 Susana González-Suárez
Susana González-Suárez María Grao Roca
María Grao Roca Juan-Camilo Vivas5
Juan-Camilo Vivas5- 1Department of Surgery, Universitat Autònoma de Barcelona, Barcelona, Spain
- 2Department of Anesthesia and Intensive Care, University Hospital Vall d'Hebron, Barcelona, Spain
- 3Cardiovascular Diseases Research Group, Vall d'Hebron Institut de Recerca (VHIR), Barcelona, Spain
- 4Department of Anesthesia and Intensive Care, University Hospital Vall d´Hebron, Barcelona, Spain
- 5Department of Thoracic Surgery and Lung Transplant, University Hospital Vall d´Hebron, Barcelona, Spain
- 6Department of Surgery, Universitat Autònoma de Barcelona, Barcelona, Spain
The aim of this study was to show the efficacy described in the scientific literature of lung ultrasound (LU) during video-assisted thoracic surgery (VATS) to determine the location and characterization of pulmonary nodules. The results showed that intraoperative LU is especially useful in localizing lung lesions by VATS with a sensitivity close to 100%. It was also shown to be useful in planning very precise lung resections, reducing the resection of healthy lung tissue. Although general criteria could be established for the degree of benignity/malignancy of lung lesions based on the ultrasound patterns obtained, the great variability observed in these patterns does not offer sufficient guarantees to make a reliable diagnosis. In this sense, the application of Doppler ultrasound or the utilization of Intraoperative Contrast-Enhanced Ultrasound (Io-CEUS) in a completely collapsed lung can be advantageous for the accurate localization and characterization of pulmonary lesions. Even so, at present, definitive confirmation of the nature of lung lesions usually requires biopsy and histopathological study. The development of artificial intelligence algorithms that integrate the results of histological analyses with various types of ultrasonographic patterns (based on pulmonary aeration obtained, as well as Doppler and Io-CEUS records) will likely represent the future of ultrasonographic differentiation of these lesions.
Introduction
Since its introduction in 1990, video-assisted thoracic surgery (VATS) has become increasingly prevalent. This minimally invasive technique involves accessing the thoracic cavity through an incision of less than 4 cm, enabling visualization and endoscopic instrumentation of the lung without the need to sever muscles, as is necessary in traditional thoracotomy. Due to its less invasive nature, VATS offers several advantages, including reduced morbidity (1), shorter hospital stays (1), diminished postoperative pain, and improved oncologic outcomes (2), particularly in patients with limited respiratory reserve. Despite these benefits, VATS requires specialized training (3) due to the constrained surgical access and challenges in locating pulmonary lesions, especially when dealing with underlying pulmonary conditions, small lesions, or those situated in deep, basomedial, or postero-medial regions (4, 5).
In this context, lung ultrasonography has proven to be a valuable tool (6, 7). The use of ultrasound is expanding across various medical fields, including cardiology (8), internal medicine (9), anesthesiology, and intensive care (10). It is also instrumental in examining pleural and subpleural lesions, guiding the placement of thoracic drains (11, 12), and performing percutaneous needle biopsies of the lung (13, 14). In the postoperative setting, ultrasound has reduced the reliance on x-rays (15) by effectively detecting atelectasis, pleural effusion, pneumonia, pneumothorax, and diaphragmatic dysfunction with sensitivities of 88%, 100%, 88%, 100%, and 91%, respectively, and specificities of 92%, 100%, 86%, 82%, and 91% (16–20).
During VATS, ultrasonography (VATS-US) has been introduced to locate and differentiate pulmonary nodules and their adjacent structures (21, 22). Since it can be performed directly on the lung surface through the thoracoscopic ports, it provides a direct and detailed visualization of the lung parenchyma, as the probe is in direct contact with the lung and free from the interference of air in the lung tissue, provided a complete lung collapse is achievable (23). Moreover, no complications have been reported in the use of intraoperative LU for identifying pulmonary nodules. However, other techniques, such as the insertion of a hooked wire or metal coils, technetium-99-labeled human serum albumin microspheres, and radiotracer-guided thoracoscopic biopsy, while achieving success rates of up to 100% and reducing the need for open thoracotomy in more than 50% of cases, are associated with notable complications including air embolism, pneumothorax, and intraparenchymal hemorrhage (24–30). In addition, technical difficulties may arise during the execution of these pre-surgical tests. Issues such as failed hook wire placement, migration of the coil between its insertion and the time of surgical resection (occurring in 3%–10% of cases), or the injection of methylene blue far from the lung lesion, can result in unsuccessful nodule localization if displacements exceed 10 mm (28, 31–33).
To evaluate the efficacy of VATS-US in the localization and characterization of pulmonary nodules, and to identify potential measures for improving nodule identification rates, a comprehensive literature search was conducted using the Medical Literature Analysis and Retrieval System Online (MEDLINE-PubMed), EMBASE (Elsevier), and the Web of Science Core Collection (Clarivate). This review assessed variables including the ultrasonographic patterns of pulmonary nodules, the size and depth of the nodules, the types of ultrasonographic probes used, the results of Doppler and Intraoperative Contrast-Enhanced Ultrasound (Io-CEUS recordings, the correlation between ultrasonographic findings and lesions identified via CT and/or histological analysis, as well as the limitations of the ultrasonographic technique.
Efficacy of VATS-US for the localization of pulmonary nodules
Comparison of VATS-US with traditional methods of palpation and visual inspection for pulmonary nodule localization
Most solid pulmonary nodules can be palpated and/or visualized. Manual palpation of lung lesions is the oldest method used and can achieve a 100% success rate in detecting solid lung metastases during conventional thoracotomies, although it carries a false-positive rate of 13–48.5% (34). It can even detect lung metastases that were not identified by preoperative CT scans (35). However, manual palpation presents challenges during VATS and is rarely used as the sole technique for localizing pulmonary nodules. Instead, it is typically combined with other techniques, such as intraoperative ultrasound. According to the literature, the percentage of lung lesions detected by ultrasound during VATS ranges from 76% to 100% (20, 36, 37). Some authors have reported detecting more nodules using VATS-US than with VATS alone or simple manual palpation (37, 38). Kondo et al. (23) also achieved a higher sensitivity with lung ultrasonography (93%) compared to palpation (40%). Khereba et al. (39) found that, during VATS, 93.5% of pulmonary nodules were detected by ultrasound, compared to 27% detected by visual inspection, 40% identified by digital palpation, and 38% by palpation with instrumental slide techniques. The sensitivity of VATS-US was 93%, with a positive predictive value of 100%. In 20 cases (43%), pulmonary nodules were not identified by any of the traditional methods and were only detected by VATS-US, thus avoiding conversion to thoracotomy or lobectomy (39). Hou et al. (40) demonstrated successful localization of pulmonary nodules in 97% of patients who underwent intrapulmonary ultrasonography, compared to only 48.5% in those who underwent lung palpation (p < 0.05). This success rate with intrathoracic ultrasonography is comparable to that reported by other authors using alternative methods for nodule identification, such as CT-guided metal hook insertion, methylene blue or isotope injection, and intraoperative tracheal endoscopic magnetic navigation (40–43).
Overall, it should be noted that although VATS-US adds an additional 10–15 minutes to the surgery, its use could reduce the need for conversion to thoracotomy by up to 59% of cases (44–48). Furthermore, compared to the manual palpation method, intraoperative ultrasonography demonstrated an even shorter time for lesion identification, with an average of 7.09 ± 1.80 minutes for ultrasonography vs. 9.67 ± 2.62 minutes for palpation (P < 0.05), thus improving the feasibility of minimally invasive surgery (39). Some authors, such as Hou et al. (40), considered the palpation method to have failed if it took more than 12 minutes to identify the lesions. The rationale for this decision was based on various factors, beyond simply avoiding prolonged surgical time. In their experience, the likelihood of detecting lung lesions decreased as palpation time increased, and there is scientific evidence indicating that excessive surgical duration elevates the risk of tumor metastasis (49, 50).
Effectiveness of pulmonary ultrasound depending on the size and depth of pulmonary nodules
Thanks to VATS-US, some authors have successfully identified very small pulmonary nodules, even those smaller than 2 mm, as well as deeply located nodules (39, 45). Khereba et al. (39) identified peripheral nodules (not in contact with the visceral pleural line on CT) as small as 2 mm. Other authors, such as Piolanti et al. (7), although able to detect two small nodules that had not been identified by helical CT, were unable to identify a very peripheral subpleural lesion measuring 3 mm in diameter. Therefore, when a lesion is located very peripherally, its detection with ultrasound may be missed. In such cases, the use of high-frequency ultrasound transducers could prove helpful, in addition to visual inspection of the lung surface by the surgeon. However, in general, most peripheral pulmonary nodules can be identified.
Other authors have also been able to identify small nodules located intraparenchymally within the lung. In ex vivo samples, Fiorelli et al. (51) detected nodules up to 7 mm in diameter at a depth of 5 mm. Using VATS-US, Gambardella et al. (52) identified deep subcentimeter intraparenchymal nodules (less than 1 cm in diameter, with a mean size of 7.3 ± 1.2 mm) located at a distance of 16.2 ± 2.4 mm from the visceral pleura. Taurchini et al. (46) also demonstrated a high sensitivity (100%) of LU in detecting small pulmonary nodules less than 2 cm in size and centrally located (53). Furthermore, LU was even able to identify small nodules that had not been previously detected by preoperative CT (7, 37, 47, 48) (Table 1).
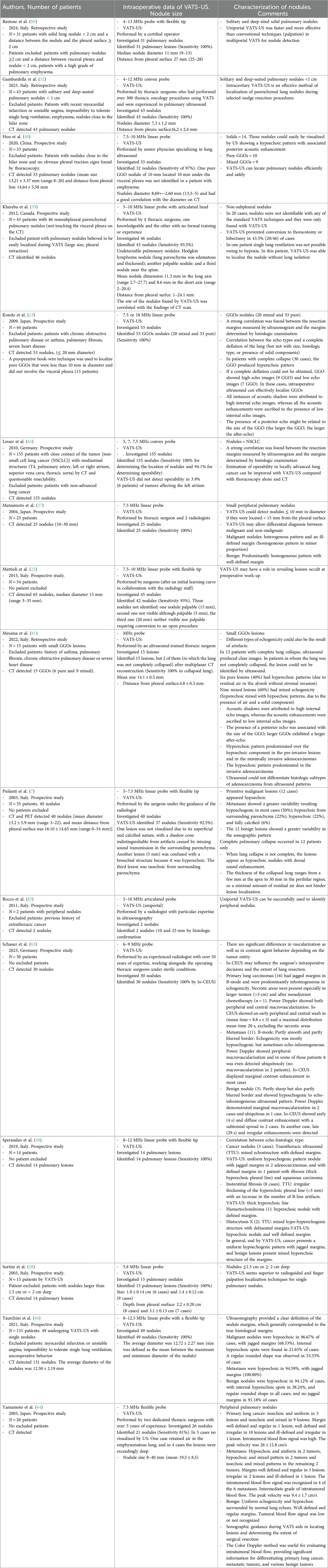
Table 1. Location and characterization of pulmonary nodules according to various authors.
Correlation of pulmonary nodule characteristics obtained by LU with preoperative CT and histological analysis data
The size of pulmonary nodules identified by intraoperative ultrasound is often correlated with the size observed on preoperative CT scans. For example, Hou et al. (40) found that the mean diameter of pulmonary nodules detected by LU was significantly correlated with the mean diameter obtained by CT (R = 0.860, P < 0.05) (ranging from 5 to 13.5 mm by LU and 8–20 mm by CT). However, other authors observed that the size range of ground-glass opacities (GGO) detected by LU was significantly smaller than that found by CT (23). Furthermore, the size and margins of pulmonary nodules identified by LU were correlated with data obtained from histological analysis (6, 23, 51, 54). According to some authors, this strong correlation may be partly due to the use of high-frequency ultrasound probes (55). Other authors have reported a weaker correlation between intraoperative ultrasound and histological analysis regarding the depth of the lung lesion (51). The pressure applied by the ultrasound probe on the lung surface of the sample, intended to eliminate residual peritumoral air and improve the visualization of the GGO, is likely responsible for this reduced correlation (55).
Effectiveness of LU for localization of GGOs
Particular attention should be given to the location of GGOs. This term refers to the tomographic appearance of a focal opacity characterized by increased density in the lung parenchyma. Nodules detected by CT can be classified as solid or subsolid, with subsolid nodules further divided into partially solid nodules and GGOs. GGOs represent a hazy area of increased pulmonary attenuation while preserving bronchial and vascular markings. These lesions can be either mixed or pure, depending on the presence of a solid component within (56). GGOs encompass benign conditions, such as infections, as well as malignancies, including lung cancer (adenocarcinoma). Opacities smaller than 1 cm are typically indicative of atypical adenomatoid hyperplasia or adenocarcinoma in situ, whereas lesions exceeding this size increase the likelihood of invasive adenocarcinoma, with the risk rising from 10% to 50%. Their malignant and invasive potential is further elevated when a solid component is present within the lesion (57).
Many GGOs, unlike solid tumors, are not easily detected during VATS surgical procedures (7, 22, 55, 58). Aside from the fact that they are generally not palpable, the density of these lesions is similar to that of the adjacent normal parenchyma, making their sonographic identification challenging even for experienced surgeons, especially when dealing with pure GGOs (those with no solid component) or deeply located GGOs (51). Furthermore, their identification in the specimen can pose technical challenges for pathologists and may require sectioning and microscopic examination of the entire specimen. In such cases, marking the lesion with an ultrasound-guided needle can facilitate rapid localization by the pathologist, reducing the number of sections needed and shortening operative time. This approach is less cumbersome than CT-guided needle identification of lung nodules in reaerated lung specimens. When using this technique, in addition to a radiology room, moderate mechanical aeration is required to enable the detection of GGO with CT. This, however, is not feasible when the sample is compromised by air leaks (59).
In some GGOs, a posterior echo may be observed, which could assist in their identification and might be related to the size of the GGO; however, further studies are needed to confirm this finding (23, 60). Achieving a complete lung collapse, as well as using electrocautery to mark the visceral pleura and better define the margins of the lesions, can be helpful when resecting these tumors (23, 51). Kondo et al. (23) considered resections with margins 1.5 times the diameter of the lung nodule, or at least 2 cm, as safe. Other authors have proposed preoperative marking of tumors for pulmonary nodules ≤10 mm in size, located more than 5 mm from the pleural surface, as they observed intraoperative detection failures of up to 63% (61). Jian Hu et al. (62) also advocated for marking with methylene blue, 2 hours before thoracoscopic wedge resection, those nodules that, on CT, showed a distance greater than 1.5 cm from the pleural surface and were difficult to identify due to their location. Despite the challenges in identifying these tumors, some authors, such as Fiorelli et al. (51), were able to identify 100% of GGOs in an ex vivo analysis, with an average size of 13.9 ± 0.5 mm, and in 11 of 17 (65%) cases, the lesions were smaller than 15 mm, with a mean depth of 4.4 ± 0.3 mm. In all cases, pathologists were able to conclusively identify these lesions with the initial analysis.
Effectiveness of ultrasound in determining the severity of injuries
Based on echogenicity patterns
Some authors have distinguished between primary lesions, metastases, and benign lesions based on various ultrasound patterns. Regarding primary tumors, Khereba et al. (39) reported no correlation between the ultrasound patterns and the malignancy or benignity of the lesions. Conversely, other studies (39, 52) identified a heterogeneous pattern with punctile hyperechoic areas and ill-defined or jagged margins in primary tumors. Schauer et al. (63) noted well-defined necrotic areas in larger tumors (>3 cm), potentially contributing to the observed punctile hyperechoic pattern. Similarly, Piolanti (7) and Sperandeo et al. (48) found a predominance of hypoechoic lesions with jagged margins, while Yamamoto et al. (64) described these as predominantly isoechoic with irregular, well-defined margins.
In the case of metastatic lesions, some authors could not distinguish between primary or metastatic origins based on ultrasound patterns (37, 48). Piolanti et al. (7) found that 50% of metastatic lesions were hypoechoic, while the remaining showed a more variable pattern, with some appearing hyperechoic. Schauer et al. (63) similarly reported that most metastases were hypoechoic, occasionally non-homogeneous, with both smooth and blurred edges. Yamamoto et al. (64) observed a predominance of hypoechoic patterns in metastases, with margins ranging from well-defined to irregular. Benign lesions displayed significant variability in ultrasound patterns, appearing as both hyperechoic and hypoechoic, typically with well-defined margins (37, 48, 64).
Regarding GGOs, Hou et al. (40) found no correlation between ultrasound patterns and the malignancy or benignity of the lesions. However, Fiorelli et al. (51) concluded that pure and mixed GGOs with predominantly hyperechoic patterns were associated with preinvasive or minimally invasive lesions, while those with hypoechoic patterns indicated invasive adenocarcinoma. Kondo et al. (23) found that the echogenicity of GGOs, whether hyperechoic or hypoechoic, was influenced by the degree of lung aeration during lung collapse. Complete lung collapse typically resulted in a hyperechoic pattern, whereas incomplete collapse produced a mixed or speckled hyperechoic pattern due to residual air.
Based on the Doppler echocardiographic record
Several researchers have identified a correlation between the type of lesion -whether malignant or benign- and its vascularization pattern as observed through Color Doppler imaging. In cases of primary lung carcinomas, Schauer et al. (63) demonstrated the presence of both peripheral and central macrovascularization using Color-Coded Doppler Sonography (CCDS) or Power Doppler techniques. Similarly, Yamamoto et al. (64) reported a significant intratumoral blood flow signal in all primary lesions, with a peak velocity averaging 26 ± 12.8 cm/s. Notably, this elevated blood flow was particularly pronounced in eight out of twelve examined lesions.
In the context of metastasis, Schauer et al. (63) observed a predominance of peripheral macrovascularization in these lesions, with some cases exhibiting either ubiquitous or even undetectable vascularization. Yamamoto et al. (64) found a medium-grade intratumoral blood flow signal in four of the six metastatic lesions studied, with a peak velocity of 9.4 ± 1.7 cm/s, marking a statistically significant contrast to the higher velocities seen in primary tumors.
For benign lesions, the findings were distinct. Schauer et al. (63) documented marginal macrovascularization in two cases and ubiquitous macrovascularization in one. In contrast, Yamamoto et al. (64) found no evidence of tumor flow signals in benign lesions, suggesting a markedly different vascular profile when compared to malignant tumors. These observations underscore the potential of Color Doppler imaging as a diagnostic tool in distinguishing between different types of pulmonary lesions based on their vascular characteristics.
Based on the results obtained by Io-CEUS
Pulmonary nodules were further characterized by the pattern of contrast distribution, specifically regarding peripheral and/or central enhancement, using Io-CEUS. Schauer et al. (63) explored the application of Io-CEUS in identifying pulmonary nodules that were challenging to visualize and characterize before resection. In their study, bolus injections of 2.4–5 ml sulfur hexafluoride microbubbles (SonoVue®, Bracco, Milan, Italy) were administered, followed by 10–20 ml of NaCl, delivered through a central venous catheter by the anesthesiologist. The behavior of the contrast agent varied significantly with the tumor type. In primary lung carcinomas, early peripheral and central washout was observed, with a mean time of 8.8 s ± 3, and a mean maximum distribution time of 20 s, excluding necrotic areas when present. For metastatic lesions, Schauer et al. (63) noted marginal contrast enhancement in most cases; the timing of contrast enhancement varied, occurring early in some cases (t = 6 s) and late in others (t = 16 s). For benign nodules, Io-CEUS demonstrated early (as early as 4 s) and diffuse contrast enhancement in two cases, while in another case, it revealed late (29 s) and irregular enhancement. These findings highlight the potential of Io-CEUS in differentiating pulmonary nodule types based on their contrast enhancement patterns, offering valuable real-time intraoperative insights.
Determining tumor resectability using ultrasound
The use of intrathoracic ultrasound to assess tumor resectability has been explored in limited studies. Santambrogio et al. (55) investigated the cardiovascular and metastatic invasion of malignant lung lesions. Upon identifying the lung nodule, they evaluated its proximity to the vessels and heart by methodically moving the ultrasound probe from the upper to the lower mediastinum and towards the hilum, considering lymph nodes measuring 15 mm or more as indicative of metastasis. Lesser et al. (65) also assessed the resectability of 155 nodules, all classified as non-small cell lung cancer (NSCLC, T4 N0-1) and meeting criteria for invasiveness. In all patients, CT scans revealed close contact between the tumor and mediastinal structures (T4), such as the pulmonary artery, left or right atrium, superior vena cava (SVC), and thoracic aorta, raising concerns about operability. The ultrasound probe was strategically placed over hilar and mediastinal structures to evaluate operability criteria, which included: less than one-third circumference infiltration of the SVC without right atrium invasion, no aortic wall infiltration, at least 1 cm of tumor-free intrapericardial pulmonary artery, and less than 1 cm invasion of the left atrium near the origin of the pulmonary veins. The pulmonary lesion locations were accurately established in all patients. Resectability staging using VAT-US demonstrated a sensitivity of 94.1% and a specificity of 98.1%. However, false negative and false positive rates for the pulmonary artery and left atrium were notably high (16.1% and 14.8%, respectively). The study suggested that positioning the probe over the pulmonary hilum in various planes and intrapericardially could enhance the assessment of tumor infiltration in the left atrium and heart. Employing high-frequency ultrasound probes was also recommended for improved accuracy. The authors concluded that utilizing ultrasound to determine operability could be beneficial for patients deemed inoperable, potentially reducing the need for diagnostic thoracotomies.
Pulmonary collapse for the identification of pulmonary nodules using lung ultrasound
During lung surgery, the target lung is typically deflated, often through the use of a lung ventilation device that enables single-lung ventilation. This process reduces the air content in the bronchoalveolar spaces of the excluded lung, facilitating deeper exploration with an ultrasound probe. In fully deflated lungs, pulmonary arterioles and venules appear as homogeneous hypoechoic areas, while bronchioles are visualized as hyperechoic spots, enhancing the identification of lung nodules.
Khereba and Kondo et al. (23, 39) proposed that the varying echogenicities observed during intraoperative LU recordings could be attributed to artifacts rather than the size, histological type of the lesions, or the presence of solid components. In a fully deflated lung, GGOs typically present a hyperechoic pattern. However, if the lung is not entirely deflated, as might occur in cases of chronic obstructive pulmonary disease, the internal lung structures are likely to exhibit a “mottled hyperechoic pattern” due to residual air echo artifacts. Additionally, dorsal sound enhancement may be noted around lung lesions, resulting from the greater transmission of the ultrasound beam through the nodules compared to the surrounding parenchyma, where ultrasound reflection is more pronounced due to residual air (23). Nevertheless, a minimal presence of residual air should not significantly hinder lesion identification (55), as the thickness of the collapsed lung ranges from a few millimeters at the apex to 30 mm in the perihilar region, with residual air primarily limiting studies beyond a depth of approximately 20 mm.
Anesthesiologists can enhance the ultrasound image by minimizing the amount of air within the lung parenchyma. This can be accomplished through the proper placement of the double-lumen tube (DLT). Incorrect placement, which occurs in up to 14% of cases, may result in intraoperative desaturation and inadequate lung protection against hemorrhage, pus, and secretions (66). The replacement of these tubes should be carried out with caution due to the potential complications, such as tracheal injury, which may include irritation, laryngitis, or airway rupture. The membranous part of the trachea (52%) and the left main bronchial trunk (37%) are the most common sites of rupture (67). These complications are more frequent in patients who have undergone radiotherapy or corticosteroid treatment, which weakens the tracheobronchial wall and contributes to several risk factors (53, 68). These factors include difficulties in intubation, multiple attempts at repositioning the DLT, use of oversized tubes, or overinflation of the bronchial cuff, leading to mucosal ischemia. Therefore, a proper lung collapse should be confirmed using a fiberoptic bronchoscope, and the correct choice of DLT size is essential (66). Preoperative CT scans can aid in selecting the appropriate DLT size by assessing the diameters of the main left bronchus and cricoid cartilage (69). Transthoracic ultrasound is also a valuable tool in DLT sizing, as it allows for the measurement of the trachea's external diameter or the cricoid (70, 71) and confirms the correct positioning of the left DLT (72). Furthermore, transthoracic ultrasound can be used to assess lung aeration after DLT placement, facilitating ventilation optimization. Loss of lung aeration can be visualized through B-lines or vertical hyperechoic lines emanating from the pleural line, which move with respiration. The separation of these lines indicates moderate loss of aeration, while their merging suggests severe loss due to alveolar filling. The absence of diaphragmatic and pleural movement also signals lung collapse (73–79).
However, despite the correct selection of the DLT, complete lung isolation cannot always be assured, particularly in patients with severe chronic obstructive pulmonary disease (COPD) (45), which can introduce errors in ultrasound evaluation (21–23). Some authors, while emphasizing the importance of deflating the lung, were unable to achieve full lung deflation in 30% of patients, even after applying gentle pressure to the lung surface with an instrumental probe (23). For this reason, patients with asthma and COPD were excluded from some ultrasound studies. Additionally, the time required to achieve complete lung exclusion is not negligible, with an average time of 40 minutes documented from the selective exclusion of the affected lung (45). Furthermore, it must be acknowledged that in some cases, maintaining proper single-lung ventilation to ensure tissue oxygenation and patient stability may be difficult or even impossible.
Discussion
Data from the scientific literature show the usefulness of VATS-US in the identification of both very small peripheral pulmonary nodules [<2 mm (37)] and deep nodules (38, 45, 80), allowing safe and small resection margins and decreasing conversion to thoracotomy (39). In addition, performing LU does not entail complications such as those described in other nodular identification techniques (insertion of metals with CT-guided wire hook, injection of methylene blue or isotopes, intraoperative endoscopic tracheal magnetic navigation, among others). No patient presented arrhythmias, changes in blood pressure, bleeding or other complications during the examination performed with intrathoracic ultrasound, so it is considered a safe technique, in addition to being able to be performed in real time and at low cost. In addition, Colour Doppler and Io-CEUS have helped to differentiate lung lesions according to their benignity/malignancy, although further studies are needed to define and confirm the different vascular patterns and contrast distribution (63, 64). With the data currently available, primary lesions present both central and peripheral vascularization; in metastases, vascularization seems to have a peripheral predominance, and in benign lesions both marginal macrovascularization and avascularization have been described. This vascular distribution was correlated with the different patterns of Io-CEUS contrast distribution in the lesions. Thus, primary lung carcinomas showed early peripheral and central washout, metastases showed marginal contrast enhancement and benign lesions showed more diffuse enhancement. Confirmation of these results could allow what some authors have called “living histology” in thoracic surgery, potentially influencing decision-making on the extent of lung resection in the future (63). Nevertheless, given that the pulmonary vasculature is influenced by lung collapse, it should be considered that the use of contrast-enhanced ultrasound for the characterization of pulmonary lesions remains controversial. Further research is required to determine its degree of utility, as the existing literature is limited. However, despite the impact of lung collapse on normal pulmonary perfusion, the residual perfusion of the bronchial arteries in primary or metastatic tumors may be utilized to enhance intraoperative localization. Its implementation as a complementary tool in VATS could optimize surgical precision and reduce the morbidity associated with unnecessary resections.
Finally, VATS-US has also been shown to be useful in staging the resectability of T4 non-small cell lung cancer (NSCLC). Resectability depends on the degree of tumor involvement of mediastinal structures, and CT does not always allow distinction between tumor bordering the mediastinum and tumor invading mediastinal structures. By allowing mediastinal dissection, albeit to a limited extent, VATS-US has been shown to be useful in determining whether tumor has infiltrated the descending aorta, superior vena cava, or right atrium. It has also allowed determination of the exact margin of tumor infiltration in the left atrium (65). However, it should be considered that, currently, PET-CT and MRI remain the gold standard for evaluating mediastinal invasion. Intraoperative ultrasound can play a complementary role in the intraoperative assessment, for example, in helping to define the degree of invasion or identify abnormal vasculature, but it should not replace these advanced techniques.
The application of VATS-US has certain limitations. The presence of COPD or heart disease can make it challenging to identify pulmonary nodules via ultrasound. In such cases, as well as in situations involving GGOs and non-peripheral lung lesions smaller than 10 mm in diameter (located more than 5 mm from the pleural surface), preoperative marking may be considered (23). Furthermore, there are other factors that can lead to incorrect ultrasound interpretation, such as recent myocardial infarction or unstable angina, pulmonary edema, pleural retraction, pulmonary fibrosis, among others. Thus, several authors choose to exclude these patients from their studies (23, 39, 52). Moreover, the interpretation of images is subjective and requires specialized training, education, and experience—factors that significantly limit the use of this technique. Although some authors suggest that VATS-US is a straightforward technique with a rapid learning curve (39), most published studies indicate that VATS-US was performed by thoracic surgeons, sometimes guided by radiologists, or by radiologists with over 10 years of experience (63) (Table 1).
Additionally, drawing conclusions about the benignity or malignancy of lesions based solely on the echogenicity pattern is challenging. Typically, primary lesions are predominantly heterogeneous, with mixed echogenicity (hypoechoic and hyperechoic areas) and irregular margins. In metastases, a hypoechoic pattern with irregular margins is predominant, although to a lesser extent than in primary tumors. In benign lesions, there is significant variability in echogenicity, with well-defined margins being more common. However, these criteria alone do not confirm the benignity or malignancy of the lesions, and histological confirmation is necessary.
Moreover, scientific literature highlights a lack of homogeneous ultrasound criteria for defining lung lesions, complicating their characterization. It is essential to distinguish between concepts such as hyperechogenicity and heterogeneity, or hypoechogenicity and homogeneity, as well as to clearly define the margins of lesions, specifying whether they are irregular or well-defined. When describing ultrasound lesions, it is also necessary to mention the degree of lung collapse achieved, as residual air can create artifacts (81) and errors in the ultrasound interpretation of lesions. This residual air depends not only on the correct placement and inflation of the DLT but also on the intrinsic characteristics of patients, particularly whether they suffer from respiratory or cardiac conditions.
In summary, the identification of pulmonary nodules can be enhanced by implementing specific measures. Firstly, the preoperative identification of pulmonary lesions via CT is crucial. Performing VATS-US does not eliminate the need for intraoperative visual inspection and palpation of pulmonary lesions identified by CT (22, 23). The selection of the most appropriate probe for the lesion to be resected should be based on its depth. High-frequency ultrasound probes (>5 MHz) are recommended for visualizing more superficial or smaller tumors (≤2 mm), while low-frequency probes (3.5 MHz) are preferable for deeper lesions (>4 mm) (46, 81). Additionally, the use of ultrasound probes with flexible tips facilitates multiplanar exploration of the area of interest (22, 82), making it necessary to insert the ultrasound probe between the fissures to visualize the lung parenchyma from all angles. To optimize the imaging, complete lung deflation is essential. Inducing lung collapse prior to lesion excision, when the patient is positioned for surgery, can promote greater lung deflation. Moreover, careful air suction through the DLT and the application of pressure on the lung by the ultrasound probe help release lung air and facilitate lung collapse (6, 23). It is important to note that the pressure exerted by the ultrasound probe can influence the precise measurement of the distance between the lesion and the pleural surface. Once the lung has collapsed, filling the pleural space with saline (500 ml) may enhance ultrasound definition (23). Finally, the success of the VATS-US technique relies heavily on the practitioner's learning and experience (63).
Further research is needed to enhance the VATS-US technique, thereby enabling a more reliable characterization of lung lesions in terms of their benignity or malignancy. In this context, artificial intelligence could play a pivotal role by integrating various algorithms that take into account not only the tumor's features—such as echogenicity, margins, vascular patterns, and contrast distribution—but also the patient's intrinsic characteristics that may influence the degree of lung collapse. Additionally, ethnic and regional variations, which may imply differences in lung lesions, should be considered in the development of these algorithms.
Author contributions
SG-S: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. MG: Data curation, Investigation, Writing – review & editing. J-CV: Validation, Writing – review & editing. AJ: Formal analysis, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to express our gratitude to Míriam Basagaña i Farrés, the librarian of our Hospital, for providing the necessary bibliographic materials for the completion of this review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fra-Fernández S, Muñoz-Molina GM, Cabañero-Sánchez A, del Campo-Albendea L, Bolufer-Nadal S, Embún-Flor R, et al. Postoperative morbidity after anatomical lung resections by VATS vs thoracotomy: treatment and intention-to-treat analysis of the Spain video-assited thoracic surgery group. Cirugía Española. (2023) 101(11):778–6. doi: 10.1016/j.ciresp.2023.05.001
2. Ng CSH, Lee TW, Wan S, Wan IYP, Sihoe ADL, Arifi AA, et al. Thoracotomy is associated with significantly more profound suppression in lymphocytes and natural killer cells than video-assisted thoracic surgery following major lung resections for cancer. J Invest Surg. (2005) 18(2):81–8. doi: 10.1080/08941930590926320
3. Saito H, Minamiya Y, Matsuzaki I, Tozawa K, Taguchi K, Nakagawa T, et al. Indication for preoperative localization of small peripheral pulmonary nodules in thoracoscopic surgery. J Thorac Cardiovasc Surg. (2002) 124(6):1198–202. doi: 10.1067/mtc.2002.127331
4. Tatsumura T. Preoperative and intraoperative ultrasonographic examination as an aid in lung cancer operations. J Thorac Cardiovasc Surg. (1995) 110(3):606–12. doi: 10.1016/S0022-5223(95)70091-9
5. Cheng J, Li C, Wang L, Liang J, Yan Z, Hu J, et al. Precise localization pulmonary nodules using Pre-VATS with Xper-CT in combination with real-time fluoroscopy-guided coil: report of 15 patient. J Interv Med. (2019) 1(2):102–5. doi: 10.19779/j.cnki.2096-3602.2018.02.08
6. Ujiie H, Kato T, Hu H-P, Hasan S, Patel P, Wada H, et al. Evaluation of a new ultrasound thoracoscope for localization of lung nodules in ex vivo human lungs. Ann Thorac Surg. (2016) 103(3):926–34. doi: 10.1016/j.athoracsur.2016.08.031
7. Piolanti M, Coppola F, Papa S, Pilotti V, Mattioli S, Gavelli G. Ultrasonographic localization of occult pulmonary nodules during video-assisted thoracic surgery. Eur Radiol. (2003) 13(10):2358–64. doi: 10.1007/s00330-003-1916-6
8. Di Salvo G, Miller O, Babu Narayan S, Li W, Budts W, Valsangiacomo Buechel ER, et al. Imaging the adult with congenital heart disease: a multimodality imaging approach-position paper from the EACVI. Eur Heart J Cardiovasc Imaging. (2018) 19(10):1077–98. doi: 10.1093/ehjci/jey102
9. Mozzini C, Di Dio Perna M, Pesce G, Garbin U, Fratta Pasini AM, Ticinesi A, et al. Lung ultrasound in internal medicine efficiently drives the management of patients with heart failure and speeds up the discharge time. Intern Emerg Med. (2017) 13(1):27–33. doi: 10.1007/s11739-017-1738-1
10. Zieleskiewicz L, Cornesse A, Hammad E, Haddam M, Brun C, Vigne C, et al. Implementation of lung ultrasound in polyvalent intensive care unit: impact on irradiation and medical cost. Anaesth Crit Care Pain Med. (2015) 34(1):41–4. doi: 10.1016/j.accpm.2015.01.002
11. Patella M, Saporito A, Puligheddu C, Mongelli F, La Regina D, Pini R, et al. Lung ultrasound to detect residual pneumothorax after chest drain removal in lung resections. Ann Thorac Surg. (2018) 105(5):1537–42. doi: 10.1016/j.athoracsur.2017.12.008
12. Goudie E, Bah I, Khereba M, Ferraro P, Duranceau A, Martin J, et al. Prospective trial evaluating sonography after thoracic surgery in postoperative care and decision making. Eur J Cardiothorac Surg. (2011) 41(5):1025–30. doi: 10.1093/ejcts/ezr183
13. Sperandeo M, Filabozzi P, Varriale A, Carnevale V, Piattelli ML, Sperandeo G, et al. Role of thoracic ultrasound in the assessment of pleural and pulmonary diseases. J Ultrasound. (2008) 11(2):39–46. doi: 10.1016/j.jus.2008.02.001
14. Sperandeo M, Del Colle A, Frongillo E, Rea G, Dimitri L, Cipriani C, et al. Safety maximization of percutaneous transthoracic needle biopsy with ultrasound guide in subpleural lesions in the evaluation of pulmonary consolidation. Respir Res. (2019) 20(1):68. doi: 10.1186/s12931-019-1031-0
15. Cantinotti M, Giordano R, Volpicelli G, Kutty S, Murzi B, Assanta N, et al. Lung ultrasound in adult and paediatric cardiac surgery: is it time for routine use? Interact Cardiovasc Thorac Surg. (2015) 22(2):208–15. doi: 10.1093/icvts/ivv315
16. Yu X, Zhai Z, Zhao Y, Zhu Z, Tong J, Yan J, et al. Performance of lung ultrasound in detecting peri-operative atelectasis after general anesthesia. Ultrasound Med Biol. (2016) 42(12):2775–84. doi: 10.1016/j.ultrasmedbio.2016.06.010
17. Brogi E, Gargani L, Bignami E, Barbariol F, Marra A, Forfori F, et al. Thoracic ultrasound for pleural effusion in the intensive care unit: a narrative review from diagnosis to treatment. Crit Care. (2017) 21(1):325. doi: 10.1186/s13054-017-1897-5
18. Long L, Zhao H-T, Zhang Z-Y, Wang G-Y, Zhao H-L. Lung ultrasound for the diagnosis of pneumonia in adults: a meta-analysis. Medicine (Baltimore). (2017) 96(3):e5713. doi: 10.1097/MD.0000000000005713
19. Galetin T, Defosse J, Schieren M, Marks B, Lopez-Pastorini A, Koryllos A, et al. Sensitivity of chest ultrasound for postoperative pneumothorax in comparison to chest x-ray after lung resecting surgery. Eur J Cardiothorac Surg. (2020) 57(5):846–53. doi: 10.1093/ejcts/ezz332
20. Gil-Juanmiquel L, Gratacós M, Castilla-Fernández Y, Piqueras J, Baust T, Raguer N, et al. Bedside ultrasound for the diagnosis of abnormal diaphragmatic motion in children after heart surgery. Pediatr Crit Care Med. (2017) 18(2):159–64. doi: 10.1097/PCC.0000000000001015
21. Greenfield AL, Steiner RM, Liu JB, Cohn HE, Goldberg BB, Rawool NM, et al. Sonographic guidance for the localization of peripheral pulmonary nodules during thoracoscopy. AJR Am J Roentgenol. (1997) 168(4):1057–60. doi: 10.2214/ajr.168.4.9124115
22. Mattioli S, D’Ovidio F, Daddi N, Ferruzzi L, Pilotti V, Ruffato A, et al. Transthoracic endosonography for the intraoperative localization of lung nodules. Ann Thorac Surg. (2005) 79(2):443–9. doi: 10.1016/j.athoracsur.2004.07.087
23. Kondo R, Yoshida K, Hamanaka K, Hashizume M, Ushiyama T, Hyogotani A, et al. Intraoperative ultrasonographic localization of pulmonary ground-glass opacities. J Thorac Cardiovasc Surg. (2009) 138(4):837–42. doi: 10.1016/j.jtcvs.2009.02.002
24. Ciriaco P, Negri G, Puglisi A, Nicoletti R, Del Maschio A, Zannini P. Video-assisted thoracoscopic surgery for pulmonary nodules: rationale for preoperative computed tomography-guided hookwire localization. Eur J Cardiothorac Surg. (2004) 25(3):429–33. doi: 10.1016/j.ejcts.2003.11.036
25. Partrick DA, Bensard DD, Teitelbaum DH, Geiger JD, Strouse P, Harned RK. Successful thoracoscopic lung biopsy in children utilizing preoperative CT-guided localization. J Pediatr Surg. (2002) 37(7):970–3. doi: 10.1053/jpsu.2002.33820
26. Nomori H, Horio H, Naruke T, Suemasu K. Fluoroscopy-assisted thoracoscopic resection of lung nodules marked with lipiodol. Ann Thorac Surg. (2002) 74(1):170–3. doi: 10.1016/s0003-4975(02)03615-9
27. Miyoshi T, Kondo K, Takizawa H, Kenzaki K, Fujino H, Sakiyama S, et al. Fluoroscopy-assisted thoracoscopic resection of pulmonary nodules after computed tomography–guided bronchoscopic metallic coil marking. J Thorac Cardiovasc Surg. (2006) 131(3):704–10. doi: 10.1016/j.jtcvs.2005.09.019
28. Wang Y-Z, Boudreaux JP, Dowling A, Woltering EA. Percutaneous localisation of pulmonary nodules prior to video-assisted thoracoscopic surgery using methylene blue and TC-99. Eur J Cardiothorac Surg. (2009) 37(1):237–8. doi: 10.1016/j.ejcts.2009.07.022
29. Daniel TM, Altes TA, Rehm PK, Williams MB, Jones DR, Stolin AV, et al. A novel technique for localization and excisional biopsy of small or ill-defined pulmonary lesions. Ann Thorac Surg. (2004) 77(5):1756–62. doi: 10.1016/j.athoracsur.2003.10.099
30. Chella A, Lucchi M, Ambrogi MC, Menconi G, Melfi FM, Gonfiotti A, et al. A pilot study of the role of TC-99 radionuclide in localization of pulmonary nodular lesions for thoracoscopic resection. Eur J Cardiothorac Surg. (2000) 18(1):17–21. doi: 10.1016/s1010-7940(00)00411-5
31. Morita R, Kaneko K, Suga M, Omoto R. Computed tomography-guided hookwire localization of small pulmonary nodules for thoracoscopic biopsy. Nihon Kokyuki Gakkai Zasshi. (1999) 37(6):439–42.10434541
32. Mayo JR, Clifton JC, Powell TI, English JC, Evans KG, Yee J, et al. Lung nodules: cT-guided placement of microcoils to direct video-assisted thoracoscopic surgical resection. Radiology. (2009) 250(2):576–85. doi: 10.1148/radiol.2502080442
33. Krüger K, Eyl G, Morgenroth C, Schneider P, Hoelscher A, Lackner K. Success and complication rate of CT-guided marking of pulmonary nodules with coil wires for video-assisted thoracoscopic surgery (VATS). Rofo. (2006) 178(12):1250–4. doi: 10.1055/s-2006-926956
34. Macherey S, Doerr F, Heldwein M, Hekmat K. Is manual palpation of the lung necessary in patients undergoing pulmonary metastasectomy? Interact Cardiovasc Thorac Surg. (2015) 22(3):351–9. doi: 10.1093/icvts/ivv337
35. Parsons AM, Detterbeck FC, Parker LA. Accuracy of helical CT in the detection of pulmonary metastases: is intraoperative palpation still necessary? Ann Thorac Surg. (2004) 78(6):1910–6. doi: 10.1016/j.athoracsur.2004.05.065
36. de Kerviler E, Gossot D, Célérier M, Frija J. Limitations of intraoperative sonography for the localization of pulmonary nodules during thoracoscopy. AJR Am J Roentgenol. (1998) 170(1):214–5. doi: 10.2214/ajr.170.1.9423634
37. Matsumoto S, Hirata T, Ogawa E, Fukuse T, Ueda H, Koyama T, et al. Ultrasonographic evaluation of small nodules in the peripheral lung during video-assisted thoracic surgery (VATS). Eur J Cardiothorac Surg. (2004) 26(3):469–73. doi: 10.1016/j.ejcts.2004.05.013
38. Sortini D, Feo CV, Carcoforo P, Carrella G, Pozza E, Liboni A, et al. Thoracoscopic localization techniques for patients with solitary pulmonary nodule and history of malignancy. Ann Thorac Surg. (2005) 79(1):258–62. doi: 10.1016/j.athoracsur.2004.06.012
39. Khereba M, Ferraro P, Duranceau A, Martin J, Goudie E, Thiffault V, et al. Thoracoscopic localization of intraparenchymal pulmonary nodules using direct intracavitary thoracoscopic ultrasonography prevents conversion of VATS procedures to thoracotomy in selected patients. J Thorac Cardiovasc Surg. (2012) 144(5):1160–5. doi: 10.1016/j.jtcvs.2012.08.034
40. Hou Y-L, Wang Y-D, Guo H-Q, Zhang Y, Guo Y, Han H. Ultrasound location of pulmonary nodules in video-assisted thoracoscopic surgery for precise sublobectomy. Thorac Cancer. (2020) 11(5):1354–60. doi: 10.1111/1759-7714.13384
41. Bellomi M, Veronesi G, Trifirò G, Brambilla S, Bonello L, Preda L, et al. Computed tomography-guided preoperative radiotracer localization of nonpalpable lung nodules. Ann Thorac Surg. (2010) 90(6):1759–64. doi: 10.1016/j.athoracsur.2010.08.016
42. Hanauer M, Perentes JY, Krueger T, Ris H-B, Bize P, Schmidt S, et al. Pre-operative localization of solitary pulmonary nodules with computed tomography-guided hook wire: report of 181 patients. J Cardiothorac Surg. (2016) 11:5. doi: 10.1186/s13019-016-0404-4
43. Luo K, Lin Y, Lin X, Yu X, Wen J, Xi K, et al. Localization of peripheral pulmonary lesions to aid surgical resection: a novel approach for electromagnetic navigation bronchoscopic dye marking. Eur J Cardiothorac Surg. (2017) 52(3):516–21. doi: 10.1093/ejcts/ezx114
44. Falcoz P-E, Puyraveau M, Thomas P-A, Decaluwe H, Hürtgen M, Petersen RH, et al. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: a propensity-matched analysis of outcome from the European society of thoracic surgeon database. Eur J Cardiothorac Surg. (2015) 49(2):602–9. doi: 10.1093/ejcts/ezv154
45. Gruppioni F, Piolanti M, Coppola F, Papa S, Di Simone M, Albini L, et al. Intraoperative echography in the localization of pulmonary nodules during video-assisted thoracic surgery. Radiol Med. (2000) 100(4):223–8.11155447
46. Taurchini M, Quarato CMI, Frongillo EM, Ferretti GM, Cipriani C, Bizzarri M, et al. Intraoperative lung ultrasound (ILU) for the assessment of pulmonary nodules. Diagnostics (Basel). (2021) 11(9):1191. doi: 10.3390/diagnostics11091691
47. Sperandeo M, Venuti M, Quarato CMI. Uniportal versus multiportal video-assisted thoracic surgery for lung cancer: safety and advantages in employing complementary intraoperative lung ultrasound. J Thorac Dis. (2020) 12(6):3013–7. doi: 10.21037/jtd.2020.03.45
48. Sperandeo M, Frongillo E, Taurchini M, Del Colle A, Quarato CMI, Dimitri LMC, et al. Transthoracic ultrasound and intraoperative lung ultrasound. Biomed J Sci Tech Res. (2019) 17(3):12889–92. doi: 10.26717/BJSTR.2019.17.003014
49. Matsutani N, Sawabata N, Yamaguchi M, Woo T, Kudo Y, Kawase A, et al. Does lung cancer surgery cause circulating tumor cells?-A multicenter, prospective study. J Thorac Dis. (2017) 9(8):2419–26. doi: 10.21037/jtd.2017.07.33
50. Hashimoto M, Tanaka F, Yoneda K, Takuwa T, Matsumoto S, Okumura Y, et al. Significant increase in circulating tumour cells in pulmonary venous blood during surgical manipulation in patients with primary lung cancer. Interact Cardiovasc Thorac Surg. (2014) 18(6):775–83. doi: 10.1093/icvts/ivu048
51. Fiorelli A, Messina G, Frongillo E, Accardo M, Montella M, Panarese I, et al. The use of ultrasound in detecting and defining ground-glass opacities: results of an ex vivo evaluation. Interact Cardiovasc Thorac Surg. (2018) 26(4):551–8. doi: 10.1093/icvts/ivx373
52. Gambardella C, Messina G, Pica DG, Bove M, Capasso F, Mirra R, et al. Intraoperative lung ultrasound improves subcentimetric pulmonary nodule localization during VATS: results of a retrospective analysis. Thorac Cancer. (2023) 14(25):2558–66. doi: 10.1111/1759-7714.15027
53. Merli G, Guarino A, Della Rocca G, Frova G, Petrini F, Sorbello M, et al. Recommendations for airway control and difficult airway management in thoracic anesthesia and lung separation procedures. Minerva Anestesiol. (2008) 75(1–2):59–96.18987567
54. Daddi N, Sagrini E, Lugaresi M, Perrone O, Candoli P, Ragusa M, et al. Ex vivo pulmonary nodule detection with miniaturized ultrasound convex probes. J Surg Res. (2015) 202(1):49–57. doi: 10.1016/j.jss.2015.12.005
55. Santambrogio R, Montorsi M, Bianchi P, Mantovani A, Ghelma F, Mezzetti M. Intraoperative ultrasound during thoracoscopic procedures for solitary pulmonary nodules. Ann Thorac Surg. (1999) 68(1):218–22. doi: 10.1016/s0003-4975(99)00459-2
56. Nakata M, Saeki H, Takata I, Segawa Y, Mogami H, Mandai K, et al. Focal ground-glass opacity detected by low-dose helical CT. Chest. (2002) 121(5):1464–7. doi: 10.1378/chest.121.5.1464
57. Gould MK, Donington J, Lynch WR, Mazzone PJ, Midthun DE, Naidich DP, et al. Evaluation of individuals with pulmonary nodules: when is it lung cancer? Diagnosis and management of lung cancer, 3rd ed: american college of chest physicians evidence-based clinical practice guidelines. Chest. (2013) 143(5 Suppl):e93S–e120S. doi: 10.1378/chest.12-2351
58. MacMahon H, Naidich DP, Goo JM, Lee KS, Leung ANC, Mayo JR, et al. Guidelines for management of incidental pulmonary nodules detected on CT images: from the fleischner society 2017. Radiology. (2017) 284(1):228–43. doi: 10.1148/radiol.2017161659
59. Li M, Shen G, Gao F, Zheng X, Hua Y, Xiao L. CT-guided fine-needle localization of ground-glass nodules in re-aerated lung specimens: localization of solitary small nodules or multiple nodules within the same lobe. Diagn Interv Radiol. (2015) 21(5):391–6. doi: 10.5152/dir.2015.14516
60. Mikhak Z, Pedersen PC. Acoustic attenuation properties of the lung: an open question. Ultrasound Med Biol. (2002) 28(9):1209–16. doi: 10.1016/s0301-5629(02)00561-6
61. Suzuki K, Nagai K, Yoshida J, Ohmatsu H, Takahashi K, Nishimura M, et al. Video-assisted thoracoscopic surgery for small indeterminate pulmonary nodules: indications for preoperative marking. Chest. (1999) 115(2):563–8. doi: 10.1378/chest.115.2.563
62. Hu J, Zhang C, Sun L. Localization of small pulmonary nodules for videothoracoscopic surgery. ANZ J Surg. (2006) 76(7):649–51. doi: 10.1111/j.1445-2197.2006.03790.x
63. Schauer MI, Jung EM, Platz Batista da Silva N, Akers M, Loch E, Markowiak T, et al. Intraoperative contrast-enhanced ultrasonography (Io-CEUS) in minimally invasive thoracic surgery for characterization of pulmonary tumours: a clinical feasibility study. Cancers (Basel). (2023) 15:3854. doi: 10.3390/cancers15153854
64. Yamamoto M, Takeo M, Meguro F, Ishikawa T. Sonographic evaluation for peripheral pulmonary nodules during video-assisted thoracoscopic surgery. Surg Endosc. (2003) 17(5):825–7. doi: 10.1007/s00464-002-8900-0
65. Lesser TG. Endothoracic sonography improves the estimation of operability in locally advanced lung cancer. Ann Thorac Surg. (2010) 90(1):217–21. doi: 10.1016/j.athoracsur.2010.03.072
66. Langiano N, Fiorelli S, Deana C, Baroselli A, Bignami EG, Matellon C, et al. Airway management in anesthesia for thoracic surgery: a “real life” observational study. J Thorac Dis. (2019) 11(8):3257–69. doi: 10.21037/jtd.2019.08.57
67. Liu S, Mao Y, Qiu P, Faridovich KA, Dong Y. Airway rupture caused by double-lumen tubes: a review of 187 cases. Anesth Analg. (2020) 131(5):1485–90. doi: 10.1213/ANE.0000000000004669
68. Ceylan KC, Kaya SO, Samancilar O, Usluer O, Gursoy S, Ucvet A. Intraoperative management of tracheobronchial rupture after double-lumen tube intubation. Surg Today. (2012) 43(7):757–62. doi: 10.1007/s00595-012-0315-5
69. Shah SB, Hariharan U, Chawla R. Choosing the correct-sized adult double-lumen tube: quest for the holy grail. Ann Card Anaesth. (2023) 26(2):124–32. doi: 10.4103/aca.aca_140_22
70. Roldi E, Inghileri P, Dransart-Raye O, Mongodi S, Guinot P-G, Mojoli F, et al. Use of tracheal ultrasound combined with clinical parameters to select left double-lumen tube size: a prospective observational study. Eur J Anaesthesiol. (2019) 36(3):215–20. doi: 10.1097/EJA.0000000000000939
71. Sustić A, Miletić D, Protić A, Ivancić A, Cicvarić T. Can ultrasound be useful for predicting the size of a left double-lumen bronchial tube? Tracheal width as measured by ultrasonography versus computed tomography. J Clin Anesth. (2008) 20(4):247–52. doi: 10.1016/j.jclinane.2007.11.002
72. Diaz NGA. A prospective comparative study to evaluate the utility of lung ultrasonography to improve the accuracy of traditional clinical methods to confirm position of left sided double lumen tube in elective thoracic surgeries. Indian J Anaesth. (2016) 60(3):226–7. doi: 10.4103/0019-5049.177880
73. Acosta CM, Maidana GA, Jacovitti D, Belaunzarán A, Cereceda S, Rae E, et al. Accuracy of transthoracic lung ultrasound for diagnosing anesthesia-induced atelectasis in children. Anesthesiology. (2014) 120(6):1370–9. doi: 10.1097/ALN.0000000000000231
74. Monastesse A, Girard F, Massicotte N, Chartrand-Lefebvre C, Girard M. Lung ultrasonography for the assessment of perioperative atelectasis: a pilot feasibility study. Anesth Analg. (2017) 124(2):494–504. doi: 10.1213/ANE.0000000000001603
75. Ford JW, Heiberg J, Brennan AP, Royse CF, Canty DJ, El-Ansary D, et al. A pilot assessment of 3 point-of-care strategies for diagnosis of perioperative lung pathology. Anesth Analg. (2017) 124(3):734–42. doi: 10.1213/ANE.0000000000001726
76. Sunohara M, Maeda A, Nakanishi Y, Amano E, Okada T, Shibuya H. Ultrasound for perioperative lung monitoring of patients undergoing thoracic surgery with one-lung ventilation. Arch Anesthesiol Crit Care. (2023) 9(3):220–6. doi: 10.18502/aacc.v9i3.13117
77. Terkawi AS, Karakitsos D, Elbarbary M, Blaivas M, Durieux ME. Ultrasound for the anesthesiologists: present and future. Sci World J. (2013) 2013:683685. doi: 10.1155/2013/683685
78. Lichtenstein DA. Lung ultrasound in the critically ill. Ann Intensive Care. (2014) 4(1):1. doi: 10.1186/2110-5820-4-1
79. Girard M, Généreux V, Monastesse A. Lung ultrasonography for the detection of anesthesia-induced lung atelectasis. Anesthesiology. (2015) 122(1):213–4. doi: 10.1097/ALN.0000000000000499
80. Bastone SA, Patirelis A, Luppichini M, Ambrogi V. Ultrasound for intra-operative detection of peri-centimetric pulmonary nodules in uniportal video-assisted thoracic surgery (VATS): a comparison with conventional techniques in multiportal VATS. J Clin Med. (2024) 13(15):4448. doi: 10.3390/jcm13154448
81. Messina G, Bove M, Natale G, Noro A, Martone M, Opromolla G, et al. Ultrasound location of ground-glass opacity during thoracoscopic surgery. Interact Cardiovasc Thorac Surg. (2022) 35(6):ivac234. doi: 10.1093/icvts/ivac234
Keywords: VATS-US, pulmonary nodules, echogenic pattern, nodule identification, nodule characterization
Citation: González-Suárez S, Grao Roca M, Vivas J-C and Jauregui A (2025) Role of VATS-US in identifying and characterizing pulmonary nodules: a narrative review. Front. Surg. 12:1567390. doi: 10.3389/fsurg.2025.1567390
Received: 27 January 2025; Accepted: 30 April 2025;
Published: 20 May 2025.
Edited by:
Giovanni Vicidomini, University of Campania Luigi Vanvitelli, ItalyCopyright: © 2025 González-Suárez, Grao Roca, Vivas and Jauregui. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susana González-Suárez, c3VzYW5hLmdvbnphbGV6QHVhYi5jYXQ=; c3VzYW5hLmdvbnphbGV6QHZhbGxoZWJyb24uY2F0