 Mohammad Khursheed Alam
Mohammad Khursheed Alam Ahmed Ali Alfawzan
Ahmed Ali Alfawzan- 1Orthodontic Division, Department of Preventive Dental Science, College of Dentistry, Jouf University, Sakaka, Saudi Arabia
- 2Department of Preventive Dentistry, College of Dentistry in Ar Rass, Qassim University, Ar Rass, Saudi Arabia
Objective: The objective of this study was to compare the novel artificial intelligence (A.I.)-driven lateral cephalometric (Late. Ceph.) analysis of 14 different dental characteristics (DC) among different types of cleft lip and palate (CLP) and non-cleft (NC) individuals.
Materials and Methods: A retrospective study was conducted on 123 individuals [31 = NC, 29 = BCLP (bilateral cleft lip and palate), 41 = UCLP (unilateral cleft lip and palate), 9 = UCLA (unilateral cleft lip and alveolus), and 13 = UCL (unilateral cleft lip)] with an average age of 14.77 years. Demographic details were gathered from the clinical records. A novel artificial intelligence-driven Webceph software has been used for the Late. Ceph. analysis. A total of 14 different types of angular and linear DC measurements were analyzed and compared among groups. Two-way ANOVA and multiple-comparison statistics tests were applied to see the differences between gender and among different types of CLP versus NC subjects.
Results: Of the 14 DC tested, no significant gender disparities were found (p > 0.05). In relation to different types of CLP versus NC subjects, 8 over 14 DC were statistically significant (p < 001 to p = 0.03). Six other DC variables show insignificant (p > 0.05) noteworthy alterations in relation to type of CLP.
Conclusion: Based on the results, type of CLP revealed significantly altered DC compared to NC. Among different types of CLP, BCLP exhibited a maximum alteration in different DC.
Introduction
Any deformations (anatomical or chromosomal) that start during pregnancy and their belongings identified after birth are considered intrinsic oddities (Sekhon et al., 2011). Among them, cleft lip and palate (CLP) is one of the most widely recognized and major inherent craniofacial peculiarities in humans, brought about by strange facial development during embryogenesis that presents during childbirth and portrayed by halfway or complete clefting of the upper lip, with or without clefting of the alveolar edge or the hard or soft palate (Erverdi and Motro, 2015). Cleft can happen along with CLP or independently like a detached cleft lip and or isolated cleft palate. The point when cleft lip and palate emerge together is named as CLP. The highlights of CLP went from the least serious to the most extreme structure with a unilateral or bilateral manner. CLP can be syndromic or non-syndromic. Clinically, when CLP shows up with other deformities (normally at least two or more), for an inconspicuous example, it is delegated syndromic CLP. In the event that it shows up as a secluded deformity or if the disorder cannot be recognized, the term non-syndromic CLP (NSCLP) is utilized (Kohli and Kohli, 2012).
The etiology of CLP is still controversial. According to previous studies, it is to be thought that both genetic and environmental factors are responsible for CLP (Alam et al., 2012; Berkowitz, 2013; Haque et al., 2015; Haque and Alam, 2015a, c). Studies of the etiology of non-syndromic clefts pivot on candidate genes associated with craniofacial development, genes influenced by environmental teratogens or deficiencies, and genes associated with syndromic clefts (Murray, 2002; Haque et al., 2015). CLP shows significant heterogeneity among different ethnic groups.
Numerous strategies for the evaluation of the craniofacial characteristics, dental relationship, and maxillary morphometry measurement of CLP individuals have been depicted already (Alam et al., 2008, 2013, 2019; Kajii et al., 2013; Asif et al., 2016; Arshad et al., 2017a, b, 2018; Haque et al., 2017a, b, 2018). The result of the craniofacial characteristics of CLP can be evaluated from multifacets of factors, for example, dental relationship (Haque et al., 2018), cephalogram (Alam et al., 2013, 2019; Wu et al., 2013; Batwa et al., 2018; Alam and Alfawzan, 2020), cone-beam computed tomography (Parveen et al., 2018), and maxillary morphometry (Haque et al., 2020). Oral clefts show an assortment of clinical inconsistencies (Batwa et al., 2018). Lee et al. (2020) and Kunz et al. (2020) uncovered artificial intelligence (A.I.) into dentistry, particularly in orthodontics ready to break down obscure Late. Ceph. at nearly a similar quality level as the ongoing highest-quality level estimated by a calibrated specialist. Lee et al. (2020) used A.I.-driven profound convolutional neural system-based assessment of Late. Ceph. for the sign of orthognathic surgery cases of differential determination and discovered 95.6% exactness.
This first-in-human study in a Saudi Arabian population, among different types of NSCLP and NC individuals, is yet to be investigated in regard to different dental characteristics (DC). Hence, in the present study an attempt is made to contribute a novel A.I.-driven analysis of different DC in multiple types of NSCLP and to compare the findings with gender- and age-matched NC individuals. Hence, this study aimed to investigate (1) how the DC are different among gender, (2) how the disparities in DC exist in multiple types of NSCLP and NC individuals, and (3) how the disparities exist in gender times multiple types of NSCLP and NC individuals. The hypothesis of this study is as follows: types of DC are different in relation to gender, type of NSCLP, and NC subjects.
Materials and Methods
All the records (clinical and demographic details, X-rays) were collected from Saudi Board of dental residents. The research protocol was arranged by one calibrated orthodontist, and the data was stored. The research protocol was presented to the Ethical Committee of Al rass Dental Research Center, Qassim University. Full Ethical approval was obtained with the code #: DRC/009FA/20. The following inclusion and exclusion criteria are followed, non-syndromic cleft subjects with good-quality x-ray images. There was no history of craniofacial surgical treatment besides cleft lip and palate surgery. No orthodontic treatment was done. A match with healthy control without any craniofacial deformity was found.
Digital Late. Ceph. X-rays were used to investigate 14 different DC of 123 NC and cleft subjects based on convenient sampling following inclusion and exclusion criteria. Among them, 31 NC subjects and 92 cleft subjects [29 had BCLP (bilateral cleft lip and palate), 41 had UCLP (unilateral cleft lip and palate), 9 had UCLA (unilateral cleft lip and alveolus), and 13 had UCL (unilateral cleft lip)]. According to gender, male = 14 NC + 19 BCLP + 26 UCLP + 3 UCLA + 7 UCL and female = 17 NC + 10 BCLP + 15 UCLP + 6 UCLA + 6 UCL. Ages of the subjects were 13.29 ± 3.52 NC, 14.07 ± 4.73 BCLP, 14.32 ± 4.46 UCLP, 12.78 ± 4.09 UCLA, and 13.31 ± 4.46 UCL. In this retrospective study, clinical and radiographic details were used. Fourteen (14) different DC were measured by one examiner using automated A.I.-driven Webceph software (South Korea). The angular and linear measurements used in this study are detailed in Table 1 and Figure 1.
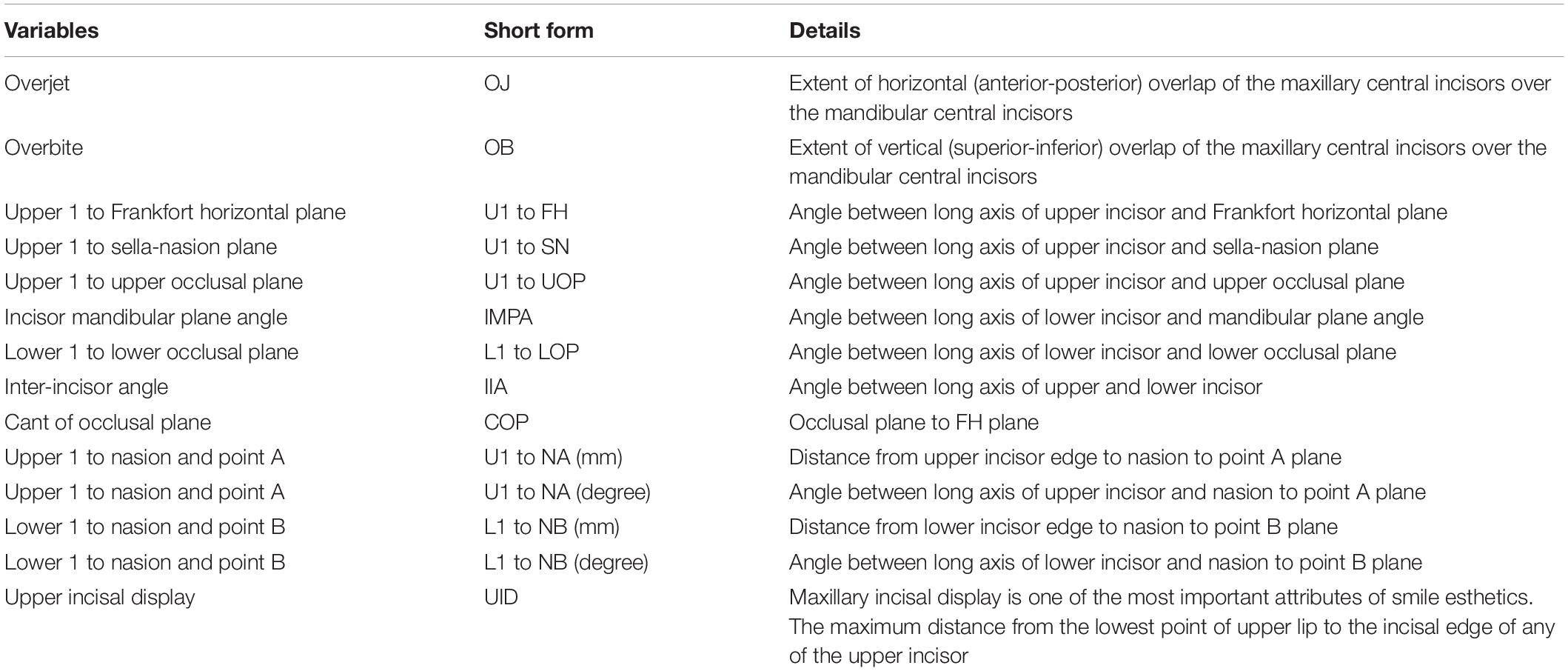
Table 1. Dental characteristic measured in NSCLP and NC individuals.
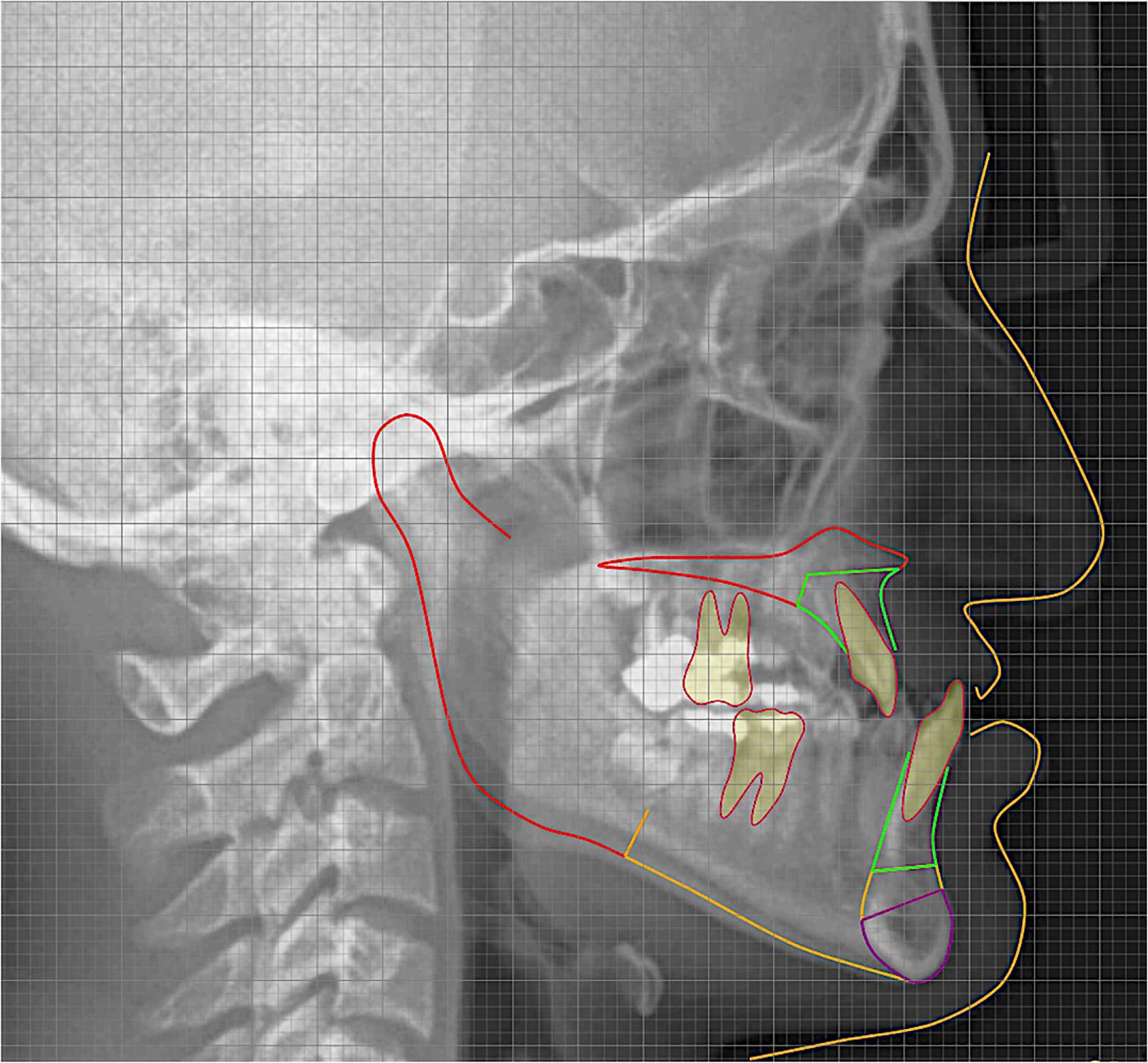
Figure 1. Artificial intelligence-driven lateral cephalometric analysis.
Statistical Analyses
To survey the estimation mistake, 20 Late. Ceph. cases were arbitrarily chosen and the means of A.I.-driven investigation were rehashed by one analyst following 2 weeks of first examination. Intra-class correlation coefficients were performed to evaluate the unwavering quality for the two arrangements of estimations. The estimations of coefficients of unwavering quality were seen as more prominent than 0.95 and 0.91 for all linear and angular variables, respectively. Data were analyzed in SPSS (SPSS Inc., Chicago, IL, United States). The Kolmogorov–Smirnov test was utilized to check the normality of the estimations. A two-way ANOVA examination was utilized for gender orientation, types of cleft and gender∗types of cleft. A p-esteem < 0.05 was considered as significant statistically.
Results
Tables 2–8 show the details of the analyzed results of 14 different DC among gender, types of cleft and gender∗types of cleft. Figures 2A–C show the profile plot of estimated marginal means of types of cleft and gender∗types of cleft.
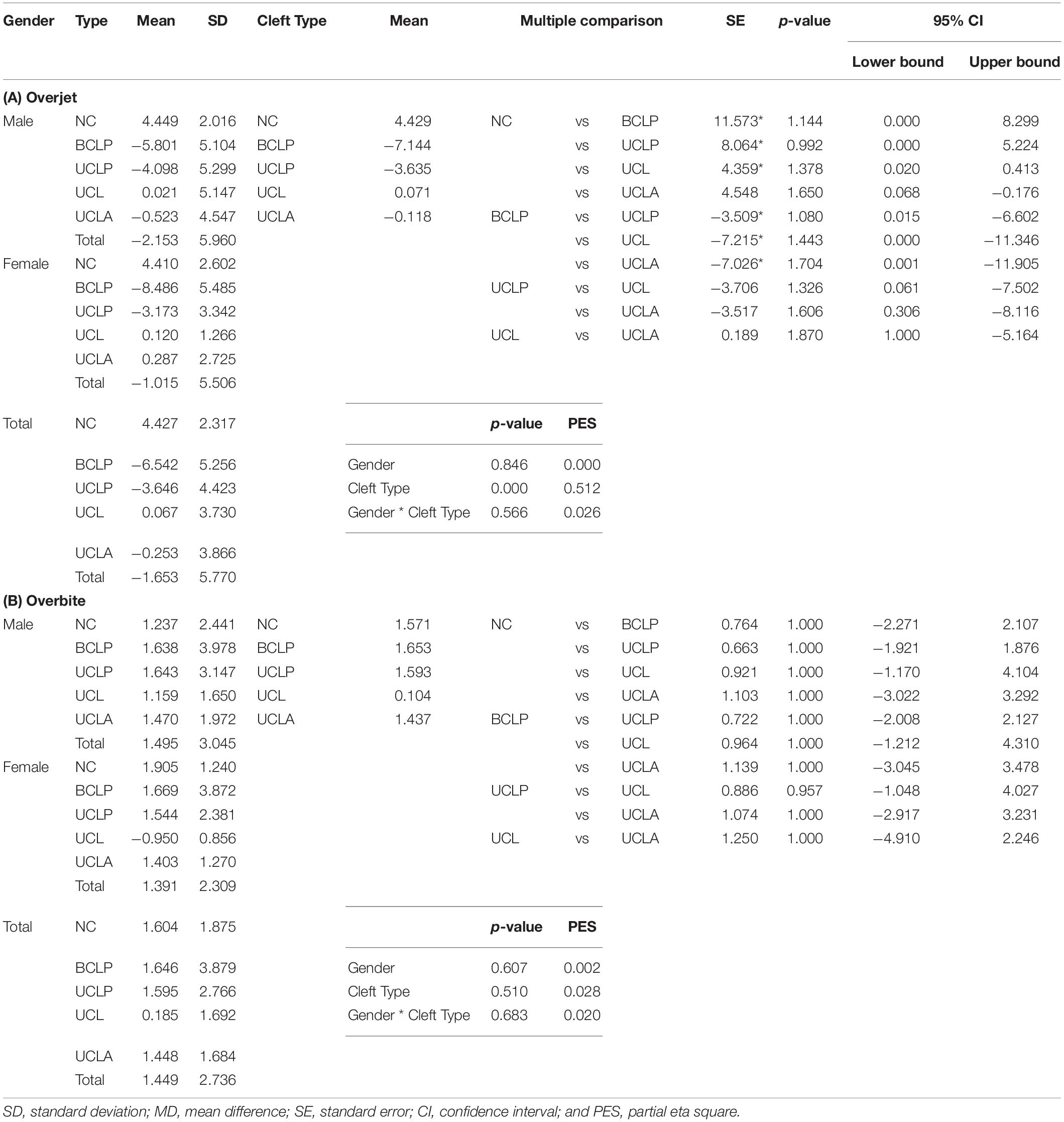
Table 2. Dental characteristics – (A) Overjet and (B) Overbite: Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
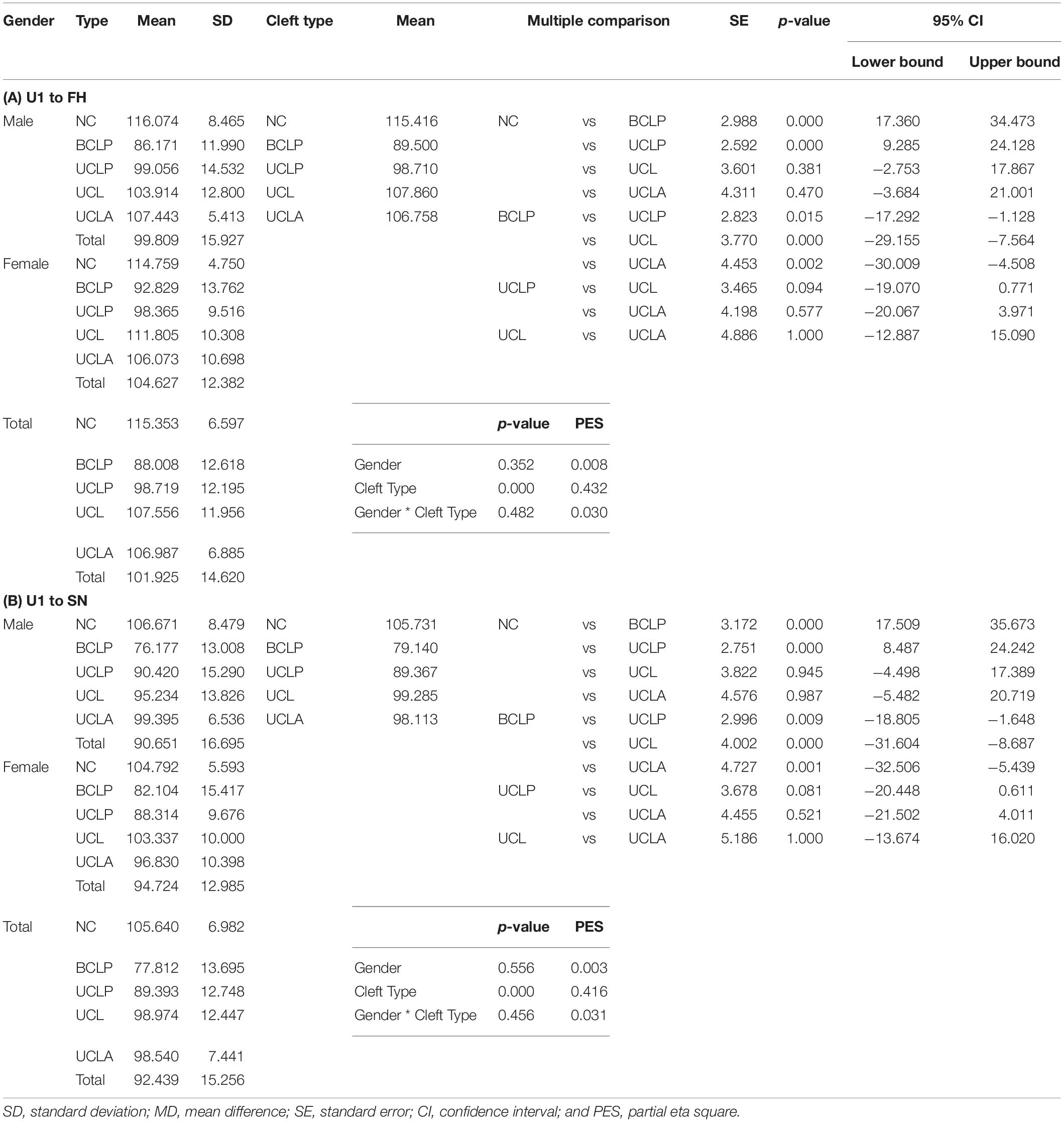
Table 3. Dental characteristics – (A) U1 to FH and (B) U1 to SN: Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
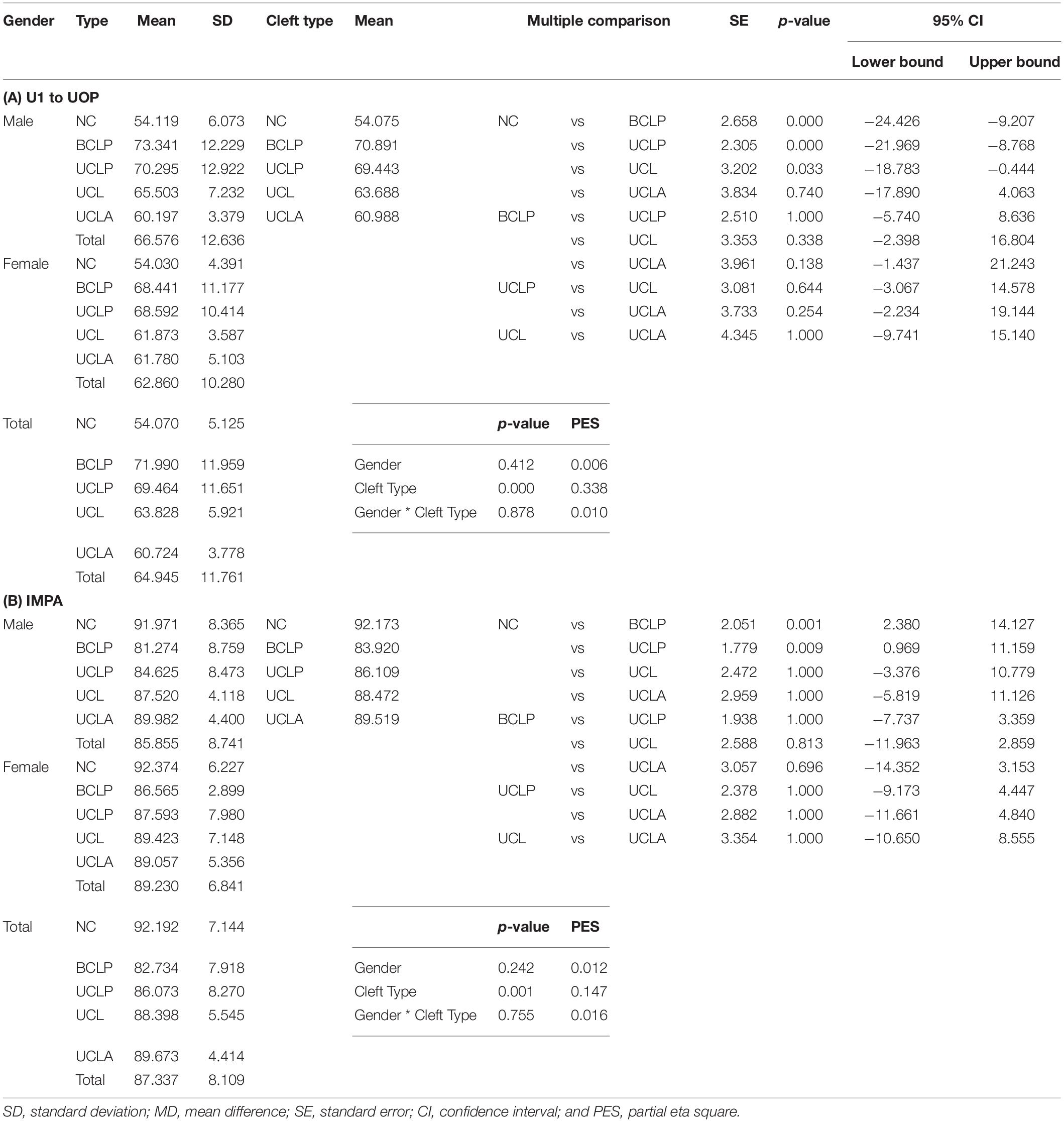
Table 4. Dental characteristics – (A) U1 to UOP and (B) IMPA: Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
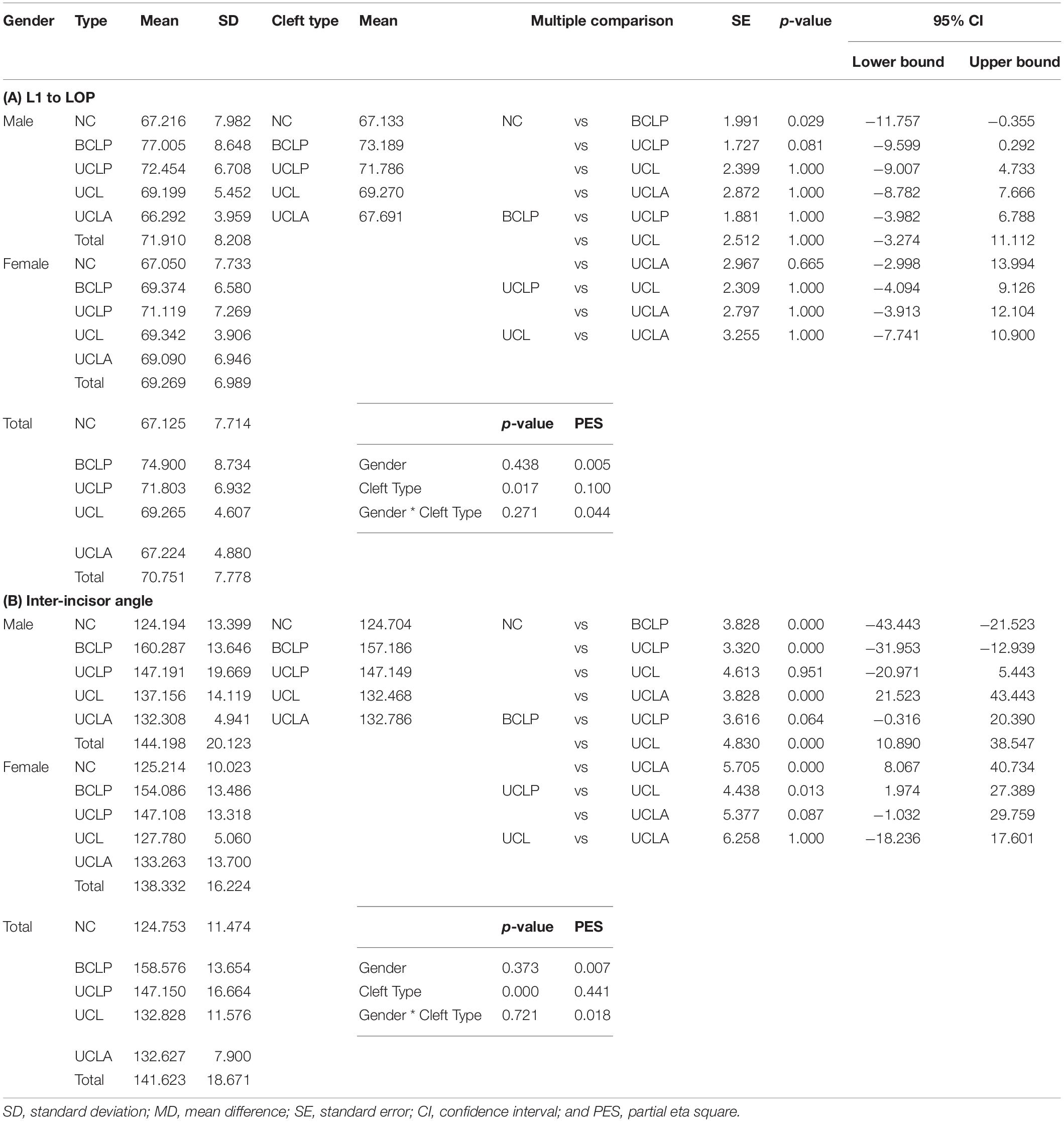
Table 5. Dental characteristics – (A) L1 to LOP and (B) inter-incisor angle: Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
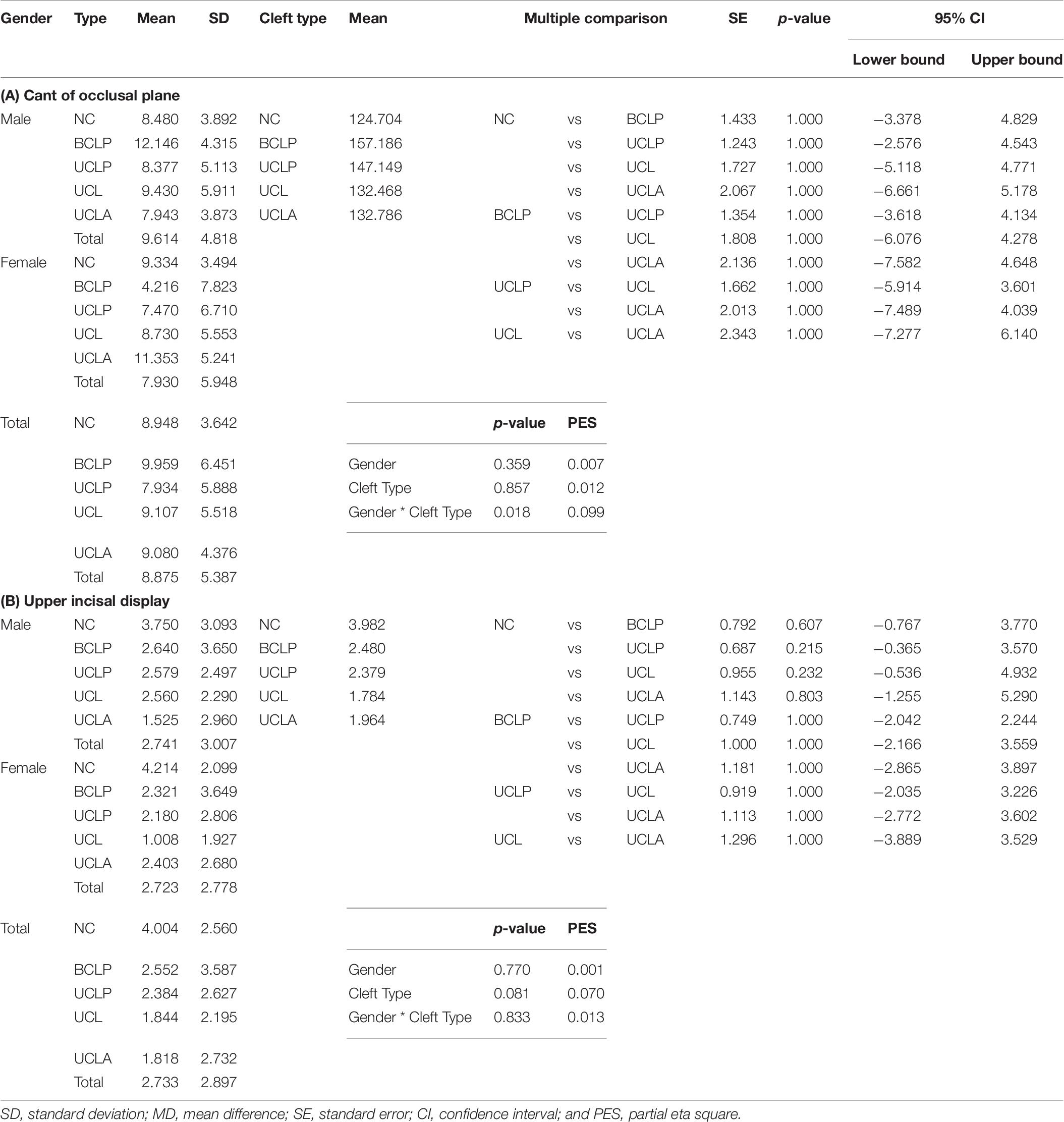
Table 6. Dental characteristics – (A) Cant of occlusal plane and (B) Upper incisal display: Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
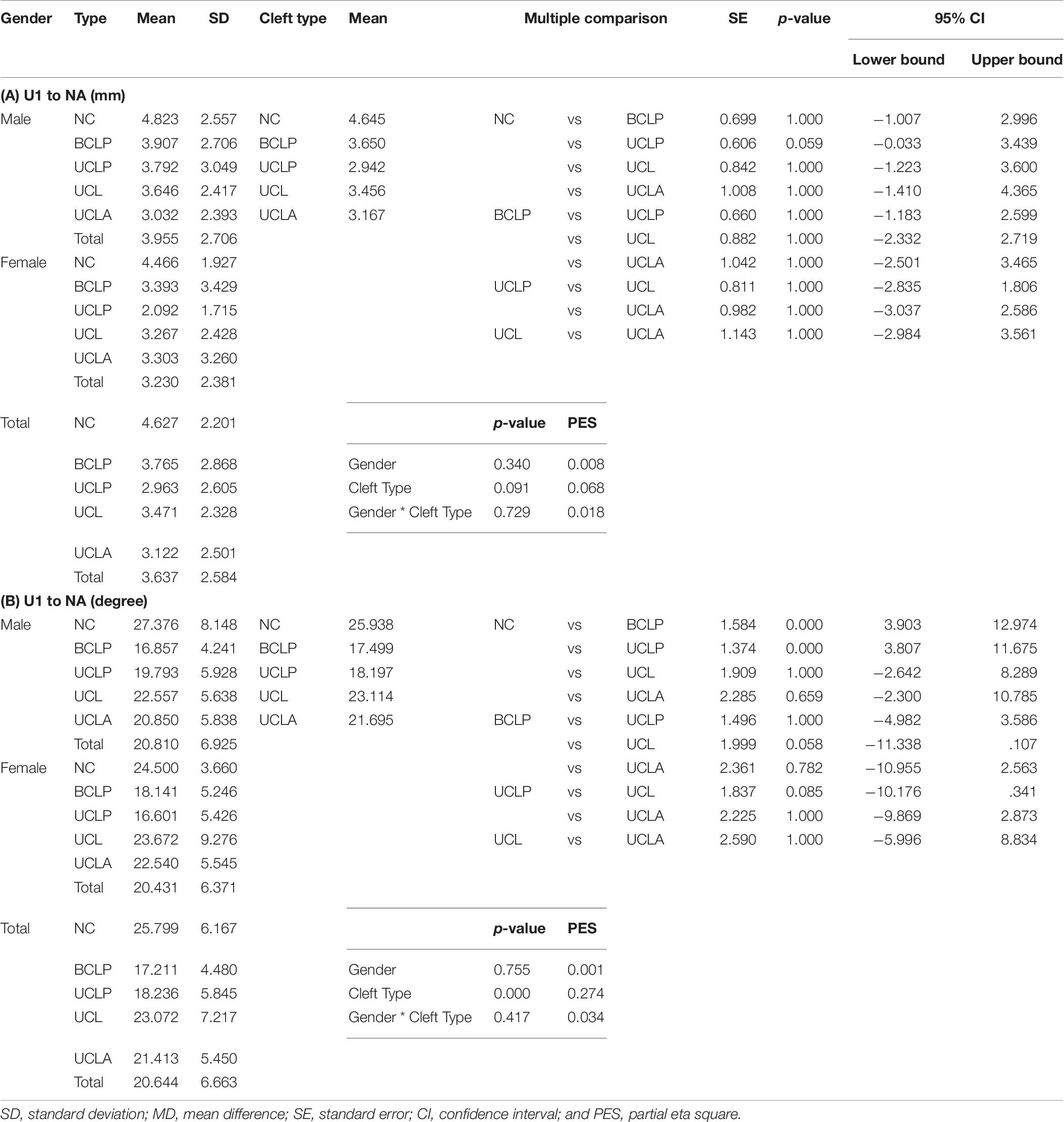
Table 7. Dental characteristics – (A) U1 to NA (mm) and (B) U1 to NA (degree): Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
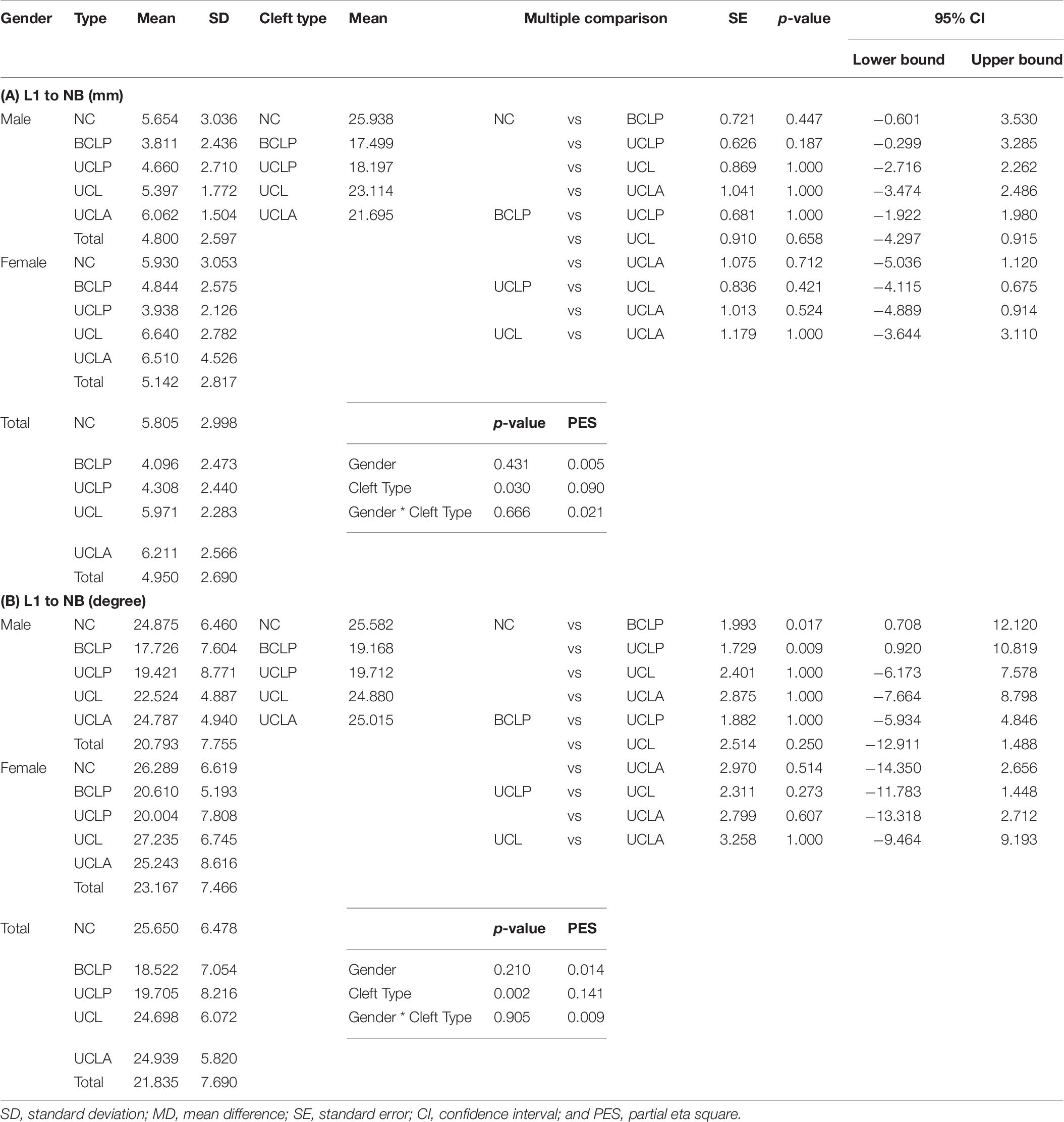
Table 8. Dental characteristics – (A) L1 to NB (mm) and (B) L1 to NB (degree): Gender, types of cleft and gender times types of cleft two-way ANOVA analysis results.
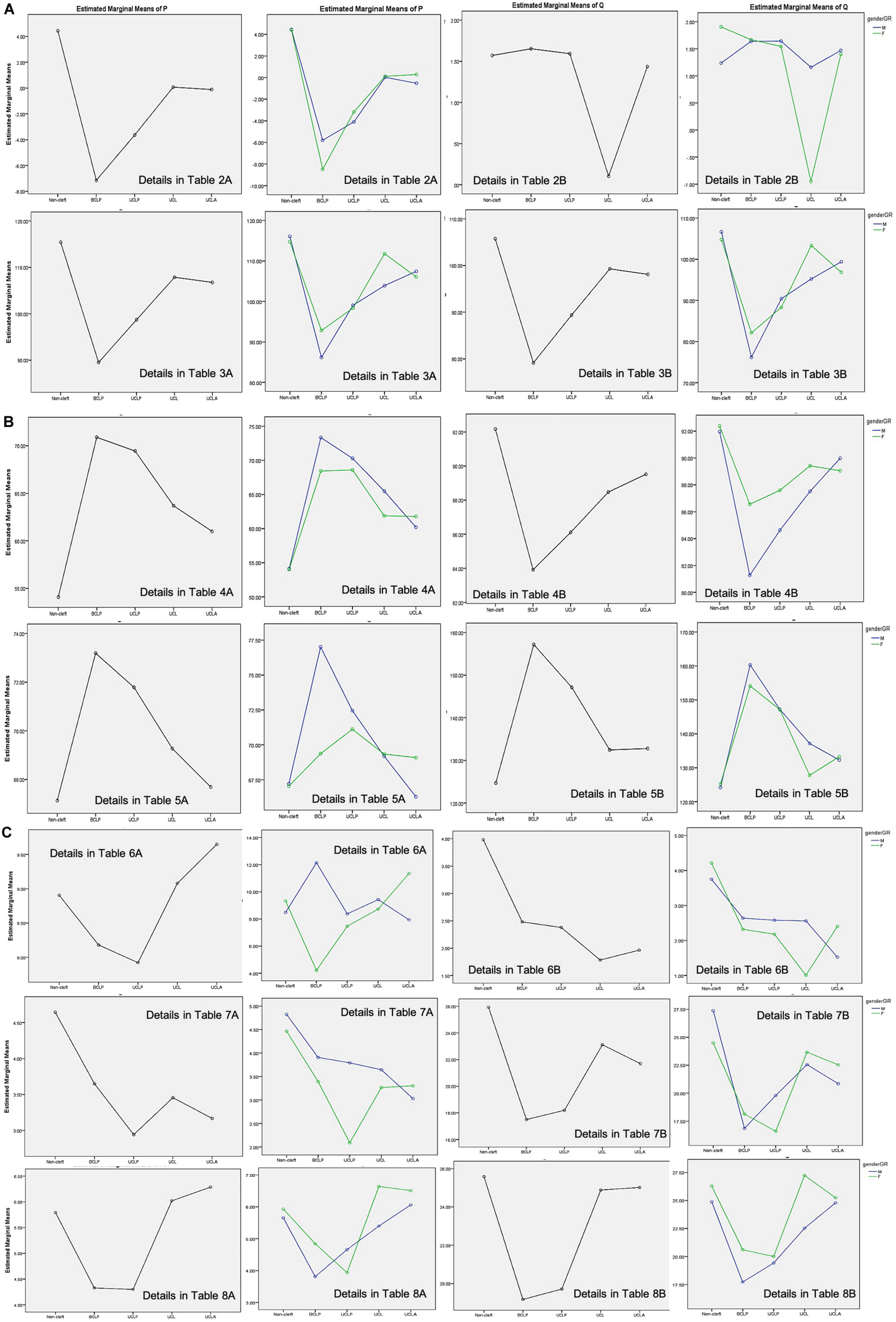
Figure 2. (A–C) Profile plot of the estimated marginal means of types of cleft and gender∗types of cleft.
In Table 2A, overjet DC is presented, which shows no significant gender disparities and highly significant disparities among NC and different types of clefts (BCLP p < 0.001, UCLP p < 0.001 and UCL, p = 0.020). UCLP p = 0.015, UCL p < 0.001, and UCLA, p = 0.001, showed a significant difference in comparison with BCLP. In relation to overbite DC, no significant disparities were observed (Table 2B).
Tables 3A,B shows U1 to FH and U1 to SN DC with no significant gender disparities and highly significant disparities among NC and different types of clefts (BCLP p < 0.001 and UCLP p < 0.001) in comparison with NC. UCLP p = 0.015, UCL p < 0.001, and UCLA, p = 0.002, showed significant difference in comparison with BCLP in relation to U1 to FH DC. Moreover, UCLP p = 0.009, UCL p < 0.001, and UCLA, p = 0.001, showed a significant difference in comparison with BCLP in relation to U1 to SN DC.
Tables 4A,B shows U1 to UOP and IMPA DC with significant disparities among NC and different types of clefts (BCLP < 0.001 and p = 0.001 and UCLP < 0.001 and p = 0.009, respectively).
In relation to L1 to LOP DC, no significant disparities were observed (Table 5A). Table 5B shows inter-incisor angle DC with highly significant disparities among NC and different types of clefts (BCLP < 0.001, UCLP < 0.001, and UCLA < 0.001). UCL < 0.001 and UCLA < 0.001 showed a significant difference in comparison with BCLP. UCL p = 0.03 showed a significant difference in comparison with UCLP.
In relation to Cant of occlusal plane, upper incisal display DC, and U1 to NA (mm), no significant disparities were observed (Tables 6A,B, 7A). Table 7B shows U1 to NA (degree) DC with significant disparities among NC and different types of clefts (BCLP p = 0.001 and UCLP p = 0.009).
Table 8A shows L1 to NB (mm) DC, no significant disparities were observed. L1 to NB (degree) DC show significant disparities among NC and different types of clefts (BCLP p = 0.017 and UCLP p = 0.009) (Table 8B).
Discussion
Fourteen (14) distinctive DC of five unique groups of individuals are researched in the present study. As far as we could possibly know, A.I.-driven computerized Late. Ceph. examination in such gatherings and populace is yet to be researched. Irrelevant mistake in the estimations; exact, automated, basic, brisk, savvy, future orthodontic computerized apparatuses; and different types of cleft examples are the novelty of the current examination (Lee et al., 2020; Kunz et al., 2020). The current investigation results may help the clinician in approaching where the impacts of essential CLP medical procedures are on various DC, supporting the restoration procedure in subjects with various sorts of NSCLP in building up a positive administration convention.
Batwa et al. (2018) recommended broadly that analysts in the CLP field should embrace exhaustive activities to survey a wide range of CLP. Longitudinal and extensive examination studies will empower social insurance suppliers to actualize substantial treatment conventions that are suitable for the extraordinary nature and intricacy of the CLP populace. The unilateral complete type of CLP subjects with multiple missing teeth had the significantly smallest overjet (–3.89 ± 2.75 mm) among the three groups (without missing teeth, with only one missing tooth, and with two or more missing teeth). In the current study, overjet in NC = 4.429, BCLP = −7.144, UCLP = −3.635, UCL = 0.071, and UCLA = −0.118 exhibits significant disparities. Maximum alterations are found in the BCLP group. UCLP results almost coincide with the results of Batwa et al. (2018) in which the smallest overjet was found in the unilateral complete type of CLP subjects with multiple missing teeth.
These disparities may be due to multiple-factor relations. When a patient is born with CLP, a number of surgeries take place in the 1st 2 years of life. One study used the presurgical orthopedic feeding plate after birth (Haque and Alam, 2015b); at 3–6 months of age, the patients underwent cheiloplasty (Haque and Alam, 2014), and at 9–18 months of age they underwent palatoplasty (Haque and Alam, 2015c). There was a formation of excessive scar tissues, and the undermining of soft tissue was observed after these surgeries, which may have resulted in maxillary contracture which finally leads to class III malocclusion. Maxillary growth retardation is often observed in patients with repaired unilateral cleft lip and palate (UCLP) (Alam et al., 2008; Kajii et al., 2013). Altered craniofacial morphology was also observed in relation to postnatal treatment factors and congenital factors in the Japanese population (Alam et al., 2013, 2019).
Wu et al. (2013) proposed that further investigations are expected to investigate the skeletal and dental attributes of individuals with CLP in other ethnic gatherings, especially in the Middle Eastern region. They assessed only individuals with unilateral complete CLP among various kinds of CLP. They found various cephalometric characteristics present in Taiwanese people with unilateral complete CLP and found a general decrease in their skeletal vertical measurements and a decrease in the overjet. The current study also revealed a significant alteration in overjet. However, overbite, which determines the vertical dental relationship, shows no significant alterations. Five other DC—L1 to LOP, Cant of occlusal plane, U1 to NA (mm), L1 to NB (mm), and upper incisal display DC—also showed no significant disparities among genders, types of CLP, and NC individuals.
Alam et al. (2019), Alam and Alfawzan (2020) investigated the craniofacial morphology of Japanese UCLP patients and investigated the association with congenital (2019) and postnatal treatment factors (2013). Among congenital factors, gender and DC (U1-SN) showed insignificant disparities, which coincide with the results of the present study. Among postnatal treatment factors, significantly larger U1-SN measurements are found in subjects that underwent preoperative orthopedic treatment with a Hotz plate in comparison with the subjects that underwent no preoperative orthopedic treatment (HOTZ plate) or an active plate. These investigations are researched in UCLP subjects only. The current study compared four types of NSCLP and NC individuals. These disparities may be due to the fact that the management protocol of a patient with cleft is complex and requires a lengthy procedure. The involvement of multi-specialties working in tandem is suggested to bring out physical, psychological, and social rehabilitation. Likewise, maxillary arch constriction (maxillary growth retardation) is a common dental problem of CLP patients, resulting in a concave facial profile (Alam et al., 2019), class III malocclusion (Alam et al., 2013), midfacial growth deficiency (Alam et al., 2013, 2019), and congenitally missing and malformed teeth. Orthodontic anomalies like crowding, rotation, and malposition of teeth are also commonly observed (Haque and Alam, 2015a; Haque et al., 2018; Adetayo et al., 2019). In the current study, maximum alterations in 8 different DC were found to be mostly altered in relation to upper incisors [U1-FH, U1-SN, U1-UOP, IIA, and U1-NA (degree)]. Our results clearly indicate that NSCLP subjects exhibit a class III malocclusion pattern based on investigated multiple DC. Also, the results are more prominent in BCLP individuals.
Batwa et al. (2018) found U1-SN values of 85.04 ± 12.13 and 91.63 ± 10.62 (mean ± SD) in the control and case groups (UCCLP), respectively. Utilizing the mean ± SD values of the two groups, the calculated Cohen’s d and effect-size r were 0.578 and 0.277, respectively. Sample power analysis was done using G∗Power software, and the effect size was calculated (Batwa et al., 2018). Based on this, the total sample in the five groups is required to be 103. In each group, 20 or 21 individuals are required with α err prob and power (1-β err prob) values of 0.05 and 80, respectively. Strict inclusion criteria were followed to recruit the data. A good number of BCLP and UCLP samples and age- and sex-matched NC individuals are recruited; however, the sample size of UCLA and UCL is lacking. To draw any strong conclusion in different CLP problems, a genetic investigation may play a beneficial role. Furthermore, genetic/congenital/postnatal treatment factors may influence or alter the shape/growth of the DC. Future studies involving effects of genetic/congenital/postnatal treatment factors along with a greater number of samples may be beneficial in drawing a strong conclusion. The current study cannot state whether comparative discoveries may have been obtained from different individuals with numerous sorts of NSCLP. It may be helpful to do this type of two-way ANOVA examination in bunches from different hospitals/clinics. Future investigations with bigger example sizes are justified.
Conclusion
• The current study investigated 14 different DC. Among 14 different DC, 8 variables showed a significant alteration among different types of NSCLP and NC individuals.
• No significant gender disparities were found in relation to types of different NSCLP and NC individuals.
• Among CLP, BCLP showed maximum alterations in different DC in relation to NC individuals as well as within other types of CLP individuals.
Data Availability Statement
All datasets presented in this study are included in the article/Supplementary Material.
Ethics Statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Al Rass Dental Research Center, Qassim University, Code #: DRC/009FA/20. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcell.2020.00789/full#supplementary-material
References
Adetayo, A. M., Adetayo, M. O., Adeyemo, W. L., James, O. O., and Adeyemi, M. O. (2019). Unilateral cleft lip: evaluation and comparison of treatment outcome with two surgical techniques based on qualitative (subject/guardian and professional) assessment. J. Korean Assoc. Oral. Maxillofac. Surg. 45, 141–151.
Alam, M. K., and Alfawzan, A. A. (2020). Evaluation of sella turcica bridging and morphology in different types of cleft patients. Front. Cell Dev. Biol. 8:656. doi: 10.3389/fcell.2020.00656
Alam, M. K., Iida, J., Sato, Y., and Kajii, T. S. (2013). Postnatal treatment factors affecting craniofacial morphology of unilateral cleft lip and palate (UCLP) patients in a Japanese population. Br. J. Oral. Maxillofac. Surg. 51, 205–210.
Alam, M. K., Kajii, T. S., and Iida, J. (2012). “Spectrum of factors affecting dental arch relationships in japanese unilateral cleft lip and palate patients,” in Orthodontics-Basic Aspects and Clinical Considerations ed. F. Bourzgui, (London: Intech Open). 13, 301–324.
Alam, M. K., Kajii, T. S., Matsuno, M. K., Kato, Y. S., and Iida, J. (2008). Multivariate analysis of factors affecting dental arch relationships in Japanese unilateral cleftlip and palate patients at Hokkaido University Hospital. Orthod. Waves. 67, 45–53. doi: 10.1016/j.odw.2007.12.001
Alam, M. K., Kajii, T. S., Sato, Y., and Iida, J. (2019). Clinical investigation of congenital factor affecting craniofacial morphology of unilateral cleft lip and palate in japanese patients. Pesqui Bra. Odontopediatria Clín. Integr. 19:4642.
Arshad, A. I., Alam, M. K., and Khamis, M. F. (2017a). Assessment of complete unilateral cleft lip and palate patients: determination of factors effecting dental arch relationships. Int. J. Paed. Otorihnolaryng. 92, 70–74. doi: 10.1016/j.ijporl.2016.11.006
Arshad, A. I., Alam, M. K., and Khamis, M. F. (2017b). Assessment of complete unilateral cleft lip and palate treatment outcome using EUROCRAN index and associated factors. Int. J. Paed. Otorihnolaryng. 100, 91–95. doi: 10.1016/j.ijporl.2017.06.025
Arshad, A. I., Alam, M. K., and Khamis, M. F. (2018). Dentoalveolar cleft treatment outcome using modified Huddart-Bodenham index and regression analysis of associated factors. Cleft. Palate. Craniofac. J. 55, 682–687. doi: 10.1177/1055665618758278
Asif, J. A., Alam, M. K., Haque, S., and Pohchi, A. (2016). Treatment outcome and factors affecting dental arch relationship in Malay children with unilateral cleft lip and palate (UCLP). J. Hard. Tissue Biolog. 25, 371–376. doi: 10.2485/jhtb.25.371
Batwa, W., Almarhoon, H. A., Almoammar, K. A., Alqahtani, N., Albarakati, S. F., and Al-Jewair, T. (2018). Dento-skeletal characteristics of cleft patients with missing teeth. Clin., Cosmet. Investig. Dent. 10, 237–244. doi: 10.2147/ccide.s170717
Erverdi, N., and Motro, M. eds (2015). “Cleft lip and palate treatment,” in, Alveolar Distraction Osteogenesis. Berlin: Springer, 7–17.
Haque, S., Alam, M. K., and Basri, R. (2015). Gene involvement in cleft lip and palate (CLP) patients. Bangladesh J. Med. Sci. 14, 113–116. doi: 10.3329/bjms.v14i1.20928
Haque, S., Alam, M. K., and Khamis, M. F. (2017a). Factors responsible for unfavorable dental arch relationship in non syndromic unilateral cleft lip and palate children. J. Clin. Pediatr. Dent. 41, 236–242. doi: 10.17796/1053-4628-41.3.236
Haque, S., Alam, M. K., and Khamis, M. F. (2017b). The effect of various factors on the dental arch relationship in non-syndromic unilateral cleft lip and palate children assessed by new approach: a retrospective study. BMC Pediatr. 17:119. doi: 10.1186/s12887-017-0870-4
Haque, S., Alam, M. K., and Khamis, M. F. (2018). Treatment outcome of Bangladeshi UCLP patients based on both phenotype and postnatal treatment factors using modified Huddart Bodenham (mHB) index. Cleft. Palate. Craniofac. J. 55, 966–973. doi: 10.1597/15-293
Haque, S., and Alam, M. K. (2014). Spectrum of cheiloplasty has detrimental effect on maxillary growth: myth or fact? Bangladesh J. Med. Sci. 13, 473–476. doi: 10.3329/bjms.v13i4.20653
Haque, S., and Alam, M. K. (2015a). Common dental anomalies in cleft lip and palate patients. Malaysian J. Med. Sci. 22, 55–60.
Haque, S., and Alam, M. K. (2015b). Pre-surgical orthopedic treatment using Hotz plate: an update. Int. J. Pharm. Bio. Sci. 6, 318–327.
Haque, S., and Alam, M. K. (2015c). Spectrum of palatoplasty has detrimental effect on: myth or fact? Bangladesh J. Med. Sci. 14, 109–110. doi: 10.3329/bjms.v14i1.20926
Haque, S., Khamis, M. F., Alam, M. K., and Ahmed, W. M. A. W. (2020). Effects of multiple factors on treatment outcome in the 3d maxillary arch morphometry of unilateral cleft lip and palate children. J. Craniofac. Surg. doi: 10.1097/SCS.0000000000006464 Online ahead of print
Kajii, T. S., Alam, M. K., Milkoya, T., Oyama, A., Matsuno, M. K., Kato, Y. S., et al. (2013). Congenital and postnatal factors including malocclusion in Japanese unilateral cleft lip and patient- determination using logistic regression analysis. Cleft. Palate. Craniofac. J. 50, 466–472. doi: 10.1597/11-150
Kohli, S. S., and Kohli, V. S. (2012). A comprehensive review of the genetic basis of cleft lip and palate. J. Oral. Maxillofac. Pathol. 16, 64–72.
Kunz, F., Stellzig-Eisenhauer, A., Zeman, F., and Boldt, J. (2020). Evaluation of a fully automated cephalometric analysis using a customized convolutional neural network. J. Orofac. Orthop. 81, 52–68. doi: 10.1007/s00056-019-00203-8
Lee, K. S., Ryu, J. J., Jang, H. S., Lee, D. Y., and Jung, S. K. (2020). Deep convolutional neural networks based analysis of cephalometric radiographs for differential diagnosis of orthognathic surgery indications. Appl. Sci. 10:2124. doi: 10.3390/app10062124
Murray, J. C. (2002). Gene/environment causes of cleft lip and/or palate. Clin. Genet. 61, 248–256. doi: 10.1034/j.1399-0004.2002.610402.x
Parveen, S., Shetty, R., Husain, A., Mascarenhas, R., D’Souza, N., and Shetty, N. K. (2018). Three-dimensional assessment of alveolar bone thickness in individuals with nonsyndromic unilateral complete cleft lip and palate. J. Cleft Lip Palate Craniofac. Anomal. 5, 106–112. doi: 10.4103/jclpca.jclpca_11_18
Sekhon, P. S., Ethunandan, M., Markus, A. F., Krishnan, G., and Rao, C. B. (2011). Congenital anomalies associated with cleft lip and palate-an analysis of 1623 consecutive patients. Cleft. Palate. Craniofac. J. 48, 371–378. doi: 10.1597/09-264
Keywords: non-syndromic cleft lip and palate, bilateral cleft lip and palate, unilateral cleft lip and palate, dental characteristics, overjet, overbite, incisal display
Citation: Alam MK and Alfawzan AA (2020) Dental Characteristics of Different Types of Cleft and Non-cleft Individuals. Front. Cell Dev. Biol. 8:789. doi: 10.3389/fcell.2020.00789
Received: 21 June 2020; Accepted: 28 July 2020;
Published: 25 August 2020.
Edited by:
Rafaela Scariot, Universidade Positivo, BrazilReviewed by:
Renato Assis Machado, Campinas State University, BrazilGuilherme Trento, Universidade Positivo, Brazil
Copyright © 2020 Alam and Alfawzan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mohammad Khursheed Alam, ZHJhbGFtQGdtYWlsLmNvbQ==; bWthbGFtQGp1LmVkdS5zYQ==
†These authors have contributed equally to this work