 Daniel Holanda Barroso1,2*
Daniel Holanda Barroso1,2* Renata Trindade Gonçalves1Joadyson Silva Barbosa1
Renata Trindade Gonçalves1Joadyson Silva Barbosa1 Jorgeth de Oliveira Carneiro da Motta1
Jorgeth de Oliveira Carneiro da Motta1 Gustavo Subtil Magalhães Freire1
Gustavo Subtil Magalhães Freire1 Ciro Martins Gomes1,2,3
Ciro Martins Gomes1,2,3 Raimunda Nonata Ribeiro Sampaio1,2,3,4
Raimunda Nonata Ribeiro Sampaio1,2,3,4- 1Hospital Universitário de Brasília, Universidade de Brasília, Brasília, Brazil
- 2Laboratório de Dermatomicologia da Faculdade de Medicina, Universidade de Brasília, Brasília, Brazil
- 3Programa de Pós-Graduação em Ciências Médicas, Faculdade de Medicina, Universidade de Brasília, Brasília, Brazil
- 4Pós-Graduação de Ciências da Saúde da Faculdade de Ciências Saúde, Universidade de Brasília, Brasília, Brazil
Background: Pentavalent antimonials (PAs) are the primary therapeutic option for American tegumentary leishmaniasis (ATL). However, the use of these drugs is complicated by adverse events (AEs), resistance and contraindications. Alternative therapies relative effectiveness is not well established.
Objective: This study compared the effectiveness of liposomal amphotericin B (LAB) with intravenous meglumine antimoniate (NMG) in the treatment of ATL. We also analysed and compared associated AEs and treatment interruption rates.
Methods: This was a retrospective cohort study from Brazil. The potential risk factors for the primary outcome were age, sex, total cutaneous lesion area, presence of mucosal lesions, AEs and treatment interruption. The primary outcome was lesion healing within 6 months of treatment. AEs and treatment interruption were also analysed. Multiple analytic strategies were employed to evaluate the reliability of the results.
Results: Before propensity score (PS) matching, patients in the LAB group were older and had a higher frequency of mucosal lesions. The NMG group had a higher cure rate than the LAB group (cure rate 88% versus 55% respectively) in the adjusted analysis (relative risk (RR)=1.55 95% CI: 1.19 - 2.02) and after PS matching (RR=1.63 95% CI: 1.20 - 2.21). NMG group had a higher AE rate (event rate 52% versus 44%) in the adjusted analysis (RR= 1.61, 95% CI: 1.06 - 2.43, p=0.02), but this result was not observed after PS matching (RR= 0.87, 95% CI: 0.49 -1.52, p= 0.61).
Conclusions: We observed that the NMG group had a higher cure rate than the LAB group, with an equivocally higher EV rate in the adjusted analysis.
Introduction
Leishmaniasis is a vector-borne disease caused by a protozoan in the Leishmania genus (Burza et al., 2018); it is known to cause a wide variety of clinical syndromes, with an estimated world incidence of 700,000 to 1 million cases each year (World Health organization, 2021). The disease burden is estimated to be higher than those of leprosy, dengue fever and Chagas disease (Hotez et al., 2004). American tegumentary leishmaniasis (ATL) is likely to have a greater impact on a patient`s quality of life due to the possible development of deforming mucosal lesions (Motta et al., 2007; Luz et al., 2014).
Although the therapeutic landscape is slowly changing, pentavalent antimonials (PAs) (including N-methyl glucamine, NMG) are currently the first-line treatment for ATL (González et al., 2009; Pinart et al., 2020). The use of these drugs is problematic because they can induce severe and potentially fatal adverse events (AEs), such as arrhythmias, renal toxicity, hepatitis and pancreatitis (Kopke et al., 1993; Oliveira et al., 2011; Lyra et al., 2016). Alternatives to PAs include amphotericin B formulations, pentamidine, miltefosine, fluconazole, and ketoconazole (Aronson et al., 2017). According to a recent systematic review, however, for ATL, none of these drugs can be considered equivalent to PAs with a high or moderate level of evidence (Pinart et al., 2020). This may reflect poor designs of and reporting in most studies (Pinart et al., 2020).
Amphotericin B is an antifungal agent that has been used to treat leishmaniasis since 1960 (SAMPAIO et al., 1960); it is generally considered a second-line treatment in cases of therapeutic failure, contraindications or intolerance to PAs (Berman, 1988; Lima et al., 2007). Despite its recommendation in therapeutic guidelines (Aronson et al., 2017; Transmissíveis, 2017), published studies have shown ambiguous results regarding its efficacy (González et al., 2009; Pinart et al., 2020). Additionally, amphotericin B use has been classically associated with moderate to severe AEs, but high-quality studies evaluating this topic are scarce (Oliveira et al., 2011). Furthermore, lipid formulations of this drug, with better safety and efficacy profiles, have been studied (Walsh et al., 1999; Kleinberg, 2006; Grazziotin et al., 2018), making it challenging to derive definitive conclusions about the optimal drug for treatment. Liposomal amphotericin B (LAB) is a currently available systemic antileishmanial agent that has been successfully used in case series to treat old world cutaneous leishmaniasis due to Leishmania major (Wortmann et al., 2010), Leishmania tropica (Solomon et al., 2011) and Leishmania aethiopica (Zanger et al., 2011). In ATL, this drug was initially proposed in Brazil by our group with World Health Organization (WHO) sponsorship (Sampaio and Marsden, 1997), being reportedly useful to treat the main new world species: Leishmania braziliensis, Leishmania guyanensis (Senchyna et al., 2020), L. amazonensis(Soares et al., 2020) and Leishmania panamensis(Cannella et al., 2011). The liposomal formulation of amphotericin has high potential for clinical benefit due to its well-known effective management of other infections (Guery et al., 2017) and better safety profile than its conventional form with less nephrotoxicity, infusion reactions and hypomagnesemia (Wade et al., 2013). However, due to its high cost, few data from clinical studies on the clinical benefit of this formulation in the treatment of ATL are available (Guery et al., 2017). Additional challenges in the completion of clinical trials comparing amphotericin B and PAs are the high dropout and interruption rates, which are possibly related to AEs and rigorous therapeutic schedules (Neves et al., 2011; Solomon et al., 2013).
The main objective of the present study was to evaluate the ATL cure rate in patients receiving LAB and to compare the cure rate with that in those receiving intravenous meglumine antimoniate (IV-NMG) in a tertiary Brazilian leishmaniasis reference centre. We also aimed to compare the incidence rates of AEs and the rates of treatment interruption between the two treatment groups.
Materials and methods
Population and case definition
This retrospective cohort study included ATL patients treated with NMG or LAB at the University Hospital of Brasília, Brazil, from 1992 to 2017. Inclusion criteria was the presence of a clinical lesion compatible with ATL associated with a positive parasitological test (direct examination, culture, polymerase chain reaction or the presence of amastigotes in the histopathological exam) or at least two non-parasitological exams(serology, leishmanin skin test or compatible histopathological exam) (Gomes et al., 2014). We excluded patients who received treatment 6 months prior to the main evaluation, those with a follow-up period of less than six months. We also excluded patients in use of immunosuppressive drugs or with immunosuppressive diseases including HIV/AIDS, solid organ transplant, chronic kidney disease and cancer diagnosis. In the primary analysis one hundred and ten patients were included (63 in the NMG group and 47 in the LAB group).
Ethics
This study was approved by the research ethics committee of the faculty of medicine of the University of Brasília, with the following CAAE 62110616.8.0000.5558. The referred committee waived the requirement to obtain informed consent since the present real-world data involves no more than minimal risk to subjects.
Sampling
Sample size calculation was performed using Stata 17 software (College Station, TX: Stata Press. StataCorp, 2021) considering the response rates of 81% in the LAB group and 99.9% in the NMG group obtained in a previous pilot study (Motta and Sampaio, 2012). Based on these rates, a sample of 37 patients in each group would result in 80% power to identify significant differences between the groups, with a significance level of 5%. Additional evaluations including the analysis of other outcomes and the analysis of simultaneous predictors were accessed by a post hoc strategy.
Intervention
We compared the NMG and LAB interventions. NMG was used in accordance with the recommendations of Brazil`s Ministry of Health (10 to 20 mg SbV/kg/day for 20 days for the cutaneous form and for 30 days for the mucosal form). LAB was administered at a dosage of 1-3 mg/kg/day in at least 5 days.
Outcomes
The main outcome was cure, defined as complete healing (reepithelization without infiltrations or erythema) of the lesion by the 180th day after the first medication dose. Interruption of treatment for more than 7 days and AEs of any grade were secondary outcomes. According to the institutional protocol, patients were monitored at least weekly during treatment and at 2, 3 and 6 months after treatment. Laboratorial alterations in electrocardiogram results, liver enzyme levels or kidney function indicators were monitored at each visit to monitor for AEs.
Statistical analysis
The cure rate, occurrence of AEs and treatment interruption rate were individually considered dependent variables, and the treatment group (NMG or LAB) was considered an independent variable. Initially, we performed univariate analyses to identify associations between the independent and dependent variables. Sensitivity analysis was performed to evaluate whether methodological shortcomings could be responsible for the identified associations. To evaluate whether patient characteristics associated with the intervention allocation or with the outcome could be responsible for the results, Poisson regression with robust variance was performed to obtain adjusted relative risks (RRs) based on sex (male; female), age (years), presence of mucosal lesions and total area of lesions, including no cutaneous lesions. To evaluate the outcome of cure, we added treatment interruption and AE rates into the model. To evaluate the outcome of treatment interruption, the presence of AEs was also added. To further evaluate cure, patients were matched in a 1:1 ratio based on propensity scores (PS) using the “greedy” strategy considering a calibration of 0.2 standard deviations (SDs) using the same variables analysed in the multivariate analysis. Univariate analysis of the associations of predictors variables using Poisson regression with robust variance were also done in the whole population. To evaluate whether LAB dosage variation could explain the cure rates observed in this group, a univariate Poisson regression with robust variance model was constructed considering cure as a dependent variable and LAB dosage as the independent variable. Statistical analysis was performed in SAS 9.4 (SAS Institute, Cary, NC) and Stata 17 (StataCorp, College Station, TX). The results were considered statistically significant if p<0.05.
Results
The NMG group received the standard dosage recommended by the Brazilian Ministry of Health (15 mg SbV/kg/day for 20 days if there was no mucosal disease or for 30 days if there was mucosal disease). The total LAB dosage administered was 21.61 mg/kg ± 17.37 (SD). Patients who received LAB were older, had a higher frequency of mucosal lesions and had a lower cure rate than patients who received NMG (Tables 1, 2).
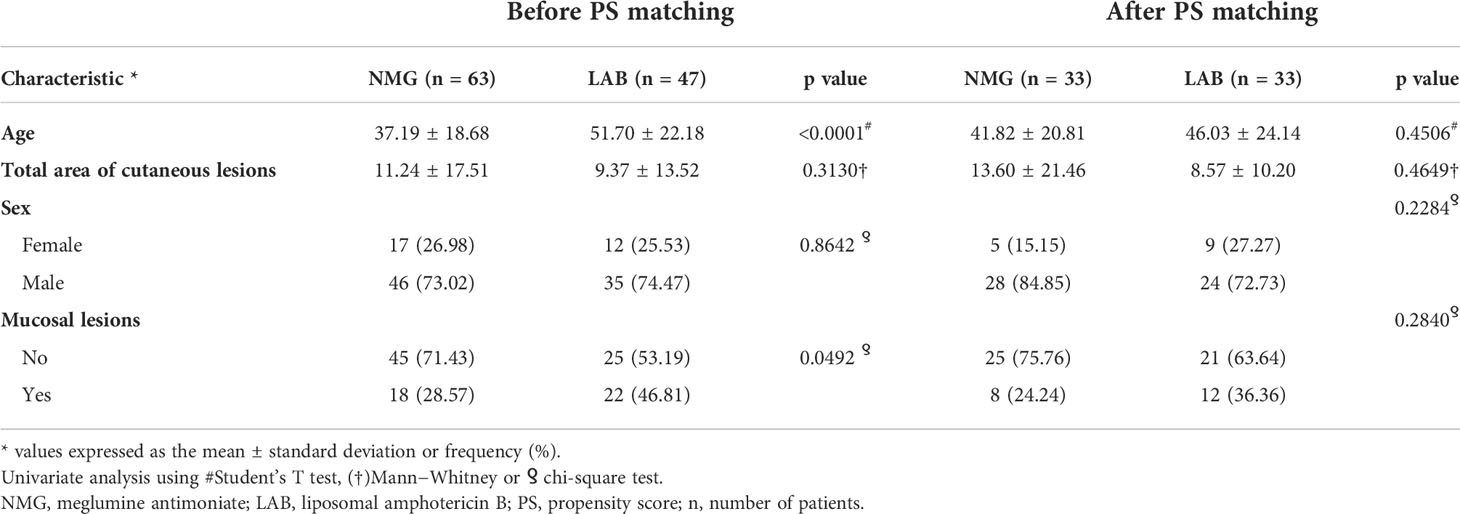
Table 1 Sample characteristics stratified by drug before and after PS matching.
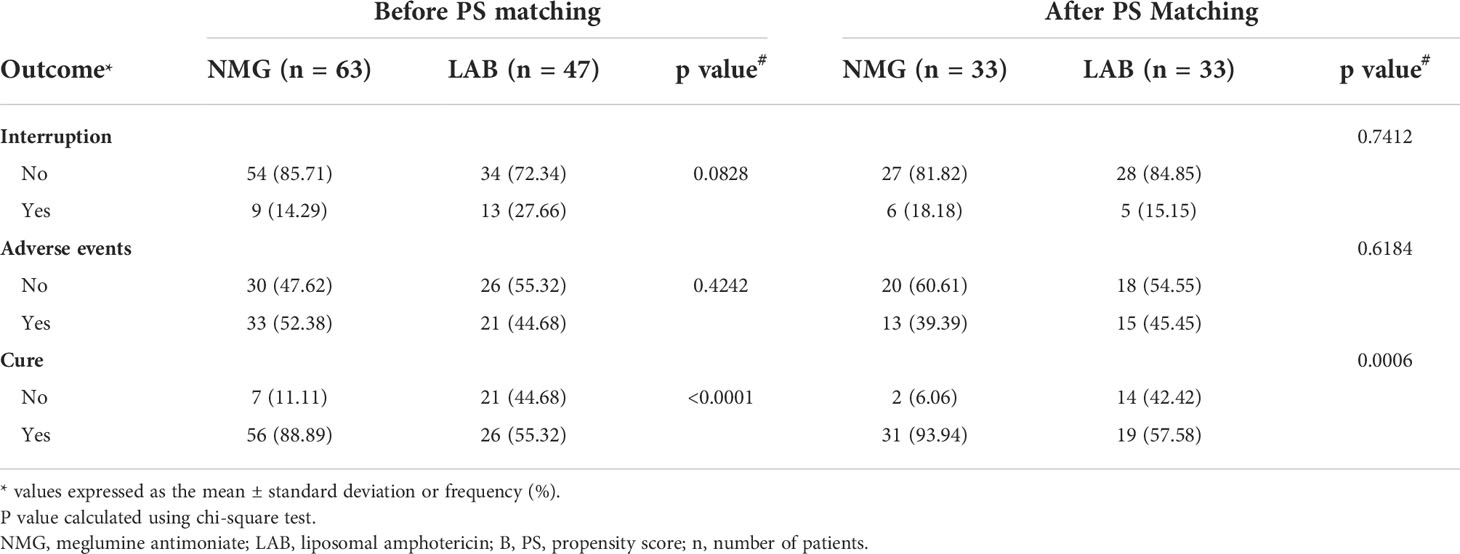
Table 2 Outcomes before and after PS matching.
We were able to match 33 patients in each treatment arm based on their PSs, obtaining well-balanced groups (Figure 1). The NMG group had a higher cure rate than the LAB group (cure rate 88% versus 55% respectively) in the adjusted analysis (RR=1.55 95% CI: 1.19 - 2.02) and after PS matching (RR=1.63 95% CI: 1.20 - 2.21). NMG group had a higher AEs rate (event rate 52% versus 44%) in the adjusted analysis (RR= 1.61, 95% CI: 1.06 - 2.43, p=0.02), but this result was not observed after PS matching (RR= 0.87, 95% CI: 0.49 -1.52, p= 0.61) (Table 3).
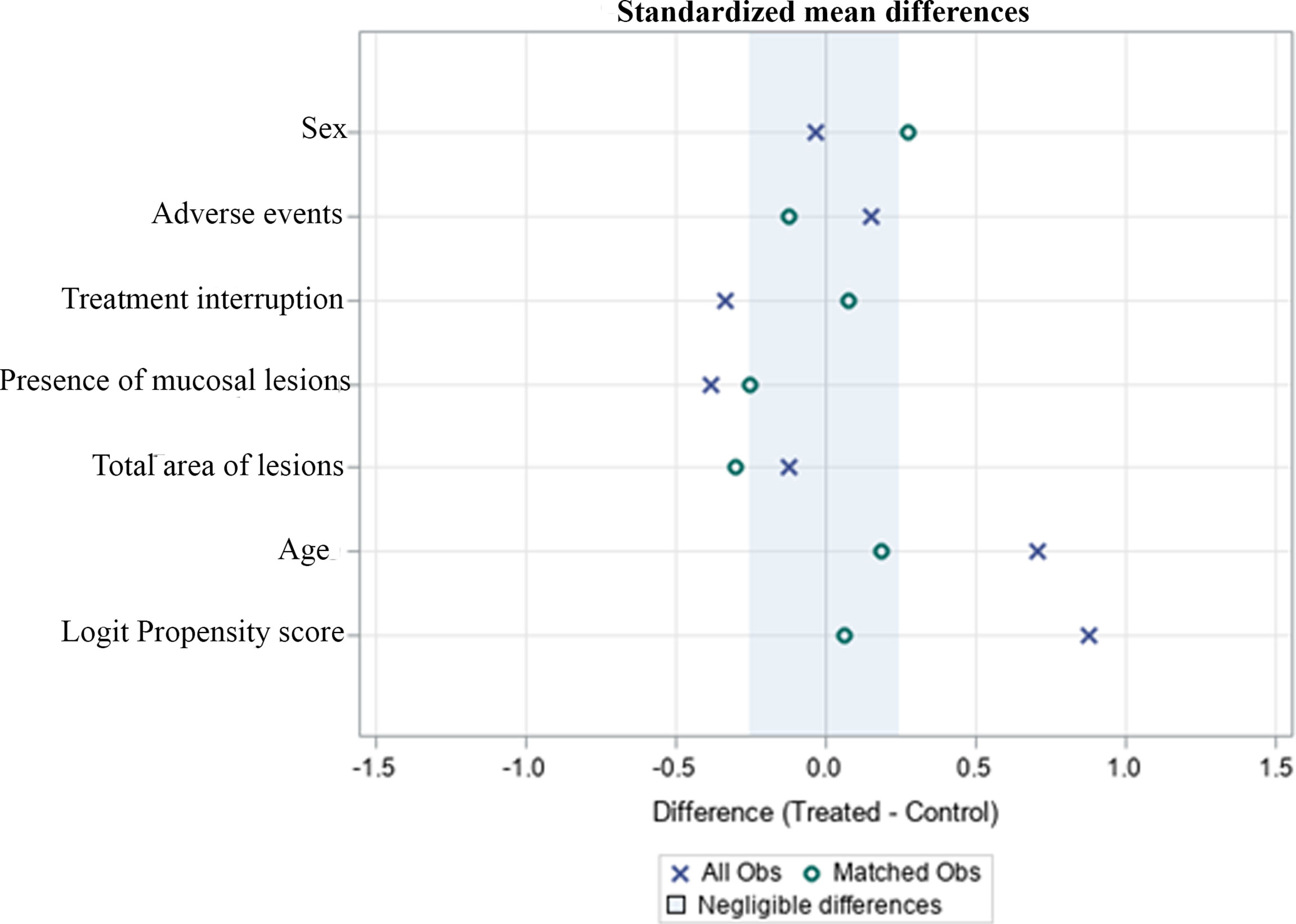
Figure 1 Standardized differences before and after PS matching comparing variables for patients treated with NMG and LAB drugs.
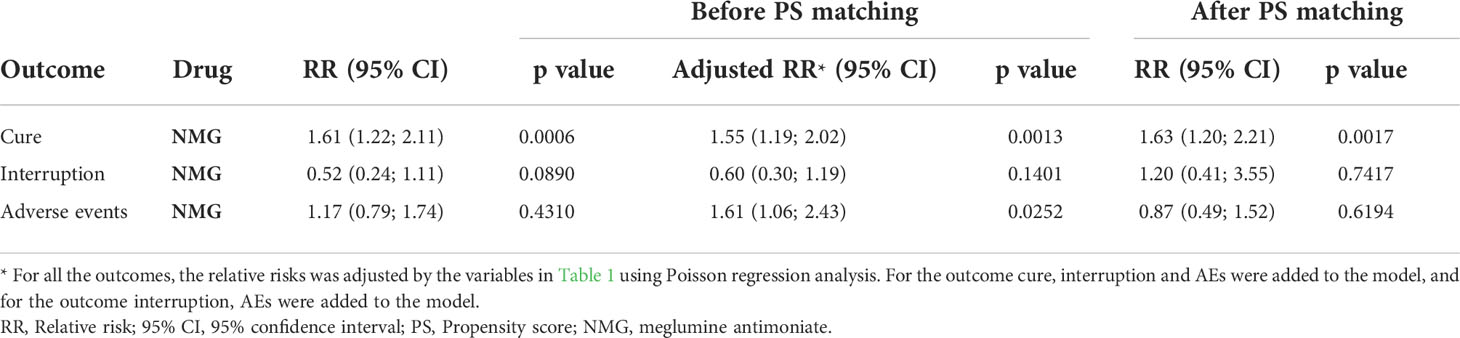
Table 3 Unadjusted and adjusted relative risks (RRs) and 95% confidence intervals (CIs) for cure, interruption and AEs before and after propensity score matching.
The LAB dosage was not associated with cure in the dosage range applied in this study. In the whole population, we found significant association between age 60 or greater and the outcome interruption of treatment (RR= 3.68, 95% CI: 1.75-7.73, p<0.01) and adverse events (RR= 1.75, 95% CI: 1.23- 2.48, p<0.01). Other relevant influences on the tested outcomes were not detected.
Discussion
High-quality clinical trials comparing the use of PAs with amphotericin B in ATL patients are lacking, and the recommendations of health agencies are based on case series and retrospective studies (Aronson et al., 2016; Pinart et al., 2020). The reported efficacy of amphotericin B in the literature is greater than 90% (Sampaio et al., 1971; Wortmann et al., 2010; Amato et al., 2011; Rocio et al., 2014). In a study from Bolivia, LAB had a superior cure rate when compared with sodium stibogluconate (SSG) (84% versus 70%), but the results were nonsignificant (Solomon et al., 2013). We expected that increasing the sample size would lead to significant differences between the groups. The better effectiveness of NMG observed in our study is not surprising since this is the standard drug for ATL treatment and the treatment with which other treatments are compared (Pinart et al., 2020). A study from French Guyana also showed a lower cure rate in patients who received LAB than in those who received NMG (Senchyna et al., 2020), although the difference did not reach statistical significance. The overall cure rate in LAB patients in this study (55.32%) was similar to that in the study by Guery et al. (44%), which also included patients with Old-World leishmaniasis (Guery et al., 2017). In another case series that included only mucosal leishmaniasis patients from Brazil, the cure rate was 93.1% (Cunha et al., 2015). This difference may be explained by the fact that in their study, therapeutic failure was defined as the absence of clinical response after two successive therapeutic cycles (Cunha et al., 2015), whereas retreatment with the same therapeutic scheme has been reported to promote clinical cure in some patients (Nogueira and Sampaio, 2001).
We also investigated the associations between treatment interruption and AEs. A previous study showed a higher rate of treatment interruption in patients who received PAs (SSG) than in those who received LAB (Solomon et al., 2013). In the study by Senchyna et al., NMG was associated with a higher rate of moderate AEs, defined as those with clinical symptoms but that did not lead to treatment interruption (Senchyna et al., 2020). Despite the possible development of formulation-specific adverse reactions (Szebeni et al., 2000; Roden et al., 2003), LAB is known to have a better safety profile than the other formulations (Wasan et al., 1994; Walsh et al., 1999; Wade et al., 2013). Accordingly, in this study, the adjusted RR for adverse events was higher in patients who received NMG than patients who received LAB. Although this result reached statistical significance, it was not reproduced after matching. Thus, the higher AE rate in the NMG group should be interpreted with caution and deserves further evaluation in larger studies specifically powered to evaluate comparative AEs between medication groups.
The age of patients and proportion of mucosal lesions in the current study are likely to be different from those in the overall population of ATL patients since older people and those with mucosal lesions are more likely to be referred to a tertiary care centre. In an epidemiological study performed in a primary care setting in Bahia, Brazil, only 4.3% of patients had mucosal lesions, and the average age of cutaneous leishmaniasis patients was 21 years (Jirmanus et al., 2012), which was younger than 37 years (NMG group) and 51 years (LAB group), as reported in our study. Thus, the convenience sample used in this study may limit the generalizability of our results. Additionally, in the primary analysis, patients who received LAB were significantly older and had a significantly higher frequency of mucosal lesions. Again, this may be explained by the increased risk of mucosal lesions with age (Machado-Coelho et al., 2005) and by the recommendation that people aged 50 years or older should be treated with amphotericin B according to the national guidelines(Transmissíveis, 2017). The lower cure rate observed in patients who received LAB, however, is unlikely explained by their basic characteristics since these results were consistent across multiple analytic strategies that included controlling for confounders.
One of the limitations of this study is its observational design. Although randomized clinical trials (RCTs) are the gold standard for analysing the intended effects of therapies, observational studies are as valid as RCTs to investigate AEs associated with medications (Vandenbroucke, 2008).Additionally, Interruption and dropout rates can be a treat to internal validity of clinical trials (Ravani et al., 2007) and have been important in studies of LAB for the treatment of leishmaniasis (Neves et al., 2011; Solomon et al., 2013). LAB studies have been limited by the cost of the medication, especially considering that ATL is highly prevalent in low-income countries (Guery et al., 2017). Thus, the relatively low cost, wide range of patients and rapidly obtained conclusions make observational studies an interesting approach to investigate the effects of LAB in ATL patients (Benson and Hartz, 2000). The main limitation of observational studies is related to treatment allocation, but the strategy used by our team, propensity analysis, is known to offset this issue (Feneck, 2007). Provided that important confounders are controlled for (Vandenbroucke, 2008), it has been shown that observational studies can produce results similar to those of RCTs (Benson and Hartz, 2000).
We therefore attempted to overcome the limitations of previous studies using an observational design coupled with an adequate analytical strategy. To do this we performed post hoc adjusted and PS matched analysis including clinical and individual characteristics to try to explain the associations found in the unadjusted analysis. As shown by other studies, age is associated with increased adverse events rate (Araujo-Melo et al., 2010; Diniz et al., 2012; do Lago et al., 2018) and immunological responses (Carvalho et al., 2015). As expected, we have found that elderly patients had a higher rate of adverse events and interruption of treatment but, as previously suggested, we were not able to find an association between age and treatment response (do Lago et al., 2018). Although sex (de Araújo Albuquerque et al., 2021), total area of lesions (Valencia et al., 2012) and the presence of mucosal lesions (García-Bustos et al., 2021) were all previously related with treatment failure, we were not able to find significant relationship with the outcome in our data.
In this cohort study from a L. braziliensis-endemic area (Gomes, 2014), NMG was associated with a higher cure rate than LAB, although it also had an equivocally higher AE rate. The consistency of the primary results across multiple analysis and their applicability in the real world setting of a Brazilian reference centre are the main strengths of this study. Is important to state, however, that their validity in the overall population is limited. Possible known confounders were controlled for in the analysis, but the presence of unknown covariates is a limitation in any observational study. As randomization is the only way to balance these covariates, our results should be confirmed in a large RCT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comitê de Ética em Pesquisa da Faculdade de Medicina da Universidade de Brasília, CAAE 62110616.8.0000.5558. Written informed consent for participation was not provided by the participants’ legal guardians/next of kin because: The referred committee waived the requirement to obtain informed consent since the present real-world data involves no more than minimal risk to subjects.
Author contributions
DB – conception, design, data acquisition, analysis, interpretation of data, drafting; RG - data acquisition, analysis, interpretation of data; JB - data acquisition, analysis, interpretation of data; JM - data acquisition, analysis; GM- data acquisition, analysis and interpretation; CG - conception, design, data acquisition, analysis, interpretation of data, drafting; RS - conception, design, data acquisition, analysis, interpretation of data, drafting, supervision. All: Final approval.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Amato, V. S., Tuon, F. F., Camargo, R. A., Souza, R. M., Santos, C. R., Nicodemo, A. C. (2011). Can we use a lower dose of liposomal amphotericin b for the treatment of mucosal American leishmaniasis? Am. J. Trop. Med. Hygiene 85 (5), 818. doi: 10.4269/ajtmh.2011.11-0287
Araujo-Melo, M., Meneses, A., Schubach, A., Moreira, J., Conceição-Silva, F., Salgueiro, M., et al. (2010). Risk factors associated with dizziness during treatment of mucosal leishmaniasis with meglumine antimoniate: 16-year retrospective study of cases from Rio de Janeiro, Brazil. J. Laryngology Otology 124 (10), 1056–1060. doi: 10.1017/S0022215110001325
Aronson, N., Herwaldt, B. L., Libman, M., Pearson, R., Lopez-Velez, R., Weina, P., et al. (2016). Diagnosis and treatment of leishmaniasis: clinical practice guidelines by the infectious diseases society of America (IDSA) and the American society of tropical medicine and hygiene (ASTMH). Clin. Infect. Dis. 63 (12), e202–e264. doi: 10.1093/cid/ciw670
Aronson, N., Herwaldt, B. L., Libman, M., Pearson, R., Lopez-Velez, R., Weina, P., et al. (2017). Diagnosis and treatment of leishmaniasis: Clinical practice guidelines by the infectious diseases society of America (IDSA) and the American society of tropical medicine and hygiene (ASTMH). Am. J. Trop. Med. Hygiene 96 (1), 24–45. doi: 10.4269/ajtmh.16-84256
Benson, K., Hartz, A. J. (2000). A comparison of observational studies and randomized, controlled trials. New Engl. J. Med. 342 (25), 1878–1886. doi: 10.1056/NEJM200006223422506
Berman, J. D. (1988). Chemotherapy for leishmaniasis: biochemical mechanisms, clinical efficacy, and future strategies. Rev. Infect. Dis. 10 (3), 560–586. doi: 10.1093/clinids/10.3.560
Burza, S., Croft, S. L., Boelaert, M. (2018). Leishmaniasis. Lancet 392 (10151), 951–970. doi: 10.1016/S0140-6736(18)31204-2
Cannella, A. P., Nguyen, B. M., Piggott, C. D., Lee, R. A., Vinetz, J. M., Mehta, S. R. (2011). A cluster of cutaneous leishmaniasis associated with human smuggling. Am. J. Trop. Med. Hygiene 84 (6), 847. doi: 10.4269/ajtmh.2011.10-0693
Carvalho, A. M., Amorim, C. F., Barbosa, J. L., Lago, A. S., Carvalho, E. M. (2015). Age modifies the immunologic response and clinical presentation of American tegumentary leishmaniasis. Am. J. Trop. Med. Hyg 92 (6), 1173–1177. doi: 10.4269/ajtmh.14-0631
Cunha, M. A., Leão, A. C., de Cassia Soler, R., Lindoso, J. A. (2015). Efficacy and safety of liposomal amphotericin b for the treatment of mucosal leishmaniasis from the new world: A retrospective study. Am. J. Trop. Med. Hyg 93 (6), 1214–1218. doi: 10.4269/ajtmh.15-0033
de Araújo Albuquerque, L. P., da Silva, A. M., de Araújo Batista, F. M., de Souza Sene, I., Costa, D. L., Costa, C. H. N. (2021). Influence of sex hormones on the immune response to leishmaniasis. Parasite Immunol. 43 (10-11), e12874. doi: 10.1111/pim.12874
Diniz, D. S., Costa, A. S. V., Escalda, P. M. F. (2012). The effect of age on the frequency of adverse reactions caused by antimony in the treatment of American tegumentary leishmaniasis in governador valadares, state of minas gerais, Brazil. Rev. da Sociedade Bras. Medicina Trop. 45, 597–600. doi: 10.1590/S0037-86822012000500011
do Lago, A. S., Nascimento, M., Carvalho, A. M., Lago, N., Silva, J., Queiroz, J. R., et al. (2018). The elderly respond to antimony therapy for cutaneous leishmaniasis similarly to young patients but have severe adverse reactions. Am Trop Med Hygiene 98 (5), 1317–1324. doi: 10.4269/ajtmh.17-0736
Feneck, R. (2007). Clinical research in anaesthesia; randomized controlled trials or observational studies? Eur. J. Anaesthesiology 24 (1), 1–5. doi: 10.1017/S0265021506001967
García-Bustos, M. F., González-Prieto, G., Paniz-Mondolfi, A. E., Parodi, C., Beckar, J., Monroig, S., et al. (2021). Risk factors for antimony treatment failure in American cutaneous leishmaniasis in northwestern-Argentina. PLoS Negl. Trop. Dis. 15 (1), e0009003. doi: 10.1371/journal.pntd.0009003
Gomes, C. M. (2014). Acurácia da reação em cadeia da polimerase em amostras de saliva, swab nasal e papel filtro oral no diagnóstico da leishmaniose tegumentar americana: estudo clínico, revisão sistemática da literatura e meta-análise. (Brasília, Brazil: Universidade de Brasília).
Gomes, C. M., Paula, N. A., Morais, O. O., Soares, K. A., Roselino, A. M., Sampaio, R. N. (2014). Complementary exams in the diagnosis of American tegumentary leishmaniasis. Bras. Dermatol. 89 (5), 701–709. doi: 10.1590/abd1806-4841.20142389
González, U., Pinart, M., Rengifo-Pardo, M., Macaya, A., Alvar, J., Tweed, J. (2009). Interventions for American cutaneous and mucocutaneous leishmaniasis. Cochrane Database Systematic Rev (2), CD004834–CD004834. doi: 10.1002/14651858.CD004834.pub2
Gordón-Núñez, M. A., Ferreira, S. J., Andrade, A. L.D.L.D., Luz, K. G., Milan, E. P., Galvão, H. C. (2014). New World Mucocutaneous Leishmaniasis with Oral Manifestations: Case Report and Damage Repair. Am J Infectious Dis 10 (4), 167–173. doi: 10.3844/ajidsp.2014.167.173
Grazziotin, L. R., Moreira, L. B., Ferreira, M. A. P. (2018). Comparative effectiveness and safety between amphotericin b lipid-formulations: a systematic review. Int. J. Technol. Assess. Health Care 34 (3), 343–351. doi: 10.1017/S026646231800034X
Guery, R., Henry, B., Martin-Blondel, G., Rouzaud, C., Cordoliani, F., Harms, G., et al. (2017). Liposomal amphotericin b in travelers with cutaneous and muco-cutaneous leishmaniasis: Not a panacea. PLoS Negl. Trop. Dis. 11 (11), e0006094. doi: 10.1371/journal.pntd.0006094
Hotez, P. J., Remme, J. H., Buss, P., George, G., Morel, C., Breman, J. G. (2004). Combating tropical infectious diseases: report of the disease control priorities in developing countries project. Clin. Infect. Dis. 38 (6), 871–878. doi: 10.1086/382077
Jirmanus, L., Glesby, M. J., Guimaraes, L. H., Lago, E., Rosa, M. E., Machado, P. R., et al. (2012). Epidemiological and clinical changes in American tegumentary leishmaniasis in an area of leishmania (Viannia) braziliensis transmission over a 20-year period. Am. J. Trop. Med. Hygiene 86 (3), 426–433. doi: 10.4269/ajtmh.2012.11-0378
Kleinberg, M. (2006). What is the current and future status of conventional amphotericin b? Int. J. antimicrobial Agents 27, 12–16. doi: 10.1016/j.ijantimicag.2006.03.013
Kopke, L. F. F., Café, M. E. M., Neves, L. B., Scherrer, M. A. R., Machado Pinto, J., Souza, M., et al. (1993). Morte após uso de antimonial pentavalente em leishmaniose tegumentar americana. An. Bras. Dermatol. 261, 259–260.
Lima, E., Porto, C., Motta, J., Sampaio, R. N. R. (2007). Tratamento da leishmaniose tegumentar americana. An. Bras. Dermatol. 82 (2), 111–124. doi: 10.1590/S0365-05962007000200002
Lyra, M. R., Passos, S. R. L., Pimentel, M. I. F., Bedoya-Pacheco, S. J., Valete-Rosalino, C. M., Vasconcellos, E. C. F., et al. (2016). Pancreatic toxicity as an adverse effect induced by meglumine antimoniate therapy in a clinical trial for cutaneous leishmaniasis. Rev. do Instituto Medicina Trop. São Paulo 58 (1), 68–73. doi: 10.1590/S1678-9946201658068
Machado-Coelho, G. L., Caiaffa, W. T., Genaro, O., Magalhaes, P. A., Mayrink, W. (2005). Risk factors for mucosal manifestation of American cutaneous leishmaniasis. Trans. R Soc. Trop. Med. Hyg 99 (1), 55–61. doi: 10.1016/j.trstmh.2003.08.001
Motta, A. C., Lopes, M. A., Ito, F. A., Carlos-Bregni, R., de Almeida, O. P., Roselino, A. M. (2007). Oral leishmaniasis: a clinicopathological study of 11 cases. Oral. Dis. 13 (3), 335–340. doi: 10.1111/j.1601-0825.2006.01296.x
Motta, J., Sampaio, R. (2012). A pilot study comparing low-dose liposomal amphotericin b with n-methyl glucamine for the treatment of American cutaneous leishmaniasis. J. Eur. Acad. Dermatol. Venereology 26 (3), 331–335. doi: 10.1111/j.1468-3083.2011.04070.x
Neves, L. O., Talhari, A. C., Gadelha, E. P., Silva Júnior, R. M., Guerra, J. A., Ferreira, L. C., et al. (2011). A randomized clinical trial comparing meglumine antimoniate, pentamidine and amphotericin b for the treatment of cutaneous leishmaniasis by leishmania guyanensis. Bras. Dermatol. 86 (6), 1092–1101. doi: 10.1590/s0365-05962011000600005
Nogueira, L. S. C., Sampaio, R. N. R. (2001). Estudo hospitalar de leishmaniose tegumentar americana (LTA): epidemiologia e tratamento. An. Bras. Dermatol. 76 (1), 51–62.
Oliveira, L. F., Schubach, A. O., Martins, M. M., Passos, S. L., Oliveira, R. V., Marzochi, M. C., et al. (2011). Systematic review of the adverse effects of cutaneous leishmaniasis treatment in the new world. Acta Trop. 118 (2), 87–96. doi: 10.1016/j.actatropica.2011.02.007
Pinart, M., Rueda, J.-R., Romero, G. A., Pinzón-Flórez, C. E., Osorio-Arango, K., Maia-Elkhoury, A. N. S., et al. (2020). Interventions for American cutaneous and mucocutaneous leishmaniasis. Cochrane Database Systematic Rev. 8, 1–337. doi: 10.1002/14651858.CD004834.pub3
Ravani, P., Parfrey, P. S., Dicks, E., Barrett, B. J. (2007). Clinical research of kidney diseases II: problems of study design. Nephrol. Dialysis Transplant. 22 (10), 2785–2794. doi: 10.1093/ndt/gfm433
Rocio, C., Amato, V. S., Camargo, R. A., Tuon, F. F., Nicodemo, A. C. (2014). Liposomal formulation of amphotericin b for the treatment of mucosal leishmaniasis in HIV-negative patients. Trans. R. Soc. Trop. Med. Hygiene 108 (3), 176–178. doi: 10.1093/trstmh/tru011
Roden, M. M., Nelson, L. D., Knudsen, T. A., Jarosinski, P. F., Starling, J. M., Shiflett, S. E., et al. (2003). Triad of acute infusion-related reactions associated with liposomal amphotericin b: analysis of clinical and epidemiological characteristics. Clin. Infect. Dis. 36 (10), 1213–1220. doi: 10.1086/374553
Sampaio, S. A. P., Castro, R. M., Dillon, N. L., Costa Martins, J. E. (1971). Treatment of mucocutaneous (American) leishmaniasis with amphotericin b: report of 70 cases. Int. J. Dermatol. 10 (3), 179–181. doi: 10.1111/j.1365-4362.1971.tb01694.x
Sampaio, S. A., Godoy, J. T., Paiva, L., Dillon, N. L., LACAZ, C. D. S. (1960). The treatment of American (mucocutaneous) leishmaniasis with amphotericin b. Arch. Dermatol. 82 (4), 627–635. doi: 10.1001/archderm.1960.01580040145026
Sampaio, R., Marsden, P. (1997). Treatment of the mucosal form of leishmaniasis without response to glucantime, with liposomal amphotericin b. Rev. da Sociedade Bras. Medicina Trop. 30 (2), 125–128. doi: 10.1590/S0037-86821997000200007
Saúde, S.d.V.e. (2017). Manual for Surveillance of cutaneous leishmaniasis Biblioteca Virtual em Saúde do Ministério da Saúde: Editora MS.
Senchyna, A., Simon, S., Cissé, H., Ginouves, M., Prevot, G., Alcoba, G., et al. (2020). American Cutaneous leishmaniasis in French Guiana: a retrospective comparison between liposomal amphotericin b and meglumine antimoniate. Br. J. Dermatol. 183 (2), 389. doi: 10.1111/bjd.18964
Soares, G. H. C., da Silva, A. B. S., de Sousa Ferreira, L. S., Ithamar, J. S., de Alencar Medeiros, G., Pereira, S. R. F., et al. (2020). Case report: coinfection by leishmania amazonensis and HIV in a Brazilian diffuse cutaneous leishmaniasis patient. Am. J. Trop. Med. Hygiene 103 (3) 1076, 1076–1080. doi: 10.4269/ajtmh.20-0131.
Solomon, M., Pavlotsky, F., Leshem, E., Ephros, M., Trau, H., Schwartz, E. (2011). Liposomal amphotericin b treatment of cutaneous leishmaniasis due to leishmania tropica. J. Eur. Acad. Dermatol. Venereol 25 (8), 973–977. doi: 10.1111/j.1468-3083.2010.03908.x
Solomon, M., Pavlotzky, F., Barzilai, A., Schwartz, E. (2013). Liposomal amphotericin b in comparison to sodium stibogluconate for leishmania braziliensis cutaneous leishmaniasis in travelers. J. Am. Acad. Dermatol. 68 (2), 284–289. doi: 10.1016/j.jaad.2012.06.014
Szebeni, J., Baranyi, L., Savay, S., Bodo, M., Morse, D. S., Basta, M., et al. (2000). Liposome-induced pulmonary hypertension: properties and mechanism of a complement-mediated pseudoallergic reaction. Am. J. Physiol. Heart Circ. Physiol. 279 (3), H1319–H1328. doi: 10.1152/ajpheart.2000.279.3.H1319
Valencia, C., Arévalo, J., Dujardin, J. C., Llanos-Cuentas, A., Chappuis, F., Zimic, M. (2012). Prediction score for antimony treatment failure in patients with ulcerative leishmaniasis lesions. PLoS Negl. Trop. Dis. 6 (6), e1656. doi: 10.1371/journal.pntd.0001656
Vandenbroucke, J. P. (2008). Observational research, randomised trials, and two views of medical science. PLoS Med. 5 (3), e67. doi: 10.1371/journal.pmed.0050067
Wade, R. L., Chaudhari, P., Natoli, J. L., Taylor, R. J., Nathanson, B. H., Horn, D. L. (2013). Nephrotoxicity and other adverse events among inpatients receiving liposomal amphotericin b or amphotericin b lipid complex. Diagn. Microbiol. Infect. Dis. 76 (3), 361–367. doi: 10.1016/j.diagmicrobio.2013.04.001
Walsh, T. J., Finberg, R. W., Arndt, C., Hiemenz, J., Schwartz, C., Bodensteiner, D., et al. (1999). Liposomal amphotericin b for empirical therapy in patients with persistent fever and neutropenia. New Engl. J. Med. 340 (10), 764–771. doi: 10.1056/NEJM199903113401004
Wasan, K. M., Morton, R. E., Rosenblum, M. G., Lopez-Berestein, G. (1994). Decreased toxicity of liposomal amphotericin b due to association of amphotericin b with high-density lipoproteins. J. Pharm. Sci. 83 (7), 1006–1010. doi: 10.1002/jps.2600830716
World Health organization (2021)Leishmaniasis. In: World health organization webpage newsroom (World Health organization). Available at: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis (Accessed 07/02/2021).
Wortmann, G., Zapor, M., Ressner, R., Fraser, S., Hartzell, J., Pierson, J., et al. (2010). Lipsosomal amphotericin b for treatment of cutaneous leishmaniasis. Am. J. Trop. Med. Hygiene 83 (5), 1028–1033. doi: 10.4269/ajtmh.2010.10-0171
Zanger, P., Kötter, I., Raible, A., Gelanew, T., Schönian, G., Kremsner, P. G. (2011). Case report: Successful treatment of cutaneous leishmaniasis caused by leishmania aethiopica with liposomal amphothericin b in an immunocompromised traveler returning from Eritrea. Am. J. Trop. Med. Hygiene 84 (5), 692. doi: 10.4269/ajtmh.2011.10-0712
Keywords: therapy, liposomal amphotericin B (LAB), N-methyl glucamine antimoniate, adverse effect, American cutaneous leishmaniasis (ACL), mucosal leishmaniasis
Citation: Barroso DH, Gonçalves RT, Barbosa JS, Motta JOC, Freire GSM, Gomes CM and Sampaio RNR (2022) Meglumine antimoniate was associated with a higher cure rate than liposomal amphotericin B in the treatment of American tegumentary leishmaniasis: A retrospective cohort study from a Leishmania braziliensis-endemic area. Front. Cell. Infect. Microbiol. 12:993338. doi: 10.3389/fcimb.2022.993338
Received: 13 July 2022; Accepted: 02 September 2022;
Published: 23 September 2022.
Edited by:
Rubem Figueiredo Sadok Menna-Barreto, Oswaldo Cruz Foundation (Fiocruz), BrazilReviewed by:
Iraj Sharifi, Kerman University of Medical Sciences, IranKwame Kumi Asare, University of Cape Coast, Ghana
Copyright © 2022 Barroso, Gonçalves, Barbosa, da Motta, Freire, Gomes and Sampaio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Daniel Holanda Barroso, ZGFuaWVsaGJhcnJvc29AdW5iLmJy