doi: 10.1159/000541670
53. Evans, NR, Todd, OM, Minhas, JS, Fearon, P, Harston, GW, Mant, J, et al. Frailty and cerebrovascular disease: concepts and clinical implications for stroke medicine. Int J Stroke. (2022) 17:251–9. doi: 10.1177/17474930211034331
54. Yang, F, Li, N, Yang, L, Chang, J, Yan, A, and Wei, W. Association of pre-stroke Frailty with Prognosis of elderly patients with acute cerebral infarction: a cohort Study. Front Neurol. (2022) 13:855532. doi: 10.3389/fneur.2022.855532
55. Zhang, Q, Gao, X, Huang, J, Xie, Q, and Zhang, Y. Association of pre-stroke frailty and health-related factors with post-stroke functional independence among community-dwelling Chinese older adults. J Stroke Cerebrovasc Dis. (2023) 32:107130. doi: 10.1016/j.jstrokecerebrovasdis.2023.107130
56. Pilotto, A, Brass, C, Fassbender, K, Merzou, F, Morotti, A, Kämpfer, N, et al. Premorbid frailty predicts short- and long-term outcomes of reperfusion treatment in acute stroke. J Neurol. (2022) 269:3338–42. doi: 10.1007/s00415-022-10966-7
57. He, H, Liu, M, Li, L, Zheng, Y, Nie, Y, Xiao, LD, et al. The impact of frailty on short-term prognosis in discharged adult stroke patients: a multicenter prospective cohort study. Int J Nurs Stud. (2024) 154:104735. doi: 10.1016/j.ijnurstu.2024.104735
58. Cui, Y, Meng, C, Xiang, L, Luo, Y, Song, X, Cheng, D, et al. Association between patient-reported frailty and nonhome discharge among older patients with acute stroke: a prospective study. Clin Rehabil. (2024) 38:1691–702. doi: 10.1177/02692155241290258
59. Zeng, W, Zhou, W, Pu, J, Tong, B, Li, D, Yao, Y, et al. Physical frailty trajectories in older stroke survivors: findings from a national cohort study. J Clin Nurs. (2024) 34:912–20. doi: 10.1111/jocn.17101
60. Mayeda, ER, Glymour, MM, Quesenberry, CP, and Whitmer, RA. Inequalities in dementia incidence between six racial and ethnic groups over 14 years. Alzheimers Dement. (2016) 12:216–24. doi: 10.1016/j.jalz.2015.12.007
61. Feigin, VL, Brainin, M, Norrving, B, Martins, SO, Pandian, J, Lindsay, P, et al. World stroke organization: global stroke fact sheet 2025. Int J Stroke. (2025) 20:132–44. doi: 10.1177/17474930241308142
Keywords: stroke, dementia, cognitive impairment, aging, outcome, frailty
Citation: Kassir S and Béjot Y (2025) Preexisting cognitive impairment in patients with acute stroke. Front. Neurol. 16:1629461. doi: 10.3389/fneur.2025.1629461
Edited by:
Marialuisa Zedde, IRCCS Local Health Authority of Reggio Emilia, ItalyReviewed by:
Luis Rafael Moscote-Salazar, Colombian Clinical Research Group in Neurocritical Care, ColombiaMohamed G. Zeinhom, Kafrelsheikh University, Egypt
Copyright © 2025 Kassir and Béjot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yannick Béjot, eWFubmljay5iZWpvdEBjaHUtZGlqb24uZnI=