 Conrad Leitsmann
Conrad Leitsmann Marianne Schmid1
Marianne Schmid1 Arne Strauss
Arne Strauss- 1Department of Urology, University Medical Center Goettingen, Goettingen, Germany
- 2Department of Nuclear Medicine, University Medical Center Goettingen, Goettingen, Germany
Purpose: Several studies have demonstrated an advantage of 68Ga-PSMA-PET/CT as staging modality for detection of prostate cancer (PCa) metastases. Data concerning metastatic manifestation and impact on PCa development of mesorectal lymph nodes (MLN) is limited. Our investigation describes MLN metastases as index lesion in 68Ga-PSMA PET/CT imaging for recurrent PCa.
Methods: Twelve PCa patients with biochemical recurrence (BCR) after primary therapy who prospectively underwent a baseline 68Ga-PSMA-PET/CT initially showed MLN metastases. Eight of these patients received a follow-up 68Ga-PSMA-PET/CT to evaluate treatment response and further evolution. Prostate-specific antigen (PSA)-levels, changes in PSMA-uptake of MLN metastases and further 68Ga-PSMA PET/CT findings were recorded.
Results: Median PSA at the first 68Ga-PSMA-PET/CT was 5.39 ng/ml. In all patients therapeutic management changed after the first 68Ga-PSMA-PET/CT. Androgen deprivation therapy (ADT) was initiated in seven of eight patients, one patient restarted initial ADT. Three patients additionally received salvage radiation therapy (sRT) including the prostatic lodge and docetaxel chemotherapy was started in one case. At follow-up, a decrease of PSA-level was detected in all patients (median 2.05 ng/ml) after median 10 months. In six of eight patients we observed a decrease or complete regress of PSMA-uptake in MLN in the follow-up 68Ga-PSMA-PET/CT.
Conclusion: MLN metastases detected by 68Ga-PSMA-PET/CT seem to be a relevant localization of tumor manifestation and may serve as index lesion in the treatment of recurrent PCa. Besides the known oncological benefits of ADT and sRT, in case of sole MLN metastases individualized therapy like salvage lymphadenectomy or RT with a defined radiation field could be options for these patients.
Introduction
In Europe the most common cancer in male is prostate cancer (PCa) with growing incidence in the past two decades (1). Radical prostatectomy (RP) and radiation therapy (RT) are curative therapeutic options (2). Nonetheless, within 10 years after primary therapy up to 40% of patients develop biochemical recurrence (BCR) (3). Here, due to limited sensitivity and specificity conventional imaging methods, such as computed tomography (CT) and magnetic resonance imaging (MRI), might struggle to accurately determine the presence or absence of metastatic or recurrent PCa (4, 5).
The Type-II transmembrane protein prostate specific membrane antigen (PSMA) is overexpressed in almost all PCa cells (6). Luiting et al. demonstrated promising results for detecting PCa relapse by Gallium (68Ga)-labeled PSMA positron emission tomography/computed tomography (PET/CT) (68Ga-PSMA PET/CT) (7). Further studies have confirmed the advantage of 68Ga-PSMA PET/CT compared to conventional imaging as well as functional 18F-choline-based PET/CT for patients with BCR (5, 8–11). Increasingly discussed salvage treatment of recurrent PCa also demands exact staging (4, 10, 12, 13). Roach et al. prospectively investigated the value of 68Ga-PSMA PET/CT in the management of PCa (14). They found that 68Ga-PSMA PET/CT scans detected previously unsuspected disease and assumed a greater impact in patients with BCR.
PCa typically spreads to the proximal external iliac, the lower sacral vessel, the obturator, the upper sacral, the common iliacal and, at last, the paraaortic lymph nodes (15). A previous retrospective analysis by Hijazi et al. however showed PCa metastases in mesorectal lymph nodes (MLN) in 12 of 76 patients with BCR, which were detected by 68Ga-PSMA PET/CT (11). Current studies addressing this issue are limited. Previous reports either described MLN metastases of PCa occurring in sentinel lymph node scintigraphy or as a random result during anterior rectal resection in patients with rectal cancer (16–19). We are considering MLN as a relevant region for lymph node metastasis in patients with recurrent PCa and as an important therapeutic target. The rationale behind is to further improve PCa-outcomes. A recent analysis by Horn et al. mentioned the correlation of a single lesion on PSMA PET/CT and low PSA as favorable prognosticators following PSMA-targeted radioguided surgery (20).
The current study presents observations of MLN metastases as index lesion for recurrent PCa and describes the depiction of treatment changes in patients with BCR and confirmed MLN metastases. In this context we discuss therapeutic options such as the surgical challenge of MLN dissection and the definition of the radiation field.
Methods
Patients' Characteristics
Patients with BCR after RT or RP or primary androgen deprivation therapy (ADT) were included. Twelve patients with BCR according to the EAU guidelines showed solitary MLN metastases in a baseline 68Ga-PSMA PET/CT (21). These 12 patients derive from a cohort, which was previously reported by Hijazi et al. of 76 patients with BCR, which were detected by 68Ga-PSMA PET/CT (11). One patient died during follow-up and was excluded from further investigation. Three of 12 patients were not available for follow-up. A total of eight patients received a follow-up 68Ga-PSMA PET/CT.
For each patient initial TNM (2), initial Gleason-Score, initial PSA-value (iPSA), year and type of primary treatment, date of the baseline 68Ga-PSMA PET/CT, date of the follow-up 68Ga-PSMA PET/CT, PSA-value at the follow-up 68Ga-PSMA PET/CT, treatment since the baseline 68Ga-PSMA PET/CT, treatment (change) after the second 68Ga-PSMA PET/CT, oncological status and PSA-value at follow-up were available. The study was performed as an individual diagnostic pathway per patient in consensus with the patient and was approved by the local Ethics Committee of the University Medical Center Goettingen (approval June 7, 2015).
68Ga-PSMA-PET/CT Imaging
Baseline 68Ga-PSMA PET/CT was performed between November 2014 and June 2015. Eight patients underwent a follow-up 68Ga-PSMA PET/CT between February and May 2016 to measure changes in the PSMA-uptake of MLN metastases or other PCa metastases. The 68Ga-PSMA PET/CT was performed as previously described (11, 22). An experienced nuclear medicine physician analyzed the images. The maximal standard uptake volume (SUVmax) 1 and 3 h post injection was recorded.
Statistical Analysis
Descriptive statistics of variables focused on frequencies. Means and standard deviations, medians and interquartile ranges were reported. Covariates consisted of initial TNM, initial Gleason-Score, iPSA, year and type of primary treatment, date of the baseline 68Ga-PSMA PET/CT, date of the follow-up 68Ga-PSMA PET/CT, PSA-value at the follow-up 68Ga-PSMA PET/CT, treatment since the first 68Ga-PSMA PET/CT, treatment change since the follow-up 68Ga-PSMA PET/CT, oncological status and PSA-value at follow-up.
All analyses were performed using Statistical Package for the IBM (SPSS, Inc., Chicago, IL, version 25). All parameters were analyzed with Fisher exact test.
Results
Patients' Characteristics
Characteristics of the total cohort are displayed in Table 1. Median age was 74 years (range 66–81 years), median iPSA was 19.25 ng/ml (range 4.6–90 ng/ml). Eight of the 12 patients underwent RP with standardized lymph node dissection as primary therapy (21). Two patients received primary ADT, one received a prostate-hyperthermia therapy and one received percutaneous RT. Median PSA at the first 68Ga-PSMA PET/CT was 5.39 ng/ml (range 0.31–67.21 ng/ml). Baseline 68Ga-PSMA-PET/CT showed predominantly one MLN metastasis (only one patient had two lesions). Time interval between primary therapy and first 68Ga-PSMA PET/CT was median 36 month (range 9–231 months). Median FU of the total study period was 32 months (range 29–38 months).
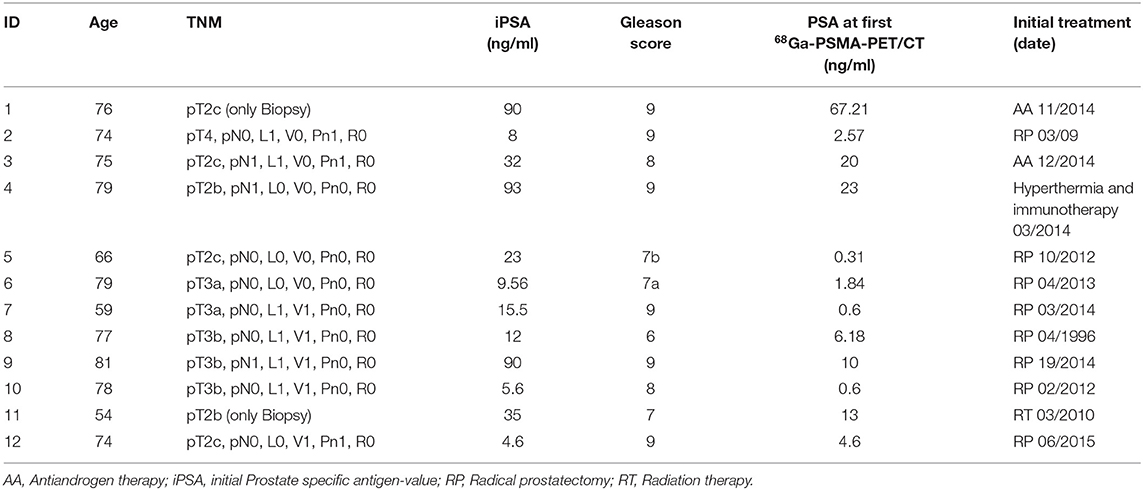
Table 1. Patients' characteristics of the initial study group (n = 12).
Follow-Up
Follow-up data are shown in Table 2. Median time between the two 68Ga-PSMA-PET/CT imaging was 10 months (range 8–14 months). A decrease of PSA serum value was demonstrated in all patients (median decrease −2.02 ng/ml, range −0.3 to −66.9 ng/ml). In all patients therapeutic management changed after the diagnosis of MLN metastases in the baseline 68Ga-PSMA-PET/CT. ADT [Luteinizing hormone-releasing hormone (LHRH) receptor agonists and antagonists] was initiated in seven of eight patients. One patient restarted initial ADT. Three patients received additional salvage RT including the prostatic lodge and docetaxel chemotherapy was started in one case. Three of these eight patients demonstrated a PSA <0.001 at the second 68Ga-PSMA-PET/CT.
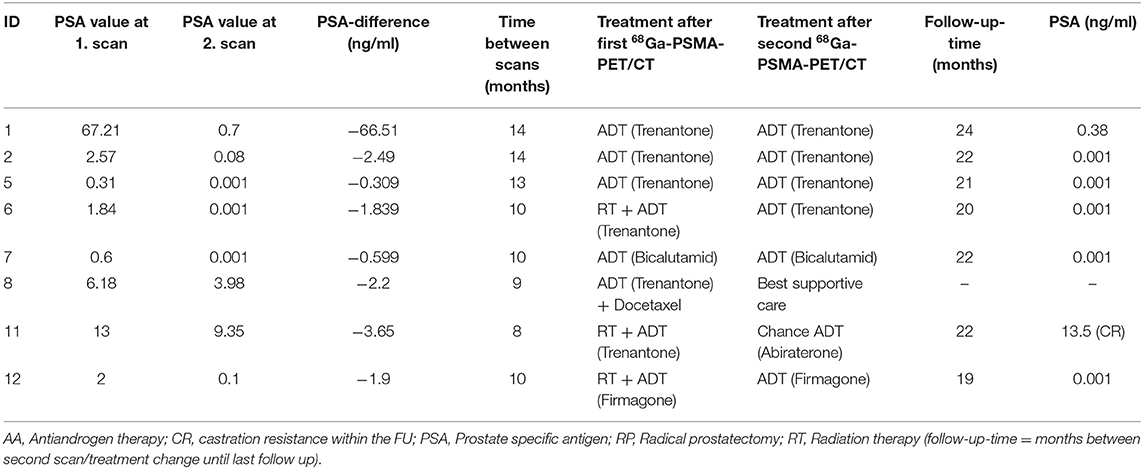
Table 2. Patient's follow up data (n = 8).
Oncologic treatments after the follow-up 68Ga-PSMA-PET/CT are shown in Table 2. Six of eight patients continued ADT and no change of treatment was needed. These patients showed hormone-sensitive PCa. In one patient antiandrogen therapy was changed (LHRH agonist replaced by Abiraterone acetate) as the follow-up 68Ga-PSMA-PET/CT showed a regression of the MLN metastasis but revealed one new metastasis next to the left kidney vessel. This patient developed castration resistant disease. Because of a massive disease progression decision for best supportive care strategy was made for one patient. For this patient we could not evaluate the castration level in the follow up.
PSA-values at the last follow-up between November 2017 and March 2018 [follow-up time median 22 months (range 19–24 months)] measured below 0.001 ng/ml in five of these six patients.
Comparison of 68Ga-PSMA-PET/CT Imaging
We summarized results of the baseline and follow-up 68Ga-PSMA-PET/CT in Table 3. Median SUVmax of the MLN 3 h post injection (p.i.) was 7.5 (range 3.2–13.8). Only one patient showed more than one MLN metastasis in the baseline scan.

Table 3. Comparison of 68Ga-PSMA-PET/CT imaging (n = 8).
In the follow-up scan five patients showed no more uptake of PSMA in 68Ga-PSMA-PET/CT imaging at all. An example is shown in Figure 1. The uptake declined in one patient from SUVmax 10.5–3.5 3 h p.i. One patient presented an increase of the one MLN metastasis from SUVmax 7.7–8.8 3 h p.i. and revealed new metastases in the liver (SUVmax 7.1 3 h p.i.), retroperitoneal (SUVmax 12.7 3 h p.i.), and mediastinal (SUVmax 8.1 3 h p.i.) as well as local tumor recurrence (SUVmax of 5.8 3 h p.i.). Another patient showed regression of the two MLN metastases (SUVmax 5.5–3.7 3 h p.i.), but the follow-up 68Ga-PSMA-PET/CT revealed one new metastasis next to the left kidney vessels (SUVmax of 7.8 3 h p.i.).
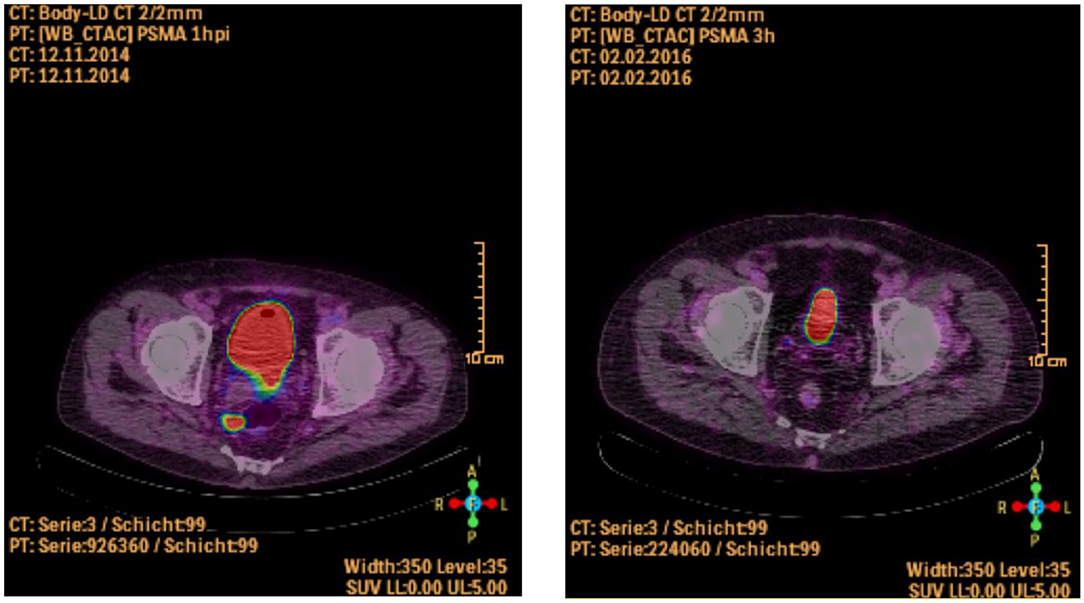
Figure 1. Patient with a singular MLN metastasis in the first 68Ga-PSMA-PET/CT (picture on the left side) and showing no more PSMA-uptake following ADT in the second scan after 13 months (picture on the right side, Patient ID 1).
Discussion
The aim of our study was to evaluate MLN metastases as “index lesion” in patients with recurrent PCa. Hijazi et al. showed solitary metastasis in MLN detected by 68Ga-PSMA-PET/CT in 12 of 76 patients (11). We could include eight of these 12 patients into a follow-up and present our observations. All of these patients started ADT with LHRH agonists or antagonists after the first scan. Two of these six patients were additionally treated with RT including pelvic lymph nodes and the prostatic bed. Six patients showed definitive benefit of secondary treatments and PSA-values decreased significantly (p < 0.01). ADT and RT resulted in complete regress or at least reduced PSMA-uptake of MLN metastases in six of eight patients in the follow-up 68Ga-PSMA-PET/CT. Additionally, PSA was <0.001 ng/ml in three of these patients at the second 68Ga-PSMA-PET/CT and in five at last follow-up. Usually, in PCa patients with PSA-values below 0.001 ng/ml after treatment further imaging would not be recommend. However, previous investigations report of superior imaging and detection of metastases with 68Ga-PSMA PET/CT (14). As our study intended to investigate its value in treatment monitoring, five patients with PSA-values below 0.001 ng/ml underwent a follow-up 68Ga-PSMA-PET/CT in this context. In these patients no additional metastases were found.
In the current literature comparable studies are rare. For a long time MNL have been never considered as a route of PCa spread. Murray et al. and Mourra et al. identified metastases of PCa in MLN in 4.5 and 9.4% of histologically examined lymph nodes in patients who underwent anterior rectal resection (16, 17). These studies demonstrated a relevant number of patients with MLN metastases of PCa. Additionally, Swanson et al. showed in an investigation of lymphatic drainage of PCa that PCa rarely metastasizes in MLN and that an assessment of nodal staging based on obturator lymph node dissection had an accuracy of 50% (15). A standard dissection of pelvic lymph nodes does not include the mesorectum region or the posterior pelvic subsite (PPS) (23).
Current data showed a promising opportunity using 68Ga-PSMA-PET/CT for assessment of lymph node metastases in PCa patients with BCR prior to salvage lymphadenectomy (24). These studies use this fact to investigate possible PSMA-guided surgery in these patients (25). A very recent review revealed PSMA-PET/CT as an indicator for metastasis targeted therapies in patients with recurrent PCa (26). So, it is most important to exactly detect and locate lymph node metastases before salvage treatment of PCa, as well as in recurrent PCa. This could affect the choice of treatment strategies like salvage lymphadenectomy or PSMA-guided surgery that has been proved to be successful concerning intraoperative detection and removal of metastatic lesions promises to improve prognosis of recurrent PCa-patients (27). However, patients with MLN metastases of PCa, like demonstrated in our study, are a small subgroup of patients which have unfavorable ratio of risk/benefit for a salvage lymph dissection because of the difficult surgical approach. Due to the difficulty of the surgical approach to MNL metastases three of eight patients of our study therefore underwent adjuvant RT. Two of these had no PSMA-uptake in the second scan and a significant decrease of PSA-values. Although our study could not prove an additional positive effect of adjuvant RT due to the small number of patients, this option may serve as possible treatment modality for patients with MLN metastases. Resent publications used 68Ga-PSMA-PET/CT for the planning of RT (28, 29). Schiller et al. and Habl et al. showed a significant influence of the higher detection rate of PCa lesions with 68Ga-PSMA-PET/CT imaging for radiation planning in recurrent PCa patients allowing individually personalized treatment compared to conventional CT or MRI staging. Of note, unless lymph node involvement is assured, the posterior pelvic subsite (PPS) below S3 or the mesorectal region is usually not comprised in the radiation filed of PCa (30).
Limitations of our study include the small number of patients, heterogenic baseline oncologic parameters like iPSA or Gleason and an incomplete follow-up of all 12 patients. Additionally, no comparison or control group was present. We focused on patients with mesorectal lymph node metastases to evaluate this index lesion and we did not investigate the total initial study group with a follow up PSMA-PET/CT. Reasons were the justification of exposure to radiation and the high rate of patients lost to follow up. Two patients seemed to have no benefit of the initiated treatment. One patient showed a new PSMA-positive lymph node next to a kidney vessel. A possible reason for this new metastasis might concern the irradiation area, which was focused on pelvic lymph nodes and the prostatic fossa and not on the aortocaval lymph node region. One patient presented a severe tumor progression in the follow-up 68Ga-PSMA-PET/CT. This patient had the longest time interval between the initial PCa therapy and the change of oncological treatment (9 years) and was one of the oldest patients in our cohort (77 years).
Further studies with larger number of patients need to be performed to evaluate the relevance of our findings. Future investigations should focus on the potential benefit of individual RT vs. (challenging) guided surgery vs. systemic treatments.
Conclusions
Recent studies showed an optimized detection of metastasis in recurrent PCa by 68Ga-PSMA-PET/CT imaging. This investigation used MLN metastases as index lesion. Considering such a rare localization like the mesorectum reveals individualized treatment options for such patients and may lead to improved oncological outcomes.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethic Committee, University Medical Center Goettingen. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CL, LT, and AS: protocol/project development, data collection and management, data analysis, and manuscript writing. MS: manuscript editing and data collection and management. C-OS: protocol/project development, data collection and management, and data analysis. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Bray F, Lortet-Tieulent J, Ferlay J, Forman D, Auvinen A. Prostate cancer incidence and mortality trends in 37 European countries: an overview. Eur J Cancer. (2010) 46:3040–52. doi: 10.1016/j.ejca.2010.09.013
2. Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. (2017) 71:618–29. doi: 10.1016/j.eururo.2016.08.003
3. Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3,478 consecutive patients: long-term results. J Urol. (2004) 172:910–4. doi: 10.1097/01.ju.0000134888.22332.bb
4. Kosuri S, Akhtar NH, Smith M, Osborne JR, Tagawa ST. Review of salvage therapy for biochemically recurrent prostate cancer: the role of imaging and rationale for systemic salvage targeted anti-prostate-specific membrane antigen radioimmunotherapy. Adv Urol. (2012) 2012:921674. doi: 10.1155/2012/921674
5. Afshar-Oromieh A, Avtzi E, Giesel FL, Holland-Letz T, Linhart HG, Eder M, et al. The diagnostic value of PET/CT imaging with the (68)Ga-labelled PSMA ligand HBED-CC in the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. (2015) 42:197–209. doi: 10.1007/s00259-014-2949-6
6. Perera M, Papa N, Christidis D, Wetherell D, Hofman MS, Murphy DG, et al. Sensitivity, specificity, and predictors of positive (68)Ga-prostate-specific membrane antigen positron emission tomography in advanced prostate cancer: a systematic review and meta-analysis. Eur Urol. (2016) 70:926–37. doi: 10.1016/j.eururo.2016.06.021
7. Luiting HB, Van Leeuwen PJ, Busstra MB, Brabander T, Van Der Poel HG, Donswijk ML, et al. Use of gallium-68 prostate-specific membrane antigen positron-emission tomography for detecting lymph node metastases in primary and recurrent prostate cancer and location of recurrence after radical prostatectomy: an overview of the current literature. BJU Int. (2020) 125:206–14. doi: 10.1111/bju.14944
8. Afshar-Oromieh A, Zechmann CM, Malcher A, Eder M, Eisenhut M, Linhart HG, et al. Comparison of PET imaging with a (68)Ga-labelled PSMA ligand and (18)F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur J Nucl Med Mol Imaging. (2014) 41:11–20. doi: 10.1007/s00259-013-2525-5
9. Ceci F, Uprimny C, Nilica B, Geraldo L, Kendler D, Kroiss A, et al. (68)Ga-PSMA PET/CT for restaging recurrent prostate cancer: which factors are associated with PET/CT detection rate? Eur J Nucl Med Mol Imaging. (2015) 42:1284–94. doi: 10.1007/s00259-015-3078-6
10. Morigi JJ, Stricker PD, Van Leeuwen PJ, Tang R, Ho B, Nguyen Q, et al. Prospective comparison of 18F-fluoromethylcholine versus 68Ga-PSMA PET/CT in prostate cancer patients who have rising PSA after curative treatment and are being considered for targeted therapy. J Nucl Med. (2015) 56:1185–90. doi: 10.2967/jnumed.115.160382
11. Hijazi S, Meller B, Leitsmann C, Strauss A, Ritter C, Lotz J, et al. See the unseen: mesorectal lymph node metastases in prostate cancer. Prostate. (2016) 76:776–80. doi: 10.1002/pros.23168
12. Heidenreich A, Moul JW, Shariat S, Karnes RJ. Role of salvage lymph node dissection in prostate cancer. Curr Opin Urol. (2016) 26:581–9. doi: 10.1097/MOU.0000000000000343
13. Pfister D, Porres D, Heidenreich A, Heidegger I, Knuechel R, Steib F, et al. Detection of recurrent prostate cancer lesions before salvage lymphadenectomy is more accurate with (68)Ga-PSMA-HBED-CC than with (18)F-Fluoroethylcholine PET/CT. Eur J Nucl Med Mol Imaging. (2016) 43:1410–7. doi: 10.1007/s00259-016-3366-9
14. Roach PJ, Francis R, Emmett L, Hsiao E, Kneebone A, Hruby G, et al. The impact of (68)Ga-PSMA PET/CT on management intent in prostate cancer: results of an Australian prospective multicenter study. J Nucl Med. (2018) 59:82–8. doi: 10.2967/jnumed.117.197160
15. Swanson GP, Hubbard JK. A better understanding of lymphatic drainage of the prostate with modern imaging and surgical techniques. Clin Genitourin Cancer. (2013) 11:431–40. doi: 10.1016/j.clgc.2013.04.031
16. Murray SK, Breau RH, Guha AK, Gupta R. Spread of prostate carcinoma to the perirectal lymph node basin: analysis of 112 rectal resections over a 10-year span for primary rectal adenocarcinoma. Am J Surg Pathol. (2004) 28:1154–62. doi: 10.1097/01.pas.0000131543.80147.3d
17. Mourra N, Parc Y, Mcnamara D, Tiret E, Flejou JF, Parc R. Lymph node metastases of prostatic adenocarcinoma in the mesorectum in patients with adenocarcinoma or villous tumor of the rectum with collision phenomenon in a single lymph node: report of five cases. Dis Colon Rectum. (2005) 48:384–9. doi: 10.1007/s10350-004-0776-8
18. Ganswindt U, Schilling D, Muller AC, Bares R, Bartenstein P, Belka C. Distribution of prostate sentinel nodes: a SPECT-derived anatomic atlas. Int J Radiat Oncol Biol Phys. (2011) 79:1364–72. doi: 10.1016/j.ijrobp.2010.01.012
19. Rousseau C, Le Thiec M, Ferrer L, Rusu D, Rauscher A, Maucherat B, et al. Preliminary results of a (68) Ga-PSMA PET/CT prospective study in prostate cancer patients with occult recurrence: diagnostic performance and impact on therapeutic decision-making. Prostate. (2019) 79:1514–22. doi: 10.1002/pros.23869
20. Horn T, Kronke M, Rauscher I, Haller B, Robu S, Wester HJ, et al. Single lesion on prostate-specific membrane antigen-ligand positron emission tomography and low prostate-specific antigen are prognostic factors for a favorable biochemical response to prostate-specific membrane antigen-targeted radioguided surgery in recurrent prostate cancer. Eur Urol. (2019) 76:517–23. doi: 10.1016/j.eururo.2019.03.045
21. Cornford P, Bellmunt J, Bolla M, Briers E, De Santis M, Gross T, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part II: treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur Urol. (2017) 71:630–42. doi: 10.1016/j.eururo.2016.08.002
22. Hijazi S, Meller B, Leitsmann C, Strauss A, Meller J, Ritter CO, et al. Pelvic lymph node dissection for nodal oligometastatic prostate cancer detected by 68Ga-PSMA-positron emission tomography/computerized tomography. Prostate. (2015) 75:1934–40. doi: 10.1002/pros.23091
23. Rigatti P, Suardi N, Briganti A, Da Pozzo LF, Tutolo M, Villa L, et al. Pelvic/retroperitoneal salvage lymph node dissection for patients treated with radical prostatectomy with biochemical recurrence and nodal recurrence detected by [11C]choline positron emission tomography/computed tomography. Eur Urol. (2011) 60:935–43. doi: 10.1016/j.eururo.2011.07.060
24. Rauscher I, Maurer T, Beer AJ, Graner FP, Haller B, Weirich G, et al. Value of 68Ga-PSMA HBED-CC PET for the assessment of lymph node metastases in prostate cancer patients with biochemical recurrence: comparison with histopathology after salvage lymphadenectomy. J Nucl Med. (2016) 57:1713–9. doi: 10.2967/jnumed.116.173492
25. Rauscher I, Duwel C, Wirtz M, Schottelius M, Wester HJ, Schwamborn K, et al. Value of (111) In-prostate-specific membrane antigen (PSMA)-radioguided surgery for salvage lymphadenectomy in recurrent prostate cancer: correlation with histopathology and clinical follow-up. BJU Int. (2017) 120:40–7. doi: 10.1111/bju.13713
26. Wondergem M, Van Der Zant FM, Broos WA, Knol RJ. Clinical impact of PSMA PET in biochemically recurrent prostate cancer; a review of the literature. Tijdschrift voor Urol. (2020) 10:109–21. doi: 10.1007/s13629-020-00296-6
27. Maurer T, Robu S, Schottelius M, Schwamborn K, Rauscher I, Van Den Berg NS, et al. (99m)Technetium-based prostate-specific membrane antigen-radioguided surgery in recurrent prostate cancer. Eur Urol. (2019) 75:659–66. doi: 10.1016/j.eururo.2018.03.013
28. Habl G, Sauter K, Schiller K, Dewes S, Maurer T, Eiber M, et al. (68) Ga-PSMA-PET for radiation treatment planning in prostate cancer recurrences after surgery: Individualized medicine or new standard in salvage treatment. Prostate. (2017) 77:920–7. doi: 10.1002/pros.23347
29. Schiller K, Sauter K, Dewes S, Eiber M, Maurer T, Gschwend J, et al. Patterns of failure after radical prostatectomy in prostate cancer - implications for radiation therapy planning after (68)Ga-PSMA-PET imaging. Eur J Nucl Med Mol Imaging. (2017) 44:1656–62. doi: 10.1007/s00259-017-3746-9
Keywords: prostate cancer, metastases, mesorectal lymph node, PSMA, 68Ga-PSMA-PET/CT imaging
Citation: Leitsmann C, Schmid M, Sahlmann C-O, Trojan L and Strauss A (2021) Mesorectal Lymph Node Metastases as Index Lesion in 68Ga-PSMA-PET/CT Imaging for Recurrent Prostate Cancer. Front. Surg. 8:637134. doi: 10.3389/fsurg.2021.637134
Received: 02 December 2020; Accepted: 22 January 2021;
Published: 01 March 2021.
Edited by:
Clemens Mathias Rosenbaum, Asklepios Klinik Barmbek, GermanyReviewed by:
Philipp Mandel, University Hospital Frankfurt, GermanySami-Ramzi Leyh-Bannurah, St. Antonius-Hospital, Germany
Copyright © 2021 Leitsmann, Schmid, Sahlmann, Trojan and Strauss. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Conrad Leitsmann, Y29ucmFkLmxlaXRzbWFubkBtZWQudW5pLWdvZXR0aW5nZW4uZGU= orcid.org/0000-0001-5158-9706