Abstract
Background:
Postoperative cognitive dysfunction (POCD) is a syndrome characterized by long-term cognitive impairment following anesthesia and surgery. Acupuncture has demonstrated potential therapeutic benefits in managing POCD. However, comparative efficacy among different acupuncture modalities remains unexplored. This study aims to systematically compare the effects of various acupuncture interventions on postoperative cognitive function in elderly patients undergoing general anesthesia.
Methods:
A comprehensive literature search was conducted across eight databases—CNKI, Wanfang, VIP, SinoMed, PubMed, Embase, Cochrane Library, and Web of Science—up to January 2025. Randomized controlled trials (RCTs) assessing acupuncture interventions for POCD in elderly patients receiving general anesthesia were included, provided cognitive outcomes were measured by the Mini-Mental State Examination (MMSE) or reported POCD incidence. Study quality was appraised using the Cochrane Risk of Bias Tool 2.0. A Bayesian network meta-analysis (NMA) was performed with the GEMTC package in R software, incorporating both direct and indirect comparisons. Intervention rankings were evaluated using the Surface Under the Cumulative Ranking Curve (SUCRA). Statistical significance was set at p < 0.05. Publication bias was assessed by funnel plots generated in Stata 18.0.
Results:
Thirty-two studies involving 2,644 patients were included. The SUCRA rankings for efficacy in improving postoperative cognitive function were: Electroacupuncture (77.93%) > Thumbtack Needle (73.89%) > Scalp Acupuncture (68.58%). Subgroup analysis by intervention timing revealed: preoperative phase—electroacupuncture was significantly superior to conventional anesthesia and thumbtack needle; intraoperative phase—electroacupuncture outperformed scalp acupuncture and placebo; postoperative phase—electroacupuncture showed the best efficacy, surpassing conventional anesthesia and Xingnao Kaiqiao acupuncture; perioperative phase—auricular acupuncture exhibited notable advantages over electroacupuncture and standard of care. Regarding POCD incidence, 23 studies with 1,886 patients demonstrated SUCRA rankings as: Xingnao Kaiqiao acupuncture (86.56%) > Thumbtack Needle (80.16%) > Electroacupuncture (58.78%).
Conclusion:
Electroacupuncture exerted the most substantial effect in mitigating postoperative declines in Mini-Mental State Examination (MMSE) scores among elderly Chinese patients receiving general anesthesia. Thumbtack needle acupuncture and scalp acupuncture also showed relatively favorable benefits. Electroacupuncture consistently achieved superior outcomes across preoperative, intraoperative, and postoperative interventions.
Systematic review registration:
Introduction
Postoperative cognitive dysfunction (POCD) is a central nervous system complication following anesthesia and surgery, characterized by impairments in memory, attention, language, and orientation (1, 2). The elderly population is particularly vulnerable to POCD (3), with incidence rates in non-cardiac surgery patients aged over 60 being 1.5 times higher than those in younger individuals (4). Hospital prevalence among older adults can reach up to 41.4% (4, 5). POCD may persist from several weeks to years, prolonging recovery time and hospitalization, while increasing mortality and the risk of psychosomatic comorbidities (6). With accelerating population aging in China, the increasing number of elderly surgical patients imposes a growing burden of POCD on families and society.
Current prevention and management strategies for POCD focus on three aspects: optimization of anesthesia protocols (e.g., total intravenous anesthesia with propofol), pharmacological interventions (e.g., dexmedetomidine, lidocaine, parecoxib), and non-pharmacological approaches (e.g., preoperative cognitive training and acupuncture). However, challenges remain due to incomplete elucidation of POCD pathogenesis, lack of evidence-based standards for individualized anesthesia, inconsistent drug efficacy, and limited clinical evidence supporting non-pharmacological interventions such as acupuncture and rehabilitation strategies (7, 8).
Among existing evidence, only one meta-analysis has addressed acupuncture intervention effects on POCD (9). Although it confirmed acupuncture significantly reduces early postoperative cognitive impairment in elderly patients, the analysis was limited by a narrow focus on specific acupoints and failed to systematically clarify efficacy heterogeneity among different acupuncture modalities. Traditional pairwise meta-analyses face methodological constraints when comparing multiple interventions simultaneously, limiting multidimensional efficacy assessment. Therefore, this study employed, for the first time, a network meta-analysis approach integrating direct and indirect evidence to comprehensively compare and rank the therapeutic effects of different acupuncture interventions on POCD. The aim is to provide evidence-based guidance for optimizing acupuncture strategies in the perioperative management of elderly patients.
Methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, including extensions for network meta-analysis (NMA) (10). The study protocol was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420250651273.
Search strategy
A comprehensive literature search was performed across eight databases: PubMed, Embase, Cochrane Library, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfang Data, VIP Database, and SinoMed. The search period spanned from the inception of each database to January 23, 2025. Language restrictions were set to English or Chinese. The search combined Medical Subject Headings (MeSH) and free-text terms related to Acupuncture Therapy, Electroacupuncture, Moxibustion, and Postoperative Cognitive Complications. Additionally, reference lists of relevant articles and gray literature were manually screened to identify further eligible studies. The detailed search strategy is provided in Appendix 1.
Inclusion and exclusion criteria
Studies were included if they met the following criteria: (1) Population: Elderly patients aged 60 years or older undergoing surgery under general anesthesia, regardless of sex; (2) Interventions: Electroacupuncture, Scalp Acupuncture, Ear Acupuncture, Acupuncture, Thumbtack Needle, Xingnao Kaiqiao Acupuncture; Comparators: General Anesthesia, Standard of Care (SoC), Placebo; (3) Study design: Randomized controlled trials (RCTs); (4) Outcomes: MMSE score (change from baseline to postoperative assessment) and incidence of postoperative cognitive dysfunction (POCD); (5) Language: Chinese or English.
Exclusion criteria were as follows: (1) animal or cell studies, case reports, study protocols, reviews, letters, editorials, conference abstracts; (2) studies with missing or erroneous data; (3) duplicate publications; (4) unavailable full texts; (5) overlapping participant data in multiple publications; (6) elderly patients with pre-existing neuropsychiatric disorders undergoing general anesthesia.
Data extraction
All retrieved records were imported into EndNote. Two independent investigators (Liang and Li) screened titles and abstracts according to the inclusion and exclusion criteria, followed by full-text review for final eligibility assessment. Discrepancies were resolved through discussion or consultation with a third investigator (Zhang). Data extraction was performed independently by two investigators using a pre-designed electronic form, including first author, publication year, country, sample size, patient age, intervention and comparator details, treatment duration, and outcome measures.
Quality assessment
The risk of bias of included RCTs was independently assessed by two authors (Liang and Li) using the Cochrane Risk of Bias tool version 2.0 (ROB2.0) (11). The ROB2.0 evaluates five domains: random sequence generation, allocation concealment, blinding of participants and personnel, incomplete outcome data, and selective reporting. Each domain was rated as “high risk,” “some concerns,” or “low risk.” Overall study risk of bias was classified as low risk if all domains were low risk or only one domain had some concerns; high risk if four or more domains had some concerns or any domain was high risk; and moderate risk for other cases. Any disagreements were resolved by the third author (Zhang).
Statistical analysis
Continuous outcomes were analyzed using mean differences (MD) with 95% credible intervals as effect measures. A Bayesian network meta-analysis model was constructed using Markov Chain Monte Carlo (MCMC) simulation implemented in the GeMTC package in R. Model parameters included four chains, 10,000 burn-in iterations, 100,000 sampling iterations with a thinning interval of 10, and initial values set to 2.5, aiming to obtain posterior distributions. Three core assumptions underpinning network meta-analysis—transitivity, homogeneity, and consistency—were evaluated. Heterogeneity was assessed using the mtc. anohe function in GeMTC; an overall I2 < 50% was considered acceptable to satisfy the homogeneity assumption. Consistency between direct and indirect evidence was examined by the node-splitting method (mtc.nodesplit function); p-values > 0.05 indicated no significant inconsistency. Convergence was assessed by calculating the Potential Scale Reduction Factor (PSRF), with a value close to 1 indicating satisfactory convergence. Network geometry was visualized with nodes representing different interventions and edges representing head-to-head comparisons. Placebo served as the reference comparator for all analyses. The Surface Under the Cumulative Ranking curve (SUCRA) was calculated to rank the interventions. Publication bias was assessed using funnel plots. All statistical analyses were conducted using R software version 4.4.1 and Stata version 18.0.
Results
Literature search and screening process
A total of 1,490 records were identified through database searches. After removal of 580 duplicates, 770 articles were excluded following preliminary screening of titles and abstracts. The remaining articles underwent full-text review, and studies were included or excluded strictly based on predefined inclusion and exclusion criteria. Ultimately, 32 studies were included in the analysis. The detailed screening process is illustrated in Figure 1.
Figure 1

Literature screening process.
Characteristics and quality assessment of included studies
The 32 included studies (12–43) originated from one country (China), encompassing a total of 2,644 patients, of whom 52.87% were male and 47.13% female, with an age range of 60–86 years. The basic characteristics of the included studies are summarized in Table 1.
Table 1
| First author | Publication year | Region | Number of cases | Gender (male/female) | Age | Intervention (specific measures) | Treatment | Intervention time point | Outcome indicators | Type of surgery | Perioperative management protocol | Acupuncture parameters | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Experimental group | Control group | Experimental group | Control group | Acupoint | Acupuncture time | |||||||||||
| Xiaoqiu Gao | 2012 | China | 60 | 60 | 52/68 | 71.65 ± 4.8373 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Non-cardiac surgery | Anesthetic Induction: Etomidate, Fentanyl, Cisatracurium; Anesthetic Maintenance: Sevoflurane Inhalation, Remifentanil |
GV20, LI4, PC6, ST36 | Initiated 30 min before induction until end of surgery | |
| Sunyan Lin | 2013 | China | 38 | 37 | 48/27 | 68.5067 ± 3.5541 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Radical resection of colorectal cancer under general anesthesia | Anesthetic Induction: Midazolam, Propofol, Fentanyl, Vecuronium Bromide; Anesthetic Maintenance: Propofol, Remifentanil | GV20, PC6, ST36, SP6 | Initiated 20 min before induction until end of surgery | |
| Sunyan Lin | 2013 | China | 25 | 24 | 34/15 | 68.1573 ± 2.9428 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Open gastrointestinal tumor resection (colorectal resection) | Anesthetic Induction: Midazolam, Propofol, Fentanyl, Vecuronium; Anesthetic Maintenance: Propofol, Remifentanil | GV20, GV29, PC6 | Initiated 30 min before induction until end of surgery | |
| Daiying Zhang | 2014 | China | 60 | 60 | 61/59 | 73.325 ± 6.4737 | Electroacupuncture | SoC | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Major open abdominal surgery (radical colectomy, radical rectal resection, radical gastrectomy, subtotal gastrectomy) | Anesthetic Induction: Midazolam, Fentanyl, Propofol, Vecuronium Bromide; Anesthetic Maintenance: Propofol, Remifentanil, Cisatracurium Besylate | GV20, GV14, PC6 | Initiated 30 min before induction until end of surgery | |
| Chenlin Zhang | 2015 | China | 35 | 35 | 37/33 | 74.5 ± 4.0027 | Electroacupuncture | General Anesthesia | 8d | Postoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Radical resection of colorectal cancer under general anesthesia | Anesthetic Induction: Midazolam Propofol Fentanyl Vecuronium Bromide Anesthetic Maintenance: Propofol Remifentanil |
GV20, PC6 | Initiated 20 min before induction until end of surgery | |
| XIcheng Dong | 2016 | China | 30 | 30 | not mentioned | 70 ± 4.601 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Rectal cancer surgery | Anesthetic Induction: Etomidate, Sufentanil, Rocuronium Bromide Anesthetic Maintenance: Propofol, Remifentanil, Rocuronium Bromide |
GV20, PC6 | Initiated 30 min before induction until end of surgery | |
| Zhi Liu | 2017 | China | 49 | 49 | 48/50 | 73.935 ± 10.7366 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Geriatric tumor resection (gastric, hepatic, gallbladder cancers) | Anesthetic Induction: Midazolam, Penehyclidine Hydrochloride, Cisatracurium, Vecuronium Bromide Anesthetic Maintenance: Propofol, Remifentanil, Rocuronium Bromide |
GV20, PC6, ST36 | Initiated 30 min before induction until end of surgery | |
| Peina Zheng | 2017 | China | 56 | 56 | 62/50 | 74.99 ± 4.2536 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Colorectal resection | / | GV20, PC6, ST36, SP6 | Initiated before induction until end of surgery | |
| Gang Jin | 2017 | China | 50 | 50 | 56/46 | 67.734 ± 2.5096 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Abdominal surgery | Anesthetic Induction: Midazolam, Propofol, Fentanyl, Vecuronium Bromide Anesthetic Maintenance: Propofol, Remifentanil |
GV20, GV29, PC6 | Initiated 30 min before induction until end of surgery | |
| Peirong Liu | 2017 | China | 40 | 40 | 33/47 | 66.5 ± 6.4973 | Electroacupuncture | General Anesthesia | 7d | Perioperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Hip arthroplasty | Anesthetic Induction: Fentanyl, Midazolam, Propofol, Cisatracurium Anesthetic Maintenance: Remifentanil, Propofol |
LI4, LR3 | 30 min on non-surgical days. Initiated 30 min before induction until end of surgery on surgical days |
|
| Kexue Zeng | 2018 | China | 50 | 50 | 58/42 | 68.3 ± 1.2 | Electroacupuncture | SoC | 30d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Lower abdominal or extremity surgery | Anesthetic Induction: Midazolam, Fentanyl, Vecuronium Bromide For Injection, Propofol Anesthetic Maintenance: Fentanyl, Vecuronium Bromide For Injection, Propofol, Isoflurane |
GV20, GB20, BL23 | 20 min | |
| Feiyi Zhao | 2018 | China | 30 | 30 | 26/34 | 65.965 ± 3.9724 | Electroacupuncture | Placebo | 5d | Preoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Knee arthroplasty | Anesthetic Induction: Fentanyl, Midazolam, Propofol, Cisatracurium Besilate Anesthetic Maintenance: Remifentanil, Propofol |
GV20, GV24, EX-HN1, GB13, LI4, LR3 | 30 min | |
| Libing Zhang | 2018 | China | 26 | 26 | 38/14 | 71 ± 7.9746 | Xingnao Kaiqiao acnpnnctnr | SoC | 7d | Postoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Hip arthroplasty under general anesthesia | Anesthetic Induction: Propofol, Remifentanil Hydrochloride, Sevoflurane, Midazolam, Vecuronium Bromide Anesthetic Maintenance: Propofol, Remifentanil Hydrochloride, Sevoflurane |
GV26, PC6, SP6, LU5, HT1, BL40 | / | |
| Xiaona Han | 2018 | China | 45 | 45 | 50/40 | 68.25 ± 2.5246 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSEscore | Colorectal resection | Anesthetic Induction: Midazolam, Propofol, Fentanyl, Vecuronium Bromide Anesthetic Maintenance: Propofol, Remifentanil |
GV20, SP6, ST36, PC6 | Initiated 20 min before induction until end of surgery | |
| Haiyan Sun | 2018 | China | 20 | 20/20 | 35/25 | 69.6 ± 2.3034 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Radical gastrectomy | Anesthetic Induction: Sufentanil, Cisatracurium, Etomidate Anesthetic Maintenance: Sevoflurane |
PC6, LI4, ST36, ST37 | Initiated 20 min before induction until end of surgery | |
| Qi Zhang | 2018 | China | 45 | 45 | 48/42 | 72.5 ± 4.5302 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSEscore | Spinal surgery | Anesthetic Induction: Sufentanil, Midazolam, Etomidate, Cisatracurium Besilate Anesthetic Maintenance: Propofol, Remifentanil |
GV20, GV14, ST36 | Initiated 20 min before induction until end of surgery | |
| Ningke Wang | 2018 | China | 48 | 48 | 58/38 | 68.55 ± 5.4748 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSEscore | Laparoscopic-assisted proximal subtotal gastrectomy | Anesthetic Induction: Midazolam, Fentanyl, Vecuronium Bromide, Propofol Anesthetic Maintenance: Fentanyl, Propofol, Vecuronium Bromide |
PC6, LI4, ST36, ST37 | Initiated 15–20 min before induction until end of surgery | |
| Qingguo Xu | 2019 | China | 50 | 50 | 61/39 | 77.7 ± 5.9015 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Total hip arthroplasty | Anesthetic Induction: Midazolam, Sufentanil, Propofol, Rocuronium Bromide Anesthetic Maintenance: Remifentanil, Propofol |
LI4, LR3 | Initiated 30 min before induction until end of surgery | |
| Suping Yuan | 2019 | China | 50 | 50 | 53/47 | 60–81 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Laparoscopic cholecystectomy | Anesthetic Induction: Midazolam, Sufentanil, Propofol, Rocuronium Bromide Anesthetic Maintenance: Remifentanil, Propofol |
GV20, PC6 | 20 min | |
| Hongnan Wang | 2019 | China | 42 | 42 | 49/35 | 63 ~ 79 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSEscore | Orthopedic surgery | Anesthetic Induction: Midazolam, Propofol, Fentanyl, Vecuronium Anesthetic Maintenance: Midazolam, Propofol, Fentanyl, Vecuronium |
GV20, ST36, PC6 | Initiated 30 min before induction until end of surgery | |
| Na Zhao | 2021 | China | 30 | 30 | 33/27 | 71.58 ± 4.6161 | Electroacupuncture | SoC | 7d | Postoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | / | Anesthetic Induction: Midazolam, Cisatracurium, Fentanyl, Propofol Anesthetic Maintenance: Sevoflurane, Propofol, Remifentanil, Cisatracurium |
GV20, HT7, PC6, LI4 | 20 min | |
| Yanhua Tang | 2022 | China | 30 | 30 | 32/28 | 69.155 ± 3.5597 | Electroacupuncture | General Anesthesia | 9d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Hip arthroplasty, tibial fracture fixation, femoral fracture fixation | / | KI1, HT7, GV20 | 30 min | |
| Ronghua Li | 2022 | China | 40 | 40 | 18/62 | 73 ± 4.1 | Thumbtack needle | Placebo | 3D | Preoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Hip fracture surgery | Anesthetic Induction: Propofol, Citric Acidsufentanil, Cisatracurium, Midazolam; Anesthetic Maintenance: Propofol, Remifentanil, Dexmedetomidine, Sevoflurane |
GV20, HT7, LI4, PC6, ST36 | 5 times daily, 2 min each | |
| Meihuang Cai | 2022 | China | 58 | 59 | 59/58 | 68.5043 ± 3.5516 | Scalp Acupuncture | SoC | 3d | Intraoperative | MMSEscore | Intertrochanteric femoral fracture surgery | / | (GV24.5 → GV20), (GV20 → GV21) | Sustained stimulation throughout the surgical procedure | |
| Yongda Luo | 2022 | China | 60 | 60 | 45/75 | 71.525 ± 5.0811 | Electroacupuncture | General Anesthesia | 3d | Postoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | / | / | GV20, PC6, ST36 | 30 min | |
| Yiqin Wan | 2023 | China | 30 | 30 | 39/21 | 73 ± 8.5022 | Electroacupuncture | General Anesthesia | 1d | Preoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Flexible ureteroscopic holmium laser lithotripsy | Anesthetic Induction: Midazolam, Sufentanil, Propofol, Cisatracurium Besylate; Anesthetic Maintenance: Propofol, Remifentanil, with supplemental Cisatracurium Besylate |
ST36, PC6 | 30 min | |
| Jie Zheng | 2023 | China | 30 | 30 | 38/22 | 70.55 ± 1.4394 | Electroacupuncture | SoC | 6d | Perioperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Hip arthroplasty under general anesthesia | Anesthetic Induction: Fentanyl, Midazolam, Propofol, Cisatracurium Anesthetic Maintenance: Propofol, Remifentanil, with supplemental Cisatracurium |
LI4, LR3 | 30 min | |
| Linyun Zhuang | 2023 | China | 32 | 29 | Not mentioned | 80.7982 ± 5.311 | Acupunture | General Anesthesia | 1d | Preoperative | MMSE score | Hip fracture surgery | Anesthetic Induction: Midazolam, Citric Acidfentanyl, Cisatracurium Besylate, Propofol Anesthetic Maintenance: Remifentanil, Propofol |
HT5, PC6, ST40 | Twice daily | |
| Linyuan Song | 2023 | China | 20 | 20 | 23/17 | 63.685 ± 2.8211 | Xingnao Kaiqiao acnpnnctnr | SoC | 5d | Postoperative | MMSEscore | / | / | PC6, GV26, SP6 BL40, HT1, LU5 |
/ | |
| Jian Xie | 2023 | China | 45 | 45 | 54/36 | 66.99 ± 6.0331 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE SCORE, NUMBER OF POCD OCCURRENCES | Radical rectal cancer resection | Anesthetic Induction: Propofol, Sufentanil, Vecuronium Bromide Anesthetic Maintenance: Propofol, Remifentanil |
ST36, PC6, SP6, GV20 | Initiated 30 min before induction until end of surgery | |
| Yong Liu | 2023 | China | 60 | 60 | 56/64 | 72.31 ± 5.7236 | Electroacupuncture | General Anesthesia | 1d | Intraoperative | MMSE score | Hip arthroplasty | Anesthetic Induction: Midazolam, Citric Acidfentanyl, Propofol, Vecuronium Bromide Anesthetic Maintenance: Remifentanil, Vecuronium Bromide, Propofol |
GB41, GB31, Dai Mai, Ah Shi Point | Throughout the surgical procedure | |
| Meini Wang | 2024 | China | 30 | 30 | 31/29 | 74.02 ± 5.4178 | Ear acupuncture | SoC | 7d | Perioperative | MMSE score | Hip arthroplasty | / | MA-IC, MA-TF1, MA-AT, MA-LO, MA-AH| | 20–30 min | |
Basic characteristics of included studies.
SoC, Standard of Care; MMSE, Mini-Mental State Examination.
Risk of bias assessment indicated that the majority of studies were at low risk. Ten studies (14–19, 25, 29, 34, 39) were judged to have moderate risk, with eight studies (15–19, 29, 34, 39) having moderate risk primarily due to unreported allocation concealment and unclear blinding of outcome assessors, which may have affected outcome measurement. The first author (Liang) and second author (Li) discussed these cases but could not reach a consensus; following consultation with the third author (Zhang), these were classified as moderate risk. One study (14) was assigned moderate risk because of unspecified allocation concealment and lack of blinding for trial implementers, with unanimous agreement among the authors. Another study (25) was also classified as moderate risk due to absence of information on blinding of implementers and outcome assessors; after discussion among the authors, it was rated as moderate risk. The methodological quality assessment for each trial is presented in Figure 2.
Figure 2

Methodological quality assessment of included studies.
Network meta-analysis results
Network geometry
In the network plots, each node represents an intervention, with node size proportional to the number of included studies investigating that intervention. Edges connecting nodes indicate direct comparisons between interventions; edge thickness reflects the number of studies for each comparison, with thicker lines representing more evidence (see Figure 3). The posterior residual deviance (PRSF) for all analyses was equal to 1, indicating model convergence. Node-splitting analyses were conducted for all closed loops, showing p-values > 0.05, thus demonstrating consistency between direct and indirect evidence.
Figure 3

Network relationship diagram. (a) MMSE, (b) preoperative intervention subgroup, (c) intraoperative intervention subgroup, (d) postoperative intervention subgroup, (e) perioperative intervention subgroup, and (f) number of POCD events.
Summary of outcome indicators
MMSE
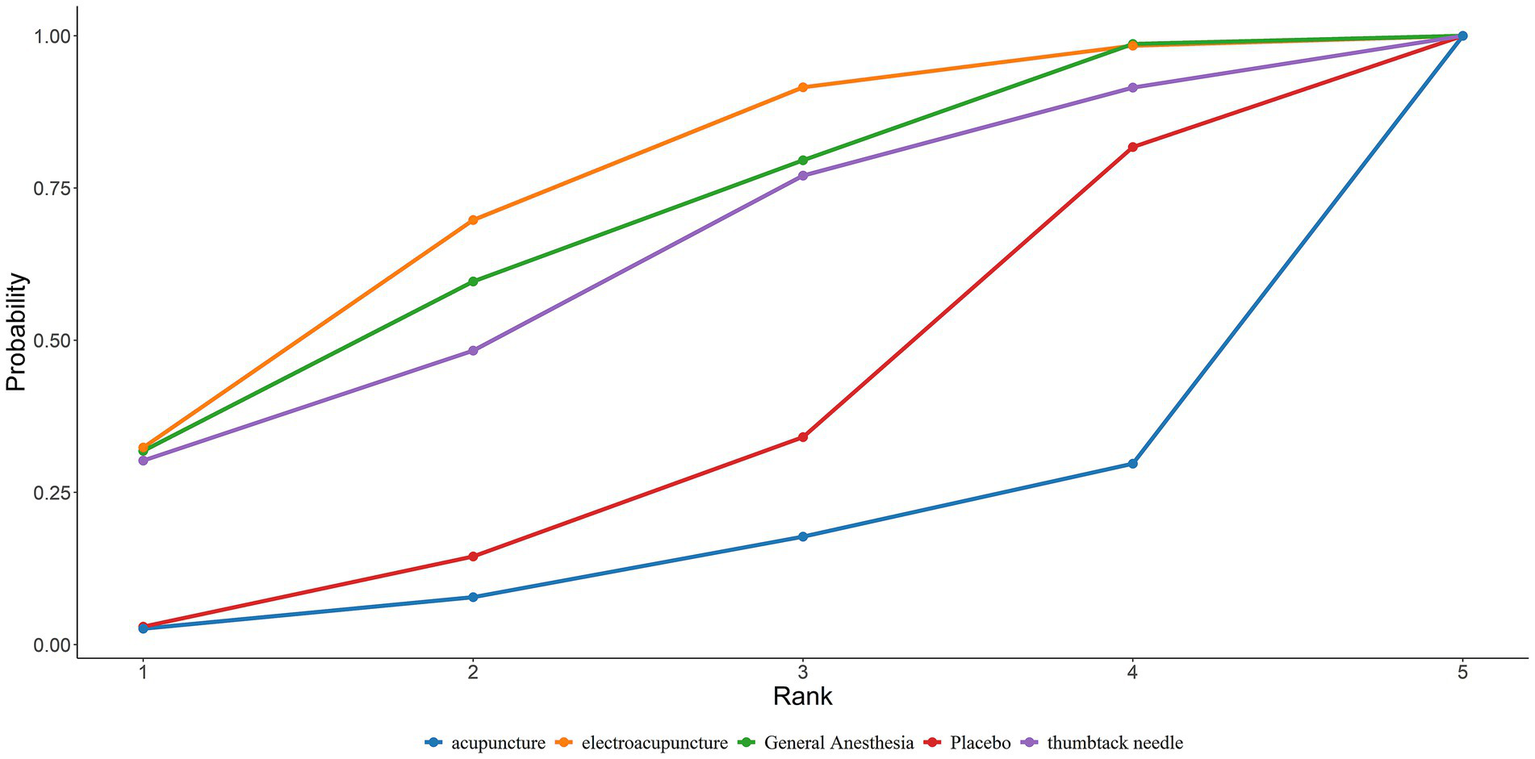
A total of 32 studies reported MMSE scores. Under the random-effects model within the network meta-analysis (NMA) framework, results indicated that: General anesthesia was associated with a significant decline in postoperative cognitive function MMSE scores compared with electroacupuncture (General Anesthesia vs. Electroacupuncture: MD = −0.70; 95% CrI: −1.31 to −0.09). Similarly, Standard of Care (SoC) showed a significant decrease in MMSE scores compared to electroacupuncture (SoC vs. Electroacupuncture: MD = −1.98; 95% CrI: −3.38 to −0.57). Conversely, general anesthesia yielded significantly higher MMSE scores than acupuncture (General Anesthesia vs. Acupuncture: MD = 2.96; 95% CrI: 0.10–5.82). Electroacupuncture was also superior to acupuncture (Electroacupuncture vs. Acupuncture: MD = 3.66; 95% CrI: 0.73–6.58). Detailed pairwise comparisons are provided in Table 2. The SUCRA rankings indicated the best efficacy of electroacupuncture in reducing postoperative MMSE decline among elderly patients undergoing general anesthesia: Electroacupuncture (77.93%) > Thumbtack Needle (73.89%) > Scalp Acupuncture (68.58%) (see Figure 4). MMSE overall ranking is shown in Table 3.
Table 2
| General anesthesia | ||||||||
|---|---|---|---|---|---|---|---|---|
| 1.28 (−0.26, 2.81) | SoC | |||||||
| −0.7 (−1.31, −0.09) | −1.98 (−3.38, −0.57) | Electroacupuncture | ||||||
| 0.18 (−1.71, 2.08) | −1.1 (−3.41, 1.23) | 0.88 (−0.97, 2.73) | Placebo | |||||
| −0.59 (−3.77, 2.59) | −1.87 (−4.64, 0.91) | 0.11 (−3, 3.22) | −0.76 (−4.4, 2.83) | Ear acupuncture | ||||
| −0.95 (−4.3, 2.4) | −2.23 (−5.84, 1.38) | −0.25 (−3.58, 3.08) | −1.13 (−3.91, 1.63) | −0.37 (−4.91, 4.21) | Thumbtack needle | |||
| −0.66 (−4.07, 2.75) | −1.94 (−4.98, 1.1) | 0.04 (−3.31, 3.4) | −0.84 (−4.68, 2.99) | −0.07 (−4.19, 4.04) | 0.29 (−4.46, 5.02) | Scalp acupuncture | ||
| 2.96 (0.1, 5.82) | 1.68 (−1.56, 4.92) | 3.66 (0.73, 6.58) | 2.77 (−0.65, 6.19) | 3.54 (−0.72, 7.81) | 3.9 (−0.49, 8.31) | 3.62 (−0.82, 8.06) | Acupuncture | |
| 1.33 (−1.21, 3.91) | 0.05 (−1.98, 2.12) | 2.03 (−0.43, 4.53) | 1.15 (−1.94, 4.26) | 1.92 (−1.51, 5.38) | 2.28 (−1.85, 6.46) | 1.99 (−1.66, 5.66) | −1.63 (−5.44, 2.23) | Xingnao Kaiqiao acupuncture |
Pairwise comparisons for the effects of various acupuncture modalities on MMSE scores in elderly patients undergoing general anesthesia surgery.
Bolded values signify that the difference in MMSE changes between the column intervention and the row intervention is statistically significant.
Figure 4

SUCRA curve of the effects of different acupuncture modalities on MMSE in elderly patients undergoing general anesthesia surgery.
Table 3
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| MMSE | Electroacupuncture (77.93%) | Thumbtack needle (73.89%) | Scalp Acupuncture (68.58%) | Ear acupuncture (67.70%) | General Anesthesia (53.59%) | Placebo (49.55%) | Xingnao Kaiqiao acupuncture (29.67%) | SoC (22.42%) | Acupuncture (6.7%) |
| MMSE (Preoperative) | Electroacupuncture (73.01%) | General Anesthesia (67.42%) | Thumbtack needle (61.77%) | Placebo (33.32%) | Acupuncture (14.47%) | ||||
| MMSE (Intraoperative) | Electroacupuncture (76.78%) | Scalp Acupuncture (65.03%) | Placebo (55.35%) | General Anesthesia (40.74%) | SoC (12.10%) | ||||
| MMSE (Postoperative) | Electroacupuncture (82.46%) | General Anesthesia (71.68%) | Xingnao Kaiqiao acupuncture (25.92%) | SoC (19.94%) | |||||
| MMSE (Perioperative) | Ear acupuncture (84.64%) | Electroacupuncture (66.32%) | SoC (25.24%) | General Anesthesia (23.79%) | |||||
| POCD | Xingnao Kaiqiao acupuncture (86.56%) | Thumbtack needle (80.16%) | Electroacupuncture (58.78%) | SoC (38.44%) | Placebo (27.78%) | General Anesthesia (8.26%) |
Summary of MMSE and POCD rankings.
Subgroup analyses by intervention timing and modality
Preoperative interventions
Network meta-analysis of four studies with preoperative interventions is summarized in Table 4. SUCRA rankings were: Electroacupuncture (73.01%) > General Anesthesia (67.42%) > Thumbtack Needle (61.77%). Electroacupuncture demonstrated the most favorable effect in reducing postoperative MMSE decline preoperatively (Figure 5). The preoperative MMSE ranking is presented in Table 3.
Table 4
| General anesthesia | ||||
|---|---|---|---|---|
| −0.19 (−4.05, 3.69) | Electroacupuncture | |||
| 1.39 (−4.06, 6.86) | 1.58 (−2.28, 5.42) | Placebo | ||
| 0.26 (−6.31, 6.9) | 0.45 (−4.91, 5.84) | −1.13 (−4.86, 2.64) | Thumbtack needle | |
| 2.95 (−0.91, 6.84) | 3.14 (−2.34, 8.59) | 1.57 (−5.15, 8.26) | 2.69 (−5, 10.35) | Acupuncture |
Pairwise comparisons for the effects of various acupuncture modalities during surgery on MMSE scores in elderly patients undergoing general anesthesia.
Bold values signify that the difference in MMSE changes between the column intervention and the row intervention is statistically significant.
Figure 5
SUCRA curve of the effects of different preoperative acupuncture on MMSE in elderly patients undergoing general anesthesia surgery.
Intraoperative
Nineteen studies assessing intraoperative interventions were analyzed (Table 5). SUCRA rankings were: Electroacupuncture (76.78%) > Scalp Acupuncture (65.03%) > Placebo (55.35%). Electroacupuncture was most effective in attenuating intraoperative cognitive decline (Figure 6). The intraoperative MMSE ranking is summarized in Table 3.
Table 5
| General anesthesia | ||||
|---|---|---|---|---|
| 1.18 (−1.12, 3.47) | SoC | |||
| −0.77 (−1.55, 0.01) | −1.95 (−4.11, 0.21) | Electroacupuncture | ||
| −0.34 (−3.07, 2.4) | −1.52 (−5, 1.96) | 0.43 (−2.3, 3.16) | Placebo | |
| −0.77 (−4.8, 3.26) | −1.94 (−5.25, 1.36) | 0.01 (−3.95, 3.95) | −0.42 (−5.24, 4.37) | Scalp acupuncture |
Pairwise comparisons for the effects of various acupuncture modalities during surgery on MMSE scores in elderly patients under general anesthesia.
Bold values signify that the difference in MMSE changes between the column intervention and the row intervention is statistically significant.
Figure 6
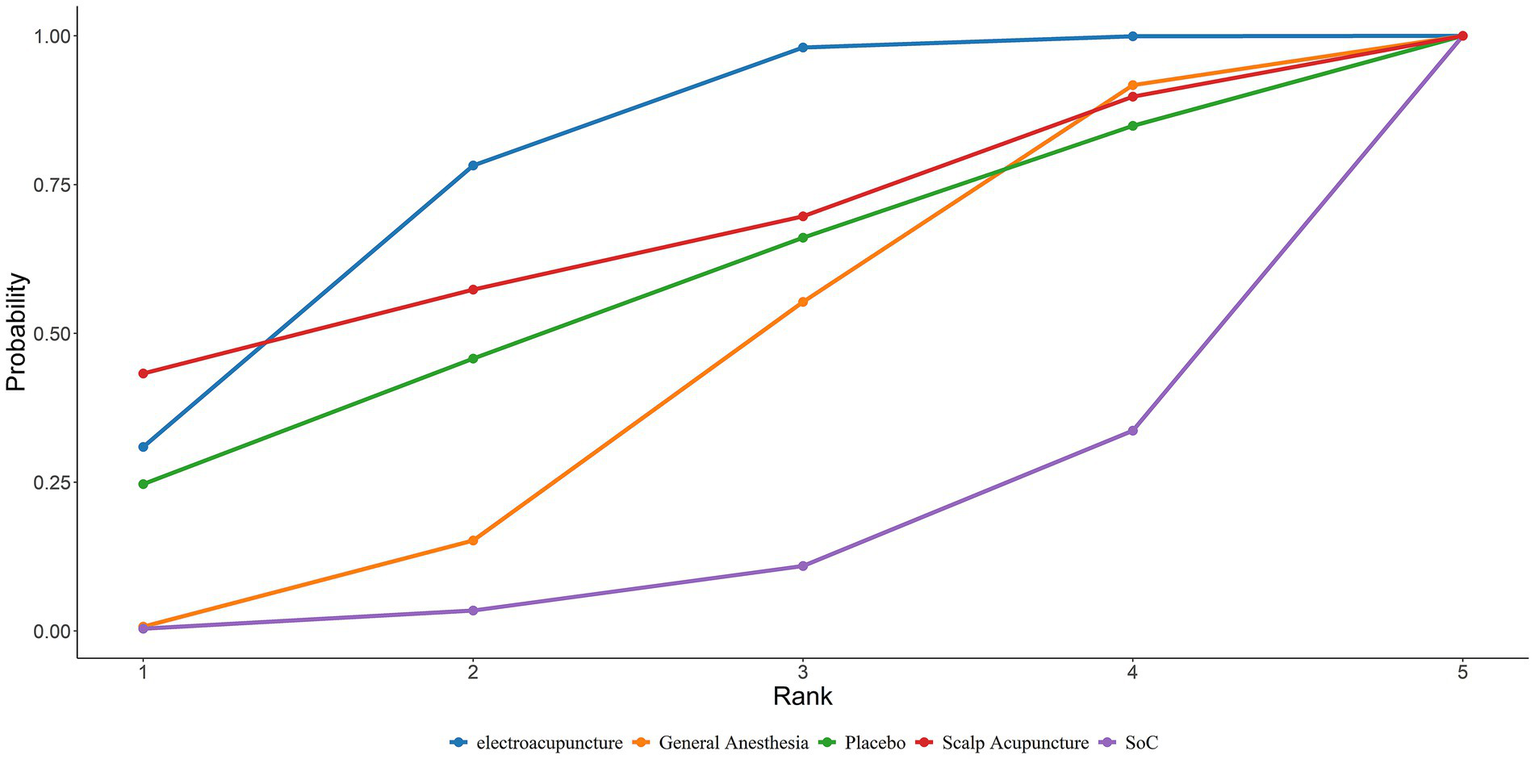
Area under the SUCRA curve of the effects of different acupuncture modalities on MMSE in elderly patients undergoing general anesthesia surgery during operation.
Postoperative
Six studies on postoperative interventions were included (Table 6). SUCRA rankings showed: Electroacupuncture (82.46%) > General Anesthesia (71.68%) > Xingnao Kaiqiao Acupuncture (25.92%). Electroacupuncture exhibited the greatest benefit postoperatively (Supplementary Figure S1). The postoperative MMSE ranking is displayed in Table 3.
Table 6
| General anesthesia | |||
|---|---|---|---|
| 2.62 (−1.72, 6.99) | SoC | ||
| −0.27 (−2.43, 1.91) | −2.88 (−6.65, 0.88) | Electroacupuncture | |
| 2.44 (−2.5, 7.88) | −0.16 (−2.75, 2.87) | 2.71 (−1.76, 7.65) | Xingnao Kaiqiao acupuncture |
Pairwise comparisons for the effects of various postoperative acupuncture modalities on MMSE scores in elderly patients undergoing general anesthesia surgery.
Bold values signify that the difference in MMSE changes between the column intervention and the row intervention is statistically significant.
Perioperative interventions
Seven studies involving perioperative interventions were analyzed (Table 7). SUCRA rankings indicated: Ear Acupuncture (84.64%) > Electroacupuncture (66.32%) > SoC (25.24%). Ear acupuncture had the best effect in reducing postoperative MMSE decline during the perioperative period (Supplementary Figure S2). The perioperative MMSE ranking is also provided in Table 3.
Table 7
| General anesthesia | |||
|---|---|---|---|
| −0.13 (−3.69, 3.41) | SoC | ||
| −1.2 (−3.65, 1.25) | −1.07 (−3.64, 1.5) | Electroacupuncture | |
| −2 (−6.29, 2.28) | −1.87 (−4.29, 0.54) | −0.8 (−4.33, 2.71) | Ear acupuncture |
Pairwise comparisons for the effects of various acupuncture modalities during surgery on MMSE scores in elderly patients undergoing general anesthesia.
Bold values indicate that the difference in MMSE changes between the column intervention and the row intervention is statistically significant.
Incidence of POCD
A total of 23 studies reported the incidence of POCD. Based on the Bayesian network meta-analysis (NMA) within a random-effects framework, the results demonstrated that the incidence of POCD postoperatively in elderly patients receiving general anesthesia was significantly higher compared to those treated with electroacupuncture (General Anesthesia vs. Electroacupuncture: RR = 2.15, 95% CrI = 1.52–3.18; see Table 8). The SUCRA ranking probabilities indicated that Xingnao Kaiqiao acupuncture (86.56%) ranked highest, followed by thumbtack needle (80.16%), and electroacupuncture (58.78%). Thus, Xingnao Kaiqiao acupuncture was associated with the lowest postoperative POCD incidence in elderly patients undergoing general anesthesia (Figure 7). The comparative ranking of POCD outcomes is summarized in Table 3.
Table 8
| General anesthesia | |||||
|---|---|---|---|---|---|
| 1.62 (0.76, 3.65) | SoC | ||||
| 1.37 (0.52, 3.78) | 0.84 (0.26, 2.7) | Placebo | |||
| 2.15 (1.52, 3.18) | 1.33 (0.66, 2.62) | 1.57 (0.61, 4.05) | Electroacupuncture | ||
| 5.05 (0.87, 37.04) | 3.11 (0.47, 24.54) | 3.65 (0.86, 20.54) | 2.34 (0.41, 16.67) | Thumbtack needle | |
| 8.6 (0.87, 265.02) | 5.21 (0.61, 148.6) | 6.31 (0.54, 214.83) | 3.97 (0.41, 120.28) | 1.74 (0.08, 74.55) | Xingnao Kaiqiao acupuncture |
Pairwise comparison of postoperative POCD incidence among elderly patients undergoing general anesthesia with different acupuncture interventions.
Values in bold denote statistically significant differences in POCD incidence between the column and row interventions.
Figure 7
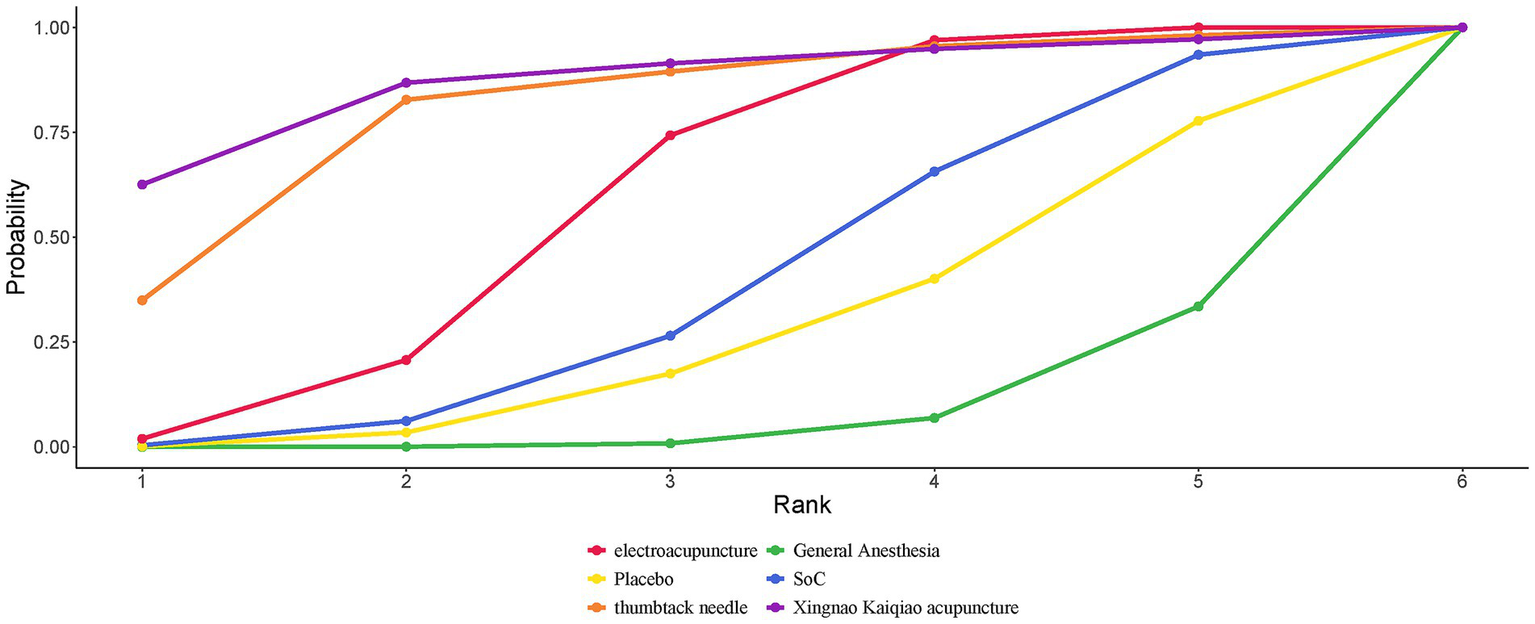
SUCRA curves for the incidence of POCD in elderly patients undergoing general anesthesia treated with different acupuncture modalities.
Publication bias
Publication bias was evaluated using contour-enhanced funnel plots, Egger’s test, and Begg’s test. For MMSE, the funnel plot appeared symmetrical (Figure 8); however, Egger’s test yielded statistical significance (p = 0.001), suggesting potential publication bias, whereas Begg’s test did not (p = 0.236). For POCD, the funnel plot was symmetric (Figure 8), and both Egger’s test (p = 0.64) and Begg’s test (p = 0.493) indicated no publication bias.
Figure 8
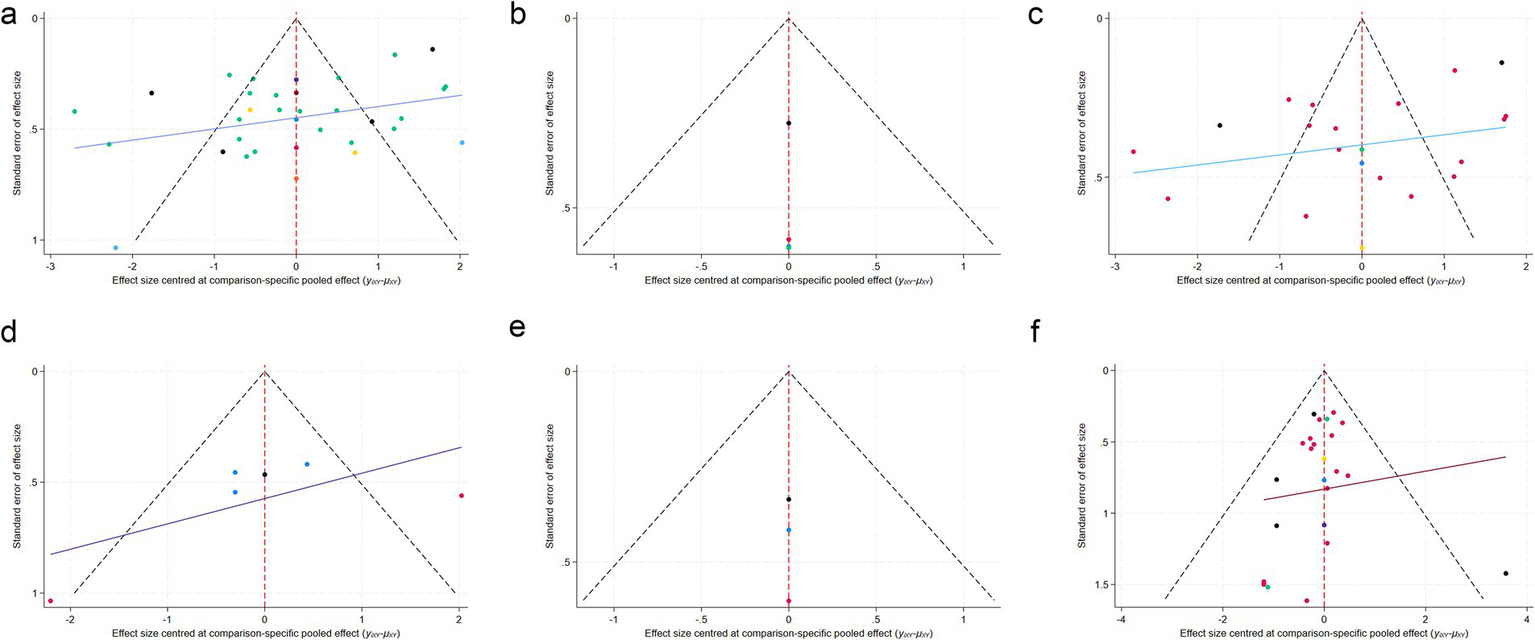
Funnel plots for publication bias assessment. (a) MMSE; (b) preoperative intervention subgroup; (c) intraoperative intervention subgroup; (d) postoperative intervention subgroup; (e) perioperative intervention subgroup; (f) POCD incidence.
Discussion
This meta-analysis incorporated 32 trials encompassing 2,644 elderly patients undergoing general anesthesia. Using a Bayesian network meta-analytic approach, we compared the efficacy of Electroacupuncture, Scalp Acupuncture, Ear Acupuncture, Acupuncture, Thumbtack Needle, Xingnao Kaiqiao Acupuncture, General Anesthesia, Standard of Care (SoC), and Placebo in mitigating postoperative declines in MMSE scores. At present, there is no universally accepted diagnostic criterion for POCD. In the included studies, POCD diagnosis relied on changes in MMSE scores from pre- to postoperative assessments. Although the Montreal Cognitive Assessment (MoCA) demonstrates higher sensitivity, evidence remains limited, and its diagnostic utility for POCD requires further validation. Consequently, MMSE was adopted as the primary outcome measure in this study. The objective was to provide evidence-based guidance for selecting acupuncture interventions in elderly patients undergoing general anesthesia. Key findings are summarized as follows: All analyses indicated that Electroacupuncture ranked highest in overall efficacy, followed by Thumbtack Needle and Scalp Acupuncture. Subgroup analyses based on intervention timing revealed that: Preoperative stage: Electroacupuncture was significantly superior to General Anesthesia and Thumbtack Needle; Intraoperative stage: Electroacupuncture demonstrated the best efficacy, outperforming Scalp Acupuncture and Placebo; Postoperative stage: Electroacupuncture remained the most effective, exceeding General Anesthesia and Xingnao Kaiqiao Acupuncture; Perioperative stage: Ear Acupuncture showed significant advantage, superior to Electroacupuncture and SoC.
For the secondary outcome of postoperative POCD incidence, 23 trials involving 1,886 elderly patients were included. The Bayesian network meta-analysis compared Electroacupuncture, Thumbtack Needle, Xingnao Kaiqiao Acupuncture, General Anesthesia, SoC, and Placebo. Results indicated that Xingnao Kaiqiao Acupuncture was associated with the lowest incidence of POCD.
Electroacupuncture, which integrates traditional acupuncture with modern electrical stimulation by delivering microcurrents at specific frequencies and intensities to acupoints, was investigated in 27 studies included herein. It ranked first in efficacy across all interventions and in subgroup analyses of preoperative, intraoperative, and postoperative periods, ranking second only in the perioperative subgroup. Notably, only two studies in the perioperative subgroup employed electroacupuncture interventions spanning pre-, intra-, and postoperative phases, while the remaining studies applied electroacupuncture at a single time point. These findings suggest that the timing and frequency of electroacupuncture may be critical determinants of its effectiveness. Our analysis confirms the significant efficacy of electroacupuncture in preventing postoperative cognitive dysfunction in elderly patients undergoing general anesthesia, supporting its clinical application for this indication. However, methodological quality varied across included electroacupuncture studies, with common deficiencies such as inadequate allocation concealment and lack of blinding, potentially introducing selection and performance biases. While current evidence is promising, further high-quality randomized controlled trials are needed to strengthen the evidence base.
The neuroprotective mechanisms of electroacupuncture likely involve inhibition of inflammation, reduction of oxidative stress, neuronal protection, and synaptic remodeling, thereby modulating POCD pathophysiology (44). In a murine femoral fracture surgical model, electroacupuncture significantly decreased peripheral and central inflammatory markers and improved cognitive function (45, 46). In a rat model of abdominal surgery, electroacupuncture pretreatment markedly increased hippocampal neuronal counts in aged rats and protected mitochondrial structure and function by reducing intracellular calcium levels, thus inhibiting neuronal apoptosis (47). Additionally, electroacupuncture may indirectly regulate central nervous system inflammation by modulating gut microbiota composition and their metabolites (e.g., short-chain fatty acids), as well as epigenetically modulating cognition-related gene expression through DNA methylation or histone modifications (47).
Thumbtack Needle is a traditional Chinese medicine external treatment tool resembling a miniature thumbtack, composed of a 1–2 mm short needle affixed to an adhesive patch base. It is secured to the skin surface at acupoints via medical tape to provide continuous mild stimulation. It is commonly used for alleviating chronic pain, regulating insomnia, anxiety, and related conditions. Thumbtack needle therapy modulates pain transmission pathways and inhibits the release of inflammatory mediators such as C-reactive protein (CRP) and prostaglandin E2 (PGE2) through sustained acupoint stimulation (48). This modality has demonstrated comparable efficacy to conventional analgesia in postoperative pain management following cesarean section (49), total knee arthroplasty (48), and laparoscopic hysterectomy (50). The widely accepted “microglia–neuroinflammation–cognitive dysfunction” pathway suggests that surgical stimuli activate central nervous system microglia, bone marrow-derived macrophages (BMDMs), mast cells, and T lymphocytes, resulting in the release of proinflammatory cytokines concentrated in specific brain regions. This cascade exacerbates postoperative neuroinflammation and subsequently induces cognitive impairment (51). Thumbtack needle therapy can alleviate postoperative pain, especially inflammatory pain, thereby reducing postoperative complications and intraoperative anesthetic requirements, and improving postoperative recovery quality. Effective analgesia may attenuate inflammation, thus mitigating pain-associated postoperative cognitive dysfunction (POCD). However, to date, only one study has evaluated the effect of thumbtack needle on cognitive impairment in elderly patients undergoing general anesthesia.
Scalp Acupuncture (Head Needle) is a specialized form of acupuncture that targets specific stimulation zones on the scalp, aiming to modulate central nervous system function by stimulating cerebral cortex projection areas on the scalp surface. It has been shown to improve memory function, with related studies elucidating its underlying biological mechanisms. Scalp acupuncture targets the left angular gyrus (Brodmann area 39) and fusiform gyrus (Brodmann area 37), modulating brain regions associated with semantic processing and memory retrieval, based on projection correlation analysis from neuroimaging databases (52). In ischemic cerebrovascular disease models, scalp acupuncture promotes microglial polarization from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, thereby alleviating neuroinflammatory injury (53). Additionally, it downregulates interferon-gamma (IFN-γ) expression, inhibits the JAK/STAT1 signaling pathway, and regulates IL-12-mediated inflammatory cascades (54). These mechanisms collectively contribute to improved memory function in ischemic cerebrovascular conditions. Scalp acupuncture may exert protective effects against POCD by suppressing neuroinflammatory pathways. Nonetheless, only one study to date has explored the effect of scalp acupuncture on cognitive dysfunction in elderly patients undergoing general anesthesia. Hence, more high-quality, large-sample RCTs with rigorous design are necessary to further investigate its clinical efficacy in this context.
Our analysis revealed that thumbtack needle acupuncture and Xingnao Kaiqiao acupuncture substantially reduced the incidence of POCD. Nevertheless, their rankings in MMSE outcomes were inconsistent. Specifically, MMSE analysis incorporated 32 trials with 2,644 patients, whereas POCD incidence analysis included only 23 trials with 1,886 patients. The smaller sample size for POCD may have undermined statistical power and obscured the true therapeutic effects of thumbtack needle and Xingnao Kaiqiao acupuncture. Variability in intervention timing and duration across acupuncture modalities may also account for divergent findings between MMSE and POCD outcomes.
This study represents the first network meta-analysis (NMA) evaluating the efficacy of various acupuncture modalities in mitigating postoperative MMSE score decline among elderly patients undergoing general anesthesia, thereby providing clinical reference for the treatment of postoperative cognitive dysfunction. Moreover, we analyzed the ranking of acupuncture efficacy according to different intervention timings. However, several limitations should be acknowledged. Some included studies carried a moderate risk of bias (due to inadequate allocation concealment and lack of blinding), which may weaken the validity of the results. The absence of allocation concealment increases the risk of selection bias, potentially leading to overestimation of treatment effects; the lack of blinding may compromise the objectivity and accuracy of subjective outcome measures. The study population consisted exclusively of Chinese patients. While such homogeneity enhanced statistical efficiency, it markedly restricted external validity. Differences in genetic background, perioperative medication practices, depth-of-anesthesia monitoring, and postoperative rehabilitation protocols across countries may influence the effectiveness of acupuncture for POCD. Direct head-to-head comparisons of different acupuncture modalities were unavailable, precluding definitive comparative conclusions. Some studies were limited by small sample sizes, thereby increasing the likelihood of bias. Follow-up time points for outcome assessment were inconsistent across studies. Reliance on a single outcome measure introduces subjectivity and restricts sensitivity, especially for detecting early or subtle cognitive decline. Although comparing pre- and postoperative MMSE scores permits detection of substantial cognitive deterioration, MMSE lacks sensitivity for early or subtle impairments, particularly in executive function, processing speed, and working memory. Consequently, mild or subclinical deficits may have been underestimated or overlooked. This study focused exclusively on the effect of acupuncture modality on POCD without investigating the influence of acupoint selection, which is also a critical determinant. Furthermore, POCD occurrence is closely associated with patient-related factors, surgical variables, anesthetic agents, and anesthesia-related risk factors. Future research should conduct multicenter RCTs directly comparing different acupuncture therapies while integrating multidimensional data such as patient baseline characteristics and perioperative anesthetic parameters to establish risk stratification models for POCD. Additionally, future studies should incorporate neuroinflammatory biomarkers alongside MMSE assessments and extend follow-up to at least 3 months postoperatively to evaluate long-term outcomes. Emphasis should be placed on elucidating (1) the specific neuroprotective effects of different acupuncture methods and acupoint combinations during surgery, and (2) how these modalities might synergistically enhance therapeutic efficacy. Such evidence will enable clinicians to select the optimal acupuncture strategy tailored to individual patients to prevent POCD.
Conclusion
In conclusion, this study indicated that electroacupuncture provided the most robust protection against postoperative MMSE decline in elderly Chinese patients undergoing general anesthesia. Thumbtack needle and scalp acupuncture demonstrated relatively favorable effects as well. Electroacupuncture was consistently the most effective intervention across preoperative, intraoperative, and postoperative phases. Nevertheless, given the methodological limitations, future research should prioritize large-scale, rigorously designed, multicenter randomized controlled trials across diverse populations and cultural contexts to validate the generalizability and safety of acupuncture interventions. Moreover, adoption of more sensitive cognitive assessment instruments, such as the MoCA, should be pursued to enhance diagnostic precision in POCD. Future research should further clarify the impacts of electroacupuncture, thumbtack needle, scalp acupuncture, and intervention timing on postoperative cognitive dysfunction in elderly surgical patients under general anesthesia.
Statements
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
WenL: Writing – original draft, Visualization, Software, Methodology, Data curation, Conceptualization, Investigation. ML: Software, Writing – original draft, Validation. JZ: Writing – review & editing. WeiL: Supervision, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1637566/full#supplementary-material
References
1.
Needham MJ Webb CE Bryden DC . Postoperative cognitive dysfunction and dementia: what we need to know and do. Br J Anaesth. (2017) 119:i115–25. doi: 10.1093/bja/aex354
2.
Rundshagen I . Postoperative cognitive dysfunction. Dtsch Arztebl Int. (2014) 111:119–25. doi: 10.3238/arztebl.2014.0119
3.
Moller JT Cluitmans P Rasmussen LS Houx P Rasmussen H Canet J et al . Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International study of post-operative cognitive dysfunction. Lancet. (1998) 351:857–61. doi: 10.1016/s0140-6736(97)07382-0
4.
Monk TG Weldon BC Garvan CW Dede DE van der Aa MT Heilman KM et al . Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology. (2008) 108:18–30. doi: 10.1097/01.anes.0000296071.19434.1e
5.
Urits I Orhurhu V Jones M Hoyt D Seats A Viswanath O . Current perspectives on postoperative cognitive dysfunction in the ageing population. Turk J Anaesthesiol Reanim. (2019) 47:439–47. doi: 10.5152/tjar.2019.75299
6.
Steinmetz J Christensen KB Lund T Lohse N Rasmussen LS . Long-term consequences of postoperative cognitive dysfunction. Anesthesiology. (2009) 110:548–55. doi: 10.1097/ALN.0b013e318195b569
7.
Sun J Du X Chen Y . Current progress on postoperative cognitive dysfunction: an update. J Integr Neurosci. (2024) 23:224. doi: 10.31083/j.jin2312224
8.
Wang CM Chen WC Zhang Y Lin S He HF . Update on the mechanism and treatment of sevoflurane-induced postoperative cognitive dysfunction. Front Aging Neurosci. (2021) 13:702231. doi: 10.3389/fnagi.2021.702231
9.
Chen X Kong D Du J Ban Y Xu H . Transcutaneous electrical acupoint stimulation affects older adults' cognition after general anesthesia: a meta-analysis. Geriatr Nurs. (2022) 46:144–56. doi: 10.1016/j.gerinurse.2022.05.010
10.
Page MJ McKenzie JE Bossuyt PM Boutron I Hoffmann TC Mulrow CD et al . The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
11.
Sterne JAC Savović J Page MJ Elbers RG Blencowe NS Boutron I et al . RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
12.
Liu P Peng S Han Z Zhang Y Diao S . Effects of electroacupuncture on cognitive function of elderly patients after hip arthroplasty at the “Siguan” point. J Tongji Univ (Med Ed). (2017) 38:67–71. doi: 10.16118/j.1008-0392.2017.06.014
13.
Xu Q Jiang L He X Chen D . Effects of electroacupuncture on postoperative cognitive function and serum HIF-1α in elderly hip arthroplasty patients. J Guizhou Med Univ. (2019) 44:1320–4. doi: 10.19367/j.cnki.1000-2707.2019.11.015
14.
Yuan S . Clinical study on the recovery of cognitive function after general anesthesia in elderly patients with electroacupuncture at Baihui and Neiguan points. China Health Nutr. (2019)
15.
Zhang D Zhou J Chen Y Shi H . Effect of electroacupuncture hyperalgesia on postoperative cognitive function in elderly patients. Chin J Mod Nurs. (2014):162–5.
16.
Zeng K Wang G . A study of the effect of electroacupuncture stimulation on postoperative cognitive impairment after general anesthesia in elderly patients. Yunnan J Tradit Chin Med. (2018) 39:54–6. doi: 10.16254/j.cnki.53-1120/r.2018.06.024
17.
Zhang C Zhu L Yan D . Effects of electroacupuncture on the recovery of cognitive function after general anesthesia in elderly patients. Shanghai J Acupunct Moxibustion. (2015) 34:132–3. doi: 10.13460/j.issn.1005-0957.2015.02.0132
18.
Gao X Zhang Z Ma W . Effects of electroacupuncture-assisted general anesthesia on postoperative cognitive function in elderly patients. Chin J Integr Med. (2012) 32:591–3.
19.
Tang Y Mei Z Zhuang H Mao H He X Ma L et al . The effect of electroacupuncture at Yongquan, Shenmen and Baihui points on postoperative cognitive dysfunction in elderly patients. J Rare Dis. (2022) 29:94–6.
20.
Wan Y Zhou M . Effect of electroacupuncture preconditioning on postoperative cognitive function in elderly patients undergoing ureteral softscopic holmium laser lithotripsy. Shanghai J Acupunct Moxibustion. (2023) 42:12–6. doi: 10.13460/j.issn.1005-0957.2023.01.0012
21.
Zhao F Zhang Z Zhao Y Yan H Hong Y Xia X et al . Effect of electroacupuncture pretreatment on cognitive dysfunction in elderly patients after knee arthroplasty: a randomized controlled trial (English. World J Acupunct-Moxibustion. (2018) 28:231–236+309.
22.
Zheng J Jiang P Mao A Zhang Y . Effect of electroacupuncture prophylaxis on postoperative cognitive function and serum HIF-1α in elderly hip arthroplasty patients. Health Wellness Guide. (2023):199–201.
23.
Wang M Wang T . The efficacy of auricular acupuncture in treating postoperative cognitive dysfunction after general anesthesia in elderly hip arthroplasty patients. Modern Drug Appl China. (2024) 18:131–3. doi: 10.14164/j.cnki.cn11-5581/r.2024.03.035
24.
Zhuang L Zou L Pan X . Effects of phlegm-expelling and opening acupuncture on cognitive dysfunction and serum brain-derived trophic factor in elderly hip surgery patients. Inner Mongolia Trad Chinese Med. (2023) 42:106–7. doi: 10.16040/j.cnki.cn15-1101.2023.08.090
25.
Dong X Yue H Gao Y Jia Q Xie S Guan X . Pre-anesthetic electroacupuncture intervention against postoperative cognitive dysfunction in elderly patients. Chinese J Front Med (Electron Ed). (2016) 8:82–5.
26.
Li R Jiang Y Jiang X Cai L . Effect of snap-pin therapy on postoperative cognitive dysfunction in elderly hip fractures. Shanghai J Acupunct Moxibustion. (2022) 41:366–71. doi: 10.13460/j.issn.1005-0957.2022.04.0366
27.
Cai M Xin L Lang Y Hong S Wang W . Effect of cephalic premedication on delirium and cognitive function in elderly postoperative patients with intertrochanteric femoral fractures. Shanghai J Acupunct Moxibustion. (2022) 41:708–12. doi: 10.13460/j.issn.1005-0957.2022.07.0708
28.
Zhang L Xing H Tu C Wu J . The effect of wakefulness acupuncture on postoperative cognitive dysfunction in elderly patients undergoing general anesthesia hip arthroplasty. Hebei Trad Chinese Med. (2018) 40:1388–93.
29.
Songlin Y Cai S . The effect of brain-awakening acupuncture on postoperative cognitive dysfunction after general anesthesia in patients with cerebral infarction. Jilin Med. (2023) 44:909–12.
30.
Liu Z Teng Y . Effect of acupuncture combined with general anesthesia on postoperative cognitive function and related inflammatory factors in elderly tumor resection patients. Chin Med Herald. (2017) 14:76–9.
31.
Han X . Effect of acupuncture combined with anesthesia on postoperative cognitive function in elderly patients undergoing resection for intestinal cancer. Heilongjiang Zhong Yi Yao. (2018) 47:68–9.
32.
Zheng P . Effect of acupuncture combined with general anesthesia on cognitive function after resection of intestinal cancer in elderly patients. Clin Med. (2017) 37:11–3. doi: 10.19528/j.issn.1003-3548.2017.11.005
33.
Lin S Yin Z Gao J Wen H Zhou L . Effect of acupuncture anesthesia on cognitive dysfunction after resection of intestinal cancer and changes in its S-100β protein in elderly patients. Chin Acupunct Moxibustion. (2013) 33:63–6. doi: 10.13703/j.0255-2930.2013.01.024
34.
Jie J Guo J . Effects of acupuncture anesthesia on postoperative cognitive function and serum S100β, MMP-9, and BDNF protein levels in elderly patients undergoing radical rectal cancer surgery. Oncol Pharmacol. (2023) 13:84–8.
35.
Wang H . Effect of acupuncture anesthesia induction on postoperative cognitive function and inflammatory factors in elderly patients. China Trad Chinese Med Modern Distance Educ. (2019) 17:123–4.
36.
Zhao N Wu X Wu X Zhang R . Clinical efficacy of acupuncture to wake up four points in promoting cognitive recovery after general anesthesia in elderly patients. Modern Doctors China. (2021) 59:107–10.
37.
Luo Y Lin G Liu X Zhang L . Effect of acupuncture pretreatment on the efficacy and inflammatory factors in elderly patients with early postoperative cognitive dysfunction. Chinese Foreign Med Care. (2022) 41:195–8. doi: 10.16662/j.cnki.1674-0742.2022.35.195
38.
Liu Y . Effect of needle-medicine combination anesthesia on cognitive function and heart rate variability in elderly hip arthroplasty patients. J Qiqihar Med College. (2023) 44:1116–20.
39.
Jin G . Effects of needle and drug combination anesthesia combined with electrical stimulation on cognitive function and serum S-100β protein in patients undergoing abdominal surgery. J Liaoning Univ Tradit Chin Med. (2017) 19:196–8. doi: 10.13194/j.issn.1673-842x.2017.02.062
40.
Lin S Gao J Yin Z Zhou L Chen X . Effects of different frequencies of electroacupuncture in needle-medicine complex anesthesia on postoperative cognitive function in patients undergoing abdominal surgery. Chinese Acupunct Moxibustion. (2013) 33:1109–12. doi: 10.13703/j.0255-2930.2013.12.020
41.
Sun H Ji J Qian M . Effect of BIS-guided acupuncture combined with general anesthesia on early postoperative cognitive function in elderly patients undergoing radical gastric cancer surgery. J Clin Anesthesiol. (2018) 34:599–601.
42.
Wang N Ou Y Qing W . Combined acupuncture and general anesthesia on immune and cognitive function in elderly patients following subtotal gastrectomy for gastric cancer. Oncol Lett. (2018) 15:189–94. doi: 10.3892/ol.2017.7262
43.
Zhang Q Li YN Guo YY Yin CP Gao F Xin X et al . Effects of preconditioning of electro-acupuncture on postoperative cognitive dysfunction in elderly: a prospective, randomized, controlled trial. Medicine (Baltimore). (2017) 96:e7375. doi: 10.1097/md.0000000000007375
44.
Ho YS Zhao FY Yeung WF Wong GT Zhang HQ Chang RC . Application of acupuncture to attenuate immune responses and oxidative stress in postoperative cognitive dysfunction: what do we know so far?Oxidative Med Cell Longev. (2020) 2020:1–21. doi: 10.1155/2020/9641904
45.
Ho YS Cheng WY Lai MS Lau CF Wong GT Yeung WF et al . Postoperative electroacupuncture boosts cognitive function recovery after laparotomy in mice. Biomolecules. (2024) 14:1274. doi: 10.3390/biom14101274
46.
Wang XF Lin Q Wang GH Zhan GM Liu W Lin ZW . Electroacupuncture stimulation suppresses postoperative inflammatory response and hippocampal neuronal injury. Mediat Inflamm. (2022) 2022:1–9. doi: 10.1155/2022/3288262
47.
Zhang Q Li Y Yin C Yu J Zhao J Yan L et al . Electro-acupuncture pretreatment ameliorates anesthesia and surgery-induced cognitive dysfunction via inhibiting mitochondrial injury and nEuroapoptosis in aged rats. Neurochem Res. (2022) 47:1751–64. doi: 10.1007/s11064-022-03567-3
48.
Zhang X Chen H Li J Liu X Wang X Xue P et al . Effectiveness and safety of auricular acupuncture on adjuvant analgesia in patients with total knee arthroplasty: a randomized sham-controlled trial. Front Neurol. (2024) 15:1275192. doi: 10.3389/fneur.2024.1275192
49.
Usichenko TI Henkel BJ Klausenitz C Hesse T Pierdant G Cummings M et al . Effectiveness of acupuncture for pain control after cesarean delivery: a randomized clinical trial. JAMA Netw Open. (2022) 5:e220517. doi: 10.1001/jamanetworkopen.2022.0517
50.
He GL Gong XZ He JL Yang Q Mai JY Wu SN et al . Evaluation of the efficacy and safety of intradermal needle therapy on the sleep quality of patients following laparoscopic hysterectomy: study protocol for a randomized controlled trial. Ann Transl Med. (2022) 10:808. doi: 10.21037/atm-22-2980
51.
Zorrilla-Vaca A Healy R Grant MC Joshi B Rivera-Lara L Brown C et al . Correction to: intraoperative cerebral oximetry-based management for optimizing perioperative outcomes: a meta-analysis of randomized controlled trials. Can J Anaesth. (2019) 66:1427–9. doi: 10.1007/s12630-019-01380-1
52.
Liu J Zhang BL Cui FY Cao J Yu SY Kong Q et al . Scalp acupuncture targets for neurological disorders: evidence from neuroimaging studies (part 2). Zhen Ci Yan Jiu. (2024) 49:777–86. doi: 10.13702/j.1000-0607.20230016
53.
Peng XY Yuan B Li XL Bao YC Luo WJ Zhang YJ et al . Study on alleviating neuroinflammatory injury in ischemic stroke rats by electrical stimulation with scalp acupuncture based on IFN-γ mediated JAK/STAT1 signaling pathway. Zhen Ci Yan Jiu. (2023) 48:852–9. doi: 10.13702/j.1000-0607.20220842
54.
Wang JH Wang NN Yuan B He WJ Du XZ Jiang H et al . Anti-inflammation mechanism of electro-scalp acupuncture in treatment of ischemic stroke based on IL-12 mediated JAK/STAT signaling pathway. Zhongguo Zhen Jiu. (2022) 42:1137–44. doi: 10.13703/j.0255-2930.20210821-0006
Summary
Keywords
acupuncture, network meta-analysis, Mini-Mental State Examination, postoperative cognitive dysfunction, electroacupuncture
Citation
Liang W, Li M, Zhang J and Liang W (2025) The effects of different acupuncture modalities on postoperative cognitive function in elderly Chinese patients undergoing general anesthesia: a network meta-analysis. Front. Neurol. 16:1637566. doi: 10.3389/fneur.2025.1637566
Received
31 May 2025
Accepted
29 August 2025
Published
19 September 2025
Volume
16 - 2025
Edited by
Yonggang Zhang, Sichuan University, China
Reviewed by
Paulo Sargento, Escola Superior de Saúde Ribeiro Sanches, Portugal
Changzhen Gong, American Academy of Traditional Chinese Medicine, United States
Updates
Copyright
© 2025 Liang, Li, Zhang and Liang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianguo Zhang, zjgtcm@163.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.