 France A. V. Pirson1*
France A. V. Pirson1* Wouter H. Hinsenveld1
Wouter H. Hinsenveld1 Julie Staals1Inger R. de Ridder1
Julie Staals1Inger R. de Ridder1 Wim H. van Zwam2Tobien H. C. M. L. Schreuder3
Wim H. van Zwam2Tobien H. C. M. L. Schreuder3 Yvo B. W. E. M. Roos4
Yvo B. W. E. M. Roos4 Charles B. L. M. Majoie5
Charles B. L. M. Majoie5 H. Bart van der Worp6
H. Bart van der Worp6 Maarten Uyttenboogaart7Geert J. Lycklama à Nijeholt8Wouter J. Schonewille9
Maarten Uyttenboogaart7Geert J. Lycklama à Nijeholt8Wouter J. Schonewille9 Robert J. van Oostenbrugge1 on behalf of MR CLEAN Registry Investigators
Robert J. van Oostenbrugge1 on behalf of MR CLEAN Registry Investigators- 1Department of Neurology, Maastricht University Medical Center, Maastricht, Netherlands
- 2Department of Radiology, Maastricht University Medical Center, Maastricht, Netherlands
- 3Department of Neurology, Zuyderland Medical Center, Heerlen, Netherlands
- 4Department of Neurology, Amsterdam University Medical Center, Amsterdam, Netherlands
- 5Department of Radiology and Nuclear Medicine, Amsterdam University Medical Center, Amsterdam, Netherlands
- 6Department of Neurology and Neurosurgery, Brain Center, University Medical Center Utrecht, Utrecht, Netherlands
- 7Department of Neurology and Radiology, University Medical Center Groningen, Groningen, Netherlands
- 8Department of Radiology, Haaglanden Medical Center, The Hague, Netherlands
- 9Department of Neurology, Sint Antonius Hospital, Nieuwegein, Netherlands
Background and Purpose: Though peripheral artery disease (PAD) is a well-known risk factor for ischemic events, better outcomes have been described in acute ischemic stroke patients with co-existing PAD. This paradoxical association has been attributed to remote ischemic preconditioning (RIPC) and might be related to better collateral blood flow. The aim of this study is to compare outcomes after endovascular thrombectomy (EVT) in acute stroke patients with and without PAD and to assess the relation between PAD and collateral grades.
Methods: We analyzed acute ischemic stroke patients treated with EVT for an anterior circulation large artery occlusion, included in the Dutch, prospective, multicenter MR CLEAN Registry between March 2014 and November 2017. Collaterals were scored on CT angiography, using a 4-point collateral score. We used logistic regression analysis to estimate the association of PAD with collateral grades and functional outcome, assessed with the modified Rankin Scale (mRS) at 90 days. Safety outcomes included mortality at 90 days, symptomatic intracranial hemorrhage, and stroke progression.
Results: We included 2,765 patients for analysis, of whom 254 (9.2%) had PAD. After adjustment for potential confounders, multivariable regression analysis showed no association of PAD with functional outcome [mRS cOR 0.90 (95% CI, 0.7–1.2)], collateral grades (cOR 0.85, 95% CI 0.7–1.1), or safety outcomes.
Conclusion: In the absence of an association between the presence of PAD and collateral scores or outcomes after EVT, it may be questioned whether PAD leads to RIPC in patients with acute ischemic stroke due to large vessel occlusion.
Introduction
Patients with previous transient ischemic attacks seem to have smaller infarct sizes and better outcomes after subsequent cerebral infarction than patients without (1, 2). This phenomenon, in which brief periods of hypoperfusion offer protection in case of subsequent prolonged ischemia, is called ischemic preconditioning. The underlying etiology is not fully understood but seems to rely on systemic immunoreactivity and metabolic changes (3).
Animal studies have suggested that a similar neuroprotective effect occurs when hypoperfusion is induced in an organ other than the brain; so-called remote ischemic preconditioning (RIPC) (4, 5). In clinical setting, a randomized controlled trial in patients with ischemic stroke treated with intravenous thrombolysis demonstrated that RIPC induced by intermittently inflating a tourniquet on one of the limbs led to smaller perfusion deficits or DWI lesions (6). However, this trial did not show effect on clinical outcome at 3 months.
Peripheral artery disease (PAD) can be regarded as a chronic remote preconditioning process. So far there are conflicting results in studies with acute stroke patients on the relation between PAD and outcome. A small retrospective case-control study found that patients with ischemic stroke who had PAD had smaller infarct volumes, better functional outcomes, and a reduced risk of death (7). On the contrary, worse outcomes have been reported in stroke patients with low ankle-brachial index (ABI), which is a measure for PAD (8).
In a mouse model of ischemic stroke, RIPC led to better cerebral blood flow and the prevention of collateral artery collapse (9, 10). Whether pre-existent PAD affects the extensiveness of collaterals in humans is unknown. Since multiple studies have shown that higher collateral grades are associated with better functional outcome after endovascular treatment (EVT) in acute ischemic stroke, PAD may have a positive effect on outcome through better collateral blood flow (11–13).
The aim of our present study is (1) to investigate if pre-existent PAD is associated with better functional outcome in acute stroke patients treated with EVT, and (2) to investigate if PAD is correlated with collateral grades on CTA before EVT.
Methods
Study Design and Patients
The MR CLEAN Registry is a prospective, nationwide registry, in which data are collected from consecutive acute stroke patients treated with EVT in the Netherlands. The study protocol has been evaluated by the medical ethics committee of the Erasmus MC in Rotterdam, and permission to carry out the study as a registry was granted. Full methods of the MR CLEAN Registry have been reported previously (14). EVT consisted of mechanical thrombectomy, thrombus aspiration, or a combination of both. The method of EVT for each patient was left to the discretion of the treating physicians. For the present study, we used data of patients who underwent EVT from March 2014 up to November 2017 meeting the following inclusion criteria: groin puncture within 6.5 hours after symptom onset; age > 18; occlusion of intracranial carotid (ICA, ICA-T), middle (M1/M2), or anterior (A1/A2) cerebral artery, demonstrated by baseline CT angiography (CTA). Patients with missing information on PAD were excluded from assessment.
Source data will not be made available because of legislator issues on patient privacy, but detailed analytic methods and study materials, including log files of statistical analyses, will be made available to other researchers on reasonable request to the first author.
Peripheral Artery Disease Assessment
PAD as well as other vascular risk factors were recorded as baseline parameters. These risk factors were mainly obtained from patient records, in which the diagnoses were recorded by the treating physicians. PAD could include vascular claudication or critical limb ischemia for which an intervention might have been performed.
Imaging Assessment
All imaging was assessed by an imaging core laboratory, whose members were blinded to clinical findings, except for side of symptoms. Collateral status was graded on baseline CTA using a 4-point scale, with 0 for absent collaterals (0% filling of the occluded vascular territory), 1 for poor collaterals (>0% and ≤ 50% filling), 2 for moderate (>50% and <100% filling), and 3 for good collaterals (100% filling) (15). Reperfusion was scored on digital subtraction angiography (DSA) by the extended Thrombolysis in Cerebral Ischemia (eTICI) score (16), which ranges from grade 0 (no reperfusion) to grade 3 (complete reperfusion). Successful reperfusion was defined as eTICI 2B or higher. Patients of whom bi-directional view on final DSA was not available (missing lateral or anterior view), were excluded from further analysis.
Outcome Assessment
The primary outcome measure was the modified Rankin Score (mRS) at 90 days, which is a 7-point scale ranging from 0 (no symptoms) to 6 (death) (17). A score of 2 points or less indicates functional independence. Secondary outcomes included functional independence, neurological deficit measured by the National Institute of Health Stroke Scale (NIHSS) at 24–48 h (18), and collateral grades. Safety outcomes included mortality at 90 days, symptomatic intracranial hemorrhage (sICH), and stroke progression. Intracranial hemorrhage was considered symptomatic if the patient had died or had deteriorated neurologically (a decline of at least four points on the NIHSS), and the hemorrhage was related to the clinical deterioration (according to Heidelberg criteria) (19).
Statistical Analysis
Baseline characteristics were described using standard statistics. For the relation between PAD and functional outcome, we used multivariable ordinal logistic regression analysis to estimate the adjusted common odds ratio (acOR) for a shift toward a better functional outcome on the mRS. For the association between PAD and collaterals, we used univariable and multivariable ordinal logistic regression. In all multivariable analysis we adjusted for potential imbalances in prespecified prognostic variables: age, sex, NIHSS at baseline, hypercholesterolemia, hypertension, diabetes mellitus, smoking, previous myocardial infarction, previous stroke (only manifest ischemic stroke), ASPECTS on baseline non-contrast CT, reperfusion grade, intracranial atherosclerosis, and atherosclerotic stenosis of the symptomatic carotid artery.
All descriptive analyses include patients with complete data, while all regression models include all patients with imputed data. STATA (version 14.1) was used for all statistical analyses.
Results
Patient Characteristics
Of the 3,180 patients in the MR CLEAN registry meeting all other inclusion criteria, 47 were excluded because of unrecorded information on PAD and 368 because of missing bi-directional view on final DSA, leaving 2,765 patients for the present post-hoc analysis. Of these, 254 (9.2%) had PAD (Figure 1).
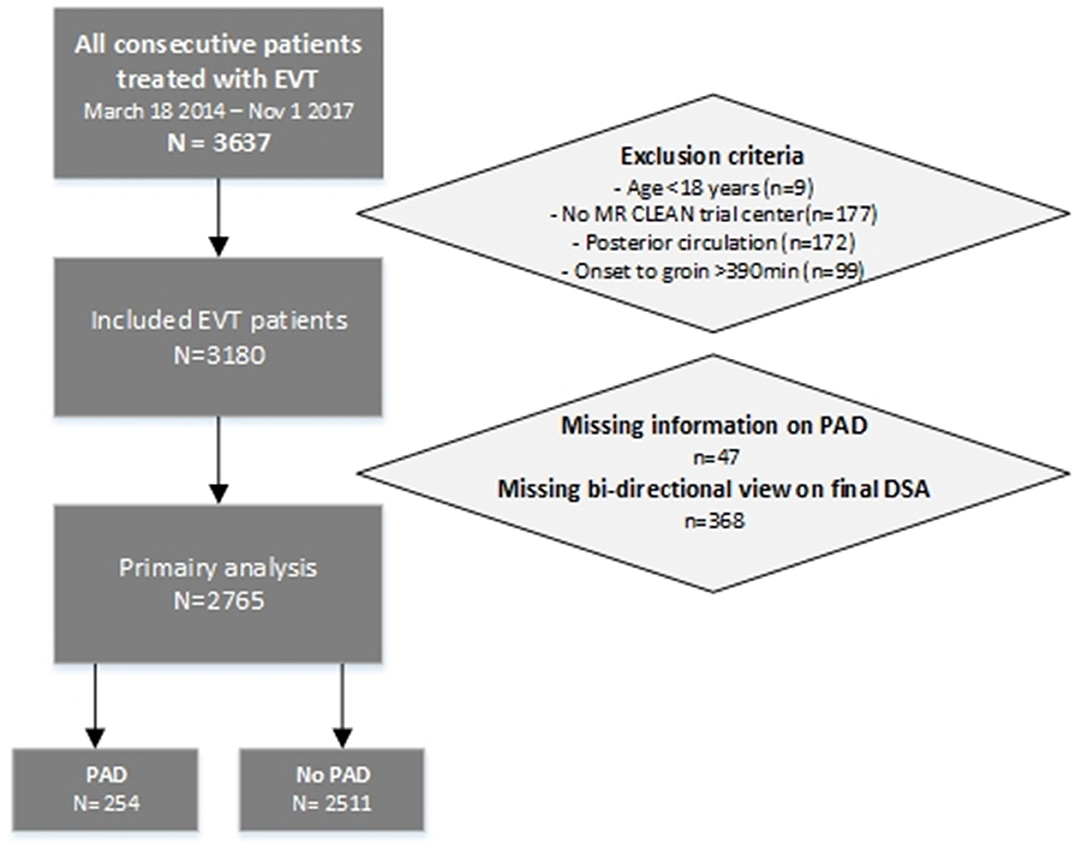
Figure 1. Flowchart patient selection.
Patients with PAD were older (median age 75 vs. 72, p < 0.02), and less often received intravenous thrombolysis (72 vs. 77%, p = 0.05) than patients without PAD (Table 1). Hypertension, myocardial infarction, hypercholesterolemia, diabetes mellitus, previous ischemic stroke, and smoking were more frequent in patients with PAD. The extent of early ischemic lesions at baseline was significantly different between groups, in favor of patients with PAD (median ASPECTS 9 (IQR 8–10) vs. 9 (IQR 7–10), p = 0.03). Patients with PAD were more likely to have intracranial atherosclerosis (76 vs. 59%, p < 0.01), and >50% atherosclerotic stenosis of the symptomatic carotid artery compared to patients without PAD (16 vs. 8%, p < 0.01). Successful reperfusion did not differ between groups (eTICI 2B-3 68 vs. 70%, p = 0.60).
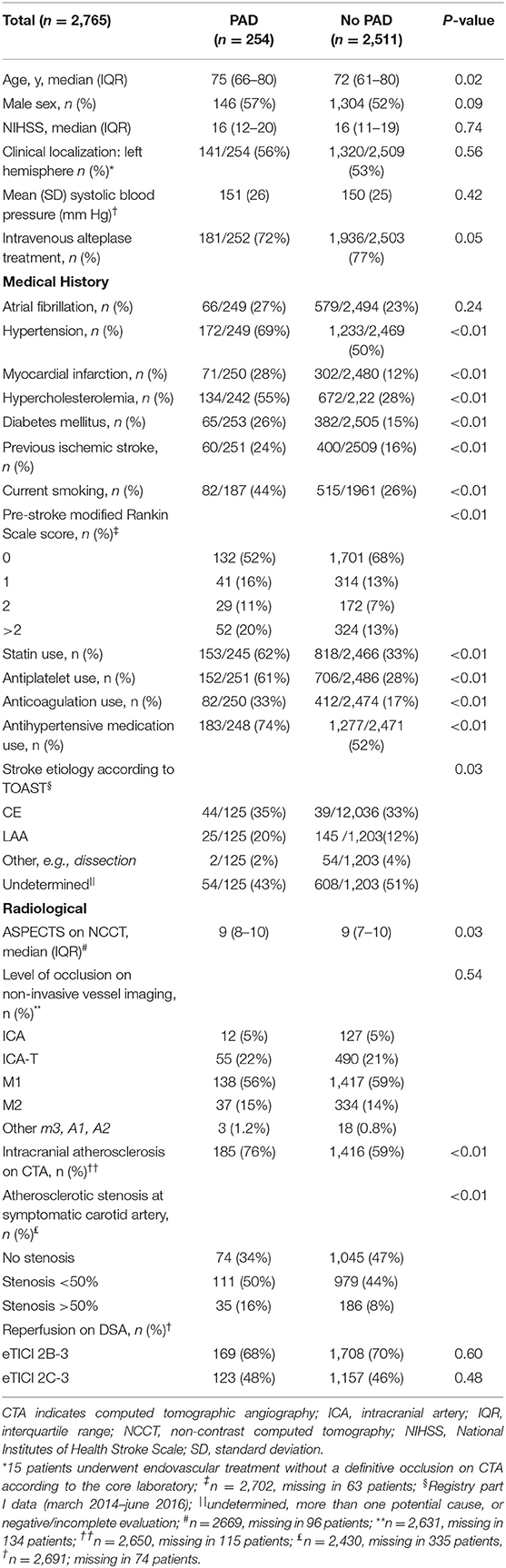
Table 1. Baseline characteristics of ischemic stroke patients with peripheral artery disease (PAD) compared with no PAD.
PAD and Outcomes
In univariable analysis, patients with PAD had worse functional outcome as compared with those without PAD (cOR 0.72, 95% CI 0.6–0.9) (Table 2). After adjustment for possible confounders, PAD was not associated with functional outcome (adjusted cOR 0.90 (95% CI, 0.7–1.2). There was no association between PAD and all other secondary outcomes: 90-days mortality (aOR 1.24, 95% CI 0.9–1.7), 24 h NIHSS (β 0.15, 95% CI −0.9–1.2), sICH (aOR 0.85, 95% CI 0.5–1.6), or stroke progression (aOR 0.99, 95% CI 0.6–1.6) (Table 2).
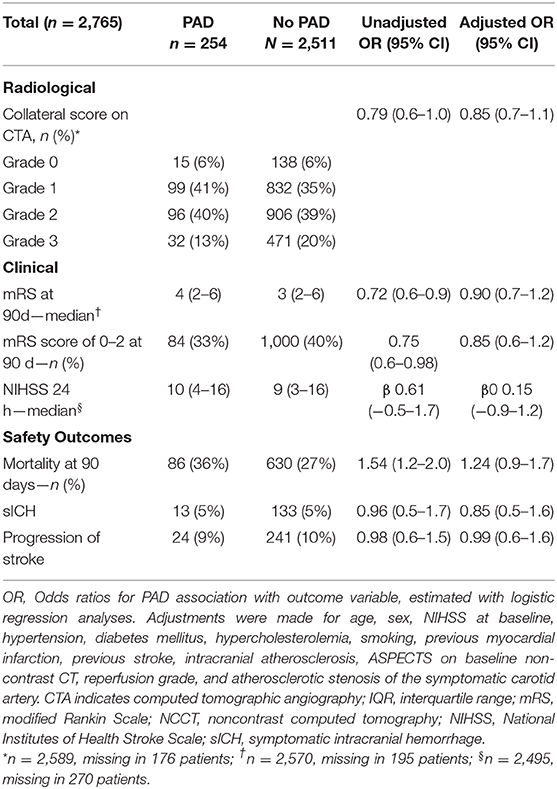
Table 2. Primary and secondary outcomes. Ischemic stroke patients with PAD compared with no PAD.
PAD and Collateral Status
In patients with PAD poor collaterals were more frequent (grade 1: 41 vs. 35%), and good collaterals were less frequent (grade 3: 13 vs. 20%) than in those without PAD (Table 1). In univariable regression analysis on the four point collateral score, this translates to an OR of 0.79 (95% CI 0.6–1.0). After adjusting for potential confounding factors, there was no significant association of PAD with collateral status (aOR 0.85, 95% CI 0.7–1.1) (Table 2).
Discussion
In this large nation-wide multicenter registry of patients with ischemic stroke treated with EVT, univariable analyses showed that PAD patients had worse collateral grades and worse functional outcomes than those without. However, after correction for possible confounders, there was no statistically significant association between PAD and functional outcome or collateral grades. As could be expected, there is a strong effect of the co-variables associated with PAD on functional outcome after EVT.
To our knowledge the association between PAD and collaterals in acute ischemic stroke has not been reported before. By comparison, ischemic stroke patients with significant carotid artery stenosis have better collateral flow on CTA than patients without carotid artery stenosis (20). In our study, patients with PAD more often had carotid artery stenosis of 50% or greater than patients without PAD, but their collateral grades were worse. This might be explained by a predominant effect of age or associated co-morbidities (21). Another contributing factor might be that nearly all patients in our study underwent single-phase CT-angiography. Assessment of collateral flow on singe phase CTA may lead to an underestimation of collaterals in case of delayed filling in combination with an early acquisition phase (12, 22). In our case, significant carotid artery stenosis could have therefore disproportionally affected the relation between PAD and collateral status through delayed intracerebral filling.
We found no association between PAD and functional outcome after ischemic stroke, in contrast to a previous case-control study (7). In that study acute stroke patients with PAD had a very low NIHSS at presentation (47% NIHSS 1–4). Our study concerns a distinct patient population with proven large vessel occlusions causing more severe strokes resulting in a rather high NIHSS and possibly less dispersion in post-stroke mRS. The influence of PAD may therefore be diminished in patients treated with EVT due to stroke severity. Another explanation might be that physicians treat less aggressively in case of persistent neurologic deficit after EVT and concomitant severe co-morbidity including PAD. With this self-fulfilling prophecy, a possible positive effect of PAD on outcome may therefore not have been investigated properly. A previous study found worse outcome after stroke in patients with low ankle-brachial index (ABI) (8). Our study did not measure ABI to determine severity of PAD. It is possible to have missed an association between severe PAD and outcome if the patients in our cohort would have had mainly moderate-to-high ABI.
The strength of our study is the large patient sample. All outcome measures have been collected prospectively according to protocol and independent of our present research question.
Nevertheless, there are limitations. First, there was no standardized assessment for peripheral artery disease which may have led to different judgment between centers or between physicians. Also, we were not able to assess the ABI in our patients. Since ABI is more reliable in identifying PAD than determination based on clinical judgment, we might have over- or underdiagnosed PAD in our cohort of ischemic stroke patients. However, previous research on PAD in stroke patients showed a comparable prevalence of around 10% (8, 23).
A second limitation concerns the presence of intracerebral atherosclerosis in our patients. Peripheral artery disease can be isolated in the lower limbs, but might also occur concurrently in the coronary arteries or cerebral arteries (24, 25). The extent of cerebral vessel atherosclerosis is associated with white-matter loss and lacunar infarctions and may therefore influence functional outcome. Although we adjusted our analysis for the presence of intracranial atherosclerosis, our model could not be corrected for the extent or specific location of this condition.
Conclusion
In summary, our study showed no association between PAD and outcome after EVT for acute ischemic stroke nor an independent association between PAD and collateral blood flow. As such, we could not confirm the occurrence of RIPC in PAD patients with acute ischemic stroke. Future studies with more standardized measurement of PAD are recommended.
Data Availability Statement
Source data will not be made available because of legislator issues on patient privacy, but detailed analytic methods and study materials, including log files of statistical analyses, will be made available to other researchers on reasonable request to the first author. Requests to access the datasets should be directed to ZmF2LnBpcnNvbkBtdW1jLm5s.
Ethics Statement
The studies involving human participants were reviewed and approved by medical ethics committee of the Erasmus MC in Rotterdam. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author's Note
MR Clean Registry Investigators are included in Supplementary Material.
Author Contributions
FP analyzed the data and wrote the first draft of the manuscript. All other authors critically reviewed the manuscript for intellectual content, read, and approved the final version of the manuscript.
Funding
The MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke) was partly funded by Stichting Toegepast Wetenschappelijk Instituut voor Neuromodulatie (TWIN), Erasmus MC University Medical Center, Maastricht University Medical Center, and Amsterdam University Medical Center.
Conflict of Interest
Erasmus MC received funds from Stryker by Diederik Dippel, Aad van der Lugt, and from Bracco Imaging by Diederik Dippel. Amsterdam UMC received funds from Stryker for consultations by CM, YR, and Olvert Berkhemer. Maastricht UMC received funds from Stryker and Cerenovus for consultations by WZ. UMC Utrecht received funds from Bayer, Boehringer Ingelheim, and LivaNova for consultation by BW.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2020.560300/full#supplementary-material
Abbreviations
ABI, ankle-brachial index; acOR, adjusted common odds ratio; ASPECTS, Alberta stroke programme early CT score; CTA, CT angiography; DSA, digital subtraction angiography; eTICI, extended Thrombolysis in Cerebral Ischemia; EVT, endovascular treatment; IQR, interquartile range; LVO, large vessel occlusion; MR CLEAN, Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands; mRS, modified Rankin Scale; NCCT, non-contrast CT; NIHSS, National Institutes of Health Stroke Scale; RIPC, Remote Ischemic Preconditioning; sICH, symptomatic intracranial hemorrhage; TOAST, Trial of Org 10172 in Acute Stroke Treatment.
References
1. Huang HL, Wang N, Zhou H, Yu CY. Study on influence of transient ischemic attack on subsequent cerebral infarction. Eur Rev Med Pharmacol Sci. (2016) 20:5164–7.
2. Zsuga J, Gesztelyi R, Juhasz B, Kemeny-Beke A, Fekete I, Csiba L, et al. Prior transient ischemic attack is independently associated with lesser in-hospital case fatality in acute stroke. Psychiatry Clin Neurosci. (2008) 62:705–12. doi: 10.1111/j.1440-1819.2008.01874.x
3. Jm. G. Cerebrovascular ischemic protection by pre-and post-conditioning. Brain Circ. (2015) 1:97–103. doi: 10.4103/2394-8108.166379
4. Hoda MN, Bhatia K, Hafez SS, Johnson MH, Siddiqui S, Ergul A, et al. Remote ischemic perconditioning is effective after embolic stroke in ovariectomized female mice. Transl Stroke Res. (2014) 5:484–90. doi: 10.1007/s12975-013-0318-6
5. Hu S, Dong H, Zhang H, Wang S, Hou L, Chen S, et al. Noninvasive limb remote ischemic preconditioning contributes neuroprotective effects via activation of adenosine a1 receptor and redox status after transient focal cerebral ischemia in rats. Brain Res. (2012) 1459:81–90. doi: 10.1016/j.brainres.2012.04.017
6. Hougaard KD, Hjort N, Zeidler D, Sorensen L, Norgaard A, Hansen TM, et al. Remote ischemic perconditioning as an adjunct therapy to thrombolysis in patients with acute ischemic stroke a randomized trial. Stroke. (2014) 45:159–67. doi: 10.1161/STROKEAHA.113.001346
7. Connolly M, Bilgin-Freiert A, Ellingson B, Dusick JR, Liebeskind D, Saver J, et al. Peripheral vascular disease as remote ischemic preconditioning, for acute stroke. Clin Neurol Neurosurg. (2013) 115:2124–9. doi: 10.1016/j.clineuro.2013.07.038
8. Kim J, Lee DH, Cha MJ, Song TJ, Park JH, Lee HS, et al. Low ankle-brachial index is an independent predictor of poor functional outcome in acute cerebral infarction. Atherosclerosis. (2012) 224:113–17. doi: 10.1016/j.atherosclerosis.2012.06.058
9. Jing Z, Shi C, Zhu L, Xiang Y, Chen P, Xiong Z, et al. Chronic cerebral hypoperfusion induces vascular plasticity and hemodynamics but also neuronal degeneration and cognitive impairment. J Cereb Blood Flow Metab. (2015) 35:1249–59. doi: 10.1038/jcbfm.2015.55
10. Ma J, Ma Y, Dong B, Bandet MV, Shuaib A, Winship IR. Prevention of the collapse of pial collaterals by remote ischemic perconditioning during acute ischemic stroke. J Cereb Blood Flow Metab. (2017) 37:3001–14. doi: 10.1177/0271678X16680636
11. Berkhemer OA, Jansen IG, Beumer D, Fransen PS, van den Berg LA, Yoo AJ, et al. Collateral status on baseline computed tomographic angiography and intra-arterial treatment effect in patients with proximal anterior circulation stroke. Stroke. (2016) 47:768–76. doi: 10.1161/STROKEAHA.115.011788
12. Jansen IG, Mulder MJ, Goldhoorn RB, Boers AM, van Es AC, Yo LS, et al. Impact of single phase ct angiography collateral status on functional outcome over time: results from the mr clean registry. J Neurointerv Surg. (2019) 11:866–73. doi: 10.1136/neurintsurg-2018-014619
13. Lima FO, Furie KL, Silva GS, Lev MH, Camargo EC, Singhal AB, et al. The pattern of leptomeningeal collaterals on ct angiography is a strong predictor of long-term functional outcome in stroke patients with large vessel intracranial occlusion. Stroke. (2010) 41:2316–22. doi: 10.1161/STROKEAHA.110.592303
14. Jansen IGH, Mulder M, Goldhoorn RB, investigators MCR. Endovascular treatment for acute ischaemic stroke in routine clinical practice: prospective, observational cohort study (mr clean registry). BMJ. (2018) 360:k949. doi: 10.1136/bmj.k949
15. Tan IY, Demchuk AM, Hopyan J, Zhang L, Gladstone D, Wong K, et al. Ct angiography clot burden score and collateral score: correlation with clinical and radiologic outcomes in acute middle cerebral artery infarct. AJNR Am J Neuroradiol. (2009) 30:525–31. doi: 10.3174/ajnr.A1408
16. Goyal M, Fargen KM, Turk AS, Mocco J, Liebeskind DS, Frei D, et al. 2c or not 2c: defining an improved revascularization grading scale and the need for standardization of angiography outcomes in stroke trials. J Neurointerv Surg. (2014) 6:83–6. doi: 10.1136/neurintsurg-2013-010665
17. van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. (1988) 19:604–7. doi: 10.1161/01.STR.19.5.604
18. Brott T, Adams HP Jr, Olinger CP, Marler JR, Barsan WG, Biller J, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. (1989) 20:864–70. doi: 10.1161/01.STR.20.7.864
19. von Kummer R, Broderick JP, Campbell BC, Demchuk A, Goyal M, Hill MD, et al. The heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. (2015) 46:2981–6. doi: 10.1161/STROKEAHA.115.010049
20. Romero JR, Pikula A, Nguyen TN, Nien YL, Norbash A, Babikian VL. Cerebral collateral circulation in carotid artery disease. Curr Cardiol Rev. (2009) 5:279–88. doi: 10.2174/157340309789317887
21. Liebeskind DS. Collateral circulation. Stroke. (2003) 34:2279–84. doi: 10.1161/01.STR.0000086465.41263.06
22. Menon BK, d'Esterre CD, Qazi EM, Almekhlafi M, Hahn L, Demchuk AM, et al. Multiphase ct angiography: a new tool for the imaging triage of patients with acute ischemic stroke. Radiology. (2015) 275:510–20. doi: 10.1148/radiol.15142256
23. Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the american heart association/american stroke association stroke council, clinical cardiology council, cardiovascular radiology and intervention council, and the atherosclerotic peripheral vascular disease and quality of care outcomes in research interdisciplinary working groups: the american academy of neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. (2007) 115:e478–534. doi: 10.1161/CIRCULATIONAHA.107.181486
24. Araki Y, Kumakura H, Kanai H, Kasama S, Sumino H, Ichikawa A, et al. Prevalence and risk factors for cerebral infarction and carotid artery stenosis in peripheral arterial disease. Atherosclerosis. (2012) 223:473–7. doi: 10.1016/j.atherosclerosis.2012.05.019
Keywords: peripheral artery disease, acute ischemic stroke, ischemic preconditioning, endovascular treatment, functional outcome
Citation: Pirson FAV, Hinsenveld WH, Staals J, de Ridder IR, van Zwam WH, Schreuder THCML, Roos YBWEM, Majoie CBLM, van der Worp HB, Uyttenboogaart M, Lycklama à Nijeholt GJ, Schonewille WJ and van Oostenbrugge RJ (2020) Peripheral Artery Disease in Acute Ischemic Stroke Patients Treated With Endovascular Thrombectomy; Results From the MR CLEAN Registry. Front. Neurol. 11:560300. doi: 10.3389/fneur.2020.560300
Received: 08 May 2020; Accepted: 24 August 2020;
Published: 07 October 2020.
Edited by:
David J. Seiffge, University Hospital Bern, SwitzerlandReviewed by:
Johannes Kaesmacher, Technical University of Munich, GermanyVasileios-Arsenios Lioutas, Beth Israel Deaconess Medical Center and Harvard Medical School, United States
Copyright © 2020 Pirson, Hinsenveld, Staals, de Ridder, van Zwam, Schreuder, Roos, Majoie, van der Worp, Uyttenboogaart, Lycklama à Nijeholt, Schonewille and van Oostenbrugge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: France A. V. Pirson, ZmF2LnBpcnNvbkBtdW1jLm5s