 Fırat Mülküt1*
Fırat Mülküt1* Cem Batuhan Ofluoğlu1Mustafa Kağan Başdoğan1İsa Caner Aydın2Osman Akdoğan3Adnan Gündoğdu1İsmail Ege Subaşı1
Cem Batuhan Ofluoğlu1Mustafa Kağan Başdoğan1İsa Caner Aydın2Osman Akdoğan3Adnan Gündoğdu1İsmail Ege Subaşı1
- 1General Surgery Department, Martyr Dr. İlhan Varank Sancaktepe Training and Research Hospital, Dudullu¸ Türkiye
- 2Gastrointestinal Surgery Department, Zonguldak Atatürk State Hospital, Zonguldak, Türkiye
- 3General Surgery Department, Ministry of Health, Keşan State Hospital, Edirne, Türkiye
Background and aim: Gastric cancer is among the commonly occurring cancers worldwide and is one of the leading causes of cancer-related deaths. Malnutrition is an important factor affecting the course of disease and treatment response in gastric cancer patients this study aimed to investigate the effect of the Prognostic Nutritional Index (PNI) on postoperative complications and long-term survival in gastric cancer patients, and to comparatively examine PNI values among different histological subtypes.
Methods: Data from patients who underwent curative surgical resection for gastric cancer between 2014 and 2020 were retrospectively analyzed. PNI values were calculated using the formula: 10 × serum albumin (g/dl) + 0.005 × lymphocyte count (cells/mm3). The optimal cut-off value for PNI was determined through ROC analysis. The relationship between PNI values and clinicopathological features, postoperative complications, 5-year overall survival (OS), and histological subtypes was evaluated.
Results: A total of 220 patients (161 males, 59 females; mean age: 60.63 ± 10.56) were included in the study. The mean PNI value was 47.15 ± 6.07. ROC analysis established an optimal PNI cut-off value of 46.2 (AUC = 0.673, 95% CI: 0.599-0.747, p<0.001; sensitivity 78.8%, specificity 51.9%). Complication rates were significantly higher in the patient group with PNI < 46.2 (p = 0.006). The 5-year OS rate was 30.0%. Patients with low PNI values had significantly shorter survival (log-rank p = 0.001). Major complications were more frequent in patients with low PNI (p = 0.006). Patients diagnosed with signet ring cell carcinoma (SRCC) had significantly lower PNI values compared to other adenocarcinoma subtypes (p = 0.001). PNI values were lower in the presence of perineural invasion (p = 0.005) and lymphovascular invasion (p = 0.032). In multivariate analysis, tumor stage (for Stage I p = 0.01, Stage II p = 0.034, Stage III p = 0.002) and PNI value (p = 0.001) were identified as independent prognostic factors affecting 5-year OS. Conclusion: PNI is an important marker for predicting long-term survival and postoperative complication risk in patients with gastric cancer. The significantly lower PNI values in the SRCC subtype compared to other histological subtypes indicate the necessity of closer monitoring of nutritional status in this patient group. Our results suggest that preoperative PNI assessment could be a valuable parameter in planning patient-specific treatment approaches.
Introduction
Gastric cancer is among the commonly occurring cancers worldwide and is one of the leading causes of cancer-related deaths (1). Malnutrition is an important factor affecting the course of disease and treatment response in gastric cancer patients (2). Biomarkers such as the Prognostic Nutritional Index (PNI) are objective parameters used to assess the nutritional status of patients. PNI reflects the nutritional status of patients based on serum albumin and total lymphocyte count, and recent studies have demonstrated the prognostic and post-operative value of PNI in gastric cancer patients (3). Additionally, signet ring cell gastric cancer (SRCC) constitutes approximately 8%–30% of all gastric cancers and is a subtype with a more aggressive course and poor prognosis. The tendency of SRCC to occur at a younger age, the risk of late diagnosis, and its resistance to treatment necessitate special examination of this subtype (4).
Many patients undergoing gastrectomy for gastric carcinoma experience significant nutritional management challenges upon hospital discharge. The transition from structured hospital nutritional protocols to self-administered dietary care presents considerable difficulties and frequently results in compromised nutritional status. Investigational studies have demonstrated that dietary habit modification is particularly problematic when these individuals cohabitate with family members maintaining conventional nutritional regimens. Pre-operative dietary patterns likely persist into the post-operative period. Despite established evidence regarding the prognostic significance of nutritional status, these persistent behavioral patterns frequently result in patients reverting to previous suboptimal dietary regimens following surgical intervention (3).
It is well established that all cancer patients experience some degree of nutritional impairment, with this effect being particularly pronounced in patients with cancers of the upper digestive tract and pancreas, often due to mechanical impediments to food intake. The metabolic demands of cancer create a competition for nutrients between the tumor and the host, disrupting the normal functioning of the human body. Therefore, comprehensive nutritional assessment and intervention by dedicated nutritionists in oncology units are essential components of cancer care. These specialists can evaluate individual patient needs and establish appropriate nutritional treatment protocols tailored to each patient's specific requirements (5).
In this study, we aimed to investigate the effect of PNI on perioperative complications and prognosis. Additionally, we aimed to determine whether PNI varies according to tumor type by comparing it across histological subtypes.
Materials and methods
Data collection
Data from patients who underwent surgery for gastric cancer between 2014 and 2020 in the general surgery departments that serve as reference centers for their regions were retrospectively reviewed through patient files and electronic medical record systems.
Patients over 18 years of age, with an Eastern Cooperative Oncology Group (ECOG) performance score (6) of 0–2, histopathologically diagnosed with adenocarcinoma, who underwent curative resection, and had blood values within 1 week before surgery or before the start of neoadjuvant therapy were included in the study.
Patients with positive surgical margins, inadequate lymph node dissection, perioperative mortality, additional malignancies, irregular follow-up, missing follow-up or laboratory data, distant metastasis, ECOG performance score ≥3, incomplete neoadjuvant therapy, lack of stage-appropriate adjuvant therapy, non-adenocarcinoma cancers, HER2-positive status receiving immunomodulatory therapy, and active infection at the time of blood collection that could affect inflammatory markers were excluded from the study.
Operated patients were called for follow-up to evaluate physical examination and laboratory parameters by the oncology clinic during the first year, monthly for the first 3–6 months, and then every three months. Computed tomographic imaging covering the thorax and abdomen was performed at the 6th month and 1st year. Endoscopic evaluation was performed at the end of the first year for patients who underwent total gastrectomy, and at the sixth month and first year for those who underwent subtotal gastrectomy. After the 1st year, physical examination and laboratory analysis were performed every 6 months, while endoscopy and imaging were performed annually. In patients with histological findings suggestive of aggressive tumor behavior or surgical margin proximity, examinations were conducted at more frequent intervals on an individual basis.
Patients were examined for age, gender, body mass index (BMI), The American Society of Anesthesiologists (ASA) score (7), comorbidities, histological type of tumor (WHO classification), number of lymph nodes removed, number of positive lymph nodes, tumor location, neoadjuvant therapy status, surgical procedure (total/subtotal gastrectomy), perineural invasion (PeNI), lymphovascular invasion (LVI), follow-up duration, mortality, and laboratory parameters. According to NCCN (National Comprehensive Cancer Network) guidelines, the cancer stage is determined for gastric cancer (8). Tumor size was measured at pathological examination by opening the stomach specimens from greater or lesser curvature depending on the tumor's location. Tumor size was not measured in pathology specimens reported as linitis plastica.
Postoperative complications were systematically documented and classified according to the Clavien-Dindo scoring system, which provides a standardized approach to grading surgical complications based on the therapeutic interventions required to treat them (9). Grade I complications require no pharmacological treatment or only simple medications such as antiemetics or analgesics; Grade II complications require pharmacological intervention beyond those permitted for Grade I; Grade III complications require surgical, endoscopic, or radiological intervention (IIIa without general anesthesia, IIIb with general anesthesia); Grade IV complications are life-threatening and require Intensive Care Unit management. All complications occurring within 30 days of surgery were documented and classified according to these criteria.
When examining the response to neoadjuvant therapy, scores determined according to the modified Ryan scoring system (TRG) in pathology reports were considered (10). Patients with TRG 0-1-2 were categorized as having a response to neoadjuvant therapy, while those with TRG 3 were categorized as having no response.
Neoadjuvant therapy was administered to patients with clinical T3-T4 tumors, lymph node positivity, and locally advanced disease. The 5-Fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) regimen was the preferred treatment protocol. Neoadjuvant therapy was administered for a total of 4 cycles for each patient.
All laboratory data used to calculate preoperative nutritional parameters were obtained within 1 week before surgery or neoadjuvant therapy. The Prognostic Nutritional Index (PNI) was calculated using the following formula: 10 × serum albumin concentration (g/dl) + 0.005 × lymphocyte count (number/mm³) (11).
Ethical approval
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of the Sancaktepe Education and Research Hospital (decision number 2024/365). The requirement for informed consent was waived owing to the retrospective nature of the study.
Statistical analysis
All statistical analyses were performed using the SPSS (Statistical Package for Social Sciences) for Windows 28.0 software. Normality was tested using the Kolmogorov–Smirnov test and graphical methods. As descriptive statistics, mean and standard deviation were used for non-parametric variables. Categorical data were expressed as counts (n) and percentages (%). The Chi-square test was employed for the comparison of two categorical variables. However, when comparing one categorical variable with a numeric value, the Mann–Whitney U test was used for the non-parametric data. Survival analyses of patients were performed using the Kaplan–Meier test. ROC analysis was performed to determine the optimal cut-off value. All statistical calculations were two-sided, and p < 0.05 indicated statistical significance at the confidence level of 95% (p < 0.05).
Results
Data from a total of 373 operated patients were retrospectively screened. Forty-two patients (11.2%) were excluded due to insufficient follow-up and laboratory data, 38 patients (10.2%) due to metastatic disease detected during operation, perioperative mortality, and R1–R2 resection, 31 patients (8.3%) due to ECOG score ≥3 or failure to complete neoadjuvant-adjuvant treatments for any reason, 24 patients (6.4%) due to inadequate lymph node dissection, and 18 patients (4.8%) due to history of a second malignancy and additional organ resection. A total of 220 patients met the inclusion criteria for the study (Figure 1).
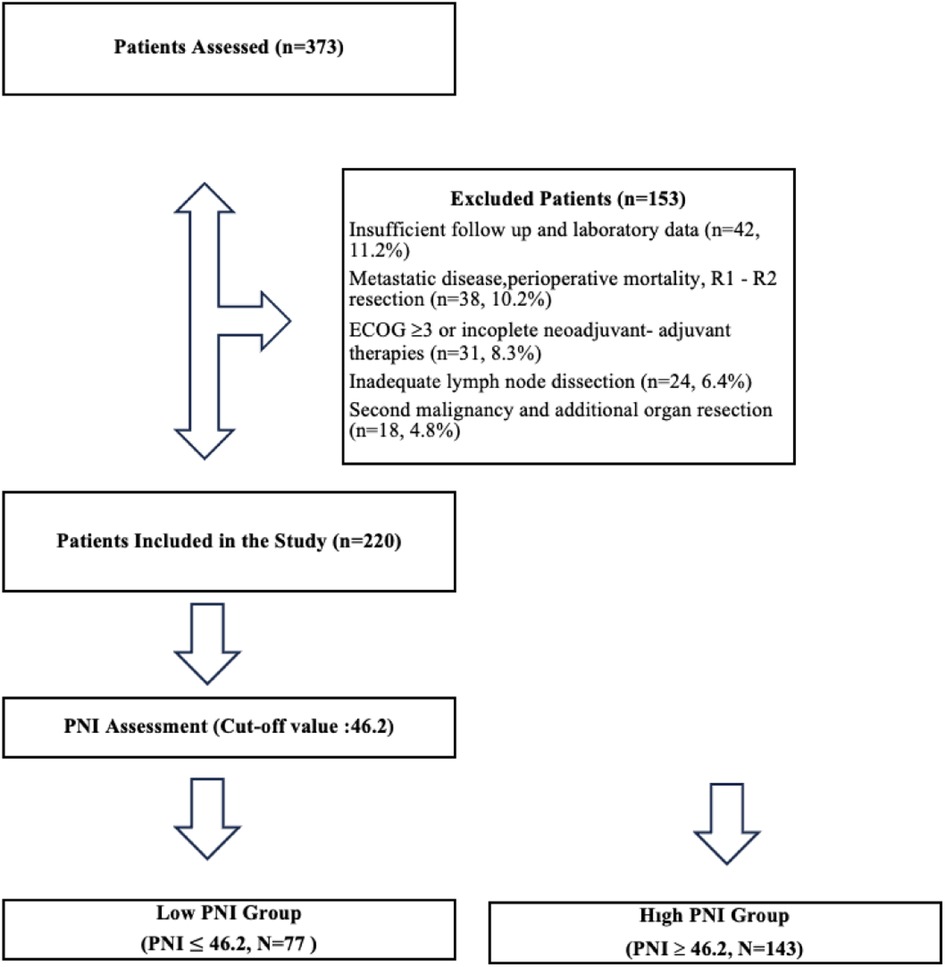
Figure 1. Flow-chart.
According to the normality test, age, BMI, tumor size, number of lymph nodes removed, and PNI values were not normally distributed. The mean age of all patients was 60.63 ± 10.56, BMI was 24.49 ± 3.44, and PNI value was 47.15 ± 6.07.
Of the patients, 73.2% (n = 161) were male and 26.8% (n = 59) were female; 8.2% (n = 18) were ASA 1, 36.8% (n = 81) ASA 2, 51.8% (n = 114) ASA 3, and 3.2% (n = 7) ASA 4; 9.5% (n = 21) were stage 1, 26.4% (n = 58) stage 2, and 64.1% (n = 141) stage 3; 29.5% (n = 65) had hypertension (HT), 27.3% (n = 60) had diabetes mellitus (DM), 6.8% (n = 15) had chronic obstructive pulmonary disease, and 14.1% (n = 31) had coronary artery disease (CAD); 20.9% (n = 46) had SRCC, 12.7% (n = 28) had well-differentiated, 30.5% (n = 67) had moderately differentiated, 29.5% (n = 65) had poorly differentiated, and 6.4% (n = 14) had mucinous adenocarcinoma; 57.3% (n = 126) had PeNI, and 63.9% (n = 140) had LVI. The tumor was located in the upper 1/3 in 33.6% (n = 74) of the patients, in the middle 1/3 in 25.9% (n = 57), and in the lower 1/3 in 35.9% (n = 79). Total gastrectomy was performed in 64.1% (n = 141) and subtotal gastrectomy in 35.9% (n = 79) (Table 1).
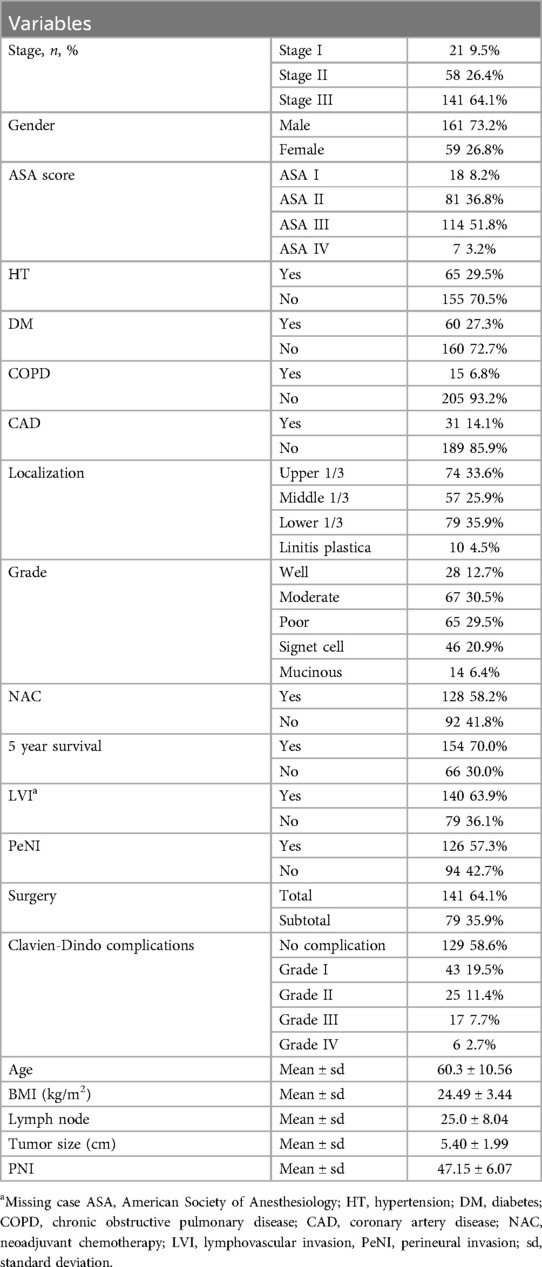
Table 1. Demographic and clinicopathologic distribution of patients.
In the ROC analysis performed to find the cut-off value for evaluating 5-year overall survival (OS) for PNI, the PNI value was found to be 46.2 (AUC = 0.673, 95%CI: 0.599–0.747, p < 0.001; sensitivity 78.8%, specificity 51.9%) (Figure 2).
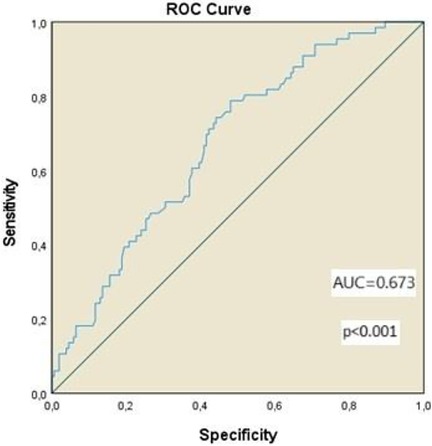
Figure 2. ROC curve of PNI for 5-year OS. (AUC = 0.673, 95%CI: 0.599–0.747, p < 0.001; sensitivity 78.8%, specificity 51.9%).
The 5-year survival rate was found to be 30.0%. When comparing the survival of patients with PNI values less than 46.2 and those greater than 46.2, it was observed that survival was worse in patients with low nutritional index (log rank p = 0.001) (Figure 3).
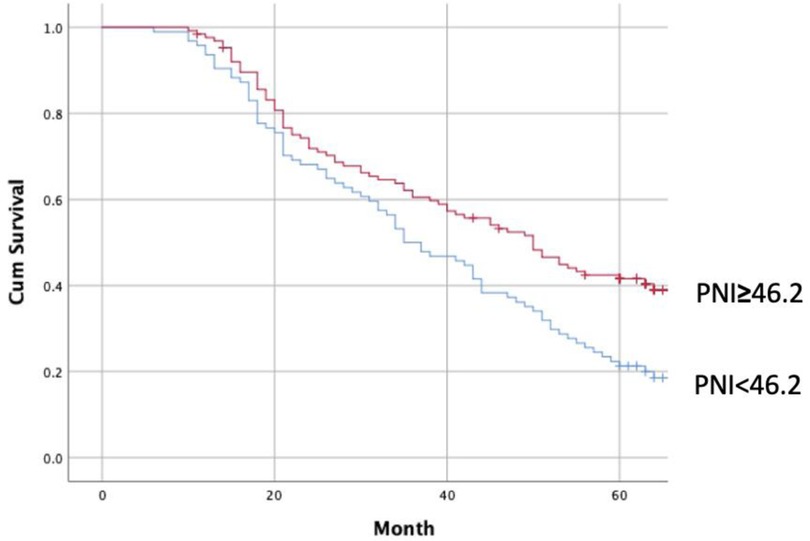
Figure 3. Survival analysis between Low and high PNI groups. (Log Rank p:0.001).
In the examination conducted by dividing patients with PNI values less than 46.2 as poor and those with values greater than 46.2 as good nutritional status into two categories, it was observed that PNI was lower in the group where PeNI and LVI were more common (p values 0.005 and 0.032, respectively). Patients with SRCC had statistically lower PNI compared to other adenocarcinoma types (p = 0.001). Between the two groups, 5-year survival was statistically worse in the low PNI group (p < 0.001). There was no statistically significant difference between response to neoadjuvant therapy and PNI value in patients receiving neoadjuvant therapy (p = 0.095). When comparing complications according to the Clavien-Dindo classification, Grade 1 (23.4% vs. 16.7%), Grade 2 (16.0% vs. 7.9%), Grade 3 (11.7% vs. 4.8%), and Grade 4 complication rates were higher in the low PNI group, whereas patients without complications were higher among the high PNI group (44.7% vs. 69.0%) (p = 0.006) (Table 2).
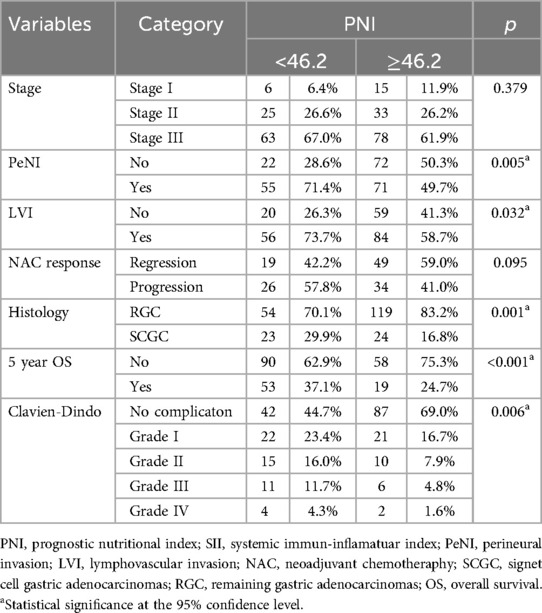
Table 2. Evaluation of patients Due to Cut-off value of PNI.
In the logistic regression analysis based on 5-year survival, while chronic obstructive pulmonary disease (COPD), tumor stage, LVI, PeNI, histological type being SRCC, and low PNI values were significant according to univariate analysis, in multivariate analysis, tumor stage (for stage I p = 0.01, for stage 2 p = 0.034, and for stage 3 p = 0.002) and PNI value (p = 0.001) stood out as the only parameters affecting 5-year survival (Table 3).
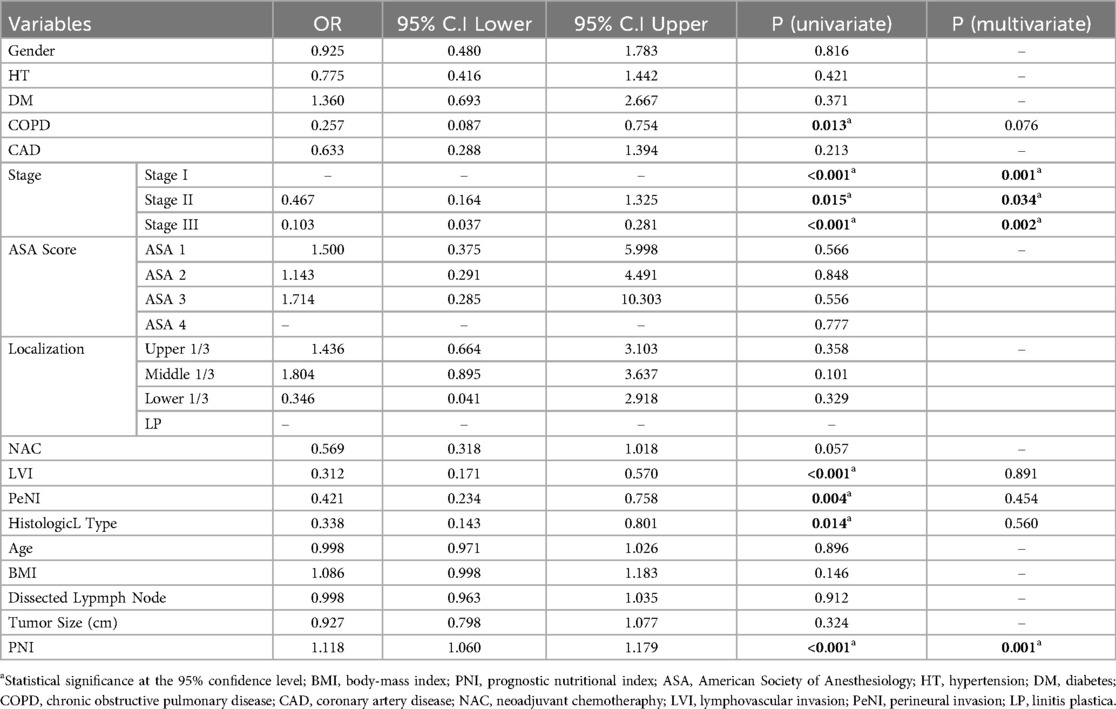
Table 3. Logistic regression analysis for 5-year overall survival.
Discussion
Gastric cancer is a complex clinical condition requiring the development of individualized strategies in treatment approaches, especially considering the factor of malnutrition. This study demonstrates not only the value of the Prognostic Nutritional Index (PNI) in predicting postoperative complications and long-term survival in patients with gastric cancer but also highlights the differences among histological subtypes. Particularly, the association of signet ring cell carcinoma (SRCC) with lower PNI values compared to other adenocarcinoma subtypes emphasizes the necessity of closer monitoring of nutritional status in the treatment of this aggressive subtype. The results of the study indicate that preoperative PNI assessment could be a valuable parameter in predicting patients’ risk of postoperative complications and forecasting long-term survival, thus helping clinicians in planning patient-centered treatment approaches.
Nutritional status inevitably affects tumor patients’ prognosis through their resistance to the tumor's catabolic activity. An increasing number of studies show that patients’ basic nutritional status is associated with long-term prognosis (12). Inadequate nutrition, decreased immunity, and increased inflammation not only affect cancer patients’ response to treatment but may also increase the likelihood of recurrence and metastasis of malignant tumors (13). Based on this, the Prognostic Nutritional Index (PNI), which reflects both the immune status (lymphocytes) and nutritional reserves (albumin) of patients, provides information about the overall physiological condition of patients. This simplicity confers a significant advantage in terms of ease of use (14).
PNI was first reported by Onodera et al. in 1984 to have prognostic value in patients undergoing surgery for gastrointestinal cancer (15). Since then, numerous studies have been conducted on this topic. It was reported that preoperative PNI was a good prognostic indicator of hepatocellular carcinoma, gastric cancer, colorectal carcinoma, and pancreatic cancer (16). A 2024 meta-analysis examining 18,596 patients found a significant relationship between PNI and OS (17). In our study, consistent with the literature, low PNI was associated with poor prognosis, and in multivariate analysis, it was found to be a risk factor affecting survival on its own.
There are various studies investigating the cut-off value for PNI, but there is no consensus on this issue. Some studies accept 45 as the cut-off value, as stated in Onodera's study (18, 19). However, when the literature is examined, <43, <44.8, ≤49.2, <52, and <52.9 have been found to be associated with poor prognosis (17). In our study, similar to the value in the original study, <46.2 with sensitivity 78.8% and specificity 51.9% was found to be associated with poor prognosis.
An inverse relationship is observed between PNI and the pathological stage of the tumor (20). According to a meta-analysis conducted in 2016, it was stated that there is a correlation between low PNI values and advanced pathological stage. However, according to the same meta-analysis, a direct relationship between stage and PNI could not be demonstrated in 5 different studies examined. In our study, while a direct relationship was found between stage and OS, no statistically significant relationship was found between stage and PNI (19).
In addition, it has been shown that there is a relationship between LVI and PeNI and PNI; PeNI and LVI were more common in patients with low PNI (19, 21). In a similar study published in 2024, no statistically significant relationship was found between PeNI and LVI in patients with PNI > 39.8 (11). In our study, PeNI and LVI were found to be more common in patients with lower PNI. Additionally, in our study, PNI was found to be lower in patients diagnosed with gastric cancer with signet ring cell histology compared to the other group. In light of the studies examined, it is understood that there is a relationship between these parameters, which are related to tumor aggressiveness and have been proven by various studies to have a negative effect on survival, and PNI. Probably, PNI values are found to be lower because the catabolic process is more intense in tumors with more aggressive behavior (22, 23). Prospective studies with large patient populations are needed to resolve conflicting findings on this issue.
There are studies examining the relationship between pre-neoadjuvant nutritional status and response to neoadjuvant therapy in gastric cancer. In a study published in 2024, it was found that patients with low PNI values had worse responses to neoadjuvant therapy (24). In their article published in 2021, Meng F. et al. developed a scoring system combined with a systemic immune-inflammatory index in addition to PNI, and according to this, they state that patients with low PNI values respond worse to neoadjuvant therapy (25). In another study, the frequency of pathological complete response was found to be higher in non-metastatic gastric cancer patients with better immune-nutritional status, but no statistical difference was found (6.6% vs. 1.2%, P = 0.107) (26). In our study, regression was observed in 59.2% of those receiving neoadjuvant therapy in the high PNI group and in 44.2% of patients in the low PNI group, but the effect of PNI value calculated before neoadjuvant therapy on the response to neoadjuvant therapy was not statistically determined (p = 0.095). It is seen that nutritional status is related to the response to neoadjuvant therapy, but additional studies are needed to determine whether PNI values can be used to predict response to neoadjuvant therapy.
PNI value also has an effect on surgical complications in the postoperative period. In our study, complication rates according to the Clavien-Dindo classification were found to be significantly higher in the patient group with PNI < 46.2 (p = 0.006). In a meta-analysis published by Yang et al. in 2016, including 3396 gastric cancer patients, a strong association was demonstrated between low PNI values and postoperative complications (OR = 1.74, 95% CI = 1.41–2.16, p < 0.01). In this meta-analysis, pooled results from five different studies revealed that patients with poor nutritional status were more vulnerable to postoperative complications (19). In the current literature, no study reporting the absence of a relationship between PNI and postoperative complications has been found. Similarly, in our study, while Grade 1 (23.4% vs. 16.7%), Grade 2 (16.0% vs. 7.9%), Grade 3 (11.7% vs. 4.8%), and Grade 4 complication rates were higher in the low PNI group, the rate of patients without complications was higher in the high PNI group (44.7% vs. 69.0%). This suggests that well-nourished patients may be better able to tolerate the immunosuppression associated with circulating inflammatory cytokines that could be induced by post-operative complications (27). Therefore, when planning surgical treatment for gastric cancer patients, preoperative assessment of PNI value can be used as a valuable parameter in predicting the risk of postoperative complications and planning patient-specific approaches.
In our study, the PNI value in patients receiving neoadjuvant therapy is the PNI value calculated from blood taken before the start of neoadjuvant therapy. It may be thought that taking the PNI value before treatment in the group receiving neoadjuvant therapy and before operation in the group not receiving neoadjuvant therapy may harm homogeneity, but in patients who underwent surgery after neoadjuvant therapy, there was a relationship between the PNI value calculated before neoadjuvant chemotherapy and OS, while no relationship was found between the PNI value calculated in blood taken before surgery after neoadjuvant therapy and OS. The probable reason for this is the hematological toxicity of chemotherapeutic agents and bone marrow suppression. Therefore, it has been stated that it would be more appropriate to use the value taken before neoadjuvant therapy in order to use PNI as a prognostic indicator (28).
The clinical implications of our findings extend beyond mere prognostic assessment. Given that lower PNI values correlate with increased complications and reduced survival, the role of nutritional intervention becomes paramount. In the pre-neoadjuvant or preoperative phase, ensuring optimal nutritional status through daily nutritionist consultation and intervention is crucial. The availability of specialized immunonutrition formulations provides additional tools for optimizing patient outcomes. Our results reinforce the principle that improved nutritional status directly translates to better treatment outcomes, emphasizing the need for proactive nutritional management as an integral component of gastric cancer treatment protocols.
Future prospective studies should consider incorporating serial PNI measurements during the postoperative period to evaluate the dynamic changes in nutritional status and their impact on long-term outcomes. Such longitudinal assessment could provide valuable insights into the optimal timing and effectiveness of nutritional interventions.”
There are some limitations in our study. Primarily, our study is a retrospective study. Recurrence timing and disease-free survival analysis could not be performed because all data on patients’ adjuvant treatment protocols and durations and recurrence timing could not be fully accessed. However, in the survival analysis performed, only tumor-related deaths were referenced. The sensitivity and specificity of the detected cut-off value are not sufficient, but there is no study in the literature that finds a cut-off value with high sensitivity and specificity.
Due to sample size limitations and the retrospective nature of the study, propensity score matching analysis could not be performed to create matched cohorts based on PNI and tumor stage.
Despite these limitations, our study provides valuable information on 5-year OS, surgical complications, and nutritional status according to histological subtypes with PNI and contributes to the literature.
Conclusion
In conclusion, PNI is one of the parameters that can determine survival in gastric cancer. Major surgical complications are more common in patients with low PNI. It is observed that low PNI values are associated with SRCC, LVI, and PeNI, which have a worse prognosis. It is observed that PNI decreases directly proportional to tumor aggressiveness. However, it is evident that prospective studies with large patient populations are needed both to increase the reliability of this parameter and to find an optimal cut-off value. We believe that conducting prospective studies with large populations regarding parameters such as PNI and including these parameters in the evaluation is important for planning patient-specific treatment.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Sancaktepe Education and Research Hospital (decision number 2024/365). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FM: Investigation, Project administration, Supervision, Writing – original draft, Writing – review & editing. CO: Conceptualization, Data curation, Methodology, Resources, Writing – original draft. MB: Data curation, Formal analysis, Software, Validation, Writing – review & editing. İA: Data curation, Resources, Visualization, Writing – review & editing. OA: Investigation, Resources, Visualization, Writing – review & editing. AG: Resources, Software, Visualization, Writing – review & editing. İS: Data curation, Methodology, Resources, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Yang WJ, Zhao HP, Yu Y, Wang JH, Guo L, Liu JY, et al. Updates on global epidemiology, risk and prognostic factors of gastric cancer. World J Gastroenterol. (2023) 29(16):2452–68. doi: 10.3748/wjg.v29.i16.2452
2. Zhao W, Jia Y, Sun G, Yang H, Liu L, Qu X, et al. Single-cell analysis of gastric signet ring cell carcinoma reveals cytological and immune microenvironment features. Nat Commun. (2023) 14(1):2985. doi: 10.1038/s41467-023-38426-4
3. Wang HM, Wang TJ, Huang CS, Liang SY, Yu CH, Lin TR, et al. Nutritional status and related factors in patients with gastric cancer after gastrectomy: a cross-sectional study. Nutrients. (2022) 14(13):2634. doi: 10.3390/nu14132634
4. Ding P, Guo H, Sun C, Yang P, Kim NH, Tian Y, et al. Combined systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) predicts chemotherapy response and prognosis in locally advanced gastric cancer patients receiving neoadjuvant chemotherapy with PD-1 antibody sintilimab and XELOX: a prospective study. BMC Gastroenterol. (2022) 22(1):121. doi: 10.1186/s12876-022-02199-9
5. De Felice F, Malerba S, Nardone V, Salvestrini V, Calomino N, Testini M, et al. Progress and challenges in integrating nutritional care into oncology practice: results from a national survey on behalf of the NutriOnc research group. Nutrients. (2025) 17(1):188. doi: 10.3390/nu17010188
6. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the eastern cooperative oncology group. Am J Clin Oncol. (1982) 5(6):649–55. doi: 10.1097/00000421-198212000-00014
7. Hendrix JM, Garmon EH. American Society of Anesthesiologists Physical Status Classification System. In: Zeppieri M, Zito PM, Zubair M, Zulfiqar H, editors. StatPearls. Treasure Island, FL: StatPearls Publishing (2025). p. 21. Available online at: http://www.ncbi.nlm.nih.gov/books/NBK441940/ (Accessed February 13, 2025).
8. Ajani JA, D’Amico TA, Bentrem DJ, Chao J, Cooke D, Corvera C, et al. Gastric cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2022) 20(2):167–92. doi: 10.6004/jnccn.2022.0008
9. Pollhammer MS, Duscher D, Pagani A, Zaussinger M, Wenny R, Zucal I, et al. The Clavien-Dindo classification for body-contouring surgery complications: evaluation of 602 cases. Life (Basel). (2024) 14(9):1120. doi: 10.6004/jnccn.2022.0008
10. Ryan R, Gibbons D, Hyland JMP, Treanor D, White A, Mulcahy HE, et al. Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology. (2005) 47(2):141–6. doi: 10.1111/j.1365-2559.2005.02176.x
11. Özcan P, Çarkman MS. The relationship between the prognostic nutritional index and lymphovascular and perineural invasion of the tumor in patients diagnosed with gastric cancer, and its effect on overall survival. Medicine (Baltimore). (2024) 103(42):e40087. doi: 10.1097/MD.0000000000040087
12. Xishan Z, Ye Z, Feiyan M, Liang X, Shikai W. The role of prognostic nutritional index for clinical outcomes of gastric cancer after total gastrectomy. Sci Rep. (2020) 10:17373. doi: 10.1038/s41598-020-74525-8
13. Kosuga T, Konishi T, Kubota T, Shoda K, Konishi H, Shiozaki A, et al. Value of prognostic nutritional Index as a predictor of lymph node metastasis in gastric cancer. Anticancer Res. (2019) 39(12):6843–9. doi: 10.21873/anticanres.13901
14. Taşkın K, Yediyıldız MB, Durmuş İ, Fidan R. The prognostic nutritional index as a predictor of in-hospital mortality in geriatric intensive care patients. J Health Sci Med. (2025) 8(3):502–6. doi: 10.32322/jhsm.1666689
15. Onodera T, Goseki N, Kosaki G. [Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients]. Nihon Geka Gakkai Zasshi. (1984) 85(9):1001–5.6438478
16. Wang P, Wang H, Qiu G, Liu J, Fan L, Liao X, et al. A nomogram model involving preoperative fibrinogen and prognostic nutritional Index score for predicting postoperative outcome in patients with gastric cancer. Cancer Manag Res. (2021) 13:4191–201. doi: 10.2147/CMAR.S311347
17. Deng H, He Y, Huang G, Huang Y, Wu J, Qin X. Predictive value of prognostic nutritional index in patients undergoing gastrectomy for gastric cancer: a systematic review and meta-analysis. Medicine (Baltimore). (2024) 103(41):e39917. doi: 10.1097/MD.0000000000039917
18. Maejima K, Taniai N, Yoshida H. The prognostic nutritional index as a predictor of gastric cancer progression and recurrence. J Nippon Med Sch. (2022) 89(5):487–93. doi: 10.1272/jnms.JNMS.2022_89-507
19. Yang Y, Gao P, Song Y, Sun J, Chen X, Zhao J, et al. The prognostic nutritional index is a predictive indicator of prognosis and postoperative complications in gastric cancer: a meta-analysis. Eur J Surg Oncol. (2016) 42(8):1176–82. doi: 10.1016/j.ejso.2016.05.029
20. Okubo K, Arigami T, Matsushita D, Tanaka T, Tsuruda Y, Noda M, et al. Clinical impact of the prognostic nutritional Index as a predictor of outcomes in patients with stage II/III gastric cancer: a retrospective cohort study. Oncology. (2021) 99(6):380–8. doi: 10.1159/000514572
21. Eo WK, Chang HJ, Suh J, Ahn J, Shin J, Hur JY, et al. The prognostic nutritional Index predicts survival and identifies aggressiveness of gastric cancer. Nutr Cancer. (2015) 67(8):1260–7. doi: 10.1080/01635581.2015.1082112
22. Bayram E, Kidi MM, Camadan YA, Biter S, Yaslikaya S, Toyran T, et al. Can the pathological response in patients with locally advanced gastric cancer receiving neoadjuvant treatment be predicted by the CEA/albumin and CRP/albumin ratios? J Clin Med. (2024) 13(10):2984. doi: 10.3390/jcm13102984
23. Fan M, Tang J, Du W, Du YF, Liu HJ. Systemic immunoinflammatory index and prognostic nutrition index for predicting pathologic responses of patients with advanced gastric cancer after neoadjuvant therapy for advanced gastric cancer. Am J Cancer Res. (2024) 14(8):3922–34. doi: 10.62347/PAYM2267
24. Jin H, Zhu K, Wang W. The predictive values of pretreatment controlling nutritional status (CONUT) score in estimating short- and long-term outcomes for patients with gastric cancer treated with neoadjuvant chemotherapy and curative gastrectomy. J Gastric Cancer. (2021) 21(2):155–68. doi: 10.5230/jgc.2021.21.e14
25. Sun J, Wang D, Mei Y, Jin H, Zhu K, Liu X, et al. Value of the prognostic nutritional index in advanced gastric cancer treated with preoperative chemotherapy. J Surg Res. (2017) 209:37–44. doi: 10.1016/j.jss.2016.09.050
26. Efared B, Kadi M, Tahiri L, Lahmidani N, Hassani KIM, Bouhaddouti HE, et al. Gastric signet ring cell carcinoma: a comparative analysis of clinicopathologic features. Cancer Control. (2020) 27(1):1073274820976596. doi: 10.1177/1073274820976596
27. Jiang N, Deng JY, Ding XW, Ke B, Liu N, Zhang RP, et al. Prognostic nutritional index predicts postoperative complications and long-term outcomes of gastric cancer. World J Gastroenterol. (2014) 20(30):10537–44. doi: 10.3748/wjg.v20.i30.10537
28. Hirahara N, Tajima Y, Fujii Y, Kaji S, Kawabata Y, Hyakudomi R, et al. High preoperative prognostic nutritional index is associated with less postoperative complication-related impairment of long-term survival after laparoscopic gastrectomy for gastric cancer. J Gastrointest Surg. (2020) 24(12):2852–5. doi: 10.1007/s11605-020-04737-w
Keywords: gastric cancer, prognostic nutritional index (PNI), signet cell gastric carcinoma, survival, post-operative outcomes
Citation: Mülküt F, Ofluoğlu CB, Başdoğan MK, Aydın İC, Akdoğan O, Gündoğdu A and Subaşı İE (2025) Prognostic value of prognostic nutritional index in patients undergoing surgery for gastric cancer. Front. Surg. 12:1618111. doi: 10.3389/fsurg.2025.1618111
Received: 25 April 2025; Accepted: 14 August 2025;
Published: 3 September 2025.
Edited by:
Jae-Seok Min, Dongnam Institute of Radiological and Medical Sciences, Republic of KoreaReviewed by:
Natale Calomino, University of Siena, ItalyLinda Maximiano, Faculdade de Medicina da Universidade de São Paulo, Brazil
Copyright: © 2025 Mülküt, Ofluoğlu, Başdoğan, Aydın, Akdoğan, Gündoğdu and Subaşı. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fırat Mülküt, ZmlyYXRtdWxrdXRAaG90bWFpbC5jb20=