 Parya Khandan
Parya Khandan Benjamin Ennemoser
Benjamin Ennemoser Ryan D. Foster
Ryan D. Foster Logan Dubose3
Logan Dubose3 Zhipeng Lu
Zhipeng Lu- 1Department of Architecture, Texas A&M University, College Station, TX, United States
- 2Department of Counseling, Tarleton State University, Stephenville, TX, United States
- 3Olera Inc., Bryan, TX, United States
Death anxiety (DA) and stress pose significant psychological challenges that negatively impact health and wellbeing. Exposure therapy—a behavioral approach that reduces fear by repeatedly and safely exposing individuals to feared stimuli—has demonstrated effectiveness in treating anxiety. However, traditional exposure methods are limited in addressing DA, as individuals cannot authentically experience death. This study examined the efficacy of an immersive virtual reality (VR) near-death experience (NDE) simulation as an alternative to an actual NDE for reducing DA and stress. Sixty-one adults engaged in a first-person VR NDE experience, randomized to either a narrated or non-narrated version. Pre- and post-intervention questionnaire comparisons revealed significant reductions in both DA and stress, with no significant differences between the two versions. These findings contribute to the growing evidence on how immersive VR can modulate emotional and cognitive responses related to mortality, supporting its potential as a scalable tool for psychological interventions and fostering behavioral changes such as reduced avoidance of death-related thoughts, greater resilience, and shifts toward more positive, value-driven living.
1 Introduction
Stress is a physiological and psychological response to perceived threats, affecting cognition, behavior, and overall wellbeing (Yaribeygi et al., 2017). One significant psychological contributor to stress is death anxiety (DA). According to Terror Management Theory, DA is a distressing emotional response to mortality awareness (Eggen et al., 2020) that can trigger a wide range of reactions, from pervasive fear to emotional regulation (Arndt et al., 2005). Stress and DA reinforce each other, as heightened DA increases stress, whereas prolonged stress exacerbates DA. DA is also associated with several mental health conditions, including panic disorder, illness anxiety, obsessive-compulsive disorder, and phobias (Menzies et al., 2018). Research indicates that DA peaks during young adulthood, with the highest levels occurring in the 20s, followed by a significant decline until a second peak in later life (Russac et al., 2007). This pattern highlights the need for effective interventions targeting this age group. Exposure therapy, which gradually and safely exposes individuals to feared stimuli, is widely regarded as the most effective treatment for DA; however, alternative approaches such as relaxation training and logotherapy (help finding meaning in life), have shown mixed results (Menzies, 2018). As direct exposure to death is not a feasible option, innovative interventions should extend beyond traditional exposure methods to effectively address DA.
1.1 Near-death experiences and related psychological benefits
Near-death experiences (NDEs) are profound psychological events with transcendental and mystical elements, typically occurring in individuals close to death or in situations of intense physical or emotional danger. They are not limited to the brief transition from clinical to brain death, but can arise during real or perceived life-threatening conditions, and sometimes in non-life-threatening states (Greyson, 2023; Romand and Ehret, 2023). NDEs are associated with reduced DA and a positive shift in life attitudes (Pehlivanova et al., 2022) and may improve psychological and spiritual wellbeing (Blomstrom et al., 2020). At the same time, responses are not uniform across individuals. Multiple studies consistently show that females report higher death anxiety than males, with large-scale research confirming sex-based differences often tied to sociocultural roles or healthcare exposure (Belak and Goh, 2024). Indirect exposure to NDEs through books, media, or documentaries has been shown to influence life perspectives, while study participants reported greater self-acceptance, appreciation of life, and reduced fear of death, a minority describe adverse effects, including increased DA (Ghasemiannejad Jahromi et al., 2023). Interventions incorporating NDE elements, such as guided imagery and relaxation techniques, have shown promise in reducing DA among terminal patients (de Araújo Elias et al., 2006). However, existing NDE interventions rely on secondhand information and imagination, which may limit their effectiveness. These methods fail to replicate the emotional intensity of firsthand NDEs, prompting the search for novel approaches such as VR to provide a more immersive and realistic experience. Additionally, given that some individuals may experience heightened anxiety rather than relief, these approaches should be applied cautiously and evaluated carefully for their broader psychological impact.
1.2 VR as a therapeutic tool
VR creates immersive, interactive environments and has been widely applied in education and healthcare, especially in mental and behavioral health (Hamad and Jia, 2022). Its ability to mimic real-world scenarios makes it effective for anxiety treatment (Meyerbröker and Morina, 2021). Research has examined VR’s role in managing anxiety and stress-related conditions. An earlier scoping review by Donnelly et al. (2021) confirmed the effectiveness of VR for PTSD, phobias, and social anxiety by offering ecologically valid environments. Fereidooni et al. (2024) found that VR interventions reduce anxiety, pain, and fatigue while enhancing mood and relaxation. Kukharuk et al. (2025)further demonstrated that VR therapy improves mood and reduces both anxiety and depression.
Given success in anxiety treatment, VR also holds promise for reducing DA and stress through controlled NDE simulations. A review by Blomstrom et al. (2020) highlighted that VR-based NDEs can complement traditional interventions by providing a safe, controlled, and experiential means of confronting existential fears and reframing attitudes toward death. Two additional experimental studies offer encouraging evidence. Bourdin et al. (2017) showed that inducing out-of-body experiences in VR reduced fear of death, while Barberia et al. (2018) demonstrated that a life-cycle VR simulation culminating in virtual death fostered existential awareness and greater concern for global issues. Despite limitations (e.g., small, homogeneous samples and the use of simplified or non-human avatars), these studies suggest that VR-based NDE interventions represent a promising and uniquely experiential approach to addressing DA and warrant further empirical investigation.
Additional research also underscores the role of narrative. A study shows that immersive VR storytelling can reproduce NDE-like states and foster perspective shifts (Panaita, 2021). A systematic review reports that guided or narrative-based VR is more effective in reducing stress and anxiety than passive content (Gaina et al., 2024). These findings suggest that narration may strengthen the psychological impact of VR-based NDE simulations.
Nevertheless, ethical cautions are essential due to the sensitive, death-related topic. Evidence indicates that, although most individuals benefit, a small portion of people may experience adverse outcomes such as heightened death anxiety or, in rare cases, increased suicidal ideation (King, 2025). These risks highlight the importance of careful screening, supportive monitoring, and further research before widespread clinical application.
This study aims to examine the effects of a VR NDE simulation as an intervention for reducing DA and stress. The research team plans to first test the simulation on healthy individuals before applying it to physically and/or mentally frail patients. Unlike traditional NDE interventions that rely on secondhand narratives, VR provides an immersive, first-person experience, allowing participants to engage with the concept of death in a controlled environment. Additionally, this study evaluates the intervention’s usability and acceptability, identifying potential challenges in its implementation. By integrating emerging immersive technologies with psychological interventions, this research contributes to the growing exploration of experiential approaches to mental health. This study tests the following hypotheses:
Hypothesis 1: Participants’ DA and perceived stress are reduced after the VR NDE simulation intervention.
Hypothesis 2: Including a narration in the VR NDE simulation has different effects on DA and perceived stress reduction compared to simulations without narration.
Hypothesis 3: The VR NDE simulation invention has different effects on male and female participants in terms of DA and perceived stress reduction.
2 Methods
2.1 Research design
This study employed a pre-post quasi-experimental design to assess the effects of a VR NDE simulation on DA and stress in young adults. Participants completed self-report surveys at least 1 day before and immediately after the completion of the VR session to measure changes in DA and perceived stress. Additionally, feedback on the simulation’s usability and acceptability was gathered through the post-intervention survey. The study protocol was reviewed and approved by the first author’s university IRB.
2.2 VR NDE simulation
The VR NDE simulation was initially developed by a team led by the International Association for Near-Death Studies, which authorized its use in this study. This 11-min, 360-degree, video-based, non-interactive simulation allows users to look around in all directions, accommodating full head motion and a wide field of view. By leveraging VR and its 360-degree capability, the experience is more immersive than conventional video screens. The video begins with a man driving a car and getting into an accident. While in a coma, he is placed on a stretcher and rushed to medical care. He then witnesses scenes commonly reported in NDEs, including out-of-body experiences, tunnels of light, serene landscapes, and encounters with friends and family (Figure 1). The simulation concludes with the man waking up and returning to life. The original version includes a narration of his thoughts and feelings, which the research team removed to create a non-narrated version for the study. This VR NDE simulation was chosen because it was developed by a team of experienced NDE experts and clinicians, and it represents the best available immersive simulation containing all the components for the current study.

Figure 1. Top left: Out-of-Body Experience, top right: Lights and Dark Tunnel, bottom left: Peaceful Landscape, bottom right: Encountering Friends and Family.
2.3 Measurement instruments
This study used two questionnaires: the pre-intervention and the post-intervention questionnaires. The research team evaluated multiple validated measurement instruments for stress, death anxiety, and simulation acceptability and usability, and included those in the questionnaires based on following criteria: 1 having been rigorously tested for validity and reliability, 2 suitable for pre-and post-intervention comparisons, and 3 appropriate for testing this study’ hypotheses. The pre-intervention questionnaire included demographics and measures from the Perceived Stress Questionnaire (PSQ) (30 items, 4-point scale) (Levenstein et al., 1993) and the Death Anxiety Scale (DAS) (15 true/false items) (Templer, 1970). The post-intervention reassessed DA and stress using the same measures. PSQ scores were calculated by subtracting 30 from the raw score and dividing by 90 to yield an index from 0 to 1. Additional items from the Simulator Sickness Questionnaire (SSQ) (Walter et al., 2019) evaluated usability and acceptability, along with five open-ended questions about participants’ experiences.
2.4 Participants
This study employed convenience sampling, recruiting participants from the first author’s university. Eligible participants were 18 years or older; able to understand, read, and write in English; and free of self-reported mental-health conditions. A total of 61 participants were recruited. Three-fourths (n = 46) were randomly assigned to the VR NDE version with narration by a male voice, whereas the remaining (n = 15) experienced the non-narrated version.
2.5 Data collection
The study was conducted in a quiet, 120-square-foot room at the first author’s university. Sessions were held individually using an Oculus Quest 2 headset, with a researcher present for safety and guidance. Participants completed the pre-intervention questionnaire before the session. Upon arrival, they were seated in a swivel chair and given brief instructions on using the headset and controllers. After confirming that the pre-intervention questionnaire had been completed, the researcher provided an eye-cover mask for hygiene and assisted the participant in putting on the headset. Following the VR session, the researcher removed the headset, sanitized the equipment, and administered the post-intervention questionnaire. Upon completion, participants received a gift card as an incentive.
2.6 Data analysis
Quantitative data was cleaned and analyzed using SPSS Version 30. Descriptive statistics were computed for demographics and VR usability responses. Normality was assessed using the Shapiro-Wilk test to determine appropriate statistical tests. For normally distributed data, paired sample t-tests and independent t-tests were conducted, with Cohen’s d reported for effect sizes. For non-normally distributed data, Mann-Whitney U tests were used, with rank-based statistics (mean rank, Z-score, and rank-biserial correlation) reported. Paired-sample t-tests compared pre- and post-intervention scores on DA and perceived stress, whereas independent t-tests examined the effects of gender and intervention type on stress and DA reduction. For gender-based analyses, two participants who did not identify as male or female were excluded, resulting in a final sample of 58 participants (male = 24, female = 34) for these tests. Acceptability was assessed through post-intervention usability feedback, including mean ratings of discomfort, concentration difficulty, and fatigue. Responses to open-ended questions were analyzed via the content analysis method to identify patterns and common themes.
3 Results
3.1 Participant characteristics
Among the 61 participants, one was excluded from the analysis for not completing the pre-intervention questionnaire. The majority of participants were female (56.7%) and aged 18–24 (65%). Most were undergraduates (55%), with 16.7% in master’s and 23.3% in doctoral programs. The largest ethnic groups were White (38.3%) and Asian (38.3%). The most common religious affiliations were Christianity (36.7%) and Islam (26.7%).
3.2 Descriptive statistics of DA and perceived stress
3.2.1 Death anxiety
Before the intervention, the mean DA score was 8.57 (range: 1–15), with a standard deviation of 3.371. After the intervention, the mean DA score was 7.00 (range: 1–13), with a standard deviation of 3.298. While the overall trend indicates a reduction, 16 participants (26.7%) experienced an increase in DA following the intervention (Table 1).

Table 1. Descriptive statistics of DA and perceived stress.
3.2.2 Perceived stress
Before the intervention, the mean score was 0.469 (range: 0.22–0.74), with a standard deviation of 0.122. After the intervention, the mean score was 0.396 (range: 0.03–0.86), with a standard deviation of 0.191. Similarly, despite the overall decrease in stress, 21 participants (35%) reported higher perceived stress after the intervention (Table 1).
Hypothesis 1. Participants’ death anxiety and perceived stress are reduced after the VR NDE simulation intervention.
3.2.3 Death anxiety
A paired-sample t-test showed a significant reduction in DA (Δmean = 1.566, SD = 3.421, p < 0.001) after the intervention. The effect size (Cohen’s d = 0.458) suggests a small-to-moderate impact (Table 2).

Table 2. Effect of VR intervention on death anxiety and perceived stress.
3.2.4 Perceived stress
Similarly, the analysis revealed a significant decrease in stress levels (Δmean = 0.396, SD = 0.191, p = 0.002) from pre-to post-intervention. The effect size (Cohen’s d = 0.411) indicates a small-to-moderate impact, suggesting that although the intervention effectively reduced stress, the magnitude of change was modest (Table 2).
In summary, Hypothesis 1 (participants’ DA and perceived stress are reduced after the VR NDE simulation intervention) is supported by the results.
Hypothesis 2. Including a narration in the VR NDE simulation has different effects on death anxiety and perceived stress reduction compared to simulations without narration.
3.2.5 Death anxiety
A Mann-Whitney U test found no significant difference in DA reduction between the narration and non-narration versions (p = 0.870). The narrated version showed a slightly greater mean reduction (1.645) than the non-narrated version (1.333). The Z-score (−0.164) and effect size (r = −0.021, rank-biserial correlation) suggest that any observed differences were negligible and likely due to random variation (Table 3).
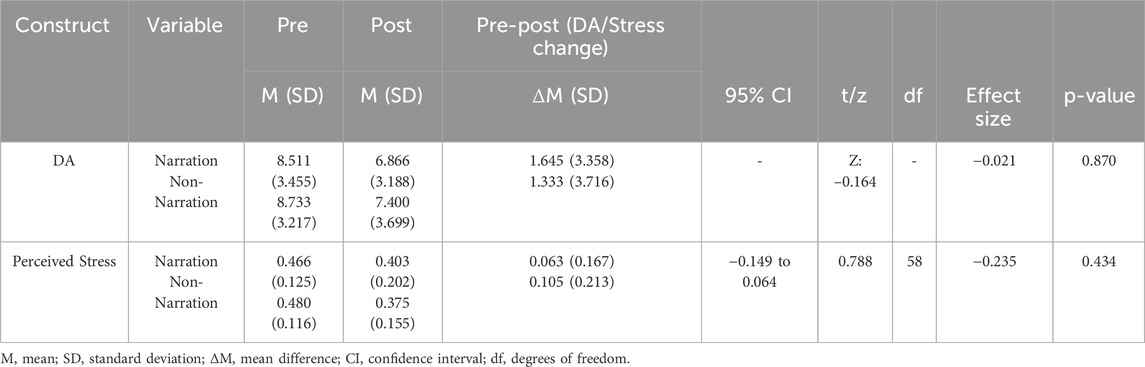
Table 3. Effect of intervention type on death anxiety reduction and stress reduction.
3.2.6 Perceived stress
An independent t-test found no significant difference in stress reduction between the two intervention versions (p > 0.05). Although the non-narrated group showed a slightly greater mean reduction (0.105) than the narrated group (0.0631), greater response variability in the non-narration group suggests that this difference was not meaningful. The effect size (Cohen’s d = −0.235) was small, confirming that both versions had a similar effect on reducing stress (Table 3).
Therefore, the results did not support Hypothesis 2 (including a narration in the VR NDE simulation has different effects on DA and perceived stress reduction compared to simulations without narration).
Hypothesis 3. The VR NDE simulation invention has different effects on male and female participants in terms of death anxiety and perceived stress reduction.
3.2.7 Death anxiety
An independent t-test found no significant difference in DA reduction between genders (p = 0.835). Male participants showed a slightly greater mean reduction (1.6667) than females (1.4706), but high standard deviations suggested considerable variability. The effect size (Cohen’s d = 0.056) was small, suggesting that gender differences did not play a significant role in DA reduction (Table 4).
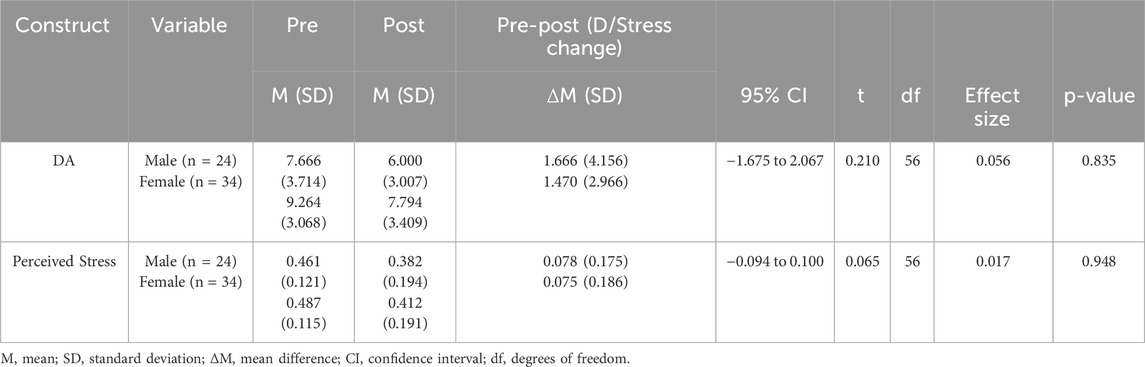
Table 4. Effect of gender on DA and stress reduction.
3.2.8 Perceived stress
An independent t-test (p = 0.948) found no significant difference in stress reduction between genders, indicating that gender did not impact the intervention’s effectiveness. The effect size (Cohen’s d = 0.017) was negligible, further confirming that observed differences were minimal (Table 4).
In summary, the results do not support Hypothesis 3 (the VR NDE simulation invention has different effects on male and female participants in terms of DA and perceived stress reduction).
3.3 The acceptability and usability results
Results from the SSQ indicate that the intervention was generally acceptable. The most frequently reported symptoms were only slight difficulty or problem with items such as concentrating (55%), focusing (50%), blurred vision (38.3%), eye strain (35%), general discomfort (26.7%), and fatigue (23.3%). No severe symptoms such as nausea or motion sickness were reported. Overall, these findings suggest that the VR NDE experience was both acceptable and usable, with only minor side effects that did not significantly hinder participant engagement.
3.4 Overall experiences and suggestions for improvement
All participants responded to the open-ended questions. Content analysis identified key patterns regarding the strengths of the VR NDE intervention:
- Relaxation Effects. Many participants described the experience as relaxing, meditative, and a peaceful escape from stress:
- Attitudes Toward Life and Death. Beyond relaxation, the intervention was engaging and thought-provoking, prompting reflection on life, death, and personal existence. Some participants reported that it helped them process their fear of death:
- Detachment from Daily Hassles. Some participants appreciated the detachment from daily concerns, allowing them to step back and reflect:
- Positive Perspectives of Life. Several participants noted a positive shift in their outlook, expressing both a desire to live meaningfully and gratitude for being alive:
- Although many participants commented positively on the visuals and music, opinions on the narration were mixed. Some preferred a more personalized approach:
Quote: “It was very relaxing, and I got to experience it during [the week of] my exams, which was a very stressful time. While using it, I felt very calm, like nothing else mattered.”
Quote: “It was eye-opening! I am afraid of dying, but I had never thought about what I might see near death. It was also relaxing and made me think about death differently. Thank you for that!”
Quote: “The scene [that most impressed me was] where they asked him to return to Earth, yet he did not want to. He was relieved from all the attachments, stress, and worries back on Earth, and he felt that place is where he belonged.”
Quote 1: “[It was] very relaxing. I wish I could try it more than once. Maybe every night before going to bed! I think the day would be more meaningful to me in this way! Appreciating every moment. Because I got to die last night and live again!”
Quote 2: “I found it interesting and strangely comforting. It reminded me that I need to live life more fully, and I appreciate that.”
Quote: “I would rather hear my voice and thoughts. Hearing someone else’s voice distracted me sometimes.”
Other suggested improvements included higher video resolution, enhanced visual quality of nature-based environments, and greater personalization for emotional alignment. Regarding the most and least favored components, participants preferred nature scenes, out-of-body floating experiences, life reflections, and family encounters, whereas the car accident and hospital settings were least favored. Most of the participants found the VR NDE intervention valuable, with relaxation and reflection as key benefits.
4 Discussion
This study examined the effectiveness of a VR NDE intervention in reducing DA and stress among adults. Results support the primary hypothesis, indicating significant reductions in the majority of the participants in both measures. Three key mechanisms likely explain these effects: 1 immersive exposure, altering self-perception, and reducing fear of mortality (Barberia et al., 2018); 2 relaxation response, lowering physiological stress markers (Mazgelytė et al., 2021); and 3 existential shifts similar to naturally occurring NDEs, fostering positive life changes (Rominger, 2009). These findings align with prior research on VR’s role in anxiety reduction (Barberia et al., 2018), offering a scalable alternative to traditional exposure therapy for addressing DA in non-clinical populations. Additionally, VR enhances emotional regulation and perspective-taking, which may contribute to reductions in distress (Colombo et al., 2021). However, a non-negligible proportion of participants experienced increases in DA (26.7%) and stress (35%) after the intervention, indicating that precautions should be taken when implementing this NDE simulation. Beyond these overall benefits, an unresolved question is whether simulating void, hellish, or inverse NDEs in VR could yield comparable psychological outcomes. Future research should systematically investigate whether these less-positive simulations have the potential to alleviate death anxiety or, conversely, pose heightened psychological risks.
Notably, the DA scale defines 7.5 as the average DA level, with 4.5–7.0 considered normal (Templer, 1970). Participants’ pre-intervention DA mean was 8.5, slightly exceeding the normal range. This aligns with previous research showing that DA peaks in adulthood and significantly declines afterward (Russac et al., 2007), though it may rise again in later life due to declining health and proximity to mortality (Menzies et al., 2018). Given the sample’s composition of young adults, their initially slightly high DA scores were expected. After the intervention, most of their DA means dropped to 7.0, indicating a successful reduction to the normal level.
The hypotheses regarding whether different genders and intervention types (with narration versus without narration) influence the intervention effectiveness were not supported. First, the small sample size in each subgroup may have limited statistical power to detect significant differences. Second, the insignificant results may suggest that visual content plays a more dominant role in reducing DA and stress compared to the audio component. Third, it may also partly be due to the misalignment of gender, especially female, with the male voice narration in VR. Some female participants reported that the male voice narration decreased the sense of immersion with the NDE VR. This concurs with Greyson (2010) argument that NDEs are highly individualized experiences shaped by personal, cultural, and situational factors. Therefore, future development of the VR NDE prototype can integrate gender-matched narration to enhance immersion.
The sample composition (university students) may have influenced the results. Although this group experiences high stress from academic pressures, they generally have a relatively lower baseline DA than terminally ill patients. Therefore, the intervention may yield stronger effects in populations facing physical, psychological, or emotional challenges. Despite minor usability issues, most of the participants reported high acceptability and positive emotional impact. No complaints were found about NDE-related content or scenes, likely due to this young, healthy population. However, self-selection bias may have played a role, as individuals uncomfortable with NDE topics or VR may have opted out of participation.
4.1 Limitations
This study has several limitations. First, it was a quasi-experimental design without a control group. Second, pre- and post-intervention measures captured only short-term effects, limiting insights into long-term outcomes. In particular, DA and stress were measured immediately after the simulation; because naturally occurring NDEs often require a period of psychological integration, immediate assessment may not fully reflect delayed or evolving effects. Third, self-reported stress and DA measures may be subject to bias. Fourth, the small sample size, constrained by time and budget, may have affected statistical power. Finally, usability concerns, including minor problems such as eye strain (35%), fatigue (23.3%), and difficulty concentrating (55%), highlight the need for improved VR design.
4.2 Future directions
Future research should assess the effectiveness of VR NDE intervention in clinical populations, including frail elderly and terminally ill patients, using a randomized controlled trial with a larger sample size. Longitudinal studies are needed to evaluate long-term effects and the persistence of benefits. Enhancing visual quality, personalization, and interactivity in the VR NDE prototype is crucial for enhancing immersion. Additionally, incorporating objective measures like skin conductance, heart rate variability, and eye-tracking may help reduce measurement errors and bias. Finally, examining cultural and religious differences can broaden the applicability of VR NDE intervention across diverse populations.
5 Conclusion
This study is among the first to empirically assess VR NDE simulations as an intervention for reducing DA and stress. Findings demonstrate that the intervention significantly reduced DA and stress for most of the participants, with high participant acceptance supporting its feasibility as a psychological intervention. These results contribute to understanding how immersive VR can modulate emotional and cognitive responses, advancing its role within the growing field of behavioral and mental health applications of VR. Advancing realism, personalization, and long-term evaluations will be key to optimizing therapeutic benefits. With continued technological advancements, VR NDE simulations could become a transformative tool for managing DA, fostering resilience, and improving mental health. At the same time, their application must remain ethically guided, with safeguards in place to protect against potential adverse effects.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Review Board (IRB), Human Research Protection Program, Texas A&M University, College Station, Texas, United States. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PK: Investigation, Writing – review and editing, Methodology, Formal Analysis, Writing – original draft, Conceptualization, Project administration. BE: Conceptualization, Methodology, Investigation, Writing – review and editing, Software. RF: Conceptualization, Writing – review and editing, Methodology. LD: Writing – review and editing, Conceptualization. ZL: Writing – original draft, Formal Analysis, Project administration, Supervision, Conceptualization, Methodology, Investigation, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project was supported by the Julie and Craig Beale Endowed Professorship for Health Facilities Design, College of Architecture, Texas A&M University.
Acknowledgments
The authors would like to thank the International Association for Near-Death Studies for authorizing the research team to use the near-death experience virtual reality prototype in this study.
Conflict of interest
Author LD was employed by Olera Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Arndt, J., Routledge, C., Cox, C. R., and Goldenberg, J. L. (2005). The worm at the core: a terror management perspective on the roots of psychological dysfunction. Appl. Prev. Psychol. 11 (3), 191–213. doi:10.1016/j.appsy.2005.07.002
Barberia, I., Oliva, R., Bourdin, P., and Slater, M. (2018). Virtual mortality and near-death experience after a prolonged exposure in a shared virtual reality may lead to positive life-attitude changes. PLOS ONE 13 (11), e0203358. doi:10.1371/journal.pone.0203358
Belak, R. M., and Goh, K. H. (2024). Death anxiety and religiosity in a multicultural sample: a pilot study examining curvilinearity, age and gender in Singapore. Front. Psychol. 15, 1398620. doi:10.3389/fpsyg.2024.1398620
Blomstrom, M., Burns, A., Larriviere, D., and Penberthy, J. K. (2020). Addressing fear of death and dying: traditional and innovative interventions. Mortality 27 (1), 18–37. doi:10.1080/13576275.2020.1810649
Bourdin, P., Barberia, I., Oliva, R., and Slater, M. (2017). A virtual out-of-body experience reduces fear of death. PLOS ONE 12 (1), e0169343. doi:10.1371/journal.pone.0169343
Colombo, D., Díaz-García, A., Fernandez-Álvarez, J., and Botella, C. (2021). Virtual reality for the enhancement of emotion regulation. Clin. Psychol. and Psychotherapy 28 (3), 519–537. doi:10.1002/cpp.2618
de Araújo Elias, A. C., Giglio, J. S., de Mattos Pimenta, C. A., and El-Dash, L. G. (2006). Therapeutical intervention, relaxation, mental images, and spirituality (RIME) for spiritual pain in terminal patients. A training program. Sci. World J. 6 (1), 2158–2169. doi:10.1100/tsw.2006.345
Donnelly, M. R., Reinberg, R., Ito, K. L., Saldana, D., Neureither, M., Schmiesing, A., et al. (2021). Virtual reality for the treatment of anxiety disorders: a scoping review. Am. J. Occup. Ther. 75 (6), 7506205040. doi:10.5014/ajot.2021.046169
Eggen, A. C., Reyners, A. K. L., Shen, G., Bosma, I., Jalving, M., Leighl, N. B., et al. (2020). Death anxiety in patients with metastatic non-small cell lung cancer with and without brain metastases. J. Pain Symptom Manag. 60 (2), 422–429.e1. doi:10.1016/j.jpainsymman.2020.02.023
Fereidooni, M., Toni, E., Toni, E., and Ayatollahi, H. (2024). Application of virtual reality for supportive care in cancer patients: a systematic review. Support. Care Cancer 32 (9), 570. doi:10.1007/s00520-024-08763-1
Gaina, A.-M., Stefanescu, C., Szalontay, A.-S., Gaina, M.-A., Poroch, V., Mosoiu, D. V., et al. (2024). A systematic review of virtual reality’s impact on anxiety during palliative care. Healthcare 12 (24), 2517. doi:10.3390/healthcare12242517
Ghasemiannejad Jahromi, A., Qaderi Bagajan, K., Jamshidi, B., and Zakiei, A. (2023). Effects of knowledge of near-death experiences (NDEs) on life changes in people without NDEs. OMEGA - J. Death Dying, 00302228231191549. doi:10.1177/00302228231191549
Greyson, B. (2010). Near-death experiences. Corsini Encycl. Psychol., 1–2. doi:10.1002/9780470479216.corpsy0589
Greyson, B. (2023). Researchers' and Experiencers' descriptions of near-death experiences: in search of a conceptual model. J. Near-Death Stud. 41 (3), 169–201. doi:10.17514/jnds-2023-41-3-p169-201
Hamad, A., and Jia, B. (2022). How virtual reality technology has changed our lives: an overview of the current and potential applications and limitations. Int. J. Environ. Res. Public Health 19 (18), 11278. doi:10.3390/ijerph191811278
King, R. A. (2025). The near-death experience and suicidal ideation. OMEGA - J. Death Dying 91 (4), 1736–1756. doi:10.1177/00302228231162175
Kukharuk, O., Tkalich, K., Kamash, N., and Georgiou, O. (2025). Effectiveness of immersive VR therapy in reducing stress-associated symptoms in Ukraine. Eur. J. Psychotraumatology 16 (1), 2488097. doi:10.1080/20008066.2025.2488097
Levenstein, S., Prantera, C., Varvo, V., Scribano, M. L., Berto, E., Luzi, C., et al. (1993). Development of the perceived stress questionnaire: a new tool for psychosomatic research. J. Psychosomatic Res. 37 (1), 19–32. doi:10.1016/0022-3999(93)90120-5
Mazgelytė, E., Rekienė, V., Dereškevičiūtė, E., Petrėnas, T., Songailienė, J., Utkus, A., et al. (2021). Effects of virtual reality-based relaxation techniques on psychological, physiological, and biochemical stress indicators. Healthcare 9 (12), 1729. doi:10.3390/healthcare9121729
Menzies, R. E. (2018). “Cognitive and behavioural procedures for the treatment of death anxiety,” in Curing the dread of death: theory, research and practice. Editors R. E. Menzies, R. G. Menzies, Iverach, and L. Samford Valley (Australian Academic Press), 167–184.
Menzies, R. E., Zuccala, M., Sharpe, L., and Dar-Nimrod, I. (2018). The effects of psychosocial interventions on death anxiety: a meta-analysis and systematic review of randomised controlled trials. J. Anxiety Disord. 59, 64–73. doi:10.1016/j.janxdis.2018.09.004
Meyerbröker, K., and Morina, N. (2021). The use of virtual reality in assessment and treatment of anxiety and related disorders. Clin. Psychol. and Psychotherapy 28 (3), 466–476. doi:10.1002/cpp.2623
Panaita, E. (2021). Atypical reality: exploring the narrative potentials of an immersive environment. Link 2021. doi:10.24135/link2021.v2i1.169
Pehlivanova, M., Carroll, A., and Greyson, B. (2022). Which near-death experience features are associated with reduced fear of death? Mortality 28 (3), 493–509. doi:10.1080/13576275.2021.2017868
Romand, R., and Ehret, G. (2023). Neuro-functional modeling of near-death experiences in contexts of altered states of consciousness. Front. Psychol. 13, 846159. doi:10.3389/fpsyg.2022.846159
Rominger, R. (2009). Exploring the integration of near-death experience aftereffects: summary of findings. J. Near-Death Stud. 28, 5–30. doi:10.17514/JNDS-2009-28-1-p3-34
Russac, R. J., Gatliff, C., Reece, M., and Spottswood, D. (2007). Death anxiety across the adult years: an examination of age and gender effects. Death Stud. 31 (6), 549–561. doi:10.1080/07481180701356936
Templer, D. I. (1970). The construction and validation of a death anxiety scale. J. General Psychol. 82 (2), 165–177. doi:10.1080/00221309.1970.9920634
Walter, H., Li, R., Munafo, J., Curry, C., Peterson, N., and Stoffregen, T. (2019). APAL coupling study 2019. Minneapolis, MN, United States: Retrieved from the Data Repository for the University of Minnesota. doi:10.13020/XAMG-CS69
Keywords: virtual reality, death anxiety, stress, near-death experience (NDE), psychological interventions, human behavior
Citation: Khandan P, Ennemoser B, Foster RD, Dubose L and Lu Z (2025) A virtual reality intervention to reduce death anxiety and stress in adults: examining the effect of a near-death experience simulation. Front. Virtual Real. 6:1644131. doi: 10.3389/frvir.2025.1644131
Received: 09 June 2025; Accepted: 17 September 2025;
Published: 29 September 2025.
Edited by:
James Harland, RMIT University, AustraliaReviewed by:
Ioannis Ladakis, Aristotle University of Thessaloniki, GreeceAzeem Kaleem, The University of Lahore Lahore School of Nursing, Pakistan
Copyright © 2025 Khandan, Ennemoser, Foster, Dubose and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhipeng Lu, bHV6aGlwZW5nQHRhbXUuZWR1