 Osvaldo Pangrazio1
Osvaldo Pangrazio1 Alex S. Aguirre
Alex S. Aguirre Tina Bastin
Tina Bastin Alcy R. Torres
Alcy R. Torres- 1Department of Orthopedics, South American Football Confederation (CONMEBOL), Luque, Paraguay
- 2Department of Family Medicine, South American Football Confederation (CONMEBOL), Luque, Paraguay
- 3Department of Pediatrics, Boston Medical Center, Boston University Chobanian and Avedisian School of Medicine, Boston, MA, United States
Introduction: Sports-related concussions (SRC) are a pressing global health concern. However, countries in the Global South often lack standardized diagnostic criteria, and limited medical resources lead to inconsistent SRC detection. Our study presents a culturally adapted concussion detection protocol implemented by the region’s governing soccer federation, CONMEBOL.
Methods: The Concussion Fast Recognition Protocol (CFRP) was developed by adapting the Sport Concussion Assessment Tool, the Standardized Assessment of Concussion, and incorporating community-level input to ensure cultural relevance. The protocol was written in English, Spanish, and Portuguese. On-field medical teams completed the CFRP after each CONMEBOL match (N = 156) from 2022 to 2024, regardless of whether an SRC occurred. Players included in the study (N = 5,928) ranged in age from 15–44 years.
Results: A total of 27 concussions were identified, all of which were immediately removed from play. Most concussions (37.04%) occurred during the 21–45-min period, and 59.26% involved away-team athletes. The incidence rate per 1,000 player-hours was 2.61. Game temperatures ranged from 7 °C to 36 °C, and the maximum altitude reached 4,150 meters. The distance covered by players ranged from 550 to 6,100 meters. Incidence rates per 1,000 player-hours were calculated.
Discussion: This first large-scale, prospective SRC study in South American soccer demonstrates effective implementation of a regional protocol and identifies context-related trends in SRC risk. The findings underscore the importance of a culturally appropriate protocol and contribute novel data to global concussion literature.
1 Introduction
Sports-related concussions represent a growing public health concern, particularly in soccer which is a sport with global participation and popularity (1, 2). Concussions account for approximately 22% of all soccer-related injuries, highlighting the substantial risk of head trauma despite the physical and mental health benefits of athletic engagement (1, 3). Concussion is defined as a traumatic brain injury that results in transient alterations in brain function, often caused by biomechanical forces. In soccer, concussions most commonly result from player-to-player contact, but may also occur due to collisions with the playing surface or equipment (1, 3). Concussions fit into the milder form of classification of a traumatic brain injury (TBI) with usually a Glasgow Coma Scale (GCS) score of 13–15. Lower scores of GCS are considered moderate or severe TBI and do not fit into a concussion definition (4). Figure 1 shows the red flags and warning signs on the CFRP protocol created by the Medical Commission of CONMEBOL to guide management of concussions (5).
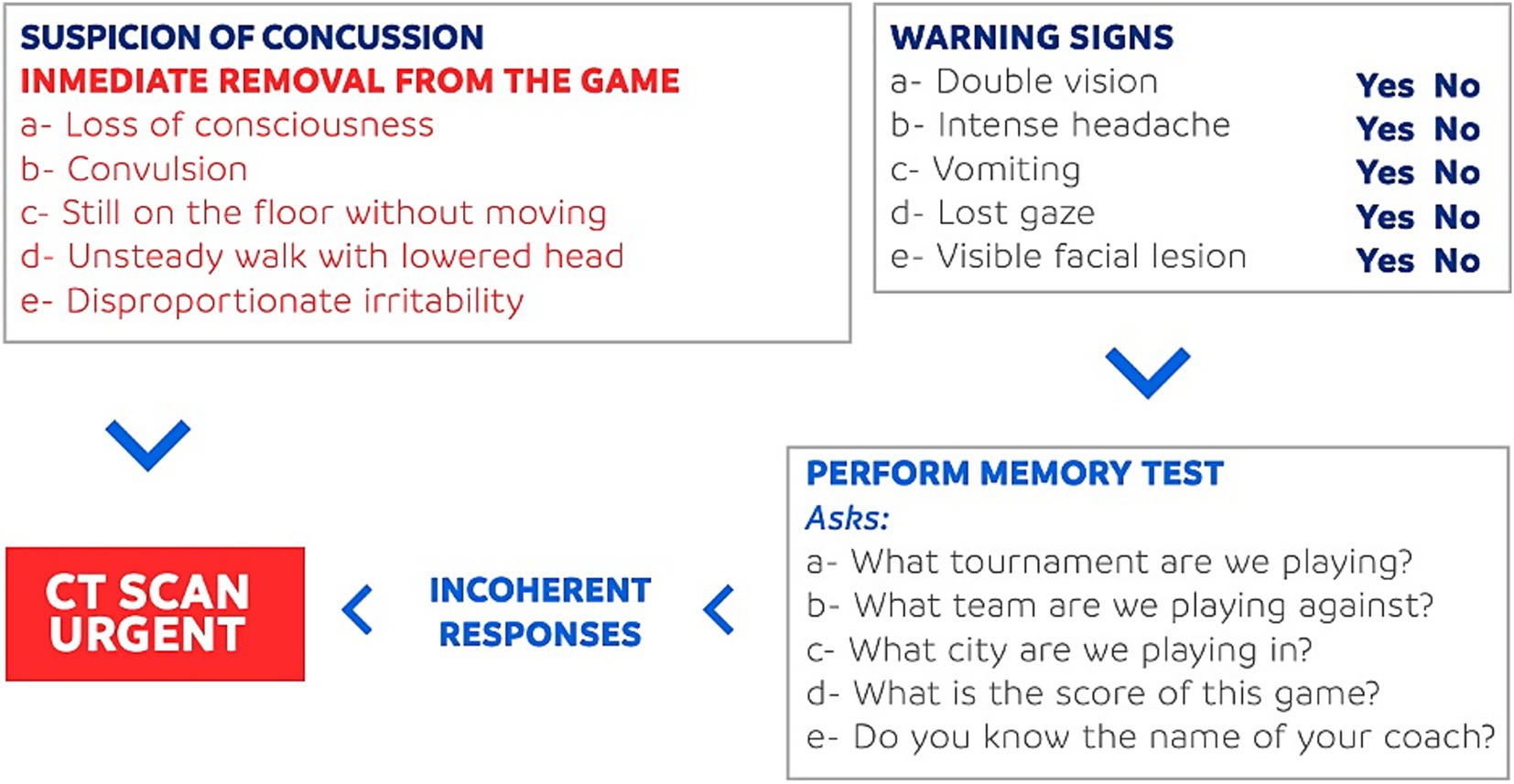
Figure 1. CFRP protocol by CONMEBOL.
Despite growing awareness, the true incidence of concussion remains underestimated (6). Current surveillance systems, such as those by the Centers for Disease Control and Prevention (CDC), primarily track cases involving loss of consciousness, a symptom present in fewer than 10% of all concussions, leading to under recognition and underreporting (7). The short and long-term consequences of concussion are well documented, ranging from impairments in cognitive processing and emotional regulation to delayed physical recovery (8). Notably, athletes who continue to play after sustaining a concussion face significantly longer recovery times, with delays in removal from play linked to prolonged symptom duration and increased risk of further injury (9, 10). These findings underscore the critical need for timely recognition and appropriate management of concussions in sport.
To address this, standardized concussion protocols have been developed and implemented at both national and international levels. Tools such as the Sport Concussion Assessment Tool (SCAT6) provide structured guidelines for identification, removal from play, and return-to-play decisions (11). In South America, the Confederación Sudamericana de Fútbol (CONMEBOL) introduced the Concussion Fast Recognition Protocol (CFRP) to improve on-field concussion detection and management in professional soccer (8, 12). Despite these advancements, the successful implementation of concussion protocols remains inconsistent across regions, often hindered by limited medical resources, lack of culturally and linguistically validated tools, and variable awareness among stakeholders. This study aims to evaluate the application and efficacy of the CFRP in South American soccer and correlate it with data from international leagues to generate informed decisions in the future.
2 Methods
Concussions from CONMEBOL Libertadores and Sudamericana tournaments were registered prospectively from the beginning to end of those tournaments during 2022 to 2024. A total of 156 games were analyzed retrospectively from the data collected to understand the concussion rates in professional soccer tournaments and consequently identify players adherence to concussion protocols (Table 1). The concussions were identified in each game by the referee, and the information was shared with the medical board of CONMEBOL using the Concussion Fast Recognition Protocol, a tool to report concussions validated by this organization. Additionally, each team’s physician staff signed a document confirming the concussion and agreeing on following the concussion protocol. A CFRP report was completed after every match even if no concussion was identified.
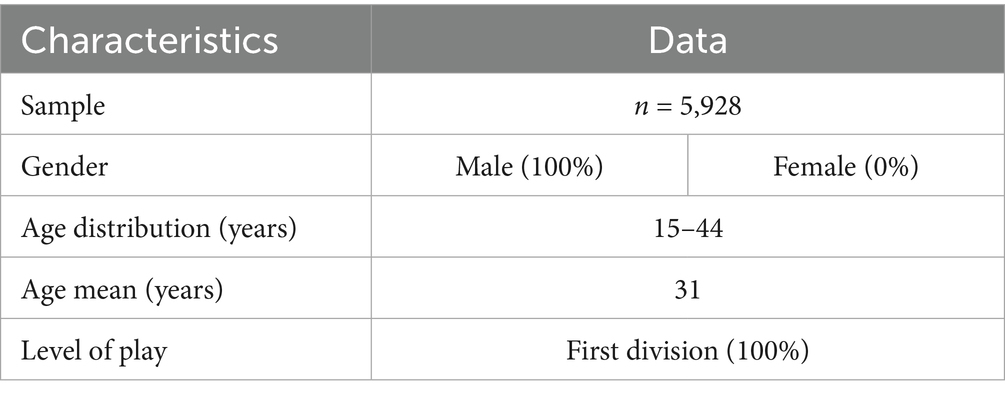
Table 1. Characteristics of study population.
If a concussion was suspected, the team’s health staff evaluated the player. The injured player was removed from the game when necessary, and a report describing all the incident details was filed. The data were analyzed in relationship with international data to provide a comprehensive review of how soccer protocols are typically applied.
3 Results
A total of 27 concussions were identified. All concussed players were removed from the field following the protocol. There were 145 teams that played over 930 games with 5,928 players. Most of the games were played between March and May, where most concussions happened compared to later stages of the tournaments (October to November). The temperature in the tournament ranged from 7 °C to 36 °C. The highest altitude for a game was 4,150 m in El Alto, Bolivia. The distance that players had to run ranged from 550 to 6,100 meters. The distance was measured by multiple camera systems with specialized software. The age of the players ranged from 15 to 44. In general, there were a higher number of concussions in the first half of games (16 compared to 11 in the later half), specifically close to the half time between minutes 21–45 as seen in Figure 2. There were 12 concussions in midfielders, 9 concussions in defenses, and 5 concussions in forwards as seen in Table 2 and Figure 3. The data show a higher number of concussions in the visitor side (16 compared to 11 in the home team). The concussion rate per 1,000 player-hours was 2.61. There was no specific team or city where concussions happened more frequently.
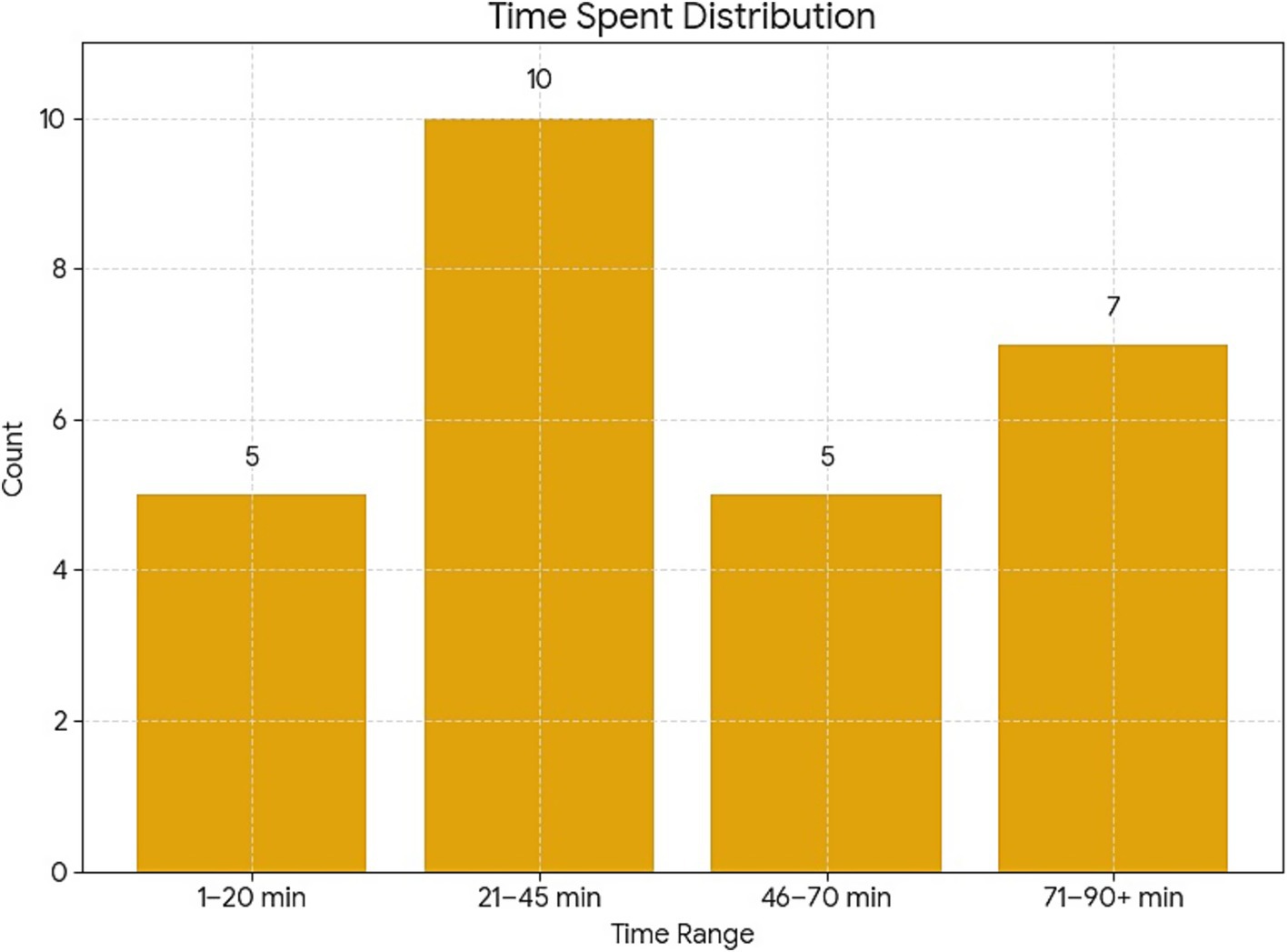
Figure 2. Concussion numbers according to period of the game.

Table 2. Concussion rates per 1,000 player-hours by position (GK: goalkeeper, DEF: defenses, MID: midfielders, FWD: forwards).
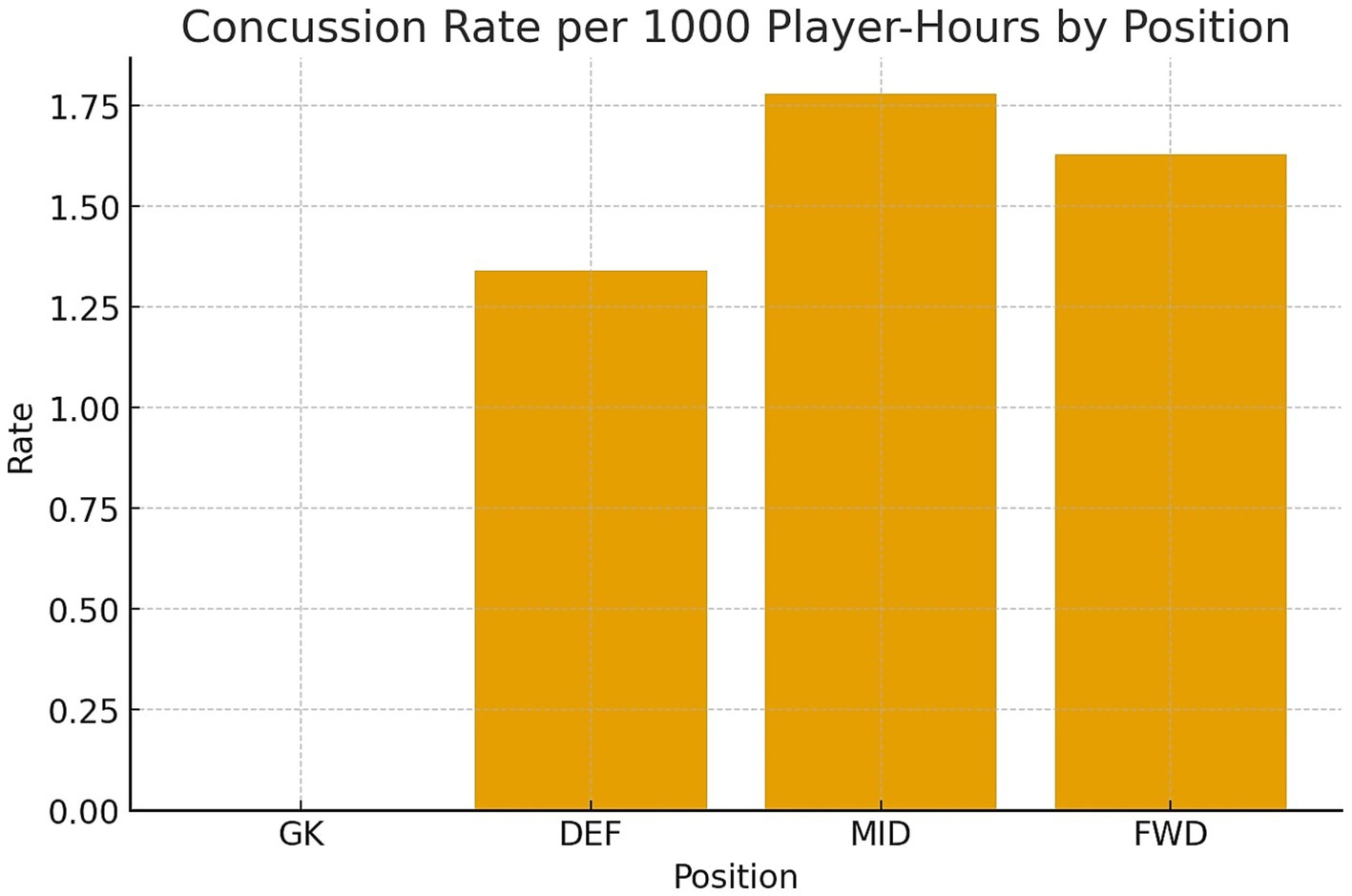
Figure 3. Concussion rates per 1,000 player-hours by specific position (GK, goalkeeper; DEF, defenses; MID, midfielders; FWD, forwards).
4 Discussion
This study underscores the critical and growing public health concern of sports-related concussions in professional soccer, particularly within South American tournaments governed by CONMEBOL. The implementation of the Concussion Fast Recognition Protocol (CFRP) appears to have contributed positively to the identification and management of concussion events. Out of all the games, only 156 games were analyzed because these were the only games included the CFRP. From the 156 games, 27 concussions were identified, yielding a concussion rate of 2.61 per 1,000 player-hours which is comparable to the upper ranges reported in leagues such as Major League Soccer (13.48 per 1,000 player-hours was calculated from article data, 20.22 per 1,000 athlete-exposures reported) and the English Premier League (12.45 per 1,000 player-hours was calculated from article data, 18.68 per 1,000 athlete-exposures reported), and significantly higher than figures from French men’s football (0.44 per 1,000 player-hours were reported) and Swedish elite soccer (1.19 per 1,000 player-hours were reported) (13–16).
Encouragingly, all concussions observed in this study were managed in accordance with CFRP guidelines, including timely removal from play and appropriate documentation. Not following protocols or allowing players to continue playing has been evidenced in other leagues such as the professional French football where a review revealed a consistent trend of disregard for concussion management guidelines. In the review of the French league, more than half (53%) of concussed players went back to the game, and over a quarter (28%) were not even medically evaluated on the field. This behavior goes against official recommendations from governing bodies (14). Nevertheless, this study reflects a growing adherence to the protocol and stands in contrast to findings from other leagues (13–16). Similarly, during the 2016 UEFA European Championship, only 27.5% of potential concussive events (PCEs) were medically evaluated, despite most of those players exhibiting clear concussion symptoms (13).
These findings emphasize that the existence of standardized protocols alone is insufficient; effective implementation, accountability, and a culture of safety are equally essential. The American Medical Society for Sports Medicine (AMSSM) has advocated for strict adherence to evidence-based concussion protocols, including rapid sideline assessment and a supervised, graduated return-to-play process (17). However, studies consistently show gaps in compliance across multiple elite leagues, suggesting that awareness and infrastructure may be lagging behind clinical guidance (13–15).
The current study also revealed patterns that may inform injury prevention strategies. A greater number of concussions occurred in the first half of games, especially between minutes 21–45, which may relate to the physical escalation of gameplay or a transitional period where mental and physical fatigue begin to emerge. There was also a higher number of concussions among visiting teams, possibly due to travel-related stressors, unfamiliar environments, or differences in acclimatization to temperature and altitude. Notably, the tournament featured different altitude conditions (up to 4,150 meters in El Alto, Bolivia) and temperatures ranging from 7 °C to 36 °C, yet no specific environmental variable appeared directly correlated with increased concussion risk, though further research with larger datasets may clarify these relationships.
The distribution of injuries by position also aligns with global data, where defenders and midfielders who are frequently involved in high-contact and high-intensity scenarios tend to have higher injury rates (18–20). Furthermore, the occurrence of increased number of concussions near the end of matches compared to the beginning of the second half suggests that fatigue and decreased vigilance may elevate risk, pointing to a need for additional medical monitoring during the closing stages of play (18, 19). This could include increasing the availability of medical staff during late-game periods or enforcing mid-game screening tools for players involved in high-impact events.
Limitations of this study include reliance on referee and medical staff identification for initial concussion recognition, which may allow some cases to go undetected, especially in the absence of loss of consciousness, which occurs in less than 10% of concussions (7). Additionally, while protocol adherence was documented, the post-removal care quality and return-to-play compliance were not assessed, which are essential components of effective concussion management. Another limitation was the retrospective analysis that does not include a follow up of the players with concussions. The sample size and gender (only male players) also limit generalizability, and the observational design precludes causal inference.
Future research should explore longitudinal follow-up of concussed athletes to assess long-term outcomes, protocol compliance over time, and the impact of educational interventions for coaching staff and referees. Integrating technology such as sideline video replay and head impact sensors may also improve detection and reporting accuracy.
5 Conclusion
In summary, this study underscores the importance and impact of standardized concussion protocols in professional soccer. The CFRP shows promise as a practical tool for improving athlete safety in South America, though its success hinges on continued investment in education, infrastructure, and regional adaptation. As awareness of concussion risks grows, ongoing research and cross-continental collaboration will be vital to ensuring player health remains a central priority in global sport.
Data availability statement
The original contributions presented in the study are publicly available. This data can be found here: https://data.mendeley.com/datasets/xdc29f7k44/1.
Author contributions
OP: Project administration, Resources, Formal analysis, Writing – review & editing, Methodology, Supervision, Writing – original draft, Conceptualization. FF: Conceptualization, Writing – original draft, Resources, Supervision, Writing – review & editing, Project administration, Methodology, Formal analysis. AA: Methodology, Data curation, Conceptualization, Visualization, Writing – review & editing, Formal analysis, Resources, Writing – original draft, Validation. TB: Writing – review & editing, Writing – original draft. AT: Writing – review & editing, Formal analysis, Writing – original draft, Methodology, Conceptualization, Supervision, Resources.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The South American Football Confederation (CONMEBOL), President Alejandro Dominguez and Arturo Montero for their support to develop the best scientific evidence available in professional soccer.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Demetriades, AK, Shah, I, Marklund, N, Clusmann, H, and Peul, W. Sport-related concussion in soccer—a scoping review of available guidelines and a call for action to FIFA & soccer governing bodies. Brain Spine. (2024) 4:102763. doi: 10.1016/j.bas.2024.102763
2. Pierpoint, LA, and Collins, C. Epidemiology of sport-related concussion. Clin Sports Med. (2021) 40:1–18. doi: 10.1016/j.csm.2020.08.013
3. Levy, ML, Kasasbeh, AS, Baird, LC, Amene, C, Skeen, J, and Marshall, L. Concussions in soccer: a current understanding. World Neurosurg. (2012) 78:535–44. doi: 10.1016/j.wneu.2011.10.032
4. Kazl, C, and Torres, A. Definition, classification, and epidemiology of concussion. Semin Pediatr Neurol. (2019) 30:9–13. doi: 10.1016/j.spen.2019.03.003
6. Kimbler, DE, Murphy, M, and Dhandapani, KM. Concussion and the adolescent athlete. J Neurosci Nurs. (2011) 43:286–90. doi: 10.1097/JNN.0b013e31823858a6
7. Clark, M, and Guskiewics, K. Translational research in traumatic brain injury. Boca Raton, FL: CRC Press (2016).
8. Pangrazio, O, Forriol, F, Aguirre, AS, Beletanga, MD, and Torres, AR. Enhancing protocols for concussion management in professional soccer events. Cureus. (2024) 16:e64064. doi: 10.7759/cureus.64064
9. Elbin, RJ, Sufrinko, A, Schatz, P, French, J, Henry, L, Burkhart, S, et al. Removal from play after concussion and recovery time. Pediatrics. (2016) 138:e20160910. doi: 10.1542/peds.2016-0910
10. Asken, BM, McCrea, MA, Clugston, JR, Snyder, AR, Houck, ZM, and Bauer, RM. “Playing through it”: delayed reporting and removal from athletic activity after concussion predicts prolonged recovery. J Athl Train. (2016) 51:329–35. doi: 10.4085/1062-6050-51.5.02
11. Echemendia, RJ, Meeuwisse, W, McCrory, P, Davis, GA, Putukian, M, Leddy, J, et al. The Sport Concussion Assessment Tool 5th edition (SCAT5): background and rationale. Br J Sports Med. (2017):848–50. doi: 10.1136/bjsports-2017-097506
12. Pangrazio, O, Forriol, F, Pagura, J, Pedrinelli, A, Roby, M, Mazzoca, G, et al. Protocolo de Recomendaciones Medicas Competencias. Luque: CONMEBOL (2023).
13. Abraham, KJ, Casey, J, Subotic, A, Tarzi, C, Zhu, A, and Cusimano, MD. Medical assessment of potential concussion in elite football: video analysis of the 2016 UEFA European championship. BMJ Open. (2019) 9:e024607. doi: 10.1136/bmjopen-2018-024607
14. Cassoudesalle, H, Laborde, B, Orhant, E, and Dehail, P. Video analysis of concussion mechanisms and immediate management in French men’s professional football (soccer) from 2015 to 2019. Scand J Med Sci Sports. (2021) 31:465–72. doi: 10.1111/sms.13852
15. Ramkumar, PN, Navarro, SM, Haeberle, HS, Luu, BC, Jang, A, Frangiamore, SJ, et al. Concussion in American versus European professional soccer: a decade-long comparative analysis of incidence, return to play, performance, and longevity. Am J Sports Med. (2019) 47:2287–93. doi: 10.1177/0363546519859542
16. Vedung, F, Hänni, S, Tegner, Y, Johansson, J, and Marklund, N. Concussion incidence and recovery in Swedish elite soccer—prolonged recovery in female players. Scand J Med Sci Sports. (2020) 30:947–57. doi: 10.1111/sms.13644
17. Harmon, KG, Drezner, JA, Gammons, M, Guskiewicz, KM, Halstead, M, Herring, SA, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. (2013) 47:15–26. doi: 10.1136/bjsports-2012-091941
18. Nilsson, M, Hägglund, M, Ekstrand, J, and Waldén, M. Head and neck injuries in professional soccer. Clin J Sport Med. (2013) 23:255–60. doi: 10.1097/JSM.0b013e31827ee6f8
19. Jo, J, Boltz, AJ, Williams, KL, Pasquina, PF, McAllister, TW, McCrea, MA, et al. Mechanisms of injury leading to concussions in collegiate soccer players: a CARE consortium study. Am J Sports Med. (2024) 52:1585–95. doi: 10.1177/03635465241240789
Keywords: concussion, trauma, brain, soccer, protocol, global
Citation: Pangrazio O, Forriol F, Aguirre AS, Bastin T and Torres AR (2025) Concussions analysis in 2022–2024 CONMEBOL soccer tournaments. Front. Neurol. 16:1645543. doi: 10.3389/fneur.2025.1645543
Edited by:
Hongyou Liu, South China Normal University, ChinaReviewed by:
Colin Wallace, Okanagan College, CanadaGerard Hageman, Medisch Spectrum Twente, Netherlands
Copyright © 2025 Pangrazio, Forriol, Aguirre, Bastin and Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alcy R. Torres, YXJ0b3JyZXNAYnUuZWR1