 Hossein Faridniya
Hossein Faridniya Reena George
Reena George- 1Sport Management, Farabi Campus, University of Tehran, Qom, Iran
- 2Industry Research Affiliate, Amity Business School, Amity University Dubai, Dubai, United Arab Emirates
- 3Amity Business School, Amity University Dubai, Dubai, United Arab Emirates
Introduction: This study aimed to evaluate the effectiveness of gamified virtual reality (VR) exercise as a strategic intervention to enhance body image perception and social interaction among overweight women with clinically diagnosed social anxiety, and further to explore the potential of VR-based physical activity in promoting inclusivity and well-being within the context of sports tourism and experiential wellness.
Methods: A quasi-experimental pretest–posttest design was employed with 128 women aged 20–40 who were categorized as having class I or II obesity (BMI 30–40). Participants were randomly assigned to either a 12-session gamified VR exercise program delivered across 4 weeks (three sessions per week) or a standard gym-based exercise group of equal duration and intensity. Validated self-report instruments were administered before and after the intervention, and analysis of covariance (ANCOVA) was conducted to examine between-group differences while controlling for baseline scores.
Results: Results indicated that the VR intervention group showed significantly greater improvements in body image flexibility (F = 51.30, p < 0.001, η2 = 0.286) and social interaction (F = 46.24, p < 0.001, η2 = 0.266) compared with the control group, along with a moderate reduction in BMI.
Discussion: These findings suggest that gamified VR-based exercise is an effective and engaging approach to improving psychological well-being and promoting inclusive participation among women who face social and emotional barriers to physical activity, while also holding promise as a strategic asset for fostering engagement in sports tourism and broader community wellness initiatives.
1 Introduction
The study on virtual reality (VR) exercise, sports tourism, and women’s wellbeing exhibits how technologies can enhance fitness experiences while contributing to enriched psychological and physical health among women. This blend analyses recent literature highlighting various aspects of immersive exercises, global tourism, and health. Obesity is considered one of the major global health challenges, disproportionately affecting women and leading to a cascade of physical, psychological, and social complications (Gómez-Ambrosi et al., 2025; Ng et al., 2014). In particular, women classified as having Class I obesity (BMI: 30–34.9) and Class II obesity (BMI: 35–39.9) are not only at higher risk for metabolic disorders but also face significant psychological consequences, such as diminished body image and increased social anxiety (Yao et al., 2025). These psychological outcomes create serious barriers to women’s social and physical participation, ultimately resulting in a cycle of isolation, physical inactivity, and psychological distress (Tomiyama et al., 2018). Studies show that 68% of obese women actively avoid social gatherings due to weight-related stigma (Dever et al., 2025; Puhl and Heuer, 2009), posing significant challenges both to individual wellbeing and to the global sports events and tourism industry, estimated at over $1.5 trillion annually (Liu-Lastres and Cahyanto, 2021). Among these psychological pressures, social anxiety is recognized as a harmful factor in the daily lives of obese women. Social anxiety refers to a persistent fear of judgment and negative evaluation by others and often prevents individuals from participating in social situations—especially those involving physical performance or exposure of the body (Wang et al., 2025). At the core of this issue lies body image—a multidimensional concept in psychology encompassing individuals’ perceptions, thoughts, and feelings about their bodies. Among women with Class I and II obesity, negative body image is directly associated with low self-esteem, depression, and avoidant behaviors in social or athletic contexts, leading to reduced social interaction and daily communication difficulties (Cash and Smolak, 2011; Tylka and Wood-Barcalow, 2015). These perceptions are not merely aesthetic; they have significant behavioral consequences that affect a person’s willingness to engage in social events, especially those that require being present in public or exposing the body (Thomas et al., 2020). Accordingly, the use of physical exercise has been recommended as a strategy to reduce anxiety and foster a more favorable body image (Kaplan, 2020). Such interventions may lead to weight and BMI reduction, improved health, and alleviation of psychological and anxiety-related pressures.
To date, various exercise-based approaches have been implemented to prevent individuals from progressing to Class III obesity, a stage considered a severe and difficult-to-reverse medical condition (Ng et al., 2024; Schuch and Vancampfort, 2021). For instance, some studies have highlighted the positive effects of high-intensity interval training (HIIT) in obese women (Wewege et al., 2017). Additionally, research has shown that combined aerobic and resistance training can effectively reduce fat mass while preserving muscle mass in women with Class I and II obesity (Villareal et al., 2017). In some cases, group-based exercise programs have been proposed as alternative strategies to promote more active participation among obese women, due to their potential to reduce anxiety and increase motivation (Cumillaf et al., 2025). Moreover, the effectiveness of yoga-based physical activity (Raghuram et al., 2021), training in gym and fitness club environments (Wang et al., 2021), and various forms of dance have been frequently recommended as exercise solutions for weight loss and anxiety regulation (Staiano et al., 2017; Zhang et al., 2024). However, a critical issue overlooked by many of these studies is that women with high BMI levels often refrain from attending gyms or group classes. These environments are frequently perceived as judgmental and appearance-focused, which in turn intensifies body dissatisfaction and anxiety. Consequently, many obese women are unwilling to participate in public physical activities (Benvenuti et al., 2021). Additionally, studies show that due to prolonged inactivity, such individuals often develop a lack of interest in physical exercise, and a tendency toward sedentary behavior becomes ingrained (Khan et al., 2024). Therefore, traditional exercise programs are generally ineffective in meaningfully engaging obese women, as they may face physical limitations, lack motivation, or experience psychological discomfort in conventional fitness environments (Carraça et al., 2021). These challenges underscore the necessity of adopting alternative and more inclusive strategies—those capable of increasing motivation, reducing social stigma, and providing participants with a positive experience.
In this context, exercise experiences within virtual reality (VR), enhanced by gamification elements, have emerged as promising innovations in the promotion of health. Virtual reality is a computer-simulated environment that enables users to interact with it using multiple senses such as sight, sound, and touch. This immersive experience can convincingly simulate a sense of presence in a virtual world (Faria et al., 2025; Levy et al., 2025). Gamification, defined as the application of game elements and features in non-game, real-life contexts, is intended to capture attention, stimulate motivation, and enhance engagement (Poliani et al., 2023). The integration of exercise with VR environments and gamified features such as goal-setting, feedback, rewards, and social interaction appears to offer an effective solution. Since engaging individuals with higher levels of obesity requires strong motivational drivers and attractive experiences, this approach could prove genuinely impactful (Dong et al., 2025; García-González et al., 2025), encouraging women to move beyond traditional, monotonous exercise settings and actively participate in physical activity. In this regard, a scoping review demonstrated that immersive VR interventions enhance motivation, affect, enjoyment, and engagement during exercise across both healthy and clinical populations (Modlin and Kuo, 2020; Mouatt et al., 2020), while a pilot randomized trial found that VR-based exercise, when compared to traditional modalities, was both effective and well-accepted among adults with obesity, yielding psychological and behavioral benefits (Touloudi et al., 2025).
Accordingly, the present study employs a quasi-experimental pre-test–post-test design to examine the effectiveness of gamified physical exercise within a virtual reality environment on enhancing social interaction and improving body image perception among women with social anxiety who are classified as having Class I and II obesity. The primary outcomes of interest were body-image flexibility and social interaction, while secondary outcomes included changes in BMI. What is new in this study is the explicit focus on women facing the dual challenges of Class I–II obesity and clinically diagnosed social anxiety—a population often excluded from digital health interventions. This group of women requires targeted, enjoyable, and low-resistance interventions that allow them to engage in meaningful physical activity without experiencing social judgment or feelings of shame. This research seeks to reposition virtual reality from merely an entertainment tool to a platform for psychosocial empowerment. By integrating VR with gamification principles, the study aims to introduce a novel, non-pharmacological, and psychologically informed approach to wellness and sports tourism promotion. The objective is to reduce not only physical barriers but also the mental and emotional obstacles that prevent obese women from participating in social and physical activities. Ultimately, the study aspires to enable this population to engage in global sports tourism events with courage and self-confidence, develop a more positive experience with their bodies, and take meaningful steps toward improved body image and greater social participation.
2 Literature review
2.1 The combined use of VR and gamification in psychological and physical empowerment
Virtual reality (VR) has emerged as a groundbreaking tool in the fields of mental health promotion and physical activity engagement. Its immersive qualities create simulated environments that divert attention away from pain, fatigue, and external judgment, making exercise more enjoyable and emotionally manageable for participants (Dong et al., 2025). Research indicates that engaging in VR-based exercise can significantly improve motivation and adherence by transforming routine physical activity into an interactive and personally meaningful experience (Al-Rasheed et al., 2022; Wang et al., 2025). For instance, studies involving overweight children found that running in a virtual setting not only reduced their perception of physical discomfort but also increased their overall enjoyment of exercise, which in turn improved their willingness to participate consistently (Finkelstein et al., 2011). Similar benefits have been observed in adult populations. Randomized trials have shown that participants in VR-enhanced programs—especially when combined with behavioral counseling—exhibited greater reductions in BMI and body fat percentage, along with notable improvements in self-efficacy and motivation compared to those in traditional exercise routines (Tatnell et al., 2022). Furthermore, VR interventions have demonstrated effectiveness in alleviating symptoms of anxiety and depression. For example, dialysis patients who engaged in cycling exercises within a VR environment reported significant psychological relief during treatment sessions (Kang et al., 2025). Notably, in studies involving women with high levels of social physique anxiety, having a virtual workout companion with similar body characteristics created a sense of safety and acceptance, which reduced fear of judgment and encouraged participation in exercise (Kroon et al., 2023). These findings point to VR’s potential in addressing the emotional and psychological barriers that often prevent overweight women from engaging in public or group-based fitness activities.
In parallel, gamification—the integration of game-like elements into non-gaming contexts—has gained traction as a motivational strategy in health and fitness interventions. By introducing features such as point systems, challenges, real-time feedback, and rewards, gamification enhances user engagement and transforms exercise into a more compelling and satisfying experience (Johnson et al., 2016). Meta-analyses of randomized controlled trials have consistently shown that gamified interventions can lead to moderate improvements in physical activity across various populations, including individuals with chronic conditions (Mazeas et al., 2022). Game design elements tap into intrinsic motivators such as competence, autonomy, and relatedness, which are key drivers of sustained behavior change. When physical activity feels purposeful and rewarding, individuals are more likely to develop a positive attitude toward exercise and stick with it over time (Koivisto and Hamari, 2019). This is especially relevant for populations that face motivational deficits or psychological barriers to exercise—gamification introduces structure, enjoyment, and a sense of progress, all of which help counteract disengagement.
Despite these promising outcomes, existing literature has focused primarily on general populations or patients with chronic diseases. There’s still a significant lack of research exploring the combined impact of VR and gamified exercise on women with Class I and II obesity who struggle with social appearance anxiety and exercise-related distress. This gap highlights an urgent need for targeted studies that assess how digital and immersive technologies can be strategically leveraged to empower these women—helping them overcome emotional barriers, build self-efficacy, and reengage with physical activity in ways that are sustainable and psychologically safe. By integrating the psychological advantages of gamification with the immersive and protective nature of VR environments, future interventions may unlock new possibilities for fostering active lifestyles among overweight women—a population that remains underserved and underrepresented in both technological innovations and public health strategies.
2.2 Sports tourism and VR experiences
Global Sports tourism events serve as critical catalysts for worldwide tourism development, influencing local economies through enhanced visitor spending on accommodations, dining, transport, and entertainment. It was estimated that the global tourism market size to be USD 683,169.3 million in 2023, with a projection to reach USD 2,137,857.0 million by 2030, with a growth CAGR of 17.7% from 2024 to 2030 (Horizon Grand View Research, 2025). The study Lipták and Tarkó (2021) revealed and highlighted how leisure and tourism activities tie into wellbeing, underscoring the necessity for more inclusive leisure and sports tourism prospects targeting women’s mental, social, and physical health. The study by Qian (2022) supports developing tourism products tailored for women, reflecting both wellbeing and lifestyle improvement motives, and focuses on the growing demand for female participation in sports tourism. New study by Cariati et al. (2025) found that out of six recent randomized controlled trials (RCTs) five had a greater impact with the use of virtual reality (VR) on their sports activities. Researchers Chang and Yang (2024) studied that VR tourism in healthcare environments with immersive VR experiences can positively affect wellbeing by reducing stress and promoting positive mental states of diverse populations, including women. Post-experience of VR consumer behavior in tourism is positively influenced, increasing tourists’ willingness to visit destinations (Zhang and Tsai, 2021). VR manages the complexities of visitor expectations and engagement within the tourism ecosystem by offering a multisensory, immersive experience, shaping positive attitudes towards destinations (Beck et al., 2019). The easy adaptability of VR technology enhances overall efficacy of marketing strategies, allowing tourism stakeholders to design customized experiences that cater to diverse visitor needs and preferences (Han and tom Dieck, 2019). The adaptability of VR technology enables tourism providers to design personalized experiences that address the diverse needs and preferences of visitors, thereby enhancing the effectiveness of their marketing strategies (Han and tom Dieck, 2019). VR’s integration into sports tourism is validating a paradigm shift towards immersive and interactive experiences that transcend traditional limits, delivering innovative fixes to augment consumer engagement and satisfaction. The Scope of VR continues to evolve, encouraging new scopes for audiences engaging with wellness and sports travel. Furthermore, adding the sports tourism market into a dynamic sector characterized by significant growth potential, driven by effective marketing strategies, technological innovations, and an awareness of the importance of sustainable practices. By participation of diverse sports participants, the tourism sector can facilitate broad global economic benefits, making sports tourism augmented with VR exercises and experiences a vital pillar of modern travel.
2.3 Physical activity, social anxiety, and obesity in women
Regular physical activity is widely acknowledged as one of the most effective strategies for weight management and mental health enhancement. Among women with Class I and II obesity (BMI 30–40), these benefits become particularly significant, not only due to physiological improvements such as fat reduction and metabolic regulation but also through psychological advantages, including decreased anxiety, improved self-esteem, and better emotional regulation (Cumillaf et al., 2025; Yao et al., 2025). Meta-analytic evidence consistently demonstrates that exercise modulates stress hormones like cortisol, improves sleep quality, and fosters increased life satisfaction and vitality (Mikkelsen et al., 2017; Rebar et al., 2015). For women within this population, physical activity acts as a dual-purpose intervention, alleviating both the physical burden of obesity and serving as a psychological buffer against social and emotional distress. However, addressing obesity purely through biomedical interventions neglects the psychosocial dimensions, particularly social physique anxiety (SPA), a subtype of social anxiety characterized by the fear of negative evaluation based on one’s body size or appearance (Hart et al., 1989; Song et al., 2025). SPA tends to be heightened in public exercise environments such as gyms, sporting events, or group classes, often leading women to avoid such settings altogether (Vartanian and Novak, 2011).
Statistical evidence paints a concerning picture. An estimated 68% of women with obesity avoid social gatherings specifically due to weight-related stigma (Puhl and Heuer, 2009), which not only affects their psychological health but also contributes to tangible economic losses in industries reliant on broad participation—particularly the global events sector, valued at over $1.5 trillion USD in 2023 (Liu-Lastres and Cahyanto, 2021; Ng et al., 2024), Also, weight stigma is not a peripheral issue—it directly erodes participation, motivation, and confidence. Women with higher BMI scores often report up to 3.2 times more anxiety in social contexts compared to their average-weight peers (Kaplan, 2020; Santonja-Ayuso et al., 2025). This avoidance is further linked to body image inflexibility, a psychological rigidity around body acceptance, and is reflected in instruments like the Glass Social Interaction Questionnaire, where women with obesity score approximately 40% lower than normal-weight individuals. Moreover, 42% of global event venues have reported a decline in attendance from women concerned about health and appearance issues, signaling the reach of this crisis far beyond individual distress (Elbarazi et al., 2024). These behavioral patterns create a feedback loop: fear of negative judgment leads to withdrawal from physical activities and public life, which in turn perpetuates isolation, emotional discomfort, and further weight gain (Puhl and Suh, 2015). Traditional interventions such as cognitive-behavioral therapy (CBT) have shown efficacy in clinical settings, but often lack scalability, affordability, and contextual fit in dynamic environments like community gyms or public events (Romano et al., 2022). In this way, a longitudinal clinical study demonstrated that women with obesity who engaged in a structured exercise program exhibited significantly reduced levels of body dissatisfaction after 24 months, compared to baseline measurements, despite not fully attaining their initial ideal body image. This sustained improvement was attributed primarily to a reduction in negative investment in physical appearance and a concurrent increase in positive body awareness, highlighting one of the key psychological benefits of regular physical exercise (Carraca et al., 2012). Moreover, systematic reviews indicate that athletes and regular physical activity participants generally possess more positive body images. There is a well-established negative correlation between engagement in sport and concerns related to physical appearance. Recent meta-analyses further confirm that exercise interventions contribute to enhanced physical self-esteem, greater satisfaction with appearance, and reduced negative self-criticism (Zhang et al., 2024b).
3 Methodology
3.1 Participants and experimental framework
This study adopts an applied, quasi-experimental research design with a pretest-posttest control group structure. The statistical population comprised adult women aged 20–40 years residing in Tehran, Iran, who met specific inclusion criteria: a body mass index (BMI) within the range of 30–40 (indicative of Class I or II obesity), and clinically confirmed social anxiety symptoms. To identify suitable participants, public announcements were disseminated across various channels including local sports clubs, psychological counseling centers, medical clinics, and social media platforms.
Candidates underwent initial screening by licensed physicians and clinical psychologists to verify BMI and social anxiety eligibility. In this regard, a CONSORT-style flow of participants was documented as follows: of the 143 women initially screened, 15 were excluded due to ineligibility or withdrawal; 128 were randomized equally into the two study arms (64 in the VR gamified intervention and 64 in the gym-based control). Attrition during the intervention was minimal, with 3 participants discontinuing in the VR group and 4 in the control group due to scheduling conflicts or non-study-related health issues. The final analyses were conducted on 121 participants, reflecting an adherence rate above 90%, which supports the robustness of the finding. Ultimately, a total of 128 participants were enrolled. After completion of baseline assessments, participants were randomly assigned (1:1) to the VR gamified intervention group (n = 64) or the control group (n = 64) using a stratified permuted-block randomization procedure to ensure balance with respect to obesity class and age group. Two stratification factors were used: obesity class (Class I: BMI 30.0–34.9; Class II: BMI 35.0–40.0) and age group (20–29 years; 30–40 years), producing four strata. Within each stratum, treatment allocations were generated in permuted blocks of size 4 using a computer-generated random sequence (SPSS v26 random number generator). The allocation sequence was prepared by an independent statistician not involved in recruitment or assessment. Allocation concealment was maintained with sequentially numbered, opaque, sealed envelopes that were opened only after baseline data collection. Outcome assessors were blinded to group assignment.
Both groups followed identical training protocols in terms of session frequency, duration, and intensity, to ensure equivalence of physical exertion and exposure across conditions. The key distinction between the two groups lay in the format and delivery environment of the exercise sessions. The experimental group engaged in structured gamified physical training within an immersive virtual reality (VR) environment, incorporating elements of game design such as visual feedback, challenges, and interactive features. In contrast, the control group participated in equivalent traditional exercise sessions conducted in a standard gym setting, without any gamification or virtual components. Both groups followed identical protocols regarding session frequency, duration, and exercise intensity to ensure that the only variable manipulated was the method of delivery. The intervention process took place over a 5-week period, from May 15 to 19 June 2025. All participants provided written informed consent prior to their inclusion in the study.
Table 1 Demographic and health characteristics of participants by study group (n = 128). Values are presented as mean (range) or n (%). Categorical comparisons were performed using chi-square tests; categorical p-values were computed from the reported counts. Continuous comparisons were tested using independent-samples t tests; because standard deviations were not provided in the original table, the p-values and Cohen’s d reported for Age and BMI above are estimated (Age SD estimated as range/4 ≈ 5.0; BMI SD assumed 3.0). Cramér’s V is reported for categorical effect sizes. All reported effect sizes indicate negligible to small differences between groups, consistent with successful randomization.
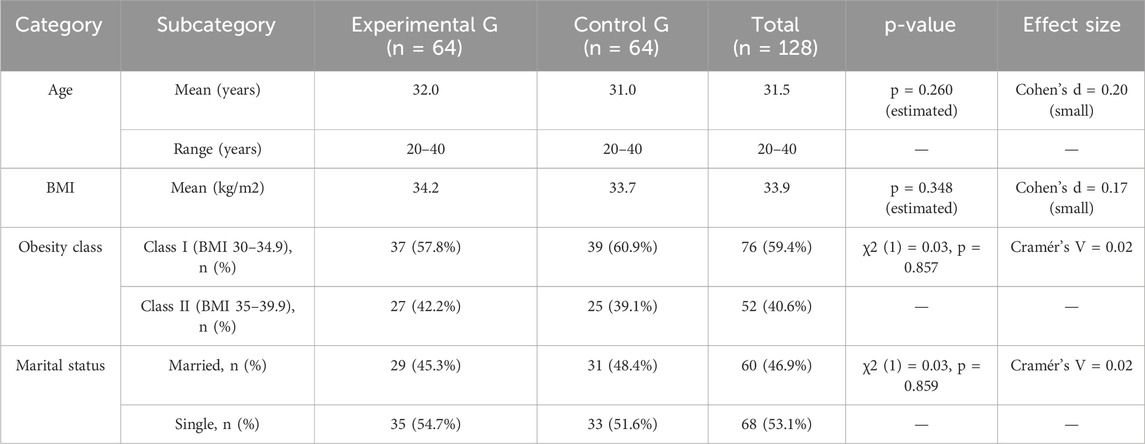
Table 1. Demographic and health characteristics of participants.
3.2 Measurement instruments and testing protocol
To evaluate the psychological outcomes of the intervention, two standardized and psychometrically validated self-report instruments were employed. Social interaction was assessed using the Social Interaction Anxiety Scale (SIAS) developed by Mattick & Clarke, (1998), and Body image flexibility was measured using the Body Image-Acceptance and Action Questionnaire (BI-AAQ) developed by Sandoz et al. (2013), comprising 12 items that assess the extent to which individuals can accept and respond flexibly to negative thoughts and emotions related to their body image. Both instruments were translated into Persian using a standard forward–backward translation procedure by bilingual experts, followed by pilot testing to ensure cultural validity and semantic clarity. Minor adjustments were made to optimize comprehensibility while retaining fidelity to the original constructs. Internal consistency was re-evaluated within this sample, with the SIAS demonstrating α = 0.83 (95% CI: 0.78–0.87) and the BI-AAQ demonstrating α = 0.80 (95% CI: 0.75–0.85) (Mattick and Clarke, 1998; Sandoz et al., 2013). Both questionnaires were administered in paper format during individual sessions conducted before and after the 4-week training program. All participants completed the assessments under standardized conditions, ensuring confidentiality and minimizing potential response bias. The internal consistency of both instruments was re-evaluated in the present sample. In addition to psychological assessments, participants’ anthropometric measures were collected to monitor physical changes related to the intervention. Height was measured using a standard stadiometer, and weight was recorded with a calibrated digital scale, both conducted under standardized conditions at baseline and post-intervention. Body Mass Index (BMI) was subsequently calculated as weight in kilograms divided by height in meters squared (kg/m2). In addition, all self-report questionnaires (Social Interaction Anxiety Scale and Body Image-Acceptance and Action Questionnaire were administered in a private setting using participant codes to preserve anonymity and reduce social-desirability pressure. Participants received standardized, written and verbal instructions and completed questionnaires without the presence of other participants. Trained research staff were available to clarify procedural questions but did not influence responses. Outcome assessors who handled scoring and data entry remained blinded to group allocation. In addition to self-report measures, objective anthropometric data (height and weight) were measured by trained personnel using calibrated instruments to calculate BMI. These procedural safeguards were implemented to reduce potential measurement bias.
3.3 Statistical analysis
To examine the distributional assumptions of the collected data, the Kolmogorov-Smirnov test was applied to verify normality. The homogeneity of variances across groups was evaluated using Levene’s test. Subsequently, to investigate the study hypotheses while controlling for potential covariates, an Analysis of Covariance (ANCOVA) was performed utilizing SPSS Statistics version 26.
3.4 Process of exercise implementation and intervention
The experimental group participated in group-based exercises conducted within an immersive virtual reality (VR) environment using Oculus Quest 2 headsets, which provided 6 degrees of freedom and wireless mobility. The VR content was developed using a Unity-based custom platform compatible with Oculus SDK, enabling real-time rendering of interactive exercise environments. A custom-designed VR platform was employed, enabling participants to interact with a virtual gym environment that simulated spacious exercise halls with mirrored walls, dynamic lighting, and synchronized background music. The system supported group sessions where participants could see their own avatars as well as those of their peers, thereby enhancing the sense of social presence and co-exercise. Safety guidelines were followed, including calibration of the play area, mandatory warm-up phases, and monitoring for motion sickness or discomfort, with the option to pause or withdraw if needed. Before participation, all individuals underwent safety screening, including cardiovascular risk check and a brief cyber sickness questionnaire; those reporting severe motion sensitivity were excluded.
The intervention included three distinct types of group exercises adapted for women with overweight or obesity: Zumba, aerobic dance routines, and low-impact cardio circuits. Each exercise session was delivered in a virtual gym environment specifically designed to replicate the spatial and social dynamics of real group classes. The environment included mirrored walls for self-monitoring, synchronized background music, and real-time visual cues that guided movement sequences. Participants were represented by customizable avatars, allowing them to observe their own movements as well as those of their peers. This avatar-based representation enhanced social presence while protecting personal privacy. Also, a trained instructor was projected as a virtual avatar located at the front of the virtual room. This avatar provided live demonstrations, verbal instructions, and corrective feedback in real time through voice integration. Movement tracking was achieved via the Oculus Quest 2 headset and hand controllers, which captured upper-body and basic full-body movements. Exercises were programmed to accommodate limited range of motion, with modifications automatically suggested by the instructor avatar if movements were not detected or were incomplete. To ensure participant safety, an on-site facilitator was physically present in the exercise room. This facilitator monitored participants’ real movements, assisted with headset adjustments, and intervened if signs of motion sickness, dizziness, or fatigue appeared. All sessions began with a standardized 5-min warm-up and concluded with stretching and cool down exercises to minimize the risk of musculoskeletal strain.
Exercise difficulty was progressively adapted over the course of the 12 sessions. In the first week, movements were simplified and pacing was slower; in later weeks, the duration of continuous activity and the complexity of dance sequences were gradually increased. The VR system provided real-time metrics (such as elapsed time, calories burned, and movement accuracy) displayed on the heads-up interface, enabling participants to track their own progress. These features ensured that the intervention was both replicable and adaptable to the needs of overweight participants.
To maintain high levels of engagement and prevent dropout, gamification elements were systematically embedded in the sessions. These included:
Reward systems: digital badges and points awarded for attendance, effort, and task completion, displayed on personal dashboards.
Friendly competition: leaderboards showing cumulative scores of participants, refreshed weekly to stimulate motivation while maintaining a supportive environment.
Social recognition: virtual applause animations and verbal praise delivered by the instructor avatar and peers when milestones were achieved.
Progress tracking: participants could visualize their performance and improvements (e.g., calories burned, time spent, consistency streaks) through simple on-screen metrics. These gamification mechanisms were chosen based on established design principles (challenge, feedback, reward, and social connection) and were intended to foster intrinsic motivation, enjoyment, and group cohesion.
The training protocol consisted of 12 sessions delivered across four consecutive weeks, with three sessions per week. Each session lasted 35–50 min, balancing sufficient physical exertion with safety for overweight participants. Intensity was progressively adjusted by modulating the difficulty of movements and the pace of virtual routines. Heart rate was monitored intermittently using wearable chest-strap monitors in 25% of randomly selected participants per session to verify that exertion levels remained within the moderate-intensity zone (50%–70% of age-predicted HRmax.Also, No dietary program was prescribed to participants, and they were instructed to maintain their usual eating patterns throughout the intervention. At each session, adherence to this instruction was verbally confirmed by facilitators. Energy expenditure was not directly monitored; however, exercise frequency, duration, and intensity were standardized and identical across groups.
In contrast, the control group engaged in standard group exercise sessions in a traditional gym setting. These sessions were matched in frequency (three times per week) and duration (35–50 min per session) to the experimental group and were led by qualified fitness instructors experienced in working with overweight populations. No gamification elements or VR components were included in the control condition.
4 Results
Descriptive statistics were calculated to summarize the performance of participants in both the experimental and control groups across the two main variables—Social Interaction and Body Image. As shown in Table 2, the post-test mean scores for both variables were consistently higher in the experimental group compared to the control group, indicating the potential positive impact of the VR-based gamified exercise intervention. The standard deviations reflect an acceptable level of variability, supporting the reliability of the observed differences before proceeding with inferential tests.
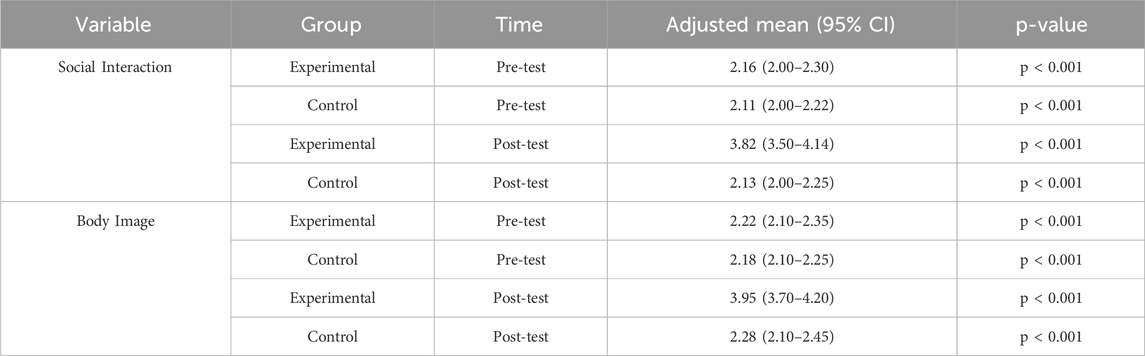
Table 2. Descriptive statistics for social interaction and body image scores.
As shown in Table 3, the results of the Kolmogorov–Smirnov test indicate that all variables across both pre-test and post-test phases in both experimental and control groups followed a normal distribution (p > 0.05). These results satisfy the assumption of normality required for conducting parametric analyses such as ANCOVA.
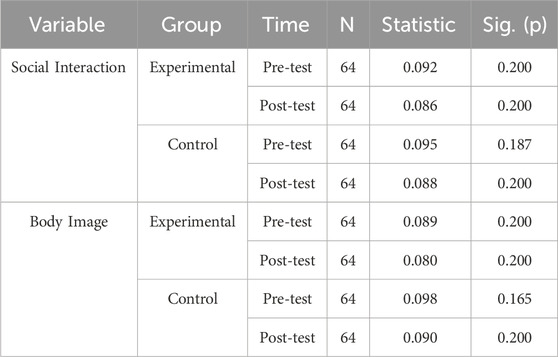
Table 3. Kolmogorov–smirnov test.
As presented in Table 4, the results of Levene’s test for equality of variances demonstrate that none of the variables violated the assumption of homogeneity (p > 0.05).
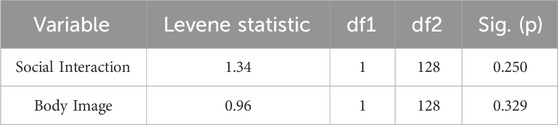
Table 4. Levene’s test result.
Table 5 shows that after 12 sessions of VR-based gamified exercise, women with obesity and social anxiety in the experimental group experienced a meaningful reduction in BMI—from 34.2 to 33.0 (−3.5%). In contrast, the control group, which engaged in traditional gym-based exercise, showed only a minimal decrease from 33.7 to 33.6 (−0.3%). These findings highlight the potential effectiveness of gamified VR training in facilitating short-term weight loss among women with obesity.

Table 5. Pre- and post-intervention changes in BMI.
According to Table 6, the ANCOVA results for Social Interaction and Body Image revealed significant differences between the experimental and control groups, supporting the effectiveness of the intervention in enhancing psychological outcomes. Pre-test scores for both variables were controlled to ensure that the observed changes in the post-test were due to the intervention rather than pre-existing differences.

Table 6. Analysis of covariance.
For Social Interaction, after adjusting for pre-test scores, the experimental group showed a significantly greater improvement compared to the control group. The F value for the group effect was 46.24 (p = 0.000), indicating a substantial and statistically significant difference between the groups. The partial eta-squared (η2) value of 0.266 reflects a medium effect size, suggesting that the intervention accounted for approximately 26.6% of the variance in the post-test social interaction scores. This indicates a meaningful impact of the VR-based gamified exercise program in improving social interaction among the experimental group. Similarly, for Body Image, the ANCOVA revealed a significant difference between the experimental and control groups. The F value for the group effect was 51.30 (p = 0.000), further confirming the intervention’s effectiveness. The partial eta-squared value of 0.286 represents a large effect size, meaning that the group factor accounted for 28.6% of the variance in post-test body image scores. This demonstrates a substantial impact of the VR-based gamification program in improving body image perceptions in the experimental group.
Figure 1 presents the extent of changes observed in the variables of body image and social interaction following the intervention.

Figure 1. Comparison of effect sizes for body image and social interaction.
5 Discussion
Social interaction plays a vital role in psychological wellbeing, fostering a sense of belonging, emotional support, and self-worth (Thomas et al., 2020). Limited participation in social and community events—often observed among individuals with social physique anxiety and obesity—not only restricts opportunities for meaningful connection but also reinforces negative self-perceptions and emotional distress (Puhl and Heuer, 2009). In line with this, the present study was conducted with the aim of exploring the effects of gamified virtual reality-based exercise on improving social interaction and body image in women with social anxiety who have Class I and II obesity. The goal was to harness the engaging potential of virtual reality technology along with the enjoyable elements of gamification to provide a non-pharmacological and effective intervention for this important and vulnerable population. The intervention sought to help prevent progression to Class III obesity and to enhance their participation in events and social interactions. The results of this study demonstrated significant and positive effects of the intervention. These findings not only align with previous research but also represent a forward step in leveraging new technologies such as virtual reality to improve the psychological and social wellbeing of this population.
One of the key findings of this study was the significant improvement in social interaction issues within the experimental group. This result aligns with previous research indicating that obese individuals—particularly women—often avoid social situations due to weight-related stigma (Puhl and Suh, 2015). Furthermore, the use of gamified virtual reality-based exercise, which simultaneously addresses both psychological and physical aspects, significantly reduced these social barriers among obese women. Recent studies have also emphasized that gamification and virtual reality interventions can enhance individuals’ social motivation and help prevent social isolation (Jingili et al., 2023). These results are especially noteworthy for obese individuals who typically experience anxiety in group settings. Other studies, such as Wang et al. (2025), have shown that virtual reality interventions—especially when combined with gamification elements—can reduce social anxiety and facilitate improvements in social interaction (Wang et al., 2025). Recent research by Dong et al. (2025) also supports these findings, demonstrating that gamified virtual reality exercises can significantly reduce suicidal ideation and anxiety in elderly populations (Dong et al., 2025).
These outcomes are consistent with the current study’s results, as the virtual reality environment provides a safe and controlled space in which participants—particularly women—may feel more secure and less exposed to social judgment. Unlike traditional gym settings where public visibility often triggers anxiety, virtual environments allow users to gradually overcome fear and stress (Kroon et al., 2023). This safe exposure process can prepare them for real-world social interactions. As participants experience tangible results—such as weight reduction—within the VR environment, their self-confidence increases, empowering them to engage more fully in public and social events. This suggests that the integration of gamification with virtual reality may be more effective than traditional approaches in improving social interaction. The interactive and engaging nature of gamification enables individuals to participate in social activities without fear of judgment (Al-Rasheed et al., 2022; Wang et al., 2025). It is noteworthy that the women participating in the present study had no prior experience with virtual reality (VR). However, after just one session of VR training that incorporated gamification elements, many of them expressed strong interest in using this innovative technology again. This observation aligns with our clinical experiences, indicating a significant willingness among individuals—particularly after direct exposure—to adopt VR-based interventions for addressing both physical and psychological issues (García-González et al., 2025). Previous studies have underscored the distinctive capabilities of this engaging technology as an effective tool for enhancing wellbeing and quality of life, especially among individuals in need of psychological support or behavioral change. As highlighted in recent literature, VR has introduced a transformative, non-pharmacological approach to healthcare with minimal side effects, which has increasingly attracted the attention of professionals in medical and mental health fields (Freeman et al., 2023). However, implementing VR-based interventions requires specialized equipment, such as Oculus Quest 2 headsets, and custom-developed VR software, which can incur significant costs. Additionally, staff members must be trained to assist participants in using the technology and ensure their safety during the virtual exercise sessions. These factors must be considered when scaling up the implementation of VR-based programs, particularly in clinical or community settings.
However, some studies have reported contradictory findings. For instance, Wechsler et al. (2019), in their systematic review, stated that certain individuals prefer traditional face-to-face therapy or real-world exposure methods over virtual environments, citing the artificial nature of VR and the lack of human interaction as reasons for their preference (Wechsler et al., 2019). This discrepancy may be attributed to the relatively underdeveloped state of virtual reality technology at the time of those studies, which may not have effectively conveyed a sense of realism or presence, preventing users from fully engaging with the experience. Czub, et al. reported that virtual reality-based exercise did not significantly increase participation in training activities among their participants (Czub and Janeta, 2021). This inconsistency could be explained by a lack of sufficient motivation and psychological readiness in the participants. In the present study, however, the incorporation of engaging gamification elements aimed to enhance the motivation and emotional readiness of women to participate in VR-based exercise. It appears that this intelligent integration of technology and gamification may be a key reason for the positive outcomes observed.
The second major finding of this study pertains to the significant improvement in body image within the experimental group. This result aligns with previous research indicating that negative body image is associated with low self-esteem and depression among obese individuals (Cash and Smolak, 2011). Additionally, recent studies such as those by Al-Rasheed et al. (2022) and Kang et al. (2025) have emphasized that physical activity—particularly when integrated with modern technologies—can enhance body image and help individuals develop a more positive perception of their bodies (Al-Rasheed et al., 2022; Kang et al., 2025). Furthermore, studies like Levy et al. (2025) have demonstrated that virtual reality environments, by enabling “body rescripting,” can reduce perceptual distortions related to body image (Levy et al., 2025). This mechanism may help explain the positive effects of the gamified exercise program used in the present study. Our findings also support those of Johnson et al. (2016), who reported that gamification elements—such as reward systems and visual progress tracking—enhance engagement and long-term commitment to body image improvement programs (Johnson et al., 2016). The use of virtual environments and engaging interactions provided a safe, low-pressure space for women—who often perceive themselves as overweight—to develop a more positive outlook toward their bodies. These results are further confirmed by recent research conducted by Cumillaf et al. (2025), which showed that virtual reality-based exercise programs helped reduce body dissatisfaction and improve body image, particularly in individuals with severe obesity (Cumillaf et al., 2025). Moreover, the study by Murphy and Creux (2021) highlighted the importance of personalizing virtual reality environments for specific populations. They found that designing avatars to match the physical characteristics of obese users helped reduce the gap between perceived and actual body image (Murphy and Creux, 2021). This alignment highlights the positive effects of engaging in physical activity within virtual reality environments on both weight reduction and enhanced body image satisfaction. These findings are consistent with the present study and underscore the potential of integrating VR-based exercise programs—particularly when combined with elements such as gamification—as an effective strategy for preventing psychological disorders and managing weight-related challenges. Moreover, by fostering a more positive body image and reducing psychological barriers such as appearance-related anxiety, these interventions can encourage greater participation in social settings and public events, ultimately enhancing individuals’ social interaction and quality of life.
6 Conclusion
Overall, the results of this study indicate that gamified virtual reality–based exercise interventions can effectively improve social interaction and body image among obese women with social anxiety classified as having Class I and II obesity. Given that increased social participation and enhanced body image in this population can contribute to reductions in anxiety, depression, and isolation, such interventions may serve as innovative strategies to promote the psychological and social wellbeing of obese individuals, while also contributing to BMI reduction alongside psychological factors. These findings further emphasize the importance of integrating gamification and virtual reality within exercise programs, as they can specifically enhance motivation and engagement among obese individuals and help overcome psychological barriers. It is hoped that the results of this research will inform the design of comprehensive digital health interventions—particularly for obese women with specific psychological needs—and pave the way for the development of individual and social empowerment programs that combine principles of exercise and technology for similar populations. The integration of virtual reality (VR) into exercise and wellness plans boons a transformative breakthrough to enhance sports tourism initiatives targeted at women. VR offers immersive and motivating environments that can foster both physical engagement and psychological wellbeing, as female travelers increasingly seek fitness experiences that balance enjoyment with health benefits. By enriching the intersection of digital adventure, wellness, and tourism, VR-driven fitness experiences encourage better participation, upkeep body confidence, and align with global trends in health-focused travel. This technological amalgamation thus serves as a strategic tool to empower women, advance inclusivity, and elevate the overall impact of wellness tourism.
7 Managerial and practical implications
The findings of this study have important implications for public health policymakers, wellness program designers, and professionals working in the fields of sports science, psychology, tourism stakeholders, and community engagement. Women with obesity and social anxiety often avoid public events and social gatherings due to negative body image and fear of social judgment, which leads to a vicious cycle of inactivity, isolation, and psychological distress.
By implementing gamified VR-based exercise interventions as part of broader community health promotion strategies, public health agencies and wellness organizations can help these individuals improve their social interaction skills and body image over time. The inclusion of gamification elements—such as rewards, progress tracking, and interactive challenges—enhances intrinsic motivation and encourages sustained engagement in physical activity. Tourism stakeholders can customize and promote their marketing strategies as per the personal needs of each participant. Moreover, the immersive and novel nature of VR creates an appealing platform that draws users into consistent movement-based experiences in a non-judgmental virtual space. This enjoyable and psychologically safe environment promotes gradual physical activation, which can contribute to weight reduction and improvements in BMI. As women become more active and begin to experience physical and psychological benefits, their body image tends to improve, reinforcing their willingness to maintain such behaviors. Importantly, the controlled VR setting enables them to confront and manage anxiety-related triggers—such as fear of evaluation or social comparison—at their own pace. Over time, this process helps participants build resilience and confidence, which may translate into increased participation in real-world social activities and public events. In this way, gamified VR-based programs not only support individual transformation but also contribute to broader social inclusion goals. Consequently, integrating such interventions into community health centers, fitness programs, and mental health services can serve as a proactive strategy to engage women who are often marginalized from traditional fitness and social platforms. These interventions are especially beneficial in low-resource or conservative environments where public participation of women may be culturally constrained or psychologically intimidating. In addition, the relatively low-cost scalability of VR technology makes it a feasible option for deployment in municipal wellness programs, corporate employee assistance schemes, and even pre-event community initiatives targeting at-risk populations.
8 Limitations and future research directions
Despite the promising results of this study, several important limitations should be acknowledged. First, the sample was restricted to women with Class I and II obesity who also experienced social anxiety, which limits the generalizability of the findings to other populations such as men, individuals with more severe obesity (Class III), or those without social anxiety. Due to Limited Generalizability scope of broader sports tourism product innovation or commercialization potential is limited unless an intentionally niche market is targeted, and also cannot be applied to male or mixed-gender athlete populations. Future studies should consider more diverse samples, including various age groups, genders, and obesity levels, to enhance the external validity of the results. Also, A limitation of this study is the relatively short duration of the intervention (4 weeks), which may not fully capture long-term psychological and physiological outcomes. With this limitation in mind, future studies should adopt longer intervention periods and include follow-up assessments to provide deeper insights into the sustained effects of gamified VR exercise on body image, social interaction, and broader wellbeing outcomes. Another limitation of the present study is its reliance on self-report measures, which may be prone to biases such as social desirability, recall error, and common-method variance. Although these risks were reduced by using validated instruments, ensuring anonymous responses, blinding assessors, and including objectively measured BMI, some residual bias cannot be excluded. Future studies should strengthen measurement validity by combining self-reports with objective behavioral or physiological measures (e.g., accelerometers, heart-rate monitors), or by using real-time approaches such as ecological momentary assessment (EMA). Another limitation is that dietary intake and total energy expenditure were not directly monitored. Although participants were asked to maintain their usual eating habits and adherence was checked verbally, future studies should include more rigorous tracking of diet and objective monitoring of energy expenditure. A further limitation is that the study relied solely on quantitative measures, without collecting qualitative data such as participant experiences or perceptions. Incorporating qualitative insights in future studies would provide greater depth, helping to contextualize quantitative findings and to better understand the subjective impact of VR-based gamified exercise. Finally, While the claim that VR encourages participation in wellness-related tourism and social events is theoretically reasonable, it was not directly measured in this study. This limitation highlights the need for future research to incorporate behavioral measures or intentions related to sports tourism participation to validate this hypothesis and further explore the engagement mechanisms involved.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Approval ID: IR.SSRC.REC.1404.029 Research Ethics Committees of Sport Sciences Research Institute (SSRI). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HF: Project administration, Writing – original draft, Writing – review and editing, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Visualization. RG: Conceptualization, Funding acquisition, Project administration, Supervision, Validation, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Al-Rasheed, A., Alabdulkreem, E., Alduailij, M., Alduailij, M., Alhalabi, W., Alharbi, S., et al. (2022). Virtual reality in the treatment of patients with overweight and obesity: a systematic review. Sustainability 14 (6), 3324. doi:10.3390/su14063324
Beck, J., Rainoldi, M., and Egger, R. (2019). Virtual reality in tourism: a state-of-the-art review. Tour. Rev. 74 (3), 586–612. doi:10.1108/tr-03-2017-0049
Benvenuti, M. B., Bø, K., Draghi, S., Tandoi, E., and Haakstad, L. A. (2021). The weight of motherhood: identifying obesity, gestational weight gain and physical activity level of Italian pregnant women. Women's Health 17, 17455065211016136. doi:10.1177/17455065211016136
Cariati, I., Bonanni, R., Cifelli, P., D'Arcangelo, G., Padua, E., Annino, G., et al. (2025). Virtual reality and sports performance: a systematic review of randomized controlled trials exploring balance. Front. Sports Act. Living 7, 1497161. doi:10.3389/fspor.2025.1497161
Carraca, E. V., Markland, D., Silva, M. N., Coutinho, S. R., Vieira, P. N., Minderico, C. S., et al. (2012). Physical activity predicts changes in body image during obesity treatment in women. Med. and Sci. Sports and Exerc. 44 (8), 1604–1612. doi:10.1249/mss.0b013e31824d922a
Carraça, E. V., Encantado, J., Battista, F., Beaulieu, K., Blundell, J. E., Busetto, L., et al. (2021). Effect of exercise training on psychological outcomes in adults with overweight or obesity: a systematic review and meta-analysis. Obes. Rev. 22, e13261. doi:10.1111/obr.13261
Cash, T. F., and Smolak, L. (2011). Body image: a handbook of science, practice, and prevention. New York, NY: Guilford press.
Chang, Y.-C., and Yang, C.-C. (2024). Examining the mechanisms of virtual reality tourism’s impact on the mental well-being of long-term care facility residents: perspectives on presence and flow. Behav. Sci. 14 (9), 781. doi:10.3390/bs14090781
Cumillaf, A. G., Fuentes-Merino, P., Giakoni-Ramírez, F., Duclos-Bastías, D., Bruneau-Chávez, J., Merellano-Navarro, E., et al. (2025). Effects of a physical exercise program executed through immersive virtual reality on physical fitness and body composition in college adults: protocol for a randomized controlled trial. Retos 65, 356–366. doi:10.47197/retos.v65.112724
Czub, M., and Janeta, P. (2021). Exercise in virtual reality with a muscular avatar influences performance on a weightlifting exercise. Cyberpsychology J. Psychosoc. Res. Cybersp. 15 (3). doi:10.5817/cp2021-3-10
Dever, M., Skouteris, H., Incollingo Rodriguez, A. C., Hailu, H., Galvin, E., and Hill, B. (2025). Weight stigma in the preconception, pregnancy, and postpartum periods: a systematic review of women's perspectives. Obes. Rev. 26, e13891. doi:10.1111/obr.13891
Dong, Y., Faridniya, H., Ebrahimi, Z., and Zhao, Z. (2025). Gamified exercise in virtual reality: a novel intervention for enhancing mental health and reducing suicidal ideation in older adults. Healthcare.
Elbarazi, I., Lootah, S., Al Shamsi, F., Al Marzouqi, N., Al Matrooshi, M., Al Awadi, F., et al. (2024). Physicians’ attitudes towards obesity management in the primary care clinics in al-ain, United Arab Emirates: a qualitative study. Int. J. Healthc. Manag. 17 (4), 914–923. doi:10.1080/20479700.2023.2256551
Faria, S., Fonseca, S. M., Marques, A., and Queirós, C. (2025). Impact of a single virtual reality relaxation session on mental-health outcomes in frontline workers on duty during the COVID-19 pandemic: a preliminary study. Healthcare,
Finkelstein, S., Nickel, A., Lipps, Z., Barnes, T., Wartell, Z., and Suma, E. A. (2011). Astrojumper: motivating exercise with an immersive virtual reality exergame. Presence Teleoperators Virtual Environ. 20 (1), 78–92. doi:10.1162/pres_a_00036
Freeman, D., Rosebrock, L., Waite, F., Loe, B. S., Kabir, T., Petit, A., et al. (2023). Virtual reality (VR) therapy for patients with psychosis: satisfaction and side effects. Psychol. Med. 53 (10), 4373–4384. doi:10.1017/s0033291722001167
García-González, J., Verdejo-Herrero, A., Romero-del Rey, R., García-López, H., Obrero-Gaitán, E., Cortés-Pérez, I., et al. (2025). Perceptions of immersive virtual reality for physical activity among individuals with hypertension at risk of cardiovascular disease: a qualitative study. Healthcare,
Gómez-Ambrosi, J., Catalán, V., and Frühbeck, G. (2025). The evolution of the understanding of obesity over the last 100 years. Int. J. Obes. 49 (2), 168–176. doi:10.1038/s41366-024-01668-3
Han, D.-I. D., and tom Dieck, M. C. (2019). Calling for user-centric VR design research in hospitality and tourism. Hosp. and Soc. 9 (2), 237–246. doi:10.1386/hosp.9.2.237_7
Hart, E. A., Leary, M. R., and Rejeski, W. J. (1989). Social physique anxiety scale. J. Sport and Exerc. Psychol. doi:10.1123/jsep.11.1.94
Horizon Grand View Research (2025). Sports tourism market size & outlook, 2030. Available online at: https://www.grandviewresearch.com/horizon/outlook/sports-tourism-market-size/global.
Jingili, N., Oyelere, S. S., Nyström, M. B., and Anyshchenko, L. (2023). A systematic review on the efficacy of virtual reality and gamification interventions for managing anxiety and depression. Front. digital health 5, 1239435. doi:10.3389/fdgth.2023.1239435
Johnson, D., Deterding, S., Kuhn, K.-A., Staneva, A., Stoyanov, S., and Hides, L. (2016). Gamification for health and wellbeing: a systematic review of the literature. Internet interv. 6, 89–106. doi:10.1016/j.invent.2016.10.002
Kang, X., Zhang, Y., Sun, C., Zhang, J., Che, Z., Zang, J., et al. (2025). Effectiveness of virtual reality training in improving outcomes for dialysis patients: systematic review and meta-analysis. J. Med. Internet Res. 27, e58384. doi:10.2196/58384
Kaplan, S. C. (2020). Body mass index and social anxiety: effects of implicit weight bias and body salience in undergraduate women. Philadelphia, PA: Temple University.
Khan, A., Ezeugwa, J., and Ezeugwu, V. E. (2024). A systematic review of the associations between sedentary behavior, physical inactivity, and non-motor symptoms of Parkinson’s disease. Plos one 19 (3), e0293382. doi:10.1371/journal.pone.0293382
Koivisto, J., and Hamari, J. (2019). The rise of motivational information systems: a review of gamification research. Int. J. Inf. Manag. 45, 191–210. doi:10.1016/j.ijinfomgt.2018.10.013
Kroon, R., Neumann, D. L., Piatkowski, T. M., and Moffitt, R. L. (2023). How the physical appearance of companions affects females with high or low social physique anxiety: a virtual reality exercise study. Virtual Real. 27 (2), 541–551. doi:10.1007/s10055-022-00676-w
Levy, D., Friedman, D., de la Campa Crespo, E. Á., Spanlang, B., and Slater, M. (2025). Self-conversation with a sporting celebrity enhances later physical exercise: an exploratory study. Virtual Real. 29 (3), 100–115. doi:10.1007/s10055-025-01154-9
Lipták, Z. M., and Tarkó, K. (2021). Leisure and tourism in the health concept of women and their health misconceptions.
Liu-Lastres, B., and Cahyanto, I. (2021). Building a resilient event industry: lessons learned during the COVID-19 pandemic.
Mattick, R. P., and Clarke, J. C. (1998). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety11Editor’s note: this article was written before the development of some contemporary measures of social phobia, such as the Social Phobia and Anxiety Inventory (Turner et al., 1989). We have invited this article for publication because of the growing interest in the scales described therein. S.T. Behav. Res. Ther. 36 (4), 455–470. doi:10.1016/s0005-7967(97)10031-6
Mazeas, A., Duclos, M., Pereira, B., and Chalabaev, A. (2022). Evaluating the effectiveness of gamification on physical activity: systematic review and meta-analysis of randomized controlled trials. J. Med. Internet Res. 24 (1), e26779. doi:10.2196/26779
Mikkelsen, K., Stojanovska, L., Polenakovic, M., Bosevski, M., and Apostolopoulos, V. (2017). Exercise and mental health. Maturitas 106, 48–56. doi:10.1016/j.maturitas.2017.09.003
Modlin, D., and Kuo, Y. T. (2020). The effects of using augmented reality in rehabilitation and recovery exercise on patients' outcomes and experiences: a systematic review. Front. Virtual Real. 6, 1641316. doi:10.3389/frvir.2025.1641316
Mouatt, B., Smith, A. E., Mellow, M. L., Parfitt, G., Smith, R. T., and Stanton, T. R. (2020). The use of virtual reality to influence motivation, affect, enjoyment, and engagement during exercise: a scoping review. Front. Virtual Real. 1, 564664. doi:10.3389/frvir.2020.564664
Murphy, K., and Creux, O. (2021). Examining the association between media multitasking, and performance on working memory and inhibition tasks. Comput. Hum. Behav. 114, 106532. doi:10.1016/j.chb.2020.106532
Ng, M., Fleming, T., Robinson, M., Thomson, B., Graetz, N., Margono, C., et al. (2014). Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the global burden of disease study 2013. lancet 384 (9945), 766–781. doi:10.1016/s0140-6736(14)60460-8
Ng, M., Dai, X., Cogen, R. M., Abdelmasseh, M., Abdollahi, A., Abdullahi, A., et al. (2024). National-level and state-level prevalence of overweight and obesity among children, adolescents, and adults in the USA, 1990–2021, and forecasts up to 2050. lancet 404 (10469), 2278–2298. doi:10.1016/s0140-6736(24)01548-4
Poliani, A., Gnecchi, S., Villa, G., Rosa, D., and Manara, D. F. (2023). Gamification as an educational approach for oncological patients: a systematic scoping review. Healthcare,
Puhl, R. M., and Heuer, C. A. (2009). The stigma of obesity: a review and update. Obesity 17 (5), 941–964. doi:10.1038/oby.2008.636
Puhl, R., and Suh, Y. (2015). Health consequences of weight stigma: implications for obesity prevention and treatment. Curr. Obes. Rep. 4, 182–190. doi:10.1007/s13679-015-0153-z
Qian, F. (2022). Factors influencing female participation in sports tourism based on logistic model. Pac. Int. J. 5 (3), 31–40. doi:10.55014/pij.v5i3.190
Raghuram, N., Ram, V., Majumdar, V., Sk, R., Singh, A., Patil, S., et al. (2021). Effectiveness of a yoga-based lifestyle protocol (YLP) in preventing diabetes in a high-risk Indian cohort: a multicenter cluster-randomized controlled trial (NMB-Trial). Front. Endocrinol. 12, 664657. doi:10.3389/fendo.2021.664657
Rebar, A. L., Stanton, R., Geard, D., Short, C., Duncan, M. J., and Vandelanotte, C. (2015). A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 9 (3), 366–378. doi:10.1080/17437199.2015.1022901
Romano, K. A., Heron, K. E., Sandoval, C. M., Howard, L. M., MacIntyre, R. I., and Mason, T. B. (2022). A meta-analysis of associations between weight bias internalization and conceptually-related correlates: a step towards improving construct validity. Clin. Psychol. Rev. 92, 102127. doi:10.1016/j.cpr.2022.102127
Sandoz, E. K., Wilson, K. G., Merwin, R. M., and Kellum, K. K. (2013). Assessment of body image flexibility: the body image-acceptance and action questionnaire. J. Contextual Behav. Sci. 2 (1-2), 39–48. doi:10.1016/j.jcbs.2013.03.002
Santonja-Ayuso, L., Andreu-Pejó, L., and Carmona-Simarro, J. V. (2025). Working on mental health stigma in education: a multicentre community-based clinical trial. Front. Public Health 13, 1515444. doi:10.3389/fpubh.2025.1515444
Schuch, F. B., and Vancampfort, D. (2021). Physical activity, exercise, and mental disorders: it is time to move on. Trends psychiatry psychotherapy 43 (3), 177–184. doi:10.47626/2237-6089-2021-0237
Song, H., Ge, S., Wang, Y., Ran, L., and Zhang, H. (2025). Aerobic exercise strategies for anxiety and depression among children and adolescents: a systematic review and meta-analysis. Front. Public Health 13, 1555029. doi:10.3389/fpubh.2025.1555029
Staiano, A. E., Marker, A. M., Beyl, R. A., Hsia, D. S., Katzmarzyk, P. T., and Newton, R. (2017). A randomized controlled trial of dance exergaming for exercise training in overweight and Obese adolescent girls. Pediatr. Obes. 12 (2), 120–128. doi:10.1111/ijpo.12117
Tatnell, P., Atorkey, P., and Tzelepis, F. (2022). The effectiveness of virtual reality interventions on smoking, nutrition, alcohol, physical activity and/or obesity risk factors: a systematic review. Int. J. Environ. Res. public health 19 (17), 10821. doi:10.3390/ijerph191710821
Thomas, A. S., Varghese, J. S., Abraham, N. M., Mathews, N. B., and Rajan, M. P. (2020). Body image and social interaction anxiety among undergraduate students. Int. J. Eng. Technol. Manag. Sci. 6 (5), 516–522. doi:10.46647/ijetms.2022.v06i05.080
Tomiyama, A. J., Carr, D., Granberg, E. M., Major, B., Robinson, E., Sutin, A. R., et al. (2018). How and why weight stigma drives the obesity ‘epidemic’and harms health. BMC Med. 16, 123–126. doi:10.1186/s12916-018-1116-5
Touloudi, E., Hassandra, M., Galanis, E., Pinnas, G., Krommidas, C., Goudas, M., et al. (2025). Effectiveness and acceptance of virtual reality vs. traditional exercise in obese adults: a pilot randomized trial. Front. Sports Act. Living 7, 1520068. doi:10.3389/fspor.2025.1520068
Tylka, T. L., and Wood-Barcalow, N. L. (2015). The body appreciation Scale-2: item refinement and psychometric evaluation. Body image 12, 53–67. doi:10.1016/j.bodyim.2014.09.006
Vartanian, L. R., and Novak, S. A. (2011). Internalized societal attitudes moderate the impact of weight stigma on avoidance of exercise. Obesity 19 (4), 757–762. doi:10.1038/oby.2010.234
Villareal, D. T., Aguirre, L., Gurney, A. B., Waters, D. L., Sinacore, D. R., Colombo, E., et al. (2017). Aerobic or resistance exercise, or both, in dieting obese older adults. N. Engl. J. Med. 376 (20), 1943–1955. doi:10.1056/nejmoa1616338
Wang, X., Zhou, Q., Zhang, M., and Zhang, Q. (2021). Exercise in the park or gym? The physiological and mental responses of obese people walking in different settings at different speeds: a parallel group randomized trial. Front. Psychol. 12, 728826. doi:10.3389/fpsyg.2021.728826
Wang, L., Faridniya, H., and Yu, H. (2025). A public health perspective on virtual reality interventions: exploring the impact of VR extreme sports on stress, anxiety, and depression in men with social anxiety disorder. Front. Public Health 13, 1617483. doi:10.3389/fpubh.2025.1617483
Wechsler, T. F., Kümpers, F., and Mühlberger, A. (2019). Inferiority or even superiority of virtual reality exposure therapy in phobias? A systematic review and quantitative meta-analysis on randomized controlled trials specifically comparing the efficacy of virtual reality exposure to gold standard in vivo exposure in agoraphobia, specific phobia, and social phobia. Front. Psychol. 10, 1758. doi:10.3389/fpsyg.2019.01758
Wewege, M., Van Den Berg, R., Ward, R., and Keech, A. (2017). The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: a systematic review and meta-analysis. Obes. Rev. 18 (6), 635–646. doi:10.1111/obr.12532
Yao, Z., Tchang, B. G., Albert, M., Blumenthal, R. S., Nasir, K., and Blaha, M. J. (2025). Associations between class I, II, or III obesity and health outcomes. NEJM Evid. 4 (4), EVIDoa2400229. doi:10.1056/evidoa2400229
Zhang, Y., and Tsai, S.-B. (2021). Application of adaptive virtual reality with AI-Enabled techniques in modern sports training. Mob. Inf. Syst. 2021 (1), 1–10. doi:10.1155/2021/6067678
Zhang, Y., Guo, Z., Liu, Y., Zhou, Y., and Jing, L. (2024a). Is dancing an effective intervention for fat loss? A systematic review and meta-analysis of dance interventions on body composition. Plos one 19 (1), e0296089. doi:10.1371/journal.pone.0296089
Keywords: virtual reality, body image, sport management, social engagement, overweight women, social anxiety, sports tourism
Citation: Faridniya H and George R (2025) Gamified virtual exercise as a strategic management tool to foster inclusivity in women’s wellbeing and sports tourism. Front. Virtual Real. 6:1672764. doi: 10.3389/frvir.2025.1672764
Received: 24 July 2025; Accepted: 03 October 2025;
Published: 15 October 2025.
Edited by:
Joao Victor Esteves, The Ohio State University, United StatesReviewed by:
Beatrix Faragó, University of Sopron, HungaryTimothy John Pattiasina, Institut Informatika Indonesia, Indonesia
Copyright © 2025 Faridniya and George. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Reena George, cmdlb3JnZUBhbWl0eXVuaXZlcnNpdHkuYWU=