 Weishang Song1,†
Weishang Song1,† Bing Chen
Bing Chen- 1Department of Anesthesia, Wushan Country People’s Hospital of Chongqing, Chongqing, China
- 2Department of Anesthesia, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, China
Spinal anesthesia by intrathecal administration of local anesthetic (LA) is a routine practice. Local anesthetic system toxicity, occurring in the central nervous system (CNS) and cardiovascular system, is a common and life-threatening adverse event of LA through a variety of routes, but is rarely encountered in spinal anesthesia when a very low dose of LA is injected into the subarachnoid space. Here, we report a case with manifestations of delayed lethal CNS toxicity after spinal anesthesia. A 55-year-old man underwent elective repair surgery for a chronic ulcer after receiving 10 mg intrathecal administration of bupivacaine. He developed nausea, agitation, paresthesia and myoclonus on the arms, legs, and trunk, as well as a gradually reduced level of consciousness one hour after intrathecal administration. He was sedated, intubated, and transferred to the intensive care unit. Both CT and MRI scans of the brain and assessments of blood showed no abnormalities. The electroencephalogram showed spike waves occurring at electrodes C3, C4, P3, P4, and T5. The patient was sedated continuously and treated with valproate. These symptoms were completely resolved in the following days without residual neurological complications. No cardiovascular complications were observed during the entire process. The delayed lethal symptoms in this case were most likely to be CNS toxicity induced by intrathecal bupivacaine administration. CNS toxicity after spinal anesthesia may be underestimated and unpredictable and should be vigilantly cared for in clinical settings.
Introduction
Spinal anesthesia by intrathecal administration of local anesthetic (LA) is a routine practice for surgery of the lower abdomen, pelvis, or lower extremities. The most commonly adverse effects of spinal anesthesia are hypotension, respiratory paralysis, or underventilation due to the block of spinal nerves above T4, but the local anesthetic systemic toxicity (LAST) is rarely encountered in spinal anesthesia for a very low dose of LA is injected into the subarachnoid space. LAST is a common and life-threatening adverse event of LA through a variety of routes after inadvertent intravascular injection, overdose, or significant systemic absorption that plasma concentration of LA reaches a toxic level (1). LAST can be further subdivided into central nervous system (CNS) toxicity and cardiovascular systemic toxicity. CNS toxicity occurs when LA crosses the blood-brain barrier, which leads to CNS excitation followed by CNS inhibition with potential respiratory depression and even death (2). Cardiovascular system toxicity with the symptoms of dysrhythmias and low systemic vascular resistance occurs when systemic LA concentration reaches a higher level (2). Here, we report a case with manifestations of delayed lethal CNS toxicity followed by intrathecal administration of 10 mg bupivacaine and reviewed cases with abnormal neurological symptoms after spinal anesthesia, which indicates CNS toxicity after spinal anesthesia may be underestimated and unpredictable and should be vigilantly cared for in clinical settings.
Case report
A 55-year-old man was presented for elective repair surgery for a chronic ulcer on the right foot induced by a 10-year history of type 2 diabetes mellitus. The chronic ulcer was debrided under general anesthesia uneventfully 142 days prior, and repaired with bone cement under local anesthesia uneventfully 132 days and 98 days prior, respectively. Moreover, he underwent an uneventful incision and drainage of the abscess of the ulcer under spinal anesthesia with ropivacaine three weeks prior. He had no history of drug abuse and seizures. Preoperative blood tests including liver function, renal function, and coagulation function of the patients were normal.
The puncture of spinal anesthesia was performed uneventfully in the L3–L4 interspace using a 25 G Quincke needle. 2 ml of 0.5% bupivacaine was injected into the subarachnoid space after obtaining cerebrospinal fluid. A good block was achieved about 5 min later. The surgery was uneventful and lasted about 50 min. No additional drugs were administered. The patient complained of nausea during transfer to the ward about 60 min after the intrathecal injection; thus, he was transferred to the post-anesthesia care unit. Finger prick blood was analyzed to detect hypoglycemia. Nausea was relieved after intravenous treatment of ondansetron 8 mg. However, about 10 min later, he became agitated and sweaty, complained of paresthesia on the skin below his neck, and developed involuntary, bilateral, asymmetrical, and arrhythmic myoclonic movements in both arms without loss of consciousness. Moreover, the heart rate, blood pressure, and arterial blood gas analysis were normal. Due to the symptoms of being sweaty and paresthesia on the skin, allergic reaction was doubted and hydrocortisone 100 mg was intravenously infused. Due to the symptoms of agitation, midazolam 5 mg was administered and dexmedetomidine was infused to sedate the patient. About 100 min after intrathecal injection, he was quickly intubated after the treatment of propofol and rocuronium for sudden blue jaundice of lips and loss of consciousness. The Glasgow coma scale was approximately 14 just before consciousness loss: eye opening was spontaneous, verbal response was responsible but a little confused, and the patient could obey commands to move his hands. The patient was transferred to the intensive care unit and a neurological doctor was consulted. Myoclonus still occurred and expanded to the legs when the muscle relaxation effect was eliminated (Supplementary Video S1). Both CT and MRI scans of the brain and assessments of blood showed no abnormalities. However, the electroencephalogram (EEG) showed spike waves occurring at electrodes C3, C4, P3, P4, and T5 (Figure 1), which showed myoclonus originated from the cortex of the parietal lobe and left temporal lobe. The patient was sedated continuously and treated with valproate. The frequency and amplitude of myoclonus decreased about 8 h after intrathecal injection. Although he still had sporadic myoclonus on postoperative day 1, he was peaceful and cooperative after stopping sedation. Therefore, he was extubated and transferred to the ward. He was discharged on postoperative day 4 without residual neurological complications. No cardiovascular complications were observed during the whole process.
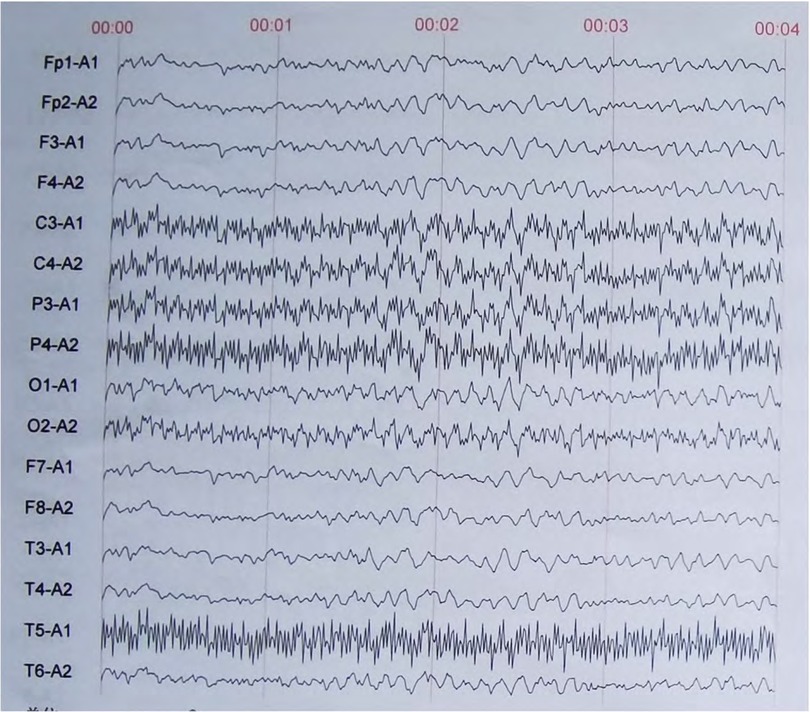
Figure 1. Representative electroencephalogram of this case after the onset of myoclonus.
Discussion
Other causes should be excluded before concluding that intrathecal bupivacaine is responsible for these delayed lethal side effects. Hypotension and underventilation are the most common adverse experiences following the administration of spinal anesthesia. However, this patient had no underventilation from intrathecal injection to the start of seizures. No hypotension occurred after intrathecal injection and even during the seizures. In addition, both the intrathecal puncture and repair surgery for chronic ulcer were performed by experienced doctors and were uneventful; no other drugs were used except for intrathecal bupivacaine; no abnormalities of CT and MRI scan of the brain and blood assessments were detected; these side effects were occurred about 1 h after intrathecal injection, relieved several hours, and completely recovered in the flowing days; the patient never underwent these symptoms before and after recovery. The total score of the Adverse Drug Reaction Probability Scale was 7 (Supplementary Table S1), which indicates that bupivacaine was the “probable” reason for these delayed lethal side effects.
The manifestations of CNS toxicity induced by LA include seizures, nausea, vomiting, perioral paresthesia, confusion, audio-visual disturbances, dysgeusia, agitation, or reduced level of consciousness (3). Moreover, spinal myoclonus, which originates from the spinal cord and is characterized by a non-generalized neuromuscular dysfunction restricted to a few somatic regions, was reported to be a side effect after spinal anesthesia (4–6). According to the manifestations of nausea, agitation, reduced level of consciousness, paresthesia and generalized myoclonus on arms, legs, and trunk, and spike waves in EEG, these side effects were compatible with CNS toxicity originating from the cerebral cortex induced by intrathecal bupivacaine administration.
Two pathways that lead to CNS toxicity after intrathecal administration of LA. One is that systemic absorbed LA crosses the blood-brain barrier, which usually occurs at high-dose LA administration (7). The mean seizure dosage of bupivacaine in rhesus monkeys was found to be 4.4 ± 1.2 mg/kg with mean plasma concentration of 4.5 ± 1.7 μ/ml (8). In this case, only 10 mg of bupivacaine was used, which is far lower than its toxic dose; thus, we believe this pathway is impossible. The other is that the drug in the cerebrospinal fluid cephalic diffused to the cerebral cortex then leads to neuron excitation (7). In this case, even if the dose of LA is low, it can affect the activity of neurons. Therefore, we speculate cephalic diffusion is the reason for CNS toxicity induced by intrathecal LA administration.
Based on the theory of LA cephalic diffusion after intrathecal administration, CNS toxicity should be not rare. We reviewed the published literature and found that 30 publications (1, 2, 4–6, 9–33) involving 31 patients and two cats had generalized tonic-clonic seizures or myoclonus after spinal anesthesia (Table 1), which is a symptom of LA-induced CNS toxicity. Although these myoclonus or generalized tonic-clonic seizures were considered to originate from the spinal cord (4–6), it could not be excluded that these side effects originated from the cerebral since the EEG assessment was absent in about 71% of the cases (Table 2) and abnormal EEGs were detected in two cases (2, 12). Moreover, these neurological symptoms presented in patients of different ages and genders, with or without neurological diseases, and different types of surgeries; they occurred quickly or slowly from several hours to one day after spinal anesthesia; and 64% of them were mild and resolved quickly and spontaneously (Table 2). Thus, CNS toxicity after spinal anesthesia is unpredictable and may be ignored in clinical settings, and underestimated. In addition, 46.7% of parturients underwent involuntary arm shaking or shivering soon after spinal anesthesia during cesarean delivery while they didn't feel cold (34), which has some similarity with myoclonus indicates that involuntary arm shaking may be a CNS toxicity induced by LA. Taken together, the rare complication of CNS toxicity induced by intrathecal LA administration may not be rare.
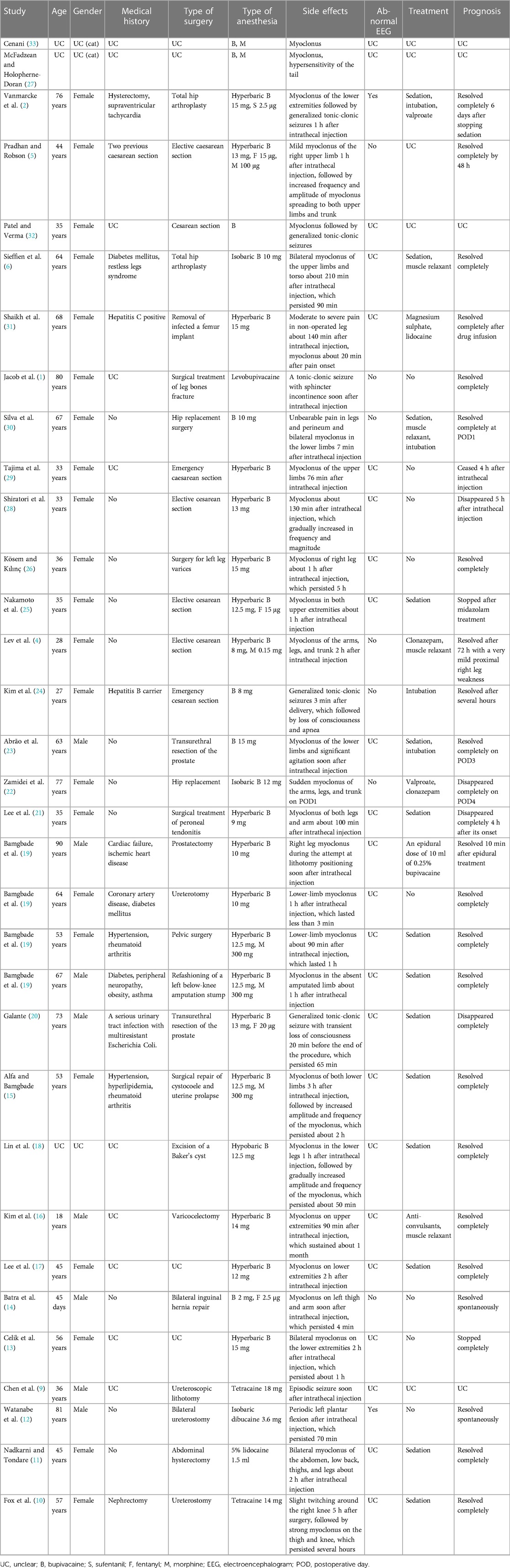
Table 1. The characteristics of the published cases with myoclonus after spinal anesthesia.
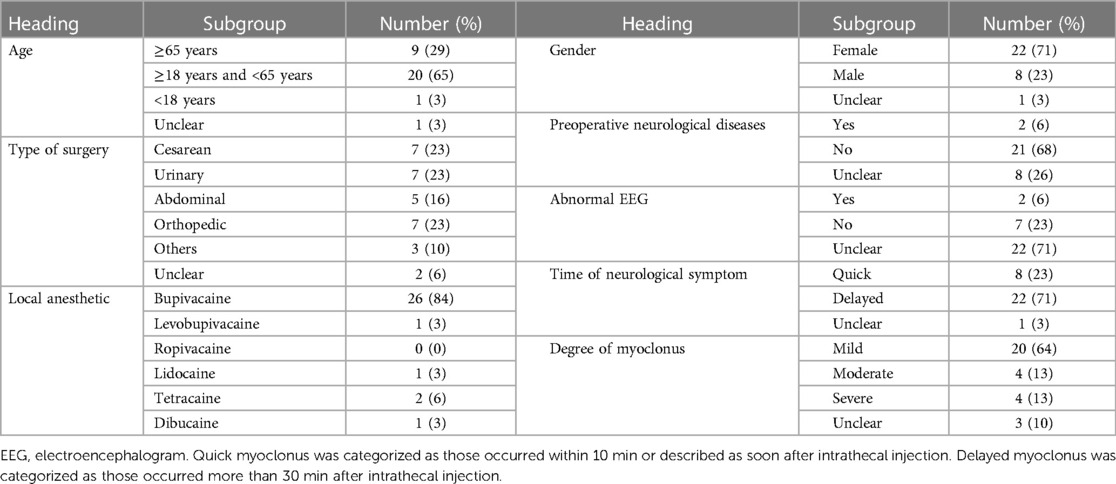
Table 2. Summary of the published cases with myoclonus after spinal anesthesia.
Although CNS toxicity after spinal anesthesia is unpredictable, our literature review found that (Table 2) it mainly occurred in female patients (75%), patients with ages between 18 and 65 years (65%), and bupivacaine administration (84%). The potential for CNS toxicity correlates with the potency of LA. Potent lipid-soluble agents such as bupivacaine can cause CNS toxicity at lower doses than less potent agents, such as levobupivacaine and ropivacaine (2). Shiratori et al. (35) found that 70% of patients had neurological symptoms after spinal and epidural anesthesia with bupivacaine. Moreover, our case underwent an uneventful incision and drainage of the abscess under spinal anesthesia with ropivacaine three weeks ago. These data indicate that intrathecal administration of bupivacaine has a high risk of CNS toxicity even if a very low dose was used.
Although 64% of the CNS toxicity induced by intrathecal LA administration was mild and resolved quickly and spontaneously, 13% of cases (2, 23, 24, 30) were severe and needed medical interventions to avoid hypoxia as presented in our case (Table 2). Importantly, the time of the CNS toxicity development after spinal anesthesia was delayed (occurred more than 30 min after intrathecal injection) in 71% of cases (Table 2). Therefore, CNS toxicity following spinal anesthesia can be fatal and delayed, which should be sustained care even if the patient leaves the operation room.
Conclusion
Intrathecal administration of a low-dose LA, especially bupivacaine, can result in delayed, lethal, and unpredictable CNS toxicity, which may be underestimated and should be vigilantly cared for in clinical settings.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
WS: Conceptualization, Writing – original draft. HZ: Conceptualization, Writing – original draft. XL: Writing – original draft, Data curation. CY: Data curation, Writing – original draft. YZ: Writing – original draft, Formal Analysis. YL: Conceptualization, Writing – review & editing. BC: Conceptualization, Writing – review & editing, Funding acquisition.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work is supported by the Grant [2021]24 from the Kuanren Talents Program of the Second Affiliated Hospital of Chongqing Medical University, and the Young and Middle-aged Outstanding Medical Team of Chongqing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fanes.2023.1298806/full#supplementary-material
Supplementary Video S1
Representative symptom of myoclonus in this case.
References
1. Jacob M, Tavares J, Portela I, Ruivo E, Lares A. Patient safety: which drug caused the seizure? Anesth Analg. (2021) 133(3 Suppl 2):1635.
2. Vanmarcke A, Lormans P, Vandewaeter C. Status epilepticus following intrathecal administration of bupivacaine: a case report. J Investig Med High Impact Case Rep. (2022) 10:23247096221090841. doi: 10.1177/23247096221090841
3. El-Boghdadly K, Pawa A, Chin KJ. Local anesthetic systemic toxicity: current perspectives. Local Reg Anesth. (2018) 11:35–44. doi: 10.2147/lra.S154512
4. Lev A, Korn-Lubezki I, Steiner-Birmanns B, Samueloff A, Gozal Y, Ioscovich A. Prolonged propriospinal myoclonus following spinal anesthesia for cesarean section: case report and literature review. Arch Gynecol Obstet. (2012) 286(1):271–2. doi: 10.1007/s00404-012-2246-1
5. Pradhan V, Robson E. Propriospinal myoclonus following neuraxial anaesthesia during elective caesarean section. Int J Obstet Anesth. (2022) 50:54. doi: 10.1016/j.ijoa.2022.103394
6. Sieffien W, Peng P, Dinsmore M. Spinal myoclonus following spinal anaesthesia in a patient with restless legs syndrome. Anaesth Rep. (2021) 9(1):73–5. doi: 10.1002/anr3.12113
7. Naguib M, Magboul MM, Samarkandi AH, Attia M. Adverse effects and drug interactions associated with local and regional anaesthesia. Drug Saf. (1998) 18(4):221–50. doi: 10.2165/00002018-199818040-00001
8. Munson ES, Tucker WK, Ausinsch B, Malagodi MH. Etidocaine, bupivacaine, and lidocaine seizure thresholds in monkeys. Anesthesiology. (1975) 42(4):471–8. doi: 10.1097/00000542-197504000-00018
9. Chen IC, Lin CS, Chou HM, Peng TH, Liu CH, Wang CF, et al. Unexpected recurrent seizures following repeated spinal injections of tetracaine—a case report. Acta Anaesthesiol Sin. (2000) 38(2):103–6.11000675
10. Fox EJ, Villanueva R, Schutta HS. Myoclonus following spinal anesthesia. Neurology. (1979) 29(3):379–80. doi: 10.1212/wnl.29.3.379
11. Nadkarni AV, Tondare AS. Localized clonic convulsions after spinal anesthesia with lidocaine and epinephrine. Anesth Analg. (1982) 61(11):945–7. doi: 10.1213/00000539-198211000-00011
12. Watanabe S, Sakai K, Ono Y, Seino H, Naito H. Alternating periodic leg movement induced by spinal anesthesia in an elderly male. Anesth Analg. (1987) 66(10):1031–2. doi: 10.1213/00000539-198710000-00024
13. Celik Y, Bekir Demirel C, Karaca S, Kose Y. Transient segmental spinal myoclonus due to spinal anaesthesia with bupivacaine. J Postgrad Med. (2003) 49(3):286.14597801
14. Batra YK, Rajeev S, Lokesh VC, Rao KLN. Spinal myoclonus associated with intrathecal bupivacaine and fentanyl in an infant. Can J Anaesth. (2007) 54(7):587–8. doi: 10.1007/bf03022328
15. Alfa JA, Bamgbade OA. Acute myoclonus following spinal anaesthesia. Eur J Anaesthesiol. (2008) 25(3):256–7. doi: 10.1017/s0265021507002578
16. Kim KM, Yoon JS, Cho HS, Gwak MS. Spinal myoclonus on upper extremities following spinal anesthesia A case report. Korean J Anesthesiol. (2008) 55(1):107–10. doi: 10.4097/kjae.2008.55.1.107
17. Lee SK, Shin JW, Im JS, Kim YM, Park JH, Choi H, et al. Myoclonus following spinal anesthesia with hyperbaric bupivacaine. Korean J Anesthesiol. (2008) 54(2):201–3. doi: 10.4097/kjae.2008.54.2.201
18. Lin CS, Wei-Hung C, Lee YW. Transient spinal myoclonus after spinal anaesthesia with bupivacaine in the perioperation period. Anaesthesist. (2008) 57(5):518. doi: 10.1007/s00101-008-1362-6
19. Bamgbade OA, Alfa JA, Khalaf WM, Zuokumor AP. Central neuraxial anaesthesia presenting with spinal myoclonus in the perioperative period: a case series. J Med Case Rep. (2009) 3:7293. doi: 10.4076/1752-1947-3-7293
20. Galante D. An unusual cause of seizures during subarachnoid anesthesia in a patient undergoing transurethral resection of the prostate: a case report. Minerva Anestesiol. (2009) 75(4):221–3.19078902
21. Lee JJ, Hwang SM, Lee JS, Jang JS, Lim S-Y, Hong SJ. Recurrent spinal myoclonus after two episodes of spinal anesthesia at a 1-year interval—a case report. Korean J Anesthesiol. (2010) 59(Suppl):S62–64. doi: 10.4097/kjae.2010.59.S.S62
22. Zamidei L, Bandini M, Michelagnoli G, Campostrini R, Consales G. Propriospinal myoclonus following intrathecal bupivacaine in hip surgery: a case report. Minerva Anestesiol. (2010) 76(4):290–3.20332743
23. Abrão J, Bianco Mde P, Roma W, Krippa JE, Hallak JE. Spinal myoclonus after subarachnoid anesthesia with bupivacaine. Rev Bras Anestesiol. (2011) 61(5):619–23. 339–640. doi: 10.1016/s0034-7094(11)70073-3
24. Kim HJ, Kwon M-Y, Kang H-J, Koo MS, Park J, Lee MA. Generalized tonic-clonic seizure following spinal anesthesia for cesarean section with bupivacaine—a case report. Anesth Pain Med. (2011) 6(4):393–6.
25. Nakamoto T, Hirota K, Iwai T, Shingu K. Complete resolution of myoclonuslike involuntary movements under subarachnoid block after midazolam administration in a patient undergoing cesarean section -a case report. Korean J Anesthesiol. (2015) 68(2):193–5. doi: 10.4097/kjae.2015.68.2.193
26. Kösem B, Kılınç H. An unusual complication of anesthesia: unilateral spinal myoclonus. Agri. (2017) 29(2):90–1. doi: 10.5505/agri.2016.92053
27. McFadzean WJM, Holopherne-Doran D. Myoclonus and hypersensitivity of the tail following intrathecal administration of morphine and bupivacaine in a cat. Vet Anaesth Analg. (2018) 45(2):238–9. doi: 10.1016/j.vaa.2017.09.038
28. Shiratori T, Hotta K, Satoh M, Kondo N, Ikeda J, Sasao S. A case of spinal myoclonus in a patient with elective cesarean section. JA Clin Rep. (2018) 4(1):47. doi: 10.1186/s40981-018-0182-1
29. Tajima M, Moriwaki K, Hashimoto K, Fujii K, Shiroyama K, Sanuki M, et al. Transient spinal segmental myoclonus during neuraxial anesthesia: a report of two cases. Anesth Resusc. (2019) 55(1):35–8.
30. Silva RM, Morais IG, Almeida AV, Pereira OM, Silva AM, Sa EC. Spinal myoclonus: is it an anesthetic mystery? Rev Esp Anestesiol Reanim. (2020) 67(2):108–11. doi: 10.1016/j.redar.2019.08.001
31. Shaikh M, Ahmed J, Shaikh K, Khan S, Mmeon GN. Spinal myoclonus after sub-arachnoid block: a case report. Pak J Med Health Sci. (2021) 15(12):3353–4. doi: 10.53350/pjmhs2115123353
32. Patel AK, Verma N. Status epilepticus following intrathecal administration of 0.5% heavy bupivacaine: a case report. NeuroQuantology. (2022) 20(19):2012–6. doi: 10.48047/nq.2022.20.19.NQ99173
33. Cenani A. A case of myoclonus in a cat after intrathecal injection of bupivacaine and morphine. J Am Vet Med Assoc. (2023) 261(10):1555–7. doi: 10.2460/javma.23.05.0277
34. Zhang Q, Xia LY, Liang WD, Rao DY, Zhu PP, Huang KN, et al. Intrathecal dexmedetomidine combined with ropivacaine in cesarean section: a prospective randomized double-blind controlled study. Front Med (Lausanne). (2022) 9:922611. doi: 10.3389/fmed.2022.922611
Keywords: spinal anesthesia, bupivacaine, toxicity, central nervous system, myoclonus
Citation: Song W, Zhang H, Li X, Yu C, Zhou Y, Li Y and Chen B (2023) Delayed lethal central nervous system toxicity induced by a low-dose intrathecal administration of bupivacaine: case report. Front. Anesthesiol. 2:1298806. doi: 10.3389/fanes.2023.1298806
Received: 22 September 2023; Accepted: 4 December 2023;
Published: 18 December 2023.
Edited by:
Andrea Meli, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, ItalyReviewed by:
Rudrashish Haldar, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGI), IndiaWilliam R. Wolowich, Nova Southeastern University, United States
© 2023 Song, Zhang, Li, Yu, Zhou, Li and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuesu Li MzU4ODM5MjUyQHFxLmNvbQ== Bing Chen Y2hlbmJpbmdAY3FtZC5lZHUuY24=
†These authors have contributed equally to this work and share first authorship