 Alessandro De Luca1*
Alessandro De Luca1* Domenico Tripodi1
Domenico Tripodi1 Lucio Fortunato2
Lucio Fortunato2 Federica Pediconi3
Federica Pediconi3 Claudio Cannistrà4
Claudio Cannistrà4 Nicola Rocco5Massimo Vergine1
Nicola Rocco5Massimo Vergine1 Maria Ida Amabile1
Maria Ida Amabile1
- 1Department of Surgery, Sapienza University of Rome, Rome, Italy
- 2Breast Center, Azienda Ospedaliera San Giovanni-Addolorata, Rome, Italy
- 3Department of Radiological, Oncological and Pathological Sciences, Sapienza University of Rome, Rome, Italy
- 4Plastic and Reconstructive Surgery Unit, Centre Hospitalier Universitaire Bichat Claude-Bernard, Paris, France
- 5Department of Advanced Biomedical Sciences, University Federico II, Naples, Italy
Introduction: Breast conservation surgery (BCS) combined with post-operative radiotherapy is the standard and preferred treatment for early-stage breast cancer (eBC), offering survival outcomes comparable to mastectomy while improving body image and quality of life. Oncoplastic breast surgery (OBS) has evolved from BCS to allow more extensive tissue removal while maintaining oncological safety and reducing the risk of post-surgical deformities. The ultrasound (US)-assisted periareolar approach in breast surgery offers several potential benefits, including reduced scarring, improved cosmetic outcomes, and enhanced surgical precision, particularly for non-palpable or small lesions, and potentially better nipple sensation preservation. This study aim to describe an US-assisted periareolar OBS approach for eBC patients with small to moderate breast ptosis.
Methods: Here we present a focus on surgical technique consisting in OBS combining a US-assisted periareolar approach with volume displacement in small- to moderate- ptosic breasts. Margin resection adequacy, surgical complications and patient satisfaction using the Breast-Q questionnaire were assessed.
Results: Thirty-two patients were considered. A negative margin of excision was achieved in all cases, and patients routinely received post-operative hypofractionated radiotherapy. Seroma was the most common complication (12.5%), while breast fat necrosis and minor wound infections occurred in 6% and 3% of cases, respectively. At a median follow-up of 12 months (range 6–18), post-treatment breast retraction occurred in 3 patients (9%), all of whom underwent fat grafting to improve outcomes. The average satisfaction score as determined by Breast-Q module was 78.6, rising to 81.3 for those who underwent contralateral mammaplasty.
Discussion: The combination of imaging, the use of oncoplastic surgical techniques and an appropriate post-operative management may provide the surgeon new tools for the treatment of eBC. In selected cases, the US-assisted periareolar oncoplastic approach is a versatile technique that can be easily adapted for tumors in any location of the breast.
Introduction
Breast conservation surgery (BCS) followed by post-operative radiotherapy represents the optimal locoregional treatment for the majority of patients with early-stage breast cancer (eBC), offering survival rates equivalent to those of mastectomy while preserving body image and significantly improving quality of life (1, 2).
It is well established that local recurrence rates after BCS combined with radiotherapy are comparable to those observed after mastectomy (2–4). However, BCS is associated with superior aesthetic and patient-reported outcomes, which can be further enhanced through the application of oncoplastic surgical techniques (5–7). Oncoplastic breast surgery (OBS) has been increasingly adopted in clinical practice as it enables wider resections while maintaining oncological safety (8). This approach helps avoiding unnecessary mastectomies and simultaneously reduces the risk of post-operative breast deformities and asymmetries (8, 9). The OBS allows for the removal of a larger volume of breast tissue (10, 11) and facilitates immediate reconstruction using plastic surgery principles. This can be achieved through either volume-displacement techniques, which involve the mobilization and reshaping of local dermo-glandular flaps (12), or volume-replacement strategies, where breast volume is restored using autologous tissue via various flap techniques (13, 14).
The increasing emphasis on aesthetic outcomes has led to growing interest in advanced oncoplastic methods (10–15), with many breast surgeons seeking additional training in reconstructive techniques or fostering closer collaboration with plastic surgery teams to improve the cosmetic results of BCS (16, 17).
In this context, the ultrasound (US)-assisted periareolar approach offers notable advantages. By integrating high-resolution intraoperative ultrasound with a minimally invasive periareolar access, this technique allows for precise tumor localization and excision with optimal margin control, all while preserving the natural breast contour and minimizing visible scarring. This approach not only supports oncological safety but also enhances cosmetic outcomes—particularly in cases involving small- to medium-sized tumors in the central or peri-areolar breast region. Furthermore, the use of ultrasound guidance reduces the likelihood of re-excision and improves intraoperative decision-making, ultimately contributing to greater patient satisfaction and overall quality of care.
In this study we present a focus on surgical technique consisting in OBS combining a US-assisted periareolar approach with volume displacement in small- to moderate- ptosic breasts, inspired by the Benelli technique described for aesthetic purposes (18).
Materials and methods
A retrospective evaluation was conducted on consecutive patients who underwent OBS using an US-assisted periareolar approach at our Breast Center (Local Ethics Committee Protocol No. 0301/2021) in breast cancer patients with small- to medium- breast size and mild to moderate ptosis. We documented that patients with pathological skin involvement or tumors located more than 8 cm far from the nipple-areola complex were not treated with this approach. The study focused on patients with eBC with a follow-up period ranging from 6 to 18 months (median follow-up 11 months).
The surgical procedures utilized volume displacement techniques. In particular, the US-assisted periareolar approach was applied to facilitate tumor excision while reshaping the remaining breast tissue to preserve aesthetic outcomes.
Post-operative evaluations were carried out by two experienced oncoplastic breast surgeons, ensuring a comprehensive and standardized assessment of both clinical and cosmetic results. Patient satisfaction was assessed using the “Satisfaction with Outcome” module of the internationally validated BREAST-Q questionnaire (19), which is routinely administered during follow-up visits at our Center before beginning adjuvant radiotherapy. The questionnaire was completed three months post-operatively.
Surgical technique description—the US-assisted periareolar approach
This oncoplastic surgical technique is structured around two essential pre-operative phases: a detailed breast ultrasound assessment and a precise pre-operative skin marking process.
The breast ultrasound is performed in both the supine and standing positions to ensure accurate identification of the area to be excised.
• In the supine position, the tumor is located and marked, and its bidimensional measurements are recorded (U1, Figure 1).
• In the standing position, additional markings are made to account for tumor displacement due to breast ptosis, integrating this information into the surgical planning (U2, Figure 2).
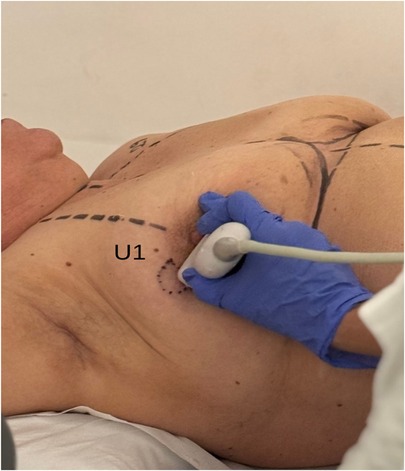
Figure 1. Breast ultrasound exam with patient in supine position (U1). Multifocal tumor was localized in the outer quadrants of the right breast.
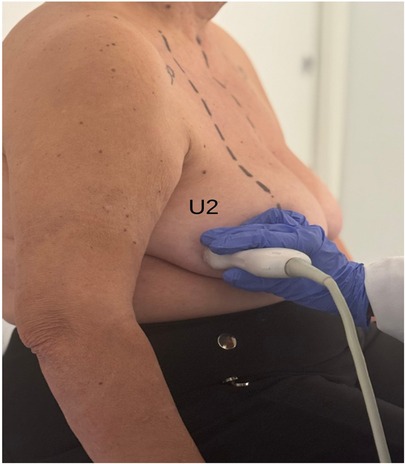
Figure 2. Breast ultrasound exam with patient in standing position (U1). Multifocal tumor was localized in the outer quadrants of the right breast.
The definitive excision area is determined by combining the data from both positions (Figure 3).
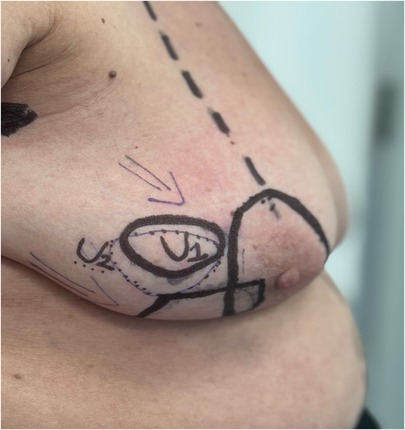
Figure 3. U1 and U2 breast markings. Multifocal tumor was localized in the outer quadrants of the right breast.
Pre-operative skin markings are carried out in the patient's room while standing, facilitating anatomical accuracy and natural breast contour assessment.
Two concentric circular markings are applied:
• An inner circle outlining the periareolar border.
• An outer circle, whose placement is guided by ultrasound findings, tailored to the tumor location, breast volume, and degree of ptosis (Figure 4). This outer marking can be either concentric or eccentric to the nipple-areola complex and is limited to a maximum diameter of 6 cm.
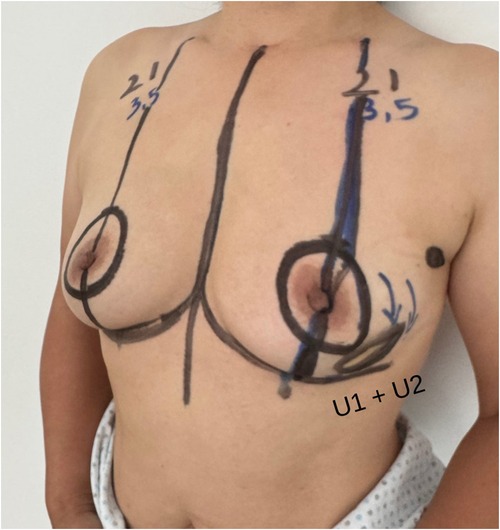
Figure 4. Preoperative drawing. Unifocal tumor was localized in the inferior external quadrant of the left breast.
Reduction of the areola is performed only if its diameter exceeds 6 cm (Figure 5). Once the markings are completed, both breasts are prepped in the surgical field to allow intraoperative comparison for symmetry.

Figure 5. Preoperative drawing. Breast unifocal tumor was localized in the upper external quadrant of the right breast.
The patient is positioned on the operating table in a way that permits both supine and upright evaluations, optimizing reshaping and symmetry outcomes.
When the tumor is in close proximity to the areola, the overlying skin is removed en bloc with the lesion. If this is not required, we perform de-epithelialization of the skin between the two circular markings, sparing the dermal layer on the side opposite the tumor to preserve the vascular plexus of the nipple-areola complex.
Intraoperative margin analysis is conducted to ensure complete oncological resection. Following tumor removal, immediate glandular reconstruction and reshaping are undertaken.
A critical element of this technique is the extensive subcutaneous undermining performed prior to tumor excision. This approach, similar to that used in skin-sparing mastectomy, involves undermining 30%–50% of the breast envelope and may extend into either the upper or lower quadrants, depending on tumor location (Figures 6, 7).

Figure 6. Subcutaneous undermining procedure. Multifocal tumor was localized in outer quadrants of the right breast.

Figure 7. Subcutaneous undermining procedure. Unifocal tumor was localized in inferior external quadrant of the left breast.
The extent of subcutaneous dissection and glandular mobilization from the muscle-fascial plane is individualized for each patient, based on tumor location, resection volume, and breast size.
The outer circular incision is reduced using a round block technique, approximating the deep dermal layer surrounding the areola with the retroareolar tissue and adjacent dermis. This technique yields a final scar confined to the periareolar region (Figures 8, 9), optimizing both cosmetic and oncological outcomes.

Figure 8. Round block technique. Unifocal tumor was localized in inferior external quadrant of the left breast.
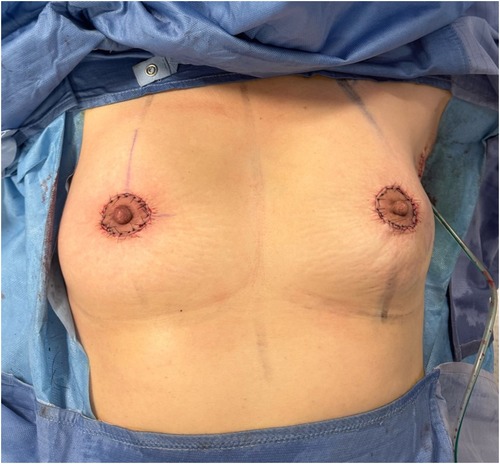
Figure 9. Post-operative result of ultrasound-assisted periareolar oncoplastic approach and contralateral mammoplasty in breast cancer patient with unifocal tumor in inferior external quadrant of the left breast.
Results
We initially considered a total of 40 potentially eligible eBC patients. Eight of these patients were excluded due to a radiological diagnosis of multicentric tumor or nipple-areola complex involvement. Therefore, 32 eBC patients undergone OBS with an US-assisted periareolar approach were considered, whose 18 patients also undergone a contralateral mammaplasty according to patient preference. The contralateral balancing surgery did not affect the surgical duration. It was performed with a 2-team approach, not lengthening the operating time.
The clinico-pathological characteristics of the patients are described in Table 1.
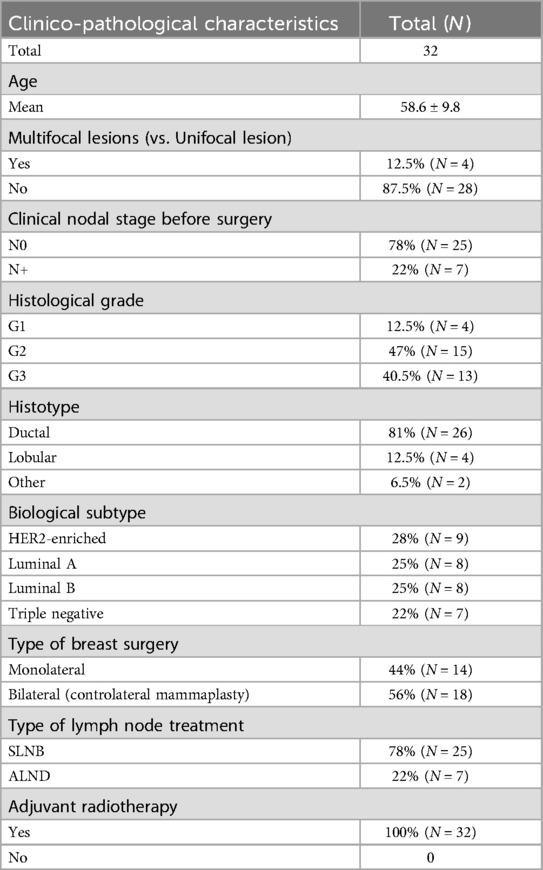
Table 1. Patients' clinico-pathological characteristics.
The mean age of patients was 58.6 ± 9.8 years and the most represented histology subtype was breast invasive ductal carcinoma (N = 26, 81%). No lesion required the removal of the nipple-areola complex.
The majority of the patients (N = 25, 78%) showed a cN0 status before surgery and all these patients (N = 25, 78%) underwent sentinel lymph node biopsy while the remaining underwent axillary lymph node dissection (N = 7; 22%).
The use of ultrasound guide shortened the surgical time because it allowed identifying the suspicious lesion/s faster and more effective than without the ultrasound guide.
In the post-operative phase, the seroma was the most prevalent complication observed (N = 4, 12.5%) (Table 2). We documented only 2 cases (6%) of breast fat necrosis and 1 case (3%) of minor wound infection, treated with specific antibiotic therapy (Table 2). No cases of major wound infection or NAC necrosis were reported. We obtained complete tumor excision (>2 mm free margins) in 100% of the patients.
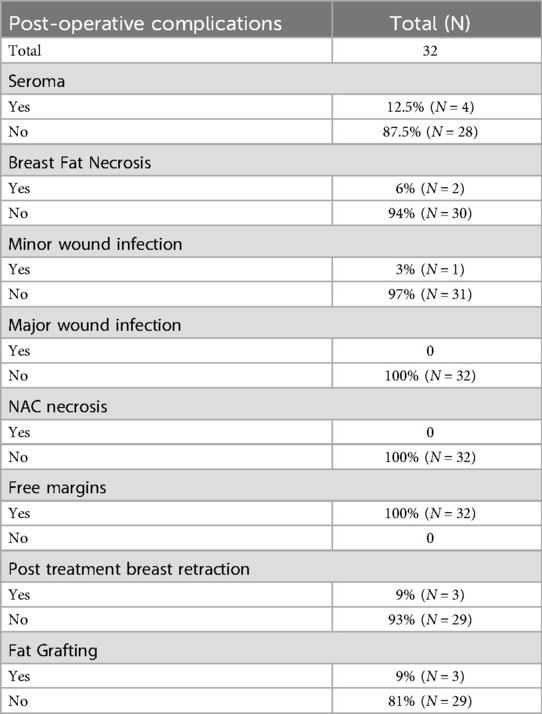
Table 2. Post-operative complications.
All enrolled patients concluded adjuvant hypofractionated radiotherapy after surgery, which was conducted within 90 days from the surgery, as per our Center's internal guidelines. The study focused on patients with eBC, with a follow-up period ranging from 6 to 18 months (median follow-up: 11 months). The overall incidence of post-treatment breast retraction in our cohort was 9% (N = 3) and all these patients underwent further fat grafting procedure to improve the aesthetic and functional outcome (Table 2). We obtained a satisfaction score of 78.6 following the Breast-Q questionnaire administration, and a greater score of 81.3 when we considered only those patients who also underwent contralateral mammaplasty (Figures 10, 11). One patient complained of asymmetries and it was addressed further correcting with a fat grafting procedure.

Figure 10. Post-operative result in ultrasound-assisted periareolar oncoplastic approach in breast cancer patient with multifocal tumor in outer quadrants of the right breast.

Figure 11. 7-day post-operative time of ultrasound-assisted periareolar oncoplastic approach and contralateral mammoplasty in breast cancer patient with unifocal tumor in inferior external quadrant of the left breast.
Discussion
Breast conservation therapy is widely recognized as a cornerstone in the treatment of eBC (1–4). Its integration with plastic surgery techniques represents a well-established approach that enables surgeons to perform wide excisions with negative margins while minimizing the risk of post-operative deformities (9, 16, 17).
In a systematic review, De La Cruz et al. reported low rates of positive surgical margins, re-excisions, and complications in patients with eBC treated with OBS, supporting its oncologic safety (8). Also our experience confirms that OBS allows for high rates of complete tumor excision—defined as clear margins >2 mm for ductal carcinoma in situ and no-ink on tumor for invasive carcinoma—without the need for reoperation. Furthermore, the use of US-assisted surgical techniques, combined with larger volumes of excised breast tissue, enabled the achievement of tumor-free margins in our patients, and this aspect may be as a rationale for implementing US-approach in clinical practice.
In this context, Giacalone et al. compared surgical margins obtained through conventional BCS vs. OBS, highlighting that margins of ≥10 mm are more frequently achieved with the oncoplastic approach (10). Similarly, Kaur et al. reported that OBS is associated with larger tissue resections and a reduced incidence of positive margins (11). Specifically, the US-assisted periareolar approach offers the dual benefit of extensive surgical access and precise intraoperative localization of the tumor, thereby increasing the likelihood of complete excision (10, 11, 20, 21).
Several studies have demonstrated that the integration of ultrasound guidance into BCS significantly improves the achievement of negative margins and reduces the need for reoperations (20–24), particularly in patients with palpable tumors. Positive margin rates as low as 3%–4% have been reported in such cases (22, 23).
Ultrasound-guided BCS is thus emerging as a reliable and effective technique for achieving negative surgical margins, with recognized feasibility and safety (20–24). Preoperative ultrasound allowed us to correct localize the lesions, supposing the feasibility of BCS with oncologically safe margins.
Patient satisfaction associated with the US-assisted periareolar approach was assessed using the BREAST-Q questionnaire (25, 26). Several studies have documented that OBS positively impacts quality of life in patients with eBC (27–31), considering that OBS is essential not only for achieving complete oncological resection but also for enhancing patient compliance with adjuvant therapies.
The main objective of OBS is to reshape the remaining breast tissue while preserving a natural and aesthetically pleasing breast contour. To this end, contralateral procedures are frequently performed to achieve optimal symmetry (25). Patient satisfaction and quality of life have become increasingly important indicators of surgical success, and these outcomes are closely linked to the extent of glandular and cutaneous undermining from the pectoralis muscle (10–12).
However, an aggressive undermining may lead to complications such as seroma formation and fat necrosis (32). Fat necrosis typically presents as a palpable mass with persistent firmness or as non-specific calcifications on mammography, usually measuring ≥1 cm (32, 33). We documented the incidence of seroma and fat necrosis was 12.5% and 6%, respectively. These complications occur principally in patients with predominantly fatty breasts on mammography (34).
In line with the literature (35–37), we found that the use of at least one surgical drain, appropriate antibiotic prophylaxis, and post-operative elastic compression bandaging contributed to a reduction in the incidence of seroma, fat necrosis, and surgical site infections.
Seroma rate may be significantly influenced by a myriad of surgical aspects, including but not limited to: a. extent of surgical undermining and dissection of the breast parenchyma; b. surgical technique, i.e., use of electrocautery vs. scalpel; c. whether drains are placed and for how long; d. the type of axillary procedures performed (i.e., axillary clearance or sampling vs. sentinel lymph node biopsy), as lymphorrhoea might be commonly mixed in or confused with serous collections, especially from axillary drains; e. patient-related factors (age, body mass index, certain comorbidities, smoking, etc.); f. use of compressing dressings or garments. In addition, judging by the fact that 30%–50% of the breast surface is undermined in the surgical approach, a considerable dead space is created. This may, in part, explain the seroma rate that we observed in our cohort.
The final aesthetic result of OBS depends on several factors, including age, comorbidity, tumor size and site, breast volume, and adjuvant treatments including radiotherapy (38, 39). Adjuvant radiotherapy is essential to reduce the risk of local recurrence (40) as well as determining late deformities through tissue fibrosis (41, 42). In our cohort 3 patients (9%) reported post-treatment breast retraction which required at least 2 fat-grafting sessions to improve the functional and aesthetic outcome (43–45). In order to minimize complications and optimize aesthetic outcomes, each clinical case should be managed by a multi-disciplinary team for a correct clinical and radiological assessment (46–48). Periareolar techniques are quite powerful as they can address small asymmetries of the nipple-areola complex. However, the main limitation is that the periareolar suture compresses the breast reducing its projection considerably, if the procedure is not accompanied by the placement of a breast implant which can help provide additional projection. Of course, placing an implant on an irradiated breast is commonly frowned upon by many surgeons due to the very high rate of complications which is upwards of 50% (49).
Furthermore, considering the patient-centered benefits, including reduced discomfort and fewer preoperative procedures, it suggests that US-assisted periareolar approach may be, in selected cases, a preferred method in managing early-stage breast lesions, particularly in high-volume cancer centers where resource optimization is critical.
We are aware that our description has limits: surely, the small cohort of considered patients and the brief follow-up period, which limits the generalizability of the findings, as well as the fact that long-term recurrence data are not yet available. We did not preoperatively collect BREAST-Q results. Assessing the BREAST-Q preoperatively is essential to establish a baseline for evaluating the true impact of surgery on patient-reported outcomes. The lack of pre-operative data makes it difficult to determine whether post-operative changes reflect improvement, decline, or no change at all. It also helps capture patient expectations, supports individualized counseling, and enhances the validity of clinical research through within-subject comparisons. By measuring both pre- and post-operative outcomes, clinicians can better assess the effectiveness of surgical interventions and continuously improve the quality of care. In addition, BREAST-Q was collected post-operatively at 3 months, before beginning adjuvant radiotherapy, and this may determine a bias when assessing aesthetic outcomes, as radiotherapy negatively affects aesthetic outcomes.
The median follow-up period was short for evaluating oncological outcomes. While early cosmetic results are informative, long-term recurrence data are not yet available for our patients. We did not perform power calculations and define the minimum number of cases performed without ultrasound to draw a comparison group and design a case-control study, matching patients in each group by demographic and oncological characteristics, and thus to find associations with tangible benefits of one technique compared to the other.
Here we present a focus on surgical technique consisting in OBS combining a US-assisted periareolar approach with volume displacement in small- to moderate- ptosic breasts. Further analysis needs to be presented with detailed descriptive data and to determine whether any number of variables may affect the clinical and/or aesthetic outcomes, which, in turn, would considerably strengthen the findings as a retrospective cohort study.
Conclusions
The combination of imaging, the use of oncoplastic surgical techniques and an appropriate post-operative management may provide the surgeon new tools for the treatment of eBC. In selected cases, the US-assisted periareolar oncoplastic approach is a versatile technique that can be easily adapted for tumors in any location of the breast.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by University Sapienza of Rome Local Ethic Committee Prot. N. 0301/2021. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
ADL: Writing – original draft, Writing – review & editing. DT: Writing – original draft, Writing – review & editing. LF: Writing – review & editing. FP: Writing – review & editing. CC: Writing – review & editing. NR: Writing – review & editing. MV: Writing – review & editing. MIA: Writing – review & editing, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The reviewer [GF] declared a shared affiliation with the authors [ADL, DT, FP, MV, MIA] to the handling editor at the time of review.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Early Breast Cancer Trialists' Collaborative Group Effects of radiotherapy and surgery in early breast cancer—an overview of the randomized trials. N Engl J Med. (1995) 333(22):1444–55. doi: 10.1056/NEJM199511303332202
2. Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. (2002) 347(16):1227–32. doi: 10.1056/NEJMoa020989
3. Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. (2002) 347(16):1233–41. doi: 10.1056/NEJMoa022152
4. van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: european organization for research and treatment of cancer 10801 trial. J Natl Cancer Inst. (2000) 92(14):1143–50. doi: 10.1093/jnci/92.14.1143
5. Beloqui L, Rainsbury RM. Surgery insight: oncoplastic breast-conserving reconstruction—indications, benefits, choices and outcomes. Nat Clin Pract Oncol. (2007) 4(11):657–64. doi: 10.1038/ncponc0957
6. Petit JY, Rietjens M, Garusi C, Greuze M, Perry C. Integration of plastic surgery in the course of breast-conserving surgery for cancer to improve cosmetic results and radicality of tumor excision. Recent Results Cancer Res. (1998) 152:202–11. doi: 10.1007/978-3-642-45769-2_19
7. Baildam AD. Oncoplastic surgery for breast cancer. J Br Surg. (2008) 95(1):4–5. doi: 10.1002/bjs.6098
8. De La Cruz L, Blankenship SA, Chatterjee A, Geha R, Nocera N, Czerniecki BJ, et al. Outcomes after oncoplastic breast-conserving surgery in breast cancer patients: a systematic literature review. Ann Surg Oncol. (2016) 23(10):3247–58. doi: 10.1245/s10434-016-5313-1
9. Santos G, Urban C, Edelweiss MI, Zucca-Matthes G, de Oliveira VM, Arana GH, et al. Long-term comparison of aesthetical outcomes after oncoplastic surgery and lumpectomy in breast cancer patients. Ann Surg Oncol. (2015) 22(8):2500–8. doi: 10.1245/s10434-014-4301-6
10. Giacalone PL, Roger P, Dubon O, El Gareh N, Rihaoui S, Taourel P, et al. Comparative study of the accuracy of breast resection in oncoplastic surgery and quadrantectomy in breast cancer. Ann Surg Oncol. (2007) 14(2):605–14. doi: 10.1245/s10434-006-9098-5
11. Kaur N, Petit JY, Rietjens M, Maffini F, Luini A, Gatti G, et al. Comparative study of surgical margins in oncoplastic surgery and quadrantectomy in breast cancer. Ann Surg Oncol. (2005) 12(7):539–45. doi: 10.1245/ASO.2005.12.046
12. Yang JD, Bae SG, Chung HY, Cho BC, Park HY, Jung JH. The usefulness of oncoplastic volume displacement techniques in the superiorly located breast cancers for Korean patients with small to moderate-sized breasts. Ann Plast Surg. (2011) 67(5):474–80. doi: 10.1097/SAP.0b013e318201fdf4
13. Lee JW, Kim MC, Park HY, Yang JD. Oncoplastic volume replacement techniques according to the excised volume and tumor location in small- to moderate-sized breasts. Gland Surg. (2014) 3(1):14–21. doi: 10.3978/j.issn.2227-684X.2014.02.02
14. Haloua MH, Krekel NM, Winters HA, Rietveld DH, Meijer S, Bloemers FW, et al. A systematic review of oncoplastic breast-conserving surgery: current weaknesses and future prospects. Ann Surg. (2013) 257(4):609–20. doi: 10.1097/SLA.0b013e3182888782
15. Pasta V, D'Orazi V, Merola R, Frusone F, Amabile MI, De Luca A, et al. Oncoplastic central quadrantectomies. Gland Surg. (2016) 5(4):422–6. doi: 10.21037/gs.2016.04.01
16. Cardoso MJ, Macmillan RD, Merck B, Munhoz AM, Rainsbury R. Training in oncoplastic surgery: an international consensus. The 7th Portuguese senology congress, vilamoura, 2009. Breast. (2010) 19(6):538–40. doi: 10.1016/j.breast.2010.03.030
17. Down SK, Pereira JH, Leinster S, Simpson A. Training the oncoplastic breast surgeon-current and future perspectives. Gland Surg. (2013) 2(3):126–7. doi: 10.3978/j.issn.2227-684X.2013.06.02
18. Benelli L. A new periareolar mammaplasty: the “round block” technique. Aesthetic Plast Surg. (1990) 14(2):93–100. doi: 10.1007/BF01578332
19. Pusic AL, Chen CM, Cano S, Klassen A, McCarthy C, Collins ED, et al. Measuring quality of life in cosmetic and reconstructive breast surgery: a systematic review of patient-reported outcomes instruments. Plast Reconstr Surg. (2007) 120(4):823–37. doi: 10.1097/01.prs.0000278162.82906.81
20. Krekel NM, Zonderhuis BM, Schreurs HW, Cardozo AM, Rijna H, van der Veen H, et al. Ultrasound-guided breast-sparing surgery to improve cosmetic outcomes and quality of life. A prospective multicentre randomised controlled clinical trial comparing ultrasound-guided surgery to traditional palpation-guided surgery (COBALT trial). BMC Surg. (2011) 11:8. doi: 10.1186/1471-2482-11-8
21. Krishna KL, Srinath BS, Santosh D, Velusamy S, Divyamala KP, Sariya Mohammadi J, et al. A comparative study of perioperative techniques to attain negative margins and spare healthy breast tissue in breast conserving surgery. Breast Dis. (2021) 39(3–4):127–35. doi: 10.3233/BD-200443
22. Moore MM, Whitney LA, Cerilli L, Imbrie JZ, Bunch M, Simpson VB, et al. Intraoperative ultrasound is associated with clear lumpectomy margins for palpable infiltrating ductal breast cancer. Ann Surg. (2001) 233(6):761–8. doi: 10.1097/00000658-200106000-00005
23. Krekel NM, Haloua MH, Lopes Cardozo AM, de Wit RH, Bosch AM, de Widt-Levert LM, et al. Intraoperative ultrasound guidance for palpable breast cancer excision (COBALT trial): a multicentre, randomised controlled trial. Lancet Oncol. (2013) 14(1):48–54. doi: 10.1016/S1470-2045(12)70527-2
24. Hoffmann J, Marx M, Hengstmann A, Seeger H, Oberlechner E, Helms G, et al. Ultrasound-assisted tumor surgery in breast cancer — a prospective, randomized, single-center study (MAC 001). Ultraschall Med. (2019) 40(3):326–32. doi: 10.1055/a-0637-1725
25. St Denis-Katz H, Ghaedi BB, Fitzpatrick A, Zhang J. Oncological safety, surgical outcome, and patient satisfaction of oncoplastic breast-conserving surgery with contralateral balancing reduction mammoplasty. Plast Surg. (2021) 29(4):235–42. doi: 10.1177/2292550320969645
26. De Lorenzi F, Hubner G, Rotmensz N, Bagnardi V, Loschi P, Maisonneuve P, et al. Oncological results of oncoplastic breast-conserving surgery: long term follow-up of a large series at a single institution: a matched-cohort analysis. Eur J Surg Oncol. (2016) 42(1):71–7. doi: 10.1016/j.ejso.2015.08.160
27. Thiessen FEF, Tjalma WAA, Tondu T. Breast reconstruction after breast conservation therapy for breast cancer. Eur J Obstet Gynecol Reprod Biol. (2018) 230:233–8. doi: 10.1016/j.ejogrb.2018.03.049
28. Cochrane RA, Valasiadou P, Wilson AR, Al-Ghazal SK, Macmillan RD. Cosmesis and satisfaction after breast-conserving surgery correlates with the percentage of breast volume excised. Br J Surg. (2003) 90(12):1505–9. doi: 10.1002/bjs.4344
29. Pirro O, Mestak O, Vindigni V, Sukop A, Hromadkova V, Nguyenova A, et al. Comparison of patient-reported outcomes after implant versus autologous tissue breast reconstruction using the BREAST-Q. Plast Reconstr Surg Glob Open. (2017) 5(1):e1217. doi: 10.1097/GOX.0000000000001217
30. Rutherford CL, Barker S, Romics L. A systematic review of oncoplastic volume replacement breast surgery: oncological safety and cosmetic outcome. Ann R Coll Surg Engl. (2022) 104(1):5–17. doi: 10.1308/rcsann.2021.0012
31. De Luca A, Amabile MI, Frusone F, Tripodi D, Costanzo ML, La Torre G, et al. Breast cancer patients’ post-operative outcomes in nipple-sparing mastectomy and reconstruction with subpectoral implant placement: a single center experience. Gland Surg. (2024) 13(7):1164–77. doi: 10.21037/gs-24-58
32. Nakada H, Inoue M, Furuya K, Watanabe H, Ikegame K, Nakayama Y, et al. Fat necrosis after breast-conserving oncoplastic surgery. Breast Cancer. (2019) 26(1):125–30. doi: 10.1007/s12282-018-0901-5
33. Rao A, Saadeh PB. Defining fat necrosis in plastic surgery. Plast Reconstr Surg. (2014) 134(6):1202–12. doi: 10.1097/PRS.0000000000000700
34. Zaha H, Motonari T, Abe N, Unesoko M. Fat necrosis in level I oncoplastic breast-conserving surgery focusing on a modified round block technique. Breast Cancer. (2020) 27(4):567–72. doi: 10.1007/s12282-020-01046-7
35. He XD, Guo ZH, Tian JH, Yang KH, Xie XD. Whether drainage should be used after surgery for breast cancer? A systematic review of randomized controlled trials. Med Oncol. (2011) 28:S22–30. doi: 10.1007/s12032-010-9673-2
36. Bolliger M, Lanmüller P, Schuetz M, Heilig B, Windischbauer A, Jakesz R, et al. The iTOP trial: comparing immediate techniques of oncoplastic surgery with conventional breast surgery in women with breast cancer—a prospective, controlled, single-center study. Int J Surg. (2022) 104:106694. doi: 10.1016/j.ijsu.2022.106694
37. De Luca A, Tripodi D, Frusone F, Leonardi B, Cerbelli B, Botticelli A, et al. Retrospective evaluation of the effectiveness of a synthetic glue and a fibrin-based sealant for the prevention of seroma following axillary dissection in breast cancer patients. Front Oncol. (2020) 10:1061. doi: 10.3389/fonc.2020.01061
38. Clough KB, Nos C, Salmon RJ, Soussaline M, Durand JC. Conservative treatment of breast cancers by mammaplasty and irradiation: a new approach to lower quadrant tumors. Plast Reconstr Surg. (1995) 96(2):363–70. doi: 10.1097/00006534-199508000-00015
39. Noguchi M, Saito Y, Mizukami Y, Nonomura A, Ohta N, Koyasaki N, et al. Breast deformity, its correction, and assessment of breast conserving surgery. Breast Cancer Res Treat. (1991) 18(2):111–8. doi: 10.1007/BF01980973
40. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Correa C, McGale P, Taylor C, Wang Y, Clarke M, et al. Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast. JNCI Monogr. (2010) 2010(41):162–77. doi: 10.1093/jncimonographs/lgq039
41. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG), Darby S, McGale P, Correa C, Taylor C, Arriagada R, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. (2011) 378(9804):1707–16. doi: 10.1016/S0140-6736(11)61629-2
42. Barnett GC, West CM, Dunning AM, Elliott RM, Coles CE, Pharoah PD, et al. Normal tissue reactions to radiotherapy: towards tailoring treatment dose by genotype. Nat Rev Cancer. (2009) 9(2):134–42. doi: 10.1038/nrc2587
43. Silva-Vergara C, Fontdevila J, Descarrega J, Burdio F, Yoon TS, Grande L. Oncological outcomes of lipofilling breast reconstruction: 195 consecutive cases and literature review. J Plast Reconstr Aesthet Surg. (2016) 69(4):475–81. doi: 10.1016/j.bjps.2015.12.029
44. Vyas KS, DeCoster RC, Burns JC, Rodgers LT, Shrout MA, Mercer JP, et al. Autologous fat grafting does not increase risk of oncologic recurrence in the reconstructed breast. Ann Plast Surg. (2020) 84(6S Suppl 5):S405–10. doi: 10.1097/SAP.0000000000002285
45. Gigli S, Amabile MI, Di Pastena F, De Luca A, Gulia C, Manganaro L, et al. Lipofilling outcomes mimicking breast cancer recurrence: case report and update of the literature. Anticancer Res. (2017) 37(10):5395–8. doi: 10.21873/anticanres.11966
46. Agrawal A. Assessment and planning for oncoplastic and reconstructive breast surgery: a review and a proposed chart. Eur J Plast Surg. (2016) 39:321–30. doi: 10.1007/s00238-016-1221-7
47. Metz G, Snook K, Sood S, Baron-Hay S, Spillane A, Lamoury G, et al. Breast radiotherapy after oncoplastic surgery—a multidisciplinary approach. Cancers (Basel). (2022) 14(7):1685. doi: 10.3390/cancers14071685
48. Roughton MC, Shenaq D, Jaskowiak N, Park JE, Song DH. Optimizing delivery of breast conservation therapy: a multidisciplinary approach to oncoplastic surgery. Ann Plast Surg. (2012) 69(3):250–5. doi: 10.1097/SAP.0b013e31822afa99
Keywords: breast cancer, oncoplastic breast surgery, breast conservative surgery, breast ultrasound, patient satisfaction, aesthetic outcome
Citation: De Luca A, Tripodi D, Fortunato L, Pediconi F, Cannistrà C, Rocco N, Vergine M and Amabile MI (2025) Ultrasound—assisted periareolar oncoplastic approach in breast surgery: a focus on surgical technique. Front. Surg. 12:1623894. doi: 10.3389/fsurg.2025.1623894
Received: 6 May 2025; Accepted: 5 August 2025;
Published: 12 September 2025.
Edited by:
Jan A. Plock, Aarau Cantonal Hospital, SwitzerlandReviewed by:
Guido Firmani, Chair of Plastic Surgery of the Neurosciences, Mental Health and Sensory Organs (NESMOS), Department from Sapienza University, ItalyMaria Mani, Uppsala University, Sweden
Copyright: © 2025 De Luca, Tripodi, Fortunato, Pediconi, Cannistrà, Rocco, Vergine and Amabile. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandro De Luca, ZHIuYWxlc3MuZGVsdWNhQGdtYWlsLmNvbQ==