 Tong Zhi
Tong Zhi Chengcheng Zhao
Chengcheng Zhao Xin Xiang
Xin Xiang Huadong Ni
Huadong Ni- Department of Anesthesiology and Pain Research Center, The Affiliated Hospital of Jiaxing University, Jiaxing, China
Background: Recent studies have demonstrated significant advancements in the treatment of hyperhidrosis. However, a bibliometric analysis of relevant studies in this field is notably lacking. This study aims to provide a detailed analysis of research trends and key areas of interest in hyperhidrosis over the last 16 years using bibliometric methods.
Methods: We searched the Web of Science Core Collection (WoSCC) database for hyperhidrosis-related publications from 2008 to 2023 and conducted bibliometric analysis using VOS viewer and the R package “bibliometrix.”
Results: The main research institutions involved in this study are the University of São Paulo, Hospital Israelita Albert Einstein, Yonsei University and Fujian Medical University, with a total of 728 articles included from 52 countries. Authors from these institutions have published in top journals, with Dermatologic Surgery being the most popular journal and the Journal of the American Academy of Dermatology being the most cited. A total of 2,830 authors have contributed to this field, with prominent researchers including Nelson Wolosker, Paulo Kauffman, Pedro Puech-Leão, Jose Ribas Milanez de Campos, and Dee Anna Glaser. Nelson Wolosker stands out as the most co-cited author. The primary focus of research in this area is on the treatment of hyperhidrosis and the prevention of post-operative complications. Emerging re-search hotspots include keywords such as “botulinum toxin,” “oxybutynin,” “sympathectomy,” “iontophoresis,” and “compensatory sweating”.
Conclusion: The most prevalent academic emphasis within this field remains the treatment of hyperhidrosis and the management of compensatory hyperhidrosis. Despite this academic preponderance, there is a compelling necessity to foster enhanced collaboration and exchange between disparate countries and institutions.
1 Introduction
Hyperhidrosis (HH) is a disorder characterized by pathologically focal or generalized excessive sweating, with autonomic dysfunction as one of the possible pathophysiological mechanisms (1, 2). It is classified into primary hyperhidrosis and secondary hyperhidrosis. Primary Hyperhidrosis (PHH) affects approximately 2% of the population and usually starts in adolescence with localized sweating from the armpits, hands, face, or feet (3). On the other hand, Secondary Hyperhidrosis (SHH) typically manifests as generalized sweating and is often linked to underlying health conditions or substance abuse. The following factors are associated with drug-induced hyperhidrosis: antipyretic and analgesic drugs, hypoglycemic drugs, antidepressants, etc. Additional factors include tumor tissue affecting the thermoregulatory center and obesity resulting in increased thermogenesis, which may collectively lead to secondary hyperhidrosis. Primary Hyperhidrosis is known to be a stigmatizing condition that inflicts a significant mental and physical toll on afflicted individuals. Patients often grapple with feelings of embarrassment and apprehension about their symptoms and the reactions of others. This, in turn, can profoundly impact their self-esteem, social interactions, intimate relationships, and professional endeavors. The Health-Related Quality of Life (HRQoL) of HH patients is typically lower compared to those without the condition or individuals with other chronic skin ailments (4, 5). Moreover, individuals with HH face an increased risk of developing depression, anxiety, and skin infections. These additional health challenges can further exacerbate the overall disease burden experienced by HH patients, underscoring the multifaceted impact of this condition on both physical and psychological well-being (6, 7).
Bibliometrics is a method of analyzing literature that examines the output and status of publications in a specific field of study from both numerical and qualitative perspectives. During the analysis process, information about authors, keywords, journals, countries, institutions, references, and other relevant aspects of the field can be gathered. Commonly used bibliometric tools, such as VOS viewer (8) and the R package “bibliometrix”, help visualize the results of these analyses. These tools have been widely used in medical fields, including oncology (9), orthopedics (10), and rheumatology (11). However, despite their broad application, no bibliometric studies on hyperhidrosis have been identified. Therefore, the purpose of this study is to conduct a bibliometric analysis of articles on hyperhidrosis published from 2008 to 2023. Pursuant to the findings of the bibliometric analysis, the field of hyperhidrosis stands poised to embark on a range of potential courses of action. In regard to research direction, it is possible to identify current hotspots. In clinical practice, it is possible to optimize protocols based on the data on the efficacy of different treatments, and to pay attention to the use of emerging technologies in treatment. In medical education, it is necessary to adjust the teaching content to cover cutting-edge knowledge and to guide students to conduct scientific research based on the results of analysis. For clinicians, the analysis of data can facilitate the comprehension of the efficacy and safety of various treatment modalities, thereby enabling the optimization of treatment plans. For researchers, the data can facilitate the identification of research hotspots, such as the study of pathogenesis, and the comprehension of research trends. Furthermore, the identification of the core research team can provide a foundation for cooperation and the integration of resources, thereby facilitating in-depth research on hyperhidrosis.
2 Methods
2.1 Data source
On 31 December 2023, a literature search was conducted using the Web of Science Core Collection (WoSCC) database, specifically the Science Citation Index Expanded (SCIE) index. To ensure the validity and relevance of the retrieved data sources, a title search was chosen over subject and abstract searches, given the potential for retrieving a significant amount of irrelevant literature. In accordance with the search strategy and to ensure the quality of the literature, the inclusion of literature was limited to SCIE publications in English. The search was initiated in 2008, considering the trend of focusing on hyperhidrosis research in the last 15 years. The search query employed in this study on the WoSCC database was formulated as TI = (hyperhidrosis) and LA = (English), with the document types limited to “article” and “review”. The study's literature search strategy and screening process are depicted in Figure 1. To mitigate bias from database updates, data retrieval and export were both performed on December 31, 2023. Since this study did not entail animal subjects or experiments, it was deemed unnecessary to seek ethics committee approval.
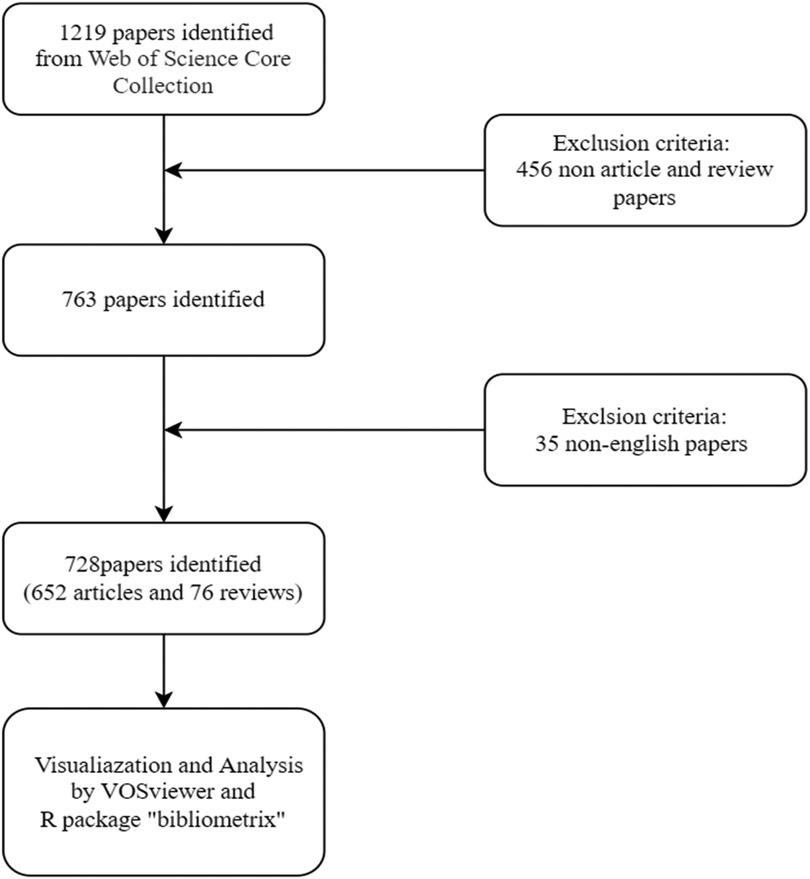
Figure 1. The flowchart for literature screening.
2.2 Statistical analysis
In our study, we utilized various tools for bibliometric analysis, including VOS viewer (version 1.6.20) and the R package “bibliometrix” (version 4.1.3). VOS viewer is a software capable of extracting key information from a vast number of publications and is commonly employed to establish collaboration, co-citation, and co-occurrence networks (12). In our analysis of publications on hyperhidrosis, we employed a range of analytical tools to gain insights. Firstly, a visual representation was created using VOS viewer. In this representation, each node corresponded to an entity, such as a country, institution, journal, or author. The node size and color indicated the quantity and classification of these entities. The thickness of the connecting lines between nodes indicated the level of collaboration or co-citation among the articles. To investigate the evolution of themes in the literature, we employed the R package “bibliometrix,” which enabled us to construct a global distribution network of hyperhidrosis publications. To provide additional context, data on journal quartile and impact factor were obtained from the 2023 Journal Citation Reports.
3 Results
3.1 Publication quantitative analysis
Our search strategy identified 728 studies on hyperhidrosis in the past 15 years, including 652 articles and 76 reviews. On average, approximately 45.5 papers were published annually. The highest number of papers was in 2014 (n = 65), closely followed by 2022 (n = 64). Figure 2 shows a small gap in the number of hyperhidrosis related papers published each year.
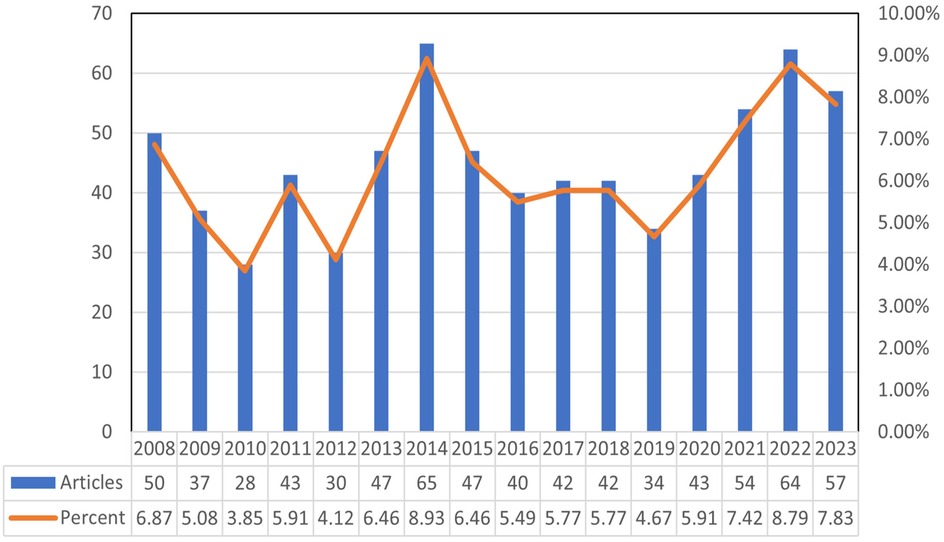
Figure 2. Annual publications from 2008 to 2023.
3.2 Co-cited references
Co-citation is defined as the phenomenon in which two or more documents are simultaneously cited by one or more other documents. Over the past 16 years, a total of 6,801 co-cited references pertaining to hyperhidrosis research have been identified. The ten most frequently co-cited references, each with a co-citation count of at least 70 and one reference exceeding 200 citations, are presented in Table 1. It is particularly noteworthy that Strutton DR's 2004 article from the Journal of the American Academy of Dermatology, which focuses on the prevalence of hyperhidrosis in the United States, emerged as the most frequently cited reference. The construction of a co-citation network diagram was pivotal in visualizing the interconnectedness and relationships among these highly co-cited references. references with a cumulative citation count equal to or higher than 35 were chosen. On the one hand, it aligns with the characteristics and data distribution of hyperhidrosis research; 35 citations approximate the threshold at which high-impact literature can be distinguished from general literature, thereby ensuring the representativeness of the included literature. On the other hand, it aligns with the practices in related fields, facilitating the articulation and comparison with other research. Figure 3 illustrates active co-citation relationships, particularly highlighting associations between references such as “Strutton DR, 2004, J Am Acad Dermatol” (13) with “Hornberger J, 2004, J Am Acad Dermatol”, “Solish N, 2007, Dermatol Surg” (14), and “Doolittle J, 2016, Arch Dermatol Res” (15). In the network map of co-cited references, each node signifies a document, with the lines demarcating the co-citation relationships between documents. That is to say, these lines indicate that the documents in question have been co-cited by the same or more other documents. The thickness of the lines connecting the nodes typically corresponds to the strength of the co-references. That is, the presence of a greater number of co-references results in thicker lines.
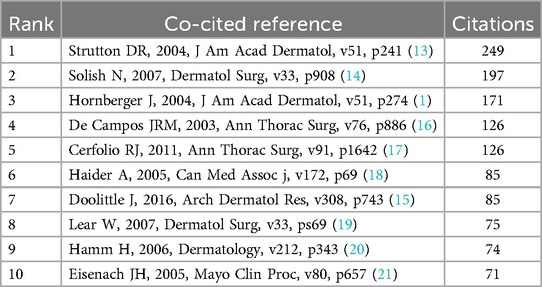
Table 1. The top 10 co-cited references on HH.
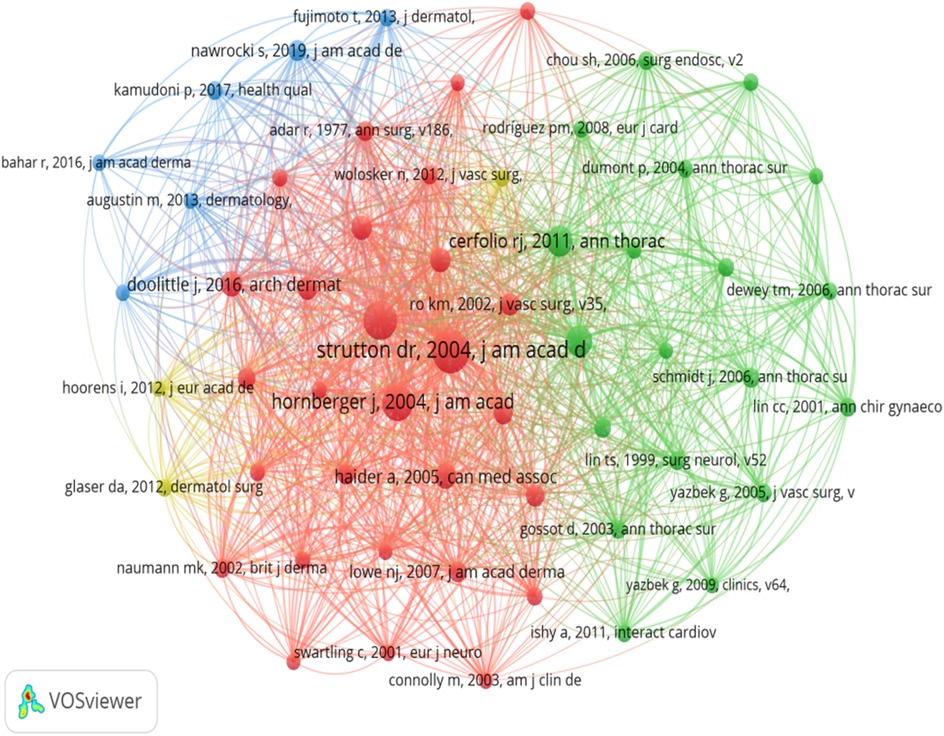
Figure 3. Network map of co-cited references.
3.3 Contributions of countries and institutions
The publications included in the study were sourced from 52 countries and 925 institutions, showcasing a global participation in the research field. Notably, the top 10 contributing countries were geographically diverse, representing Asia, North America, South America, and Europe, with a notable concentration in Asia and Europe. The United States emerged as the leading country in terms of publication output, with 154 papers (21.2%), followed by China with 95 papers (13.0%), Brazil with 77 papers (10.6%), and Germany with 55 papers (7.5%). Remarkably, the combined contributions of China and the United States accounted for nearly a third (33.2%) of all publications analyzed. To provide a comprehensive visualization of the data, we selected 41 countries with a publication count of two or more papers to construct a collaborative network diagram (Figure 4a). This collaborative network highlighted the active engagement and relationships between countries based on research collaboration. Notably, close collaborative ties were observed between China and South Korea, as well as between China and Canada. Similarly, the United States demonstrated active collab-oration with Brazil, Germany, South Korea, and the United Kingdom, indicating a robust network of international research partnerships among the countries analyzed.
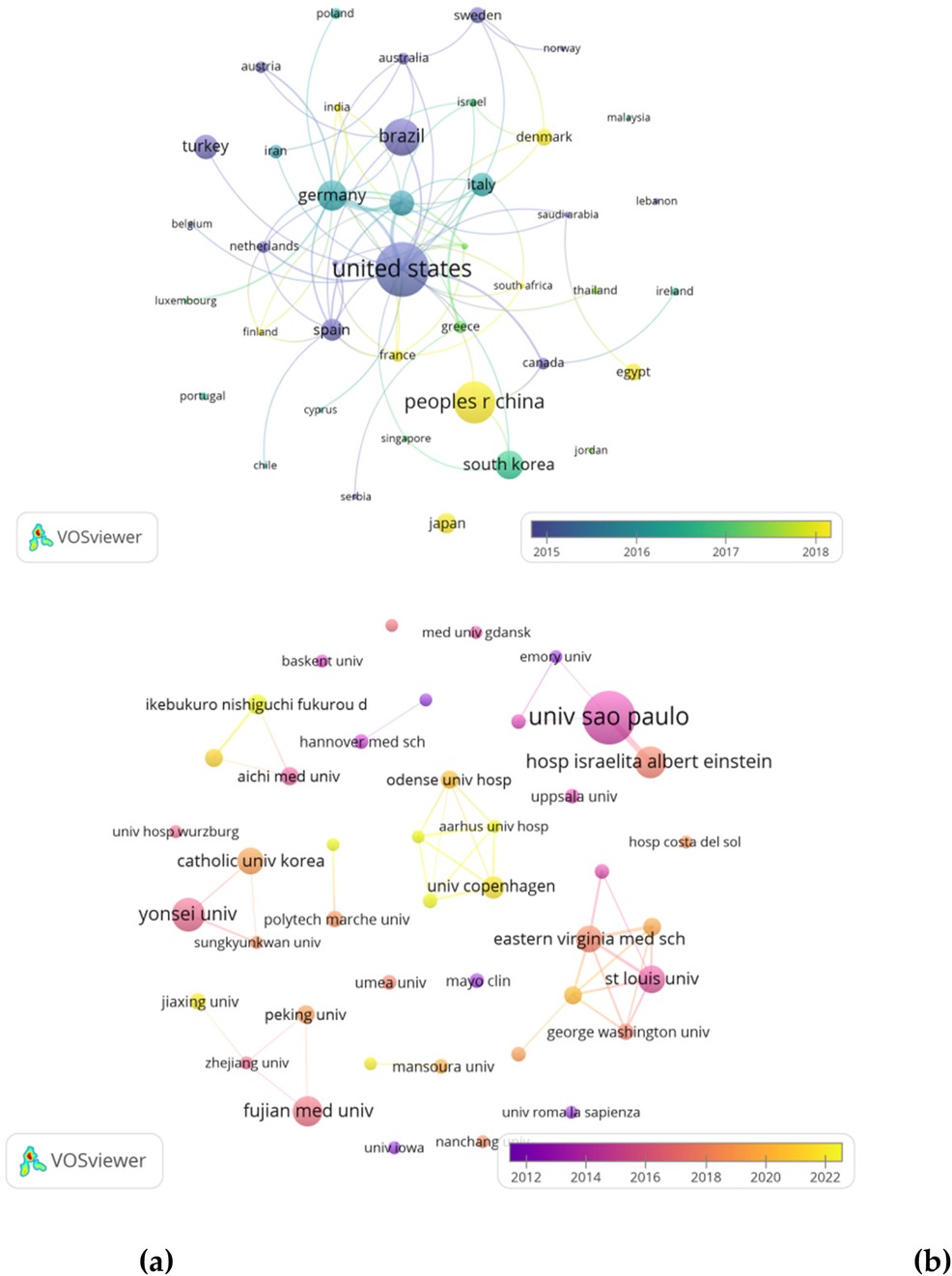
Figure 4. (a) Countries collaboration network visualization map. (b) Institutional collaboration network visualization map.
A total of 925 institutions published papers on hyperhidrosis, with 671 (72.5%) of them contributing only one paper. The top ten institutions, each with a minimum of eight publications, emerged as key players in hyperhidrosis research (Table 2). Leading the pack with 41 articles and a total of 1,124 citations is the University of São Paulo. Following closely were the Albert Einstein Hospital in Israel and Yonsei University, both with 19 publications and more than 250 citations each. To further explore collaborative networks, we focused on 43 institutions that met the criterion of having a minimum of 5 publications. Utilizing this criterion, we constructed a collaborative network based on publication numbers and institutional relationships (Figure 4b). The network analysis revealed a strong collaboration among the University of São Paulo, Albert Einstein Hospital in Israel, and Northwestern University. Moreover, the visual representation in Figure 5 highlighted an active collaboration network involving Fujian Medical University, Zhejiang University, Peking University, and Jiaxing University. The countries/institutional collaboration network visualization map employs a cartographic representation of various types of countries/institutions as nodes and the cooperation relationships between them as connecting lines. The size of the nodes can be adjusted according to specific characteristics or indicators of the countries/institutions. The connecting lines indicate the collaboration relationship between countries/institutions. Different types and intensity of cooperation can be distinguished by the color and thickness of the connecting lines.
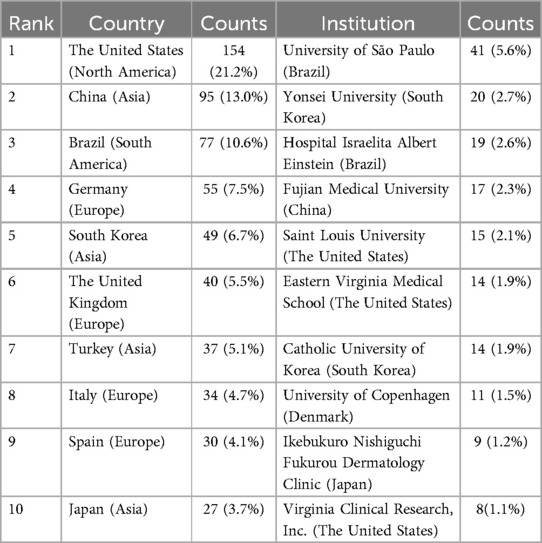
Table 2. Distribution of the Top 10 countries and institutions on HH.
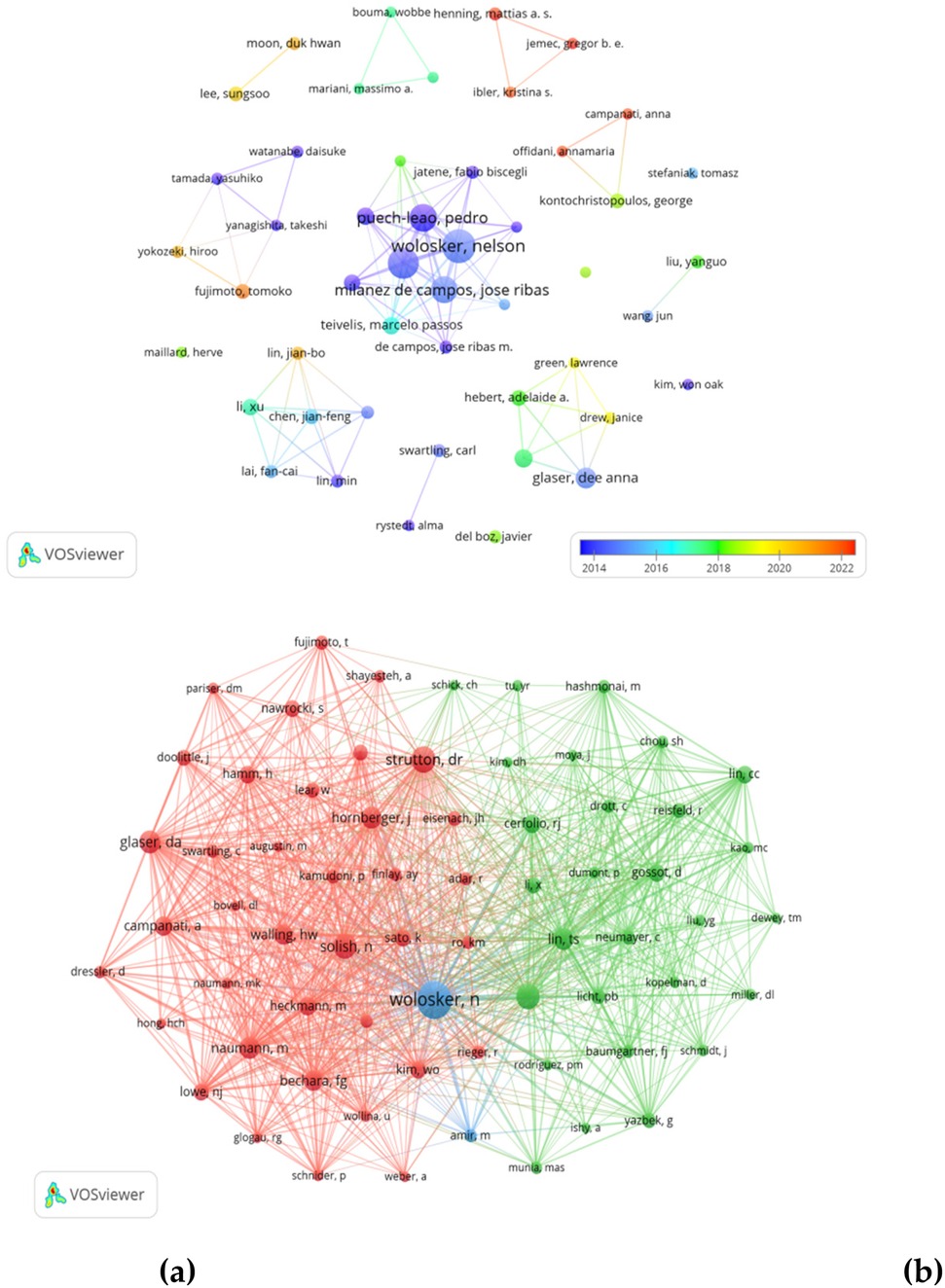
Figure 5. (a) Authorship analyses of authors carried out with VOS viewer. (b) Co-authorship analyses of authors carried out with VOS viewer.
3.4 Authors and co-cited authors
A collaborative network was created based on authors with 4 or more publications (Figure 5a). A total of 2,830 authors participated in hyperhidrosis research, with the top 10 authors publishing more than 10 papers each, as illustrated in Table 3. These authors, namely Nelson Wolosker, Paulo Kauffman, Pedro Puech-Leão, and Jose Ribas Milanez de Campos, were identified as the most influential within the network, due to their significant contributions through the publication of highly relevant papers. The network also revealed close collaborations between several authors. For example, Dee Anna Glaser collaborated closely with David M. Pariser, Adelaide A. Hebert, and Janice Drew. Similarly, Xu Li collaborated with Fancai Lai, Yuanrong Tu, Min Lin, and Jianfeng Chen.
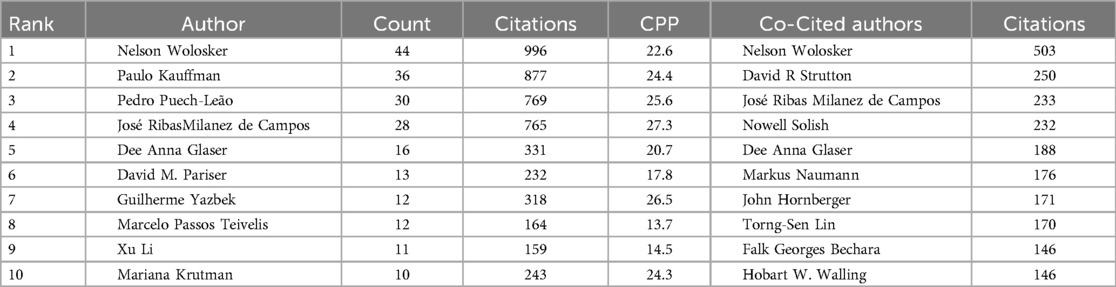
Table 3. Distribution of the top 10 authors and co-cited authors on HH.
After filtering out authors with less than 40 co-citations among the 5,128 co-cited authors, we identified 10 authors who were co-cited more than 145 times, as presented in Table 3. The author with the highest number of co-citations, 503, was Nelson Wolosker, followed by David R. Strutton with 250 co-citations, and José Ribas Milanez de Campos with 233 co-citations. Subsequently, we created a co-citation network, illustrated in Figure 5b, depicting active collaborations among various co-cited authors such as Clotilde Théry and Seon Hee Kim, and Bo Zhang and Ruenn Chai Lai. The network in Figure 6b underscores the interconnected web of collaborations within the academic community.
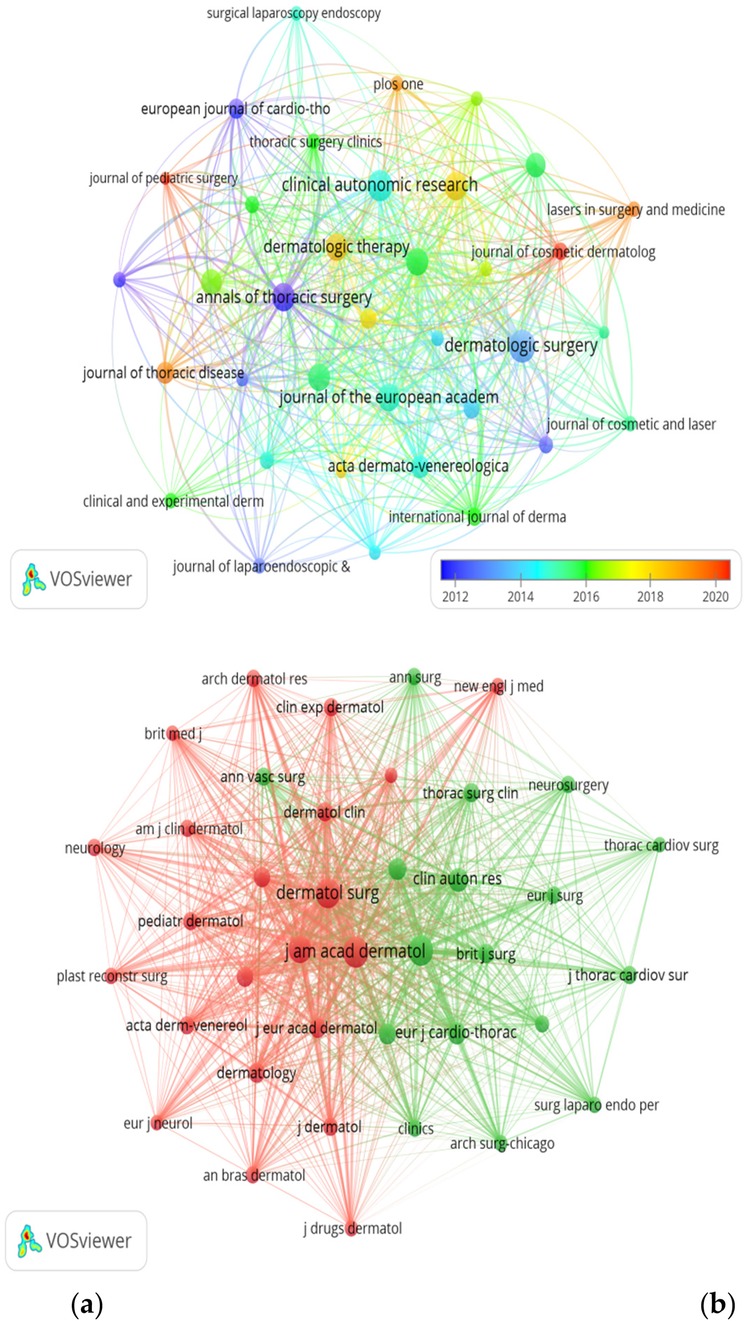
Figure 6. (a) Journals collaboration network visualization map. (b) Co-cited journals collaboration network visualization map.
3.5 Journals and co-cited journals
Of the 226 academic journals that have published papers related to hyperhidrosis, the most prominent publications include Dermatologic Surgery, Clinical Autonomic Research, Annals of Thoracic Surgery, and Journal of Dermatology, with 25 (3.4%), 23 (3.2%), 20 (2.7%), and 20 (2.7%), respectively (Table 4). An analysis of the top 15 journals in terms of impact factors reveals that the Journal of the American Academy of Dermatology has the highest impact factor (IF = 12.8), followed closely by the Journal of the European Academy of Dermatology and Venereology (IF = 9.2). Subsequently, a screening process focused on 36 journals with a minimum of 6 relevant papers was conducted to map out the journal network (Figure 6a), revealing active citation relationships of Dermatologic Surgery with the Journal of the American Academy of Dermatology, Journal of Cosmetic and Laser Therapy, Clinics in Dermatology, and Journal of Dermatological Therapeutics. Regarding co-citations within the top 15 journals, four of them received more than 500 citations, with the Journal of the American Academy of Dermatology leading in the most citations (n = 1,235), followed by Annals of Thoracic Surgery (co-citation = 1,076), Dermatologic Surgery (n = 1,051), and the British Journal of Dermatology (n = 746). In addition to being highly esteemed in the field, the Journal of the American Academy of Dermatology boasts the highest impact factor (IF = 12.8), closely followed by the JAMA Dermatology (IF = 11.0). A co-citation network diagram (Figure 6b) was constructed by identifying journals with a minimum of 100 co-citations, revealing strong positive co-citation connections between the Journal of the American Academy of Dermatology and other influential publications such as Dermatologic Surgery, British Journal of Dermatology, and Annals of Thoracic Surgery.
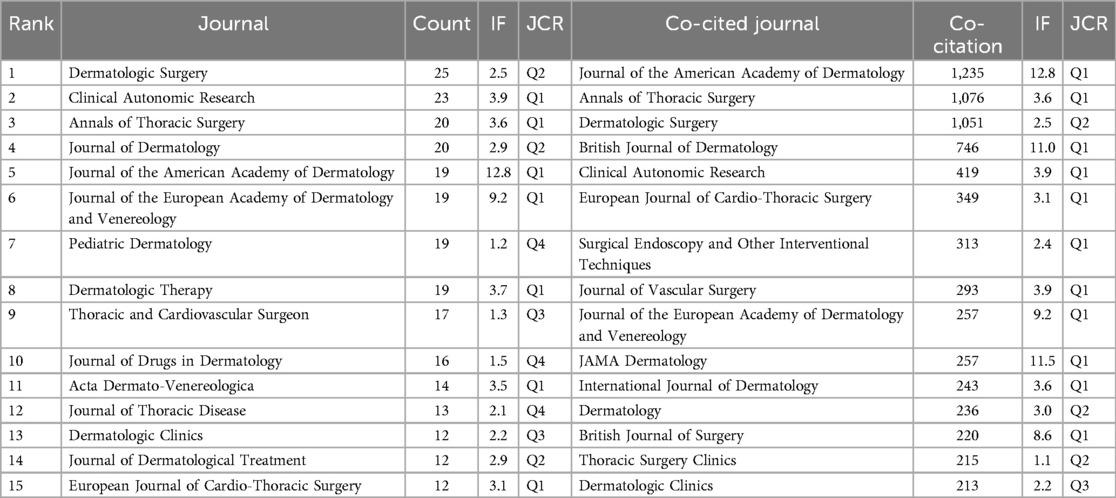
Table 4. Distribution of the top 15 journals and co-cited journals on HH.
3.6 Analysis of keywords
The top 20 high-frequency keywords in hyperhidrosis research, as displayed in Table 5, include sympathectomy, palmar hyperhidrosis, quality of life, and botulinum toxin, which appeared more than 45 times, indicating the primary research directions in hyperhidrosis. Utilizing VOS viewer, we conducted cluster analysis on keywords with seven or more occurrences, as shown in Figure 7. The visualization highlights three distinct clusters symbolizing different research directions. The green cluster encompasses keywords like sympathectomy, palmar hyperhidrosis, compensatory hyperhidrosis, endoscopic thoracic sympathectomy, and thoracoscopy. In contrast, the red cluster comprises keywords such as axillary hyperhidrosis, iontophoresis, oxybutynin, and plantar hyperhidrosis. Lastly, the blue cluster features keywords like quality of life, botulinum toxin, primary hyperhidrosis, and epidemiology. Analyzing the trending topics of the keywords between 2010 and 2019 (Figure 8), the research mainly centered around thoracoscopic surgery, with thoracoscopy and sympathectomy as key themes. However, a shift occurred post-2020, where scholars directed their focus towards postoperative complications and mental health in patients with hyperhidrosis. Key topics of interest include quality of life, safety, compensatory sweating, and depression, indicating the current research hotspots in hyperhidrosis.
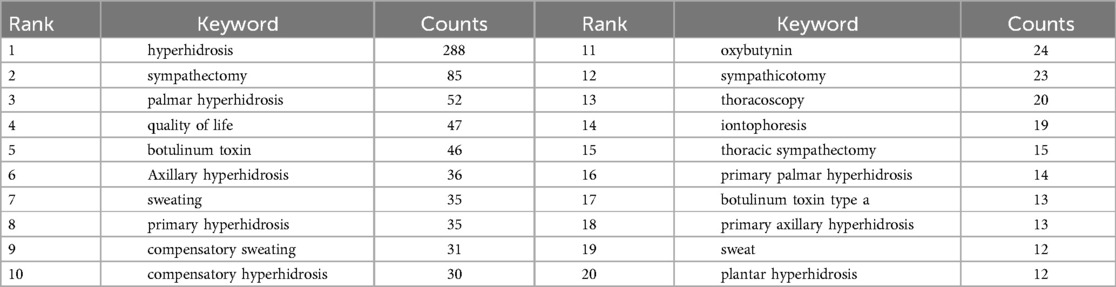
Table 5. Top 20 keywords of HH from 2008 to 2023.
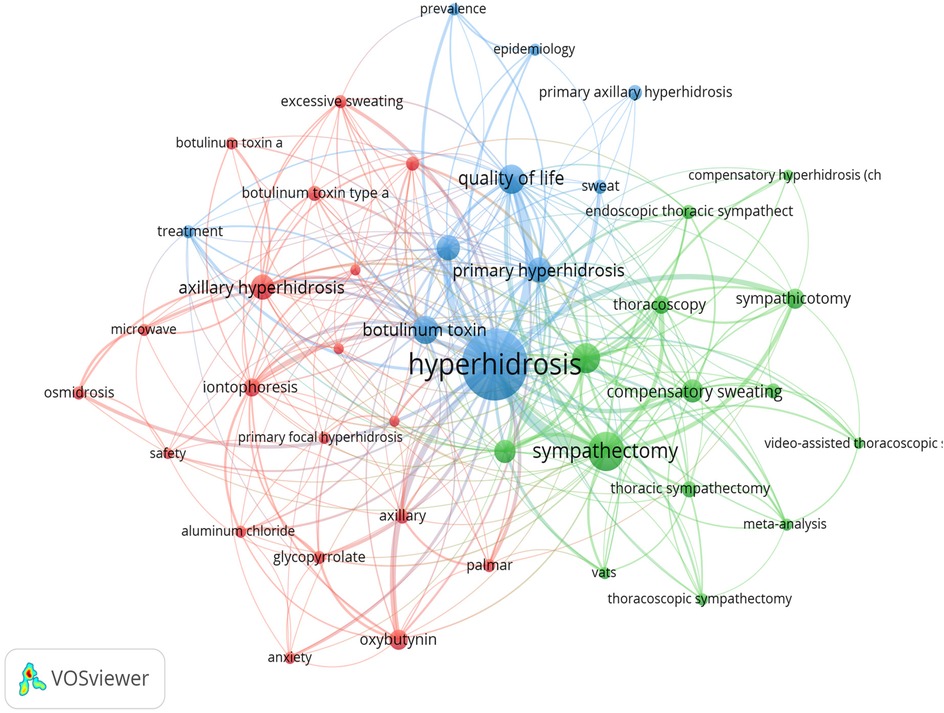
Figure 7. Co-occurrence network map of keywords.
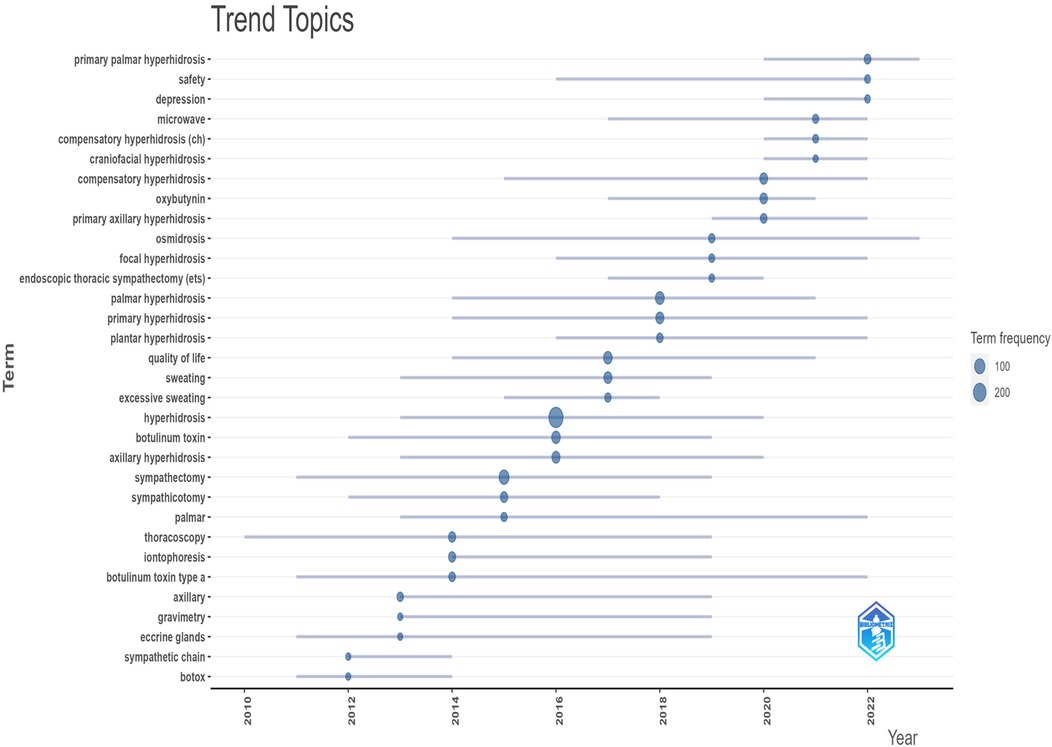
Figure 8. Trending topics of the keywords.
4 Discussion
4.1 Basic information
To gain insight into the current state of research on hyperhidrosis, the study analyzed papers published between 2008 and 2023. The characteristics examined included year of publication, number of citations, country of origin, institution, journal, author, and subject. The ten most prolific publishers were from six different countries. The University of São Paulo stands out as the institution with the highest number of publications (n = 41) and the highest citation frequency (average citations: 26.51 per article) among the selected institutions. It is noteworthy that the Journal of the American Academy of Dermatology was identified as the primary venue for highly cited articles. Moreover, the study highlighted key researchers in the field, with Nelson Wolosker from the University of São Paulo leading the pack as the most published and cited author among those who contributed to the papers. He was closely followed by David R. Strutton from Saint Louis University. Co-cited references, fundamental to a field's research foundation, were also examined in this bibliometric study. A selection of the 10 most co-cited references provided insight into the underpinnings of hyperhidrosis research. The most cited publication in the hyperhidrosis domain was identified as Strutton DR's 2004 article titled “Prevalence of hyperhidrosis in the United States and the impact on patients with axillary hyperhidrosis: results of a national survey”. This study revealed that hyperhidrosis had a more significant impact on the US population than previously recognized, signaling a growing recognition of hyperhidrosis patients among scholars.
The United States has the most articles in hyperhidrosis research and has extensive collaborations with other countries/regions, indicating that the United States is a leader in this field. China has the second highest number of publications and has collaborated with several countries/regions, indicating that China has also made some achievements in hyperhidrosis research and is actively involved in international collaborations. With respect to academic institutions, the University of Pittsburgh has the highest number of publications; however, there is a paucity of collaboration between institutions. Regarding authors, collaboration is dispersed, with the absence of a substantial collaborative team. To promote the advancement of hyperhidrosis research, future efforts should focus on enhancing collaboration among institutions and authors, as well as on integrating available resources.
4.2 Hotspots and fronts
Based on our examination of co-cited literature, high-frequency keywords, and keyword clusters, the research focus in hyperhidrosis primarily centers on pharmacological treatment, surgical treatment, and postoperative complications. In each research hotspot, the most significant research items were botulinum toxin, sympathectomy, and compensatory sweating.
4.2.1 Pharmacological treatment
Topical antiperspirants are often recommended as the initial treatment for mild hyperhidrosis due to their effectiveness in blocking distal sweat glands, leading to the degeneration of epithelial and secretory cells, thereby inhibiting local sweating (22, 23). A randomized controlled trial (RCT) investigated the impact of topical aluminum salts on axillary hyperhidrosis, treating 20 patients with aluminum chloride lotion 20% and aluminum sesquichlorohydrate lotion 20% daily in different axillae. Both treatments significantly reduced the Hyperhidrosis Disease Severity Scale (HDSS) from a mean of 3.5 points to 1.25 points after 2 weeks (24). Glycopyrronium bromide, a topical anticholinergic drug, functions by blocking acetylcholine action to inhibit local sweating. Studies have examined its efficacy and safety in two RCTs. The first RCT with 30 patients demonstrated that daily application of glycopyrronium bromide 1% or 2% reduced sweating by 75% in 87.5% of patients after 8 days, surpassing the placebo group results (25). The second RCT with 171 patients showed a significant reduction in axillary sweating levels with daily administration of 1% glycopyrronium bromide compared to the placebo group (26). Topical oxybutynin, another anticholinergic agent, competitively inhibits acetylcholine, thus reducing local sweating. In an RCT with 53 patients, the application of topical oxybutynin gel 10% twice daily led to a notable improvement in both the Hyperhidrosis Disease Severity Scale and the Dermatology Life Quality Index (27). Botulinum Toxin Type A (BTX type A) Liposomal Cream blocks acetylcholine release, effectively preventing local sweating. In a study involving 20 patients, the daily application of BTX type A liposomal cream proved more effective than placebo in reducing perspiration, as measured by Trans epidermal Water Loss (TEWL) at week 2 and week 8 (28). Furthermore, the efficacy of botulinum toxin in treating hyperhidrosis may be influenced by the dosage administered (29). Recent studies have demonstrated the efficacy of a combination of fractional laser therapy and botulinum toxin in the management of hyperhidrosis (30). Furthermore, the injection of botulinum toxin type A, facilitated by carbon dioxide fractional laser technology, has been shown to extend disease-free survival (31). Iontophoresis, on the other hand, involves exposing the skin to a weak electric current to alter the local pH, block sweat ducts, or inhibit the sympathetic nervous system (32). Sofpironium topical gel is a retrometabolically-designed topical anticholinergic with rapid metabolism, which is associated with reduced side effects and targeted efficacy. For the pooled co-primary endpoint of gravimetric sweat production at treatment end, the treatment group had greater reduction in sweat production (p = 0.0002). Secondary endpoints also showed a statistically significant benefit for sofpironium topical gel vs. control. Treatment was well-tolerated (33, 34). While new treatment options like microwave devices (35), diode lasers (36), and segmented microneedle radiofrequency (FMR) (37) have emerged to address hyperhidrosis, their efficacy and safety require further investigation through rigorous research to provide substantial evidence supporting their effectiveness.
4.2.2 Surgical treatment
Surgical treatment is primarily recommended for hyperhidrosis patients who have not responded to non-surgical treatments or are not suitable for them (38). However, surgery should be considered a second or third-line treatment due to its invasiveness and risk compared to other treatments (39). The present study will compare the efficacy of fractional microneedle radiofrequency with that of botulinum toxin type A in the treatment of primary axillary hyperhidrosis. This condition has been observed to be more amenable to non-surgical treatment (40). The most used surgical methods for treating hyperhidrosis currently are Endoscopic Thoracic Sympathectomy (ETS), CT-guided sympathectomy with radiofrequency (RFS), and local suction (41–43). ETS is the standard surgical treatment for hyperhidrosis of the palms, face, and axillae, with a success rate of over 95% (44). The preferred surgery to treat palmoplantar hyperhidrosis is to excise the sympathoadrenal chain at the R4/R5 levels. In contrast, ETS is less effective in the treatment of axillary hyperhidrosis and has a higher regret rate. Liposuction, the initial surgical procedure for primary localized hyperhidrosis, has now been modified to primarily treat axillary hyperhidrosis. Heidemann et al. compared the use of the localized scraping technique with ETS in treating patients with simple axillary hyperhidrosis, concluding that the former produced better local results and fewer adverse effects (45). However, mild recurrence of symptoms is more common with localized scraping. Therefore, it is recommended to use localized scraping for patients with simple axillary hyperhidrosis and to reduce the use of ETS at the R2–3 or R2–4 levels. Minimally invasive surgery has advanced the treatment of hyperhidrosis in recent years. Radiofrequency ablation is reported as a new treatment option for patients with poor drug control, offering advantages such as less damage, faster recovery, lower cost, and precise efficacy. In a study of 370 patients (740 sides) undergoing CT-guided percutaneous radiofrequency sympathectomy (RFS), RFS was successfully performed on 637 sides, with a technical success rate of 86.1%, indicating that it is a safe and effective method for symptomatic relief in patients with hyperhidrosis (46). A number of studies have been conducted that compare pharmacologic treatment with surgical treatment. The prevailing treatments for axillary hyperhidrosis, characterized by the presence of small sweat gland orifice obstruction and small sweat gland duct atrophy, are Botulinum toxin A (BTX) and microwave thermolysis (MWT). A comparative analysis revealed that 75% of axillae treated with MWT exhibited these characteristics, compared to the 75% observed in BTX-treated axillae (47).
4.2.3 Postoperative complication
Compensatory sweating (CS) is a prevalent issue post-sympathectomy for hyperhidrosis, potentially leading to decreased patient satisfaction. Compensatory sweating, a phenomenon observed in the aftermath of hyperhidrosis surgery, frequently manifests in the chest, abdomen, back, and thighs. The severity of CS varies, affecting up to 98% of patients, with no established standard treatment (48). Existing literature suggests several treatments, albeit with limited data and uncertain outcomes. Factors contributing to CS encompass the extent of sympathetic chain manipulation, degree of denervation, and body mass index. Some studies propose a correlation between patients' psychological traits and CS development (49, 50). Treatment options span non-surgical interventions, such as topical medications, botulinum toxin, systemic anticholinergic drugs, and iontophoresis, alongside surgical interventions like splenectomy and extended sympathectomy. However, empirical support for their efficacy remains inadequate. Han et al. introduced an innovative sympathectomy method targeting R8 or even R12 to mitigate severe CS, exhibiting noteworthy reductions in CS severity with no severe cases or major complications reported (51).
4.3 An examination of the extant research on hyperhidrosis
Recent therapeutic developments for hyperhidrosis encompass a variety of approaches, including gene therapy (currently in the research phase but showing considerable potential), novel anticholinergics (e.g., sofpironium bromide gel, approved for specific patient populations), fractional microneedle radiofrequency (FMRF), radiofrequency ablation (RFAB), and CT-guided radiofrequency thermocoagulation (CT-thermo-coagulation). These methods have demonstrated a reduction in trauma, accelerated recovery, and enhanced effectiveness (1). The broad potential for interdisciplinary applications is evident. For instance, the convergence of dermatology and genetics facilitates a more nuanched understanding of pathogenesis, thereby allowing for customized treatment approaches. Similarly, the collaboration between molecular biology and clinical medicine fosters the development of novel therapeutic agents and diagnostic techniques. Additionally, the integration of psychology and medicine leads to comprehensive treatment strategies that address both psychological and physiological dimensions of health (2). In the domain of policy evolution, there will be an ongoing refinement of drug regulatory policies, leading to enhanced approval processes and standards. Additionally, there will be a regulation of the use of emerging minimally invasive technologies under medical technology access policies. Furthermore, health insurance policies are likely to undergo adjustments in response to the development of therapeutic approaches and various other factors. The effective incorporation of tools in reimbursement will serve to enhance patient access.
As medical technology continues to advance, such as with gene technology and nanotechnology, new opportunities for research on hyperhidrosis may emerge. For instance, through genetic research, we can gain a more profound understanding of the pathogenesis of hyperhidrosis, which will provide a theoretical foundation for the development of novel treatments. Moreover, by leveraging nanotechnology, we can engineer a novel drug delivery system to enhance the efficacy of pharmaceutical therapy. Moreover, the future of hyperhidrosis research will be marked by an emphasis on multidisciplinary collaboration and the integration of knowledge from multiple fields, including medicine, biology, and psychology, to provide a comprehensive understanding of the etiology, pathogenesis, treatment, and prevention of hyperhidrosis.
5 Conclusions
Currently, the leading countries in terms of the number of articles, researchers, and institutions are the United States and China. Dermatologic Surgery is projected to have the largest number of published papers from 2008 to 2023. The most common academic focus within this field continues to be the treatment of hyperhidrosis and the management of compensatory hyperhidrosis. Despite this academic dominance, there is still a pressing need to enhance collaboration and exchange between different countries and institutions.
Author contributions
ZT: Data curation, Writing – original draft. CZ: Writing – original draft. XX: Writing – original draft. MY: Writing – original draft. HN: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Zhejiang Multidisciplinary Innovation Team of Traditional Chinese Medicine for Diagnosis and Treatment of Elderly Headache and Vertigo (2022-19), Zhejiang Clinovation Pride (CXTD202502014), and Zhejiang Provincial Clinical Key Specialties-Anesthesiology (2023-ZJZK-001).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Hornberger J, Grimes K, Naumann M, Glaser DA, Lowe NJ, Naver H, et al. Recognition, diagnosis, and treatment of primary focal hyperhidrosis. J Am Acad Dermatol. (2004) 51(2):274–86. doi: 10.1016/j.jaad.2003.12.029
2. Shih CJ, Wu JJ, Lin MT. Autonomic dysfunction in palmar hyperhidrosis. J Auton Nerv Syst. (1983) 8(1):33–43. doi: 10.1016/0165-1838(83)90021-8
3. Lai FC, Tu YR, Li YP, Li X, Lin M, Chen JF, et al. Nation wide epidemiological survey of primary palmar hyperhidrosis in the People's Republic of China. Clin Auton Res. (2015) 25(2):105–8. doi: 10.1007/s10286-014-0259-5
4. Henning MAS, Ibler KS, Loft I, Ostrowski SR, Erikstrup C, Nielsen KR, et al. The health-related quality of life in hyperhidrosis and co-morbidities. Qual Life Res. (2022) 31(8):2331–40. doi: 10.1007/s11136-022-03108-z
5. Kjeldstrup Kristensen J, Grejsen D, Swartling C, Bygum A. In hyperhidrosis quality of life is even worse than in acne, eczema, or psoriasis. A comparison of Skindex-16 and Dermatology Life Quality Index (DLQI). Int J Dermatol. (2020) 59(11):e392–3. doi: 10.1111/ijd.15164
6. Henning MAS, Ibler KS, Ostrowski SR, Erikstrup C, Nielsen KR, Bruun MT, et al. Hyperhidrosis and the risk of being treated for skin infections. J Dermatolog Treat. (2022) 33(4):2263–9. doi: 10.1080/09546634.2021.1944971
7. Bahar R, Zhou P, Liu Y, Huang Y, Phillips A, Lee TK, et al. The prevalence of anxiety and depression in patients with or without hyperhidrosis (HH). J Am Acad Dermatol. (2016) 75(6):1126–33. doi: 10.1016/j.jaad.2016.07.001
8. Arruda H, Silva ER, Lessa M, Proença D Jr, Bartholo R. VOSviewer and bibliometrix. J Med Libr Assoc. (2022) 110(3):392–5. doi: 10.5195/jmla.2022.1434
9. Shi S, Gao Y, Liu M, Bu Y, Wu J, Tian J, et al. Top 100 most-cited articles on exosomes in the field of cancer: a bibliometric analysis and evidence mapping. Clin Exp Med. (2021) 21(2):181–94. doi: 10.1007/s10238-020-00624-5
10. Wu H, Cheng K, Tong L, Wang Y, Yang W, Sun Z. Knowledge structure and emerging trends on osteonecrosis of the femoral head: a bibliometric and visualized study. J Orthop Surg Res. (2022) 17(1):194. doi: 10.1186/s13018-022-03068-7
11. Wu H, Cheng K, Guo Q, Yang W, Tong L, Wang Y, et al. Mapping knowledge structure and themes trends of osteoporosis in rheumatoid arthritis: a bibliometric analysis. Front Med (Lausanne). (2021) 8:787228. doi: 10.3389/fmed.2021.787228
12. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84(2):523–38. doi: 10.1007/s11192-009-0146-3
13. Strutton DR, Kowalski JW, Glaser DA, Stang PE. US prevalence of hyperhidrosis and impact on individuals with axillary hyperhidrosis: results from a national survey. J Am Acad Dermatol. (2004) 51(2):241–8. doi: 10.1016/j.jaad.2003.12.040
14. Solish N, Bertucci V, Dansereau A, Hong HC, Lynde C, Lupin M, et al. A comprehensive approach to the recognition, diagnosis, and severity-based treatment of focal hyperhidrosis: recommendations of the Canadian Hyperhidrosis Advisory Committee. Dermatol Surg. (2007) 33(8):908–23. doi: 10.1111/j.1524-4725.2007.33192.x
15. Doolittle J, Walker P, Mills T, Thurston J. Hyperhidrosis: an update on prevalence and severity in the United States. Arch Dermatol Res. (2016) 308(10):743–9. doi: 10.1007/s00403-016-1697-9
16. de Campos JR, Kauffman P, Werebe Ede C, Andrade Filho LO, Kusniek S, Wolosker N, et al. Quality of life, before and after thoracic sympathectomy: report on 378 operated patients. Ann Thorac Surg. (2003) 76(3):886–91. doi: 10.1016/S0003-4975(03)00895-6
17. Cerfolio RJ, Campos D, Bryant JR, Connery AS, Miller CP, DeCamp DL, et al. The society of thoracic surgeons expert consensus for the surgical treatment of hyperhidrosis. Ann Thorac Surg. (2011) 91(5):1642–8. doi: 10.1016/j.athoracsur.2011.01.105
18. Haider A, Solish N. Focal hyperhidrosis: diagnosis and management. Can Med Assoc j. (2005) 172(1):69–75. doi: 10.1503/cmaj.1040708
19. Lear W, Kessler E, Solish N, Glaser DA. An epidemiological study of hyperhidrosis. Dermatol Surg. (2007) 33(1 Spec No.):S69–75. doi: 10.1111/j.1524-4725.2006.32334.x
20. Hamm H, Naumann MK, Kowalski JW, Kütt S, Kozma C, Teale C. Primary focal hyperhidrosis: disease characteristics and functional impairment. Dermatology. (2006) 212(4):343–53. doi: 10.1159/000092285
21. Eisenach JH, Atkinson JL, Fealey RD. Hyperhidrosis: evolving therapies for a well-established phenomenon. Mayo Clin Proc. (2005) 80(5):657–66. doi: 10.4065/80.5.657
22. Wade R, Llewellyn A, Jones-Diette J, Wright K, Rice S, Layton AM, et al. Interventional management of hyperhidrosis in secondary care: a systematic review. Br J Dermatol. (2018) 179(3):599–608. 29573391
23. Gregoriou S, Sidiropoulou P, Kontochristopoulos G, Rigopoulos D. Management strategies of palmar hyperhidrosis: challenges and solutions. Clin Cosmet Investig Dermatol. (2019) 12:733–44. doi: 10.2147/CCID.S210973
24. Thianboonsong T, Kanokrungsee S, Paichitrojjana A, Udompataikul M, Kamanamool N, Rojhirunsakool S. Efficacy and tolerability of 20% aluminum sesquichlorohydrate vs 20% aluminum chloride for the treatment of axillary hyperhidrosis: a randomized controlled trial. Dermatol Ther. (2020) 33(6):e14354. doi: 10.1111/dth.14354
25. Masur C, Soeberdt M, Kilic A, Knie U, Abels C. Safety and efficacy of topical formulations containing 0·5, 1 and 2% glycopyrronium bromide in patients with primary axillary hyperhidrosis: a randomized, double-blind, placebo-controlled study. Br J Dermatol. (2020) 182(1):229–31. doi: 10.1111/bjd.18234
26. Abels C, Soeberdt M, Kilic A, Reich H, Knie U, Jourdan C, et al. A glycopyrronium bromide 1% cream for topical treatment of primary axillary hyperhidrosis: efficacy and safety results from a phase IIIa randomized controlled trial. Br J Dermatol. (2021) 185(2):315–22. doi: 10.1111/bjd.19810
27. Artzi O, Loizides C, Zur E, Sprecher E. Topical oxybutynin 10% gel for the treatment of primary focal hyperhidrosis: a randomized double-blind placebo-controlled split area study. Acta Derm Venereol. (2017) 97(9):1120–4. doi: 10.2340/00015555-2731
28. Lueangarun S, Sermsilp C, Tempark T. Topical Botulinum toxin type A liposomal cream for primary axillary hyperhidrosis: a double-blind, randomized, split-site, vehicle-controlled study. Dermatol Surg. (2018) 44(8):1094–101. doi: 10.1097/DSS.0000000000001532
29. Antón Andrés MJ, Candau Pérez ED, Bermejo de la Fuente MP. Treatment of primary axillary hyperhidrosis with two doses of Botulinum toxin A-observational study. Toxins (Basel). (2024) 16(7):320. doi: 10.3390/toxins16070320
30. Elshabory O, Mohamed HAK, Zaky M, Elsaie ML. Comparative study between fractional laser assisted drug delivery of botulinum toxin versus botulinum toxin injection in primary palmar and axillary hyperhidrosis. Arch Dermatol Res. (2025) 317(1):241. doi: 10.1007/s00403-024-03715-5
31. Elsayed M, Ghonemy S, Sheneeb N, Elradi M. Fractional CO(2) laser-assisted delivery of botulinum toxin-A versus aluminum chloride in treatment of primary palmar hyperhidrosis. Photodermatol Photoimmunol Photomed. (2024) 40(6):e13006. doi: 10.1111/phpp.13006
32. Gollins CE, Carpenter A, Steen C, Bulinski H, Mahendran R. A retrospective analysis of the use of tap water iontophoresis for focal hyperhidrosis at a district general hospital: the patients’ perspective. J Dermatolog Treat. (2019) 30(7):724–6. doi: 10.1080/09546634.2019.1569751
33. Pariser D, Glaser DA, Rosso D, Bhatia J, Hooper N, Nestor D, et al. Sofpironium topical gel, 12.45%, for the treatment of axillary hyperhidrosis: pooled efficacy and safety results from 2 phase 3 randomized, controlled, double-blind studies. J Am Acad Dermatol. (2025) (25):393–7. doi: 10.1016/j.jaad.2025.02.086
34. Odat RM, Yousef Aldalati A, Hammadeh BM, Mohammad Hussein A, Idrees M, Marzouk H, et al. Efficacy and safety of sofpironium in treatment of primary hyperhidrosis: a systematic review. J Dermatolog Treat. (2025) 36(1):2441258. doi: 10.1080/09546634.2024.2441258
35. Kaminaka C, Mikita N, Inaba Y, Kunimoto K, Okuhira H, Jinnin M, et al. Clinical and histological evaluation of a single high energy microwave treatment for primary axillary hyperhidrosis in Asians: a prospective, randomized, controlled, split-area comparative trial. Lasers Surg Med. (2019) 51(7):592–9. doi: 10.1002/lsm.23073
36. Leclère FM, Moreno-Moraga J, Alcolea JM, Vogt PM, Royo J, Cornejo P, et al. Efficacy and safety of laser therapy on axillary hyperhidrosis after one year follow-up: a randomized blinded controlled trial. Lasers Surg Med. (2015) 47(2):173–9.
37. Rummaneethorn P, Chalermchai T. A comparative study between intradermal botulinum toxin A and fractional microneedle radiofrequency (FMR) for the treatment of primary axillary hyperhidrosis. Lasers Med Sci. (2020) 35(5):1179–84. doi: 10.1007/s10103-020-02958-8
38. Housset M, Dessertenne G, Marchand E, Daligault M, Maillard H. A multicentre retrospective study of lumbar sympathectomy for plantar hyperhidrosis: satisfaction and postoperative complications. Clin Exp Dermatol. (2024) 49(3):241–6. doi: 10.1093/ced/llad373
39. Wimmer F, Ramic A, Nolte JP, Djedovic G, Dietl M. Evaluation of efficacy and safety of miraDry® procedure in the treatment of primary axillary hyperhidrosis. Aesthetic Plast Surg. (2025):e1–8. doi: 10.1007/s00266-024-04558-1
40. Eid RO, Shaarawi E, Hegazy RA, Hafez V. Long-term efficacy of fractional microneedle radiofrequency versus botulinum toxin-A in primary axillary hyperhidrosis: a randomized controlled trial. Lasers Med Sci. (2024) 39(1):177. doi: 10.1007/s10103-024-04115-x
41. Guirguis P, Girgis M, Abu Arab W, Keshk S, Ramadan AM. Comparing compensatory sweating after video-assisted thoracoscopic sympathectomy: (T2-3) versus (T2-4) levels for treating palmar hyperhidrosis. Cureus. (2024) 16(11):e74077. doi: 10.7759/cureus.74077
42. Wu X, Wu N, Hu W, Hu Y. Comparing the 5-year effectiveness of R4 and R4+5 thoracoscopic sympathectomy for palmoplantar hyperhidrosis: a cohort study. Asian J Surg. (2024):1–2. doi: 10.1016/j.asjsur.2024.09.117
43. Fan H, Xu P, Zhang E, Meng X, Xia J, Fei Y, et al. Risk factors affecting the outcomes of CT-guided radiofrequency thermocoagulation of the T3 sympathetic nerve in the treatment of craniofacial hyperhidrosis. Ther Clin Risk Manag. (2024) 20:465–72. doi: 10.2147/TCRM.S463025
44. Gossot D, Galetta D, Pascal A, Debrosse D, Caliandro R, Girard P, et al. Long-term results of endoscopic thoracic sympathectomy for upper limb hyperhidrosis. Ann Thorac Surg. (2003) 75(4):1075–9. doi: 10.1016/S0003-4975(02)04657-X
45. Heidemann E, Licht PB. A comparative study of thoracoscopic sympathicotomy versus local surgical treatment for axillary hyperhidrosis. Ann Thorac Surg. (2013) 95(1):264–8. doi: 10.1016/j.athoracsur.2012.08.103
46. Han Z, Rui M, Ni C, Zhu J, Xu L, Yao M. The success rate and associated risk factors of CT-guided percutaneous radiofrequency sympathectomy in the treatment of primary hyperhidrosis: a retrospective observational trial. J Clin Neurosci. (2023) 118:81–9. doi: 10.1016/j.jocn.2023.10.010
47. Grove GL, Jacobsen K, Maartensson NL, Haedersdal M. Subclinical effects of botulinum toxin A and microwave thermolysis for axillary hyperhidrosis: a descriptive study with line-field confocal optical coherence tomography and histology. Exp Dermatol. (2024) 33(6):e15110. doi: 10.1111/exd.15110
48. Wolosker N, Milanez de Campos JR, Fukuda JM. Management of compensatory sweating after sympathetic surgery. Thorac Surg Clin. (2016) 26(4):445–51. doi: 10.1016/j.thorsurg.2016.06.009
49. Wang HY, Zhu YJ, Liu J, Li LW, Liu YH. The relationship between preoperative psychological evaluation and compensatory sweating. J Cardiothorac Surg. (2018) 13(1):42. doi: 10.1186/s13019-018-0728-3
50. Behinaein P, Gavagan K, Waitzman J, Pourang A, Potts G. A review of the etiologies and key clinical features of secondary hyperhidrosis. Am J Clin Dermatol. (2025) 26(1):97–108. doi: 10.1007/s40257-024-00908-6
Keywords: hyperhidrosis, bibliometric, hotspots, VOS viewer, compensatory sweating
Citation: Zhi T, Zhao C, Xiang X, Yao M and Ni H (2025) Global research trends and hotspots of hyperhidrosis: a bibliometric analysis (2008–2023). Front. Surg. 12:1559951. doi: 10.3389/fsurg.2025.1559951
Received: 13 January 2025; Accepted: 8 April 2025;
Published: 22 April 2025.
Edited by:
H. Volkan Kara, Istanbul University-Cerrahpasa, TürkiyeReviewed by:
David Andrew Low, Liverpool John Moores University, United KingdomZheng Xiaodong, Shandong University of Traditional Chinese Medicine, China
Copyright: © 2025 Zhi, Zhao, Xiang, Yao and Ni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ming Yao, anh5YW9taW5nQHpqeHUuZWR1LmNu; Huadong Ni, aHVhZG9uZ25pQDEyNi5jb20=