 Simone Tassani1*
Simone Tassani1* Paula Chaves1
Paula Chaves1 Marc Beardsley1
Marc Beardsley1 Milica Vujovic2
Milica Vujovic2 Juan Ramírez3Jimena Mendoza1,4
Juan Ramírez3Jimena Mendoza1,4 Marta Portero-Tresserra5
Marta Portero-Tresserra5 Miguel Angel González-Ballester1,6
Miguel Angel González-Ballester1,6 Davinia Hernández-Leo1
Davinia Hernández-Leo1- 1Department of Information and Communication Technologies Universitat Pompeu Fabra, Barcelona, Spain
- 2Technische Universität Wien, Vienna, Austria
- 3Universidad Nacional de Colombia, Medellín, Colombia
- 4Universidad Iberoamericana, Mexico City, Mexico
- 5Universitat Autònoma de Barcelona, Barcelona, Spain
- 6Catalan Institution for Research and Advanced Studies (ICREA), Barcelona, Spain
Objective: This study aims to test the hypothesis that breathing can be directly linked to postural stability and psychological health. A protocol enabling the simultaneous analysis of breathing, posture, and emotional levels in university students is presented. This aims to verify the possibility of defining a triangular link and to test the adequacy of various measurement techniques.
Participants and Procedure: Twenty-three subjects (9 females and 14 males), aged between 18 and 23 years, were recruited. The experiment consisted of four conditions, each lasting 3 minutes: Standard quiet standing with open eyes 1), with closed eyes 2), and relaxed quiet standing while attempting deep abdominal breathing with open eyes 3) and with closed eyes 4). These latter two acquisitions were performed after subjects were instructed to maintain a relaxed state.
Main Outcome Measures: All subjects underwent postural and stability analysis in a motion capture laboratory. The presented protocol enabled the extraction of 4 sets of variables: Stabilometric data, based on the displacement of the center of pressure and acceleration, derived respectively from force plate and wearable sensors. Postural variables: angles of each joint of the body were measured using a stereophotogrammetric system, implementing the Helen Hayes protocol. Breathing compartment: optoelectronic plethysmography allowed the measurement of the percentage of use of each chest compartment. Emotional state was evaluated using both psychometric data and physiological signals. A multivariate analysis was proposed.
Results: A holistic protocol was presented and tested. Emotional levels were found to be related to posture and the varied use of breathing compartments. Abdominal breathing proved to be a challenging task for most subjects, especially females, who were unable to control their breathing patterns. In males, the abdominal breathing pattern was associated with increased stability and reduced anxiety.
Conclusion: In conclusion, difficulties in performing deep abdominal breathing were associated with elevated anxiety scores and decreased stability. This depicts a circular self-sustaining relationship that may reduce the quality of life, undermine learning, and contribute to muscular co-contraction and the development of musculoskeletal disorders. The presented protocol can be utilized to quantitatively and holistically assess the healthy and/or pathological condition of subjects.
1 Introduction
Modern society is suffering from contemporary pathologies that healthcare institutions can only partially address. Conditions and diseases traditionally linked to aging, including back pain, neck pain, and even arthrosis, are now emerging earlier in life, even during youth and adolescence (Prins et al., 2008). The rising incidence of musculoskeletal pain among younger populations is alarming, not only due to its early onset but also because of the potential to evolve into chronic musculoskeletal pain syndromes that persist into adulthood (Brattberg, 2004; Prins et al., 2008). Emerging evidence from the literature underscores the causal role of emotional distress, already related to the development of mental disorders, in the development of musculoskeletal disorders (Brattberg, 2004; Diepenmaat et al., 2006; McFarlane, 2007). Throughout our lives, we inevitably encounter various stressful situations, some of which can be avoided or mitigated, while others are an inherent part of life. Nevertheless, learning to regulate our emotional response becomes crucial for our adaptation in the environment, health, and wellbeing. Particularly, young individuals, including students, often confront stressors without the appropriate self-regulation skills (Prins et al., 2008; Sawatzky et al., 2012). Moreover, they are prone to adopting sub-optimal musculoskeletal strategies, such as maintaining poor sitting postures (Yang et al., 2020). These psychological and physical aspects, in turn, can impact their learning process and performance (Swiecki et al., 2019). Therefore, there is a need for methods that empower students to enhance their stress management skills, mitigating the potential long-term effects on both their musculoskeletal health and learning outcomes.
However, the direct correction of postural or psychological problems presents challenges. From a physical standpoint, learning correct posture is problematic due to the numerous degrees of freedom that need to be controlled, making it difficult to self-learn good posture (Sheikhhoseini et al., 2018). Technology-based solutions aimed at identifying and helping to correct poor postures have been developed (Wong and Wong, 2008; Byeon et al., 2020). However, the widespread availability of these approaches to all students remains an important challenge. On the psychological side, problems can arise even in earlier phases, with students often avoiding asking for help (Abdollahi et al., 2017). Moreover, students with mental health problems report lower engagement in campus activities (Byrd and McKinney, 2012), and few students experiencing stress-related mental health problems receive treatment (Garlow et al., 2008).
Breathing techniques offer an accessible approach to address both postural and psychological challenges (Gilbert, 2003; Busch et al., 2012) acting as a mediator between the two spheres. Unlike most physiological functions, breathing can be modulated voluntarily and serves as an entry point for both physiological and psychological regulation. Accordingly, clinical trials implementing disciplines specifically focused on breathing, like Tai Chi, Qi Gong, and Yoga, are exponentially increasing (Tassani et al., 2019). Repetitive motor tasks and long-lasting training can cause beneficial or disadvantageous postural adaptation with long-term effects on the Postural Control System (De Blasiis et al., 2022). The main advantages of these breathing practices are that they can be easily taught, are non-pharmacologic, self-administered, come at no cost, and can be performed at anytime and anywhere.
Scientific literature also suggests a clear relation between breathing and posture. Breathing and postural control are mechanically and neuromuscularly interdependent as the main muscles used during respiration (diaphragm and intercostal muscles) also contribute to postural control (Hodges and Gandevia, 2000). Poor posture (as an inclined position) impedes the proper function of the diaphragm resulting in increased activity of the upper respiratory duct (Kim et al., 2017). The effect of breathing on psychological stress is also increasingly studied (Perciavalle et al., 2017; Hopper et al., 2019) and specific breathing patterns have been found to lower physiological arousal associated with emotional distress and measures of state anxiety (Balban et al., 2023).
These findings suggest a tight link between psychological health, breathing, and posture through self-regulation. However, the actual triangular relation between posture, breathing, and stress is still unclear. Understanding this relationship could shed more light on the efficiency of breathing therapies for both aiding young adults in controlling their mental distress and predicting/preventing the development of several musculoskeletal disorders for the population of any age. In this regard, instrumentation methods for the quantitative evaluation of posture, breathing, and stress could be useful to objectively demonstrate this triangular link. In particular, the gold standard for three-dimensional analysis of posture is 3D stereophotogrammetry, an optoelectronic system that allows for the evaluation of the whole-body in standing (Chiari et al., 2002; Rocchi et al., 2004) and while walking (Cappozzo et al., 2005) by using infrared cameras and reflective skin markers placed on specific landmarks. Moreover, 3D stereophotogrammetry is also used for optoelectronic plethysmography to assess thoracic and abdominal movements during breathing (Massaroni et al., 2017). For the analysis of body oscillations, force plate, and stabilometry are used to analyze postural stability parameters in open (De Blasiis et al., 2023) and closed eyes (Fullin et al., 2022), considering their reliability and variability too. Eventually, levels of psychological stress can be evaluated by wearable sensors. Examples include an “in-ear sensor” (Ellebrecht et al., 2022) which measures body temperature and heart rate as well as stabilometric parameters, and a “galvanic skin response (GRS) device” (Ellebrecht et al., 2022), which measures the conductivity of human skin through the activity of sweat glands stimulated by the sympathetic nervous system (SNS).
Currently, there seems to be an absence of studies considering the three effects at the same time. Therefore, the present study aims to test the relationship between breathing, postural stability, and psychological health under the hypothesis that deep abdominal breathing can reduce stress and increase stability in university students. For this reason, a protocol allowing simultaneous analysis of breathing, posture, and emotional levels is presented, to verify the possibility of defining a triangular link and to test the adequacy of different measurement techniques.
2 Materials and methods
2.1 Recruitment
Twenty-three subjects were recruited for this study, 9 females and 14 males, with ages ranging between 18 and 23 years old, 174 ± 9 cm height, 67.2 ± 9.5 kg weight, and 22.1 ± 2.3 kg/m2 of BMI. Twenty-one subjects were within the normal BMI range (18.5–24.9) while two subjects were slightly overweight. No obese or underweight subjects were involved in the study. The inclusion criteria for the study were that the subjects were university students in the first to the third year of their undergraduate studies. Excluded from the study were frequent smokers (those who smoke more than 3 times a week), those with prior musculoskeletal disorders, those with reported cases of anxiety, and those who reported expert knowledge of breathing techniques. All subjects gave informed written consent before participating in the study.
2.2 Data collection
For all subjects, three sets of data collection were performed: breathing, postural/stability, and emotional.
2.2.1 Breathing and posture
Breathing and body postural/stability recordings were performed at the Motion Capture Laboratory using optoelectronic technology. Eight infrared cameras were used (BTS Smart-DX 700, 1.5Mpixels 250 fps). Four were placed on tripods close to the subject, with two in front of the subject and the other two behind. The remaining four cameras were fixed to the corners of the ceiling of the room. Two video cameras (BTS VIXTA 50HZ) were placed to record the frontal and the left side of subjects during all data acquisition as a reference for reflective marker positioning over subjects. Further, a force plate (BTS P-6000 50 Hz sampling) was used to acquire stability data. Synchronized data acquisition was guaranteed using the software SMART Capture, developed by BTS Bioengineering.
During posture and breathing analysis, a total of 105 reflective markers were attached to the subjects’ skin of as two different marker protocols were combined. Firstly, breathing data was acquired using a validated protocol implemented by BTS in the software Smart Analyzer that was used for the data analysis (Aliverti and Pedotti, 2003; De Faria Júnior et al., 2013). The protocol consists of eighty-nine reflective markers placed over the chest of subjects and requires subjects to be bare chest. A minor modification to the protocol allowed women to wear any kind of upper undergarment during this study. Secondly, posture was measured using the Helen Hayes protocol with medial markers (Davis et al., 1991). This protocol makes use of 22 reflective markers. However, the placement of some markers coincides in the two protocols. Specifically, markers placed in the shoulders, C7 vertebrae, sacrum, and left and right anterior superior iliac spine were reused. Therefore, only sixteen additional markers were placed on the legs.
Stability estimations were performed by measuring the displacement of the center of pressure (COP) over the force plate. Subjects wore a single 3D commercial accelerometer in-ear sensor, called Cosinuss◦ One, Cosinuss GmbH, Munich, Germany (Burgos et al., 2020). The three axes of the in-ear sensor are identified in Figure 1. The three-axial accelerometric data were also used as estimators of subject stability.
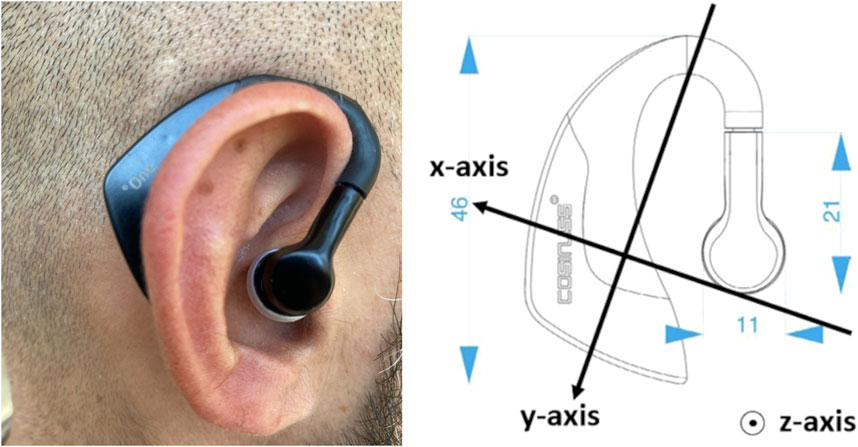
Figure 1. In-ear sensor “Cosinuss One.” On the right are displayed the acceleration directions of the sensor.
2.2.2 Emotional data
Emotional data were collected following two different approaches. Firstly, psychometric data were used to acquire baseline information and collect subjects’ feelings. Secondly, physiological signals were collected throughout to measure biometrics related to subjects’ emotional responses.
2.2.2.1 Psychometric data
During recruitment, applicants to the study were asked to complete an online survey administered in the format of a Google form. The survey included the State-Trait Anxiety Inventory (STAI—link), Rosenberg Self-Esteem Scale (RSE), and Five Facet Mindfulness Questionnaire. Subjects were also asked some general questions about their knowledge of breathing techniques and questions related to the exclusion criteria.
2.2.2.2 Physiological signals
The same in-ear device used for measuring postural stability (Cosinuss◦ One, Cosinuss GmbH, Munich, Germany) also allowed for the measurement of body temperature and heart rate which were used as estimators of anxiety. Finally, galvanic skin response (GSR) was measured with a device (Shimmer3, Shimmer Sensing, Dublin, Ireland) placed on the arm with connected electrodes positioned close to the palm on the internal side of the wrist.
2.3 Procedure
The experiment consisted of four conditions with each recording having a duration of 3 minutes. 1) Standard quiet standing with open eyes and 2) standard quiet standing with closed eyes were the two first recordings. For these conditions, subjects were asked to stand on the force plate in a normal stance that they felt comfortable with and to avoid sudden movements. After the standard condition, subjects were given instructions on performing deep abdominal breathing. They were instructed to breathe in slowly and deeply into the abdomen and to breathe out in a relaxed manner. Subjects performed from six to ten deep breaths with the lab technician while using proprioceptive input in which subjects placed one hand on their chest and the other on their abdomen. Subjects were asked to practice this breathing technique for a few minutes and to perform some exercises to relax their joints (circular motions, flex-extension, ab-adduction, and rotation of each joint: neck, shoulders, hips, knees, and ankles) while maintaining their deep breathing as described in the literature (Tassani et al., 2019). At the end of the relaxation phase, 3) a recording with open eyes and then 4) with closed eyes was taken in which subjects were asked to be in a relaxed state while trying to perform deep breathing. This is what was referred to as the relaxed state.
2.4 Data processing
2.4.1 Stability data
Displacement of the center of pressure (COP) was analyzed using the software Sway (BTS Engineering, Milan, Italy). Analysis time was normalized to 180 s and all parameters described in the table below were computed (Table 1).
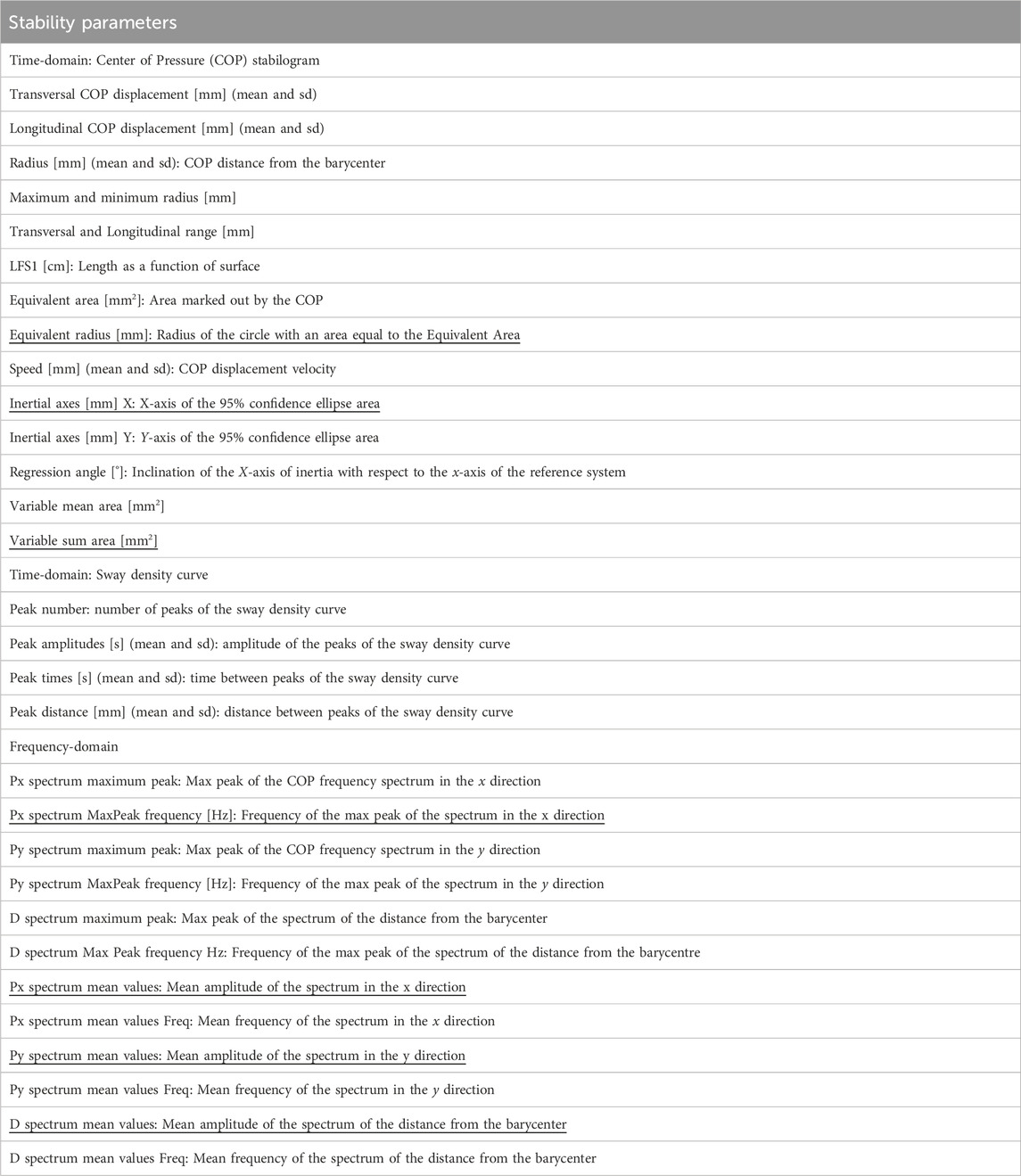
Table 1. Complete list of variables analyzed for the stability analysis. Underlined items denote variables not used in the final analysis, after feature reduction.
2.4.2 Body posture
Body posture analysis was performed using references identified by the Helen Hayes protocol as shown in Figure 2. As a general description, in the reference system of each body segment, X is the longitudinal axis of the segment and points up, Y is the sagittal axis of the segment and points forward, and Z is the transversal axis of the body and points to the left of the subject. The only exception to this definition is the reference system of the foot in which X points backward and therefore Y points up.
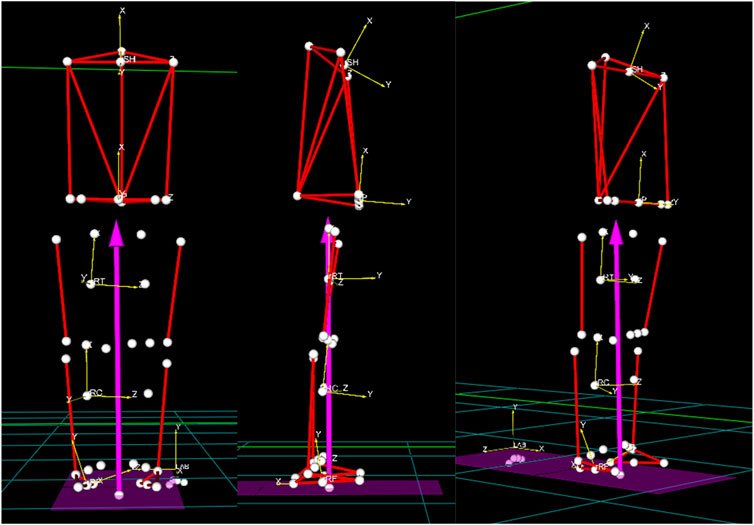
Figure 2. References systems of each body segment.
These definitions are general for all joints in the body. All measures are relative of the distal segment to the proximal one. In the case of the pelvis and trunk, Rotation refers to when there is rotation around the X-axis. Obliquity refers to when the rotation is around the Y-axis. Tilt refers to when the rotation is around the Z-axis. However, for these two segments, measures are defined with respect to the posture reference system (X-axis—vertical direction in the laboratory, Z-axis—axis passing through the two markers in the heels, Y-axis—vectorial product of X and Z). The complete list of body posture angles and their acronyms is presented in Table 2.
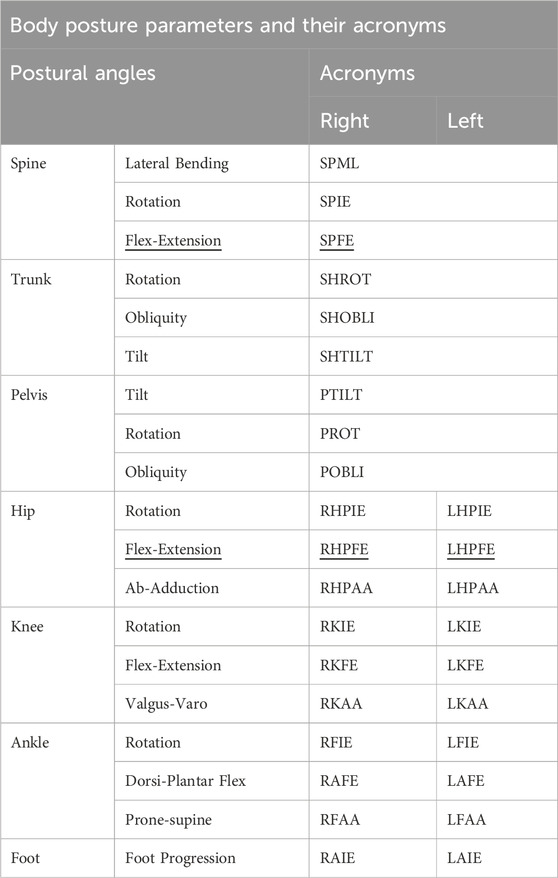
Table 2. List of postural angles obtained and their acronyms. Underline items denote variables not used in the final analysis, after feature reduction.
2.4.3 Breathing
The volumetric geometrical model of the chest wall was run through an OptoElectronic Plethysmography (OEP) protocol for quiet breathing, implemented by BTS Engineering. The protocol computes the chest’s tidal volume and the three thoracic compartments (Pulmonary Rib Cage, Abdominal Rib Cage, and Abdominal) (Figure 3).
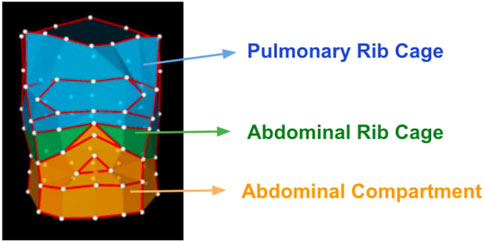
Figure 3. Compartmental 89-marker model of the chest wall in Optoelectronic Plethysmography.
2.5 Data analysis
Data analysis was performed in consecutive steps that were repeated for each typology of data acquired to test possible relations between abdominal breathing, posture, and emotions. Analyses were performed using SPSS (version 23.0; IBM Corp., Armonk, NY, United States).
Firstly, stability data were normalized by the height of subjects as suggested in the literature (Chiari et al., 2002). Normalization was not applied to postural parameters, which are angles and not affected by subject height, nor to emotional data. Breathing data were not normalized either since the analysis focussed on the percentages of use of each thoracic compartment.
The use of each breathing compartment was computed as a percentage of the sum of the three. The breathing technique of each subject was defined as pulmonary if the pulmonary compartment covered a percentage of breathing volume greater than that of the abdominal compartment. Similarly, it was defined as abdominal if the abdominal compartment covered a percentage of breathing volume greater than the pulmonary compartment. The abdominal rib cage compartment was never found to be the compartment with a highest percentage.
Secondly, a correlation analysis was performed to reduce the number of variables in the analysis. Every pair of variables presenting an absolute value of the Pearson correlation coefficient superior to 0.9 was identified as highly correlated and therefore, one of the two variables was excluded from the analysis.
2.5.1 Multivariate analysis of variance
The experiment was originally designed to perform repeated measurement tests among the four combinations of the within factors, state (standard and relaxed) and eyes (open and closed) and compare it with the between factor sex (male and female) (Tassani et al., 2019). However, a preliminary multivariate analysis of variance (MANOVA) for repeated measures showed no effect of the within factors over the breathing percentages of the pulmonary rib cage, abdominal rib cage, and abdominal compartment (p-value >0.40) nor their interactions (p-value >0.29). For this reason, in the presented analysis, results of the within variables were pooled, and the capability of each subject to breathe or not abdominally was analyzed as an independent factor, breathing.
On the other hand, the between-factor sex was significant, with females showing a higher percentage of pulmonary volume (Estimated marginal means: female 50.24 ± 2.1, male 41.18 ± 1.9), with only 8 abdominal acquisitions over 35.
Therefore, a MANOVA was performed to analyze the relationship between 3 factors and the three sets of dependent variables: stability, posture, and emotional data. The four factors under study were the state of the eyes (eyes: open or closed) posture stance (stance: standard or relaxed) and breathing (abdominal or pulmonary). Sex (male, female) where analyzed separately.
2.5.2 Classification
Binary logistic regression was applied to explore the possibility of classification of the breathing style of each subject starting from stability and postural data. Forward conditional feature selection was used.
2.5.3 Multiple linear regression
Both MANOVA and classification analysis assumed that it was possible to divide the breathing style into abdominal and pulmonary. Multiple linear regression analysis was performed to evaluate the possible continuous relationship between breathing, postural, stability, and emotional data.
2.5.4 Continuous time evaluation: statistical parametric mapping
Skin conductivity, temperature, heart rate, and acceleration of the head in three dimensions, were time-variant and therefore a time-continuous approach was proposed for their analysis. Statistical Parametric Mapping (SPM) refers to hypotheses testing of a spatially extended statistical procedure. SPM implements random field theory (Brett et al., 2003) and allows for the statistical identification of significant differences within time-variant variables.
Two-sample (independent) t-tests, performed using the MATLAB implementation “spm1d” (Pataky, 2012), were applied to examine the effects of breathing over each of the mentioned continual data.
3 Results
Abdominal breathing proved to be a difficult task for most subjects involved in the study. No significant difference in the use of breathing compartments was identified during the different phases of analysis (p-value = 0.404), showing an inability of subjects to breathe abdominally when instructed. Over a total of 81 valid breathing acquisitions, only 28 showed a dominant abdominal component (34%). Further, female subjects had greater difficulty breathing abdominally when instructed than male subjects as only 8 abdominal-dominant acquisitions (25%) were recorded from female subjects (Table 3).
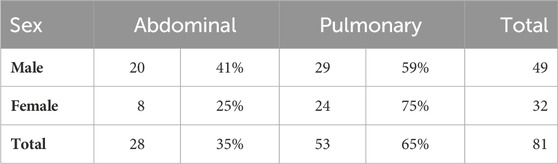
Table 3. Distribution of abdominal and pulmonary breathing of male and female subjects and their percentage over the total number of acquisitions.
Due to this disparity, male and female subject data were separated for subsequent analyses. Moreover, given the low number of female subjects able to perform abdominal breathing, MANOVA and classification analysis were only performed on data from males, while regression analysis was performed on both sets of data.
Twenty subjects filled out the survey collecting emotional data. Results showed the general emotional situation of subjects was critical. Seven subjects showed high anxiety (STAI>44—Ercan et al., 2015) of which, four also showed low levels of self-esteem (RSE<25—Isomaa et al., 2013). STAI and RSE were found to be negatively correlated (R2 = 0.47, p-value<0.001). MANOVA and classification study were not performed with this data due to the small sample size once male and female data were separated and given the unbalanced distribution of breathing capabilities in females.
Finally, 3 MANOVA analyses were performed: for stability, divided between spatio-temporal and frequency parameters, and posture variables. To maintain the family-wise error at 5%, p-values were considered significant at a level of 0.017.
3.1 Breathing and stability
From the initial 37 stability parameters, 9 were found to be highly correlated with at least one other parameter—therefore, they were removed from the analysis. The remaining parameters in the analysis are shown in Table 1. Eighty-one acquisitions were finally valid for this analysis (46 for males and 35 for females).
MANOVA did not identify any factor or interaction related to stability for spatio-temporal or frequency parameters (Table 4). However, binary logistic regression was able to properly classify 76% of male acquisitions as belonging to abdominal or pulmonary breathing groups using only three stability variables: Standard deviation of the Transversal COP displacement, Peak number, and Peak Amplitude. Subjects showing abdominal breathing presented a reduced value of the three parameters therefore suggesting higher stability. All of them are related to the time-domain. The confusion matrix is shown in Table 5.
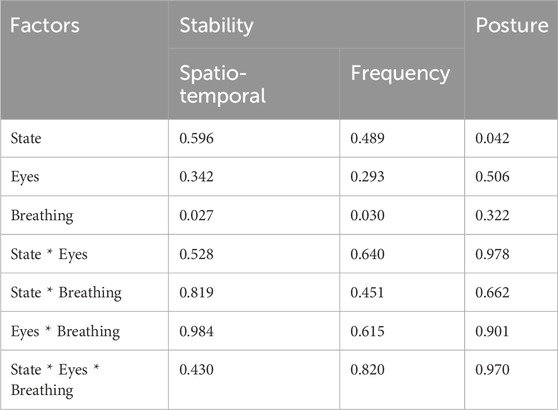
Table 4. p-values of the MANOVA analysis of Stability and Posture variables.
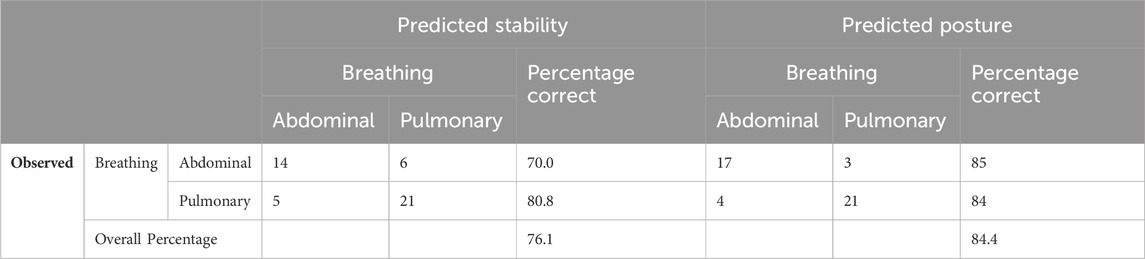
Table 5. Confusion matrix of breathing classification based on stability and posture variables. States of abdominal and pulmonary breathing were classified starting from, respectively, stability information based on the analysis of the COP displacement, and postural data obtained using stereophotogrammetric tools.
Multiple regression analysis showed a significant relation between the use of abdominal rib cage and stability parameters in women (adjR2 = 0.36). For males, each chest compartment showed a relation with different stability parameters. In particular an opposite trend was identified between abdominal rib cage (adjR2 = 0.528) and abdominal percentages (adjR2 = 0.337). In males, an increased percentage of the abdomen was related to increased stability. Detailed results are shown in Table 6.
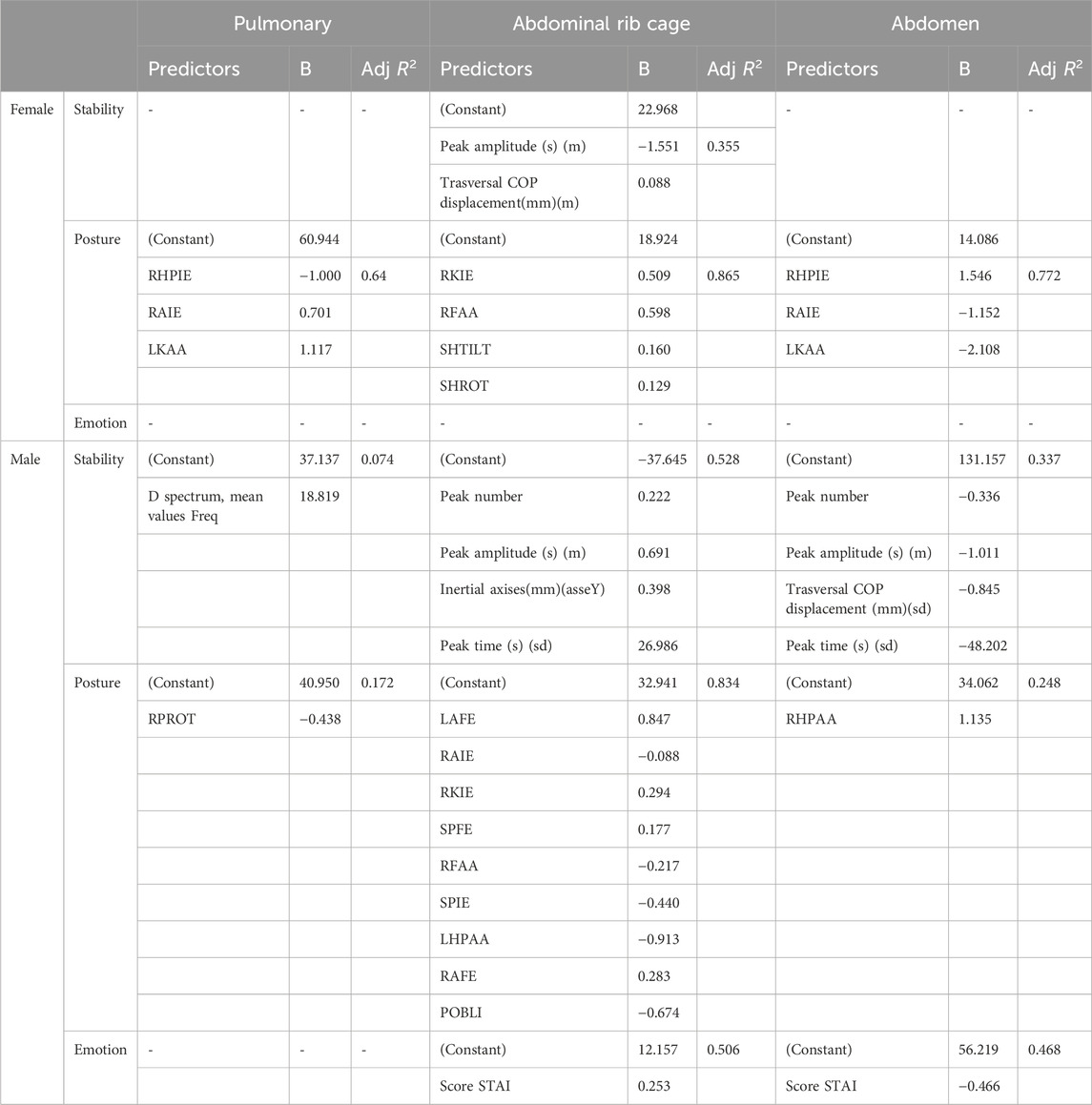
Table 6. Significant multiple linear regressions. The list of stability and postural predictors is reported along with the B coefficients and the adjusted R2 of each of the regressions. Each set of predictors was related to the used percentage of the three chest compartments: Pulmonary, Abdominal rib cage and Abdomen. Regressions are shown separately for female and male subjects. For a complete description of the variables and their acronyms, refers to Tables 1, 2.
SPM of in-ear acceleration data showed statistical differences between subjects breathing abdominally or pulmonary in axes X and Y (Figure 4). Acquisitions identified as related to abdominal breathing showed reduced acceleration compared to those related to pulmonary breathing.
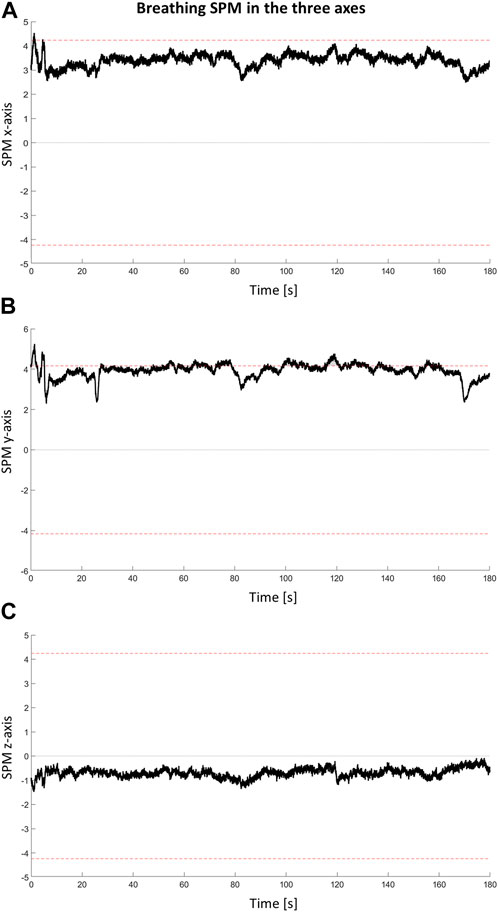
Figure 4. Statistical Parametric Mapping (SPM) of acceleration data. (A) X, (B) Y and (C) Z SPM accelerations are shown. Red dotted line identifies the significant level. When the SPM cross the red line a significant cluster is identified.
3.2 Breathing and posture
From the initial list of 29 postural parameters, 3 were found to be highly correlated with at least one other parameter—therefore, they were removed from the analysis leaving 26 parameters in the analysis (Table 2). In particular, both right and left hip flex-extension were found to be highly correlated (r > 0.9) to pelvis tilt, and spine flex-extension correlated to shoulder tilt. Seventy-three acquisitions were finally valid for this analysis (45 for males and 28 for females).
MANOVA did not identify any factor or interaction related to posture (Table 4). However, binary logistic regression was able to properly classify 84% of male acquisitions as belonging to abdominal or pulmonary breathing groups using only four postural variables: RKIE, POBLI, RHPAA, SHTILT. The confusion matrix is shown in Table 5.
Multiple regression analysis showed the relation between the use of any chest compartment and the posture of both male and female subjects. The compartment showing less relation to the posture was the pulmonary one (adjR2 = 0.64 for females and 0.172 for males), while the abdominal rib cage compartment showed high adj R2 for both male (adjR2 = 0.834) and female (adjR2 = 0.865) subjects. However, the two multiple regressions differ between sexes. In female subjects, a strong relation between the use of abdominal compartment and posture was also reported (adjR2 = 0.772). Detailed results are shown in Table 6.
3.3 Breathing and emotion
The first part of the emotional evaluation was carried out using surveys, therefore it was not possible to relate these results to all four combinations of state and eyes used to acquire breathing patterns. Hence, the analysis was carried out by relating the emotional evaluation to breathing results from the condition of “standard open eyes.” This forced a reduction in sample size to 20 acquisitions, only one for each subject (11 males and 9 females). Female subjects did not report any significant multiple regression with breathing compartments while males reported significant regressions with both Abdominal rib cage and Abdominal percentage (Table 6). STAI score was found to be positively related to the use of the abdominal rib cage and negatively related to the use of the abdominal compartment (Figure 5).
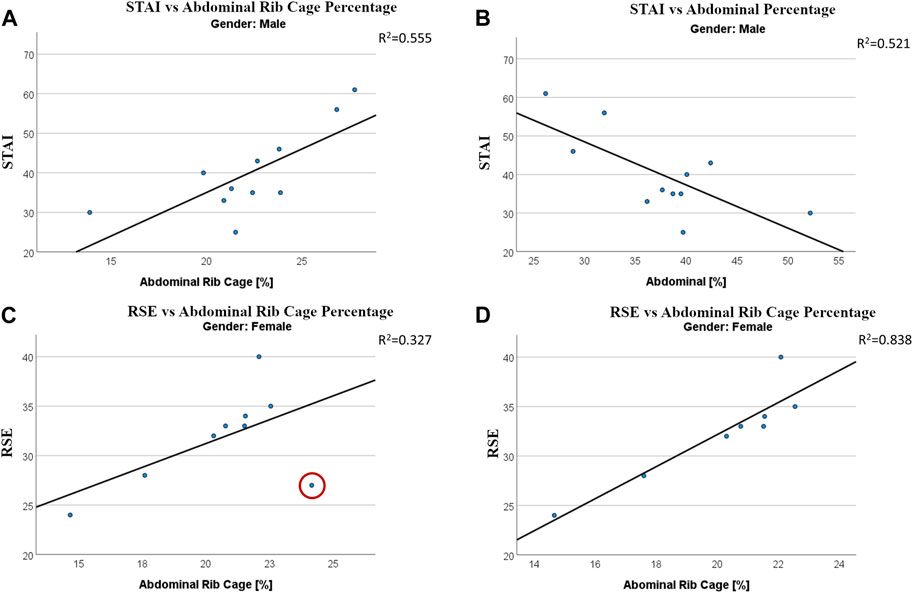
Figure 5. Regressions between emotional states and use of breathing compartments. Regression between State-Trait Anxiety Inventory (STAI) score and Abdominal Rib Cage (A) and Abdominal Compartment (B) in males. Regression between the Rosemberg Self-Esteem score and Abdominal Rib Cage in female, with (C) and without (D) the inclusion of a strong outlier.
SPM of both the in-ear sensor and the GSR identified no statistical difference related to the use of different breathing compartments.
3.4 Stability and emotion
As for the connection to breathing, the linear relation between stability and emotional scores was studied only for the results related to the state of “standard—open eyes.” Twenty acquisitions (11 males and 9 females) were available for this analysis. Women did not show any significant relation between stability predictors and any of the emotional scores used in this study. On the other side, males presented stability relations to both STAI score (adjR2 = 0.727) and 5 Facet score (adjR2 = 0.353). Results are summarized in Table 7. The mono-dimensional regression between D spectrum and 5 Facet score in males is presented in Figure 6.
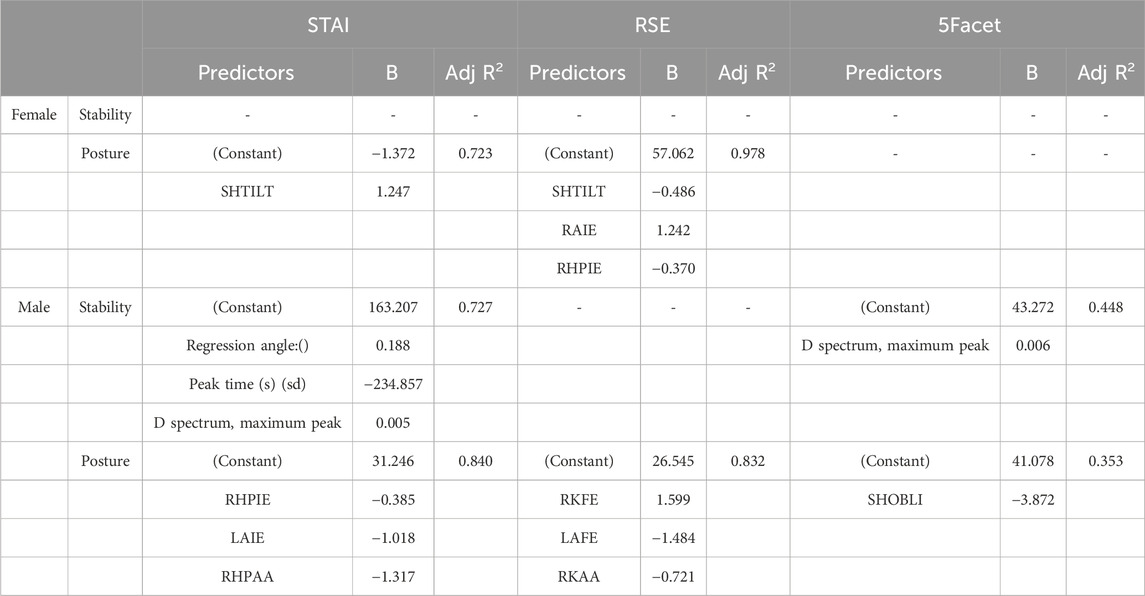
Table 7. Significant multiple linear regressions. The list of stability and postural predictors is reported along with the B coefficients and the adjusted R2 of each of the regressions. Each set of predictors was related to the three emotional scores: the State-Trait Anxiety Inventory (STAI), Rosenberg Self-Esteem Scale (RSE), and Five Facet Mindfulness Questionnaire (5Facet). Regressions are shown separately for female and male subjects. For a complete description of the variables and their acronyms, refers to Tables 1, 2.
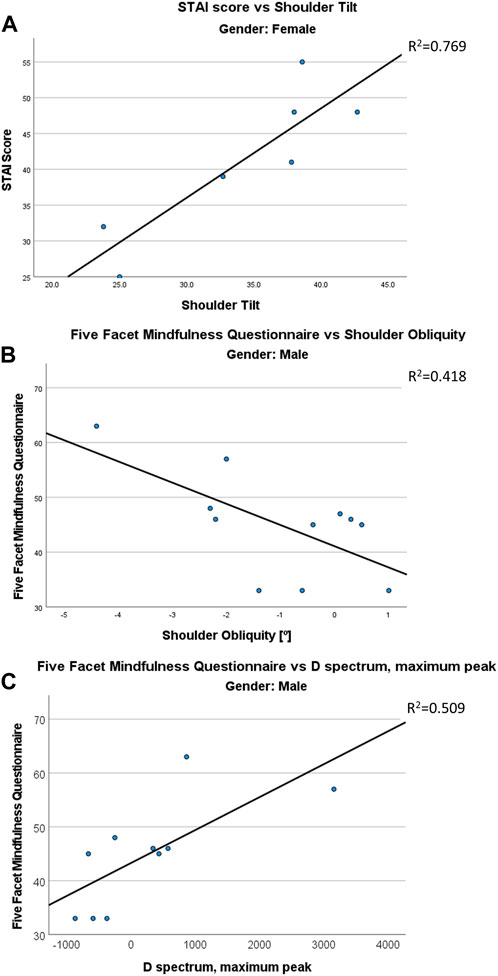
Figure 6. Regressions between emotional states and stability/postural parameters. Regression between State-Trait Anxiety Inventory (STAI) score with Shoulder Tilt in females (A). Regression between the Five Facet score and the shoulder obliquity (B) and with Max peak of the spectrum of the distance from the barycenter (C) in males.
3.5 Posture and emotion
As for the connection to breathing, the linear relation between posture and emotional scores was studied only for the results related to the state of “standard—open eyes.” Eighteen acquisitions (11 males and 7 females) were available for this analysis.
Women showed significant correlations between postural parameters and both STAI (adjR2 = 0.723) and RSE (adjR2 = 0.978) scores while men showed significant correlations between postural parameters and all emotional ones (Table 7).
4 Discussions
The proposed protocol allowed for the simultaneous analysis of breathing, postural stability, and emotional indicators. Although the high number of reflective markers used for the analysis required a lengthy preparation time (around 30 min), the protocol allowed us to test the relations between breathing, postural stability, and psychological health, observing significant results and initiating the development of a relational map among the main sets of variables in the study.
Subjects showed general difficulties in performing abdominal breathing. The majority were not able to change their breathing pattern when requested, confirming previously reported findings (Tassani et al., 2019). A few minutes of training before acquisitions were not sufficient for subjects to learn to perform abdominal breathing intentionally. This result is consistent with the literature. Studies assessing the effects of abdominal breathing on a pathology found that deep breathing training phases vary from 3 weeks to 56 months in asthma (Santino et al., 2020). It is, therefore, reasonable to consider that subjects unable to perform deep breathing could not learn to do so during a brief session of a few minutes.
In this study, some subjects were constantly breathing abdominally or pulmonary and kept the same pattern for all four acquisitions. They only changed the total volume inhaled. In other cases, subjects were breathing abdominally at first but changed to pulmonary when asked to perform deep abdominal breathing. Subjects did not seem capable of controlling their breathing pattern intentionally. Only one subject was able to start deep abdominal breathing when requested. Furthermore, it must be considered that the threshold defined for the definition of abdominal breathing was arbitrary. In this study to define a breathing pattern as abdominal, the abdominal compartment must be used more than the pulmonary one. When a more conservative threshold for deep breathing classification is applied, in which the abdominal compartment is used for 60% of the abdominal and pulmonary volumes together, the number of acquisitions classified as abdominal would drop to only 5 (data in the Supplementary Material). This forced the use of a less strict threshold to classify rather different patterns as abdominal (Figure 7).
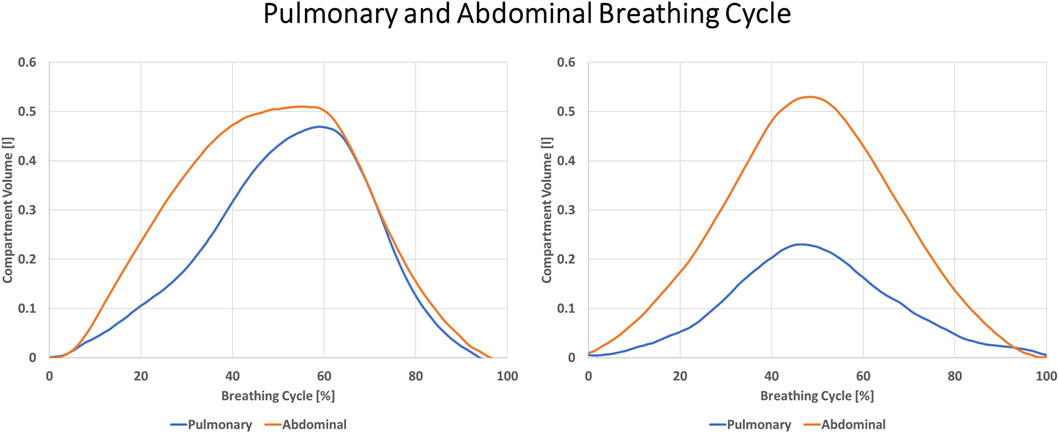
Figure 7. Two different breathing patterns are presented. On the left, Abdominal and Pulmonary patterns are similar with a small prevalence of abdominal breathing. On the right, the abdominal compartment is dominant over the whole breathing cycle. Both patterns were classified as Abdominal.
Given the importance that literature attributes to the ability to control breathing patterns for both physical (Hodges and Gandevia, 2000; Gilbert, 2003; Hodges et al., 2007) and emotional (Perciavalle et al., 2017; Hopper et al., 2019; Balban et al., 2023) management, this study presents a worrying scenario for young university students. Worries were confirmed by the number of subjects presenting high levels of anxiety in this study. The situation might be even more critical for female subjects who showed less capability of abdominal breathing (Table 3) and presented more cases of high anxiety (4 females and 3 males).
The reasons for this disparity between male and female subjects are not clear. The effect of sex on chest wall kinematics in literature is controversial. In agreement with our results, some authors have reported a relatively lower abdominal contribution to tidal volume and smaller abdominal dimensional changes in females compared to males during quiet breathing (Fugl Meyer, 1974; Gilbert et al., 1981; Romei et al., 2010). Others did not find any sex-related differences in thoraco-abdominal motion during quiet breathing in different postures (Sharp et al., 1975; Verschakelen and Demedts, 1995). However, the authors would like to stress the importance of not restricting the study of causes of this difference to biological ones. Sociological causes such as differences in gender beauty canons can lead to different perceptions of abdominal breathing and should also be explored.
Differences in behavior between sexes are another result of this study. In fact, while breathing was found to be related to both physical and emotional variables, these relations were found to be different between the two sexes. The analysis of individual indicators and their meaning was not the aim of this study; however, specific patterns can be identified and are for future research to be confirmed.
Postural characteristics were shown to be strongly related to breathing for both sexes (Table 6). The linear regression analysis showed a strong linear relation of abdominal rib cage and abdomen percentages to postural parameters. In males, postural parameters correctly classified 84% of acquisitions as abdominal or pulmonary (Table 5). This is an interesting result since posture parameters also showed the highest link to emotional scores, especially STAI and RSE, for both males and females (Table 7). These findings reinforce results obtained in the relation between breathing and emotional states and suggest the role of breathing as a mediator.
The results of the stability analysis presented weaker relations, especially in females. In males, MANOVA showed no significant results, however, the breathing factor was close to significance for both spatio-temporal (p = 0.027) and frequency (p = 0.03) parameters. In the regression analysis, both abdominal rib cage and abdomen percentages were related to stability parameters. Three out of four predictors selected by the stepwise procedure were the same, but the coefficients were inverted. This result suggests that, while an increase in the use of the abdominal rib cage compartment was related to the decrease in stability, the increased use of the abdominal compartment increased stability. SPM results of accelerometer data were found to be in the same direction. In several moments along the 3-min acquisition, subjects classified as using abdominal breathing showed a reduced acceleration of the head, suggesting higher stability (Figure 4). This supports the idea that a relaxed posture, decreasing co-contraction, can increase subject stability (Tassani et al., 2019). In males, stability was also found to be related to emotional states, whereas an increase in STAI score was related to a decrease in stability.
The main limitation of this study is in its aim of presenting a holistic protocol for the study of a breathing-physical-emotional relation. The physical sphere was analyzed in the form of stability and posture, and the emotional sphere in terms of anxiety and self-esteem, and for both measurement and analysis protocols had to be defined. For this reason, statistical analyses were presented as parts within a whole protocol. Results must be considered with caution and confirmed by future studies involving a bigger sample size. This limitation becomes clearer in the relation between breathing and emotional scores in females. In Figure 5 we can see how a single bivariate outlier can change the relation between RSE score and Abdominal Rib Cage percentage from not significant to R2 = 0.838. Nonetheless, this study allows us to underline difficulties and criticisms that, based on this research and presented literature, might be common to many young university students.
In conclusion, this study shows how difficulties in performing deep abdominal breathing can be related to elevated anxiety scores and decreased stability, depicting a circular self-sustaining relationship that can decrease quality of life, undermine learning, produce muscular co-contraction and, in the long term, lead to the development of musculoskeletal disorders. While holistic techniques are more frequently appearing in literature to address these problems, the presented protocol can be used to quantify the effect of such techniques on subjects.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Institutional Committee for Ethical Review of Projects of Universitat Pompeu Fabra (CIREP-UPF). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
ST: Conceptualization, Investigation, Methodology, Supervision, Writing–original draft, Writing–review and editing, Project administration, Funding acquisition. PC: Data curation, Investigation, Methodology, Writing–original draft, Writing–review and editing. MB: Conceptualization, Investigation, Methodology, Writing–original draft, Writing–review and editing. MV: Methodology, Writing–review and editing. JR: Conceptualization, Investigation, Writing–review and editing. JM: Data curation, Investigation, Writing–review and editing. MP-T: Investigation, Writing–review and editing. MiG-B: Funding acquisition, Writing–review and editing. DH-L: Conceptualization, Funding acquisition, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Funds from the Spanish Government (MDM-2015-0502) and from Center for the Studies on Planetary Wellbeing (BYMBOS-PLAWB00420) are acknowledged. This work has been also partially funded by MICIU/AEI/10.13039/501100011033 (PID2020-112584RB-C33). DHL (Serra Húnter) also acknowledges the support by ICREA under the ICREA Academia programme.
Acknowledgments
A special thanks to all the volunteers who participated in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fbioe.2024.1347939/full#supplementary-material
References
Abdollahi, A., Hosseinian, S., Beh-Pajooh, A., and Carlbring, P. (2017). Self-concealment mediates the relationship between perfectionism and attitudes toward seeking psychological help among adolescents. Psychol. Rep. 120, 1019–1036. doi:10.1177/0033294117713495
Aliverti, A., and Pedotti, A. (2003). Opto-Electronic plethysmography. Monaldi Arch. Chest Dis. 59, 12–16. doi:10.1007/978-88-470-2916-3_5
Balban, M. Y., Neri, E., Kogon, M. M., Weed, L., Nouriani, B., Jo, B., et al. (2023). Brief structured respiration practices enhance mood and reduce physiological arousal. Cell Rep. Med. 4, 100895. doi:10.1016/j.xcrm.2022.100895
Brattberg, G. (2004). Do pain problems in young school children persist into early adulthood? A 13-year follow-up. Eur. J. Pain 8, 187–199. doi:10.1016/j.ejpain.2003.08.001
Brett, M., Penny, W., and Kiebel, S. (2003). Introduction to random field theory. Human brain function. Second Edition. doi:10.1016/B978-012264841-0/50046-9
Burgos, C. P., Gartner, L., Ballester, M. A. G., Noailly, J., Stocker, F., Schonfelder, M., et al. (2020). In-ear accelerometer-based sensor for gait classification. IEEE Sens. J. 20, 12895–12902. doi:10.1109/JSEN.2020.3002589
Busch, V., Magerl, W., Kern, U., Haas, J., Hajak, G., and Eichhammer, P. (2012). The effect of deep and slow breathing on pain perception, autonomic activity, and mood processing — an experimental study. Pain Med. 13, 215–228. doi:10.1111/j.1526-4637.2011.01243.x
Byeon, Y. H., Lee, J. Y., Kim, D. H., and Kwak, K. C. (2020). Posture recognition using ensemble deep models under various home environments. Appl. Sci. Switz. 10, 1287. doi:10.3390/app10041287
Cappozzo, A., Della Croce, U., Leardini, A., and Chiari, L. (2005). Human movement analysis using stereophotogrammetry. Part 1: theoretical background. Gait Posture 21, 186–196. doi:10.1016/j.gaitpost.2004.01.010
Chiari, L., Rocchi, L., and Cappello, A. (2002). Stabilometric parameters are affected by anthropometry and foot placement. Clin. Biomech. 17, 666–677. doi:10.1016/S0268-0033(02)00107-9
Davis, R. B., Õunpuu, S., Tyburski, D., and Gage, J. R. (1991). A gait analysis data collection and reduction technique. Hum. Mov. Sci. 10, 575–587. doi:10.1016/0167-9457(91)90046-Z
De Blasiis, P., Caravaggi, P., Fullin, A., Leardini, A., Lucariello, A., Perna, A., et al. (2023). Postural stability and plantar pressure parameters in healthy subjects: variability, correlation analysis and differences under open and closed eye conditions. Front. Bioeng. Biotechnol. 11, 1198120. doi:10.3389/fbioe.2023.1198120
De Blasiis, P., Fullin, A., Caravaggi, P., Lus, G., Melone, M. A., Sampaolo, S., et al. (2022). Long-term effects of asymmetrical posture in boxing assessed by baropodometry. J. Sports Med. Phys. Fit. 62, 350–355. doi:10.23736/S0022-4707.21.12040-7
De Faria Júnior, N. S., Santos, I. R., Dias, I. S., Urbano, J. J., Da Palma, R. K., Fonsêca, N. T., et al. (2013). Opto-electronic plethysmography: noninvasive and accurate measurement of the volume of the chest wall and its different thoraco-abdominal compartments. Clin. Exp. Med. Lett. 54, 147–150. doi:10.12659/mst.889664
Diepenmaat, A. C. M., Van Der Wal, M. F., De Vet, H. C. W., and Hirasing, R. A. (2006). Neck/shoulder, low back, and arm pain in relation to computer use, physical activity, stress, and depression among Dutch adolescents. Pediatrics 117, 412–416. doi:10.1542/peds.2004-2766
Ellebrecht, D. B., Gola, D., and Kaschwich, M. (2022). Evaluation of a wearable in-ear sensor for temperature and heart rate monitoring: a pilot study. J. Med. Syst. 46, 91. doi:10.1007/s10916-022-01872-6
Ercan, I., Hafizoglu, S., Ozkaya, G., Kirli, S., Yalcintas, E., and Akaya, C. (2015). Examinando los puntajes de corte para el inventario de ansiedad estado-rasgo. Rev. Argent. Clinica Psicol. 24.
Fugl Meyer, A. R. (1974). Relative respiratory contribution of the rib cage and the abdomen in males and females with special regard to posture. Respiration 31, 240–251. doi:10.1159/000193113
Fullin, A., Caravaggi, P., Picerno, P., Mosca, M., Caravelli, S., De Luca, A., et al. (2022). Variability of postural stability and plantar pressure parameters in healthy subjects evaluated by a novel pressure plate. Int. J. Environ. Res. Public Health 19, 2913. doi:10.3390/ijerph19052913
Gilbert, C. (2003). Clinical applications of breathing regulation: beyond anxiety management. Behav. Modif. 27, 692–709. doi:10.1177/0145445503256322
Gilbert, R., Auschincloss, J. H., and Peppi, D. (1981). Relationship of rib cage and abdomen motion to diaphragm function during quiet breathing. Chest 80, 607–612. doi:10.1378/chest.80.5.607
Hodges, P. W., and Gandevia, S. C. (2000). Changes in intra-abdominal pressure during postural and respiratory activation of the human diaphragm. J. Appl. Physiol. 89, 967–976. doi:10.1152/jappl.2000.89.3.967
Hodges, P. W., Sapsford, R., and Pengel, L. H. M. (2007). Postural and respiratory functions of the pelvic floor muscles. Neurourol. Urodyn. 26, 362–371. doi:10.1002/nau.20232
Hopper, S. I., Murray, S. L., Ferrara, L. R., and Singleton, J. K. (2019). Effectiveness of diaphragmatic breathing for reducing physiological and psychological stress in adults: a quantitative systematic review. JBI Database Syst. Rev. Implement Rep. 17, 1855–1876. doi:10.11124/JBISRIR-2017-003848
Isomaa, R., Väänänen, J. M., Fröjd, S., Kaltiala-Heino, R., and Marttunen, M. (2013). How low is low? Low self-esteem as an indicator of internalizing psychopathology in adolescence. Health Educ. Behav. 40, 392–399. doi:10.1177/1090198112445481
Kim, M. S., Cha, Y. J., and Choi, J. D. (2017). Correlation between forward head posture, respiratory functions, and respiratory accessory muscles in young adults. J. Back Musculoskelet. Rehabil. 30, 711–715. doi:10.3233/BMR-140253
Massaroni, C., Carraro, E., Vianello, A., Miccinilli, S., Morrone, M., Levai, I. K., et al. (2017). Optoelectronic plethysmography in clinical practice and research: a review. Respiration 93, 339–354. doi:10.1159/000462916
McFarlane, A. C. (2007). Stress-related musculoskeletal pain. Best. Pract. Res. Clin. Rheumatol. 21, 549–565. doi:10.1016/j.berh.2007.03.008
Pataky, T. C. (2012). One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Engin 15, 295–301. doi:10.1080/10255842.2010.527837
Perciavalle, V., Blandini, M., Fecarotta, P., Buscemi, A., Di Corrado, D., Bertolo, L., et al. (2017). The role of deep breathing on stress. Neurol. Sci. 38, 451–458. doi:10.1007/s10072-016-2790-8
Prins, Y., Crous, L., and Louw, Q. (2008). A systematic review of posture and psychosocial factors as contributors to upper quadrant musculoskeletal pain in children and adolescents. Physiother. Theory Pract. 24, 221–242. doi:10.1080/09593980701704089
Rocchi, L., Chiari, L., and Cappello, A (2004). Feature selection of stabilometric parameters based on principal component analysis. Med. Biol. Eng. Comput. 42, 71–79. doi:10.1007/BF02351013
Romei, M., Mauro, A.L, D’Angelo, M. G., Turconi, A. C., Bresolin, N., Pedotti, A., et al. (2010). Effects of gender and posture on thoraco-abdominal kinematics during quiet breathing in healthy adults. Respir. Physiol. Neurobiol. 172, 184–191. doi:10.1016/j.resp.2010.05.018
Santino, T. A., Chaves, G. S. S., Freitas, D. A., Fregonezi, G. A. F., and Mendonça, K. M. P. P. (2020). Breathing exercises for adults with asthma. Cochrane Database Syst. Rev. 2020, CD001277. doi:10.1002/14651858.CD001277.pub4
Sawatzky, R. G., Ratner, P. A., Richardson, C. G., Washburn, C., Sudmant, W., and Mirwaldt, P. (2012). Stress and depression in students: the mediating role of stress management self-efficacy. Nurs. Res. 61, 13–21. doi:10.1097/NNR.0b013e31823b1440
Sharp, J. T., Goldberg, N. B., Druz, W. S., and Danon, J. (1975). Relative contributions of rib cage and abdomen to breathing in normal subjects. J. Appl. Physiol. 39, 608–618. doi:10.1152/jappl.1975.39.4.608
Sheikhhoseini, R., Shahrbanian, S., Sayyadi, P., and O’Sullivan, K. (2018). Effectiveness of therapeutic exercise on forward head posture: a systematic review and meta-analysis. J. Manip. Physiol. Ther. 41, 530–539. doi:10.1016/j.jmpt.2018.02.002
Swiecki, Z., Ruis, A. R., Farrell, C., and Shaffer, D. W. (2019). Assessing individual contributions to Collaborative Problem Solving: a network analysis approach. Comput. Hum. Behav. 104, 105876. doi:10.1016/j.chb.2019.01.009
Tassani, S., Font-Llagunes, J. M., González Ballester, M. Á., and Noailly, J. (2019). Muscular tension significantly affects stability in standing posture. Gait Posture 68, 220–226. doi:10.1016/j.gaitpost.2018.11.034
Verschakelen, J. A., and Demedts, M. G. (1995). Normal thoracoabdominal motions: influence of sex, age, posture, and breath size. Am. J. Respir. Crit. Care Med. 151, 399–405. doi:10.1164/ajrccm.151.2.7842198
Wong, W. Y., and Wong, M. S. (2008). Smart garment for trunk posture monitoring: a preliminary study. Scoliosis 3, 7. doi:10.1186/1748-7161-3-7
Keywords: breathing, posture, stability, psychological health, emotion, Wellbeing
Citation: Tassani S, Chaves P, Beardsley M, Vujovic M, Ramírez J, Mendoza J, Portero-Tresserra M, González-Ballester MA and Hernández-Leo D (2024) Breathing, postural stability, and psychological health: a study to explore triangular links. Front. Bioeng. Biotechnol. 12:1347939. doi: 10.3389/fbioe.2024.1347939
Received: 01 December 2023; Accepted: 14 March 2024;
Published: 02 April 2024.
Edited by:
Andrea Malandrino, Universitat Politecnica de Catalunya, SpainReviewed by:
Paolo De Blasiis, University of Campania Luigi Vanvitelli, ItalyFranco Simini, Universidad de la República, Uruguay
Copyright © 2024 Tassani, Chaves, Beardsley, Vujovic, Ramírez, Mendoza, Portero-Tresserra, González-Ballester and Hernández-Leo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simone Tassani, c2ltb25lLnRhc3NhbmlAdXBmLmVkdQ==