 Tim Rahmel1*†
Tim Rahmel1*† Hartmuth Nowak1† Sandra Frisenda1Katharina Rump1
Hartmuth Nowak1† Sandra Frisenda1Katharina Rump1 Björn Koos1Peter Schenker2Richard Viebahn2Michael Adamzik1
Björn Koos1Peter Schenker2Richard Viebahn2Michael Adamzik1 Lars Bergmann1
Lars Bergmann1- 1Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie, Universitätsklinikum Knappschaftskrankenhaus Bochum, Bochum, Germany
- 2Klinik für Chirurgie, Universitätsklinikum Knappschaftskrankenhaus Bochum, Bochum, Germany
Background: The aquaporin 5 (AQP5) −1364A/C promoter single nucleotide polymorphism affects key mechanisms of inflammation and immune cell migration. Thus, it could be involved in the pathogenesis of cytomegalovirus infection. Accordingly, we tested the hypothesis that the AQP5 promoter −1364A/C polymorphism is associated with the risk of cytomegalovirus infection in kidney transplantation recipients.
Methods: We included 259 adult patients who received a kidney transplant from 2007 and 2014 in this observational study. Patients were genotyped for the AQP5 promoter −1364A/C single nucleotide polymorphism and followed up for 12 months after transplantation. Kaplan–Meier plots and multivariable proportional hazard analyses were used to evaluate the relationship between genotypes and the incidence of cytomegalovirus infection.
Results: The incidences of cytomegalovirus infection within 12 months after kidney transplantation were 22.9% for the AA genotypes (43/188) and 42.3% for the AC/CC genotypes (30/71; p = 0.002). Furthermore, multivariable COX regression revealed the C-allele of the AQP5 −1364A/C polymorphism to be a strong and independent risk factor for cytomegalovirus infection. In this analysis, AC/CC subjects demonstrated a more than 2-fold increased risk for cytomegalovirus infection within the first year after kidney transplantation (hazard ratio: 2.28; 95% CI: 1.40–3.73; p = 0.001) compared to that in individuals with homozygous AA genotypes.
Conclusions: With respect to opportunistic cytomegalovirus infections (attributable to immunosuppression after kidney transplantation), the C-allele of the AQP5 −1364A/C promoter polymorphism is independently associated with an increased 12-months infection risk. These findings emphasize the importance of genetic variations as additional risk factors of cytomegalovirus infection after solid organ transplantations and might also facilitate the discovery of novel therapeutic targets.
Introduction
Cytomegalovirus (CMV) is one of the most common opportunistic infections in kidney transplant recipients, which affects transplant rejection and graft function, triggers harmful CMV-associated diseases, and might also influence mortality rates (1, 2). Antiviral chemoprophylaxis seems to be a successful strategy in preventing major complications related to CMV infections, but universal prophylaxis is also detrimental, due to drug toxicity, late CMV disease, and the development of ganciclovir-resistant mutants (3). Therefore, risk-adapted strategies appear to be a cornerstone of modern antiviral chemoprophylaxis and identifying associated risk factors seems to be crucial to improve current post-transplantation care. In this context, the incidence of CMV infections is highly dependent on the serostatus of the recipient (R) and the donor (D) with the highest risk noted in D positive and R negative (D+/R−) transplantations (4). However, CMV infection risk cannot be solely attributed to this single risk factor, as some of additional variability might be caused by genetic variations (5).
An interesting candidate for investigations regarding such genetic variations is the single nucleotide polymorphism (SNP; rs3759129) in the aquaporin 5 (AQP5) promoter region (−1364A/C). Previously, we described that the substitution of cytosine for adenine at position −1364 is associated with lower AQP5 messenger RNA and protein expression (6). In this context, AQP5 expression mediates water transport across biologic membranes, regulating cellular water fluid homeostasis during inflammation, proliferation, and cell migration, processes that involve the transient formation of membrane protrusions (lamellipodia and membrane ruffles) at the leading edge of the cell (7–9). The crucial effect of this AQP5 SNP in mediating key mechanisms of inflammation and altering related host–pathogen communication was demonstrated in patients with sepsis and acute respiratory distress syndrome (10–12). In this regard, the AQP5 −1364A/C promoter SNP was found to affect neutrophil migration into the lungs and the AA genotypes were associated with aggravated pulmonary inflammation in acute respiratory distress syndrome evoked by bacteria (10). Strikingly, increased AQP5 expression and the AA genotype of the AQP5 SNP were also shown to be associated with improved bacterial eradication, and therefore an enhanced antimicrobial immune response (10, 13).
Taken together, this AQP5 polymorphism could contribute to the risk of CMV infection in kidney transplant recipients due to an altered resistance to viral infections, but data addressing this topic are completely lacking. Accordingly, we tested the hypothesis that the AQP5 promoter −1364A/C polymorphism is associated with the risk of CMV infection in kidney transplantation recipients.
Materials and Methods
Patients and Treatments
This study was reviewed and approved by the local ethics board of the Faculty of Medicine, Ruhr-University of Bochum (Bochum, Germany; protocol no. 4870-13). Patients were enrolled in this study upon receiving a kidney or combined pancreas–kidney transplant between 2007 and 2014 at the Department of General Surgery of the University Hospital Knappschaftskrankenhaus Bochum (Bochum, Germany). For study inclusion written informed consent was obtained from all 259 participating patients, according to the Declaration of Helsinki, good clinical practice guidelines and applicable to local regulatory requirements.
Patients were recruited to donate a buccal swab for DNA extraction and the evaluation of AQP5 SNPs after transplantation. Clinical and demographic data were gathered upon study inclusion and patients were observed for 1 year after organ transplantation. All patients received immunosuppressive induction and maintenance therapy according to locally specific standard operating procedures, which included steroids, calcineurin inhibitors, and mycophenolic acid (Table 1), as well as risk-adapted perioperative and post-operative antiviral chemoprophylaxis with ganciclovir or valganciclovir. In this context, 59 high-risk patients (D+/R−) received chemoprophylaxis for 6 months (except five patients in this group with unknown or shorter duration), 144 medium-risk patients (D+/R+ and D−/R+) received prophylaxis for 3 months (except 10 patients in this group with unknown or shorter duration), and 41 low-risk patients (D−/R−) received perioperative prophylaxis, for whom chemoprophylaxis was expanded to 3 months in 20 cases, for example, due to CMV-positive blood transfusions.
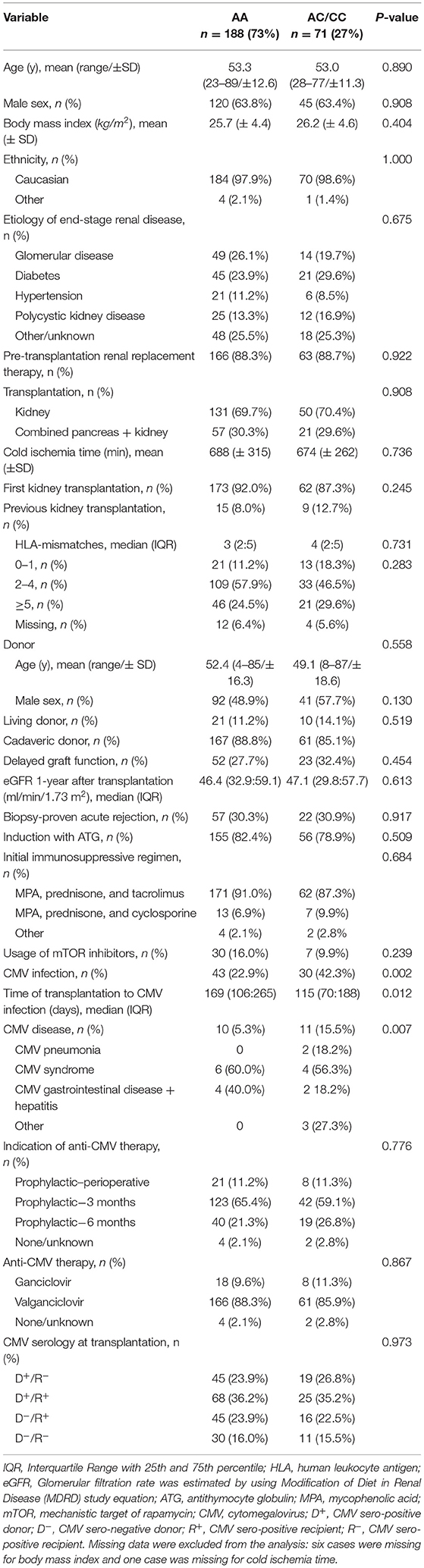
Table 1. Characteristics of kidney transplantation patients (n = 259) at baseline stratified by AQP5 −1364 A/C genotype.
Routine surveillance for viral reactivation or infection comprised weekly determinations of CMV viremia based on whole blood samples via PCR, until hospital discharge from index-admission and continuing monthly thereafter and when clinically indicated. Additionally, all patients were screened for CMV infection at the 1-year follow up examination after transplantation. Delayed graft function was defined as the necessity for dialysis in the first week after surgery.
DNA Genotyping
DNA was extracted from buccal swabs using the QIAamp DNA Mini Kit (QIAGEN, Hilden, Germany). To genotype the −1364A/C AQP5 promoter SNP, a nested polymerase chain reaction was performed with the forward AQP5-SE 5′-CCCAGACCAGGGGTAGAAGA-3′, and the reverse AQP5-AS 5′-TCTTCCTGCTAGAAGCCCCT-3′ primers followed by tetra-primer ARMS-PCR with Forward inner primer (A allele): 5′-GAGAGAGACAGAGAGACTAAGACAGCGAA-3′, Reverse inner primer (C allele): 5′-CATTTTCTGTTTTTCCTTCCTGCTTG-3′, Forward outer primer 5′-GACCACATGTAAGAGAGAGAGACATGGA-3′ and Reverse outer primer 5′-CTGTCAGTCAGTCTTTGCAAAACCCTAT-3′ resulting in a 223 base pair fragment for A allele and a 189 base pair fragment for C allele.
Study Groups and End Points
Study patients were assigned to two groups (AA genotype vs. AC/CC genotype) depending on the −1364A/C SNP in the AQP5 promoter. The AC and CC genotypes were combined because of the low frequency (3.1%; 8/289) of the CC genotype.
The primary end point was CMV-free survival in the first year after kidney transplantation. The key secondary end point was the effect of chemoprophylaxis duration on the time of CMV infection onset.
Clinical Definitions and Diagnostics
CMV infection was defined as the detection of viral nucleic acid in accordance to the definition of Ljungman and colleagues (14). CMV DNA was evaluated using a commercially available PCR assay (Roche Ampliprep Assay; Roche Molecular Diagnostics, Pleasanton, CA, USA) as per the manufacturer's instructions and calibrated to the World Health Organization International Standard for Human CMV.
CMV disease and related entities (e.g., CMV pneumonia and CMV syndrome) were defined as the presence of CMV in the blood based on a local assay plus the presence of compatible symptoms as described by Ljungman and colleagues (14).
Statistical Analysis
The characteristics of patients at baseline (timepoint of transplantation) were reported as percentages for categorical variables and as means with standard deviations (±SD) or medians with interquartile ranges (25th; 75th percentile) for continuous variables, as appropriate. Categorical variables were compared with chi-square or Fisher's exact tests, and continuous variables were compared with a parametric Student's t-test or non-parametric Wilcoxon-Mann-Whitney-Test. The AQP5 −1364A/C SNP distributions were tested for deviations from the Hardy–Weinberg equilibrium (exact two-sided P-value; significance value, 0.05). Explorative comparisons based on AQP5 −1364A/C genotypes (AC/CC vs. AA) were performed for several clinical patient characteristics (Table 1).
CMV infection probabilities were graphically assessed by the Kaplan–Meier method. The log-rank test was used to evaluate the univariate relationship between the AQP5 −1364A/C genotype and incidence of CMV infection. Next, we performed Cox regression analyses assessing the joint effect of the AQP5 −1364A/C genotype and potential predictors on CMV-free survival. At first, Cox regression was performed with several models based on a single predictor (Table 3, left column). Thereafter, multiple variable Cox regression was performed with an initial model investigating multiple predictors simultaneously (Table 3, right column). To avoid overfitting, a restricted model with only four predictors was assessed subsequently using only those predictors with a P-value 0.05 or lower based on either the single or multiple predictor comparisons (Table 4). Confidence intervals (CI) were calculated with a coverage of 95%. All reported P-values were nominal and two-sided with an a priori α error of <0.05. All analyses were performed using SPSS (version 24, IBM, USA); for graphical presentations, GraphPad Prism 7 (Graph-Pad, USA) was used.
Results
The baseline characteristics of the 259 kidney transplant recipients stratified for the AQP5 −1364A/C promoter SNP are presented in Table 1. The mean age of the recipients at the time of transplantation was 53.2 ± 12.2 years and most were male (63.7%; 165/259). The observed 1-year CMV infection rate of the entire cohort was 28.1% (73/259) and the median duration of CMV infection onset after transplantation was 150 days [90; 217]. Regarding the distribution of genetic variations according to the Hardy–Weinberg equilibrium of the AQP5 SNPs, we observed a frequency of 188 for the AA-genotype (expected: n = 186), 63 for the AC-genotype (expected: n = 67), and eight for the CC-genotype (expected: n = 6) in our cohort. Accordingly, no deviation from the Hardy–Weinberg equilibrium was observed (p = 0.8475).
In addition, 69.9% (181/259) received a kidney and 30.1% (78/259) received a combined pancreas and kidney transplantation, without statistically significant distribution among AA and AC/CC genotypes (p = 0.908; Table 1). Furthermore, we found no evidence of statistically significant associations between the AQP5 −1364A/C genotypes and age (p = 0.890), sex (p = 0.908), etiology of end-stage renal disease (p = 0.675), rate of pre-transplantation renal replacement therapy (p = 0.922), delayed graft function (p = 0.454), and CMV serology at transplantation (p = 0.973). Cases of ganciclovir-resistant CMV strains were not detected among the study patients.
One-year CMV infection risk was significantly associated with the AQP5 −1364A/C genotypes (p = 0.001; Figure 1). CMV infection rates were 23% (43/188) for the AA genotype and 42% (30/71; p = 0.001) for the AC/CC genotypes. In addition, CMV disease was more common in individuals with the AC/CC genotypes (15.5%; 11/71), when compared to the association with the AA genotype (5.3%; 10/188; p = 0.007). Further, stratifying patients according to the presence of CMV infections and CMV-associated diseases, there were no statistically significant differences between the AC (39.7%; 25/63 and 14.2%; 9/63, respectively) and CC (62.5%; 5/8; p = 0.269 and 25.0%; 2/8; p = 0.601, respectively) genotypes (Table 2).
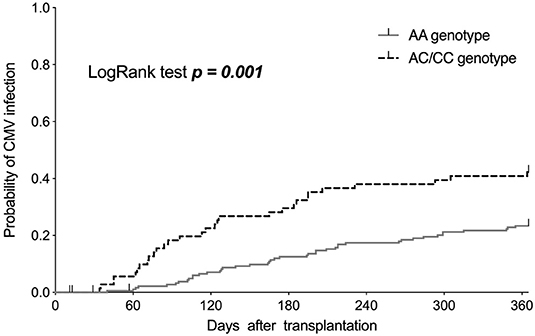
Figure 1. Kaplan–Meier curves showing the incidence of cytomegalovirus (CMV) infections in the first year after kidney transplantation, stratified based on the AA and AC/CC genotypes of the AQP5 −1364A/C single nucleotide polymorphism.
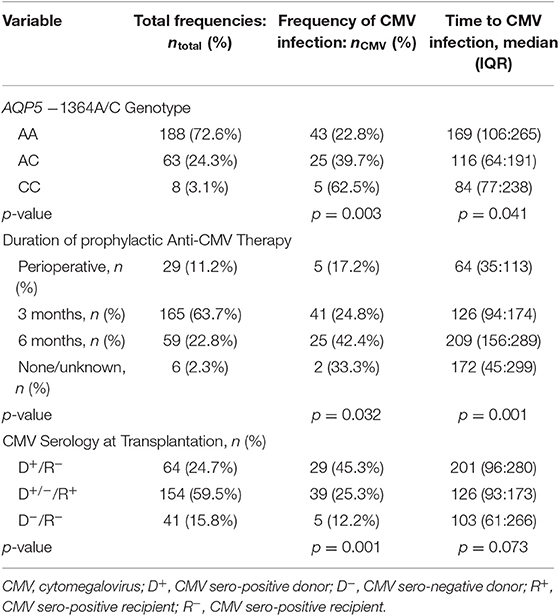
Table 2. Characteristics of kidney transplantation recipients (n = 259) stratified by frequencies and time of CMV infection onset.
Multivariate Cox regression analysis revealed the AQP5 −1364A/C genotype was both an independent and strong (due to the estimated effect size) risk factor for CMV infection (Tables 3, 4). In this context, C-allele carriers had a more than 2-fold greater risk of CMV infection in the first year after kidney transplantation (hazard ratio 2.28; 95% CI: 1.40–3.73; p = 0.001) compared to that with the AA genotype. Furthermore, the D+/R− CMV serostatus (hazard ratio 8.61; 95% CI: 2.0–5.7; p = 0.003) was confirmed as an important risk factor for CMV infection based on our cox-regression model.
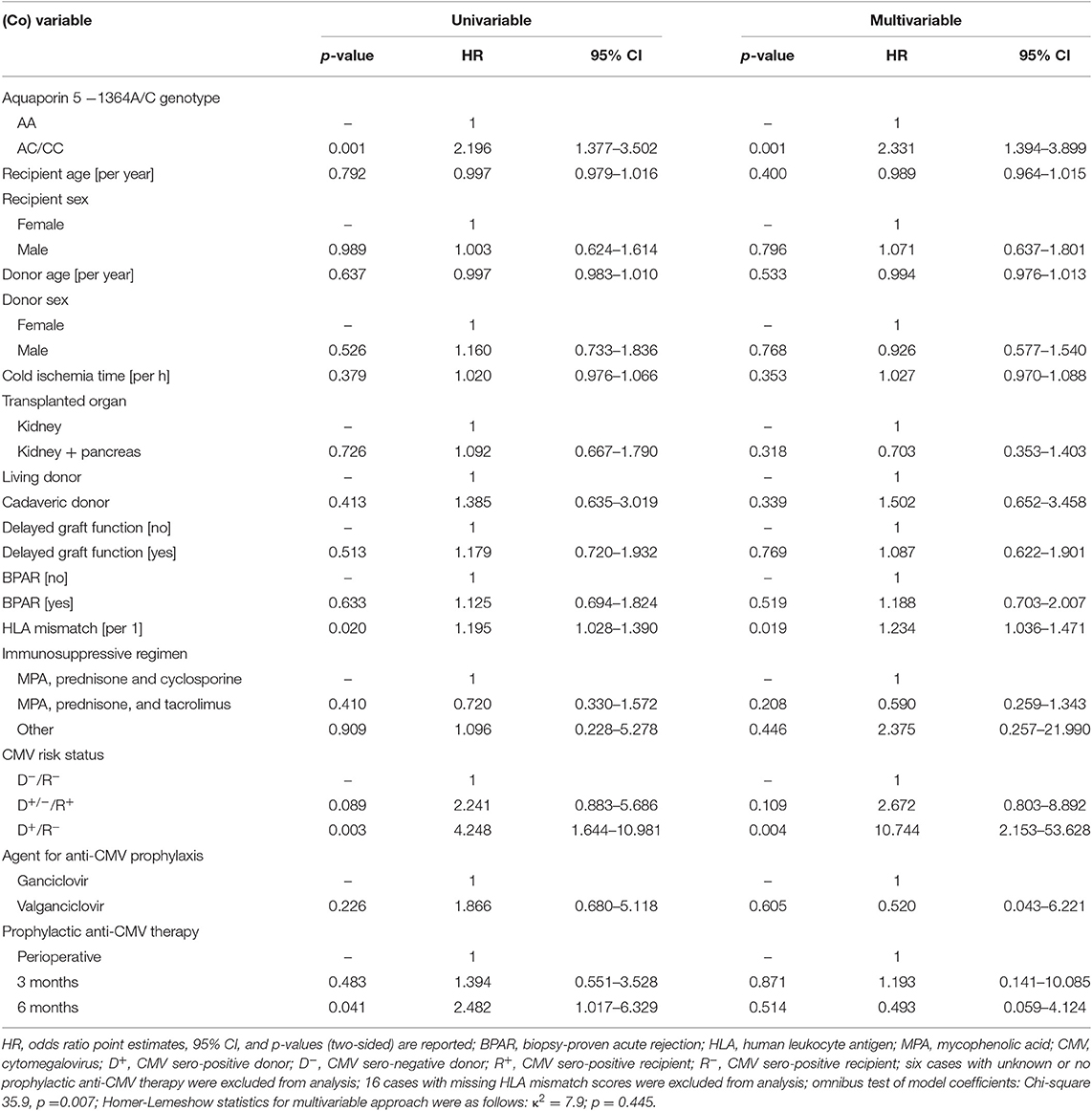
Table 3. Univariable and multivariable Cox regression analysis of kidney transplantation recipients regarding the effect on cytomegalovirus infection risk.
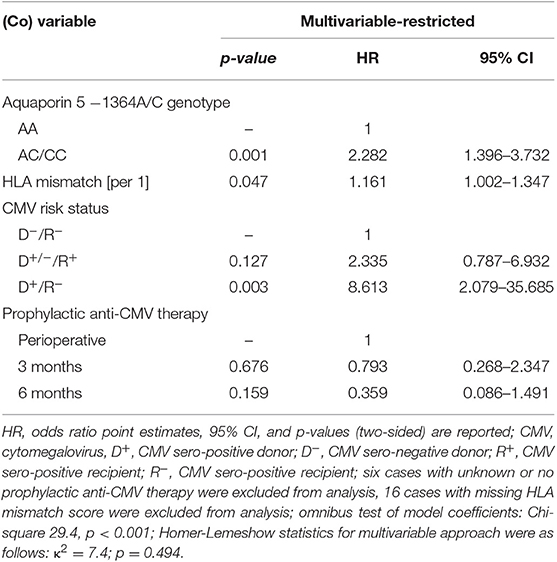
Table 4. Restricted multivariable Cox regression analysis of kidney transplantation recipients with respect to the effect on cytomegalovirus infection risk.
Strikingly, the duration of prophylactic anti-CMV therapy did not seem to affect the sustainably of the 1-year CMV infection risk (Table 4, Figure 2). In this context our Kaplan–Meier estimations showed the highest CMV infection rate after 1 year in patients treated with anti-CMV chemoprophylaxis for 6 months (42%, 25/59) compared to that with treatment for 3 months (25%; 41/165) and only perioperative treatment (17.2%; 5/29, p = 0.043).
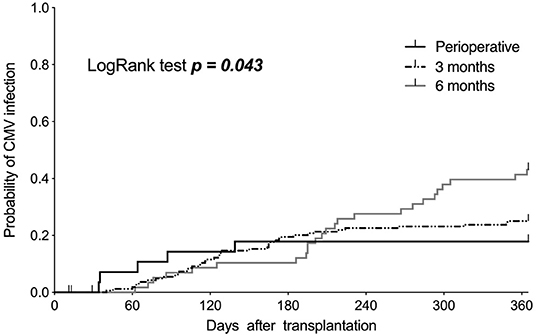
Figure 2. Kaplan–Meier curves showing the incidence of cytomegalovirus (CMV) infections in the first year after kidney transplantation, stratified based on the duration of applied anti-CMV prophylaxis.
Discussion
This study shows that the C-allele of the AQP5 −1364/A/C single nucleotide promoter polymorphism is associated with a marked increase in CMV infection and CMV disease risk in the first year after kidney transplantation. Furthermore, this SNP represents an independent and clinically meaningful risk factor of post-transplant CMV infection, with an estimated hazard ratio of nearly 2.3 for the AC/CC-genotypes. Hence, the AQP5 −1364A/C promoter SNP might play a pivotal role in the management of post-transplantation CMV prophylaxis.
Since CMV infections continue to have a tremendous effect on outcome in kidney transplant recipients, anti-CMV chemoprophylaxis is a cornerstone of modern post-transplantation management (2). Antiviral prophylaxis involves the administration of antiviral drugs, preferably valganciclovir (15), to all patients at-risk of CMV infection, and is given for up to 6 months, in accordance with the IMPACT trial (16). In this context, the decision on antiviral prophylaxis duration is usually based only on the serostatus of the donor and recipient. However, one major drawback of current antiviral chemoprophylaxis is late-onset CMV infection and disease that is most commonly observed among high-risk CMV D+/R− patients after the completion of antiviral prophylaxis (17). This is in line with our results demonstrating a median CMV infection onset time of 129 and 209 days after receiving prophylactic anti-CMV therapy for 3 and 6 months, respectively. Therefore, most cases of CMV infections in patients who received antiviral prophylaxis occur after the cessation of antiviral drug administration, and still predominantly occur in the high-risk D+/R− group (17, 18). In this regard, we also found the highest infection rate of 42% 1 year after transplantation, despite the fact that anti-CMV chemoprophylaxis was applied for 6 months in 92% of the D+/R− cases. Thus, there seems to be room to further improve the current anti-CMV approaches for post-transplantation management (19, 20). In this context, a recent study elucidates that assessing the cell-mediated anti-CMV immunity could help to identify patients at-risk of developing late-onset CMV infections supporting a guided decision-making to safely stop or better continue antiviral treatment (21). Hence, advances in the field of post-transplantation anti-CMV management will partly be facilitated by the development of first, a better diagnostic assay including genetic variations to the stratify risk of CMV infection, and second, new antiviral agents with unique mechanisms of action and ideally less toxicity.
A promising candidate for further investigation is the common AQP5 −1364A/C promoter SNP, potentially addressing the aforementioned issues. Obviously, the exact mechanisms associated with genotype-related increased mortality, associated with the AA and AC/CC genotypes, cannot be pinpointed by our study due to absence of profound mechanistical and immunological examinations. However, based on our clinical data and considering previous evidence (8, 22, 23), we speculate that the AQP5 −1364A/C SNP or rather altered AQP5 expression might shape the efficiency of immune responses, thereby influencing the efficacy of microbial clearance, and with respect to our study, CMV elimination.
The immune response to CMV infection is highly complex and includes innate and adaptive immune responses (24). Accordingly, CMV infection is first detected by the innate immune system, which seems to be crucial during the early phase of an CMV infection (25). Surprisingly, an important role has been suggested for neutrophils as potent antiviral effector cells that restrict viral replication and associated pathogenesis (26). In this context, it is of note that AQP5 expression significantly affects the migration and associated activity of neutrophil granulocytes (8, 10). AQP5-knockout mice exhibit the attenuated migration of neutrophil granulocytes, which was also associated with higher survival compared to those in wild-type animals after intraperitoneal LPS injection (8). Furthermore, the target-oriented migration of human neutrophils in vitro was found to be slower and occurred to a lesser extent with reduced AQP-5 expression. In patients suffering from acute respiratory distress syndrome, attributed to bacterial pneumonia, the AA genotype of the AQP5 promoter SNP was associated with aggravated pulmonary inflammation accompanied by a significant increase in neutrophil counts in the bronchoalveolar lavage fluid (10). Thus, the AA-genotype of the AQP5 genotype seems likely to be associated with better neutrophil granulocyte reactivity, which could at least in part explain the lower risk of CMV infection described by this study.
In addition, the sustained control of CMV infection is largely driven by adaptive immunity, involving broadly targeted CMV-specific T-cells to achieve viral control (27). Furthermore, patients with the delayed emergence of CMV-specific CD4+ T-helper cells are more likely to develop a CMV infection (28). In addition, evidence from kidney transplantation has confirmed that the frequency of CMV-specific T-helper cells is inversely correlated with the incidences of CMV replication, high CMV load, and onset of CMV-related disease (29–31).
Strikingly, AQP5 expression also seems to profoundly affect the T-cell response. A recent study demonstrated that T-cell specific cytokines are significantly down-regulated in AQP5-knockout mice (32), thus suggesting the crucial contribution of AQP5 to the effectiveness of T-cell driven immune responses. More recently, the relationship between the AQP5 deletion and elevated IFN-α and IL-2 production was shown, indicating an effect on the shift from type 2 T-helper cells toward a type 1 phenotype (33). Considering these results, it can be suggested that the AQP5 −1364A/C promoter SNP critically shapes the innate and adaptive immune response in response to CMV infections. These hypotheses are in line with our results demonstrating that AC/CC genotypes of the AQP5 −1364A/C SNP are strong and independent risk factors of CMV infection, as compared to the risk with AA genotypes.
Our results could be considered contradictory as the AA genotype of the AQP5 −1364A/C SNP was found to be associated with worse outcome in our previous studies on sepsis (11) and ARDS (10). In contrast, the present study reports that the AA-genotype can diminish the risk of CMV infection and thus can potentially confer protective effects for kidney transplant recipients. However, sepsis and ARDS are phenomena in which an exaggerated immune response prevails, and therefore, the collateral damage observed with AA genotypes would be in the foreground and caused by a more potent immune system. In kidney transplantation recipients, exactly the opposite must be presumed, because of the profound immunosuppression. In this context, the enhanced immunoreactivity observed with the AA genotypes might mediate immunological benefits in immunosuppressed patients.
Nevertheless, these relationships, and especially the mechanistic associations, must be elucidated in the future, since this approach might also offer a new therapeutic target. In this context, it has been demonstrated that dexamethasone and ambroxol can upregulate AQP-5 expression in-vitro (34). Modulating AQP5 expression depending on the genotype could be an interesting focal point for additional or rather optimized CMV prophylactic strategies. However, whether this approach offers therapeutic or prophylactic benefits, needs to be elucidated in future investigations.
Limitations
The limitations of this study must also be mentioned. First, unrecognized selection bias, inherent to many genetic association studies, cannot be entirely excluded. Second, our study was almost exclusively conducted on patients of European-Caucasian descent, and therefore, findings cannot be generalized to subjects of other ancestries. Third, although all patients were treated with a rather standardized multimodal regimen, undetected confounding factors might have distorted the results because of the multidimensionality of solid organ transplantation, immunosuppression, and immune responses against CMV infection. However, the single center nature of this study might be an advantage as it limits the varied protocols that can be used when treating kidney transplant recipients. Finally, the observational design, the absence of a reasonable control group, and lack of histologic and mechanistic examinations precludes verification of the causality and underlying mechanisms. Additional studies, especially to uncover mechanistic insights, are needed to further asses the effect of AQP5 expression on inflammation and immune cell migration, as it relates to CMV infection risk.
Conclusions
During opportunistic CMV infections attributed to immunosuppression after kidney transplantation, the C-allele of the AQP5 −1364A/C promoter polymorphism is independently associated with an increased 12-months infection risk. These findings emphasize the importance of genetic variations as additional risk factors of CMV infection after solid organ transplantation, which might also facilitate the discovery of novel therapeutic targets. Consequently, increasing AQP5 expression in AC and CC genotypes could be an interesting therapeutic approach for organ transplant recipients.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
Author Contributions
TR, HN, PS, RV, MA, and LB: conceived and designed the research. SF, TR, HN, KR, BK, and LB: performed the experiments. KR and BK: contributed the reagents. TR, SF, PS, RV, MA, and LB: collected and provided the clinical data. TR, HN, BK, PS, MA, and LB: interpreted the data. TR, HN, MA, and LB: performed the statistical analysis. TR, HN, PS, and LB: wrote the initial draft. All authors critically revised and approved the manuscript and are accountable for the accuracy and integrity of the work.
Funding
We acknowledge support by the DFG Open Access Publication Funds of the Ruhr-University Bochum (Ref. No. IN-1214264), just for financial support for publication charges. This had no impact on our study design or collection, analysis, and interpretation of our data. Further support was provided solely from institutional and/or departmental sources.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank Thomas Klein (Klinik für Chirurgie, Universitätsklinikum Knappschaftskrankenhaus Bochum, Bochum Germany), Svenja Vornweg (Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie, Universitätsklinikum Knappschaftskrankenhaus Bochum, Bochum), and SF (Klinik für Anästhesiologie, Intensivmedizin und Schmerztherapie, Universitätsklinikum Knappschaftskrankenhaus Bochum, Bochum) for supporting patient recruitment, study inclusion, and genotyping.
References
1. Fishman JA, Rubin RH. Infection in organ-transplant recipients. N Engl J Med. (1998) 338:1741–51. doi: 10.1056/NEJM199806113382407
2. Kotton CN, Kumar D, Caliendo AM, Huprikar S, Chou S, Danziger-Isakov L, et al. The third international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. (2018) 102:900–31. doi: 10.1097/TP.0000000000002191
3. Fehr T, Cippa PE, Mueller NJ. Cytomegalovirus post kidney transplantation: prophylaxis versus pre-emptive therapy? Transpl Int. (2015) 28:1351–6. doi: 10.1111/tri.12629
4. Gjertson DW. Look-up survival tables for living-donor renal transplants: OPTN/UNOS data 1995–2002. Clin Transpl. (2003) 5:337–86.
5. Fernandez-Ruiz M, Corrales I, Arias M, Campistol JM, Gimenez E, Crespo J, et al. Association between individual and combined SNPs in genes related to innate immunity and incidence of CMV infection in seropositive kidney transplant recipients. Am J Transplant. (2015) 15:1323–35. doi: 10.1111/ajt.13107
6. Adamzik M, Frey UH, Bitzer K, Jakob H, Baba HA, Schmieder RE, et al. A novel-1364A/C aquaporin 5 gene promoter polymorphism influences the responses to salt loading of the renin-angiotensin-aldosterone system and of blood pressure in young healthy men. Basic Res Cardiol. (2008) 103:598–610. doi: 10.1007/s00395-008-0750-z
7. Papadopoulos MC, Saadoun S, Verkman AS. Aquaporins and cell migration. Pflugers Arch. (2008) 456:693–700. doi: 10.1007/s00424-007-0357-5
8. Rump K, Unterberg M, Bergmann L, Bankfalvi A, Menon A, Schafer S, et al. AQP5-1364A/C polymorphism and the AQP5 expression influence sepsis survival and immune cell migration: a prospective laboratory and patient study. J Transl Med. (2016) 14:321. doi: 10.1186/s12967-016-1079-2
9. Towne JE, Krane CM, Bachurski CJ, Menon AG. Tumor necrosis factor-alpha inhibits aquaporin 5 expression in mouse lung epithelial cells. J Biol Chem. (2001) 276:18657–64. doi: 10.1074/jbc.M100322200
10. Rahmel T, Rump K, Peters J, Adamzik M. Aquaporin 5-1364A/C promoter polymorphism is associated with pulmonary inflammation and survival in acute respiratory distress syndrome. Anesthesiology. (2019) 130:404–13. doi: 10.1097/ALN.0000000000002560
11. Adamzik M, Frey UH, Mohlenkamp S, Scherag A, Waydhas C, Marggraf G, et al. Aquaporin 5 gene promoter-1364A/C polymorphism associated with 30-day survival in severe sepsis. Anesthesiology. (2011) 114:912–7. doi: 10.1097/ALN.0b013e31820ca911
12. Rahmel T, Nowak H, Rump K, Siffert W, Peters J, Adamzik M. The aquaporin 5-1364A/C promoter polymorphism impacts on resolution of acute kidney injury in pneumonia evoked ARDS. PLoS ONE. (2018) 13:e0208582. doi: 10.1371/journal.pone.0208582
13. Zhang ZQ, Song YL, Chen ZH, Shen Y, Bai CX. Deletion of aquaporin 5 aggravates acute lung injury induced by Pseudomonas aeruginosa. J Trauma. (2011) 71:1305–11. doi: 10.1097/TA.0b013e3182128528
14. Ljungman P, Boeckh M, Hirsch HH, Josephson F, Lundgren J, Nichols G, et al. Definitions of cytomegalovirus infection and disease in transplant patients for use in clinical trials. Clin Infect Dis. (2017) 64:87–91. doi: 10.1093/cid/ciw668
15. Paya C, Humar A, Dominguez E, Washburn K, Blumberg E, Alexander B, et al. Efficacy and safety of valganciclovir vs. oral ganciclovir for prevention of cytomegalovirus disease in solid organ transplant recipients. Am J Transplant. (2004) 4:611–20. doi: 10.1111/j.1600-6143.2004.00382.x
16. Humar A, Lebranchu Y, Vincenti F, Blumberg EA, Punch JD, Limaye AP, et al. The efficacy and safety of 200 days valganciclovir cytomegalovirus prophylaxis in high-risk kidney transplant recipients. Am J Transplant. (2010) 10:1228–37. doi: 10.1111/j.1600-6143.2010.03074.x
17. Harvala H, Stewart C, Muller K, Burns S, Marson L, MacGilchrist A, et al. High risk of cytomegalovirus infection following solid organ transplantation despite prophylactic therapy. J Med Virol. (2013) 85:893–8. doi: 10.1002/jmv.23539
18. Arthurs SK, Eid AJ, Pedersen RA, Kremers WK, Cosio FG, Patel R, et al. Delayed-onset primary cytomegalovirus disease and the risk of allograft failure and mortality after kidney transplantation. Clin Infect Dis. (2008) 46:840–6. doi: 10.1086/528718
19. Lisboa LF, Preiksaitis JK, Humar A, Kumar D. Clinical utility of molecular surveillance for cytomegalovirus after antiviral prophylaxis in high-risk solid organ transplant recipients. Transplantation. (2011) 92:1063–8. doi: 10.1097/TP.0b013e31822fa4b7
20. Kumar D, Mian M, Singer L, Humar A. An interventional study using cell-mediated immunity to personalize therapy for cytomegalovirus infection after transplantation. Am J Transplant. (2017) 17:2468–73. doi: 10.1111/ajt.14347
21. Jarque M, Melilli E, Crespo E, Manonelles A, Montero N, Torras J, et al. CMV-specific cell-mediated immunity at 3-month prophylaxis withdrawal discriminates D+/R+ kidney transplants at risk of late-onset CMV infection regardless the type of induction therapy. Transplantation. (2018) 102:e472–80. doi: 10.1097/TP.0000000000002421
22. Rump K, Adamzik M. Function of aquaporins in sepsis: a systematic review. Cell Biosci. (2018) 8:10. doi: 10.1186/s13578-018-0211-9
23. Meli R, Pirozzi C, Pelagalli A. New perspectives on the potential role of aquaporins (AQPs) in the physiology of inflammation. Front Physiol. (2018) 9:101. doi: 10.3389/fphys.2018.00101
24. Carbone J. The immunology of posttransplant CMV infection: potential effect of CMV immunoglobulins on distinct components of the immune response to CMV. Transplantation. (2016) 100:S11–8. doi: 10.1097/TP.0000000000001095
25. Boehme KW, Guerrero M, Compton T. Human cytomegalovirus envelope glycoproteins B and H are necessary for TLR2 activation in permissive cells. J Immunol. (2006) 177:7094–102. doi: 10.4049/jimmunol.177.10.7094
26. Stacey MA, Marsden M, Pham NT, Clare S, Dolton G, Stack G, et al. Neutrophils recruited by IL-22 in peripheral tissues function as TRAIL-dependent antiviral effectors against MCMV. Cell Host Microbe. (2014) 15:471–83. doi: 10.1016/j.chom.2014.03.003
27. Sylwester AW, Mitchell BL, Edgar JB, Taormina C, Pelte C, Ruchti F, et al. Broadly targeted human cytomegalovirus-specific CD4+ and CD8+ T cells dominate the memory compartments of exposed subjects. J Exp Med. (2005) 202:673–85. doi: 10.1084/jem.20050882
28. van Leeuwen EM, Remmerswaal EB, Vossen MT, Rowshani AT, Wertheim-van Dillen PM, van Lier RA, et al. Emergence of a CD4+CD28− granzyme B+, cytomegalovirus-specific T cell subset after recovery of primary cytomegalovirus infection. J Immunol. (2004) 173:1834–41. doi: 10.4049/jimmunol.173.3.1834
29. Sester M, Sester U, Gartner B, Heine G, Girndt M, Mueller-Lantzsch N, et al. Levels of virus-specific CD4 T cells correlate with cytomegalovirus control and predict virus-induced disease after renal transplantation. Transplantation. (2001) 71:1287–94. doi: 10.1097/00007890-200105150-00018
30. Tu W, Potena L, Stepick-Biek P, Liu L, Dionis KY, Luikart H, et al. T-cell immunity to subclinical cytomegalovirus infection reduces cardiac allograft disease. Circulation. (2006) 114:1608–15. doi: 10.1161/CIRCULATIONAHA.105.607549
31. Egli A, Binet I, Binggeli S, Jager C, Dumoulin A, Schaub S, et al. Cytomegalovirus-specific T-cell responses and viral replication in kidney transplant recipients. J Transl Med. (2008) 6:29. doi: 10.1186/1479-5876-6-29
32. Karras JG, Crosby JR, Guha M, Tung D, Miller DA, Gaarde WA, et al. Anti-inflammatory activity of inhaled IL-4 receptor-alpha antisense oligonucleotide in mice. Am J Respir Cell Mol Biol. (2007) 36:276–85. doi: 10.1165/rcmb.2005-0456OC
33. Shen Y, Wang Y, Chen Z, Wang D, Wang X, Jin M, et al. Role of aquaporin 5 in antigen-induced airway inflammation and mucous hyperproduction in mice. J Cell Mol Med. (2011) 15:1355–63. doi: 10.1111/j.1582-4934.2010.01103.x
Keywords: AQP5, single nucleotide polymorphism (SNP), cytomegalovirus, immunosuppression, infection risk, kidney transplantation
Citation: Rahmel T, Nowak H, Frisenda S, Rump K, Koos B, Schenker P, Viebahn R, Adamzik M and Bergmann L (2019) The Aquaporin 5 −1364A/C Promoter Polymorphism Is Associated With Cytomegalovirus Infection Risk in Kidney Transplant Recipients. Front. Immunol. 10:2871. doi: 10.3389/fimmu.2019.02871
Received: 28 March 2019; Accepted: 22 November 2019;
Published: 05 December 2019.
Edited by:
Guseppe Grandaliano, University of Foggia, ItalyReviewed by:
Josep M. Grinyó, University of Barcelona, SpainFabian Dusse, University Hospital of Cologne, Germany
Copyright © 2019 Rahmel, Nowak, Frisenda, Rump, Koos, Schenker, Viebahn, Adamzik and Bergmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tim Rahmel, dGltLnJhaG1lbEBydWhyLXVuaS1ib2NodW0uZGU=
†These authors have contributed equally to this work