 Yannick Prié1*
Yannick Prié1* Toinon Vigier1
Toinon Vigier1 Didier Acier2
Didier Acier2 Hélène Bonneville1Manon Georges1Solène Thévenet3Samuel Bulteau3,4
Hélène Bonneville1Manon Georges1Solène Thévenet3Samuel Bulteau3,4- 1Nantes Université, École Centrale Nantes, CNRS, LS2N, UMR 6004, Nantes, France
- 2Nantes Université, Centre de recherche en Éducation de Nantes, CREN, UR 2661, Nantes, France
- 3CHU Nantes, Nantes, France
- 4Nantes Université, CHU Nantes, INSERM, MethodS in Patients-centered outcomes and HEalth Research, SPHERE, Nantes, France
Virtual Reality (VR) and Metaverse technologies open new avenues for telemedicine, particularly for teleconsultations. Our goal is to explore how these remote medical interactions can take place within immersive teleclinics. Neuropsychological testing in VR is especially promising for diagnosing and monitoring cognitive disorders. This study presents our overall approach to immersive teleclinics and the development of a social VR platform for conducting such assessments. The application enables clinicians to perform remote testing sessions that begin in a virtual waiting room and continue with a combination of clinician-guided desk-based tasks and independent test activities. Clinicians can monitor patient performance in real time through dedicated dashboards. We evaluated the system with healthy participants (pseudo-patients) and clinicians using standard measures of usability (SUS), presence (MPS), and acceptability (UTAUTQ). Initial results indicated good usability, a strong sense of presence, and high acceptability among pseudo-patients. Clinicians were more hesitant, citing usability issues, uncertainty about the clinical validity of VR-based tests, and concerns about avatar quality for psychological interviews. We discuss our design choices, the potential of our prototype for remote cognitive assessment, and broader lessons learned for teleclinics in the Metaverse. While challenges remain, our work highlights the promise of such immersive teleclinics for future medical practice.
1 Introduction
Immersive1 Virtual Reality (VR) technologies allow their users to experience a deep sense of immersion and presence in virtual environments, as well as the illusion of being embodied in a virtual avatar. VR has long been studied and used in medicine, for a large variety of use cases in care, rehabilitation, diagnosis, or education and training. Successful examples range from management of pain relief (Matamala-Gomez et al., 2019) to low-vision rehabilitation treatment (Ehrlich et al., 2017), or surgical (Mao et al., 2021) and nursing education (Cieslowski et al., 2023). Medical Extended Reality is rising (Spiegel et al., 2024),2 and one of its fastest growing fields (Liu et al., 2022) is related to mental health. VR proved useful for early assessment of Alzheimer’s disease (Howett et al., 2019); to improve cognition, memory, and executive function in dementia population (Papaioannou et al., 2022); to support the treatment of anxiety or depression (Baghaei et al., 2021); or to carry out exposure therapy against various phobia (Carl et al., 2019). Apart from research, VR is now routinely used by practitioners in their offices, mostly by having their patients carry Head-Mounted Displays (HMD) with dedicated commercial applications,3 that they can control on handheld tablets. Also they can lend HMD to their patients who can exercise at home.4
Metaverse is a term introduced in (Stephenson, 1992) to describe a 3D space where people could interact with each other as avatars. It has been used since to denote any 3D avatar-mediated virtual world that can be inhabited, shared, and where social activities can take place, be it for education, gaming, leisure, business, or work. Barely hinted at in 2010, when environments such as Second life (Kaplan and Haenlein, 2009) were the most striking examples, the close links between the Metaverse and immersive technologies became evident with the advent of both accessible and high-quality HMDs. Indeed, HMDs seem the best devices for humans to experience 3D worlds immersively, as is the use of body-worn controllers to physically embody avatars, and the Metaverse can now be considered as mostly based on VR, avatars, and persistent 3D worlds (Park and Kim, 2022). Despite the sudden hype of the term in 2021 with the apparition of the Meta company, shortly followed by the announcement of its death, the Metaverse seems here to stay (Dwivedi et al., 2022), even if its exact form beyond social VR5 may take years to emerge.
It is no surprise that the “Medical Metaverse” also gained attention in 2021 and was the subject of a wealth of papers dedicated to various medical specialties6 (Lee, 2022). Many definitions were proposed, mostly based on enabling technologies,7 which rarely took into account the social aspects of the Metaverse. Other proposals based on applications, such as that of (Massetti and Chiariello, 2023) who described five main domains—medical education and training, collaborative medical visualization, telerehabilitation, virtual consultation & telemedicine, and social support—seem more adapted to acknowledging what the Metaverse has to offer as a place where healthcare can happen as a collective activity.
Patient-to-patient support is such an activity, and patient groups have been using social VR technology for a long time.8 However, virtual consultations between patients and medical practitioners did not take,9 studies remain scarce, and examining how the Metaverse can contribute to teleconsultation is needed (Dwivedi et al., 2022). That is why our ambition is to investigate immersive teleconsultation, a specific collaborative activity in the medical Metaverse, as well as the associated concept of immersive teleclinic, the environment where such activity should takes place. We focused on mental health, and on the activity of cognitive evaluation carried out by neuro-psychologists during dedicated sessions, building a working prototype of what could be an immersive teleclinic to explore how such patient-practitioner encounter could take place.
In this paper we present the rationale, design, implementation, and preliminary evaluation of a teleclinic for distant neuro-psychological assessment of a patient by a practitioner. Our contributions are, a) our vision of what could be teleclinics in the Metaverse; b) the design and implementation of a working immersive teleclinic for cognitive testing, notably its activity spaces; c) a pilot study aiming to evaluate the usability, sense of presence, and initial acceptability of the teleclinic for pseudo-patients and practitioners. To our knowledge, our prototype is the first implementation of a social VR clinical platform for psychological evaluation based on cognitive tests. It is focused on a specific use case, but its principles could be extended to other medical practices as well as some lessons we learned.
2 Immersive telemedicine
Telemedicine aims to provide distant clinical healthcare services using information technologies. Here we review the two main possibilities with regards to the use of VR for telemedicine, namely telerehabilitation, where patients perform VR activities at home with some supervision, and virtual teleconsultation, where practitioner and patient meet in VR.
Telerehabilitation patients of various conditions use HMD at home to carry out exercises regularly for a certain period of time. It has proved its value and feasibility, with medical results corresponding to those obtained in health facilities. A 2008 seminal study compared the use of a (non-immersive) VR system at home/at hospital for post-stroke arm motor-impairment rehabilitation, with distant data and videoconference monitoring, showing significant improvement in motor performance and better satisfaction for the at-home condition (Piron et al., 2008). Another early study had acrophobic patients undergo VR Exposure Therapy (VRET) on their own (deemed e-VRET, though still at the hospital). The comparison of 3 e-VRET and 3 VRET sessions showed no difference on anxiety, heart rate, presence or therapeutic alliance, demonstrating the feasibility of at-home immersive VR activity (Levy et al., 2016). For chronic obstructive pulmonary disease, patients had a 8 weeks program VR exercises for pulmonary rehabilitation. Qualitative and quantitative data showed better compliance, engagement, satisfaction, as well as improvements in all physical measures (Jung et al., 2020). A study was also conducted on 8 patients who underwent individualized AR home training to reduce pain associated with phantom limbs, with both good adherence and successful effect (Thøgersen et al., 2020). Patients with multiple sclerosis had 30 sessions of 45 min of at home VR rehabilitation training during 6 weeks, with asynchronous supervision. Compared with usual care, they showed higher adherence and greater improvement in metrics, as well as improvement in their quality of life (Pagliari et al., 2021). 82 patients with low back and neck pain where treated at-home using the XRHealth commercial VR application, after a training, and with and without remote monitoring. A retrospective analysis showed that there were no problematic adverse events or side effects, as well as significant improvements in measured or patient reported outcomes (Orr et al., 2023). In a double-blind, randomized, placebo-controlled study, 168 participants with chronic low back pain had a self-administered behavioral skills-based 8 weeks program composed of 56 VR experiences related to pain diaphragmatic breathing, biofeedback, cognition and emotion regulation, mindfulness, and pain education. The treatment group had significant pain reduction, even 24 months after, showing durable, non-pharmacological, in-home treatment of pain is possible (Maddox et al., 2023).
Due to the Covid pandemics, telehealth services have gained significant attention and acceptance (Wong et al., 2021), and Metaverse-based telehealth is on the agenda (Sampaio et al., 2021). With regards to immersive VR clinical teleconsultation in the Metaverse, there are surprisingly few studies available.10 In 2012, a pioneering remote neuro-rehabilitation system allowed a patient in VR to see the practitioner’s avatar and physically interact with his hand using an active haptic hand. The clinician used a screen and had access to patient’s physiological data (Perez-Marcos et al., 2012). Another proposal was remote clinical consultation where the patient could use a tablet to view the avatar of a doctor whose skeleton movements were captured (Zhang et al., 2019). Another system successfully allowed to perform a clinical and electrocardiographic follow-up of a patient with vasospastic angina, using social VR and ECG, blood pressure and oxygen saturation sensors (Skalidis et al., 2022). Therapists and patients could also see their respective arms movements in the case of upper limb rehabilitation (Sobota et al., 2022). With regards to mental health consultation and teletherapy, where the use of avatars may combine the benefits of face-to-face communication with the anonymity of online text-based communication (Baccon et al., 2019), a study compared the experiences of psychotherapeutic counseling delivered to workers in remote locations in VR and using Skype, showing VR was easy to use, and outperformed videoconference for presence and perceived realism of the session (Pedram et al., 2020). At the group level, telemindfulness has been tested with an early system allowing a mindfulness instructor could lead group sessions of patients in VR (Cikajlo et al., 2017). Another study compared face-to-face, teleconference, and social VR delivered therapeutic group singing interventions by music therapist for people living with spinal cord injury. VR was easy to use, and though it reduced social cues, was praised both for allowing to meet in settings different from daily ones and for reducing inhibition (Tamplin et al., 2020). Social VR was also used to organize focus groups with patients and healthcare professionals on the design of a VR application for low back pain (Amestoy Alonso et al., 2024).
As a conclusion, we can say that, on the one hand, telerehabilitation, which is overrepresented in telemedicine studies (Worlikar et al., 2023), allows patients to self-administer VR activities at home while remaining in contact with health institution. The studies show good adherence and satisfaction, related to the easiness of staying at home versus going to a care center, and VR can effectively be considered as an “immersive therapeutic (ITx) delivery device” (Maddox et al., 2024). Moreover, data can be collected, be it from VR devices or additional sensors (e.g., fine tracking of body positions, or heart rate) so as to provide real time feedback (e.g., correct a leg position), exercise adaptation (e.g., lower the difficulty), as well as dashboards for clinicians. Yet, synchronous monitoring, if any, is only provided using audio communication: to our knowledge there is no system with avatar-based/social VR monitoring or interaction during telerehabilitation, where the practitioner would be present as an avatar to guide and monitor telerehabilitation sessions. On the other hand, VR teleconsultation between patient and clinician avatars, possibly completed by supplementary sensors and devices, has been shown feasible, but only in a few cases. It seems then important to explore how clinical encounter between patients and practitioners could take place in social VR, be it in rehabilitation scenarios, or for actual consultations. This is all the more important for two reasons. First, the lack of social interaction in virtual worlds (whether therapeutic interaction with the clinician or with real or simulated people) has been considered one of the main limitations of current VR applications. Second, impersonating and interacting with an avatar in simulated social activities has proved “crucial for increasing treatment efficacy” (Cerasa et al., 2022). In the next section we present the application domain we chose, our design process, and the main decisions we took.
3 Design of our teleclinic
The research we present here has been developed in the frame of the TECNIS project (22-24), a joint program between the University and the University Hospital of Nantes. The interdisciplinary team was composed of one neuro-psychologist, one psychiatrist, several clinical psychologists, several XR/UX/HCI scientists, a UX researcher and a development engineer. We decided to focus on neuro-psychological testing, because we already had experience in designing ecological VR tools for the testing of executive functions (Ribeiro et al., 2024). Another reason is that testing is a time-consuming activity in a overloaded healthcare sector, that does not rely solely on dialog between clinician and patient, can be instrumented with data from build-in HMD and controller sensors, and can re-occur for longitudinal follow-up. Moreover, to our knowledge, remote VR cognitive testing during teleconsultations in the Metaverse had never been studied, although it seemed technologically feasible, desirable and acceptable. Our aim was then to use current standard VR technology to develop a social VR neuro-psychological testing system, with clinicians remotely supervising testing sessions with patients at home.
3.1 The context of VR neuro-psychological testing
3.1.1 Neuro-psychological/cognitive testing
Neuro-psychological testing aims to characterize individuals in cognitive domains such as memory, learning, motor skills, personality, attention, decision-making, etc. They are used to: a/establish a baseline of cognitive functioning for people at risk, e.g., with neuro-developmental disorders or a family history of neurological disorders; b/distinguish normal changes from aging, depression/anxiety, neurological diseases (e.g., Alzheimer’s disease or stroke) and other factors affecting cognitive functions; c/monitor changes over time and adapt the environment and caregiver support accordingly; and d/formulate plans for future interventions or treatments (medication changes, cognitive training, rehabilitation). Many practitioners are likely to deliver cognitive tests. Psychiatrists, geriatricians, neurologists, pediatricians or neuro-psychologists are specifically trained to administer, calculate and interpret scores in relation to expected results for a given age and condition, taking into account other variables such as motivation, stress, medication, etc.
A test is a set of exercises designed to assess specific cognitive functions, e.g., attention, language, praxis, visuo-spatial ability, memory, social cognition, or executive functions such as working memory, inhibition or flexibility. It typically involves writing (e.g., linking letters and numbers in the Trail Making Test, or symbols in the Digit Substituting Symbol test); drawing (e.g., reproducing a Rey figure); solving problems (finding the best way to achieve a visit, a shopping task); manipulating and putting in a certain order objects such as cubes or rings; completing puzzles; answering questions about events or rules; describing images; and responding to triggers presented on a computer (e.g., reaction time can be used to detect a cue for attention or recognize an emotion). The results of a test can be compared with normative thresholds available for the target population (disease, age, level of education). The validity and fidelity of these tests, and their ability to causally reflect a specific function are still being debated, but, importantly, they can be of predictive interest. That is why neuro-psychological testing is crucial in many areas of medicine and the expertise of practitioners for conducting it is invaluable. Nonetheless, its use is still non-optimal because of: controversial and even obsolete standards across populations; a lack of ecological validity and correlation to concrete real-life situated functioning; a lack of automation to save practitioners’ time; and a lack of availability at the population level, for large screening and monitoring. Distant VR cognitive testing would help tackle some of these challenges.
3.1.2 Neuro-psychological testing in VR
Computers have long been used for neuro-psychological testing, because they allow both to precisely control the stimuli, and to easily collect data and calculate results, saving practitioners’ time. Classical paper and pencil tests could be simply adapted to screen and keyboard use, but brand new ones could also be designed, taking into account the different input and output possibilities offered by the medium. Those tests could also be deemed “virtual reality”-based when 3D gaming environments and controllers were used, and ecological when tasks resembled those that could be carried out in reality (Parsons, 2012). The level of immersion offered by VR based on HMD and body-tracked controllers provides means to largely enhance the ecological validity of the activity (Parsons, 2015), but also to carry out embodied tasks, which imply moving the head, the hands, or more generally the body when standing.
VR cognitive testing benefits from embodied tasks situated in realistic and dynamic environments resembling real-life. Compared to traditional methods, this allows a function-based approach to testing (Parsons et al., 2017), where functions (e.g., the use of memory to carry out a task) are evaluated, rather than constructs (e.g., the size of one’s short term memory). This offers much potential to a more ecological assessment that matches the actual behaviors of patients in their everyday life. The possibility to control the situation in a parameterized way, and to collect behavioral data, unlocks a whole new way to foster innovation. For instance, besides time or error-based classical scores, VR-enabled tracking of activity can be used to understand and assess with a finer grain various aspects of behavior, e.g., using inhibition with hand-tracking (Ribeiro et al., 2021), or attentional bias with eye-tracking (Ghita et al., 2024).
Many VR tests have been proposed and evaluated mostly through their capability to assess problems, practical feasibility, and correlation with classical tests, on that matter, see for instance (Jang et al., 2023). Some are dedicated to assessing one specific function, or several at the same time, for instance using one unique task (Kourtesis et al., 2021). Various cognitive domains have been addressed, such as executive functions (Kim et al., 2021; Ribeiro et al., 2024), attention (Mendez-Encinas et al., 2023), spatial navigation, memory profile, memory deficits (Sobral and Pestana, 2020). Population range from children and adolescents to elder people, with tests aiming at evaluating problems related to ADHD, autism, depression, mild-cognitive impairment, etc. If commercial solutions already exist, large scale clinical evaluations are still needed to converge towards normalized environments, parameters, settings, etc. with stabilized psychometric properties that can be fully integrated into medical practices with standardized indicators.
Current neuro-psychological tests are mainly used in healthcare facilities, with patients being the only ones in VR, either with an automated battery of several tests, or with the accompaniment of a practitioner using a laptop or tablet. Studies on testing at home have been limited,11 and the present research constitute a first step in allowing practitioners to conduct cognitive tests with their distant patients in social VR, providing them with “a sense of ‘being at’ the place [both] critical and beneficial for patient monitoring” (Chengoden et al., 2023). Our proposal takes place in the more general agenda of the “mental Metaverse”, where various mental-health activities would be carried out by patients with both therapist and peers (Navas-Medrano et al., 2023).
3.2 Design process
3.2.1 User research
We followed classical user-centered design. In the first phase we carried out several interviews and focus groups with around 10 stakeholders (neuro-psychologists, psychiatrists, neurologists, geriatrician, general practitioner, expert patient, hospital patient) outside of the team. Our objective was to document what psychiatric patients’ journey are, from detection to long-term follow-up or remission, as well as current medical practices with regards to the use of neuro-psychological testing. We could precisely describe current psychiatric workflows and patient journeys, and create patient and clinician personae. We also confirmed that social VR could be used by patients, by having 3 patients test social VR (Meta Workrooms) to discuss with their practitioner as part of a real appointment at the hospital. This research allowed us to develop our general vision, identify where and when immersive teleconsultations could be useful in patients’ journeys, and write numerous scenarios related to these various possibilities. We could then settle on the topic we would be focusing on, namely neuro-psychological social VR teleconsultation, for carrying out cognitive tests remotely.
3.2.2 Cognitive test workflow
We also observed several test sessions, and described how cognitive tests sessions were conducted. Those testing sessions occur when a comprehensive assessment of one or several cognitive domains is required. Patients are invited to pass several tests that are selected according to medical hypothesis and their history. Sessions begin with neuro-psychologists putting the patients at ease and informing them of the tasks to be performed. Patients then do their best to complete the tasks, the neuro-psychologists observing their behavior and adapting the session according to understanding, difficulty, stress, fatigue or intellectual level, helping them stay focused. It then takes hours to calculate, interpret, report and return the results to the patients. Raw scores are generally transformed into standardized scores to enable comparison with the reference population and with other tests. It also demands good psychological skills to adapt the information to patients’ representations, fears and expectations. Neuro-psychologists or doctors are able to recognize some pattern of abnormalities compatible with certain diagnosis rather than others.
3.2.3 Design process
In the second phase, we held 8 interdisciplinary co-design workshops, each lasting between 2 and 3 h, with at least 6 participants. They were dedicated to specific topics such as the spaces we needed and the transitions between them, the roles of the practitioners, the tests we would use, the waiting room activities, or the contents of the clinicians dashboards. They helped us make our key design decisions, and define the teleclinics we aimed at, its spaces, tools, and interactions. We used classical tools such as Figma for 2D interface design (e.g., panels), and also held immersive collaborative prototyping sessions.12 We had our prototypes tested and commented upon by practitioners, partner patient, several nurses and hospital patients. There were several (at least 2) iterations for all the spaces and the tools we provided to the users.
3.3 Major decisions
Our main design decisions were as follows.
First, immersive remote consultations in the Metaverse between medical practitioners and patients should take place in immersive teleclinics, run by socioeconomic players, such as public or private hospitals or clinics, telemedicine operators, who make VR consultation rooms available to their staff, or lend them to independent practitioners. Teleclinics are mainly a set of spaces, e.g., welcoming spaces, social rooms, waiting rooms, consultation rooms, collective or individual activity rooms, etc. Patients accessing a teleclinic can either possess their own HMD and be autonomous, or necessitate that an assistant be present, who would bring the HMD, set up the access, and accompany them during the session. Activities can be proposed as external modules by third-party vendors.
Second, in the case of a teleclinic for neuro-psychological teleconsultation, we should consider in our scenarios that immersive sessions are integrated within patients’ healthcare paths in a coherent way. A patient should probably have such teleconsultation after a first in-person visit to the practitioner where social VR would have been explained to him. In addition, assistants could be present at home for one-off sessions, while for routine tests and longitudinal follow-up, patient woulds use VR devices themselves.
Third, we should allow patients and clinicians to meet in VR for a full neuro-psychological consultation led by the practitioner, composed of discussions, neuro-psychological testing activities, and debriefings. Moreover, as in conventional practice, both participants should be sitting most of the time, so the meeting would take place on a virtual desk, with each user seating in front of a table/desk in reality. Testing activities could be carried out either on the practitioner’s desk in the consultation room (“desk-based” tests), or in independent VR environments (“independent” tests). In the latter case the patient would have to stand in a free space. In both cases, tests should be driven and accompanied by the practitioner.
Fourth, as in real life, we should provide a waiting room for patients to wait for the practitioner, who could be late. This is because it acts as an important transition space before any medical meeting, all the more so in psychotherapy, to help patients focus.
Fifth, practitioners should be able to decide of the activities beforehand, or during the session. They should be provided with a control panel featuring data-based tools for lived enriched observation of the patient performance during interviews and activities, as well as summary dashboards for post-activity or post-session debriefing. In both desk-based and independent activities, behavioral data should be automatically collected so as to produce indicators for practitioners to access to in dedicated real-time, post-session or longitudinal dashboards.
4 An immersive teleclinic for neuro-psychological testing
The prototype we have built corresponds to our main design choices. It is a working implementation of our vision. The patient and practitioner workflows within the environments are described on Figure 1. We rapidly describe each space (more information is available in the accompanying video13) and the technical architecture of the prototype.

Figure 1. Simplified workflow for a consultation in the TECNIS project. Both users are welcomed in their home space, where they can consult their agenda, specify their avatar, follow tutorials. From there, patients teleport in the waiting room, where several waiting activities are proposed, to spend between 5 and 20 min, while practitioners teleport in the consultation room where they can prepare the upcoming session. When they are ready, practitioners teleport into the waiting room so as to welcome patients, engage in discussion, and invite them to join the consultation room. Once there, practitioners can lead the consultation, propose desk test activities, and discuss the results. At some point, they can invite patients to stand up and head towards the independent activity space, where standing testing can take place, before going back at the desk for other activities or data-based debriefing. Elements provided by the clinic are in white, activity modules plugged into the clinic in gray.
4.1 Spaces
4.1.1 Home space
As in any social VR application, users arrive in and leave the teleclinic through their private home environment, where they can consult personal information and appointments on a command panel, check their avatar, train on the various interactions, etc.
4.1.2 Waiting room
The waiting room (Figure 2, left) is an environment that allows the user to teleport from chair to chair (or bench when outside in the garden), where they can carry out dedicated activities. First, the waiting room is the place where the patient can wait. Among the activities we have designed with the medical members of our team, we implemented the following: one for controlling one’s respiration by looking at a ball changing size (meditation); another for consulting medical information and newspapers on a tablet (therapeutical education); another for looking at large scale videos accompanied with sound (contemplation); and a gardening stand where patients can select and plant flowers creatively (manual activity). Patients can also simply enjoy the garden and its pond from a bench, which would be a second contemplation activity. Second, the waiting room is the place where the patient will meet the practitioner: when ready, the practitioner enters by teleporting on a stool (Figure 2, left). He can then meet with the patient, and ask him to proceed to the consultation room (it is the patient who triggers the teleportation).

Figure 2. Left: The waiting room and the garden feature several chairs where patients can carry out various waiting activities (e.g., on the left of the image, the patient holds a tablet with therapeutical information). When ready, the practitioner teleports into the room to meet the patient (right of the image), before they enter together the consultation room. Middle: The consultation room features a desk where desk-based testing activities can take place (here Tower of London). The practitioner has a control panel for the test, a personal screen and a shared screen if needed. The green teleportation mat behind the patient is where he needs to go to teleport to an independent testing environments. Right: Independent environment for testing executive functions where the patient has to take books from a pile on the table and put them at the right place in the library. The practitioner is also present in the environment, observing the patient directly and by attending at behavioral indicators on her panel.
4.1.3 Consultation room
The consultation room (Figure 2, middle) is the office of the practitioner. It features a desk, where the practitioner has access to a control panel (Figure 3, left) and a screen for sharing information with the patient (Figure 3, middle). The agenda, patient information, session planning and descriptions of the tests, etc. can be consulted on the panel. The control panel also allows to launch tests, monitor and control their unfolding, and access the resulting data on dashboards. In our prototype, we have implemented a fully functional version of the Tower of London test (Krikorian et al., 1994), where the patient has to reproduce a model as quickly as possible. The clinician panel features information on the current step, elapsed time, success and failures, time to completion, average speed, etc. The debriefing dashboard allows commenting aloud on the performance of the patient.
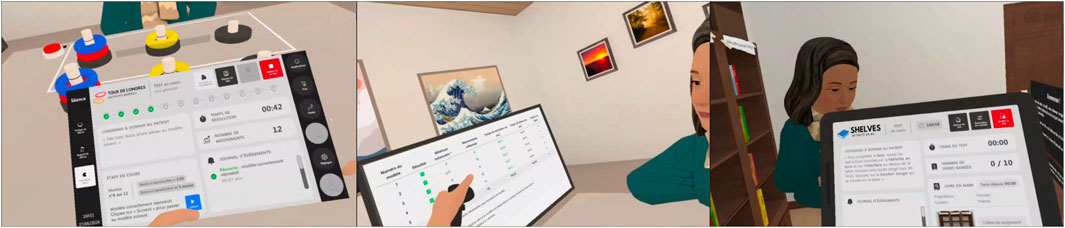
Figure 3. Clinician control panels for Tower of London (left) and Shelves (Right). Control panels contain instructions to give to the patient, buttons to control the test, some metrics such as elapsed time or number of errors, and an event journal. The debriefing dashboard features aggregated data that can be used to debrief with the patient (middle).
4.1.4 Independent activity spaces
Lastly, both can go together into independent tests environments, where patients will carry out activities under the supervision of the practitioner, who can also control and monitor the task with the control panel on the tablet (Figure 3, right). In our implementation, we reused an existing environment for embodied ecological testing of mental flexibility and switching executives functions, called Shelves (Ribeiro et al., 2024). For this test, the clinician dashboard features information on the right position for the current book, success rate, average speed, etc.
The design of the transition from the consultation room to an independent environment deserves a specific description. Indeed, when in an independent environment (Figure 2, right), both avatars are standing. However, only the patient is standing in reality, as this is necessary for embodied tests, while the practitioner remains seated and embodies a standing avatar. The “two avatars standing” situation is attained before any teleportation, on a specific place of the consultation room, represented by a mat. To get there, the patient must stop sitting in reality, walk to the designated area, and wait for the practitioner’s avatar to join, before they can both teleport. This means that configuring the space on the patient side needs defining both an horizontal space corresponding to the available desk or table (Figure 4a), as for the clinician, but also an independent activity space (Figure 4b). We implemented the patient transition from chair to mat using mixed-reality (Figure 4c): patients can see both the room and the mat they have to reach, and can safely stand and walk to the mat position (Figure 4d), where get back to the VR environment of the consultation room. Getting back from an independent environment to the desk is done the same way, only in reverse.
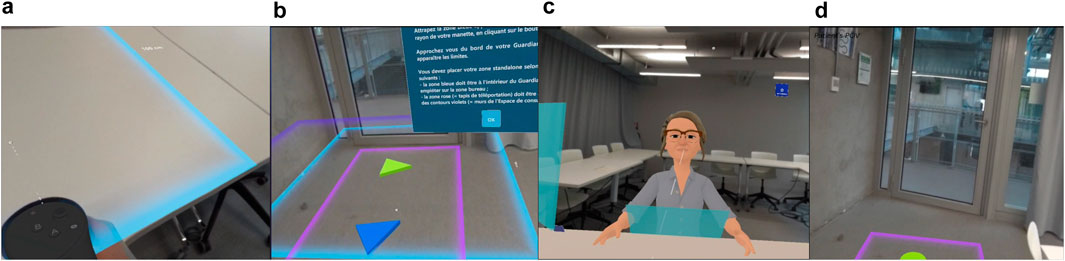
Figure 4. From left to right: (a) setting up the desk zone, (b) setting up the independent activity zone, (c) switching to mixed-reality (patient view), (d) walking to the mat in mixed-reality (patient view).
4.2 Technical architecture
The teleclinic is a set of environments (Figure 5). It was developed on Unity (2021.3.32f1) for Meta Quest HMDs, particularly Quests Pro, which feature eye- and face-tracking, allowing enhanced communication between patient and practitioner. We used Mixed Reality Toolkit 2 (MRTK2) and Oculus Integration SDK for XR interactions and Photon Unity Networking (PUN) 2 (2.46) for multiplayer and social VR activities. User behavioral data (head/hands trajectories, user interaction, system events) is collected using a custom library, and stored in a server-based MySQL database. Practitioners’ dashboards are generated from the data with Node.js, and integrated in VR as web pages. We developed some generic services14 for immersive teleclinics (navigation, zone management, control panel, dashboarding, etc.).
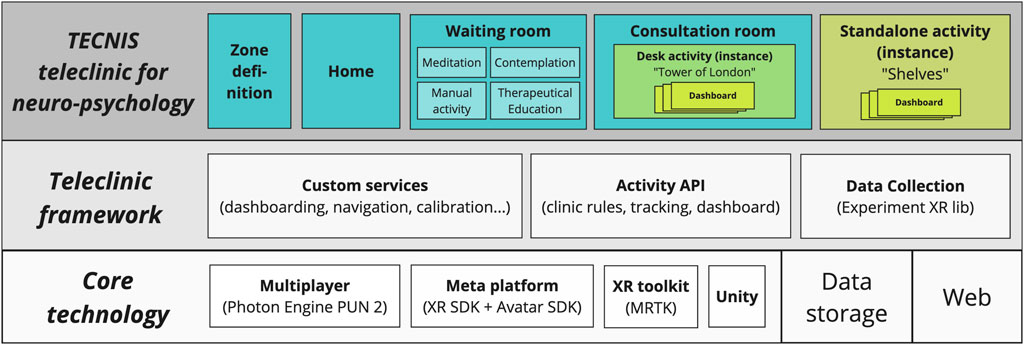
Figure 5. Technical architecture. Bottom: Core technology layer for Social VR, Web, Data. Middle: Framework layer composed of libraries for data collection, activities, and clinic services. Top: our instance of Teleclinic with the various environments, featuring two activities that implement the Activity API: Tower of London (desk activity) and Shelves (independent activity).
Following our vision, the desk-based and the independent activities we integrated are thought of as if they were implementing an “Activity API” (see Figure 5, framework layer). The idea is that any activity following such API requirements could be integrated into a clinic as a module, be it home-made or obtained from external vendor. The activity API would then define how an activity should 1/be composed of a set of assets, 2/follow “teleclinic rules” (e.g., have two users, one patient and one practitioner, with different interactions, a tutorial and a main activity, etc.), 3/implement the API for common (e.g., beginning, end, steps, etc.) or specific tracking, 4/implement adequate dashboards for the clinician panel.
5 Evaluation
5.1 Objectives
The evaluation and validation of the cognitive tests was not addressed in this evaluation phase, as this could be done later or by reusing already validated VR tests.
As a first nonclinical evaluation, the study was carried out with healthy subjects who did not have any psychological or cognitive problems, nor had any experience in neuro-psychological assessment. Healthy participants can be seen as future patients and users of teleclinic services. For the following of the paper, we will use “pseudo-patients” to talk about the group of healthy subjects testing the teleclinic from the patients’ point of view. Regarding the practitioners, we were looking for feedback from psychologists, neuro-psychologists or psychiatrists who currently have a clinical practice and regularly run clinical interviews and/or cognitive tests.
5.2 Protocol
The evaluation was carried out over two sessions, for both pseudo-patients and practitioners. It was based on a two-stage scenario: 1/discovery of the teleclinic and an initial consultation between clinician and pseudo-patient accompanied by tutorials for the tests; 2/a consultation focusing on neuro-psychological assessment with two cognitive tests and a debriefing at the end (see details in Figure 6). During the tests, practitioners could manage the activity and access real-time indicators on a control panel. Each VR session lasted around 30 min.
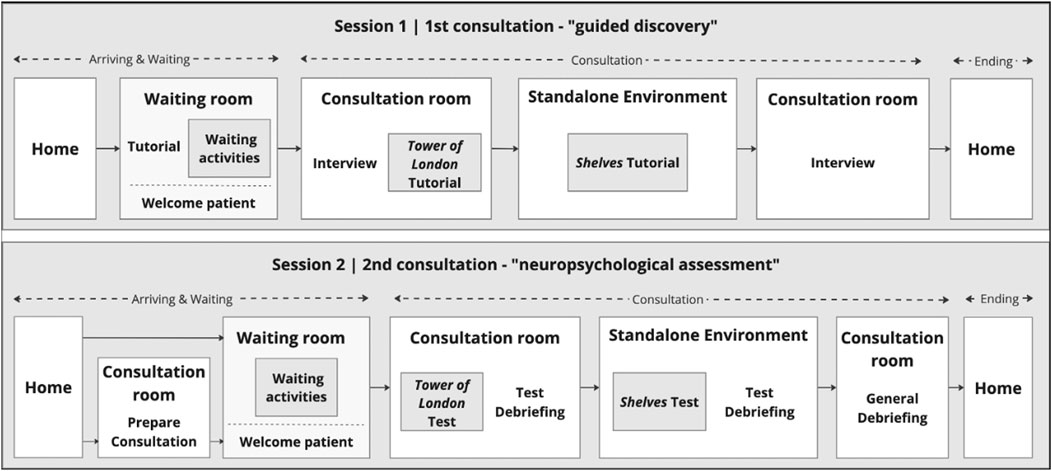
Figure 6. Description of the two evaluation test sessions.
Except for the last test, these sessions were conducted separately for pseudo-patients and practitioners, with one co-experimenter playing the second role (practitioner or pseudo-patient respectively). Another co-experimenter accompanied and observed participants through the test and conducted the interviews. The final test was carried out on the same scenario, but under more realistic conditions, bringing together in the virtual teleclinic a healthy subject—at home—and a practitioner at the University.
Various subjective and objective measures were collected during the sessions. Before the first session, sociodemographic questionnaires as well as technology and VR use questionnaires were administrated in order to better profile the participants. During the VR sessions, a first-person video (with audio) as well as various activity logs (e.g., behavior in waiting room; successes/errors in cognitive tests; grabbing/releasing a ring in Tower of London respectively a book in Shelves, etc.) were collected. After the two sessions, the Simulator Sickness Questionnaire (SSQ) (Kennedy et al., 1993), the System Usability Scale (SUS) (Peres et al., 2013) and the Multimodal Presence Scale (MPS) (Makransky et al., 2017) were completed, and an adapted UTAUT2-based questionnaire (UTAUTQ) (Venkatesh et al., 2012) was filled after the second session only. All questionnaires, except UTAUTQ, were the same for pseudo-patients and practitioners. UTAUTQ was adapted to consider the different roles. With regard to acceptability, we chose a version of the UTAUT2 questionnaire validated in French for a medical application (Pagé et al., 2023). Questions were slightly modified for our service. In addition, questions about the Habit dimension were removed for pseudo-patients.
Finally, after each session, a 30-minute semi-structured interview was conducted to explore the various dimensions covered in the questionnaires. We asked questions about: teleclinic as such, interactions, waiting room and associated activities (for patients), testing activities and debriefing (for both, but with different points of view), appropriation of the tool along the session, and projection in future use.
5.3 Experimental conditions and participants
The experiment required two rooms, one for the participant and the main experimenter, and one for the second teammate who interacted in VR with the participant. Each room was equipped with a desk table, a chair and a Meta Quest Pro HMD. 4 male/female patient/practitioner avatars were created before the experiment and assigned to the participants. With pre- and post-questionnaires, interviews and VR sessions, each test lasted around 90 min. In addition to the two test sessions, practitioners were given an introductory session to familiarize themselves with the VR application, so as to be able to accompany patients in the teleclinic and manage the tests with control panels. This session lasted about 1 h and was held just before the first test session for reasons of participants availability. The interval between the two sessions varied between 1 and 14 days for both pseudo-patients and practitioners.
11 healthy subjects (7F, age = 22 to 57, mean = 39.3, std = 10.5) took part to the experiment as pseudo-patients and 5 practitioners (3F, age = 27 to 41, mean = 32.2, std = 5.4). Healthy subjects were recruited using a convenience sampling method and were compensated €40 for their participation. Clinicians were recruited at the Nantes University Hospital as colleagues of project members. They were not compensated for their participation. The lower number of clinicians compared to healthy subjects is mainly due to the difficulty of booking hospital practitioners for two rather long test sessions. All pseudo-patients, except one (mean score = 2.7/4) were very familiar with the digital technologies (mean score
On the technical side, framerate was good (around 72fps) during all sessions. At the hospital, we had a few minor network problems due to the use of the 4G network (2 clinicians, no link to their answers). We also had a few short periods of desynchronization when returning to the consulting room from the Shelves environment, which did not prevent the collection of traces or the generation of dashboards.
5.4 Results for pseudo-patients
Participants did not experience cybersickness in either session (all SSQ scores
MPS measures the sentiment of Physical Presence, Social Presence and Self Presence on scales from 1 to 5. Figure 7 shows the presence scores for all pseudo-patients for both sessions. We observe very high level for Physical (
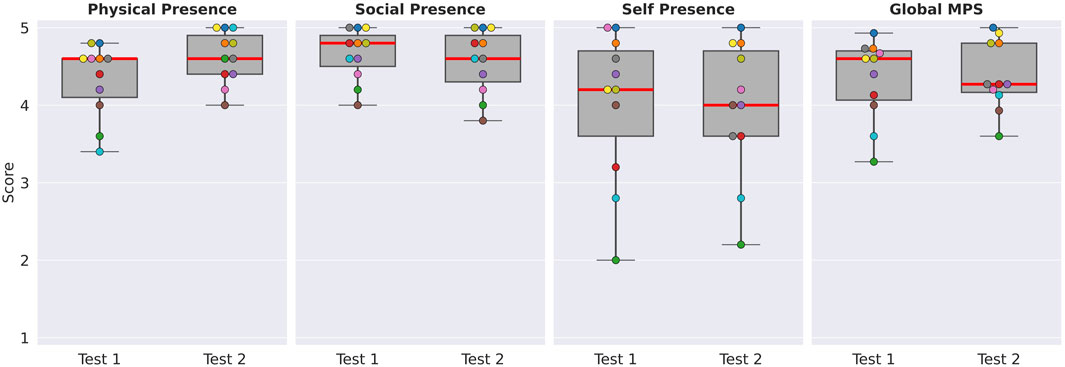
Figure 7. Presence scores (3 dimensions + global) for pseudo-patients for the first and second sessions. Each point represents a unique participant. The box plots represent the interquartile range, and the red line the median.
Acceptability was assessed only after the second session on scales from −3 to +3 for the following dimensions: Performance Expectancy, Effort Expectancy, Social Influence, Facilitating Conditions, Hedonic Motivation, Behavioral Intention.
Figure 8 shows the acceptability scores for pseudo-patients’ point of view. All the dimensions were highly positive, with a median equals to or above +2, except for Social Influence (median = +1.67, IQR = 1.67).
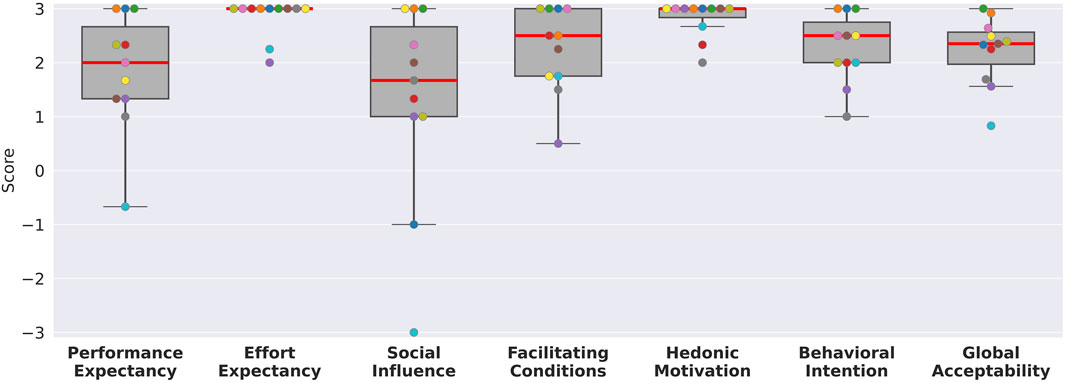
Figure 8. Acceptability scores (bottom: 6 dimensions + global) for pseudo-patients. Each point represents a unique participant. The box plots represent the interquartile range (IQR), and the red line the median.
5.5 Results for practitioners
As for pseudo-patients, SSQ scores show no or minimal symptoms of cybersickness for practitioners (
SUS scores show that usability was considered as acceptable or good for all the practitioners in the first session (
Physical and Social Presence were rated slightly positively during the first session (Physical Presence:
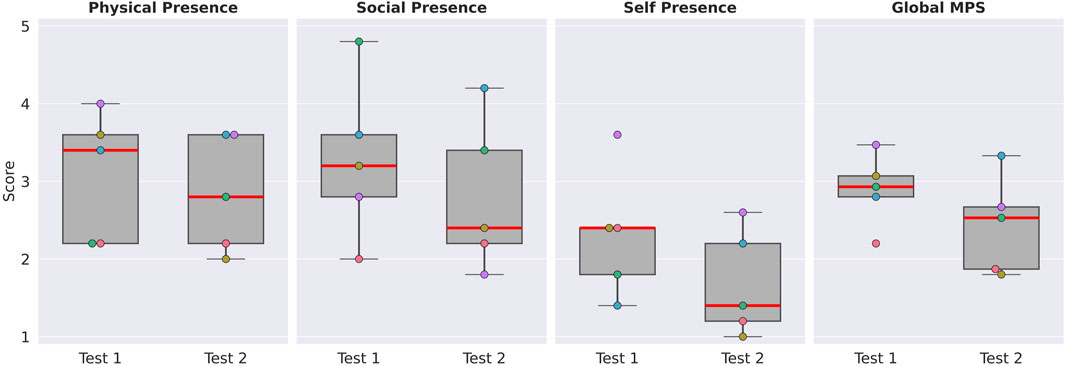
Figure 9. Presence scores (3 dimensions + global) for practitioners for the first and second sessions. Each point represents a unique participant. The box plots represent the inter-quartile range, and the red line the median.
Scores for acceptability show important dispersion between the five practitioners (Figure 10). Performance Expectancy, Social Influence and Behavioral Intention got negative or neutral scores for all. Habit got neutral or negative scores for all except one with a slightly positive score. Effort Expectancy got positive scores for all and Hedonic Motivation got positive scores for all except one with a slightly negative score. Facilitating conditions got 3 medium positive scores, one slightly negative and one strongly negative scores.
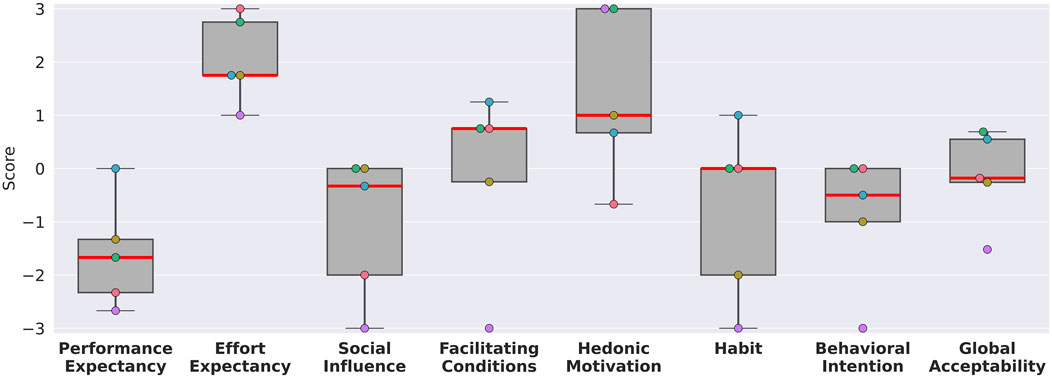
Figure 10. Acceptability scores (bottom: 6 dimensions + global) for practitioners. Each point represents a unique participant. The box plots represent the inter-quartile range, and the red line the median.
6 Discussion
Our results show strong differences between the perceptions of healthy subjects playing the role of patients, and neuro-psychology and psychiatry practitioners. We will discuss them considering our main objectives to evaluate the system and its clinical potential, illustrated with some qualitative observations and verbatims extracted from the interviews. We will then discuss the more general lessons we learned with regards to teleclinics in the Metaverse.
6.1 On the design choices for our prototype
6.1.1 User interactions and communication
From the pseudo-patients’ points of view, the VR clinic application was judged pleasant and highly usable. Observations show that none of the participants had to repeat the tutorials during the second session, indicating easy learning even for people without VR experience. Practitioners, for their part, raised more issues about usability, mentioning problems linked to the multiplicity of actions and the complexity of using control panels while observing patients (e.g., PR1 Test1: “Apart from the tablet, which may be a little obtrusive.”; PR2 Test2: “I did not even see that it was there [the panel with indicators]. But instinctively there, in any case, what I looked at was what the patient was doing in front of me.”). This may be explained by the little time they had to get used to a system in which they had to guide patients through consultations and cognitive tests. In addition, some double-checking actions designed to reinforce the sense of agency of clinicians leading the consultation and guiding patients step by step through activities were deemed complex (e.g., PR3 Test2: “I think there are a lot of steps here”), and should probably be simplified.
Unlike pseudo-patients, clinicians did not feel a high level of presence in the virtual environment, though they were using the same technical system. At a general level, we can hypothesize that this is due to the difference in the tasks they had to carry, as well as to the natural reflective practice of professionals who may have also applied to the virtual environment and its status. Concerning Self Presence, it can be explained by the fact that, to shorten the test duration, participants could not choose their own avatar; furthermore, they had no opportunity to look at themselves in the virtual world (e.g., using a virtual mirror). This can be easily improved in a new version of the VR application and a new evaluation phase. More relevant to the proposed service, healthy subjects found interactions and communication with the practitioner natural. They reported a feeling of closeness and confidence in the clinicians, and the social dimension of the presence was highly rated (e.g., PA1 Test1: “I felt she was benevolent.”; PA4 Test1: “You really get the impression of a real person, a real human presence, […], and it gives more proximity.”). On contrast, Social Presence was judged weak by the practitioners, particularly during the second session in which they had to conduct a clinical interview and observe the patient performing cognitive tests (e.g., PR5 Test2: “It is not just a matter of voice […] In clinical interviews [we talk about] mimicry, […], how we position ourselves in relation to the person we are meeting. But then, we cannot do that at all.”; PR2 Test2: “I always come back to the same thing, but I miss the person in front of me. […] to have all the non-verbal reactions, the little mimics”). Mental health caregivers can be considered experts in interpreting subtle nonverbal cues in communication, and the quality of avatars appeared not good enough to reproduce the gestures, postures, facial expressions and gazes essential for conducting psychological and psychiatric consultations, despite the eye- and face-tracking capabilities of the HMDs we used.
6.1.2 Spaces
Concerning the design of the clinical spaces, the interviews show that the waiting room was much appreciated by the pseudo-patients, especially gardening and video meditation activities. It helped reduce the perception of waiting time and feelings of stress before consultation (e.g., PA10 Test1: “What was nice was that the different activities kept us busy, because you never really know what to do in a waiting room, especially if you do not have a phone.”; PA6 Test1: “It was a nice surprise to find the garden, because it gives a feeling of openness. […] of serenity.”).
All pseudo-patients and clinicians felt they were actually in a consultation room and that the distance between them was similar to real conditions (e.g., PA8 Test1: “It is like a real office […]. Yes, you feel safe, you feel you can talk, […] as if you were there, in the same room physically”; PR2 Test1: “it recreates quite well the office atmosphere you might find here, or even elsewhere in consulting.”). However, the consultation office was perceived as too empty, white and cold from both clinicians and pseudo-patients’ point of view, especially compared to the waiting room, which was cozier (e.g., PR4 Test1: “As a result, it is a bit, how do you say, sanitized. […], it is not very personalized. […] I do not know if the practitioners, for example, will be able to choose the works they put in, to personalize them a little?”; PA9 Test1: “Otherwise, the room, it seems to me, was a little emptier, but at the same time decorated.”). We designed something neutral to allow everyone to project themselves, but consultation spaces could clearly made more enjoyable.
6.1.3 Design
Mock-ups were an essential part of the co-design process that led to the aforementioned spaces and interaction. Using ShapesXR gave us the opportunity to test and adjust prototypes in VR directly. This tool was particularly crucial in ensuring clear communication between members of the working group who had different VR experiences, and it saved development time. Using such a tool also facilitated communication between the UX designer and VR programmer, who were working full-time on the project, to better share technical and UX constraints, which made alignment easier for future iterations.
6.2 On the potential for clinical purposes
Usability and presence issues may, to a certain extent, explain low results on acceptability for practitioners but we assume that the following other elements were also implicated.
Firstly, some essential features for neuro-psychologists, although designed, had not been integrated into the current version of the teleclinic, such as note-taking and changing the point of view for observation in independent test (e.g., PR3 Test2: “Afterwards, once again, what I miss is being able to note at the same time”). In addition, in the instructions, we entitled the name of the second session “neuro-psychological assessment” which was understood by practitioners in the strict sense of as a comprehensive checkup prior to diagnosis or medical care decision, often based on a full battery of standardized tests, that may be more difficult to conduct remotely. Interviews show that the practitioners found more potential in the service for longitudinal follow-up mixing testing and remediation activities (e.g., PR3 Test2: “Afterwards, for different types of follow-up or care, it could work”). Also, in order to simplify the experimental protocol, the consultation plan was fixed for both sessions and based on only two cognitive tests. This implies that the consultation did not fully correspond the current clinical practice of all participants. Even though it was clearly stated, in the test instructions, that the consultation procedure, the available cognitive tests and the information displayed in the debriefing dashboards could be tailored by the practitioner, participants showed difficulties in going beyond the choices made for the test in order to project the proposed tool into their clinical practice. Another barrier to acceptability seems to be a lack of knowledge about cognitive testing in VR and its scientific validity (e.g., PR3 Test2: “It is not possible to compare tests performed in virtual reality with those performed in the office.”), whereas it has been widely studied and it is already used in real clinical context (see 3.1.2). The benefits of cognitive testing in VR support the value of this teleclinic, and there would certainly be a need to train practitioners in its use. Furthermore, during the interviews, practitioners expressed concern about the patients’ ability to use the VR system, whereas results show the opposite.15 This means that clinicians should have means to be reassured about the way their patients are actually using the system. It is also worth noting that all the practitioners were working in a public hospital where they may have less freedom in their clinical practice and a high work pace making them less open and less inclined to change.
For healthy subjects as pseudo-patients, the underlying immersive teleconsultation service achieved a high level of acceptability. During interviews, they indicated that they would be willing to use this service if it were offered by their caregivers and made clinical diagnosis and follow-up more accessible, easier, quicker (e.g., PA11 Test2: “sometimes it is practical to be able to do it at home, for all sorts of reasons […] will I make it to my appointment on time? Well, you do not have that problem at home […] You just go home, log on and do it.”.) It was stressed as important that a real doctor (and not an AI) should be behind the avatar, and that patients could be accompanied by a professional during the consultation if necessary. A limitation of the study might be the age of the participants for the pseudo-patients’ point of view (under 57 years old), whereas older people should be more concerned by neuro-psychological assessment and follow-up. Although previous work shows us that VR cognitive testing is well accepted and successful with elderly patients (Ribeiro et al., 2024), suggesting that this should not be a problem, it will be necessary to extend this evaluation to older users to confirm the good results obtained on usability and acceptability. Finally, both practitioners and pseudo-patients stressed that a real first consultation is necessary to meet for the first time and to ensure a good therapeutic alliance.
For us, all these results validate the main principles of the medical (neuro-)psychological encounter in social VR, although work is still needed to assess the real added value in clinical use, so as to get better acceptance by practitioners. One limitation of our study is that the second role was played by a co-experimenter and not a real clinician/patient in both conditions. In the short term, to assess the clinical potential more accurately, it will be essential to test the prototype in a realistic situation with practitioners and patients, enabling clinicians to organize their consultation according to their habits and real clinical objectives.
6.3 Towards teleclinics in the metaverse
A first point to discuss is the generalizability of our results. Our prototype focuses on neuro-psychological testing in social VR, but if some findings may only apply to equivalent systems, other may provide us with information on how to build mental health or even general immersive teleclinics. For instance, on the patient side, our results show that patients should easily follow immersive consultations of any sort in a teleclinic if the system is well designed, so the important question for immersive teleclinics may be mostly related for them to the availability of HMDs at home, or of assistants to supervise sessions at home,16 or of local facilities where both HMD and assistance could be provided. On the clinician side, the low number of participants, and their belonging to a public hospital may not allow generalization to all neuro-psychologists, or mental health practitioners, or clinicians.
Clinical validation will obviously be needed for immersive teleclinics to develop, which would implicate comparison to non-VR alternatives on several metrics, such as patient adherence or effectiveness of care at different timescales, as well as acceptability both for patients and practitioners. This would allow to determine for which healthcare practices social VR-based distant care may be useful, and in what conditions, ranging from fully distant interactions to occasional VR encounters between otherwise classical sessions. With regards to our specific use case, it would be difficult to compare our clinic to a videoconferencing system, because to our knowledge there are no real cognitive tests in such teleconsultations, so the comparison would be more feasible with simpler mental healthcare (e.g. patient interviews in videoconference vs. social VR). We would better compare our system to neuro-cognitive consultations in reality, or to the use of VR test in medical venues. Our experience suggests that immersive distant neuro-cognitive testing would be, for now, better suited for early detection or longitudinal following than for full-fledged neuro-cognitive assessment. Indeed, the stakes may be too high for distant decision, with respect to the important consequences on the life of the patients, so clinical validation should rather focus on detection/follow-up. Another topic that deserves interest is the construction and maintenance of the therapeutic alliance in social VR. At the session level, work is needed to determine which visual and animation quality of avatars is necessary to build adequate therapeutic relationship, be it for psychotherapy, where it is very important, or other medical practice where it might be. At the multi-session level, the maintenance of the relationship along the sessions should be studied, either for full VR relation or a mix of VR and in-person sessions.
Now, when it comes to adoption, as we already said, it is necessary to give more knowledge to clinicians about the scientific and clinical validity of the VR healthcare tools and activities for diagnosis and remediation that are offered in an immersive teleclinics. It also seems necessary that the institution (hospital, clinic) provide clinicians with adequate infrastructure, by integrating consultation in VR in their daily work organization. This means having dedicated time slots for VR remote consultations, or the possibility to easily switch from real to virtual consultation, and in the case of shared offices, the availability of quiet small rooms.17 A factor for adoption may also be the freedom for clinicians to personalize their consultation space as we have seen for our clinic, and to adapt the sessions as they see fit (even for testing, having a fixed consultation plan was deemed too constrained in our case). Considering infrastructure needs, social VR can only work with an adequate network connection, which means that a health facility such as an hospital would probably need a dedicated network separated from the main one to ensure both security and guaranteed bandwidth.
With regards to training, and even if one training session was enough for clinicians to use our system, it was not sufficient for guiding patients, nor going deeper into the parameters of the system, i.e. to use precisely clinical indicators and carry their own consultation as they wished. This means that more training is needed for professionals, as for any domain application, but this could complicate experimenting with them. One training session seemed enough for patients. In any case, we did not let practitioners nor patient set up the HMD by themselves, so minimal training also seems important for both so as to learn how to keep an HMD powered, launch applications, etc. Taking example on mobile phones that the vast majority of the population knows how to handle, we are inclined to think it is may not be too complicated.
On the technological side of immersive teleclinics, even if our general approach (cf. Figure 5) is that there should be an activity API that would allow us to include third party activities into a teleclinic, the associated technology does not already exist. In our case, for example, even if we tried our best to separate the activities from the main teleclinic codebase, adding an existing desk cognitive test would still need us to add its code into the consultation room. Another approach would be to directly integrate the execution of a VR environment inside another one (e.g., embedded at runtime Tower of London in the consultation room), which is still an open technical challenge.18 Now if we consider independent activities such as the Shelves environment, even if multiplayer transition was available, we would still have to add the code of the environment into our global project, so as to access services such as trace collection or practitioner’s control panel. Full-fledge Metaverse technology would here be needed, allowing to smoothly integrate teleclinic spaces, activities that can be carried inside them, external spaces belonging to the clinic, global multiplayer interaction with avatars, as well as data-related services.19
Lastly, lots of challenges remain to effectively build immersive teleclinics integrated in the medical ecosystem, as this would implicate multiple medical and technological stakeholders, and pose legal and regulatory issues related to patients’ data management and medical certification. Questions may also arise in relation to cost-effectiveness and resource implications for medical facilities, and business models for activity providers, etc. To us, the only way to advance in that direction is to develop and assess the value of research prototypes of sufficient ambition that would allow to identify the main issues. This means that designing adequate workflows and associated prototypes is a necessity. For our application, we adopted a user-centered approach to design, from ethnographic study to co-design workshops up to development iterations including prototype testing. The diversity of skills and expertise within the co-design group enabled us to approach the project with an holistic perspective, ensuring that usability, clinical, technical and data issues were taken into account throughout. All these considerations reinforce the legitimacy of the proposed system, however, despite our best efforts, problems and challenges remained at several levels, notably related to the diversity of concrete clinical practices. On our side this shows the need to open the approach to a wider range of mental health caregivers, e.g. work with private practices. On a more general note, this illustrates the difficulty of designing such complex and innovative systems, that can only be tackled by integrating a lot of stakeholders into ambitious projects.
7 Conclusion
In this paper we first justified the need to explore what teleclinics in the Metaverse could be, then we presented the rationale, the design, the implementation, and a preliminary evaluation of the first of its kind social VR application for neuro-cognitive teleconsultation. Our clinic features a waiting room, a consultation room for interview and desk-based testing, and a space for independent testing. We evaluated the system and the consultation workflow with 11 healthy participants playing the role of patients, and 5 practitioners. The results show that all participants were able to project on how they would use the system in the future. Pseudo-patients had no problem with the system, and were willing to use it for neuro-psychological appointment. Practitioners were more reluctant, explanations being related to remaining usability problems, the lack of knowledge on the value of VR tests, as well as a the quality of the avatars deemed insufficient for psychological interviews. Our system has the status of a working prototype allowing a first assessment of what could be a teleclinic in the Metaverse where patients and practitioners would carry out their activity. Though numerous challenges remain ahead of us before the medical Metaverse becomes a reality, our activities and spaces clearly showed their value. Our next step it to conduct clinical studies with real patients by focusing on the most promising use cases, given the state of the technology, which would be longitudinal following of the cognitive capacities from known patients at home. We will evaluate this scenario, among others, in our follow-up project on immersive prevention centers for mental health.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité d’Ethique, de Déontologie et d’Intégrité Scientifique de Nantes Université (CEDIS) IRB00013074 (approval number 07052024). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YP: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. TV: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. DA: Conceptualization, Writing – review and editing. HB: Investigation, Methodology, Software, Writing – review and editing. MG: Investigation, Software, Writing – review and editing. ST: Conceptualization, Writing – review and editing. SB: Conceptualization, Funding acquisition, Investigation, Supervision, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project (September 22- August 2024) was partially funded by French Competitivity program “Plan de relance.”
Acknowledgments
Professionals and patients who were interviewed, participants to the experiment.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2025.1545569/full#supplementary-material
Footnotes
1We insist on the adjective, as in the medical domain or in psychology, virtual reality can still denote “video games” experienced on 2D screens.
2See two recently appeared journals: JMIR XR and Spatial Computing and Journal of Medical Extended Reality.
3e.g., Nesplora for cognitive testing, HealthyMind for pain management during small surgery, C2Care for exposure therapy.
4e.g., Eyesoft for orthopsy, XRHealth for neuro-rehabilitation, AppliedVR for chronic pain management.
5Various sub-communities meet regularly on platforms such as VRChat or Rec Room.
6With innovative naming, e.g., MedVerse (Cerasa et al., 2022) or CardioVerse (Skalidis et al., 2023).
7For instance XR, 3D modeling, edge computing, computer vision, HCI, quantum computing, big data, digital twins, 5G, IoT, AI, robotics, and blockchain (Chengoden et al., 2023), all considered likely to enable new healthcare service offerings and new distribution channels.
8Either on ad hoc environment on social VR platform such as VRChat, or in dedicated tools such as the “Connect” application from XRHealth.
9There were some proposals of clinics or hospitals in the Metaverse, but those merely corresponded to announcements during the Metaverse hype, and remained mere ideas that did not survive it.
10A search on “Metaverse” gave 0 result in May 2025 for the Journal of telemedicine and telecare, “Social VR” 1 result; “social virtual reality” 0 result.
11We can however mention an early proposal for astronauts (Galunder et al., 2018), and the fact that exercising systems such as EnhanceVR could play this role (Brugada-Ramentol et al., 2022).
12Using ShapesXR.
13See https://www.youtube.com/watch?v=fLZfp1H8gas
14For a full-fledge framework, we would have to add services related to management of agendas, users, patient pathway, billing, etc.
15Our informal initial evaluations in the hospital also showed no problem with real patients interacting in VR with their practitioner, and patients use prescribed mental health-related products at home.
16The space needed on the patient side is limited to a table and some free space nearby for stand-up activities (around 150 × 150 cm), and can be easily found.
17All the space needed for consultation on the practitioners’ side is a chair and a small desk.
18Reflections from Steed (2024) may be of use on that matter.
19In our case, data was collected in a server, and dashboards integrating behavioral and scoring indicators for neuro-psychological tests were implemented on the web, facilitating the access of data, avoiding overly complex 2D panels in native VR and enabling the reuse of these dashboards in web applications for clinical follow-up. However, this also addresses technical issues for sharing and updating web views in multiplayer VR applications.
References
Amestoy Alonso, B., Donegan, T., Calvis, I., Swidrak, J., Rodriguez, E., Vargas-Reverón, C. L., et al. (2024). Focus groups in the metaverse: shared virtual spaces for patients, clinicians, and researchers. Front. Virtual Real. 5. doi:10.3389/frvir.2024.1432282
Baccon, L. A., Chiarovano, E., and MacDougall, H. G. (2019). Virtual reality for teletherapy: avatars may combine the benefits of face-to-face communication with the anonymity of online text-based communication. Cyberpsychology, Behav. Soc. Netw. 22, 158–165. doi:10.1089/cyber.2018.0247
Baghaei, N., Chitale, V., Hlasnik, A., Stemmet, L., Liang, H.-N., and Porter, R. (2021). Virtual reality for supporting the treatment of depression and anxiety: scoping review. JMIR Ment. Health 8, e29681. doi:10.2196/29681
Brugada-Ramentol, V., Bozorgzadeh, A., and Jalali, H. (2022). Enhance VR: a multisensory approach to cognitive training and monitoring. Front. Digital Health 4, 916052. doi:10.3389/fdgth.2022.916052
Carl, E., Stein, A. T., Levihn-Coon, A., Pogue, J. R., Rothbaum, B., Emmelkamp, P., et al. (2019). Virtual reality exposure therapy for anxiety and related disorders: a meta-analysis of randomized controlled trials. J. Anxiety Disord. 61, 27–36. doi:10.1016/j.janxdis.2018.08.003
Cerasa, A., Gaggioli, A., Marino, F., Riva, G., and Pioggia, G. (2022). The promise of the metaverse in mental health: the new era of MEDverse. Heliyon 8, e11762. doi:10.1016/j.heliyon.2022.e11762
Chengoden, R., Victor, N., Huynh-The, T., Yenduri, G., Jhaveri, R. H., Alazab, M., et al. (2023). Metaverse for healthcare: a survey on potential applications, challenges and future directions. IEEE Access 11, 12765–12795. doi:10.1109/ACCESS.2023.3241628
Cieslowski, B., Haas, T., Oh, K. M., Chang, K., and Oetjen, C. A. (2023). The development and pilot testing of immersive virtual reality simulation training for prelicensure nursing students: a quasi-experimental study. Clin. Simul. Nurs. 77, 6–12. doi:10.1016/j.ecns.2023.02.001
Cikajlo, I., Staba, U. C., Vrhovac, S., Larkin, F., and Roddy, M. (2017). A cloud-based virtual reality app for a novel telemindfulness service: rationale, design and feasibility evaluation. JMIR Res. Protoc. 6, e6849. doi:10.2196/resprot.6849
Dwivedi, Y. K., Hughes, L., Baabdullah, A. M., Ribeiro-Navarrete, S., Giannakis, M., Al-Debei, M. M., et al. (2022). Metaverse beyond the hype: multidisciplinary perspectives on emerging challenges, opportunities, and agenda for research, practice and policy. Int. J. Inf. Manag. 66, 102542. doi:10.1016/j.ijinfomgt.2022.102542
Ehrlich, J. R., Ojeda, L. V., Wicker, D., Day, S., Howson, A., Lakshminarayanan, V., et al. (2017). Head-mounted display technology for low-vision rehabilitation and vision enhancement. Am. J. Ophthalmol. 176, 26–32. doi:10.1016/j.ajo.2016.12.021
Galunder, S. S., Gottlieb, J. F., Ladwig, J., Hamell, J., Keller, P. K., and Wu, P. (2018). “A VR ecosystem for telemedicine and non-intrusive cognitive and affective assessment,” in 2018 IEEE 6th international conference on serious games and applications for health (SeGAH), 1–6. doi:10.1109/SeGAH.2018.8401347
Ghita, A., Hernandez-Serrano, O., Moreno, M., Monras, M., Gual, A., Maurage, P., et al. (2024). Exploring attentional bias toward alcohol content: insights from eye-movement activity. Eur. Addict. Res., 1–15doi. doi:10.1159/000536252
Howett, D., Castegnaro, A., Krzywicka, K., Hagman, J., Marchment, D., Henson, R., et al. (2019). Differentiation of mild cognitive impairment using an entorhinal cortex-based test of virtual reality navigation. Brain 142, 1751–1766. doi:10.1093/brain/awz116
Jang, S., Choi, S.-W., Son, S. J., Oh, J., Ha, J., Kim, W. J., et al. (2023). Virtual reality-based monitoring test for MCI: a multicenter feasibility study. Front. Psychiatry 13, 1057513. doi:10.3389/fpsyt.2022.1057513
Jung, T., Moorhouse, N., Shi, X., and Amin, M. F. (2020). A virtual realityâ-supported intervention for pulmonary rehabilitation of patients with chronic obstructive pulmonary disease: mixed methods study. J. Med. Internet Res. 22, e14178. doi:10.2196/14178
Kaplan, A. M., and Haenlein, M. (2009). The fairyland of Second Life: virtual social worlds and how to use them. Bus. Horizons 52, 563–572. doi:10.1016/j.bushor.2009.07.002
Kennedy, R. S., Lane, N. E., Berbaum, K. S., and Lilienthal, M. G. (1993). Simulator sickness questionnaire: an enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 3, 203–220. doi:10.1207/s15327108ijap0303_3
Kim, E., Han, J., Choi, H., Prie, Y., Vigier, T., Bulteau, S., et al. (2021). Examining the academic Trends in neuropsychological Tests for executive functions using virtual reality: systematic literature review. JMIR Serious Games 9, e30249. doi:10.2196/30249
Kourtesis, P., Collina, S., Doumas, L. A. A., and MacPherson, S. E. (2021). Validation of the virtual reality everyday assessment lab (VR-EAL): an immersive virtual reality neuropsychological battery with enhanced ecological validity. J. Int. Neuropsychological Soc. 27, 181–196. doi:10.1017/S1355617720000764
Krikorian, R., Bartok, J., and Gay, N. (1994). Tower of london procedure: a standard method and developmental data. J. Clin. Exp. Neuropsychology 16, 840–850. doi:10.1080/01688639408402697
Lee, C. W. (2022). Application of metaverse service to healthcare industry: a strategic perspective. Int. J. Environ. Res. Public Health 19, 13038. doi:10.3390/ijerph192013038
Levy, F., Leboucher, P., Rautureau, G., and Jouvent, R. (2016). E-virtual reality exposure therapy in acrophobia: a pilot study. J. Telemedicine Telecare 22, 215–220. doi:10.1177/1357633X15598243
Liu, Z., Ren, L., Xiao, C., Zhang, K., and Demian, P. (2022). Virtual reality aided therapy towards health 4.0: a two-decade bibliometric analysis. Int. J. Environ. Res. Public Health 19, 1525. doi:10.3390/ijerph19031525
Maddox, T., Sparks, C., Oldstone, L., Maddox, R., Ffrench, K., Garcia, H., et al. (2023). Durable chronic low back pain reductions up to 24 months after treatment for an accessible, 8-week, in-home behavioral skillsâ-based virtual reality program: a randomized controlled trial. Pain Med. 24, 1200–1203. doi:10.1093/pm/pnad070
Maddox, T., Sparks, C. Y., Oldstone, L., Chibbaro, M., Sackman, J., Judge, E., et al. (2024). Perspective: the promise of virtual reality as an immersive therapeutic. J. Med. Ext. Real. 1, 13–20. doi:10.1089/jmxr.2023.0003
Makransky, G., Lilleholt, L., and Aaby, A. (2017). Development and validation of the Multimodal Presence Scale for virtual reality environments: a confirmatory factor analysis and item response theory approach. Comput. Hum. Behav. 72, 276–285. doi:10.1016/j.chb.2017.02.066
Mao, R. Q., Lan, L., Kay, J., Lohre, R., Ayeni, O. R., Goel, D. P., et al. (2021). Immersive virtual reality for surgical training: a systematic review. J. Surg. Res. 268, 40–58. doi:10.1016/j.jss.2021.06.045
Massetti, M., and Chiariello, G. A. (2023). The metaverse in medicine. Eur. Heart J. Suppl. J. Eur. Soc. Cardiol. 25, B104–B107. doi:10.1093/eurheartjsupp/suad083
Matamala-Gomez, M., Donegan, T., Bottiroli, S., Sandrini, G., Sanchez-Vives, M. V., and Tassorelli, C. (2019). Immersive virtual reality and virtual embodiment for pain relief. Front. Hum. Neurosci. 13, 279. doi:10.3389/fnhum.2019.00279
Mendez-Encinas, D., Sujar, A., Bayona, S., and Delgado-Gomez, D. (2023). Attention and impulsivity assessment using virtual reality games. Sci. Rep. 13, 13689. doi:10.1038/s41598-023-40455-4
Navas-Medrano, S., Soler-Dominguez, J. L., and Pons, P. (2023). Mixed Reality for a collective and adaptive mental health metaverse. Front. psychiatry 14, 1272783. doi:10.3389/fpsyt.2023.1272783
Orr, E., Arbel, T., Levy, M., Sela, Y., Weissberger, O., Liran, O., et al. (2023). Virtual reality in the management of patients with low back and neck pain: a retrospective analysis of 82 people treated solely in the metaverse. Archives Physiother. 13, 11. doi:10.1186/s40945-023-00163-8
Pagé, I., Roos, M., Collin, O., Lynch, S. D., Lamontagne, M.-E., Massé-Alarie, H., et al. (2023). Utaut2-based questionnaire: cross-cultural adaptation to canadian French. Disabil. Rehabilitation 45, 709–716. doi:10.1080/09638288.2022.2037746
Pagliari, C., Di Tella, S., Jonsdottir, J., Mendozzi, L., Rovaris, M., De Icco, R., et al. (2021). Effects of home-based virtual reality telerehabilitation system in people with multiple sclerosis: a randomized controlled trial. J. Telemedicine Telecare 30, 344–355doi. doi:10.1177/1357633X211054839
Papaioannou, T., Voinescu, A., Petrini, K., and Stanton Fraser, D. (2022). Efficacy and moderators of virtual reality for cognitive training in people with dementia and mild cognitive impairment: a systematic review and meta-analysis. J. Alzheimer’s Dis. 88, 1341–1370. doi:10.3233/JAD-210672
Park, S.-M., and Kim, Y.-G. (2022). A metaverse: taxonomy, components, applications, and open challenges. IEEE Access 10, 4209–4251. doi:10.1109/ACCESS.2021.3140175
Parsons, T. D. (2012). “Virtual simulations and the second life metaverse: paradigm shift in neuropsychological assessment,” in Virtual worlds and Metaverse platforms: new communication and identity paradigms (IGI Global), 234–250. doi:10.4018/978-1-60960-854-5.ch016
Parsons, T. D. (2015). Virtual reality for enhanced ecological validity and experimental control in the clinical, affective and social neurosciences. Front. Hum. Neurosci. 9, 660. doi:10.3389/fnhum.2015.00660
Parsons, T. D., Carlew, A. R., Magtoto, J., and Stonecipher, K. (2017). The potential of function-led virtual environments for ecologically valid measures of executive function in experimental and clinical neuropsychology. Neuropsychol. Rehabil. 27, 777–807. doi:10.1080/09602011.2015.1109524
Pedram, S., Palmisano, S., Perez, P., Mursic, R., and Farrelly, M. (2020). Examining the potential of virtual reality to deliver remote rehabilitation. Comput. Hum. Behav. 105, 106223. doi:10.1016/j.chb.2019.106223
Peres, S. C., Pham, T., and Phillips, R. (2013). Validation of the system usability scale (SUS): SUS in the wild. Proc. Hum. Factors Ergonomics Soc. Annu. Meet. 57, 192–196. doi:10.1177/1541931213571043
Perez-Marcos, D., Solazzi, M., Steptoe, W., Oyekoya, W., Frisoli, A., Weyrich, T., et al. (2012). A fully immersive set-up for remote interaction and neurorehabilitation based on virtual body ownership. Front. Neurology 3, 110. doi:10.3389/fneur.2012.00110
Piron, L., Turolla, A., Tonin, P., Piccione, F., Lain, L., and Dam, M. (2008). Satisfaction with care in post-stroke patients undergoing a telerehabilitation programme at home. J. Telemedicine Telecare 14, 257–260. doi:10.1258/jtt.2008.080304
Ribeiro, N., Vigier, T., Han, J., Kwon, G. H., Choi, H., Bulteau, S., et al. (2024). Three virtual reality environments for the assessment of executive functioning using performance scores and kinematics: an embodied and ecological approach to cognition. Cyberpsychology Behav. Soc. Netw. 27, 127–134. doi:10.1089/cyber.2023.0314
Ribeiro, N., Vigier, T., and Prié, Y. (2021). Tracking motor activity in Virtual Reality to reveal cognitive functioning: a preliminary study. Int. J. Virtual Real. 21, 30–46. doi:10.20870/IJVR.2021.21.1.4782
Sampaio, M., Navarro Haro, M. V., De Sousa, B., Vieira Melo, W., and Hoffman, H. G. (2021). Therapists make the switch to telepsychology to safely continue treating their patients during the COVID-19 pandemic. Virtual reality telepsychology may Be next. Front. Virtual Real. 1, 576421. doi:10.3389/frvir.2020.576421
Skalidis, I., Muller, O., and Fournier, S. (2023). CardioVerse: the cardiovascular medicine in the era of Metaverse. Trends Cardiovasc. Med. 33, 471–476. doi:10.1016/j.tcm.2022.05.004
Skalidis, I., Muller, O., Fournier, S., Antiochos, P., Kaldasch, M., Idrissi, B. E., et al. (2022). Feasibility of using the metaverse as telecardiology platform: remote follow-up of a patient with vasospastic angina. Can. J. Cardiol. 38, 1768–1769. doi:10.1016/j.cjca.2022.07.020
Sobota, B., Gvuscova, J., and Mattova, M. (2022). “Therapist-patient interaction in virtual reality at the level of the upper limbs,” in 2022 20th international Conference on Emerging elearning Technologies and applications (ICETA), 584–588. doi:10.1109/ICETA57911.2022.9974677
Sobral, M., and Pestana, M. H. (2020). Virtual reality and dementia: a bibliometric analysis. Eur. J. Psychiatry 34, 120–131. doi:10.1016/j.ejpsy.2020.04.004
Spiegel, B. M., Rizzo, A., Persky, S., Liran, O., Wiederhold, B., Woods, S., et al. (2024). What is medical extended reality? A taxonomy defining the current breadth and depth of an evolving field. J. Med. Ext. Real. 1, 4–12. doi:10.1089/jmxr.2023.0012
Steed, A. (2024). Three technical challenges of scaling from social virtual reality to metaverse(s): interoperability, awareness and accessibility. Front. Virtual Real. 5. doi:10.3389/frvir.2024.1432907
Tamplin, J., Loveridge, B., Clarke, K., Li, Y., and J Berlowitz, D. (2020). Development and feasibility testing of an online virtual reality platform for delivering therapeutic group singing interventions for people living with spinal cord injury. J. Telemedicine Telecare 26, 365–375. doi:10.1177/1357633X19828463
Thøgersen, M., Andoh, J., Milde, C., Graven-Nielsen, T., Flor, H., and Petrini, L. (2020). Individualized augmented reality training reduces phantom pain and cortical reorganization in amputees: a proof of concept study. J. Pain 21, 1257–1269. doi:10.1016/j.jpain.2020.06.002
Venkatesh, V., Thong, J. Y. L., and Xu, X. (2012). Consumer acceptance and use of information technology: extending the unified theory of acceptance and use of technology. MIS Q. 36, 157–178. doi:10.2307/41410412
Wong, M. Y. Z., Gunasekeran, D. V., Nusinovici, S., Sabanayagam, C., Yeo, K. K., Cheng, C.-Y., et al. (2021). Telehealth demand trends during the COVID-19 pandemic in the top 50 most affected countries: infodemiological evaluation. JMIR Public Health Surveillance 7, e24445. doi:10.2196/24445
Worlikar, H., Coleman, S., Kelly, J., O’Connor, S., Murray, A., McVeigh, T., et al. (2023). Mixed reality platforms in telehealth delivery: scoping review. JMIR Biomed. Eng. 8, e42709. doi:10.2196/42709
Keywords: cognitive testing, dashboards, immersive teleclinic, metaverse, neuro-psychology, teleconsultation, telemedicine, virtual reality
Citation: Prié Y, Vigier T, Acier D, Bonneville H, Georges M, Thévenet S and Bulteau S (2025) Towards teleconsultations in the metaverse: design and preliminary study of an immersive teleclinic for neuro-psychological assessment. Front. Virtual Real. 6:1545569. doi: 10.3389/frvir.2025.1545569
Received: 15 December 2024; Accepted: 16 June 2025;
Published: 01 July 2025.
Edited by:
Mel Slater, University of Barcelona, SpainReviewed by:
Marta Matamala-Gomez, University of Barcelona, SpainTony Donegan, August Pi i Sunyer Biomedical Research Institute (IDIBAPS), Spain
Copyright © 2025 Prié, Vigier, Acier, Bonneville, Georges, Thévenet and Bulteau. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yannick Prié, eWFubmljay5wcmllQHVuaXYtbmFudGVzLmZy