 Xiong Lv
Xiong Lv Chun Xiang
Chun Xiang- Plastic Surgery Department, The Quzhou Affiliated Hospital of Wenzhou Medical University, Quzhou People’s Hospital, Quzhou, China
Background: Since 1929, when scientists first identified estrogen in urine and coined the term “sex hormones,” these vital steroid hormones have been recognized for their critical role in tissue repair and wound healing. This is particularly evident in the postoperative recovery of plastic surgery patients. While the effects of sex hormones differ between males and females, their mechanisms in wound healing, angiogenesis, and collagen regulation have drawn significant attention.
Methods: This narrative review synthesizes key literature from four databases including PubMed (up to 2024) focusing on the effects of sex hormones on healing after plastic surgery.Key terms such as “sex hormones,” “tissue repair,” and “postoperative recovery” were used. The analysis highlights the differential roles of estrogen and testosterone in skin healing, angiogenesis, and inflammatory responses. Additionally, it explores the effects of sex, age, and hormone replacement therapy (HRT) in transgender patients on surgical outcomes.The main target audience of this article is professional surgeons and endocrinologists, medical students and scientific researchers.
Results: Existing evidence suggests that estrogen enhances wound healing by upregulating vascular endothelial growth factor (VEGF), stimulating angiogenesis, and playing a pivotal role in collagen regulation. Testosterone may influence fibroblast proliferation and angiogenesis, although its effects vary by sex and age. Postmenopausal women exhibit diminished healing capacity due to decreased estrogen levels, whereas transgender patients undergoing HRT show improved postoperative recovery.
Conclusion: Sex hormones significantly influence postoperative recovery in plastic surgery. The distinct mechanisms of estrogen and testosterone in wound healing provide valuable insights for personalized medical approaches, optimizing surgical outcomes across diverse patient populations.
Introduction
Sex hormones, as steroid hormones, have long been studied as critical chemical messengers influencing human physiological functions in the modern era. In addition to defining human sex characteristics, sex hormones play a crucial role in systemic metabolic regulation. Estrogens promote protein synthesis and cell proliferation in target tissues through estrogen receptors (such as ERα/β) and membrane-associated signaling pathways (1) [Level D]. In the skin, estrogen stimulates fibroblasts to synthesize collagen by upregulating the expression of transforming growth factor-β (TGF-β) (2). Similarly, testosterone activates protein synthesis pathways by binding to androgen receptors (AR), enhancing the efficiency of protein synthesis in muscle and skin cells while simultaneously inhibiting protein breakdown (3, 4). These anabolic effects provide a physiological basis for the role of sex hormones in postoperative repair.Sara Merlo et al. described how selectively activating Estrogen Receptor beta(ER β) might positively influence wound healing (5), a factor of paramount importance in plastic surgery.
The human pursuit of beauty has driven the evolution of plastic surgery. As early as 600 BCE in India, texts documented the use of forehead flaps for nasal reconstruction (6). Today, plastic surgery remains a classic treatment for repairing damage to external organs. Concurrently, the rapid development of media and social networks has increased public acceptance of plastic surgery. For instance, in South Korea, there are 13.5 cosmetic surgeries per 1,000 people; in the United States, the number of cosmetic procedures grew to 15.7 million by 2016, marking a substantial increase since the mid-20th century (7, 8).
This review aims to explore the impact of sex hormones on postoperative outcomes in plastic surgery, the mechanisms underlying their effects, and the differences in their roles across various populations and genders. Additionally, it discusses the direction for developing personalized medical approaches to optimize patient care.
Search strategy
We searched four databases (PubMed, Embase, Cochrane Library, and Web of Science) and the Yandex search engine until June 2024. The language was restricted to English and Russian, and the search strategy included the following keywords: “human sex hormones,” “androgens,” “estrogens,” “plastic surgery,” “Gender-affirming surgery,” “sex,” “thrombosis,” “surgical history,” and “nursing.” There were no restrictions on study design. Initially, we screened the titles and abstracts of the articles for relevance to hormonal mechanisms, postoperative healing, and clinical significance. Key articles were selected, and we subsequently evaluated the full-text versions of the remaining articles. Inclusion was determined by the authors and aimed to highlight representative studies of the main findings and controversies in the field. This narrative review does not infer causation nor claim systematic evidence synthesis. The review did not involve the collection of primary patient data; therefore, ethical approval was not required.
Evidence grading approach
As a narrative review, this article synthesizes evidence without formal meta-analysis. To enhance transparency, we categorized findings by evidence strength: Level A: Large human studies(Sample size ≥ 200); Level B: Clinical human studies with limitations(Sample size < 200); Level C: Preclinical/animal data; Level D: Mechanistic hypotheses. Annotated all key conclusions with evidence levels in text, the level of evidence is noted in the table. Clinical recommendations prioritize Level A-B evidence.
Impact and mechanisms of sex hormones on plastic surgery outcomes
Human sex hormones
Sex glands, including the placenta and the zona reticularis of the adrenal cortex, synthesize steroid hormones such as estrogen and testosterone using cholesterol as a precursor. These hormones not only promote sexual organ maturation and maintain secondary sexual characteristics but also play a critical role in tissue repair, as summarized in Figure 1. Testosterone can affect fibroblasts and activate extracellular matrix; Estrogen primarily functions in an endocrine manner, reaching target tissues such as the uterus, vagina, skin, and pelvis via circulation. However, it's also worth noting that in some local microenvironments, like within the ovary, estrogen produced by granulosa cells can act in a paracrine manner to regulate the function of adjacent cells. In these tissues, it binds to specific receptors, playing a significant physiological role in the processes of repair and healing (Figure 1).
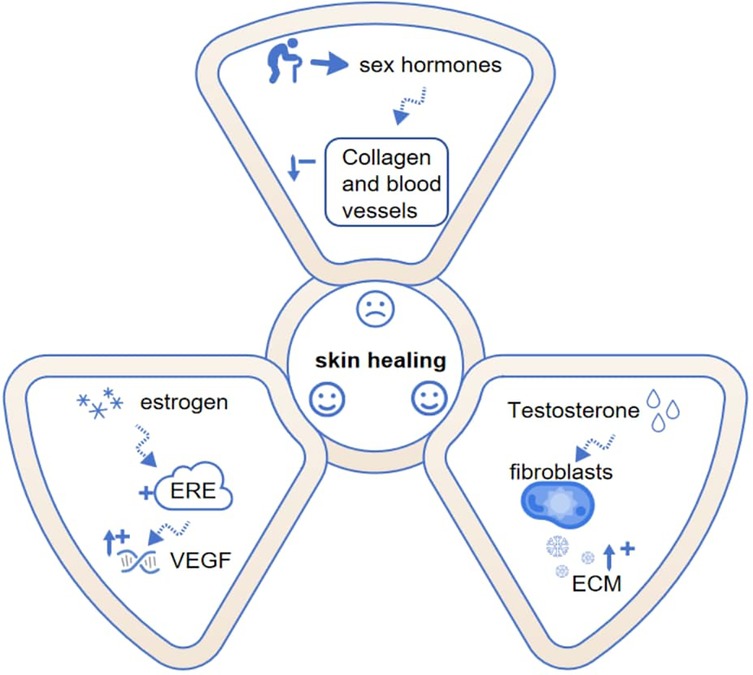
Figure 1. Mechanistic pathways of sex hormones in skin healing. Dashed lines indicate effects, while arrows with “+” and “−” symbols represent enhancement and weakening. Estrogen and testosterone promote healing through distinct mechanisms, though capacity declines with age. ECM, extracellular matrix; VEGF, vascular endothelial growth factor; ERE, estrogen response element.
Tissue healing after plastic surgery
Compared to conventional surgical procedures, plastic surgery plays a pivotal role in improving external appearance, particularly in facial surgeries. Since 2022, the proportion of procedures such as blepharoplasty, facelifts, and rhinoplasty has steadily increased in plastic surgery (9). Facial skin is richly vascularized, with the facial artery (a branch of the external carotid artery) supplying blood to regions like the lips, nose, and eyelids. During surgery, damage to local vascular structures reduces perfusion, creating a hypoxic microenvironment. In response to hypoxia, vascular endothelial growth factor (VEGF) is released, binding VEGFR2 receptors to stimulate endothelial proliferation and vascular permeability (10, 11). This process is initiated by hypoxia-inducible factor 1-alpha (HIF-1α) which accumulates when prolyl hydroxylase (PHD)-mediated degradation is inhibited (12). HIF-1α then translocates to the nucleus, dimerizes with HIF-1β, and activates VEGF expression by binding hypoxia response elements (HREs) in its promoter (13), thereby facilitating angiogenesis. Moreover, VEGF enhances HIF-1α activity through positive feedback, synergistically promoting angiogenesis and tissue healing (14).
Estrogen-related postoperative skin healing
Estrogen rapidly upregulates vascular endothelial growth factor (VEGF) expression, evidenced by a significant increase in VEGF mRNA within one hour of subcutaneous estrogen administration (40 mg/kg) (15). This effect extends transplacentally, as demonstrated by elevated fetal skeletal muscle VEGF and enhanced microvascular development in baboons following maternal estrogen injection (16) [Level C]. The systemic vascular regulatory role of estrogen—mediated through classical nuclear signaling where estrogen dimers activate the VEGF gene's estrogen response element (ERE) (17–19) [Level D]—confirms its mechanistic consistency across multiple target tissues including skin, uterus, heart, and bone.
Collagen is an essential structural matrix of the skin, responsible for regulating its mechanical properties and elasticity (20). Collagen secretion and estrogen levels peak during early adulthood (ages 20–30), demonstrating a strong correlation (21). Postmenopausal women experience a yearly reduction of approximately 1.13% in skin thickness and a 2% annual decline in collagen content (22). Tissue damage from plastic surgery activates matrix metalloproteinase-9 (MMP9), which rises significantly within 12 h post-surgery. MMP9 degrades the extracellular matrix (ECM), facilitating keratinocyte migration and accelerating wound healing (23). However, excessive MMP9 activity may hinder the formation of new tissue (24).
Estrogen protects tissues by inhibiting MMP9 activity, maintaining it at an appropriate level (25). Additionally, estrogen stimulates the production of type I and III collagen and fibrinogen, preserving skin thickness (26). Certain phytochemicals, such as resveratrol, exhibit estrogen-like effects by upregulating Tissue Inhibitor of Metalloproteinases-1(TIMP1), inhibiting MMPs activity, and increasing collagen and elastin synthesis, thus preventing collagen degradation (27–29). However, excessive collagen deposition may lead to scar formation, which is associated with hyperactive fibroblasts and increased vascular density (30, 31).
Androgen-related postoperative skin healing
Testosterone significantly influences tissue healing. A recent study demonstrates that supraphysiological doses accelerate early wound healing in castrated male rats (32) [Level C]. Fibroblasts—key cells secreting extracellular matrix (ECM) to support skin integrity against mechanical stress (33, 34)—interact with ECM via integrins and matrix receptors to regulate cellular responses (35). Testosterone further modulates fibroblast proliferation and ECM remodeling through synergistic actions with insulin-like growth factors (36) [Level D]. This dynamic balance underpins testosterone's role in granulation tissue formation, where subsequent angiogenesis is critical (37). Evidence indicates castrated mice exhibit impaired angiogenesis (38) [Level C], while testosterone metabolites (e.g., 17β-estradiol) maintain skin perfusion (39) [Level C], confirming its multifaceted repair function.
Interestingly, different studies have reported conflicting conclusions regarding testosterone's role in wound healing. Some suggest that testosterone may negatively affect tissue repair (40). For instance, older males often heal more slowly than their female counterparts, possibly due to testosterone exacerbating inflammatory responses during healing (41, 42). These findings suggest that testosterone's impact on wound healing may depend on factors such as age, hormone levels, and its regulatory capacity on inflammation.
Plastic surgery reshapes sex hormones
While sex hormones critically influence surgical outcomes, emerging evidence suggests that plastic surgery itself may actively reshape endocrine homeostasis, creating a feedback loop that extends beyond the operating room. Forces work against each other—not only in physics but also in the interplay between sex hormones and plastic surgery. Bariatric surgery exemplifies this interaction. A previous study indicated that women who underwent bariatric surgery (vertical banded gastroplasty) and lost 40% of their initial weight experienced significant reductions in estradiol and total testosterone (43). Another prospective cohort study on bariatric surgery revealed that not only did women's sex hormone levels change post-surgery, but there was also a significant improvement in their sexual arousal, lubrication, desire, and satisfaction. Given that collagen synthesis requires local estrogen intervention, surgery also impacts body shape (44). This outcome may be linked to fat loss and alterations in intestinal hormones. The reduction of adipose tissue diminishes aromatase activity, thereby decreasing the conversion of androgens to estrogens, while surgery modifies the secretion of intestinal hormones (such as glucagon-like peptide-1), which may indirectly regulate sex hormone levels while also affecting appetite (45). Notably, some surgical procedures can reverse hormonal imbalances. Patients with gynecomastia may experience sex hormone imbalances and sexual dysfunction. A 2024 study demonstrated that 32 patients who underwent gynecomastia surgery exhibited significantly decreased estrogen levels post-surgery (p < 0.001), attributed to the removal of excess breast tissue. Simultaneously, the surgery alleviated the embarrassment associated with excessive breast development, thereby significantly enhancing sexual function assessments (46)[Level B]. These research findings underscore the importance of postoperative monitoring of sex hormones and necessitate that doctors consider the impact on patients' sex hormone levels when formulating surgical plans.
Men and women differ in how their skin heals after surgery
The impact of different genders on skin healing is complex, contributing to uncertainties in plastic surgery outcomes. Generally, males of all age groups have thicker skin on average compared to females (47) [Level B]. An earlier study attributed this to higher testosterone levels in males, which promote the production of collagen and elastic fibers in the skin (48). However, another study found that after 24 weeks of topical estrogen application on the face, the natural skin thickness (dermis plus epidermis) of women aged 52–70 increased (49), suggesting that testosterone's positive effect on skin thickness may outweigh that of estrogen.
Regarding skin healing, the mechanisms of testosterone appear to be more intricate than those of estrogen. For example, under the influence of testosterone, males often exhibit faster healing of oral mucosal wounds but slower healing of dermal wounds (50–52)[Level A]. Immune responses play a significant role in this process. In male mice, castration has been shown to markedly accelerate local skin wound healing (53). Similar results were observed in hairless mouse models, likely due to testosterone's suppression of macrophage production of tumor necrosis factor-α(TNF-α), which reduces systemic TNF-α levels and suppresses immune function (54). This immunosuppressive effect directly impacts the immune cell population in the wound, particularly macrophages, prolonging the transition to the proliferative phase and resulting in slower wound healing outcomes (Table 1).
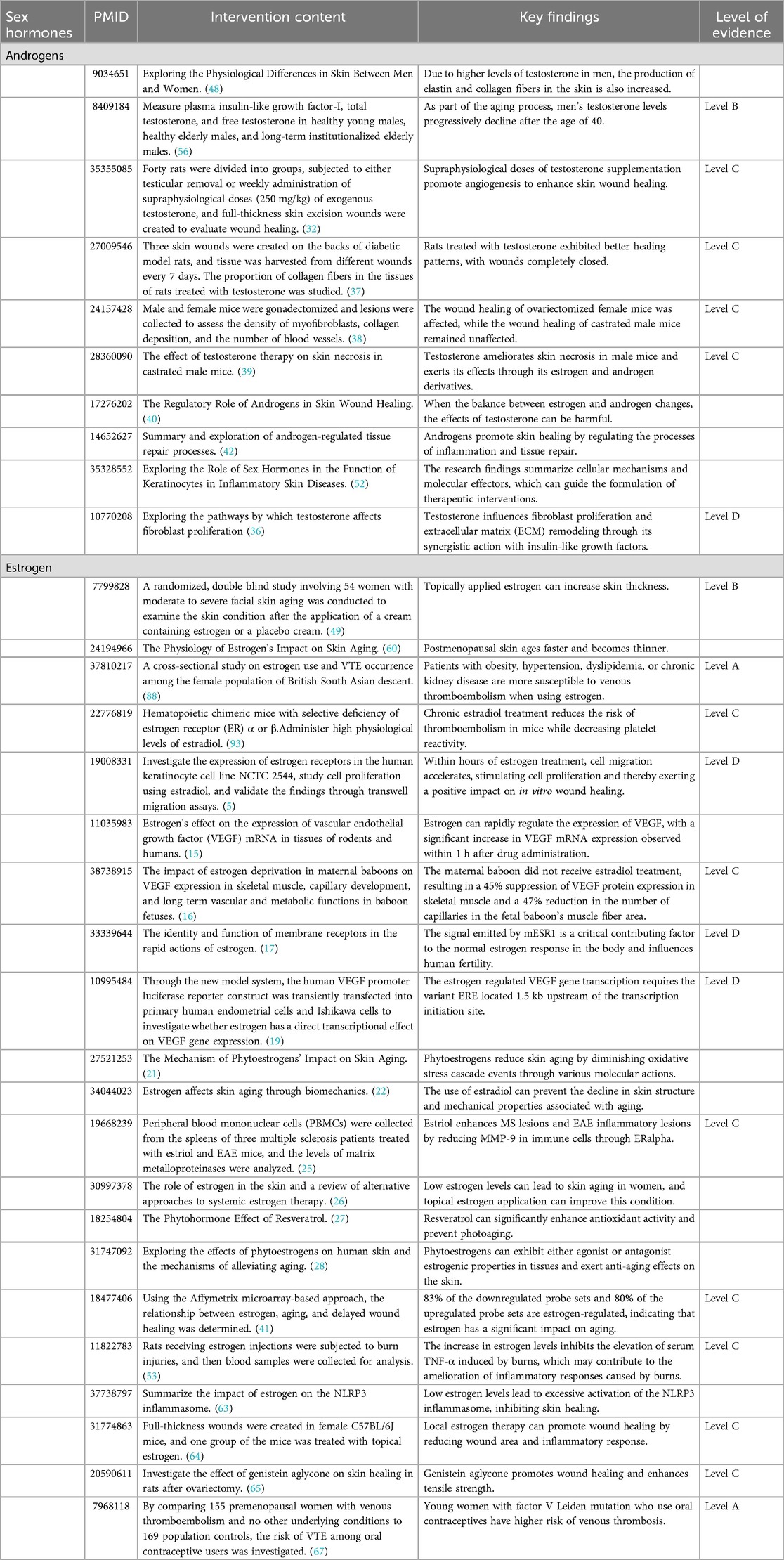
Table 1. Evidence summary: differential effects of androgens and estrogens.
Effects of menopausal estrogen changes on postoperative wound healing
Aging and skin
One of the core objectives of medicine is to enhance human quality of life, with age playing a critical role in this process. Research indicates that wound healing capacity declines with advancing age, which is associated with increased mortality and a higher risk of postoperative complications. For example, studies have shown that the incidence of postoperative complications following free flap transplantation surgery is significantly higher in elderly patients (55), highlighting the profound impact of age on recovery outcomes.
Skin healing during menopause related to sex hormones and nutrition
In males, testosterone levels typically begin to decline gradually after the age of 40, closely linked to the aging process (56). In females, menopause occurs between the ages of 40 and 60, characterized by the depletion of ovarian follicular reserves and reduced ovarian responsiveness to gonadotropins, leading to a significant decrease in sex hormones such as estrogen (57, 58)[Level A]. Postmenopausal women often experience symptoms such as insomnia and mood swings, and the decline in estrogen levels has a profound impact on skin characteristics and skin healing ability (Table 1).
As the most estrogen-responsive non-reproductive organ in the body, the skin becomes thinner and more prone to dryness after menopause (59, 60). These changes are closely associated with reduced sebaceous gland activity and collagen loss. Additionally, low estrogen levels promote the production of interleukin-6 (IL-6) and suppress macrophage anti-inflammatory activity in response to lipopolysaccharide and interferon-γ stimulation, increasing the risk of inflammation. In some cases, low estrogen levels may also lead to overactivation of the NOD-like receptor thermal protein domain associated protein 3(NLRP3) inflammasome, exacerbating inflammatory responses and inhibiting skin healing (61–63). Thus, postmenopausal women face unique challenges in postoperative skin healing.
Several intervention strategies have been explored to address these issues. In addition to traditional systemic hormone replacement therapy (HRT), topical estrogen application has demonstrated promising efficacy. An animal study demonstrated that, for full-thickness wounds approximately 4 mm in diameter in 80-week-old female mice, the elderly group treated with topical estrogen exhibited significant advantages over the elderly group treated with vehicle wound therapy. This treatment notably reduced the wound area and inflammation, thereby accelerating the wound healing process (64) [Level C]. Moreover, phytoestrogens, such as genistein, have been identified for their anti-inflammatory properties and are thought to effectively improve wound healing in women with declining estrogen levels. Even at low doses, genistein significantly increases the levels of vascular endothelial growth factor and transforming growth factor-β1 in wounds, while enhancing the skin's resistance to rupture (65) [Level C].
Beyond hormonal interventions, adequate nutritional supplementation is equally essential. Key nutrients such as vitamin C, vitamin E, and omega-3 fatty acids play a vital role in reducing postoperative bruising, swelling, and other adverse reactions (66). However, whether these nutrients synergize with hormonal therapies to further enhance postoperative recovery remains an area requiring further investigation.
Genetic and environmental factors and patient response to hormones
When patients undergo hormone therapy, genetic factors can influence its effectiveness. Research by Vandenbroucke et al. indicates that genetic factors may modulate the beneficial and adverse effects of estrogen. For instance, women with coagulation factor V Leiden mutations who take oral contraceptives face a thrombosis risk about 30 times higher than that of non-carriers not using such contraceptives (67) [Level B]. Certain gene mutations, like those in the ESR1 gene, can render individuals completely unresponsive to estrogen. These mutations typically impair receptor function, leading to lost estrogen signaling and cellular insensitivity to both endogenous and exogenous estrogen, thus impacting estrogen's effects (68).
Beyond genetics, environmental factors also shape patients' hormone responses in various ways. The natural environment is rife with endocrine—disrupting chemicals (EDCs) that can mimic or interfere with natural hormones. For example, some plastics (e.g., bisphenol A) and pesticides may disrupt estrogen function, potentially affecting wound healing and even causing cancer (69). Human activities impact the environment, which in turn affects us. Studies show that artificial light and electromagnetic waves can influence ovarian steroid hormone secretion, possibly via the hypothalamus—pituitary axis (70). Although research in this area is still limited, based on existing findings, we have reason to believe that external environmental factors can impact hormone therapy effectiveness, warranting more in-depth investigation.
Transgender patients: the effects of hormone replacement therapy HRT on surgical outcomes for gender-confirmation surgeries
Transgender individuals
According to the World Professional Association for Transgender Health (WPATH), transgender patients encompass all individuals whose gender identity is inconsistent with their sex assigned at birth. MTF (Male-to-Female) refers to transgender individuals who identify as female (assigned male at birth); FTM (Female-to-Male) refers to transgender individuals who identify as male (assigned female at birth). In recent years, the number of transgender individuals, particularly among adolescents and young adults, has significantly increased (71). This population often experiences social, psychological, and physiological stressors, leading many to seek gender-affirming medical interventions, including hormone HRT and gender-affirming surgeries.
Hormone therapy for transgender individuals
HRT is a cornerstone of transgender healthcare, involving the administration of exogenous hormones (such as estrogen or testosterone) to align physical characteristics with an individual's gender identity. For male-to-female (MTF) patients, estrogen and anti-androgens are the primary treatments. Estrogen binds to estrogen receptors in the body, promoting breast development and other feminizing characteristics, while anti-androgens inhibit testosterone activity, reducing masculine traits (72). For female-to-male (FTM) patients, testosterone therapy binds to androgen receptors, activating the expression of genes associated with masculinization and promoting the development of male secondary sexual characteristics. Additionally, estrogen inhibitors are used to suppress the effects of endogenous estrogen, further aiding in masculinization (73).
Impact of sex hormones in gender-affirming surgery patients
Gender-affirming surgery, defined as surgery aimed at reconciling physiology with gender identity (e.g., mastectomy, phalloplasty), presents unique physiological demands, with preoperative hormone replacement therapy (HRT) playing a key role in optimizing surgical outcomes by regulating tissue quality and enhancing postoperative healing. Preoperative Hormonal Preparation: HRT is essential for aligning patients' hormonal status with surgical goals. In male-to-female (MTF) patients, estrogen is associated with breast tissue development and increases dermal thickness and elasticity, which are critical for procedures requiring precise skin incisions (e.g., breast augmentation) (74). In female-to-male (FTM) patients, testosterone correlates with muscle hypertrophy and extracellular matrix (ECM) remodeling, thereby improving structural integrity during phalloplasty. Animal models have demonstrated that testosterone supplementation at supraphysiological doses can improve and accelerate granulation tissue maturation, promote early-stage skin wound healing, and enhance granulation tissue maturation (32) [Level C]. Furthermore, clinical studies have reported a lower rate of wound dehiscence in FTM patients receiving testosterone HRT, which is attributed to enhanced fibroblast activity (75).
Postoperative Healing and Recovery: Hormone Replacement Therapy (HRT) sustains benefits during recovery by improving tissue perfusion and reducing inflammation. Estrogen is linked to microvascular perfusion at surgical sites, thereby reducing the risk of necrosis. For instance, male-to-female (MTF) patients undergoing mastectomy while on HRT exhibit accelerated healing due to improved oxygenation and nutrient delivery (76, 77). Testosterone, on the other hand, suppresses inflammatory cytokines (e.g., TNF-α) in female-to-male (FTM) patients, facilitating a smoother transition to the proliferative healing phase (78) (Table 2).
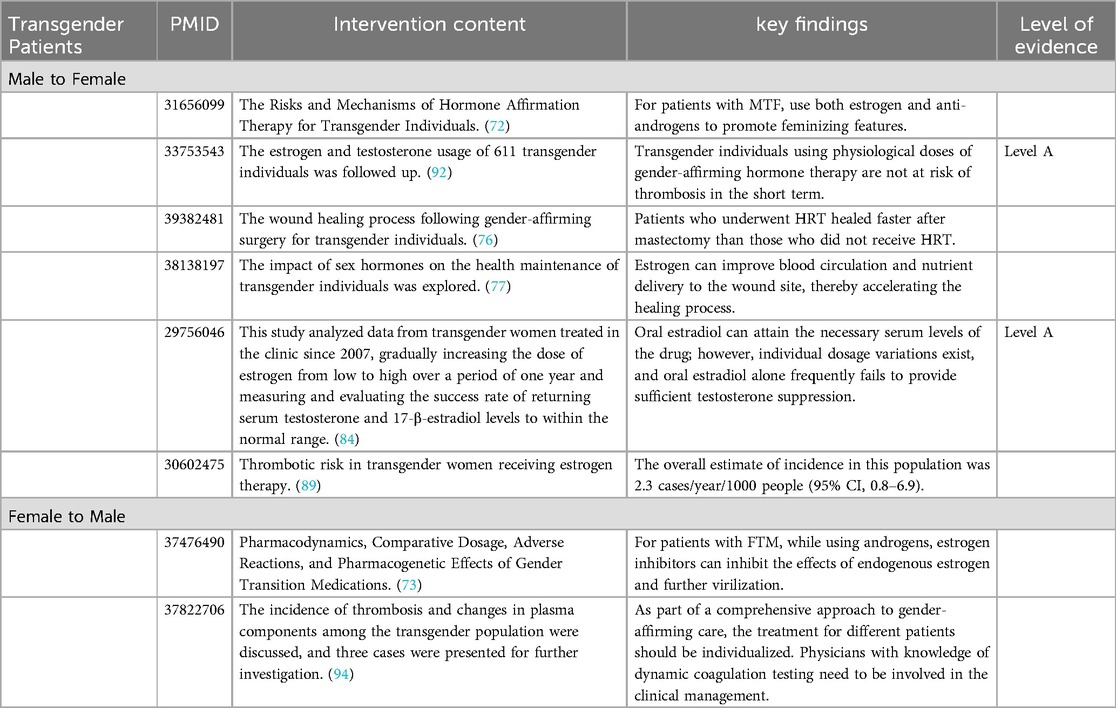
Table 2. Characteristics of transgender patients (MTF/FTM).
Risk-benefit considerations: Although HRT can enhance recovery efficacy, its associated risks necessitate personalized management. Patients undergoing transgender surgery or other specialized surgical procedures are often in a hypercoagulable state due to factors such as postoperative bed rest, slow blood flow, and surgical trauma. Prolonged use of sex hormones may further elevate the risk of thromboembolism (e.g., pulmonary embolism). Therefore, preoperative evaluation, medication adjustment, and postoperative anticoagulation therapy are essential for these patients.
Long-term outcomes of hormone therapy
In addition to its physical benefits, HRT significantly improves psychological well-being. Many patients report enhanced emotional health and social functioning after initiating HRT, with marked improvements observed within six months of starting treatment (79) [Level B]. HRT also effectively alleviates gender dysphoria, helping patients achieve a greater sense of self-alignment. Studies have shown that patients receiving HRT report significantly higher body image satisfaction and lower levels of gender-related anxiety compared to those who do not undergo HRT (80). Among transgender and nonbinary adolescents, HRT suggests a protective psychological effect, significantly reducing suicide risk (81).
Overall, HRT not only facilitates the physiological preparation and recovery from gender-affirming surgeries but also enhances patients' psychological health and overall quality of life. This comprehensive treatment approach improves surgical success rates and significantly enriches the long-term life experiences of transgender individuals. However, further research is warranted to evaluate the adverse effects and long-term outcomes of HRT.
It should be pointed out that varying hormone treatment plans and treatment durations can impact surgical results. Appropriately arranged hormone therapy can keep sex hormone levels within the normal range following gender confirmation surgery while curbing the body's natural production of sex hormones (82). Generally, transgender women need to use estrogen for an extended period to maintain typical female characteristics. The recommended oral dose of 17-β estradiol for transgender women who have not had an orchiectomy is around 2–6 mg (83, 84), whereas patients who have had the surgery can take about 1–5 mg, which shows that individual differences lead to differences in hormone therapy. In addition to dosage, the length of hormone treatment can influence self-identity after gender transition, such as the transgender voice. Even though some transgender men rely on surgery to address physiological changes, the anatomical structure of their larynx has not changed, and there is no significant change in the resonance and pitch of their voice (85). Prolonging the duration of hormone treatment helps improve this issue. A study on the self-perception of voice in transgender individuals showed that after 12 months of testosterone treatment, the pitch of transgender men decreased and produced a significant masculinization effect (86). Overall, these findings indicate that when conducting hormone therapy, changes in treatment plans, treatment duration, or individual metabolic differences must be considered, all of which can significantly impact surgical outcomes.
Adverse effects of hormone therapy
Hormone therapy, while effective in many cases, is not without its drawbacks. A significant concern is the potential for adverse effects, which can include fatigue, loss of libido, and digestive system disorders. One of the most severe side effects is thromboembolism induced by estrogen. In general, patients undergoing abdominal plastic surgery, particularly those with obesity and longer operating times, face an increased risk of deep vein thrombosis (DVT). This risk is associated with hypercoagulability and potential flap failure. Treatment with a specified dose of enoxaparin has been shown to reduce the risk of venous thromboembolism (87). However, the use of estrogen in patients may complicate this scenario. A recent cross—sectional study of women in the British—South Asian cohort found that women with underlying conditions such as obesity, hypertension, and chronic kidney disease had an increased risk of venous thromboembolism when using estrogen (88). This finding is consistent with a previous large-scale case-control study, suggesting that estrogen may be an independent risk factor for venous thromboembolism.
For transgender patients, the risks associated with hormone therapy are particularly noteworthy. Transgender women who receive estrogen treatment are at a higher risk of thromboembolism due to the long-term nature of their hormone therapy. A meta-analysis has shown that transgender women receiving estrogen replacement therapy have a higher risk of venous thromboembolism (89). Combined oral contraceptives (COCs) and systemic hormone replacement therapy (HRT) significantly increase the risk of deep vein thrombosis (DVT) by 2–3 times, primarily due to the effects of estrogen on the synthesis of coagulation factors in the liver (90, 91). Patients who are taking oral contraceptives and require elective surgery, along with prolonged bed rest, may face an elevated risk of thrombosis. Therefore, it is essential to discontinue the use of oral contraceptives three to four weeks prior to surgery to mitigate the risk of pulmonary embolism and mortality. In contrast, existing case reports and retrospective studies have indicated that the use of testosterone in transgender men does not appear to increase the risk of thrombosis (92). Interestingly, an animal experiment once demonstrated that chronic estradiol treatment could protect mice from thromboembolism by reducing platelet reactivity (93) [Level C]. This finding suggests that estrogen may have some unrecognized effects on thromboembolism. We can use in vitro coagulation data to help manage thromboembolic risk in transgender individuals (94).
In summary, while hormone therapy has significant benefits for wound healing and skin regeneration, the potential side effects, especially the risk of thromboembolism associated with estrogen use, should be carefully considered. Future research should continue to explore strategies to minimize these side effects and ensure the safe and effective use of hormone therapy.
Gender-affirming surgery patients affected by lack of information
Despite the growing awareness of gender-affirming surgery, patients continue to experience significant information gaps. This lack of knowledge arises from systemic barriers, including unreliable information sources and insufficient communication with healthcare providers. A recent evaluation of 20 medical websites utilizing a modified EQIP scale yielded an average score of 22.5, which falls short of the standard score of 26. This finding highlights critical deficiencies: only 10% of the websites provided detailed descriptions of the surgical process, associated risks, and potential complications, leaving patients ill-equipped to navigate the challenges of postoperative recovery. Furthermore, only 15% of the websites referenced peer-reviewed studies, which diminishes their credibility. These shortcomings exacerbate the existing barriers faced by transgender patients (95). The Internet should not be relied upon as a primary source of medical information. It is essential for healthcare providers to elucidate the complexities of gender-affirming surgery to patients, while the information available online must be meticulously curated and vetted by experts. Reliable data, articulated in clear language, should be presented on online platforms. Comprehensive information regarding complications should also be included to ensure patients have a complete understanding. Only in this manner can patients access high-quality information that supports their decision-making and promotes appropriate use of Internet resources.
Research heterogeneity, limitations, and future directions
This narrative review aims to synthesize key ideas rather than systematically assess all available evidence. The selection of studies was based on their relevance to the topic and the authors' judgment, consequently, the literature search was not exhaustive and may have been subject to selection bias, potentially affecting the interpretation of the findings. Firstly, differences existed in the patient demographics across the studies, encompassing variations in age, gender, and baseline health conditions. Such disparities can impact the broader applicability of the results, as different patient populations may exhibit distinct responses to hormone therapy. For instance, younger patients may demonstrate differing hormonal levels and recovery capacities in comparison to older patients, which might interact with the effects of hormonal treatment. Additionally, the surgical techniques utilized were not consistent, with some studies favoring minimally invasive methods while others employed traditional open surgical techniques. The level of tissue trauma and inflammatory reaction associated with varying surgical strategies can affect postoperative recovery and the effectiveness of hormone therapy. Minimally invasive surgery may result in less tissue damage and a quicker recovery, which could modify the impact of hormone therapy on the healing process. Finally, the ways in which hormones were administered varied among studies, including routes like oral, topical, and injectable formulations. The method of hormone delivery can affect their absorption, distribution, and metabolism, ultimately influencing the treatment outcomes. For example, topical administration might provide more localized effects, while oral routes could lead to systemic responses that affect the entire body. This research presents several limitations: most of the cited studies are correlational and do not establish direct causal relationships. The causal effects of hormones on surgical outcomes warrant further investigation. Confounding factors, such as baseline health, surgical techniques, and variations in immune responses, may interact with hormonal treatments and influence the results. It is important to note that the potential cumulative effects of long-term hormone treatment on wound healing, immune response, and tissue integrity warrant further investigation. Future studies should address these limitations by employing well-designed prospective cohort studies and randomized controlled trials to determine the direct effects of hormones. While we graded evidence quality using a narrative approach, future systematic reviews with standardized tools (e.g., GRADE) may provide higher certainty for clinical guidance. Additionally, studies should control for confounding factors and focus on differences in patient responses based on genetic and environmental influences. Genetic variations and environmental factors, including diet, lifestyle, and exposure to toxins, can significantly affect hormone metabolism and response. Finally, research is needed to investigate the impact of different surgical techniques and hormone administration methods on healing to identify the most effective strategies. In summary, while this review provides insights into the role of hormones in postoperative healing, significant limitations persist. Future research should aim to establish causality, understand variations in patient responses, and explore different surgical and hormonal approaches to enhance the quality of evidence and treatment protocols.
Conclusion
Current evidence suggests sex hormones significantly influence plastic surgery recovery through distinct biological pathways. Topical estrogen formulations (e.g., 17β-estradiol gel) may help counteract collagen depletion and enhance angiogenesis in menopausal and transgender patients. Testosterone's effects appear context-dependent: while potentially beneficial for granulation tissue maturation in phalloplasty, its pro-inflammatory tendencies in elderly males could warrant consideration of targeted anti-androgen strategies. Given documented thrombotic risks with estrogen, preoperative hormonal assessment combined with enoxaparin prophylaxis might be prudent for high-risk surgical cohorts.
Potential future clinical approaches could explore: rapid hormone receptor assays for reconstruction planning, adaptable hormone therapy regimens, and nutrient combinations like genistein/ascorbate to support tissue repair. Research gaps highlight the need for better mapping of cutaneous hormone receptors and integration of endocrine biomarkers into surgical planning.
These findings imply surgeons should consider endocrine profiles during treatment planning. Attention to these biological factors may contribute to improved functional and aesthetic outcomes beyond basic wound healing.
Author contributions
XL: Data curation, Methodology, Visualization, Writing – original draft. CX: Data curation, Formal analysis, Methodology, Writing – original draft. YZ: Methodology, Project administration, Resources, Writing – original draft. XL: Data curation, Formal analysis, Software, Writing – original draft. WZ: Formal analysis, Investigation, Validation, Writing – original draft. JZ: Conceptualization, Project administration, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We thank our colleagues in the plastic surgery and endocrinology departments who provided assistance with this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
HRT, hormone replacement therapy; VEGF, vascular endothelial growth factor; VEGFR2, vascular endothelial growth gactor receptor 2; HIF-1α, hypoxia-inducible factor 1-alpha; PHD, prolyl hydroxylase; HREs, hypoxia response elements; mRNA, messenger RNA; ERE, estrogen response element; MMP9, matrix metalloproteinase-9; ECM, extracellular matrix; TIMP1, tissue Inhibitor of metalloproteinases-1; TNF-α, tumor necrosis factor-α; NLRP3, NOD-like receptor thermal protein domain associated protein 3; MTF, male-to-female; FTM, female-to-male; ER β, estrogen receptor beta.
References
1. Fox EM, Andrade J, Shupnik MA. Novel actions of estrogen to promote proliferation: integration of cytoplasmic and nuclear pathways. Steroids. (2009) 74(7):622–7. doi: 10.1016/j.steroids.2008.10.014
2. Zomer HD, Cooke PS. Targeting estrogen signaling and biosynthesis for aged skin repair. Front Physiol. (2023) 14:1281071. doi: 10.3389/fphys.2023.1281071
3. Slominski A, Zbytek B, Nikolakis G, Manna PR, Skobowiat C, Zmijewski M, et al. Steroidogenesis in the skin: implications for local immune functions. J Steroid Biochem Mol Biol. (2013) 137:107–23. doi: 10.1016/j.jsbmb.2013.02.006
4. Gharahdaghi N, Phillips BE, Szewczyk NJ, Smith K, Wilkinson DJ, Atherton PJ. Links between testosterone, oestrogen, and the growth hormone/insulin-like growth factor axis and resistance exercise muscle adaptations. Front Physiol. (2020) 11:621226. doi: 10.3389/fphys.2020.621226
5. Merlo S, Frasca G, Canonico PL, Sortino MA. Differential involvement of estrogen receptor alpha and estrogen receptor beta in the healing promoting effect of estrogen in human keratinocytes. J Endocrinol. (2009) 200(2):189–97. doi: 10.1677/JOE-08-0442
6. Bouhadana G, Aljerian A, Thibaudeau S. The reconstruction of plastic surgery: a historical perspective on the etymology of plastic and reconstructive surgery. Plast Surg (Oakv). (2023) 31(4):366–70. doi: 10.1177/22925503211064377
7. The international society of aesthetic plastic surgery (ISAPS). Okla Nurse. (2012) 57(1):18. Available online at: https://link.gale.com/apps/doc/A281459684/HRCA?u=anon~deffe14b&sid=sitemap&xid=03d8644e22523920
8. Alotaibi AS. Demographic and cultural differences in the acceptance and pursuit of cosmetic surgery: a systematic literature review. Plast Reconstr Surg Glob Open. (2021) 9(3):e3501. doi: 10.1097/GOX.0000000000003501
9. Aesthetic Society. Aesthetic plastic surgery national databank statistics 2022. Aesthet Surg J. (2023) 43(Suppl 2):1–19. doi: 10.1093/asj/sjad354
10. Hu K, Olsen BR. The roles of vascular endothelial growth factor in bone repair and regeneration. Bone. (2016) 91:30–8. doi: 10.1016/j.bone.2016.06.013
11. Melincovici CS, Boşca AB, Şuşman S, Mărginean M, Mihu C, Istrate M, et al. Vascular endothelial growth factor (VEGF)—key factor in normal and pathological angiogenesis. Rom J Morphol Embryol. (2018) 59(2):455–67.30173249
12. Kuschel A, Simon P, Tug S. Functional regulation of HIF-1α under normoxia–is there more than post-translational regulation? J Cell Physiol. (2012) 227(2):514–24. doi: 10.1002/jcp.22798
13. Muz B, Khan MN, Kiriakidis S, Paleolog EM. Hypoxia. The role of hypoxia and HIF-dependent signalling events in rheumatoid arthritis. Arthritis Res Ther. (2009) 11(1):201. doi: 10.1186/ar2568
14. Ramakrishnan S, Anand V, Roy S. Vascular endothelial growth factor signaling in hypoxia and inflammation. J Neuroimmune Pharmacol. (2014) 9(2):142–60. doi: 10.1007/s11481-014-9531-7
15. Hyder SM, Huang JC, Nawaz Z, Boettger-Tong H, Mäkelä S, Chiappetta C, et al. Regulation of vascular endothelial growth factor expression by estrogens and progestins. Environ Health Perspect. (2000) 108(Suppl 5):785–90. doi: 10.1289/ehp.00108s5785
16. Aberdeen GW, Babischkin JS, Pepe GJ, Albrecht ED. Estrogen stimulates fetal vascular endothelial growth factor expression and microvascularization. J Endocrinol. (2024) 262(1):e0364. doi: 10.1530/JOE-23-0364
17. Cooke PS, Mesa AM, Sirohi VK, Levin ER. Role of nuclear and membrane estrogen signaling pathways in the male and female reproductive tract. Differentiation. (2021) 118:24–33. doi: 10.1016/j.diff.2020.11.002
18. Pagès G, Pouysségur J. Transcriptional regulation of the vascular endothelial growth factor gene–a concert of activating factors. Cardiovasc Res. (2005) 65(3):564–73. doi: 10.1016/j.cardiores.2004.09.032
19. Mueller MD, Vigne JL, Minchenko A, Lebovic DI, Leitman DC, Taylor RN. Regulation of vascular endothelial growth factor (VEGF) gene transcription by estrogen receptors alpha and beta. Proc Natl Acad Sci U S A. (2000) 97(20):10972–7. doi: 10.1073/pnas.200377097
20. Naylor EC, Watson RE, Sherratt MJ. Molecular aspects of skin ageing. Maturitas. (2011) 69(3):249–56. doi: 10.1016/j.maturitas.2011.04.011
21. Lephart ED. Skin aging and oxidative stress: equol’s anti-aging effects via biochemical and molecular mechanisms. Ageing Res Rev. (2016) 31:36–54. doi: 10.1016/j.arr.2016.08.001
22. Wilkinson HN, Hardman MJ. A role for estrogen in skin ageing and dermal biomechanics. Mech Ageing Dev. (2021) 197:111513. doi: 10.1016/j.mad.2021.111513
23. Krejner A, Litwiniuk M, Grzela T. Matrix metalloproteinases in the wound microenvironment: therapeutic perspectives. Chronic Wound Care Manag Res. (2016) 2016(3):29–39. doi: 10.2147/cwcmr.s73819
24. Caley MP, Martins VL, O'Toole EA. Metalloproteinases and wound healing. Adv Wound Care (New Rochelle). (2015) 4(4):225–34. doi: 10.1089/wound.2014.0581
25. Gold SM, Sasidhar MV, Morales LB, Du S, Sicotte NL, Tiwari-Woodruff SK, et al. Estrogen treatment decreases matrix metalloproteinase (MMP)-9 in autoimmune demyelinating disease through estrogen receptor alpha (ERalpha). Lab Invest. (2009) 89(10):1076–83. doi: 10.1038/labinvest.2009.79
26. Rzepecki AK, Murase JE, Juran R, Fabi SG, McLellan BN. Estrogen-deficient skin: the role of topical therapy. Int J Womens Dermatol. (2019) 5(2):85–90. doi: 10.1016/j.ijwd.2019.01.001
27. Baxter RA. Anti-aging properties of resveratrol: review and report of a potent new antioxidant skin care formulation. J Cosmet Dermatol. (2008) 7(1):2–7. doi: 10.1111/j.1473-2165.2008.00354.x
28. Liu T, Li N, Yan YQ, Liu Y, Xiong K, Liu Y, et al. Recent advances in the anti-aging effects of phytoestrogens on collagen, water content, and oxidative stress. Phytother Res. (2020) 34(3):435–47. doi: 10.1002/ptr.6538
29. Lephart ED. Resveratrol, 4′ acetoxy resveratrol, R-equol, racemic equol or S-equol as cosmeceuticals to improve dermal health. Int J Mol Sci. (2017) 18(6):1193. doi: 10.3390/ijms18061193
30. Honvo G, Lengelé L, Charles A, Reginster JY, Bruyère O. Role of collagen derivatives in osteoarthritis and cartilage repair: a systematic scoping review with evidence mapping. Rheumatol Ther. (2020) 7(4):703–40. doi: 10.1007/s40744-020-00240-5
31. Yuan B, Upton Z, Leavesley D, Fan C, Wang XQ. Vascular and collagen target: a rational approach to hypertrophic scar management. Adv Wound Care (New Rochelle). (2021) 12(1):38–55. doi: 10.1089/wound.2020.1348
32. de Paiva Gonçalves V, Steffens JP, Junior CR, Spolidorio LC. Supraphysiological testosterone supplementation improves granulation tissue maturation through angiogenesis in the early phase of a cutaneous wound healing model in rats. Inflamm Res. (2022) 71(4):473–83. doi: 10.1007/s00011-022-01553-7
33. Ustuner O, Anlas C, Bakirel T, Ustun-Alkan F, Diren Sigirci B, Ak S, et al. In vitro evaluation of antioxidant, anti-inflammatory, antimicrobial and wound healing potential of thymus sipyleus boiss subsp rosulans (borbas) jalas. Molecules. (2019) 24(18):3353. doi: 10.3390/molecules24183353
34. Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature. (2008) 453(7193):314–21. doi: 10.1038/nature07039
35. Eckes B, Nischt R, Krieg T. Cell-matrix interactions in dermal repair and scarring. Fibrogenesis Tissue Repair. (2010) 3:4. doi: 10.1186/1755-1536-3-4
36. Yoshizawa A, Clemmons DR. Testosterone and insulin-like growth factor (IGF) I interact in controlling IGF-binding protein production in androgen-responsive foreskin fibroblasts. J Clin Endocrinol Metab. (2000) 85(4):1627–33. doi: 10.1210/jcem.85.4.6517
37. Gonçalves RV, Novaes RD, Sarandy MM, Damasceno EM, da Matta SL, de Gouveia NM, et al. 5α-Dihydrotestosterone enhances wound healing in diabetic rats. Life Sci. (2016) 152:67–75. doi: 10.1016/j.lfs.2016.03.019
38. Romana-Souza B, Assis de Brito TL, Pereira GR, Monte-Alto-Costa A. Gonadal hormones differently modulate cutaneous wound healing of chronically stressed mice. Brain Behav Immun. (2014) 36:101–10. doi: 10.1016/j.bbi.2013.10.015
39. Chenu C, Adlanmerini M, Boudou F, Chantalat E, Guihot AL, Toutain C, et al. Testosterone prevents cutaneous ischemia and necrosis in males through complementary estrogenic and androgenic actions. Arterioscler Thromb Vasc Biol. (2017) 37(5):909–19. doi: 10.1161/ATVBAHA.117.309219
40. Gilliver SC, Ashworth JJ, Ashcroft GS. The hormonal regulation of cutaneous wound healing. Clin Dermatol. (2007) 25(1):56–62. doi: 10.1016/j.clindermatol.2006.09.012
41. Hardman MJ, Ashcroft GS. Estrogen, not intrinsic aging, is the major regulator of delayed human wound healing in the elderly. Genome Biol. (2008) 9(5):R80. doi: 10.1186/gb-2008-9-5-r80
42. Gilliver SC, Wu F, Ashcroft GS. Regulatory roles of androgens in cutaneous wound healing. Thromb Haemost. (2003) 90(6):978–85. doi: 10.1160/TH03-05-0302
43. Bastounis EA, Karayiannakis AJ, Syrigos K, Zbar A, Makri GG, Alexiou D. Sex hormone changes in morbidly obese patients after vertical banded gastroplasty. Eur Surg Res. (1998) 30(1):43–7. doi: 10.1159/000008556
44. Sarwer DB, Spitzer JC, Wadden TA, Mitchell JE, Lancaster K, Courcoulas A, et al. Changes in sexual functioning and sex hormone levels in women following bariatric surgery. JAMA Surg. (2014) 149(1):26–33. doi: 10.1001/jamasurg.2013.5022
45. Holst JJ, Madsbad S, Bojsen-Møller KN, Svane MS, Jørgensen NB, Dirksen C, et al. Mechanisms in bariatric surgery: gut hormones, diabetes resolution, and weight loss. Surg Obes Relat Dis. (2018) 14(5):708–14. doi: 10.1016/j.soard.2018.03.003
46. Akdag T, Akdag A, Ozkan M, Aydın OE. Evaluating the role of gynecomastia surgery in improving sexual function and hormonal profiles. Aesthet Surg J. (2025) 45(6):584–8. doi: 10.1093/asj/sjaf026
47. Sandby-Møller J, Poulsen T, Wulf HC. Epidermal thickness at different body sites: relationship to age, gender, pigmentation, blood content, skin type and smoking habits. Acta Derm Venereol. (2003) 83(6):410–3. doi: 10.1080/00015550310015419
48. Tur E. Physiology of the skin–differences between women and men. Clin Dermatol. (1997) 15(1):5–16. doi: 10.1016/s0738-081x(96)00105-8
49. Creidi P, Faivre B, Agache P, Richard E, Haudiquet V, Sauvanet JP. Effect of a conjugated oestrogen (premarin) cream on ageing facial skin. A comparative study with a placebo cream. Maturitas. (1994) 19(3):211–23. doi: 10.1016/0378-5122(94)90074-4
50. Engeland CG, Bosch JA, Cacioppo JT, Marucha PT. Mucosal wound healing: the roles of age and sex. Arch Surg. (2006) 141(12):1193–7. doi: 10.1001/archsurg.141.12.1193
51. Balikji J, Hoogbergen MM, Garssen J, Roth T, Verster JC. Insomnia complaints and perceived immune fitness in young adults with and without self-reported impaired wound healing. Medicina (Kaunas). (2022) 58(8):1049. doi: 10.3390/medicina58081049
52. Gratton R, Del Vecchio C, Zupin L, Crovella S. Unraveling the role of sex hormones on keratinocyte functions in human inflammatory skin diseases. Int J Mol Sci. (2022) 23(6):3132. doi: 10.3390/ijms23063132
53. Ozveri ES, Bozkurt A, Haklar G, Cetinel S, Arbak S, Yeğen C, et al. Estrogens ameliorate remote organ inflammation induced by burn injury in rats. Inflamm Res. (2001) 50(12):585–91. doi: 10.1007/PL00000238
54. Padgett DA, Loria RM. Endocrine regulation of murine macrophage function: effects of dehydroepiandrosterone, androstenediol, and androstenetriol. J Neuroimmunol. (1998) 84(1):61–8. doi: 10.1016/s0165-5728(97)00244-0
55. Hwang K, Lee JP, Yoo SY, Kim H. Relationships of comorbidities and old age with postoperative complications of head and neck free flaps: a review. J Plast Reconstr Aesthet Surg. (2016) 69(12):1627–35. doi: 10.1016/j.bjps.2016.08.018
56. Abbasi AA, Drinka PJ, Mattson DE, Rudman D. Low circulating levels of insulin-like growth factors and testosterone in chronically institutionalized elderly men. J Am Geriatr Soc. (1993) 41(9):975–82. doi: 10.1111/j.1532-5415.1993.tb06764.x
57. Stuenkel CA, Gompel A. Primary ovarian insufficiency. N Engl J Med. (2023) 388(2):154–63. doi: 10.1056/NEJMcp2116488
58. Zhu D, Chung HF, Dobson AJ, Pandeya N, Giles GG, Bruinsma F, et al. Age at natural menopause and risk of incident cardiovascular disease: a pooled analysis of individual patient data. Lancet Public Health. (2019) 4(11):e553–64. doi: 10.1016/S2468-2667(19)30155-0
59. Hall G, Phillips TJ. Estrogen and skin: the effects of estrogen, menopause, and hormone replacement therapy on the skin. J Am Acad Dermatol. (2005) 53(4):555–68. doi: 10.1016/j.jaad.2004.08.039
60. Thornton MJ. Estrogens and aging skin. Dermatoendocrinol. (2013) 5(2):264–70. doi: 10.4161/derm.23872
61. Vural P, Akgul C, Canbaz M. Effects of hormone replacement therapy on plasma pro-inflammatory and anti-inflammatory cytokines and some bone turnover markers in postmenopausal women. Pharmacol Res. (2006) 54(4):298–302. doi: 10.1016/j.phrs.2006.06.006
62. Toniolo A, Fadini GP, Tedesco S, Cappellari R, Vegeto E, Maggi A, et al. Alternative activation of human macrophages is rescued by estrogen treatment in vitro and impaired by menopausal status. J Clin Endocrinol Metab. (2015) 100(1):E50–8. doi: 10.1210/jc.2014-2751
63. Dong W, Peng Q, Liu Z, Xie Z, Guo X, Li Y, et al. Estrogen plays an important role by influencing the NLRP3 inflammasome. Biomed Pharmacother. (2023) 167:115554. doi: 10.1016/j.biopha.2023.115554
64. Mukai K, Nakajima Y, Asano K, Nakatani T. Topical estrogen application to wounds promotes delayed cutaneous wound healing in 80-week-old female mice. PLoS One. (2019) 14(11):e0225880. doi: 10.1371/journal.pone.0225880
65. Marini H, Polito F, Altavilla D, Irrera N, Minutoli L, Calò M, et al. Genistein aglycone improves skin repair in an incisional model of wound healing: a comparison with raloxifene and oestradiol in ovariectomized rats. Br J Pharmacol. (2010) 160(5):1185–94. doi: 10.1111/j.1476-5381.2010.00758.x
66. Rahm D. A guide to perioperative nutrition. Aesthet Surg J. (2004) 24(4):385–90. doi: 10.1016/j.asj.2004.04.001
67. Vandenbroucke JP, Koster T, Briët E, Reitsma PH, Bertina RM, Rosendaal FR. Increased risk of venous thrombosis in oral-contraceptive users who are carriers of factor V Leiden mutation. Lancet. (1994) 344(8935):1453–7. doi: 10.1016/s0140-6736(94)90286-0
68. Li Y, Hamilton KJ, Perera L, Wang T, Gruzdev A, Jefferson TB. ESR1 mutations associated with estrogen insensitivity syndrome change conformation of ligand-receptor complex and altered transcriptome profile. Endocrinology. (2020) 161(6):bqaa050. doi: 10.1210/endocr/bqaa050
69. Scsukova S, Rollerova E, Bujnakova Mlynarcikova A. Impact of endocrine disrupting chemicals on onset and development of female reproductive disorders and hormone-related cancer. Reprod Biol. (2016) 16(4):243–54. doi: 10.1016/j.repbio.2016.09.001
70. Rannaud-Bartaire P, Demeneix BA, Fini JB. Pressures of the urban environment on the endocrine system: adverse effects and adaptation. Mol Cell Endocrinol. (2024) 583:112125. doi: 10.1016/j.mce.2023.112125
71. Coleman E, Radix AE, Bouman WP, Brown GR, de Vries ALC, Deutsch MB, et al. Standards of care for the health of transgender and gender diverse people, version 8. Int J Transgend Health. (2022) 23(Suppl 1):S1–S259. doi: 10.1080/26895269.2022.2100644
72. Connelly PJ, Marie Freel E, Perry C, Ewan J, Touyz RM, Currie G, et al. Gender-affirming hormone therapy, vascular health and cardiovascular disease in transgender adults. Hypertension. (2019) 74(6):1266–74. doi: 10.1161/HYPERTENSIONAHA.119.13080
73. Sehgal I. Review of adult gender transition medications: mechanisms, efficacy measures, and pharmacogenomic considerations. Front Endocrinol (Lausanne). (2023) 14:1184024. doi: 10.3389/fendo.2023.1184024
74. White Hughto JM, Reisner SL. A systematic review of the effects of hormone therapy on psychological functioning and quality of life in transgender individuals. Transgend Health. (2016) 1(1):21–31. doi: 10.1089/trgh.2015.0008
75. Santos RB, Lemos C, Saraiva M. Gender-affirming hormone therapy: physical and sociopsychological effects, impact and satisfaction. Cureus. (2023) 15(3):e36484. doi: 10.7759/cureus.36484
76. Carroll EF, Rogers C, Summerside M, Cortina CS. Breast care considerations for transgender and gender-diverse patients. Womens Health (Lond). (2024) 20:17455057241289706. doi: 10.1177/17455057241289706
77. Moustakli E, Tsonis O. Exploring hormone therapy effects on reproduction and health in transgender individuals. Medicina (Kaunas). (2023) 59(12):2094. doi: 10.3390/medicina59122094
78. White AA, Lin A, Bickendorf X, Cavve BS, Moore JK, Siafarikas A, et al. Potential immunological effects of gender-affirming hormone therapy in transgender people—an unexplored area of research. Ther Adv Endocrinol Metab. (2022) 13:20420188221139612. doi: 10.1177/20420188221139612
79. Foster Skewis L, Bretherton I, Leemaqz SY, Zajac JD, Cheung AS. Short-term effects of gender-affirming hormone therapy on dysphoria and quality of life in transgender individuals: a prospective controlled study. Front Endocrinol (Lausanne). (2021) 12:717766. doi: 10.3389/fendo.2021.717766
80. Olson-Kennedy J, Chan YM, Garofalo R, Spack N, Chen D, Clark L, et al. Impact of early medical treatment for transgender youth: protocol for the longitudinal, observational trans youth care study. JMIR Res Protoc. (2019) 8(7):e14434. doi: 10.2196/14434
81. Green AE, DeChants JP, Price MN, Davis CK. Association of gender-affirming hormone therapy with depression, thoughts of suicide, and attempted suicide among transgender and nonbinary youth. J Adolesc Health. (2021) 70(4):643–9. doi: 10.1016/j.jadohealth.2021.10.036
82. Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Hassan Murad M. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2017) 102(11):3869–903. doi: 10.1210/jc.2017-01658
83. Korpaisarn S, Safer JD. MON-198 feminizing regimen requirements in transgender females following orchiectomy. J Endocr Soc. (2019) 3(Supplement_1):MON-198. doi: 10.1210/js.2019-mon-198
84. Leinung MC, Feustel PJ, Joseph J. Hormonal treatment of transgender women with oral estradiol. Transgend Health. (2018) 3(1):74–81. doi: 10.1089/trgh.2017.0035
85. Zamponi V, Mazzilli R, Mazzilli F, Fantini M. Effect of sex hormones on human voice physiology: from childhood to senescence. Hormones (Athens). (2021) 20(4):691–6. doi: 10.1007/s42000-021-00298-y
86. Bultynck C, Pas C, Defreyne J, Cosyns M, Heijer Md, T’Sjoen G. Self-perception of voice in transgender persons during cross-sex hormone therapy. Laryngoscope. (2017) 127(12):2796–804. doi: 10.1002/lary.26716
87. Paolini G, Firmani G, Sorotos M, Ninković M, di Pompeo FS. European guidelines on peri-operative venous thromboembolism prophylaxis: first update: chapter 8: plastic surgery. Eur J Anaesthesiol. (2024) 41(8):598–603. doi: 10.1097/EJA.0000000000001998
88. Magavern EF, Smedley D, Caulfield MJ. Factor V Leiden, estrogen, and multimorbidity association with venous thromboembolism in a British-South Asian cohort. iScience. (2023) 26(10):107795. doi: 10.1016/j.isci.2023.107795
89. Khan J, Schmidt RL, Spittal MJ, Goldstein Z, Smock KJ, Greene DN. Venous thrombotic risk in transgender women undergoing estrogen therapy: a systematic review and metaanalysis. Clin Chem. (2019) 65(1):57–66. doi: 10.1373/clinchem.2018.288316
90. Douxfils J, Morimont L, Bouvy C. Oral contraceptives and venous thromboembolism: focus on testing that may enable prediction and assessment of the risk. Semin Thromb Hemost. (2020) 46(8):872–86. doi: 10.1055/s-0040-1714140
91. Shiffman MA. Estrogen and thromboembolic disorders: should patients stop hormones prior to cosmetic surgery? J Womens Health (Larchmt). (2003) 12(9):853–5. doi: 10.1089/154099903770948078
92. Mullins ES, Geer R, Metcalf M, Piccola J, Lane A, Ann EL. Thrombosis risk in transgender adolescents receiving gender-affirming hormone therapy. Pediatrics. (2021) 147(4):e2020023549. doi: 10.1542/peds.2020-023549
93. Valéra MC, Gratacap MP, Gourdy P, Lenfant F, Cabou C, Toutain CE. Chronic estradiol treatment reduces platelet responses and protects mice from thromboembolism through the hematopoietic estrogen receptor α. Blood. (2012) 120(8):1703–12. doi: 10.1182/blood-2012-01-405498
94. Bouck EG, Grinsztejn E, Mcnamara M, Evi X. Thromboembolic risk with gender-affirming hormone therapy: potential role of global coagulation and fibrinolysis assays. Res Pract Thromb Haemost. (2023) 7(6):102197. doi: 10.1016/j.rpth.2023.102197
Keywords: estrogen, testosterone, plastic surgery, skin healing, transgender patients
Citation: Lv X, Xiang C, Zheng Y, Lv X, Zhou W and Zhu J (2025) Impact of sex hormones on postoperative outcomes in plastic surgery: a narrative review. Front. Surg. 12:1587708. doi: 10.3389/fsurg.2025.1587708
Received: 4 March 2025; Accepted: 7 August 2025;
Published: 21 August 2025.
Edited by:
Ming Pei, West Virginia University, United StatesReviewed by:
Guido Firmani, Sapienza University of Rome, ItalyDomenico Tripodi, Sapienza University of Rome, Italy
Copyright: © 2025 Lv, Xiang, Zheng, Lv, Zhou and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiajun Zhu, ODkxNzY4NjA4QHFxLmNvbQ==