 José F. Carrillo1
José F. Carrillo1 Rafael Vázquez-Romo2
Rafael Vázquez-Romo2 Margarita C. Ramírez-Ortega3Liliana C. Carrillo4Edgar Gómez-Argumosa5
Margarita C. Ramírez-Ortega3Liliana C. Carrillo4Edgar Gómez-Argumosa5 Luis F. Oñate-Ocaña6*
Luis F. Oñate-Ocaña6*- 1Departmento de Cabeza y Cuello, Instituto Nacional de Cancerología, Mexico, Mexico
- 2Subdirección de Cirugía, Instituto Nacional de Cancerología, Mexico, Mexico
- 3Departmento de Farmacología, Instituto Nacional de Cardiología Ignacio Chávez, Mexico, Mexico
- 4Departmento de Cuidados Paliativos, Instituto Nacional de Cancerología, Mexico, Mexico
- 5Departmento de Medicina Nuclear, Instituto Nacional de Cancerología, Mexico, Mexico
- 6Subdirección de Investigación Clínica, Instituto Nacional de Cancerología, Mexico, Mexico
Background: Patients treated for intermediate- or high-risk differentiated thyroid carcinoma (DTC) and Thyroglobulin (TG) elevation during follow-up, require a diagnostic whole-body scan (DWBS) and if positive, 131I treatment. This approach can lead to a delay in treatment and increased costs. The purpose of this study is to compare the oncologic outcomes associated to administration of direct therapy with 131I at first biochemical recurrence.
Methods: Retrospective cohort study of patients with intermediate- or high-risk DTC treated with total thyroidectomy, 131I ablation and who developed TG elevation during follow-up, between January 2007 and December 2015. Cohort A included patients who underwent a DWBS with 5 mCi of 131I, and if negative an MRI and/or 18FDG PET-CT prior to the therapeutic dosage, and cohort B included those who only received a therapeutic dosage of 131I, without a DWBS or extensive image studies. Main outcomes were second recurrence (SR) and disease-free survival (DFS). The diagnostic accuracy of DWBS was analyzed.
Results: Cohorts A and B had 74 and 41 patients, each. By multivariate analysis, age, differentiation grade, TN classification, ablation dose, and performed DWBS (odds ratio 55.1; 95% CI 11.3–269) were associated with SR (p < 0.0001); age, male gender, ablation dose and performed DWBS (hazard ratio 7.79; 95% CI 3.67–16.5) were independent factors associated with DFS (p < 0.0001). DWBS diagnostic accuracy was 36.48%.
Conclusion: 131I treatment in patients with DTC biochemical recurrence and no DWBS or extensive image studies is associated with a significantly lower frequency of SR and an increased DFS. The diagnostic accuracy of DWBS is low, and its clinical efficiency should be defined in prospective phase III studies.
Synopsis
Biochemical recurrences after treatment of intermediate- or high-risk thyroid cancer require a diagnostic whole-body scan and if positive, 131I treatment. This study suggests that patients could receive treatment without a scan, extensive image studies or long follow-up, to decrease recurrence rate and increase disease-free survival.
Introduction
The management of patients with differentiated thyroid carcinoma (DTC) treated with thyroidectomy and 131I ablation and who during follow-up develop progressive elevation of serum Thyroglobulin (TG), is the administration of 5 milliCuries (mCi) of 131I to obtain an exploratory diagnostic whole-body scintigraphy scan (DWBS), CT (computed tomography), or MRI (magnetic resonance image), and even a 18FDG PET-CT or continued follow up of thyroglobulin levels. If image studies are positive, or TG levels continue to increase, patients receive an 131I therapeutic dose of 50–200 mCi (1, 2).
The diagnostic accuracy of a 5 mCi 131I DWBS in the presence of a detected or suspected biochemical recurrence has not been reported and has been insufficiently investigated in studies yielding mostly inconclusive results (3–6). This raises the possibility of greater false-negative rates than those previously reported, and the consequent impact on final outcomes. Patients with a progressive increase in TG or anti-TG antibodies levels –even when high-risk factors are present– and a negative DWBS, the so called TENIS syndrome (7), are continuously followed with periodic DWBS until clinical recurrence, a positive DWBS or a greater increase in TG or anti-TG antibodies occurs. Moreover, some studies suggest performance of a 99mTc-3PRGD2 SPECT/CT in these circumstances (8). This policy delays treatment, increases costs, and induces stunning in the recurrent thyroid tissue, with its possible deleterious impact on prognosis.
The administration of 150–200 mCi of 131I in the presence of a biochemical recurrence without a DWBS, aforementioned image studies or continuous follow-up, is not routinely dispensed due to the assumed low 131I uptake and the risk of secondary malignancies, bone marrow dysplasia, toxic secondary effects, and endocrine dysfunction (9, 10). Therefore, the uptake rate and the oncologic outcomes of this treatment strategy have not been reported, but indirect study conclusions on 131I administration when TG is elevated and the DWBS is negative (11).
We analyzed the prognostic impact of direct 131I therapeutic dose in DTC after biochemical recurrence, in a cohort of patients with intermediate- and high-risk DTC, in terms of the frequency of a second recurrence (SR) and disease-free survival (DFS). The diagnostic accuracy of the DWBS was also evaluated.
Materials and Methods
Patients
Retrospective cohort study of patients with intermediate- or high-risk DTC, treated at our Institution between January 2007 and December 2015. Inclusion criteria: patients older than 18 years with histopathology reports demonstrating DTC (papillary, follicular, or mixed papillary/follicular carcinoma). High-risk was defined as an age above 55 years and one or more of these factors: tumor size over 4 cm, extension to soft tissue, clinical lymph node involvement, or poor differentiation. Patients younger than 55 but with two or more of the aforementioned factors, were considered intermediate-risk (1, 2). Patients treated with total thyroidectomy followed by adjuvant 131I ablation (100–150 mCi) were included if, during follow-up, they developed a biochemical recurrence defined as a Tg elevation ≥2 ng/ml and/or anti-Tg antibodies ≥50 IU/ml, under Thyroid stimulating hormone (TSH) suppression (serum level <0.5 mIU/L), with no clinical or image evidence of disease (4, 10). Follow-up visits were scheduled every 4 months during the first 2 years after thyroidectomy, then twice a year, and annually afterwards. Neck ultrasound and chest x-ray were obtained every year, and when the TG value increased.
Cohort A were treated according to ATA guidelines. Patients underwent a DWBS with 5 mCi of 131I prior to the therapeutic dosage. If uptake was positive, they received a 131I dosage of 150–200 mCi. A head/neck and chest CT scan and/or magnetic resonance imaging (MRI) was performed if the DWBS was negative, as well as a 18FDG PET/CT since 2011. If the aforementioned tests were negative for metastases or recurrent disease, follow-up continued until the DWBS was positive or if TG levels continued to increase, and a therapeutic 131I dosage was administered. If clinical-image (structural) recurrences ensued, these were treated with surgery if feasible, and/or radiation therapy, followed by a 131I therapeutic dose.
Patients assigned to one of the authors' (JFC) outpatient clinic for follow-up after thyroidectomy and ablative 131I treatment represent cohort B. To avoid delay in management and according to reports which advice direct administration of 131I in case of increasing TG levels, these patients received a therapeutic dosage of 131I without a prior DWBS or extensive image studies, but if this scan was negative an MRI and/or an 18FDG PET/CT were performed -as in cohort A- to search for structural recurrences elsewhere.
There were no major differences regarding outpatient clinic visits or follow-up tests in cohorts A or B, except regarding diagnostic and therapeutic strategy when a biochemical recurrence occurs.
The study protocol is STROBE-compliant and was accepted by the IRB and Ethics committee (01/2017). Both committees have waived the requirement for written informed consent because of the retrospective nature of the study.
Variables
Clinical, baseline and follow-up blood cytology and biochemistry, ultrasonography and x-ray data were recorded. Serum TG (ELSA-HTG immunoradiometric assay, CISBio International, Codolet, France), and anti-TG antibodies levels (Immulite 2000 Analyzer, Siemens Healthcare GmbH, Erlangen, Germany), as well as serum TSH (radioimmunometric assay, SPAC-5TSHkit, Daiichi, Japan) were measured. DWBS was performed after TSH stimulation after a 20–30 days withdrawal of levothyroxine administration. If TSH levels were ≥30 mIU/L, a 5 mCi 131I dosage was administered and the DWBS was obtained 48 h later (Symbia T6, Siemens Medical Solutions USA, Inc., Malvern, PA, USA). 131I treatment was conducted following the same parameters and with the equipment mentioned above; a dose of 150–200 mCi was administered and a scan was obtained 5–10 days later. Scan with planar images was performed in 100% of cases. SPECT-CT was performed in 47 cases (40.86%).
Statistical Analysis
Sample size was calculated assuming a frequency of SR of 90% in cohort A and 70% in cohort B, with 80% power, a probability value of 0.05, and an allocation ratio of 2:1; a total of 132 patients was necessary (88 in cohort A and 44 in cohort B). Student's T or the Chi squared tests were used for comparisons. Factors associated with SR were tested in a logistic regression model (12). SR was defined as the event characterized by an increase in Tg (≥2 ng/ml), increased anti-TG antibodies (≥50 IU/ml) under TSH suppression (serum level ≤ 0.5 mIU/L), or a clinical or image recurrence detected by neck ultrasound, MRI of the neck and mediastinum or 18FDG PET/CT. Factors associated with DFS were tested with the Kaplan–Meier method, and the log-rank test was used for comparisons. DFS was calculated from the date of surgery until the SR event or the last visit. Multivariate analysis of prognostic factors associated with DFS was conducted with Cox's model (13). The diagnostic accuracy of DWBS in biochemical recurrences was determined (14). The standard for positivity in DWBS refers to clinical or imaging recurrence during follow-up, a positive follow-up DWBS, or persistent elevation of TG or anti-TG antibodies levels after DWBS, which made surgical resection imperative and/or the final administration of a therapeutic dosage of 131I. Probability values of 0.05 or lower were considered significant using two-tailed statistics. SPSS software for Mac, version 23 was used (IBM Corp., Armonk, NY, USA).
Results
Patients
One-hundred and fifteen patients were included, 85 women (73.9%) and 30 men (26.1%), with a mean age of 50.9 years (Standard deviation 15.7, range 19–93); 74 (64.3%) were allocated to cohort A and 41 (35.7%) to cohort B. Demographic and clinical characteristics are presented in Table 1. There were 105 papillary tumors, one Hürthle cell carcinoma, three insular carcinomas and six other histopathologic varieties (tall cell and poorly-differentiated carcinomas). No significant differences were detected in terms of gender, histology, tumor and node classification (TNM), original thyroid tumor size, median TG levels, and pre- or post-operative radiotherapy treatment between cohorts. TSH mean value was 0.2 mIU/L for cohort A, range 0.01–4.5 mIU/L, median 0.1 mIU/L. Cohort B values were: mean 0.1 mIU/L, range 0.005–2 mIU/L median: 0.8 mIU/L.
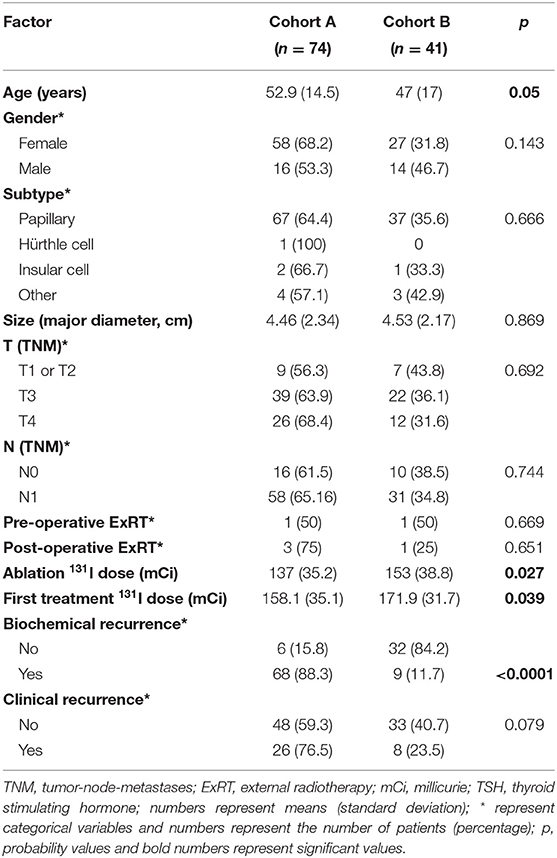
Table 1. Clinical characteristics of patients per cohort (n = 115).
Cohort A median Tg was 4 ng/ml (minimum 0.2, maximum 6.4); Cohort B, median Tg was 2.5 ng/ml (minimum 0.1; maximum 4.96). Median anti-TG antibodies level was 60 IU/ml (range 55–5,450 IU/ml) at time of recurrence.
Transient recurrent laryngeal nerve lesion (RLNL) and hypoparathyroidism were recorded in 16 (13.9%) and 34 (29.6%) cases, respectively. At 1-year follow-up, permanent hypoparathyroidism had developed in 15 (13%) cases and RLNL in 10 (8.7%) cases. In cohort A, the DWBS was positive in 22 (29.7%) patients.
Positive uptake after therapeutic 131I dosage was 69 (93.2%) and 40 (97.6%) in cohorts A and B, respectively (p = 0.332).
Sites of uptake with planar images were located at: locoregional level, mediastinum, and lung in 40 (34.78%), 29 (25.2%), and 39 (33.91%) patients, respectively. One case had bone uptake and in 6 (5.21%) cases no uptake was detected.
DWBS sensitivity, specificity, negative and positive predictive values were 31, 100, 9.6, and 100% respectively. Diagnostic accuracy was 36.4%.
Recurrences
SR during follow-up and after treatment of a first recurrence, was identified in 77 patients (67%). In cohort A, 68 patients (93.2%) presented a SR and in cohort B, 9 patients (22%) (p < 0.0001). The odds ratio was 3.85 (95% CI 2.15–6.89) (p < 0.0001) and the necessary number to treat was 1.55 (95% CI 1.28–1.99), both favoring cohort B. There were 34 patients (29.6%) with clinical recurrences during follow-up; 26 in cohort A (35.1%) and eight in cohort B (19.5%) (p = 0.061).
In cohort A, from 22 cases who had a positive DWBS, four (18.18%) patients finally developed a clinical recurrence which was treated with surgery in three cases-a neck dissection was performed because of neck recurrence-, and one with radiotherapy because of bone metastases.
Two patients received radiotherapy -in each cohort- because of unresectable disease considered by the treating surgeon. Afterwards all of them were subjected to an R0 resection. Three patients received adjuvant radiotherapy because of concerns on microscopic disease because of the locoregional extent of the malignancy.
Table 2 describes the bivariate association of relevant factors and the SR outcome. Risk factors significantly associated to SR by bivariate analysis were age, 131I ablation dose, first 131I therapeutic dose and exposure to DWBS. Risk factors associated with SR by multivariate analysis were age, non-papillary histology subtype, T and N classification, first 131I ablative dose, and exposure to DWBS (Table 3).
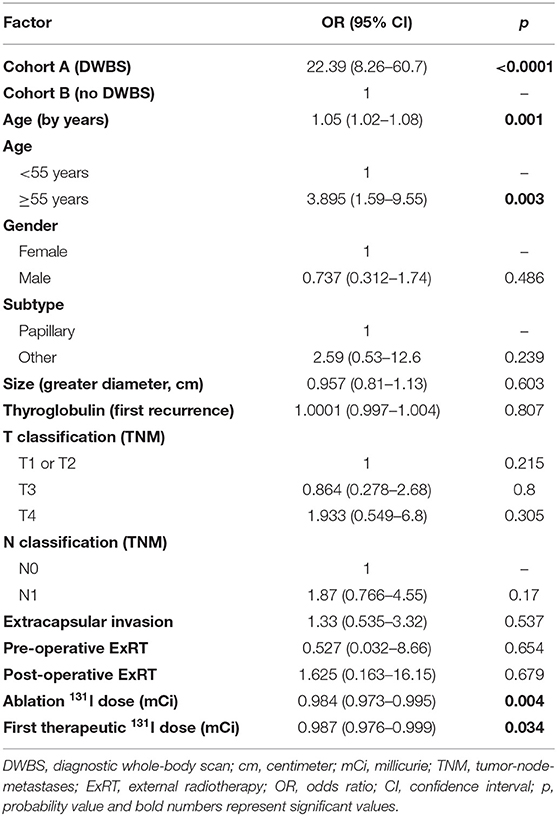
Table 2. Bivariate association of clinical factors with secondary biochemical recurrence (n = 115).
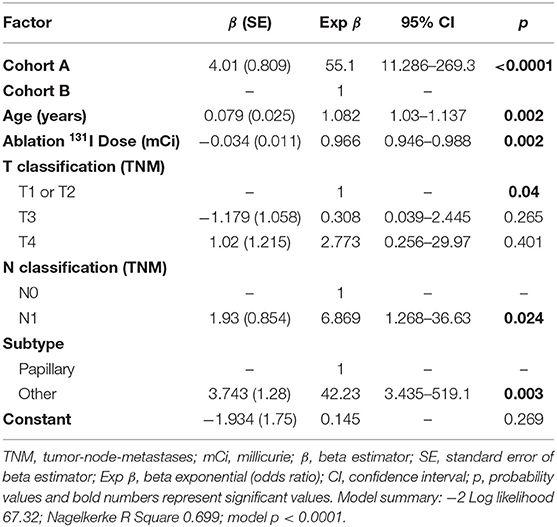
Table 3. Multivariate association of clinical factors with second biochemical recurrence (n = 115).
Survival
Median follow-up of patients in both cohorts was 3.2 years (interquartile range 1.9–5.7). Disease-specific (DSS) and Overall survival (OS) were not calculated because only two patients (2%) in cohort A and one (2.4%) in cohort B have died due to DTC (p = 0.532). The median DFS of both cohorts was 4.66 years (95% CI 3.2–6.04).
Median DFS for cohorts A and B were 3.36 (95% CI 2.42–4.3) and 16.02 years (95% CI 4.7–27.4), respectively (p < 0.0001). Kaplan-Meier DFS curves of cohort A and B are depicted in Figure 1.
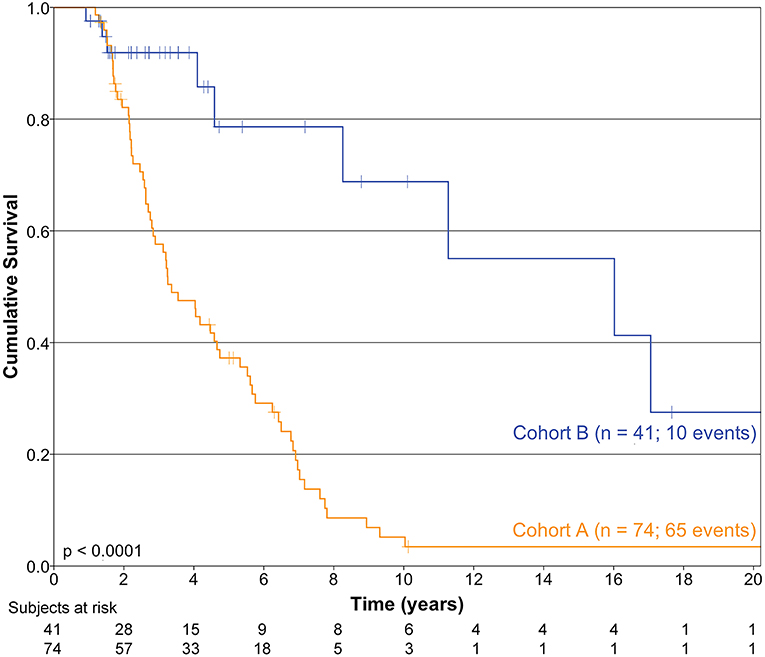
Figure 1. Kaplan-Meier curves depicting disease-free survival in cohorts A and B.
The association of relevant factors and DFS by bivariate and multivariate analyses is described in Tables 4, 5, respectively.
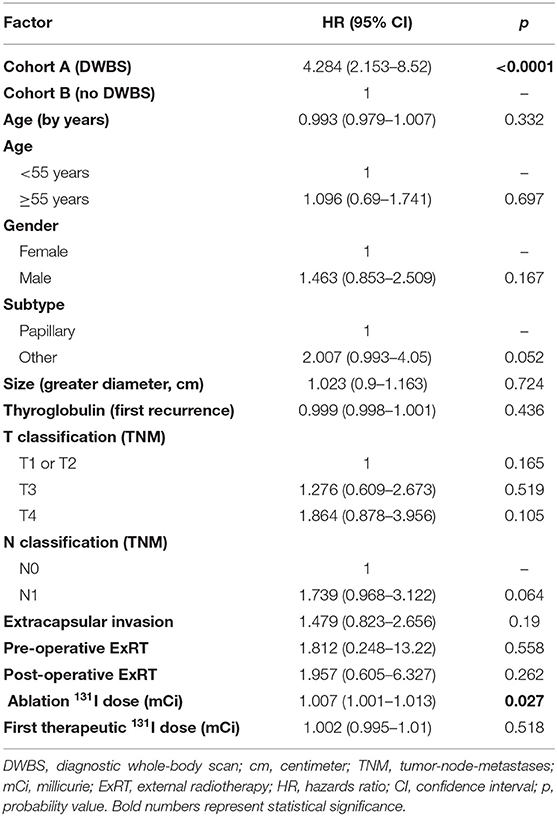
Table 4. Bivariate association of clinical factors with disease-free survival (n = 115).
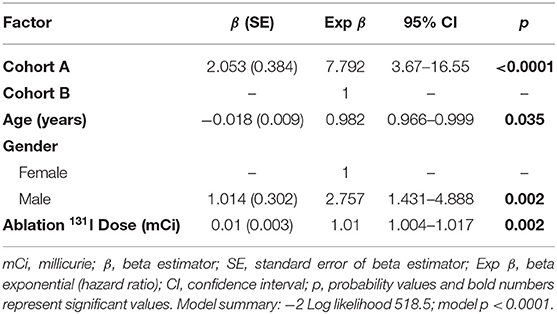
Table 5. Multivariate association of clinical factors with disease-free survival (n = 115).
Discussion
The incidence of DTC and far advanced cases has increased, especially in low-income societies with access to specialized care, yielding intermediate- or high-risk cohorts (15–17).
Total thyroidectomy followed by adjuvant 131I ablation is the current treatment of DTC (18). However, long-term cancer control rates between doses have led to conflicting results. In low-risk cases, results of ablative therapy with 131I are probably equivalent between doses of 30–50 mCi and doses ≥100 mCi (19). In intermediate- and high-risk patients, higher-doses of 131I might produce better cancer control (20, 21).
There are reports of patients with no clinical or imaging recurrences in spite of persistently elevated TG or anti-TG antibodies, and in the presence of a negative DWBS during follow-up. In some cases, elevated marker levels (5–10%) decrease or disappear, and several authors analyze outcomes with the administration of “131I empirical therapy” at dosages ≥100 mCi, and lag spans up to 4 years (22, 23).
A cohort study of patients with DTC and long-term follow-up from a single cancer center with homogeneous surgical and radioiodine treatment protocols is presented. Cohort A received 131I treatment after confirmatory DWBS, Head and neck CT or MRI. From 2011 a 18FDG PET-CT was performed in these cases-which demonstrated a recurrence- or persistent elevation and increase of TG levels which prompted administration of 131I therapeutic dose. Cohort B received 131I treatment but no DWBS or further diagnostic studies or follow-up were performed.
An intermediate- to high-risk category was established in our patients because ≥80% had a T3 or above classification; their mean age was 51 years, lymph nodes were positive in >75% of cases, mean tumor size was 4.5 cm, major extrathyroidal extension was present in >90% of cases, and a small number of patients had aggressive histopathology (1, 24).
Mazzaferri reported the limited value of DWBS because of high false-negative rates and recommended a therapeutic dose of 131I with increasing TG values, in the presence of a negative neck ultrasound (6). However, he considered the detection of recombinant human TSH (rhTSH)-stimulated TG ≥2 ng/ml as indicative of treatment and this policy was used even in low-risk patients. This is controversial because of the slow progression of DTC and the high-cost of rhTSH (22). Others have considered the administration of an 131I dose when TG increases during follow-up, because of a high DWBS false-negative rate (67%), although they do not elaborate any further (6, 25, 26).
We address these controversies establishing a high efficiency strategy in the presence of biochemical recurrence, consisting in the direct administration of a therapeutic 131I dosage in high-risk patients. The administration in intermediate- and high-risk cases of a therapeutic 131I dose ≥100 mCi without the performance of a DWBS, follow up or extensive image studies, in the presence of a biochemical recurrence, was associated with a decrease in SR and increased DFS (4, 6).
Although we agree with recommendation 67B from ATA guidelines, sections (i) and (ii) regarding DWBS in patients with abnormal uptake outside the thyroid bed and large thyroid remnants on post-therapy WBS (1), these two situations are probably indicative of metastatic or residual disease and not necessarily represent biochemical recurrence, which is the subject of our study. Regarding section (iii) of same recommendation, anti-TG antibodies elevation in our series was successfully treated with direct 131I therapy in six cases. Two other cases belonged to cohort A and finally developed clinical recurrence which was treated surgically. The 123I isotope is not currently available in our country and its high-cost hampers its widespread use.
We agree with recommendation 68B from ATA guidelines which states that 18FDG PET-CT scan should be considered in high-risk patients with negative radioiodine scan, and this was included recently-as established in the manuscript- in the diagnostic strategy of cohort A. Even in cohort B cases if a negative uptake ensued after a direct 131I dose, we performed an MRI and 18FDG PET-CT of the mediastinum and neck from year 2011. However, a word of caution should be given because the sensitivity and specificity of this tool have been reported as 60 and 80% (27) in patients with stimulated TG ≥30 ng/ml. Aside, a major limit for its diagnostic accuracy is that significant findings are related to a ≥5 mm diameter of the lesion. Moreover, larger lesions could be considered structural recurrences which could be detected with CT and or MRI of head and neck and chest areas. Although our analyses was not designed to evaluate the diagnostic accuracy of 18FDG PET-CT diagnostic accuracy, sensitivity and specificity were 30.77, 25, and 100%, respectively, in those patients who had this test performed in our study, regarding biochemical recurrences.
The differentiation grade was associated with SR by multivariate analysis as has been reported (21, 24), and underscores the need to effectively treat patients with biochemical recurrence and high-risk factors, and avoid a DWBS (6). Although, as stated by ATA guidelines, recommendations for 18FDG PET-CT should be considered in cases with aggressive histology and metastatic disease to identify lesions at risk for rapid progression and evaluate the response after local or systemic therapy for invasive and metastatic disease, same aforementioned 18FDG PET-CT limitations regarding diagnostic accuracy of the test should be considered regarding this issue.
There is a tendency to administer lower ablation and therapeutic doses of 131I in DTC patients, even in intermediate-risk cases (1). In our study, higher ablative 131I doses were associated with decreased SR by multivariate analysis; this underscores the need to define the treatment strategy according to the clinical-histopathological characteristics and risks, especially in advanced stages (21).
RLNL and permanent hypoparathyroidism rates were high. Of note, these cases had more advanced disease and a high surgical risk (28, 29).
As in any cohort study, a potential pitfall in this study is the non-random and open nature of patient allocation in each cohort. The actual sample size is adequate because the observed differences between cohorts were greater than expected.
A clear difference exists in the uptake rate of DWBS compared with that after therapeutic doses in the setting of biochemical recurrences; the diagnostic accuracy of DWBS was 36.48%. This was analyzed in spite of the lack of a histopathological gold standard but the follow-up and TG levels are sufficient to establish the diagnostic accuracy values for DWBS (6, 26, 30). Moreover, no explanation exists for the positive 131I uptake after a direct therapeutic dose, after a 1-year follow-up with negative TG levels.
There are reports on the so-called “empiric” 131I dose administration after a negative DWBS, the TENIS syndrome (7), in patients who maintained persistent or elevated values of biochemical markers which made the administration of 131I therapy imperative or until clinical or image recurrence ensued (4, 10). These reports refer a high 131I uptake rate (≥65%) in the post-therapy scans. However, major drawbacks include the length of time before a therapeutic decision is made, stunning after repeated DWBS, and the high cost and delay of treatment because of the usually performed image studies (CT and 18FDG PET-CT scans). Also, over 50% of patients were low-risk and early-stage in these series, which decreases the clinical impact of this strategy (4, 10). In our study, over 95% of cases who received 131I therapy had a positive uptake.
Shinohara categorized TG and DWBS. Two groups with negative DWBS were described, one with TG elevation and another with normal TG (21). The first group had higher risk factors and a lower DFS. This suggests the need to take biochemical recurrences into consideration in high-risk patients and use a different strategy, perhaps a direct therapeutic dosage, as we have proposed.
We agree with some authors (1, 10) who consider that a biochemical incomplete response is not uncommon, with final return to normal limits in a majority of cases. Although a special consideration should be given to the fact that this regression refers mostly (10) to stimulated TG levels in low risk patients. Our study refers to a group of patients selected as intermediate- and high-risk with more stringent criteria for risk stratification, and to a non-stimulated cutoff of 2 ng/ml which is highly suspicious for a recurrence as demonstrated in our study. In intermediate- and high-risk cases -as established in our study-, spontaneous remission of high TG levels occurred in only 5 cases (6.75%) from patients who had a DWBS, with progressive increase of TG levels in the rest of them.
We agree with the ATA guidelines recommendations 80, 81, and 82 (1), regarding empiric radioiodine therapy in patients with increasing TG and anti-TG levels, although our success rate was higher (probably because of the inclusion in our series of high- and intermediate-risk patients), with 97% positive uptake rate and second recurrence rate of 21% after direct 131I therapy. A word of caution should be given considering the low sensitivity and negative predictive value of 18FDG-PETCT already mentioned.
With direct 131I therapy, the possibility of developing clinical or imaging metastases is decreased, since our strategy has the potential to prevent the appearance of resistant cell strains and therefore avoid stunning—which when unresectable, are frequently reported as resistant to radiotherapy (31, 32). Although there is evidence for the use of multitargeted kinase inhibitors in 131I-resistant cases, resistance and the need to administer these agents should be avoided (31).
There are reports of acute myeloid leukemia in patients with DTC treated with radioiodine (9). However, the total dosages used are usually not described. Furthermore, as stated by the same authors, the recurrence risk if no 131I therapy is used, is higher than the possibility of developing leukemia in high-risk cases.
In spite of a good prognosis in low-risk patients, some do recur, and early detection is imperative. The administration of 131I therapy in these patients should be judicious because of quality of life concerns and the risk of secondary malignancies (33). Lower doses in cases of a suppressed TG increase, could be indicated and investigated in the future, given our results.
A greater number of intermediate- and high-risk cases should be recruited to establish the approach reported as standard in the treatment of biochemical recurrences. More sensitive iodine scanners and studies proposing the rational use of 18FDG-PETCT might confirm our results. Prospective and multi-institutional studies to confirm these findings with possible impact on survival are warranted (8, 34, 35).
Intermediate- and high-risk DTC patients with TG elevation during follow-up should probably receive a therapeutic dose of 131I without a prior DWBS to prevent TENIS syndrome, treatment delays and increased costs. Other image studies like CT and MRI as well as 18FDG-PETCT and follow up of TG levels could be avoided. This approach improves DFS in patients with biochemical recurrence. DWBS diagnostic accuracy is low and its performance could induce stunning, delay treatment and increase clinical recurrence rates.
Data Availability Statement
All datasets generated for this study are included in the article/supplementary material.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Investigación y Comité de Etica en Investigación, Instituto Nacional de Cancerología, México. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author's Note
This study was presented in part at the ENT World Congress (oral presentation), IFOS, Paris, June 24–28, 2017 (abstract:3665).
Author Contributions
JC and LO-O: study concepts and literature review. JC, RV-R, MR-O, LC, EG-A, and LO-O: protocol writing. JC, RV-R, LC, and MR-O: data acquisition. JC, RV-R, MR-O, LC, EG-A, and LO-O: quality control of database. JC and LO-O: data analysis and interpretation. JC, RV-R, EG-A, and LO-O: manuscript drafting. JC, RV-R, MR-O, LC, EG-A, and LO-O: manuscript final review.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to Professor Deborah Aleman-Hoey for her kind support with the English-Language review.
References
1. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. (2016) 26:1–133. doi: 10.1089/thy.2015.0020
2. Tuttle RM, Morris LF, Haugen BR, Shah JP, Sosa JA, Rohren E, et al. Thyroid differentiated and anaplastic carcinoma. In: Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Jessup JM, et al. 2017 AJCC Cancer Staging Manual, 8th ed. Chicago, IL: Springer International Publishing (2017) p. 873–90. doi: 10.1007/978-3-319-40618-3_73
3. Ma C, Xie J, Kuang A. Is empiric 131I therapy justified for patients with positive thyroglobulin and negative 131I whole-body scanning results? J Nucl Med. (2005) 46:1164–70.
4. Koh JM, Kim ES, Ryu JS, Hong SJ, Kim WB, Shong YK. Effects of therapeutic doses of 131I in thyroid papillary carcinoma patients with elevated thyroglobulin level and negative 131I whole-body scan: comparative study. Clin Endocrinol (Oxf). (2003) 58:421–7. doi: 10.1046/j.1365-2265.2003.01733.x
5. Van Wyngaarden K, McDougall IR. Is serum thyroglobulin a useful marker for thyroid cancer in patients who have not had ablation of residual thyroid tissue? Thyroid. (1997) 7:343–6. doi: 10.1089/thy.1997.7.343
6. Mazzaferri EL, Robbins RJ, Spencer CA, Braverman LE, Pacini F, Wartofsky L, et al. A consensus report of the role of serum thyroglobulin as a monitoring method for low-risk patients with papillary thyroid carcinoma. J Clin Endocrinol Metab. (2003) 88:1433–41. doi: 10.1210/jc.2002-021702
7. Silberstein EB. The problem of the patient with thyroglobulin elevation but negative iodine scintigraphy: the TENIS syndrome. Semin Nucl Med. (2011) 41:113–20. doi: 10.1053/j.semnuclmed.2010.10.002
8. Gao R, Zhang GJ, Wang YB, Liu Y, Wang F, Jia X, et al. Clinical value of 99mTc-3PRGD2 SPECT/CT in differentiated thyroid carcinoma with negative 131I whole-body scan and elevated thyroglobulin level. Sci Rep. (2018) 8:473. doi: 10.1038/s41598-017-19036-9
9. Molenaar RJ, Sidana S, Radivoyevitch T, Advani AS, Gerds AT, Carraway HE, et al. Risk of hematologic malignancies after radioiodine treatment of well-differentiated thyroid cancer. J Clin Oncol. (2018) 36:1831–9. doi: 10.1200/JCO.2018.78.4074
10. Rosario PW, Mourão GF, dos Santos JB, Calsolari. Is empirical radioactive iodine therapy still a valid approach to patients with thyroid cancer and elevated thyroglobulin? Thyroid. (2014) 24:533–6. doi: 10.1089/thy.2013.0427
11. Marti JL, Morris LGT, Ho AS. Selective use of radioactive iodine (RAI) in thyroid cancer: no longer “one size fits all.” Eur J Surg Oncol. (2018) 44:348–56. doi: 10.1016/j.ejso.2017.04.002
12. Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. 3rd ed. Hoboken, NJ: Wiley & Sons, Inc. (2013).
13. Hosmer DW, Lemeshow S, May S. Applied Survival Analysis: Regression Modeling of Time to Event Data. 2nd ed. Hoboken, NJ: Wiley & Sons, Inc. (2008).
14. Galen RS, Gambino SR. Beyond Normality: The Predictive Value and Efficiency of Medical Diagnosis. New York, NY: Wiley (1975). p. 30–40.
15. Sanabria A, Kowalski LP, Shah JP, Nixon IJ, Angelos P, Williams MD, et al. Growing incidence of thyroid carcinoma in recent years: factors underlying overdiagnosis. Head Neck. (2018) 40:855–66. doi: 10.1002/hed.25029
16. Finlayson A, Barnes I, Sayeed S, McIver B, Beral V, Ali R. Incidence of thyroid cancer in England by ethnic group, 2001–2007. Br J Cancer. (2014) 110:1322–7. doi: 10.1038/bjc.2014.4
17. Vigneri R, Malandrino P, Vigneri P. The changing epidemiology of thyroid cancer: why is incidence increasing? Curr Opin Oncol. (2015) 27:1–7. doi: 10.1097/CCO.0000000000000148
18. Nixon IJ, Ganly I, Shah JP. Thyroid cancer: surgery for the primary tumor. Oral Oncol. (2013) 49:654–8. doi: 10.1016/j.oraloncology.2013.03.439
19. Wang LY, Ganly I. Post-treatment surveillance of thyroid cancer. Eur J Surg Oncol. (2018) 44:357–66. doi: 10.1016/j.ejso.2017.07.004
20. Andresen NS, Buatti JM, Tewfik HH, Pagedar NA, Anderson CM, Watkins JM. Radioiodine ablation following thyroidectomy for differentiated thyroid cancer: literature review of utility, dose, and toxicity. Eur Thyroid J. (2017) 6:187–96. doi: 10.1159/000468927
21. Shinohara S, Kikuchi M, Suehiro A, Kishimoto I, Harada H, Hino M, et al. Characteristics and prognosis of patients with thyroglobulin-positive and radioactive iodine whole-body scan-negative differentiated thyroid carcinoma. Jpn J Clin Oncol. (2015) 45:427–32. doi: 10.1093/jjco/hyv021
22. Chao M. Management of differentiated thyroid cancer with rising thyroglobulin and negative diagnostic radioiodine whole body scan. Clin Oncol (R Coll Radiol). (2010) 22:438–47. doi: 10.1016/j.clon.2010.05.005
23. Ma C, Kuang A, Xie J. Radioiodine therapy for differentiated thyroid carcinoma with thyroglobulin positive and radioactive iodine negative metastases. Cochrane Database Syst Rev. (2009) 1:CD006988. doi: 10.1002/14651858.CD006988.pub2
24. Perrier ND, Brierley JD, Tuttle RM. Differentiated and anaplastic thyroid carcinoma: major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. (2018) 68:55–63. doi: 10.3322/caac.21439
25. Zanotti-Fregonara P, Keller I, Calzada-Nocaudie M, Devaux JY, Hindié E. Thyrotropin variations may explain some positive radioiodine therapy scans in patients with negative diagnostic scans. J Endocrinol Invest. (2009) 32:267–71. doi: 10.1007/BF03346465
26. Pacini F, Agate L, Elisei R, Capezzone M, Ceccarelli C, Lippi F, et al. Outcome of differentiated thyroid cancer with detectable serum Tg and negative diagnostic 131I whole body scan: comparison of patients treated with high 131I activities versus untreated patients. J Clin Endocrinol Metab. (2001) 86:4092–7. doi: 10.1210/jcem.86.9.7831
27. Stangierski A, Kaznowski J, Wolinski K, Jodlowska E, Michaliszyn P, Kubiak K, et al. The usefulness of fluorine-18 fluorodeoxyglucose PET in the detection of recurrence in patients with differentiated thyroid cancer with elevated thyroglobulin and negative radioiodine whole-body scan. Nucl Med Commun. (2016) 37:935–8. doi: 10.1097/MNM.0000000000000563
28. Francis DO, Pearce EC, Ni S, Garrett CG, Penson DF. Epidemiology of vocal fold paralyses after total thyroidectomy for well-differentiated thyroid cancer in a Medicare population. Otolaryngol Head Neck Surg. (2014) 150:548–57. doi: 10.1177/0194599814521381
29. Chadwik DR. Hypocalcaemia and permanent hypoparathyroidism after total/bilateral thyroidectomy in the BAETS Registry. Gland Surg. (2017) 6:S69–74. doi: 10.21037/gs.2017.09.14
30. Schlumberger M, Mancusi F, Baudin E, Pacini F. 131I therapy for elevated thyroglobulin levels. Thyroid. (1997) 7:273–6. doi: 10.1089/thy.1997.7.273
31. Gild ML, Topliss DJ, Learoyd D, Parnis F, Tie J, Hughes B, et al. Clinical guidance for radioiodine refractory differentiated thyroid cancer. Clin Endocrinol (Oxf). (2018) 88:529–37. doi: 10.1111/cen.13508
32. Yin Y, Mao Q, Chen S, Li N, Li X, Li Y. A quantitative study about thyroid stunning after diagnostic whole-body scanning with 74 MBq 131I in patients with differentiated thyroid carcinoma. Q J Nucl Med Mol Imaging. (2015) 59:455–61.
33. Bohinc BN, Perkins JM. Appropriate dosing of adjuvant radioactive iodine for differentiated thyroid cancer. Curr Opin Oncol. (2014) 26:31–5. doi: 10.1097/CCO.0000000000000039
34. Maruoka Y, Abe K, Baba S, Isoda T, Sawamoto H, Tanabe Y, et al. Incremental diagnostic value of SPECT/CT with 131I scintigraphy after radioiodine therapy in patients with well-differentiated thyroid carcinoma. Radiology. (2012) 265:902–9. doi: 10.1148/radiol.12112108
35. Bertagna F, Albano D, Bosio G, Piccardo A, Dib B, Giubbini R. 18F-FDG-PET/CT in patients affected by differentiated thyroid carcinoma with positive thyroglobulin level and negative 131I whole body scan. Its value confirmed by a bicentric experience. Curr Radiopharm. (2016) 9:228–34. doi: 10.2174/1874471009666160523145005
Keywords: differentiated thyroid cancer, 131I treatment, thyroglobulin, diagnostic whole body scan, cohort studies
Citation: Carrillo JF, Vázquez-Romo R, Ramírez-Ortega MC, Carrillo LC, Gómez-Argumosa E and Oñate-Ocaña LF (2019) Prognostic Impact of Direct 131I Therapy After Detection of Biochemical Recurrence in Intermediate or High-Risk Differentiated Thyroid Cancer: A Retrospective Cohort Study. Front. Endocrinol. 10:737. doi: 10.3389/fendo.2019.00737
Received: 29 May 2019; Accepted: 11 October 2019;
Published: 29 October 2019.
Edited by:
Leon Bach, Monash University, AustraliaReviewed by:
Gabriella Pellegriti, University of Catania, ItalyMarialuisa Appetecchia, Istituti Fisioterapici Ospitalieri (IRCCS), Italy
Copyright © 2019 Carrillo, Vázquez-Romo, Ramírez-Ortega, Carrillo, Gómez-Argumosa and Oñate-Ocaña. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis F. Oñate-Ocaña, bGZvbmF0ZUBnbWFpbC5jb20=