Abstract
Benign paroxysmal positional vertigo (BPPV)-related residual dizziness (RD), a type of dizziness following successful treatment of BPPV, has been increasingly recognized, with a reported prevalence ranging from 23 to 70%. BPPV-related RD is characterized by non-specific dizziness in the absence of positional vertigo and nystagmus. It can be very distressing and lead to substantial impacts on the quality of life and morbidity, especially the risk of falling. This review examines the risk factors and underlying mechanisms contributing to BPPV-related RD, focusing on peripheral and central mechanisms. Based on clinical experience, two subtypes of BPPV-related RD are suggested: type 1, the classic BPPV-related RD occurring after canalith repositioning maneuvers; and type 2, a novel subtype arising after spontaneously resolved BPPV that requires a history of BPPV but not previous confirmation by clinical examination (subjective BPPV). This review introduces a special online algorithm, the Clinician-Led Evaluation for Assessment of Residual dizziness (CLEAR), to help clinicians recognize patients with BPPV-related RD, and reviews follow-up strategies. The aim is to help specialist ear, nose, and throat clinicians and neurologists recognize BPPV-related RD quickly and follow up appropriately to resolve symptoms as quickly as possible.
Graphical Abstract

CLEAR (Clinician-Led Evaluation for Assessment of Residual dizziness): Recognition, risk factors and potential follow-up strategies for BPPV-related RD.
1 Introduction
Benign paroxysmal positional vertigo (BPPV)-related dizziness (RD) is defined as a sensation of non-specific dizziness in the absence of positional vertigo and typical nystagmus that follows successful treatment with canalith repositioning maneuvers (CRMs) of BPPV (1). BPPV-related RD is being reported increasingly (1). Given the high levels of undiagnosed BPPV at all ages (2), particularly in older individuals (3), it is reasonable to consider that the prevalence of BPPV-related RD is much higher than that currently reported in the literature. In addition, the increase in the reported prevalence is mirrored by an increase in the number of studies investigating the risk factors for RD, especially in patients aged >50 years. BPPV-related RD is likely to be a heterogeneous condition, and this review focuses on how to improve the recognition of patients with a high risk of BPPV-related RD and provide follow-up strategies to reduce or manage this risk according to the underlying etiology.
Patients with BPPV-related RD have reported symptoms, such as continuous or intermittent lightheadedness (4–7), floating sensation (5), head heaviness (8), and imbalance/unsteadiness (4, 7, 8), combined with a clinical history of BPPV resolved after CRMs.
Although BPPV-related RD may be evaluated using scores generated by questionnaires such as the Dizziness Handicap Inventory, Visual Vertigo Analog Scale, and Vertigo Symptom Scale, these have not yet been validated for the diagnosis of BPPV-related RD. Displacement of otoconia from the utriculus into the semicircular canals has been suggested as the primary cause of BPPV (1), and the associated utricular pathology might also play a role in BPPV-related RD. However, objective measures to assess utricular function have not been established yet (1).
Whether dizziness symptoms that remain after a successful CRM for BPPV are present at the time of BPPV diagnosis or whether they are new symptoms that develop after CRM is not known and will be hard to differentiate due to factors that may obscure the distinction between vertigo and dizziness, such as the following:
-
i) the similarity between dizziness and vertigo symptoms and the often interchangeable use of the terms (although dizziness is a general feeling of being off-balance, whereas vertigo is the feeling that you or your surroundings are moving or spinning),
-
ii) the vertigo symptoms may overwhelm the dizziness, such that the dizziness is simply absorbed into the vertigo diagnosis, and
-
iii) patients may have been feeling dizzy before the BPPV but were managing their symptoms and did not report them.
There is clearly an unmet need to improve the definition and diagnosis of BPPV-related RD so that patients can be given appropriate advice or treatment to assist in their recovery.
2 Prevalence of BPPV-related RD
A systematic review and meta-analysis of risk factors for BPPV-related RD from 31 papers highlighted a wide range of reported prevalence, from 23 to 70% (9). Most of the studies included in the review had small sample sizes, ranging from 20 to 281 patients with BPPV-related RD (17/31 studies included < 50 patients with BPPV-related RD; Figure 1). The two largest cohorts were from >10 years ago, highlighting the limitations of the available data in making accurate statements regarding the prevalence of BPPV-related RD. The disparities in reported prevalence may also reflect the focus of the studies (Figure 2) and/or population differences, as 22 studies were conducted in China.
Figure 1

Studies in BPPV-related RD have small cohorts, with a trend toward an association between cohort size and prevalence (9). BPPV, benign paroxysmal positional vertigo; RD, residual dizziness.
Figure 2

The relatively narrow focus of interest for studies of risk factors for BPPV-related RD (9). BPPV, benign paroxysmal positional vertigo; CRP, canalith repositioning procedure; cVEMP, cervical vestibular evoked myogenic potential; DHI, Dizziness Handicap Inventory; oVEMP, ocular vestibular evoked myogenic potential; RD, residual dizziness.
Positional nystagmus may be considered a common finding amongst healthy individuals without a typical history of BPPV (10). However, this common finding does not increase the incidence of BPPV-related RD (or result in its overdiagnosis), as BPPV-related RD can only be defined when there is a confirmed diagnosis of prior BPPV or a clinical history that has been confirmed by a specialist as highly suggestive of spontaneously resolved BPPV. Furthermore, in patients with a confirmed diagnosis of previous BPPV or a clinical history strongly indicative of spontaneously resolved BPPV as confirmed by a specialist, any remaining nystagmus should not be classified as RD but rather suggests the presence of an otolith that has not yet been repositioned. Accurate diagnosis requires a detailed clinical history to assess whether the patient has no clinical history of BPPV or a clinical history highly suggestive of BPPV.
3 Impact of BPPV-related RD
BPPV-related RD symptoms are very distressing to patients, and the ensuing morbidity and poor quality of life (QOL) have been described as formidable and intimidating in a study in India (7). Although this study had relatively few patients reporting BPPV-related RD, those who did reported that they had not regained their sense of stability, indicating that the impact of the BPPV-related RD was worse than the BPPV itself, as they could avoid vertigo by not bending the head into the provoking position but could not avoid the BPPV-related RD symptoms (7). In a meta-analysis of 14 articles, dizziness in older adults was associated with significantly higher odds of any type of future fall and was an independent predictor of future falls (11). Dizziness in the elderly has also been linked to isolation, depression, and reduced self-autonomy and self-control (12). Data from the 2001 to 2004 National Health and Nutrition Examination Surveys in 5,086 US adults aged ≥40 years identified that 35.4% had vestibular dysfunction, as measured by the modified Romberg Test of Standing Balance on Firm and Compliant Support Surfaces, with increased odds based on age and the presence of diabetes mellitus (13). Participants with vestibular dysfunction who reported dizziness had a 12-fold increase in the odds of falling, which is noted as being among the most morbid and costly health conditions affecting older individuals in the US (13). We hypothesize that BPPV-related RD might have a similar impact as the dizziness mentioned above.
Studies on BPPV have reported that ~86% of patients with BPPV will suffer some interrupted daily activities, and, for patients of working age, this includes lost workdays (14). Although BPPV can occur at all ages, there are few, if any, studies on BPPV-related RD in children or young adults, and very few that include adults aged < 50 years. A retrospective analysis of 203 children (mean age, 11.16 ± 3.87, range 1–17 years) who underwent vestibular assessment in a vertigo center in a tertiary hospital over a 3-year period reported that BPPV was the most common diagnosis (49%), which included both primary and secondary BPPV that was associated with other vestibular pathologies (15). Another pediatric study reported that BPPV is a relatively frequent cause of dizziness in children, with common delays in identification and treatment (16). In a study of recurrent dizziness, defined as episodes of dizziness several times a week during the last 6 months, in >40,000 Danish children aged 11–15 years, dizziness was significantly associated with short sleep duration, skipping breakfast, use of alcohol and tobacco, loneliness, low life satisfaction, low self-esteem, exposure to bullying at school, high schoolwork pressure, low school satisfaction, underweight, overweight, poor self-rated health, chronic illness, injuries in the last year, headache, stomach ache, back pain, feeling low, irritability/bad temper, nervousness, difficulties falling asleep, and poor/restless sleep (17). Although this form of dizziness is not related to BPPV, we hypothesize that the impact of any significant dizziness, including BPPV-related RD in children, would be similar. However, to the best of our knowledge, no BPPV-related RD has been reported in pediatric studies.
4 Risk factors for BPPV-related RD
Several risk factors have been proposed for BPPV-related RD symptoms (1). A meta-analysis of 4,487 patients from 31 studies identified age, female sex, secondary BPPV, a longer duration of BPPV before treatment, abnormal ocular vestibular evoked myogenic potential (oVEMP), abnormal cervical vestibular evoked myogenic potential (cVEMP), a higher Dizziness Handicap Index (DHI) score before treatment, anxiety, osteopenia, onset in winter, and a history of BPPV as risk factors for BPPV-related RD in patients with BPPV after successful repositioning. The following did not correlate with the occurrence of BPPV-related RD: the affected side, location or type of semicircular involvement, hyperlipidaemia, diabetes, hypertension, heart disease, migraine, sleep disorders, canalolithiasis/cupulolithiasis, the number of times a CRM was performed, and the number of vertigo attacks (9). A correlation between BPPV-related RD and age has also been reported in studies not included in the meta-analysis (18, 19). Although 12 studies in the meta-analysis by Ke et al. (9) reported that the number of CRMs may be a risk factor, the classification of the number of CRMs varied between studies, and the authors concluded that the reliability of the results was questionable. Other studies have reported that hypertension and diabetes are risk factors (20, 21). In addition, despite a high level of interest in the potential for vitamin D deficiency to be a risk factor for BPPV-related RD, only one study has reported a potential association between low levels of 25(OH)D in female patients aged < 50 years and an increased risk of moderate-to-severe BPPV-related RD 1 week after successful CRMs (22).
With regard to the relationship between oVEMPs and cVEMPs, there is currently no indisputable evidence in humans that VEMPs can provide specific information on otolith function. Some studies in patients with BPPV have noted abnormal cVEMP and oVEMP values compared with healthy controls (23, 24). One study suggested that most changes were noted in oVEMPs, suggesting that utricular dysfunction may be more common (especially in the earlier stages) than saccular dysfunction, although the entire vestibule was affected (24). Furthermore, patients with greater utricle and superior vestibular nerve involvement, as measured by oVEMP, showed delayed clinical recovery, suggesting a possible prognostic role of the test (24). In contrast, studies in patients with BPPV-related RD have suggested that the absence of cVEMP could increase the risk of BPPV-related RD (25, 26). Nevertheless, despite the debate regarding the contribution of non-otolith afferents to VEMPs, it is agreed that VEMPs originate from the transient otolith system and not from the sustained otolith system. BPPV-related RD is more likely to be caused by dysfunction in the sustained system, thereby making the use of VEMPs less useful (27). Overall, more research is needed to fully understand the implications of normal or abnormal VEMP responses in BPPV- and BPPV-related RD, and it should be noted that abnormal responses in any other vestibular test might be correlated with BPPV-related RD.
It is clear from the wide range of reported incidence rates and risk factors that BPPV-related RD is a heterogeneous condition with several underlying etiologies. It has been suggested that there may be no explanation for the cause of BPPV-related RD in >50% of patients (28). It is also likely that BPPV-related RD may differ between populations. For example, it has been reported that Asian people are 2.6 times more likely to present with BPPV compared with their Caucasian counterparts (29), possibly related to the higher prevalence of diabetes mellitus and its complications in the Asian population (30).
The recurrence of BPPV shares many of the same risk factors with BPPV-related RD. A recent meta-analysis of 14 predominantly Asian studies involving 3,060 BPPV patients reported that BPPV recurrence was closely related to female sex, hypertension, diabetes mellitus, hyperlipidaemia, osteoporosis, and vitamin D deficiency (31). This supports an earlier study of >1,000 BPPV patients in 11 centers across seven countries, in which ≥1 and ≥2 comorbid disorders (hypertension, diabetes, osteoarthrosis, osteoporosis, or depression) were found in 20 and 37% of subjects with recurrent BPPV, respectively (32). A reduction in bone mineral density has been reported to be independently associated with BPPV-related RD (33). More large-scale prospective studies in different countries are required to further investigate the risk factors for BPPV-related RD and how they might differ based on ethnicity.
5 Proposed mechanisms for BPPV-related RD
The proposed mechanisms for the development of BPPV-related RD are related to effects in the peripheral and central vestibular systems (1) (Figure 3). These mechanisms are not mutually exclusive, and their relative contributions may explain the reported differences in the risks and/or incidence of BPPV-related RD and relate to the duration and/or severity of symptoms. Understanding their roles and identifying them in patients may help guide clinicians in the management of patients.
Figure 3

Peripheral and central causes of residual dizziness. Adapted from Özgirgin ON, et al. Corrigendum: Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers. Front Neurol. 2024 Jul 29;15:1461600. doi: 10.3389/fneur.2024.1461600 Erratum for: Front Neurol. 2024 May 24;15:1382196. doi: 10.3389/fneur.2024.1382196 (1). BPPV, benign paroxysmal positional vertigo; RD, residual dizziness; VOR, vestibular ocular reflex; VSR, vestibular spinal reflex.
5.1 Peripheral causes of BPPV-related residual dizziness
5.1.1 Persistence of otoconial debris
Incomplete repositioning during CRM can result in residual otoconial debris that is sufficient to cause mild positional vertigo or less specific chronic or positional dizziness but insufficient to deflect the cupula to the degree required to provoke overt nystagmus (1). Furthermore, although CRM may clear debris from the canal, it may not completely resolve the utricular pathophysiology and, therefore, contribute to or cause BPPV-related RD.
5.1.2 Effects of aging
The incidence of both BPPV and BPPV-related RD increases with age, thought to be due, in part, to age-related otoconial degeneration and vestibular hair cell loss (34). Animal studies have provided evidence for a relationship between osteopenia and changes in otoconial structure (35), which is supported by several clinical studies on BPPV (2). For example, among 32 women aged 50–85 years with idiopathic BPPV, 75% had osteopenia/osteoporosis on dual X-ray absorptiometry (36). A seasonal incidence of BPPV (37, 38) and BPPV-related RD has also been reported (9), which may be related to the association between winter months and low vitamin D levels and subsequently on bone mass through effects on calcium and bone metabolism (39, 40). Older adults are already at risk of vitamin D insufficiency due to decreased cutaneous synthesis and dietary intake (41). In addition, cupulolithiasis, in which free-floating endolymph debris adheres to the cupular membrane and renders the canal responsive to gravity, appears to be more likely in older patients and is more resistant to effective treatment with CRMs (1, 42).
5.1.3 Endolymph calcium levels
Animal studies have shown that otoconia can dissolve in the endolymph within approximately 20 h; however, high endolymphatic Ca2+ levels slow the time of otoconia dissolution considerably (2, 43). Therefore, it is possible that a critical mass of otolith debris may accumulate in patients with high endolymphatic Ca2+ levels and cause BPPV-related RD symptoms (1). The biologically active form of vitamin D is involved in the upregulation of epithelial Ca2+ channel transporters that maintain low endolymph Ca2+ concentrations in the inner ear (22).
5.1.4 Microcirculatory dysfunction
Blood vessels inside the cochlea have no collateral circulation. Otolith detachment in idiopathic BPPV may be secondary to ischaemia of the neuroepithelium of the utricular macula or semicircular canals (1). A combination of hypertension and diabetes may lead to tissue hypoxia and cochleovestibular degeneration (44). Hyperinsulinism may disrupt inner ear haemostasis and alter the ionic and metabolic characteristics of the stria vascularis, while hyperglycaemia increases vascular resistance by inhibiting nitric oxide-related vasodilation (45). Arterial plaques may trigger intravascular thrombosis and cause hypoperfusion of the inner circulation (45). Comorbid type 2 diabetes is associated with an increase in BPPV rates, often mediated by concurrent hypertension (29), which may be undiagnosed in around one-third of patients presenting with any type of vertigo (46). The incidence of hypertension and orthostatic hypotension in patients with BPPV-related RD has been reported as significantly higher than that in patients without BPPV-related RD (6, 47). Patients with BPPV and a combination of cardiovascular comorbidities, especially elderly patients with white matter hyperintensity, an indicator of chronic microvascular ischaemia, are more likely to develop BPPV-related RD (48). In a study of 149 patients with BPPV-related RD, 78 did not resolve spontaneously; most had high blood pressure and/or diabetes, 47 had hyperlipidaemia, 110 had heart disease, and 43 had ischaemic encephalopathy (21). Epidemiological evidence has also indicated an association between low vitamin D levels and diseases that affect microcirculation, such as hypertension (49) and diabetes (41, 50).
5.1.5 Insufficient/inadequate CRMs
The outcome of CRM is dependent on the type and precise execution of the maneuver, the latter being affected by the angle and angular velocity of the head and the duration of each step, fluid dynamics, and the amount, size, and location of otoconia in the canal (1). CRMs may be less effective in patients with secondary BPPV or lateral canal cupulolithiasis, with the latter being more common than other types of BPPV in older patients (1, 51).
The clinical relevance of the various proposed risk factors is summarized in Table 1, which includes evaluation of the evidence available for BPPV-related RD, which is largely variable and based on small studies and the authors' combined clinical experience.
Table 1
| Peripheral risk factor | Mechanism | Impact score |
|---|---|---|
| Previous BPPV episodes (9) | More episodes may indicate persistent otolith degeneration and/or the presence of comorbid conditions that increase the risk of RD* | 2 |
| History of recurrent BPPV (>2 episodes per year) (9) | Suggests ongoing otolith instability and/or the presence of comorbid conditions that increase the risk of RD* | 3 |
| Vitamin D deficiency (9) | The biologically active form of vitamin D is involved in the upregulation of epithelial Ca2+ channel transporters that help maintain low endolymph Ca2+, retain the capacity to dissolve exfoliated otoconia, and prevent abnormal otoconia (1, 22) Decreased serum levels of 25(OH)D were associated with recurrence of BPPV in a Chinese population (52) Vitamin D serum level is lower in canalolithiasis vs. cupulolithiasis of the horizontal canal (53) Epidemiological evidence indicates an association between low vitamin D and diseases that affect the microcirculation (41) | 2 |
| Osteopenia (9, 54) | Calcium metabolism abnormalities could affect otolith regeneration and vestibular compensation (1) | 2 |
| Hearing loss or cochlear damage | Experiencing both hearing loss and RD suggests an inner ear problem, most commonly Ménière's disease* Complications post-cochlear implant may cause dizziness (55) | 1 |
| Female sex (9, 56) | Otoconia may be more prone to degeneration and detachment in women (56, 57) Females are more likely than males to be affected by vitamin D deficiency (53, 58) Fluctuations in estrogen levels can lead to increased vestibular dysfunction (59) | 2 |
| Peripheral risk factors specific to BPPV diagnosis | ||
| BPPV not restricted to one canal (9) | Bilateral BPPV is associated with greater impairment of vestibular function* Multi-canal BPPV involvement is associated with resistance to treatment with standard CRMs (60) | 2 |
| Severe vertigo before CRM | Indicates greater inner ear disturbance* | 2 |
| Multiple maneuvers required for resolution (20) | Suggests more severe dysfunction* | 3 |
| Peripheral risk factors due to systemic and metabolic factors | ||
| Diabetes or metabolic syndrome (20) | Affects microcirculation and may delay otolith recovery (29) | 2 |
| Hypertension (20) | May affect inner ear microcirculation, potentially leading to hypoxia and cochleovestibular degeneration (46) | 3 |
CLEAR risk factor checklist for peripheral causes of BPPV-related RD.
The proposed risk level is based on the combination of published evidence (cited where available) and clinical experience*: 1 (yellow), low risk of developing BPPV-related RD; 2 (amber), medium risk of developing BPPV-related RD; 3 (red), high risk of developing BPPV-related RD.
BPPV, benign paroxysmal positional vertigo; CRM, canalith repositioning maneuver; RD, residual dizziness.
5.2 Central causes of BPPV-related residual dizziness
5.2.1 Incomplete vestibular compensation
The static components of dizziness after vestibular loss (those that occur when the head is kept still) are due to the spontaneous resting activity imbalance between the bilateral vestibular nuclei complexes (61, 62). Complete recovery of vestibular symptoms requires adequate vestibular compensation in the central nervous system (63). Incomplete vestibular compensation may be associated with some of the same factors that increase the risk of BPPV-related RD, such as the duration of BPPV, the patient's emotional state, or the inability of the central nervous system to quickly readjust to a new functional status (64, 65). It has been proposed that the persistence of otoconial debris may alter the tonic discharge from the affected labyrinth, causing a functional asymmetry that induces a new adaptation due to rebalancing of the activity between the vestibular nuclei (4, 66). This new adaptation becomes more established the longer the otoconial debris remains in the endolymph, hence the association between the duration of BPPV and BPPV-related RD. While the brain is able to adapt quickly in the first instance, BPPV-related RD symptoms may occur when the brain takes an extended time to readapt to the old pattern after resolution of BPPV due to successful CRM(s) (66) (Figure 4). Dynamic deficits (those that occur when the head is moving) may be poorly compensated and exhibited over a longer time (67), as they are related to whole-brain activity involved in developing sensory substitution processes to develop new behavioral strategies that mimic lost vestibular functions.
Figure 4
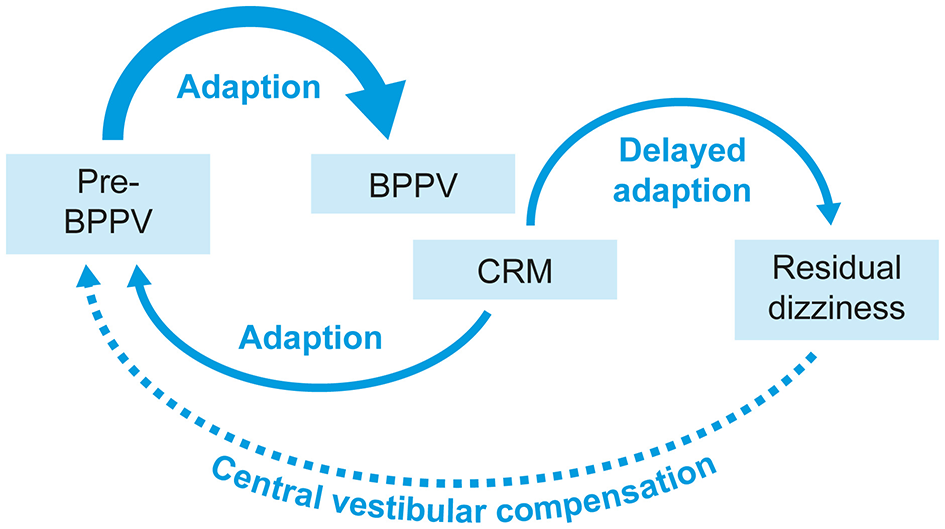
A visual representation of how delayed adaptation might cause BPPV-related RD symptoms. BPPV, benign paroxysmal positional vertigo; CRM, canalith repositioning maneuver; RD, residual dizziness.
5.2.2 Duration of BPPV
The persistence of debris in the semicircular canal after CRM can alter tonic discharge from the affected labyrinth. Such functional asymmetry (Figure 5) can induce a new adaptation through rebalancing of the activity between the vestibular nuclei, and this new condition tends to neutralize the imbalance produced in the peripheral vestibular system (4, 5, 66). A small study reported that patients with a long duration of BPPV were more likely to have moderate-to-severe BPPV-related RD after successful CRM and that the RD impacted mainly the areas of social function and emotional psychology (67). As the rate of undiagnosed BPPV is high at all ages (2), many patients might have BPPV that has already existed for a long time at diagnosis, potentially putting them at a high risk of RD. Although most reports of BPPV-related RD are in adults, long delays in the diagnosis of BPPV are common in children (mean 172.2 days), reflecting a lack of awareness about BPPV among pediatric healthcare providers (68), and also a potential cause of BPPV-related RD, although this does appear to be rare in children.
Figure 5

A visual representation of how altered tonic discharge from the affected labyrinth affects the vestibular nuclei. Adapted from Özgirgin ON, et al. Corrigendum: Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers. Front Neurol. 2024 Jul 29;15:1461600. doi: 10.3389/fneur.2024.1461600 Erratum for: Front Neurol. 2024 May 24;15:1382196. doi: 10.3389/fneur.2024.1382196 (1). H1, H2, and H3 are the histamine receptors in the vestibular nuclei.
5.2.3 Comorbid vestibular conditions
The risk of BPPV-related RD in secondary BPPV is 1.88 times that of idiopathic BPPV, with Ménière's disease and vestibular neuritis being two of the most common causes of secondary BPPV, along with head trauma (9). This is supported by a retrospective analysis of data from the US Vestibular Disorders Association Registry reporting that 83% of adults with BPPV had received an additional vestibular diagnosis or may have had atypical BPPV (69). Patients with BPPV and other concomitant vestibular pathologies have been reported to have a proportionally higher persistence of symptoms after CRMs than patients with pure BPPV (70).
5.2.4 Anxiety and/or depression
The high comorbidity between balance disorders and anxiety is a complex, two-way interaction whereby patients with psychological symptoms commonly report vestibular symptoms, such as dizziness, and conversely, patients with vestibular dysfunction report psychological symptoms (71, 72). Overlapping neural circuits between anxiety and the balance control system may provoke increased anxiety levels in patients after BPPV, and patients who develop higher anxiety have incomplete central adaptation (72). There is evidence that dopamine plays an important role in anxiety modulation in different parts of the brain, and disruption of dopaminergic efferent pathways could be associated with vestibular dysfunction (73, 74). Dopamine has been shown to improve vestibular compensation in aged rats, likely via a mechanism involving vestibular nuclei (74). Varying expression of dopamine has been reported in the subepithelial stroma of the saccule, along with intense expression of the H3 receptor in epithelial lining cells of the saccule (75); H3 agonism plays a role in reducing dopaminergic signaling (76).
Based on the evaluation of the evidence available and combined clinical experience, the impact of the central risk factors is summarized in Table 2.
Table 2
| Central risk factor | Mechanism | Impact score |
|---|---|---|
| Age >65 years (9, 19, 20, 28) | Slower central compensation (34) | 2 |
| History of vestibular migraine (1) | Central vestibular dysfunction delays compensation (77, 78) | 3 |
| Cognitive impairment (79, 80) | Slows adaptation to new vestibular input (81), especially in the elderly | 2 |
| Female sex (9, 56) | Fluctuations in estrogen levels can lead to impaired compensation after BPPV treatment (82) Changes to hormone receptor stimulation may be central to the pathogenesis of BPPV (57, 59, 83) |
2 |
| Physical inactivity (66) | Reduces vestibular compensation efficiency (84) | 1 |
| Longer duration of BPPV (9, 85) Symptoms >4 weeks before CRM* |
Prolonged compensation period (64, 66) | 2 |
| Severe oscillopsia during a BPPV episode | Indicates prolonged adaptation difficulty, especially when combined with VM comorbidity* | 3 |
| Residual mild dizziness post-maneuver (9) | Suggests incomplete adaptation (4, 64) | 3 |
| Persistent non-typical BPPV nystagmus post-maneuver | Could indicate residual debris or incomplete adaptation* | 1 |
| Anxiety or depression (9, 20, 80) | Increases hypervigilance, prolongs symptom perception (86, 87) Anxiety disorders are linked to chronic dizziness conditions, such as persistent postural-perceptual dizziness (88) | 2 |
| Chronic stress or PTSD | Prolongs hypervigilance and dizziness perception* | 2 |
CLEAR risk factor checklist for central causes of BPPV-related RD.
The proposed risk level is based on the combination of published evidence (cited where available) and clinical experience*: 1 (yellow), low risk of developing BPPV-related RD; 2 (amber), medium risk of developing BPPV-related RD; 3 (red), high risk of developing BPPV-related RD.
BPPV, benign paroxysmal positional vertigo; CRM, canalith repositioning maneuver; PTSD, post-traumatic stress disorder; RD, residual dizziness; VM, vestibular migraine.
6 Important differential diagnoses
If a patient presents with RD after successful CRM for BPPV or after suspected spontaneous resolution of BPPV, several key differential diagnoses should be considered in addition to BPPV-related RD. These include vestibular migraine and Ménière's disease, as well as other central or peripheral causes of dizziness. The diagnostic criteria for vestibular migraine are ≥5 episodes of vestibular symptoms of moderate-to-severe intensity, lasting between 5 min and 72 h; at least 50% of these episodes accompanied by ≥1 migraine symptom(s), including headache (with ≥2 features of unilateral, throbbing, moderate/severe intensity, aggravated by routine physical activity), photophobia and phonophobia, or visual aura; current or previous history of migraine with or without aura; and not better accounted for by another diagnosis (89). Several vestibular symptoms may be reported in vestibular migraine, including spontaneous and triggered vertigo/dizziness (90). A confirmed diagnosis of Ménière's disease is assumed with ≥2 episodes of spontaneous vertigo, each lasting 20 min to 12 h with fluctuating aural symptoms (hearing changes, tinnitus, and aural fullness) before, during, or after an episode of vertigo; audiometrically documented low-to-medium frequency sensorineural hearing loss in one ear on at least one occasion, starting before, during, or after an episode of vertigo; and not better explained by another vestibular diagnosis (91). Key differential diagnoses of central origin include stroke and other neurological findings such as a tumor or vertebrobasilar insufficiency. Key differential diagnoses of peripheral origin include anxiety, concomitant medications, cardiometabolic conditions, and orthostatic hypertension.
7 Introducing the concept of type 1 and type 2 BPPV-related RD
Based on the authors' combined clinical experience of over 90 years in treating thousands of patients with vestibular disorders, we propose that there are two types of BPPV-related RD, differentiated by their initial presentation (Table 3). Type 1 BPPV-related RD is defined as an initial presentation with a typical BPPV nystagmus that is resolved with ≥1 CRM, with RD symptoms reported at the follow-up appointment (at 1–2 weeks post-CRM). However, we recognize that some patients present with dizziness symptoms without positional nystagmus but with a clear history of BPPV, which was not examined or diagnosed and has apparently resolved spontaneously, and we propose that this type of RD can be defined as type 2 BPPV-related RD. Current evidence indicates that BPPV may resolve spontaneously without intervention in approximately 35%−50% of patients (92). The Consensus Document of the Committee for the Classification of Vestibular Disorders of the Bárány Society designates this presentation as “probable BPPVo, spontaneously resolved” (pBPPVsr). This entity is defined as recurrent, brief (< 1 min) episodes of positional vertigo or dizziness precipitated by lying down or turning over in the supine position, in the absence of observable nystagmus or vertigo during positional maneuvers, and not attributable to any alternative disorder (93). With careful questioning to obtain a detailed clinical and symptom history, we can determine whether there was indeed a BPPV that spontaneously resolved. As has been previously reported, patients' descriptions of symptoms are not reliable (94), and they may find it difficult to differentiate between vertigo and dizziness. However, patient reports of timing and triggers have been found to be reliable (94). An experienced neurologist/ear, nose, and throat (ENT) specialist can identify cases of spontaneously resolved BPPV from the characteristic timing and triggers associated with BPPV and, after confirming the absence of suggestive nystagmus and excluding other potential causes, can then reliably recognize BPPV-related RD (Table 4).
Table 3
| Type 1 BPPV-related RD | Type 2 BPPV-related RD |
|---|---|
| • Initial presentation: vertigo with a typical BPPV nystagmus • Treatment: ≥1 CRM to resolve nystagmus • At follow-up: RD symptoms |
• Initial presentation: dizziness symptoms but absence of a typical BPPV nystagmus • Clinical history: symptoms that allow retrospective diagnosis of BPPV with a high level of certainty by an experienced neurologist/ENT/otologist |
A new concept for the identification of BPPV-related RD based on initial presentation.
BPPV, benign paroxysmal positional vertigo; CRM, canalith repositioning maneuver; ENT, ear, nose, and throat specialist; RD, residual dizziness.
Table 4
| Feature | Features that are suggestive of BPPV |
|---|---|
| Onset | Sudden or after a provocative movement, e.g., getting up too fast, after a head bump, viral illness, or prolonged bed rest |
| Time of onset | There is no minimum/maximum timing between the event and the presentation |
| Trigger | Vertigo triggered positionally, e.g., rolling over in bed, lying down, sitting up, bending forward, or looking up (“top shelf vertigo”) |
| Type of dizziness | Classic spinning sensation (true vertigo), often described as “the room spinning” |
| Duration of attacks | Short-lived (typically < 30–60 s), with abrupt start and stop |
| Latency | A few seconds delay (1–5 s) between head movement and symptom onset |
| Associated symptoms | Nausea may occur, but no hearing loss, tinnitus, diplopia, or limb symptoms |
| Frequency | Episodes often cluster, then spontaneously remit; recurrences are common |
| Pattern of recovery | Vertigo subsides when the patient avoids provocative movements |
Key clinical features of BPPV that have resolved spontaneously.
BPPV, benign paroxysmal positional vertigo.
While the management options are the same for both type 1 and type 2 BPPV-related RD, it is an important distinction to ensure that we are capturing all cases of dizziness that are related to BPPV.
8 Follow-up strategies for BPPV-related RD
Once identified as type 1 or type 2 BPPV-related RD, there are several potential follow-up strategies. The first is the avoidance of pharmacological agents that act as vestibular suppressants and interfere with central compensation (96). It may seem attractive to use medication to suppress dizziness and other symptoms, but clinicians should be aware that they may interfere with central compensation (97) and make the symptoms worse. Clinicians should consider the use of techniques and/or medications that facilitate central compensation. Evidence suggests that patients with high anxiety benefit less from vestibular rehabilitation (VR) (97) and have a greater impact on their quality of life than those with lower anxiety (81). Identifying such patients could be important when considering management options. Although the DHI and visual analog scale (VAS) are the most commonly used measures to quantify RD, neither of these has been validated specifically for BPPV or RD. The DHI is a self-assessment inventory of 25 items covering the functional, emotional, and physical impacts on daily life, whereas the VAS has the advantage of being able to distinguish dizziness from vertigo, with reliable results in evaluating RD (1).
For BPPV, there is evidence that CRMs are more effective in the short term than exercise-based vestibular rehabilitation (VR), although a combination of the two is effective for long-term functional recovery (98). However, there is insufficient evidence and no consensus on the most effective form of VR (99, 100), likely due to differences in endpoints, use of pharmacological options, and patients' ability to complete VR as instructed. Although some studies have shown that VR can effectively relieve or reduce residual symptoms in patients with BPPV (101, 102), others have shown no benefit (103).
Important comorbidities should also be identified and treated appropriately to reduce the risk of recurrence (Table 5).
Table 5
| Intervention | Mechanism / Rationale | Clinical Notes / Evidence |
|---|---|---|
| A. Avoid vestibular suppressants | ||
| Pharmacotherapy • Avoid benzodiazepines (e.g., diazepam, clonazepam) |
Inhibitory effect on the electrical activity of the vestibular nuclei (104) and central compensation (95) | Benzodiazepines (BZDs) may interfere with central compensation and are not recommended for routine use in patients with BPPV • Current guidelines recommend against the routine treatment of patients with BPPV with vestibular suppressant medications such as BZDs (95) • BZDs, such as diazepam and clonazepam, have anxiolytic, sedative, muscle-relaxant, and anticonvulsant properties (95) • In prolonged dizziness, BZDs can reduce the subjective sensation of spinning but can also interfere with central compensation (95, 105) • Although BZDs may provide initial relief for acute dizziness symptoms, routine use is not recommended due to the risk of dependence, cognitive impairment, falls, and physical injury (105, 106) • In patients with BPPV, BZDs may have no effect on symptom resolution at the point of longest follow-up (107) • In the occasional patient who cannot tolerate a CRM, is exceptionally anxious about undergoing a CRM, or has RD after a CRM, it may be appropriate to treat for 2–3 days with a vestibular suppressant (107) |
| Pharmacotherapy • Avoid antihistamines (e.g., diphenhydramine, dimenhydrinate, cinnarizine, meclizine, promethazine) |
Interferes with central compensation after vestibular injury (95) | Antihistamines may interfere with central compensation and are not recommended for routine use in patients with BPPV • Current guidelines recommend against the routine treatment of patients with BPPV with vestibular suppressant medications such as antihistamines (95) • Antihistamines appear to have a suppressive effect on the central emetic center to relieve the nausea and vomiting associated with motion sickness, for example, meclizine, diphenhydramine, and promethazine (a phenothiazine with antihistamine properties), but interfere with central compensation (95, 105) • Vestibular suppressant antihistamines have the potential for significant harm, such as drowsiness, cognitive deficits, and interference with driving or operating machinery (95) • Vestibular suppressants such as antihistamines are not routinely recommended for treatment of BPPV, other than for the short-term ( ≤ 3 days) management of autonomic symptoms, such as nausea or vomiting, in a severely symptomatic patient (95, 106, 107); in patients with BPPV, pheniramine, cinnarizine, and flunarizine may have no effect on symptom resolution at the point of longest follow up (107) |
| Pharmacotherapy • Avoid phenothiazines (i.e., prochlorperazine) |
Suppresses central vestibular nuclei and pathways (108) | Current guidelines recommend against the routine treatment of patients with BPPV with vestibular suppressants (95) • Vestibular suppressants have the potential for significant harm, such as drowsiness, cognitive deficits, and interference with driving or operating machinery (95) • Vestibular suppressants are not routinely recommended for treatment of BPPV, other than for the short-term ( ≤ 3 days) management of autonomic symptoms, such as nausea or vomiting, in a severely symptomatic patient (95, 106) |
| B. Facilitate central vestibular compensation | ||
| Vestibular rehabilitation therapy (VRT; e.g., customized balance, gaze, and habituation exercises) | The goal of VRT is to enhance vestibular compensation and neuroplasticity by focusing on gaze stabilization, postural control, and sensory integration (109) to leverage multisensory input (visual, proprioceptive, and vestibular), recalibrate postural control, and reduce dizziness (110) | VRT improves RD by promoting central compensation • VRT has been shown to significantly reduce the severity and duration of BPPV-related RD, especially when individualized to patient deficits (95) • Individualized programmes can reduce RD severity (110) • Treatment typically lasts 4–8 weeks, and while home programmes exist, clinician guidance is preferred to optimize outcomes (95) |
| Encourage physical activity / mobility | • May enhance neuroplasticity phenomena, making the vestibular system more receptive to natural compensatory mechanisms (111) • Physical activity supports vestibular compensation through adaptive plasticity, reduces anxiety, and prevents deconditioning (112) |
Daily activity supports vestibular recovery and may reduce RD duration • Daily activity supports vestibular recovery (111) and may reduce RD duration, regardless of age (66) • Regardless of age, the resumption of regular daily physical activities is associated with a lack of RD after BPPV (66) • Unless contraindicated by fall risk or severe instability, patients should be encouraged to maintain daily physical activity throughout the recovery phase |
| Pharmacotherapy • Agents that facilitate central vestibular compensation (e.g., betahistine) |
• Betahistine may promote and facilitate central vestibular compensation, enhancing histamine synthesis within tuberomammillary nuclei of the posterior hypothalamus and histamine release within vestibular nuclei through antagonism of H3 autoreceptors, and increasing alertness regulation through cerebral H1 receptors (96, 113) • Additionally, betahistine may increase vestibulocochlear blood flow, supporting inner ear perfusion (113) |
Betahistine 48 mg/day for ~3 months may improve RD by promoting central compensation • There is robust strong evidence from animal studies to demonstrate the effect of betahistine on central compensation (1, 96) • In humans, the bioavailability of oral betahistine is reduced by first-pass metabolism in some patients (96). Studies are ongoing to identify strategies to overcome the first-pass effect and to identify optimal doses to support central compensation (96, 114–117) • As the administration of betahistine is dose-dependent and time-dependent, selecting the appropriate dose and duration to achieve desirable effects is important (117) • Treatment with betahistine 48 mg/d for up to 90 days was also useful to manage the nausea and vomiting that may occur during CRMs and in treating dizziness that may continue after CRM (103). Betahistine 48 mg/d in addition to CRM in patients with PV may improve symptoms (118), normalize postural stability more rapidly (119) and speed recovery rate (120) compared with CRM alone • Combining betahistine with CRM could improve the outcomes of BPPV in the long term, according to two meta-analyses (121, 122) |
| C. Manage comorbidities | ||
| Vitamin D supplementation (1,000–2,000 IU/day) | Vitamin D plays a critical role in calcium regulation and otoconial integrity, which are essential for vestibular function. Deficiency may destabilize otoconia and impair vestibular compensation, especially in patients with comorbid osteoporosis, diabetes, or hypertension (22, 123). Low vitamin D levels are also associated with microvascular dysfunction that could compromise inner ear perfusion (49, 50) | Vitamin D may help stabilize otoconia and reduce recurrence of BPPV • Serum concentrations of 25(OH)D of ≥20 ng/ml (≥50 nmol/L) are generally considered adequate for bone and overall health in healthy individuals (124) • Vitamin D supplementation, in the absence of calcium, may be beneficial for patients prone to recurrent BPPV episodes, particularly when serum vitamin D levels are suboptimal (125, 126) |
| Address systemic and psychiatric comorbidities (e.g., hypertension, diabetes mellitus, anxiety) | • Hyperglycaemia and endothelial dysfunction impair nitric oxide-mediated vasodilation, reducing blood flow to inner ear structures (45) • Uncontrolled hypertension can lead to inner ear haemorrhage or ischaemia that can compromise cochleovestibular function and/or affect central functions when areas of the brain involved in the vestibular network are involved (46) • Overlapping neural circuits between anxiety and the balance control system may provoke increased anxiety levels in patients after BPPV. Anxiety is associated with impaired central through disruption of vestibular-cortical integration, altering neuroplastic adaptation (5, 62, 72) |
Optimizing factors that can impede vestibular compensation, such as cardiometabolic health and psychological stress, is an essential component of BPPV-related RD management • Identify and optimize management of hypertension and diabetes mellitus • Manage anxiety through education initially, with referral to counseling/psychiatrist as appropriate* • Screening and referral for anxiety-related vestibular symptoms should be part of standard care, particularly in older adults, as recommended by the World Falls Guidelines (127) |
Potential management options for BPPV-related RD.
BPPV, benign paroxysmal positional vertigo; BZD, benzodiazepine; CRM, canalith repositioning maneuver; RD, residual dizziness; VRT, vestibular rehabilitation therapy.
*Based on clinical experience.
It should be noted that while there is one study reporting the benefits of Danhong injection, a traditional Chinese medicine, in reducing BPPV-related RD (128), this has been omitted from Table 5 on the basis of insufficient evidence.
EGb 761, a special extract from dried leaves of Ginkgo biloba, has been approved for the treatment of vertigo of vascular and involutional origin in several countries (129). However, a recent meta-analysis of 25 randomized controlled studies with >1,200 patients concluded that the addition of Ginkgo biloba only provided clinical efficacy in patients with vertebrobasilar insufficiency, cervical vertigo, and non-disease-specific vertigo, but not in BPPV or Meniere's disease (130); for this reason, Ginkgo biloba has also not been included as an evidence-based management consideration.
9 The future of BPPV-related RD identification and management
Improved identification and management of BPPV-related RD could help prevent morbidity and loss of QOL. Especially in older patients, it is important to manage dizziness symptoms to avoid falls and diminished QOL, to identify any other vestibular or cardiovascular conditions, and to effectively differentiate BPPV-related RD from other sinister conditions that affect balance. In younger patients, the impact of BPPV-related RD is not well-understood; however, it might be expected to exert a substantial impact on work and activities of daily living. As the world population ages, BPPV-related RD is likely to become an increasingly problematic condition; increasing age causes age-associated degeneration of otoconia (2, 34) and an increased likelihood of vestibular and/or vascular conditions (72, 131).
Objective measures to assess utricular function in the absence of a BPPV-specific nystagmus have not been established in the context of BPPV-related RD, and while the Subjective Visual Vertical test and oVEMPs may identify utricular dysfunction, they have their limitations (1). Studies suggest that the video ocular counter-roll is simple to apply and has clinical value in identifying the stage of statolith function, loss, and recovery at the bedside; it consists of a simple maneuver during which the head and torso are tilted laterally en bloc with measurement of the torsional vestibulo-ocular reflex (132–134). The unilateral centrifugation test also measures utricular sensitivity and the preponderance of the right or left utricle. During this test, subjects are rotated about a vertical axis to align one utricle with the axis of rotation and then subjected only to gravitational forces to induce ocular counterrolling, which is measured online using three-dimensional video-oculography (135). While positive subjective visual vertical, oVEMP, unilateral centrifugation, and/or video ocular counter-roll results for utricular dysfunction are highly suggestive of BPPV-related RD, there is insufficient evidence to consider them conclusive of BPPV-related RD, and all require specialist equipment that may not be available for all patients.
Based on published evidence and our combined clinical experience, we have developed the Clinician-Led Evaluation for Assessment of Residual dizziness (CLEAR) tool, a BPPV-related RD algorithm to help specialist clinicians identify and manage patients (Figure 6; click on the QR code in Figure 7 to access). This algorithm is developed according to our understanding of the underlying causes and the applicability of potential treatment options. The tool is based on the data in Tables 1−4 and is available for use by specialists in interactive form via the QR code provided or https://clear-dizziness.org. As described earlier, Tables 1, 2 provide a list of the potential risk factors and their impact scores (mild, moderate, or severe) based on the combination of published evidence and the authors' clinical experience, which may assist your clinical decision-making by highlighting patients with a greater risk of BPPV-related RD. The CLEAR tool has been developed as a click-through algorithm (Figure 6) to help recognize patients with RD, with the option to download a summary (in PDF format) of the recommendations for follow-up strategies for each patient. Future research is needed to validate independent risk factors for BPPV-related RD, and we encourage the use of the algorithm in any such studies.
Figure 6

Overview of the CLEAR algorithm for use by specialist clinicians to support in the recognition of risk factors and follow-up strategies for BPPV-related RD. BPPV, benign paroxysmal positional vertigo; ENT, ear, nose, and throat specialist; CRM, canalith repositioning maneuver; oVEMP, ocular vestibular evoked myogenic potential; RD, residual dizziness; SVV, subjective visual vertical.
Figure 7

The Clinician-Led Evaluation for Assessment of Residual dizziness (CLEAR) algorithm.
Ultimately, our aim is to help all healthcare professionals who work with patients with BPPV to promptly recognize BPPV-related RD, follow up appropriately to resolve symptoms as quickly as possible, and thereby improve patient outcomes.
Statements
Author contributions
HK: Conceptualization, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. LM: Conceptualization, Investigation, Methodology, Resources, Visualization, Writing – original draft, Writing – review & editing. NÖ: Conceptualization, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Abbott Products Operations AG, Allschwill, Switzerland. The funder had the following involvement in the study: technical and editorial support, provided by Karen Smith, Highfield Communications Consultancy, UK, in accordance with GPP2022 and for payment of the Open Access Fees and CLEAR.org website hosting.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
Özgirgin ON Kingma H Manzari L Lacour M . Residual dizziness after BPPV management: exploring pathophysiology and treatment beyond canalith repositioning maneuvers. Front Neurol. (2024) 15:1382196. doi: 10.3389/fneur.2024.1382196
2.
Parham K . Benign paroxysmal positional vertigo: an integrated perspective. Adv Otolaryngol. (2014) 2014:792635. doi: 10.1155/2014/792635
3.
Hawke LJ Barr CJ McLoughlin JV . The frequency and impact of undiagnosed benign paroxysmal positional vertigo in outpatients with high falls risk. Age Ageing. (2021) 50:2025–30. doi: 10.1093/ageing/afab122
4.
Seok JI Lee HM Yoo JH Lee DK . Residual dizziness after successful repositioning treatment in patients with benign paroxysmal positional vertigo. J Clin Neurol. (2008) 4:107–10. doi: 10.3988/jcn.2008.4.3.107
5.
Lee JY Lee IB Kim MB . Correlation between residual dizziness and modified clinical test of sensory integration and balance in patients with benign paroxysmal positional vertigo. Res Vestib Sci. (2021) 20:93–100. doi: 10.21790/rvs.2021.20.3.93
6.
Kim HA Lee H . Autonomic dysfunction as a possible cause of residual dizziness after successful treatment in benign paroxysmal positional vertigo. Clin Neurophysiol. (2014) 125:608–14. doi: 10.1016/j.clinph.2013.08.008
7.
Biswas A Dutta N . Post-BPPV syndrome: our experience in a specialized neurotology clinic in Kolkata. Ann Otol Neurotol. (2019) 02:01–9. doi: 10.1055/s-0039-1695666
8.
Zhang H Zhu M . Mechanical rotational chair-assisted multiple canalith repositioning procedures for benign paroxysmal positional vertigo: enhanced vertigo relief, comparable adverse effects, and decreased incidence of residual dizziness. Front Neurol. (2023) 14:1226138. doi: 10.3389/fneur.2023.1226138
9.
Ke Y Ma X Jing Y Diao T Yu L . Risk factors for residual dizziness in patients with benign paroxysmal positional vertigo after successful repositioning: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. (2022) 279:3237–56. doi: 10.1007/s00405-022-07288-9
10.
Rasmussen MB Sørensen R Hougaard DD . Positional nystagmus is observed in the vast majority of healthy individuals. Eur Arch Otorhinolaryngol. (2024) 281:3499–507. doi: 10.1007/s00405-024-08453-y
11.
Li Y Smith RM Whitney SL Seemungal BM Ellmers TJ . Association between dizziness and future falls and fall-related injuries in older adults: a systematic review and meta-analysis. Age Ageing. (2024) 53:afae177. doi: 10.1093/ageing/afae177
12.
Ciorba A Bianchini C Scanelli G Pala M Zurlo A Aimoni C . The impact of dizziness on quality-of-life in the elderly. Eur Arch Otorhinolaryngol. (2017) 274:1245–50. doi: 10.1007/s00405-016-4222-z
13.
Agrawal Y Carey JP Della Santina CC Schubert MC Minor LB . Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001-2004. Arch Intern Med. (2009) 169:938–44. doi: 10.1001/archinternmed.2009.66
14.
von Brevern M Radtke A Lezius F Feldmann M Ziese T Lempert T et al . Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry. (2007) 78:710–5. doi: 10.1136/jnnp.2006.100420
15.
Gedik-Soyuyuce O Gence-Gumus Z Ozdilek A Ada M Korkut N . Vestibular disorders in children: a retrospective analysis of vestibular function test findings. Int J Pediatr Otorhinolaryngol. (2021) 146:110751. doi: 10.1016/j.ijporl.2021.110751
16.
Brodsky JR Lipson S Wilber J Zhou G . Benign paroxysmal positional vertigo (BPPV) in children and adolescents: clinical features and response to therapy in 110 pediatric patients. Otol Neurotol. (2018) 39:344–50. doi: 10.1097/MAO.0000000000001673
17.
Holstein BE Damsgaard MT Pedersen TP Rasmussen M Toftager M Madsen KR . Recurrent dizziness among adolescents in Denmark: trends 1991-2022 and associations with sociodemographic factors, health, and health behaviours. Eur J Pediatr. (2025) 184:247. doi: 10.1007/s00431-025-06076-x
18.
Zhang JL Hui L . [Study on the characteristics of benign paroxysmal positional vertigo and the influencing factors of short-term residual symptoms after reposition treatment]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2018) 32:1016–9. doi: 10.13201/j.issn.1001-1781.2018.13.014
19.
Fu W He F Bai Y An X Shi Y Han J et al . Risk factors of residual dizziness after successful treatment for benign paroxysmal positional vertigo in middle-aged and older adults. Front Neurol. (2022) 13:850088. doi: 10.3389/fneur.2022.850088
20.
Zhou C Ma C Li Y Zhou X Shui L Han C . Risk factors and a nomogram model for residual symptoms of cured benign paroxysmal positional vertigo. J Int Adv Otol. (2023) 19:523–8. doi: 10.5152/iao.2023.231127
21.
Zhou F Fu M Zhang N Xu Y Ge Y . [Investigation of the relationship between chronic diseases and residual symptoms of benign paroxysmal positional vertigo]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2015) 29:1627–9. doi: 10.13201/j.issn.1001-1781.2015.18.010
22.
Wu J Jiang CY Bai YX Xu Q Sun XH Pan H et al . Effect of the serum 25-hydroxyvitamin D level on risk for short-term residual dizziness after successful repositioning in benign paroxysmal positional vertigo stratified by sex and onset age. Front Neurol. (2023) 14:1144958. doi: 10.3389/fneur.2023.1144958
23.
Niu X Han P Duan M Chen Z Hu J Chen Y et al . Bilateral dysfunction of otolith pathway in patients with unilateral idiopathic BPPV detected by ACS-VEMPs. Front Neurol. (2022) 13:921133. doi: 10.3389/fneur.2022.921133
24.
Rosa MS Campagnoli M Masnaghetti D Taranto F Pisani G Garzaro M et al . Clinical and prognostic implications of cervical and ocular vestibular evoked myogenic potentials (cVEMP and oVEMP) in benign paroxysmal positional vertigo (BPPV): a prospective study. Audiol Res. (2023) 13:700–9. doi: 10.3390/audiolres13050061
25.
Jiang CY Wu J Shu L Sun XH Pan H Xu Q et al . Clinical and cVEMP evaluation predict short-term residual dizziness after successful repositioning in benign paroxysmal positional vertigo. Front Med. (2022) 9:881307. doi: 10.3389/fmed.2022.881307
26.
Oh KH Suh KD Lee YH Lee SY Chang MY Mun SK . Clinical utility of cervical vestibular-evoked myogenic potentials in predicting residual dizziness after benign paroxysmal positional vertigo. Clin Neurophysiol. (2019) 130:95–100. doi: 10.1016/j.clinph.2018.11.005
27.
Manzari L Tramontano M . Otolithic and canal functions assessment during the acute phase of benign paroxysmal positional vertigo. Eur Arch Otorhinolaryngol. (2024) 281:2253–7. doi: 10.1007/s00405-023-08312-2
28.
Dispenza F Mazzucco W Mazzola S Martines F . Observational study on risk factors determining residual dizziness after successful benign paroxysmal positional vertigo treatment: the role of subclinical BPPV. Acta Otorhinolaryngol Ital. (2019) 39:347–52. doi: 10.14639/0392-100X-2247
29.
D'Silva LJ Staecker H Lin J Sykes KJ Phadnis MA McMahon TM et al . Retrospective data suggests that the higher prevalence of benign paroxysmal positional vertigo in individuals with type 2 diabetes is mediated by hypertension. J Vestib Res. (2016) 25:233–9. doi: 10.3233/VES-150563
30.
Shah A Kanaya AM . Diabetes and associated complications in the South Asian population. Curr Cardiol Rep. (2014) 16:476. doi: 10.1007/s11886-014-0476-5
31.
Chen J Zhang S Cui K Liu C . Risk factors for benign paroxysmal positional vertigo recurrence: a systematic review and meta-analysis. J Neurol. (2021) 268:4117–27. doi: 10.1007/s00415-020-10175-0
32.
De Stefano A Dispenza F Suarez H Perez-Fernandez N Manrique-Huarte R Ban JH et al . A multicenter observational study on the role of comorbidities in the recurrent episodes of benign paroxysmal positional vertigo. Auris Nasus Larynx. (2014) 41:31–6. doi: 10.1016/j.anl.2013.07.007
33.
Jiang X He L Gai Y Jia C Li W Hu S et al . Risk factors for residual dizziness in patients successfully treated for unilateral benign posterior semicircular canal paroxysmal positional vertigo. J Int Med Res. (2020) 48:300060520973093. doi: 10.1177/0300060520973093
34.
Zalewski CK . Aging of the human vestibular system. Semin Hear. (2015) 36:175–96. doi: 10.1055/s-0035-1555120
35.
Vibert D Sans A Kompis M Travo C Muhlbauer RC Tschudi I et al . Ultrastructural changes in otoconia of osteoporotic rats. Audiol Neurootol. (2008) 13:293–301. doi: 10.1159/000124277
36.
Vibert D Kompis M Häusler R . Benign paroxysmal positional vertigo in older women may be related to osteoporosis and osteopenia. Ann Otol Rhinol Laryngol. (2003) 112:885–9. doi: 10.1177/000348940311201010
37.
Zach H Retter D Schmoeger M Rommer P Willinger U Schwarz FK et al . Seasonality of benign paroxysmal positional vertigo: a retrospective study from Central Europe. Wien Klin Wochenschr. (2024) 136:25–31. doi: 10.1007/s00508-023-02237-w
38.
Meghji S Murphy D Nunney I Phillips JS . The seasonal variation of benign paroxysmal positional vertigo. Otol Neurotol. (2017) 38:1315–8. doi: 10.1097/MAO.0000000000001534
39.
Bhattoa HP Bettembuk P Ganacharya S Balogh A . Prevalence and seasonal variation of hypovitaminosis D and its relationship to bone metabolism in community dwelling postmenopausal Hungarian women. Osteoporos Int. (2004) 15:447–51. doi: 10.1007/s00198-003-1566-1
40.
Yetiser S . Review of the pathology underlying benign paroxysmal positional vertigo. J Int Med Res. (2020) 48:300060519892370. doi: 10.1177/0300060519892370
41.
Meehan M Penckofer S . The role of vitamin D in the aging adult. J Aging Gerontol. (2014) 2:60–71. doi: 10.12974/2309-6128.2014.02.02.1
42.
Nahm H Han K Shin JE Kim CH . Benign paroxysmal positional vertigo in the elderly: a single-center experience. Otol Neurotol. (2019) 40:1359–62. doi: 10.1097/MAO.0000000000002385
43.
Zucca G Valli S Valli P Perin P Mira E . Why do benign paroxysmal positional vertigo episodes recover spontaneously?J Vestib Res. (1998) 8:325–9. doi: 10.3233/VES-1998-8404
44.
Li X Li R Li M Zhang Y Guo K Wu L . Effects of diabetes on hearing and cochlear structures. J Otol. (2013) 8:82–7. doi: 10.1016/S1672-2930(13)50017-1
45.
Zhu CT Zhao XQ Ju Y Wang Y Chen MM Cui Y . Clinical characteristics and risk factors for the recurrence of benign paroxysmal positional vertigo. Front Neurol. (2019) 10:1190. doi: 10.3389/fneur.2019.01190
46.
Osuji AE . The Interaction of hypertension for vertigo in audiovestibular medicine clinic. Research in Vestibular Science. (2022) 21:29–39. doi: 10.21790/rvs.2022.21.2.29
47.
Fu W He F Bai Y Wang Y Wei D Shi Y et al . Assessment of residual dizziness after successful canalith repositioning maneuvre in benign paroxysmal positional vertigo patients: a questionnaire-based study. Eur Arch Otorhinolaryngol. (2023) 280:137–41. doi: 10.1007/s00405-022-07474-9
48.
Zang J Jiang X Feng S Zhang H . The influence of cerebral small vessel diseases on the efficacy of repositioning therapy and prognosis of benign paroxysmal positional vertigo. Int J Med Sci. (2022) 19:1227–34. doi: 10.7150/ijms.73080
49.
Vaidya A Forman JP . Vitamin D and hypertension: current evidence and future directions. Hypertension. (2010) 56:774–9. doi: 10.1161/HYPERTENSIONAHA.109.140160
50.
Mohd Ghozali N Giribabu N Salleh N . Mechanisms linking vitamin D deficiency to impaired metabolism: an overview. Int J Endocrinol. (2022) 2022:6453882. doi: 10.1155/2022/6453882
51.
Ismail NM Kabil SE Abdel-Hamid EF . Otolithic functions in patients with residual dizziness after successful repositioning manoeuvres for unilateral posterior canal BPPV. J Int Med Res. (2024) 52:3000605241249095. doi: 10.1177/03000605241249095
52.
Ding J Liu L Kong WK Chen XB Liu X . Serum levels of 25-hydroxy vitamin D correlate with idiopathic benign paroxysmal positional vertigo. Biosci Rep. (2019) 39:BSR20190142. doi: 10.1042/BSR20190142
53.
Nakada T Sugiura S Uchida Y Suzuki H Teranishi M Sone M . Difference in serum levels of vitamin D between canalolithiasis and cupulolithiasis of the horizontal semicircular canal in benign paroxysmal positional vertigo. Front Neurol. (2019) 10:176. doi: 10.3389/fneur.2019.00176
54.
Suh KD Oh SR Chae H Lee SY Chang M Mun SK . Can osteopenia induce residual dizziness after treatment of benign paroxysmal positional vertigo?Otol Neurotol. (2020) 41:e603–6. doi: 10.1097/MAO.0000000000002586
55.
Weinmann C Baumann U Leinung M Stöver T Helbig S . Vertigo associated with cochlear implant surgery: correlation with vertigo diagnostic result, electrode carrier, and insertion angle. Front Neurol. (2021) 12:663386. doi: 10.3389/fneur.2021.663386
56.
Smith PF Agrawal Y Darlington CL . Sexual dimorphism in vestibular function and dysfunction. J Neurophysiol. (2019) 121:2379–91. doi: 10.1152/jn.00074.2019
57.
Yang L Xu Y Zhang Y Vijayakumar S Jones SM Lundberg YYW . Mechanism underlying the effects of estrogen deficiency on otoconia. J Assoc Res Otolaryngol. (2018) 19:353–62. doi: 10.1007/s10162-018-0666-8
58.
Mithal A Wahl DA Bonjour JP Burckhardt P Dawson-Hughes B Eisman JA et al . Global vitamin D status and determinants of hypovitaminosis D. Osteoporos Int. (2009) 20:1807–20. doi: 10.1007/s00198-009-0954-6
59.
Mucci V Hamid M Jacquemyn Y Browne CJ . Influence of sex hormones on vestibular disorders. Curr Opin Neurol. (2022) 35:135–41. doi: 10.1097/WCO.0000000000001019
60.
Alfarghal M Singh NK Algarni MA Jagadish N Raveendran RK . Treatment efficacy of repositioning maneuvers in multiple canal benign paroxysmal positional vertigo: a systematic review and meta-analysis. Front Neurol. (2023) 14:1288150. doi: 10.3389/fneur.2023.1288150
61.
Tighilet B Trottier S Mourre C Lacour M . Changes in the histaminergic system during vestibular compensation in the cat. J Physiol. (2006) 573(Pt 3):723–39. doi: 10.1113/jphysiol.2006.107805
62.
Lacour M Helmchen C Vidal PP . Vestibular compensation: the neuro-otologist's best friend. J Neurol. (2016) 263(Suppl 1):S54–64. doi: 10.1007/s00415-015-7903-4
63.
Chen Z Cai Y Xiao L Wei XE Liu Y Lin C et al . Increased functional connectivity between default mode network and visual network potentially correlates with duration of residual dizziness in patients with benign paroxysmal positional vertigo. Front Neurol. (2024) 15:1363869. doi: 10.3389/fneur.2024.1363869
64.
Faralli M Lapenna R Giommetti G Pellegrino C Ricci G . Residual dizziness after the first BPPV episode: role of otolithic function and of a delayed diagnosis. Eur Arch Otorhinolaryngol. (2016) 273:3157–65. doi: 10.1007/s00405-016-3947-z
65.
Lacour M Bernard-Demanze L . Interaction between vestibular compensation mechanisms and vestibular rehabilitation therapy: 10 recommendations for optimal functional recovery. Front Neurol. (2015) 5:285. doi: 10.3389/fneur.2014.00285
66.
Martellucci S Stolfa A Castellucci A Pagliuca G Clemenzi V Terenzi V et al . Recovery of regular daily physical activities prevents residual dizziness after canalith repositioning procedures. Int J Environ Res Public Health. (2022) 19:490. doi: 10.3390/ijerph19010490
67.
Gu L Chen J Zhang Q Shen J Ma X Wang W et al . [Effect of the course of posterior semicircular canal benign paroxysmal positional vertigo on residual symptoms after successful canalith repositioning procedure]. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. (2021) 35:976–80. doi: 10.13201/j.issn.2096-7993.2021.11.004
68.
Galluzzi F Garavello W . Benign paroxysmal positional vertigo in children: a narrative review. J Int Adv Otol. (2022) 18:177–82. doi: 10.5152/iao.2022.20087
69.
Grove CR Souza WH Gerend PL Ryan CA Schubert MC . Patients' experiences with management of benign paroxysmal positional vertigo: insights from the Vestibular Disorders Association registry. Patient Relat Outcome Meas. (2022) 13:157–68. doi: 10.2147/PROM.S370287
70.
Pollak L Davies RA Luxon LL . Effectiveness of the particle repositioning maneuver in benign paroxysmal positional vertigo with and without additional vestibular pathology. Otol Neurotol. (2002) 23:79–83. doi: 10.1097/00129492-200201000-00018
71.
Coto J Alvarez CL Cejas I Colbert BM Levin BE Huppert J et al . Peripheral vestibular system: age-related vestibular loss and associated deficits. J Otol. (2021) 16:258–65. doi: 10.1016/j.joto.2021.06.001
72.
Wei W Sayyid ZN Ma X Wang T Dong Y . Presence of anxiety and depression symptoms affects the first time treatment efficacy and recurrence of benign paroxysmal positional vertigo. Front Neurol. (2018) 9:178. doi: 10.3389/fneur.2018.00178
73.
Meredith FL Rennie KJ . Dopaminergic inhibition of Na+ currents in vestibular inner ear afferents. Front Neurosci. (2021) 15:710321. doi: 10.3389/fnins.2021.710321
74.
Drago F Nardo L Rampello L Raffaele R . Vestibular compensation in aged rats with unilateral labyrinthectomy treated with dopaminergic drugs. Pharmacol Res. (1996) 33:135–40. doi: 10.1006/phrs.1996.0020
75.
Eberhard KE Kirkeby S Hansen LJ Cayé-Thomasen P . Neurotransmitter and neurotransmitter receptor expression in the saccule of the human vestibular system. Prog Neurobiol. (2022) 212:102238. doi: 10.1016/j.pneurobio.2022.102238
76.
Carthy E Ellender T . Histamine, neuroinflammation and neurodevelopment: a review. Front Neurosci. (2021) 15:680214. doi: 10.3389/fnins.2021.680214
77.
Obermann M Wurthmann S Steinberg BS Theysohn N Diener HC Naegel S . Central vestibular system modulation in vestibular migraine. Cephalalgia. (2014) 34:1053–61. doi: 10.1177/0333102414527650
78.
Guo J Wang J Liang P Tian E Liu D Guo Z et al . Vestibular dysfunction leads to cognitive impairments: state of knowledge in the field and clinical perspectives (Review). Int J Mol Med. (2024) 53:36. doi: 10.3892/ijmm.2024.5360
79.
Caixeta GC Doná F Gazzola JM . Cognitive processing and body balance in elderly subjects with vestibular dysfunction. Braz J Otorhinolaryngol. (2012) 78:87–95. doi: 10.1590/S1808-86942012000200014
80.
Sun J Ma X Yang Y He K Wang W Shen J et al . Associations between cognition, anxiety, depression, and residual dizziness in elderly people with BPPV. Front Aging Neurosci. (2023) 15:1208661. doi: 10.3389/fnagi.2023.1208661
81.
Smith LJ Wilkinson D Bodani M Surenthiran SS . Cognition in vestibular disorders: state of the field, challenges, and priorities for the future. Front Neurol. (2024) 15:1159174. doi: 10.3389/fneur.2024.1159174
82.
El Khiati R Tighilet B Besnard S Chabbert C . Vestibular disorders and hormonal dysregulations: state of the art and clinical perspectives. Cells. (2023) 12:656. doi: 10.3390/cells12040656
83.
Zhang X Zhang Z Lv X . Predictive values of serum estradiol, calcium, and 25-hydroxyvitamin D levels for recurrence of benign paroxysmal positional vertigo in postmenopausal women. Turk J Phys Med Rehabil. (2022) 68:30–6. doi: 10.5606/tftrd.2022.5964
84.
Shiozaki T Ito T Wada Y Yamanaka T Kitahara T . Effects of vestibular rehabilitation on physical activity and subjective dizziness in patients with chronic peripheral vestibular disorders: a six-month randomized trial. Front Neurol. (2021) 12:656157. doi: 10.3389/fneur.2021.656157
85.
Gu L Gao D Ma X Shen J Wang L Sun J et al . Effect of benign paroxysmal positional vertigo course on residual symptoms after successful canalith repositioning procedures: a prospective controlled trial. Sci Prog. (2025) 108:368504241308959. doi: 10.1177/00368504241308959
86.
Ellmers TJ Kal EC Young WR . Consciously processing balance leads to distorted perceptions of instability in older adults. J Neurol. (2021) 268:1374–84. doi: 10.1007/s00415-020-10288-6
87.
Knight B Bermudez F Shermetaro C . Persistent postural-perceptual dizziness. [Updated 2023 Apr 15]. In: StatPearls. Treasure Island, FL: StatPearls Publishing (2025). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK578198/
88.
Indovina I Passamonti L Mucci V Chiarella G Lacquaniti F Staab JP . Brain correlates of persistent postural-perceptual dizziness: a review of neuroimaging studies. J Clin Med. (2021) 10:4274. doi: 10.3390/jcm10184274
89.
Lempert T Olesen J Furman J Waterston J Seemungal B Carey J et al . Vestibular migraine: diagnostic criteria. J Vestib Res. (2012) 22:167–72. doi: 10.3233/VES-2012-0453
90.
Beh SC . Vestibular migraine: how to sort it out and what to do about it. J Neuroophthalmol. (2019) 39:208–19. doi: 10.1097/WNO.0000000000000791
91.
Lopez-Escamez JA Carey J Chung WH Goebel JA Magnusson M Mandalà M et al . Diagnostic criteria for Menière's disease. J Vestib Res. (2015) 25:1–7. doi: 10.3233/VES-150549
92.
Álvarez-Morujo de Sande MG González-Aguado R Guerra-Jiménez G Domènech-Vadillo E Galera-Ruiz H Figuerola-Massana E et al . Probable benign paroxysmal positional vertigo, spontaneously resolved: Incidence in medical practice, patients' characteristics and the natural course. J Otol. (2019) 14:111–6. doi: 10.1016/j.joto.2019.04.002
93.
von Brevern M Bertholon P Brandt T Fife T Imai T Nuti D et al . Benign paroxysmal positional vertigo: diagnostic criteria. J Vestib Res. (2015) 25:105–17. doi: 10.3233/VES-150553
94.
Kerber KA Newman-Toker DE . Misdiagnosing dizzy patients: common pitfalls in clinical practice. Neurol Clin. (2015) 33:565–75. doi: 10.1016/j.ncl.2015.04.009
95.
Bhattacharyya N Gubbels SP Schwartz SR Edlow JA El-Kashlan H Fife T et al . Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngol Head Neck Surg. (2017) 156(3_suppl):S1–S47. doi: 10.1177/0194599816689667
96.
Tighilet B Trico J Marouane E Zwergal A Chabbert C . Histaminergic system and vestibular function in normal and pathological conditions. Curr Neuropharmacol. (2024) 22:1826–45. doi: 10.2174/1570159X22666240319123151
97.
Kim MK Yun SY Lee S Lee JO Sung SY Lee JY et al . Efficacy of vestibular rehabilitation and its facilitating and hindering factors from real-world clinical data. Front Neurol. (2024) 15:1329418. doi: 10.3389/fneur.2024.1329418
98.
McDonnell MN Hillier SL . Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev. (2015) 1:CD005397. doi: 10.1002/14651858.CD005397.pub4
99.
Bressi F Vella P Casale M Moffa A Sabatino L Lopez MA et al . Vestibular rehabilitation in benign paroxysmal positional vertigo: reality or fiction?Int J Immunopathol Pharmacol. (2017) 30:113–22. doi: 10.1177/0394632017709917
100.
Cui Q Wen C Yan J Wang R Han R Huang L . Effects of different durations and frequencies of vestibular rehabilitation in patients with residual symptoms after benign paroxysmal positional vertigo repositioning. Ann Otol Rhinol Laryngol. (2024) 133:307–16. doi: 10.1177/00034894231216277
101.
Cohen HS Kimball KT . Effectiveness of treatments for BPPV of the posterior canal. Otol Neurotol. (2005) 26:1034–40. doi: 10.1097/01.mao.0000185044.31276.59
102.
Heydari M Ahadi M Jalaei B Maarefvand M . Talebi H. The additional effect of vestibular rehabilitation therapy on residual dizziness after successful modified Epley procedure for posterior canal benign paroxysmal positional vertigo. Am J Audiol. (2021) 30:535–43. doi: 10.1044/2021_AJA-20-00171
103.
Ugurlu B Evcimik MF Ozkurt FE Sapci T Gursel AO . Comparison of the effects of betahistine dihydrochloride and Brandt-Daroff exercises in addition to Epley maneuver in the treatment of benign paroxysmal positional vertigo. Int Adv Otol. (2012) 8:45–50.
104.
Soto E Vega R . Neuropharmacology of vestibular system disorders. Curr Neuropharmacol. (2010) 8:26–40. doi: 10.2174/157015910790909511
105.
Di Mizio G Marcianò G Palleria C Muraca L Rania V Roberti R et al . Drug-drug interactions in vestibular diseases, clinical problems, and medico-legal implications. Int J Environ Res Public Health. (2021) 18:12936. doi: 10.3390/ijerph182412936
106.
Marmor S Karaca-Mandic P Adams ME . Vestibular suppressant utilization and subsequent falls among patients 65 years and older with dizziness in the United States. J Am Geriatr Soc. (2025) 0:1–8. doi: 10.1111/jgs.19377
107.
Sharif S Khoujah D Greer A Naples JG Upadhye S Edlow JA . Vestibular suppressants for benign paroxysmal positional vertigo: a systematic review and meta-analysis of randomized controlled trials. Acad Emerg Med. (2023) 30:541–51. doi: 10.1111/acem.14608
108.
Singh KR Singh M . Current perspectives in the pharmacotherapy of vertigo. Otorhinolaryngol Clin Int J. (2012) 4:81–5. doi: 10.5005/jp-journals-10003-1091
109.
Alahmari KA Alshehri S . Evaluating the efficacy of vestibular rehabilitation therapy on quality of life in persistent postural-perceptual dizziness: the role of anxiety and depression in treatment outcomes. Front Neurol. (2025) 16:1524324. doi: 10.3389/fneur.2025.1524324
110.
Han BI Song HS Kim JS . Vestibular rehabilitation therapy: review of indications, mechanisms, and key exercises. J Clin Neurol. (2011) 7:184–96. doi: 10.3988/jcn.2011.7.4.184
111.
Rodrigues DL Ledesma ALL Pires de . Oliveira CA, Bahmad F Jr. Effect of vestibular exercises associated with repositioning maneuvers in patients with benign paroxysmal positional vertigo: a randomized controlled clinical trial. Otol Neurotol. (2019) 40:e824–9. doi: 10.1097/MAO.0000000000002324
112.
Gourgouvelis J Yielder P Murphy B . Exercise promotes neuroplasticity in both healthy and depressed brains: an fMRi pilot study. Neural Plast. (2017) 2017:8305287. doi: 10.1155/2017/8305287
113.
Lacour M Sterkers O . Histamine and betahistine in the treatment of vertigo: elucidation of mechanisms of action. CNS Drugs. (2001) 15:853–70. doi: 10.2165/00023210-200115110-00004
114.
Tighilet B Léonard J Watabe I Bernard-Demanze L Lacour M . Betahistine treatment in a cat model of vestibular pathology: pharmacokinetic and pharmacodynamic approaches. Front Neurol. (2018) 9:431. doi: 10.3389/fneur.2018.00431
115.
Antons M Lindner M Eilles E Günther L Delker A Branner C et al . Dose- and application route-dependent effects of betahistine on behavioral recovery and neuroplasticity after acute unilateral labyrinthectomy in rats. Front Neurol. (2023) 14:1175481. doi: 10.3389/fneur.2023.1175481
116.
Strupp M Churchill GC Naumann I Mansmann U Al Tawil A Golentsova A et al . Examination of betahistine bioavailability in combination with the monoamine oxidase B inhibitor, selegiline, in humans-a non-randomized, single-sequence, two-period titration, open label single-center phase 1 study (PK-BeST). Front Neurol. (2023) 14:1271640. doi: 10.3389/fneur.2023.1271640
117.
Ramos Alcocer R Ledezma Rodríguez JG Navas Romero A Cardenas Nuñez JL Rodríguez Montoya V Deschamps JJ et al . Use of betahistine in the treatment of peripheral vertigo. Acta Otolaryngol. (2015) 135:1205–11. doi: 10.3109/00016489.2015.1072873
118.
Li W Sun J Zhao Z Xu J Wang H Ding R et al . Efficacy of Epley's maneuver plus betahistine in the management of PC-BPPV: a systematic review and meta-analysis. Medicine. (2023) 102:e33421. doi: 10.1097/MD.0000000000033421
119.
Stambolieva K Angov G . Effect of treatment with betahistine dihydrochloride on the postural stability in patients with different duration of benign paroxysmal positional vertigo. Int Tinnitus J. (2010) 16:32–6.
120.
Cavaliere M Mottola G Iemma M . Benign paroxysmal positional vertigo: a study of two manoeuvres with and without betahistine. Acta Otorhinolaryngol Ital. (2005) 25:107–12.
121.
Alsolamy R Alaraifi AK Aloqaili Y . Effectiveness of betahistine as an add-on therapy to epley maneuver for benign paroxysmal positional vertigo: a systematic review and meta-analysis. World J Otorhinolaryngol Head Neck Surg. (2024) 11:116–24. doi: 10.1002/wjo2.161
122.
Guneri EA Kustutan O . The effects of betahistine in addition to epley maneuver in posterior canal benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg. (2012) 146:104–8. doi: 10.1177/0194599811419093
123.
Libonati GA Leone A Martellucci S Gallo A Albera R Lucisano S et al . Prevention of recurrent benign paroxysmal positional vertigo: the role of combined supplementation with vitamin D and antioxidants. Audiol Res. (2022) 12:445–56. doi: 10.3390/audiolres12040045
124.
National Institutes of Health (NIH) . Vitamin D Fact Sheet for Health Professionals (2024). Available online at: https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/ (Accessed May 30, 2025).
125.
Kong TH Jung SY Seo YJ Shim DB . Vitamin D supplementation in preventing the recurrence of benign paroxysmal positional vertigo. Laryngoscope Investig Otolaryngol. (2024) 9:e1225. doi: 10.1002/lio2.1225
126.
Chua KW Huang X Koh XH Soh JFJY Barrera VC Anaikatti P et al . Randomized controlled trial assessing vitamin D's role in reducing BPPV recurrence in older adults. Otolaryngol Head Neck Surg. (2025) 172:127–36. doi: 10.1002/ohn.954
127.
Montero-Odasso M van der Velde N Martin FC Petrovic M Tan MP Ryg J et al . World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing. (2022) 51:afac205. doi: 10.1093/ageing/afac205
128.
Deng W Yang C Xiong M Fu X Lai H Huang W . Danhong enhances recovery from residual dizziness after successful repositioning treatment in patients with benign paroxysmal positional vertigo. Am J Otolaryngol. (2014) 35:753–7. doi: 10.1016/j.amjoto.2014.07.001
129.
Decker L Basta D Burkart M Ernst A . Balance training with vibrotactile neurofeedback and Ginkgo biloba extract in age-related vertigo. Front Neurol. (2021) 12:691917. doi: 10.3389/fneur.2021.691917
130.
Gao X Cheng Y Liu F Han X Liu C . The clinical efficacy and safety of Ginkgo biloba in vertigo patients: a meta-analysis. Adv Integr Med. (2023) 10:158–66. doi: 10.1016/j.aimed.2023.10.001
131.
Ya J Bayraktutan U . Vascular ageing: mechanisms, risk factors, and treatment strategies. Int J Mol Sci. (2023) 24:11538. doi: 10.3390/ijms241411538
132.
Yang Y Tian J Otero-Millan J Kheradmand A . Video ocular counter roll: a bedside test of otolith-ocular function. Ann Clin Transl Neurol. (2023) 10:2426–9. doi: 10.1002/acn3.51921
133.
Kingma H Gullikers H de Jong I Jongen R Dolmans M Stegeman P . Real time binocular detection of horizontal vertical and torsional eye movements by an infra red video-eye tracker. Acta Otolaryngol Suppl. (1995) 520(Pt 1):9–15. doi: 10.3109/00016489509125176
134.
Kingma H . Clinical testing of the statolith-ocular reflex. ORL J Otorhinolaryngol Relat Spec. (1997) 59:198–208. doi: 10.1159/000276940
135.
Wuyts FL Hoppenbrouwers M Pauwels G Van de Heyning PH . Utricular sensitivity and preponderance assessed by the unilateral centrifugation test. J Vestib Res. (2003) 13:227–34. doi: 10.3233/VES-2003-134-607
Summary
Keywords
BPPV, residual dizziness, algorithm, risk factors, vestibular compensation, type 1 BPPV-related residual dizziness, type 2 BPPV-related residual dizziness
Citation
Kingma H, Manzari L and Özgirgin N (2026) Enhancing patient care in BPPV-related residual dizziness: introducing the CLEAR algorithm to support BPPV-RD recognition and follow-up strategies. Front. Neurol. 16:1689617. doi: 10.3389/fneur.2025.1689617
Received
20 August 2025
Accepted
29 September 2025
Published
02 January 2026
Volume
16 - 2025
Edited by
Andrés Soto-Varela, Complejo Hospitalario Universitario de Santiago, Spain
Reviewed by
Jose Antonio Lopez-Escamez, University of Sydney, Australia
Dietmar Basta, Unfallkrankenhaus Berlin, Germany
Updates
Copyright
© 2026 Kingma, Manzari and Özgirgin.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Herman Kingma, hermanuskingma@gmail.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.