 María Asunción Esteve-Pastor1
María Asunción Esteve-Pastor1 Martín Ruiz-Ortiz2
Martín Ruiz-Ortiz2 Javier Muñiz3
Javier Muñiz3 Inmaculada Roldán-Rabadán4Déborah Otero5Ángel Cequier6Vicente Bertomeu-Martínez7
Inmaculada Roldán-Rabadán4Déborah Otero5Ángel Cequier6Vicente Bertomeu-Martínez7 Lina Badimón8Manuel Anguita2
Lina Badimón8Manuel Anguita2 Gregory Y. H. Lip9,10†
Gregory Y. H. Lip9,10† Francisco Marín1*† on behalf of FANTASIIA investigators
Francisco Marín1*† on behalf of FANTASIIA investigators- 1Department of Cardiology, Hospital Clínico Universitario Virgen de la Arrixaca, CIBERCV, Instituto Murciano de Investigación Biosanitaria (IMIB-Arrixaca), Murcia, Spain
- 2Department of Cardiology, Hospital Universitario Reina Sofía, Córdoba, Spain
- 3Grupo de Investigación Cardiovascular, Departamento de Ciencias de la Salud e Instituto de Investigación Biomédica de A Coruña (INIBIC), CIBERCV, Universidade da Coruña, A Coruña, Spain
- 4Department of Cardiology, Hospital La Paz, Madrid, Spain
- 5ODDS, SL, A Coruña, Spain
- 6Department of Cardiology, Hospital de Bellvitge, CIBERCV, Barcelona, Spain
- 7Department of Cardiology, Hospital Universitario de San Juan, Alicante, Spain
- 8Cardiovascular Research Center (CSIC-ICCC), Hospital de la Santa Creu i Sant Pau, CIBERCV, IIB-Sant Pau, Barcelona, Spain
- 9Liverpool Centre for Cardiovascular Science, University of Liverpool and Liverpool Heart and Chest Hospital, Liverpool, United Kingdom
- 10Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Background: An integrated and holistic approach is increasingly advocated in patients with atrial fibrillation (AF), based on the “Atrial fibrillation Better Care (ABC) pathway: A, Avoid stroke with anticoagulation; B, better symptom management; C, cardiovascular and comorbidity risk management.” The aim of this study was to examine the prevalence of adherence to each component of the ABC pathway and to analyze its impact on long-term prognosis in the “real-world” cohort of AF patients from the FANTASIIA registry.
Methods: This prospective study included consecutive AF outpatients anticoagulated with direct oral anticoagulants (DOAC) or vitamin K antagonists (VKA) from June 2013 to October 2014. From the ABC pathway, adherence to the “A criterion” was defined by a time in the therapeutic range (TTR) ≥ 70% or correct dose with DOAC; “B criterion” adherence was defined by a European Heart Rhythm Association (EHRA) Symptom Scale I-II; and “C criterion” adherence was defined as optimized risk factors and comorbidity management. Baseline features and embolic events, severe bleeding, and all-cause and cardiovascular mortality rates up to 3 years of follow-up were analyzed, and a Cox multivariate analysis was performed to investigate the role of each component of the ABC pathway in predicting major events.
Results: A total of 1,955 AF patients (age: 74.4 ± 9.4 years; 43.2% female patients) were included in this study: adherence to A criterion was observed in 920 (47.1%) patients; adherence to B criterion was observed in 1,791 (91.6%) patients; and adherence to C criterion was observed in 682 (34.8%) patients. Only 394 (20.2%) of the whole population had good control of AF according to the ABC pathway. After a median follow-up of 1,078 days (IQR: 766–1,113), adherence to A criterion was independently associated with reduced cardiovascular mortality [HR: 0.67, 95%CI (0.45–0.99); p = 0.048] compared with non-adherence. Adherence to the B criterion was independently associated with reduced stroke [HR: 0.28, 95%CI (0.14–0.59); p < 0.001], all-cause mortality [HR: 0.49, 95%CI (0.35–0.69); p < 0.001], cardiovascular mortality [HR: 0.39, 95%CI (0.25–0.62); p < 0.001], and major adverse cardiovascular events (MACE) [HR: 0.41, 95%CI (0.28–0.62); p < 0.001] compared with non-adherence. AF patients with C criterion adherence had a significantly lower risk of myocardial infarction [HR: 0.31, 95%CI (0.15–0.66); p < 0.001]. Fully adherent ABC patients had a significant reduction in MACE [HR: 0.64, 95%CI (0.42–0.99); p = 0.042].
Conclusion: In real-world anticoagulated AF patients from FANTASIIA registry, we observed a lack of adherence to integrated care management of AF following the ABC pathway. AF managed according to the ABC pathway was associated with a significant reduction in adverse outcomes during long follow-up, suggesting the benefit of a holistic and integrated approach to AF management.
Introduction
Atrial fibrillation (AF) has emerged as a major public health issue, and more than two-thirds of patients older than 70 years will present with this disease, increasing hospital admissions and direct and indirect healthcare costs (1). The presence of AF increases the risk of stroke, cardiovascular events, and mortality (2).
Both hospitalization and complications related with AF could be preventable with appropriate guideline-adherent care to reduce adverse outcomes in those patients (3). The concept of integrated care was developed by Wagner et al. (4) regarding the effective interventions for patients with chronic diseases highlighting five areas, namely, the use of evidence-based therapies with planned care of interventions, reorganization of health systems, improved patient self-management support, increased access to expertise with multidisciplinary teams, and greater availability of clinical information (3, 4). Such an integrated care approach can be extended to various clinical settings (5, 6). In the case of AF, such an integrated and holistic approach is essential. AF management not only involves oral anticoagulation for stroke prevention but also needs an improvement of AF symptomatology with rate or rhythm control, management of risk factors with targeted treatments, or control of concomitant comorbidities to mitigate treatment burden (7, 8). Indeed, a multidisciplinary holistic approach to manage AF, including behavior changes and close follow-up, is associated with significantly lower cardiovascular outcomes and reduced medical costs (9, 10).
Such an integrated and holistic approach for the management of AF disease can be based on the “Atrial fibrillation Better Care” (ABC) pathway (11). The “A criterion” refers to Avoid stroke, i.e., identifying those patients who are truly at low risk, who do not need oral anticoagulation, and who do not use effective oral anticoagulation. When vitamin K antagonists (VKA) are used, a high time in therapeutic range (TTR) ≥ 70% is necessary for best effectiveness and safety of oral anticoagulation with VKA (12) or a label-adherent correct dose of direct oral anticoagulants (DOACs). The “B criterion” refers to patient-centered symptom-directed decisions on rate or rhythm control; and the “C criterion” refers to control of cardiovascular risk factors and comorbidities, including lifestyle changes (11, 13).
The aim of this study was to examine the prevalence of adherence to each component of the ABC pathway and to analyze its impact on long-term prognosis in the “real-world” cohort of AF patients from the FANTASIIA registry.
Materials and Methods
The study design of the FANTASIIA registry has been described earlier (14). FANTASIIA (Spanish Acronym for “Fibrilación Auricular: influencia del Nivel y Tipo de Anticoagulación Sobre la Incidencia de Ictus y Accidentes hemorrágicos”) registry is an observational, prospective, national, and multicenter study of clinical and demographic characteristics of Spanish AF patients. In brief, the main objective of this study is to assess the incidence of thromboembolic and bleeding events in an unselected population of patients with AF, specifically, the type of oral anticoagulant (VKA or DOACs) and quality of anticoagulation with VKAs. We excluded AF patients with valvular heart disease. When we refer to AF patients throughout the article, we analyzed non-valvular atrial fibrillation patients, but that term is deprecated according to the latest 2020 ESC clinical guidelines (12) because it can be confusing. For that reason, we only write “AF patients.”
Study Population
Between June 2013 and March 2014, all outpatients with a confirmed diagnosis of paroxysmal, persistent, or permanent AF were prospectively enrolled. Patients included in the registry had been receiving OAC (VKA or DOACs) for at least 6 months before enrollment. The study was conducted in 50 outpatient clinics by 80 investigators. To “simulate” true DOAC use during that period in Spain, in each participating center, 1 patient receiving DOACs was included for every 4 patients receiving VKAs (predefined ratio in the protocol, 1:4 for DOACs and VKAs). Each investigator had to include the first 20 consecutive AF patients who met the inclusion and exclusion criteria (first 4 with DOACs and first 16 with VKAs).
Patients with valvular heart disease (rheumatic valve disease, moderate-severe valve disease, prosthesis or valve repair surgery), younger than 18 years old, or with recent hospital admission were excluded. All subjects provided signed informed consent. The study was conducted according to the ethical principles of the Declaration of Helsinki and Good Clinical Practice Guidelines and was approved by the Clinical Research Ethics Committee at Hospital Universitario de San Juan (Spain) with the approval number 12/220 and by the Spanish Agency of Medicine and Health Products as a prospective follow-up post-authorization study with the approval number SEC-ACO-2012-01.
Data Collection
Clinical and demographic data for all AF patients were collected in a detailed medical history. Blood sample was collected at baseline and in each visit, and we collected some variables such as glucose, hemoglobin, creatinine, lipid profile, or HbA1c (hemoglobin A1c). We also collected all drug therapy of the patient at baseline. Coagulation status was determined by the International normalized ratio (INR) values of the 6 months prior to the study entry. The estimated time spent in the therapeutic range (TTR) was assessed by the Rosendaal method. Stroke risk was calculated using the CHADS2 (15) (Congestive heart failure, Hypertension, Age ≥ 75 years, Diabetes mellitus, Stroke or transient ischemic attack [TIA]) and CHA2DS2-VASc scores (16) [Congestive heart failure, Hypertension, Age ≥ 75 years, Diabetes mellitus, Stroke or transient ischemic attack, Vascular disease, Age 65–74 years and Sex category (female)]. Bleeding risk was calculated using the HAS-BLED score (17) [Hypertension (uncontrolled systolic blood pressure > 160 mmHg), Abnormal renal and/or liver function, previous Stroke, Bleeding history or predisposition (anemia), Labile INR (only applies to a VKA user; not applicable for a non-VKA user), Elderly (age ≥ 65 years), and concomitant Drugs (antiplatelet or non-steroidal anti-inflammatory drugs) and/or alcohol excess].
Definitions
Following the latest clinical guidelines and ABC pathway definitions (11), the A, B, and C components for this analysis were defined as follows (Supplementary Figure 1):
• Adherence to the “A component” was defined as “avoid stroke/high quality of oral anticoagulation.” For VKA users, this was fulfilled if TTR ≥ 70%. As all our patients were under oral anticoagulation therapy at enrollment, for DOAC users we use the definition of Pastori et al. (18); this was the use of appropriate label-adherent dose, as defined following the EHRA practical guide (19). For patients receiving dabigatran, criteria for considering reduced dose were: age ≥ 80 years; concomitant use of verapamil; ≥ 2 of the following: age 75–79 years, creatinine clearance (CrCl) 30–50 ml/min, HAS-BLED ≥ 3, amiodarone use, platelet aggregation inhibitors use, or body weight ≤ 60 kg. For patients receiving rivaroxaban, criteria for considering reduced dose were: CrCl 15–49 ml/min; ≥ 2 of the following: age ≥ 75 years, HAS-BLED ≥ 3, amiodarone use, platelet aggregation inhibitors use, or body weight ≤ 60 kg. For patients receiving apixaban, criteria for considering reduced dose were: ≥ 2 of the following: age ≥ 80 years, creatinine ≥ 1.5 mg/dl, or body weight ≤ 60 kg; CrCl 15–29 ml/min; ≥ 2 of the following: age ≥ 75 years, HAS-BLED ≥ 3, amiodarone use, platelet aggregation inhibitors use, or diltiazem use. We had no patients taking edoxaban therapy in our registry.
• Adherence to the “B component” refers to better AF symptom management. We used a validated method, i.e., the modified European Heart Rhythm Association (EHRA) score was used (20). EHRA Class I refers to asymptomatic AF disease; EHRA Class II refers to mild symptoms and normal daily activity not affected; EHRA Class III refers to severe symptoms that modified normal daily activity; and EHRA IV refers to disabling symptoms that result in the discontinuation of normal daily activity. We defined “well-controlled AF symptoms” if patients had EHRA I-II classification.
• Adherence to the “C component” refers to “Cardiovascular risk factor and comorbidity optimization.” We used strict criteria for the management of concomitant diseases according to the international guidelines. We considered the following comorbidities and diseases: hypertension, diabetes mellitus, heart failure (HF), coronary artery disease (CAD), peripheral artery disease (PAD), and stroke/TIA. For hypertension, we consider optimal management if blood pressure is < 140/90 mmHg. Optimal management of diabetes was defined as HbA1c ≤ 7.5%. If HBA1C values were not available, we consider well-controlled diabetic patients if fasting glucose levels were ≤ 126 mg/dl. For patients with HF, we consider as optimal management of the disease if treated with beta-blockers or diuretics or ACEI/ARBs (angiotensin-converting enzyme inhibitors/angiotensin receptor blockers). Optimal management of HF patients were consiedered if the patients were treated with two of those drugs. For patients with CAD, PAD, or stroke/TIA, we considered as well-managed of those entities if LDL ≤ 70 mg/dl [as per previous ESC guidelines (21)] and if the patients were treated with statins and with ACEI/ARBs.
Following each component individually, we defined the “ABC pathway adherent group” if all components were fulfilled. If not, the AF disease was considered as non-optimally managed according to the ABC criteria (non-ABC group).
Clinical Outcomes
After 3 years of follow-up, we analyzed adverse clinical outcomes according to each ABC criterion fulfilled and the “ABC pathway adherent group.” Thromboembolic events were defined as stroke or transient ischemic attack or peripheral embolism. Bleeding events were assessed according to the 2005 International Society of Thrombosis and Hemostasis criteria (20): fatal bleeding or symptomatic bleeding in a critical anatomical site (intracranial, intraspinal, intraocular, retroperitoneal, intraarticular, pericardial or intramuscular with compartment syndrome) and/or bleeding causing a fall in Hb ≥ 20 g/L, or transfusion of ≥ 2 units of packed red blood cells. We also collected all-cause mortality, and cardiovascular mortality was defined if it was secondary to a cardiovascular event (acute coronary syndrome, heart failure, lethal arrhythmia or sudden death, artery aneurysm rupture or stroke). MACE (major adverse cardiovascular events) was defined as the composite of ischemic stroke, myocardial infarction, and cardiovascular mortality. Cardiovascular events included fatal and non-fatal stroke, TIA, myocardial infarction, coronary revascularization, and cardiovascular mortality. Clinically significant events included the composite of stroke, major bleeding, all-cause mortality, acute coronary syndrome, and acute heart failure. An external event assignment committee evaluated all adverse events.
Statistical Analysis
Normal distribution of continuous variables was tested with the Kolmogorov-Smirnov method. Continuous variables are presented using the mean ± standard deviation or median [interquartile range]. Categorical variables are expressed as percentages. For between-group comparisons, we used the Student’s t-test for continuous variables and chi-square test for qualitative variables. Cox regression analyses were used to determine the associations between adverse events and each component fulfilled individually (“A” criterion, “B” criterion, and “C” criterion) and for “ABC pathway adherent group.” The independent effect of clinical variables on adverse clinical outcomes was calculated using a Cox proportional hazards regression, including in the multivariate model only those values with p < 0.15 on univariate analysis. The models included the ABC components, age, sex, hypertension, diabetes, dyslipidemia, coronary artery disease, heart failure, peripheral artery disease, stroke/TIA, chronic kidney disease, and Charlson Comorbidity Index. Differences in event-free survival were examined with log-rank test, and Kaplan–Meier curves were drafted accordingly. Statistical significance was defined as p < 0.05. Statistical analyses were performed with Stata version 12 (Stata Corporation, College Station, TX, United States).
Results
We enrolled 2,178 patients in FANTASIIA registry; 1,648 (75.6%) patients were treated with VKA and 530 (24.3%) patients were treated with DOACs, of which 267 (50.4% of DOAC group) patients were treated with dabigatran, 190 (35.8%) patients were treated with rivaroxaban, and 73 (13.8%) patients were treated with apixaban. A total of 1,956 patients (89% of the sample) completed full follow-up. Finally, we had available data from 1,955 patients (74.4 ± 9.4 years; 43.2% female patients) for all components of the ABC pathway for this analysis.
Atrial Fibrillation Better Care Components and Atrial Fibrillation Better Care Pathway Adherence
Of the whole cohort, 920 (47.1%) patients achieved good control of oral anticoagulation (A criterion fulfilled); 1,791 (91.6%) patients had good control of arrhythmia symptomatology (B criterion fulfilled); and 682 (34.8%) patients had good control of cardiovascular risk factors and comorbidities (C criterion fulfilled). Only 394 (20.2%) patients had good compliance and were in the “ABC pathway adherent” group.
In comparison with the ABC adherent group, patients with AF non-ABC adherent had high prevalence of cardiovascular risk factors such hypertension (83.9% vs. 66.8%; p < 0.001), diabetes mellitus (32.6% vs. 16.5%; p < 0.001), or chronic kidney disease (20.2% vs. 15.7%; p = 0.046). Patients with AF non-adherent to ABC pathway also had a high prevalence of heart disease (50.8% vs. 36.8%; p < 0.001), coronary artery disease (21.3% vs. 6.1%; p < 0.001), and high CHA2DS2-VASc (3.9 ± 1.6 vs. 2.9 ± 1.4; p < 0.001) and HAS-BLED scores (2.1 ± 1.1 vs. 1.6 ± 0.9; p < 0.001). No differences between sex, age and type of AF were observed (Table 1).
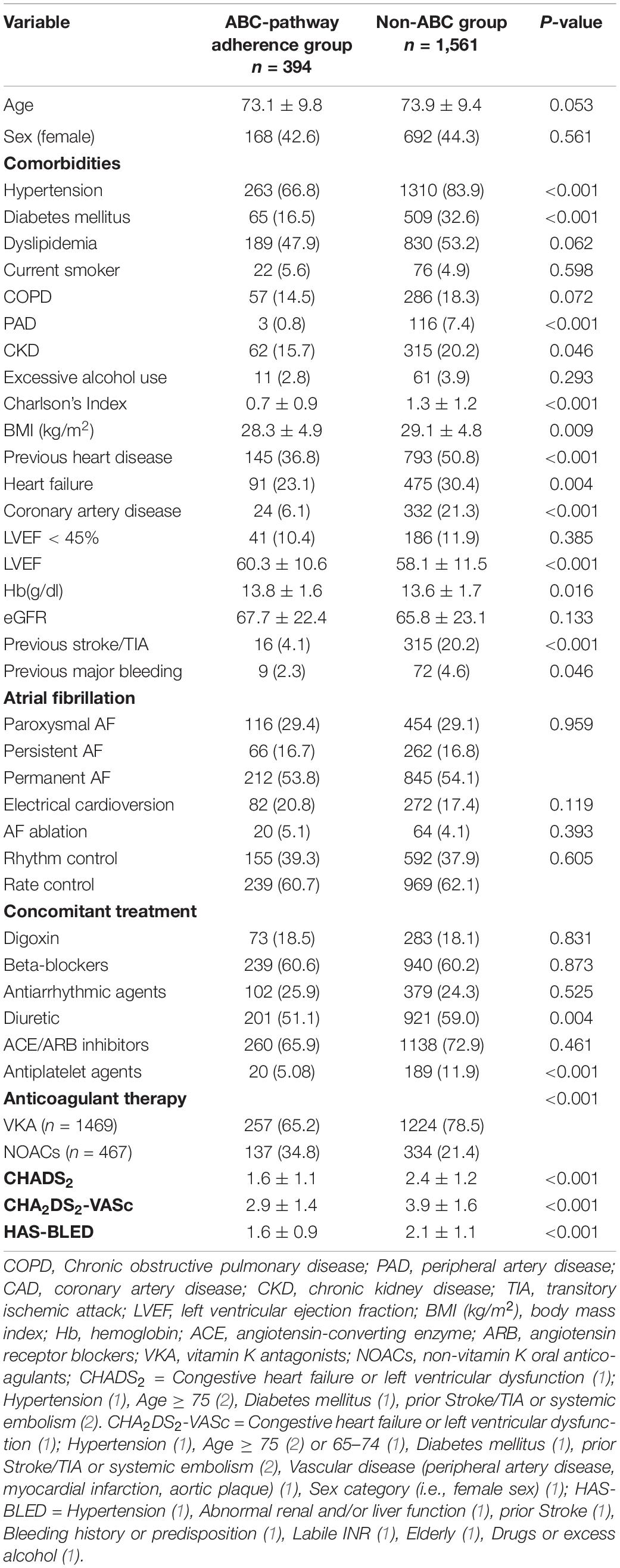
Table 1. Baseline characteristics of patients according to the Atrial fibrillation Better Care (ABC) pathway adherence.
Clinical Outcomes
After a median follow-up of 1,078 days (IQR: 766–1,113), we analyzed all the adverse events in the “ABC pathway adherent group” and to the adherence of each criterion. There was a total of 255 deaths (107 of them were related with cardiovascular causes), 45 strokes, and 136 major bleedings.
“A” Criterion
We observed patients with non-adherence to the “A” criterion had a higher rate of all-cause mortality (5.69%/year vs. 4.44%/year; p = 0.043), cardiovascular mortality (2.65%/year vs. 1.57%/year; p = 0.008), and cardiovascular events (3.63%/year vs. 2.73%/year) compared with adherent patients (see Table 2). Patients with AF non-adherence to the component A had a high risk of all-cause mortality (log-rank p-value = 0.057) and cardiovascular mortality (log-rank p-value = 0.008) (Figure 1).
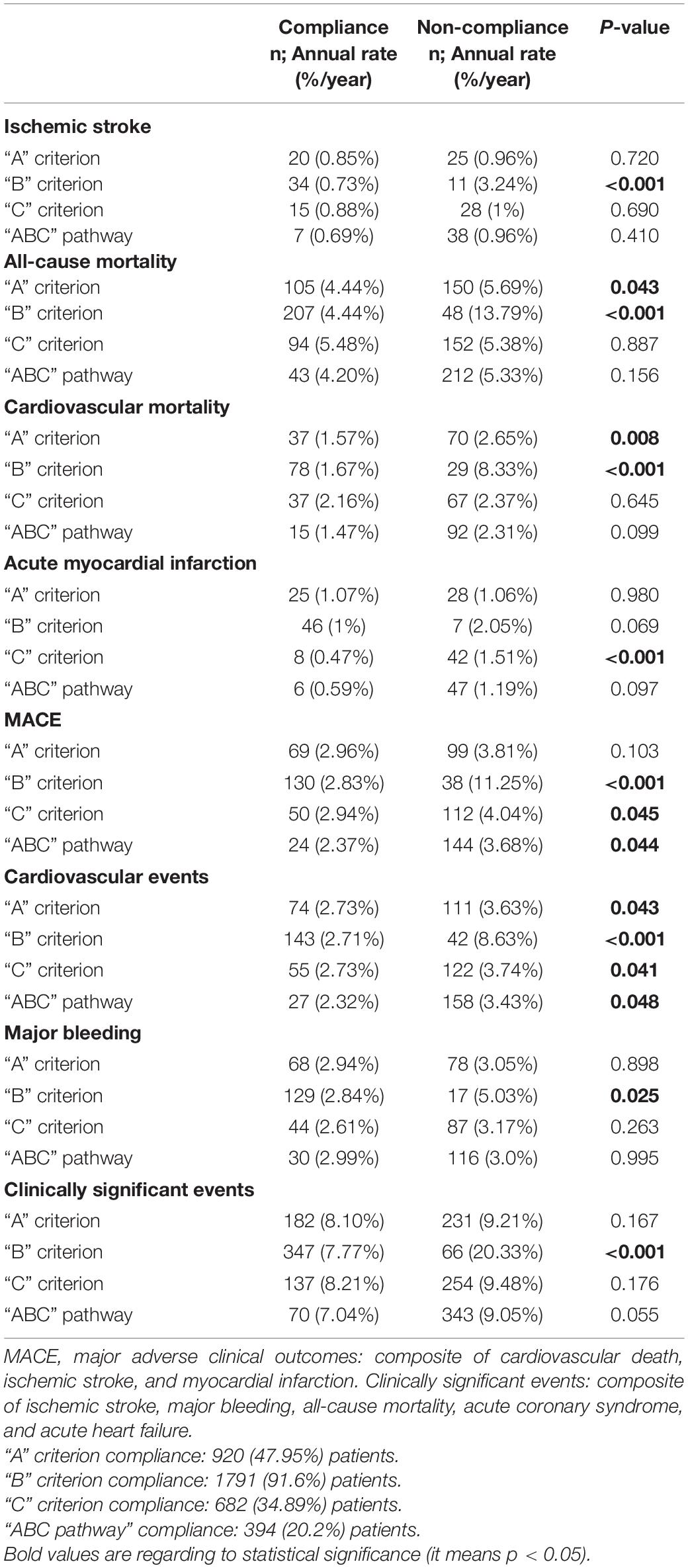
Table 2. Distribution of adverse events and annual rates according to the compliance with each criterion and with ABC pathway.
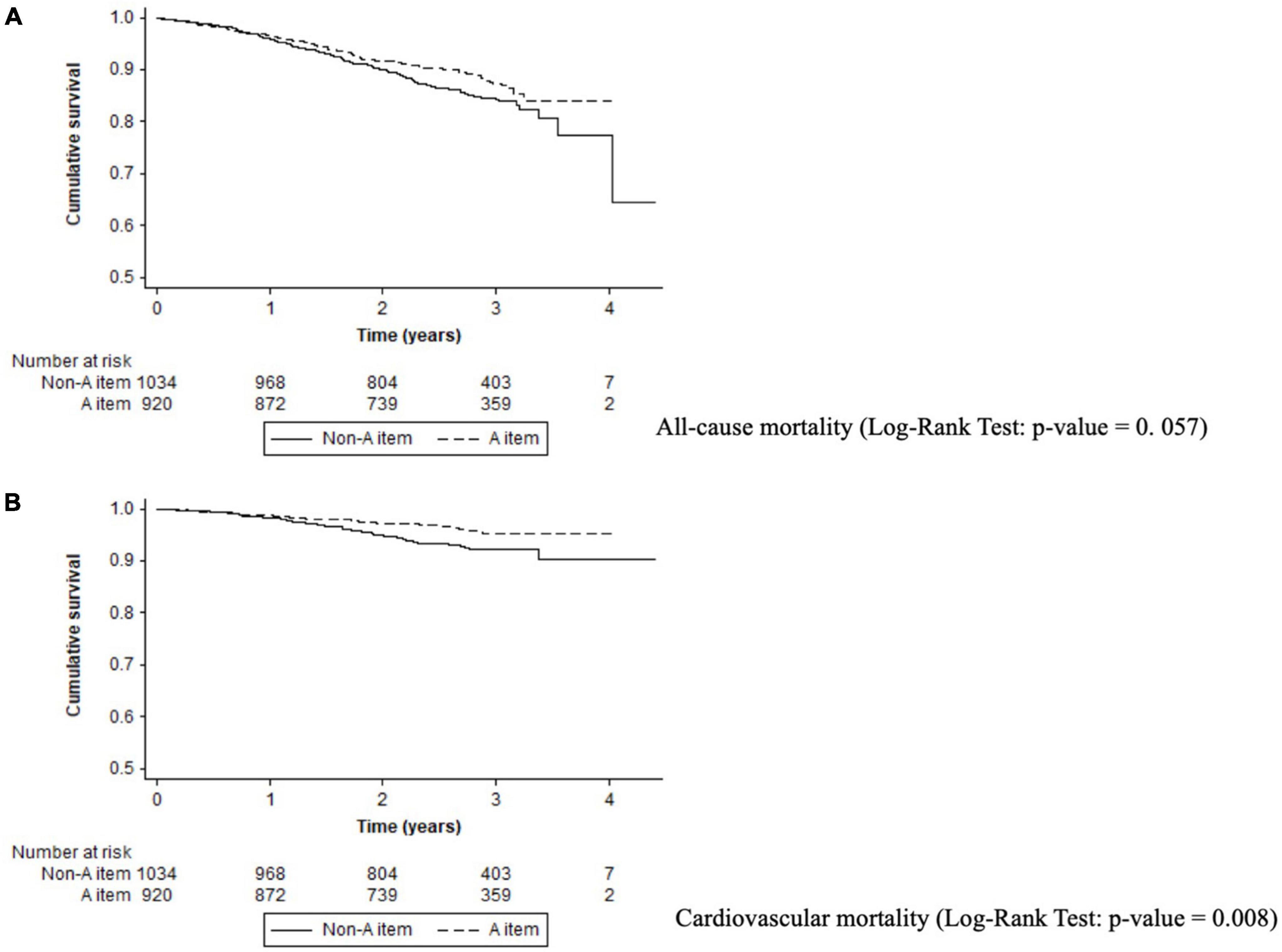
Figure 1. Kaplan–Meier curves for adverse events in A criterion. (A) All-cause mortality (log-rank test: p-value = 0.057). (B) Cardiovascular mortality (log-rank test: p-value = 0.008).
On multivariable regression analysis, “A” criterion adherence was independently related with reduced cardiovascular mortality [HR: 0.67, 95%CI (0.45–0.99); p = 0.048] in comparison with non-adherence (see Table 3 and Supplementary Table 1).
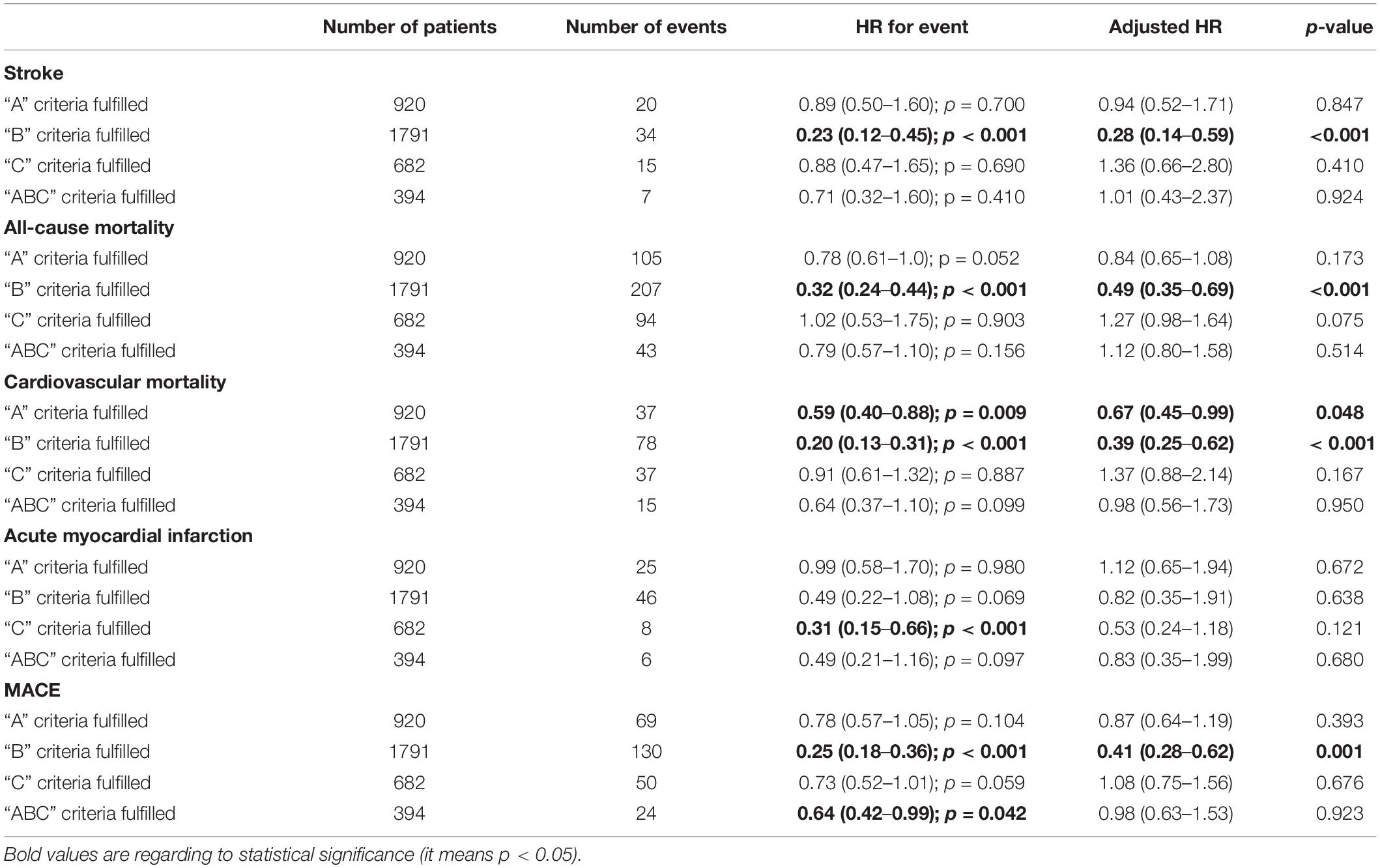
Table 3. Unadjusted and adjusted hazard ratios for adverse outcomes according to the criteria fulfilled from atrial fibrillation better care (ABC pathway adherent criteria) compared with non-optimally managed ABC group.
“B” Criterion
Poor control of AF symptoms (non-adherence to B component) had higher rate of adverse events: all-cause mortality (13.79%/year vs. 4.44%/year; p < 0.001), cardiovascular mortality (8.33%/year vs. 1.67%/year; p < 0.001), MACE (11.25%/year vs. 2.83%/year; p < 0.001), stroke (3.24%/year vs. 0.73%/year; p < 0.001), or major bleeding (5.03%/year vs. 2.84%/year; p = 0.025) compared with patients with well-controlled AF disease, see Table 2. Patients with poor control according to the “B” criterion had high risk of stroke (log-rank p-value < 0.001), all-cause mortality (log-rank p-value < 0.001), cardiovascular mortality (log-rank p-value < 0.001), MACE (log-rank p-value < 0.001), or major bleeding (log-rank p-value = 0.020) (Figure 2).
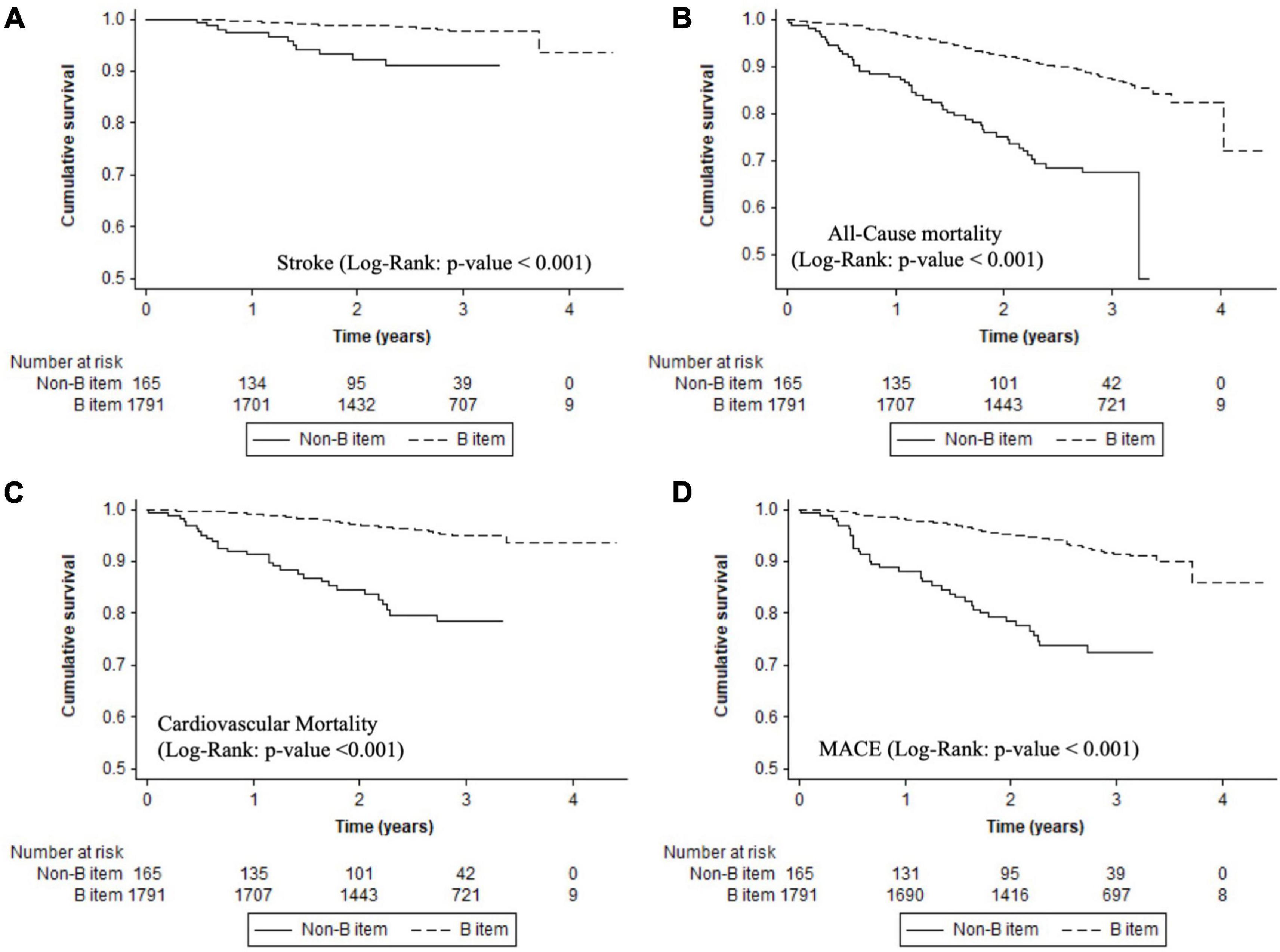
Figure 2. Kaplan–Meier curves for adverse events in B component. (A) Stroke (log-rank: p-value < 0.001). (B) All-cause mortality (log-rank: p-value < 0.001). (C) Cardiovascular mortality (log-rank: p-value < 0.001). (D) MACE (log-rank: p-value < 0.001).
On multivariable regression analysis, “B” criterion adherence was independently related with lower stroke [HR: 0.28, 95%CI
(0.14–0.59); p < 0.001], all-cause mortality [HR: 0.49, 95%CI (0.35–0.69); p < 0.001], cardiovascular mortality [HR: 0.39, 95%CI (0.25–0.62); p < 0.001], and MACE [HR: 0.41, 95%CI (0.28–0.62); p < 0.001] in comparison with non-adherence (see Table 3 and Supplementary Tables 2–5).
“C” Criterion
Non-adherence to the C-criterion had a high rate of acute myocardial infarction (1.51%/year vs. 0.47%/year; p < 0.001), cardiovascular events (3.74%/year vs. 2.73%/year; p = 0.041), or MACE (4.04%/year vs. 2.94%/year; p = 0.045) compared with adherent patients (Table 2).
Kaplan–Meier curves show that non-adherence to C-criterion had a high risk of myocardial infarction (log-rank p-value < 0.001) and a trend for MACE (log-rank p-value = 0.059). Patients with good control of comorbidities had a significantly lower risk of myocardial infarction [HR: 0.31, 95%CI (0.15–0.66); p < 0.001)] (Figure 3). On the multivariable regression analysis, there was no independent association of good adherence to C criterion and adverse events (see Supplementary Table 6).
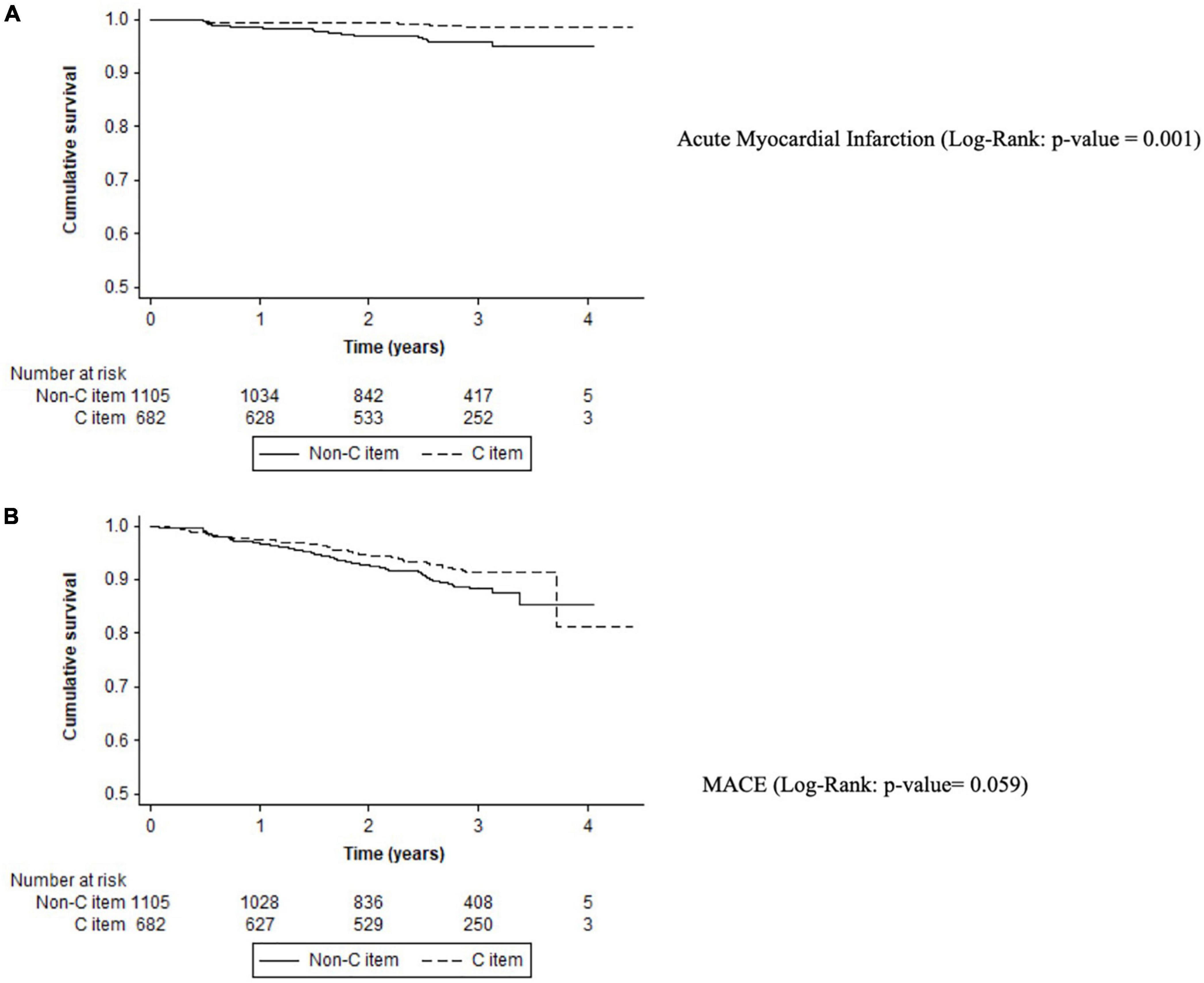
Figure 3. Kaplan–Meier curves for adverse events in C criterion. (A) Acute myocardial infarction (log-rank: p-value = 0.001). (B) MACE (log-rank: p-value = 0.059).
Full “Atrial Fibrillation Better Care Pathway Adherence”
Only 394 (20.2%) patients had full adherence to all the ABC components. Patients of the non-ABC group had a higher rate of MACE (3.68%/year vs. 2.37%/year; p = 0.044) and cardiovascular events (3.43%/year vs. 2.32%/year; p = 0.048) compared with ABC pathway adherent patients. Adherent ABC patients had a significant reduction in MACE [HR: 0.64, 95%CI (0.42–0.99); p = 0.042). All adverse events according to the ABC pathway are shown in Table 2. On Kaplan–Meier analysis, patients non-adherent to the ABC pathway had a high risk of MACE (log-rank p-value = 0.042) (Figure 4). On the multivariable regression analysis, there was no statistically significant independent association with adverse events (see Table 3).
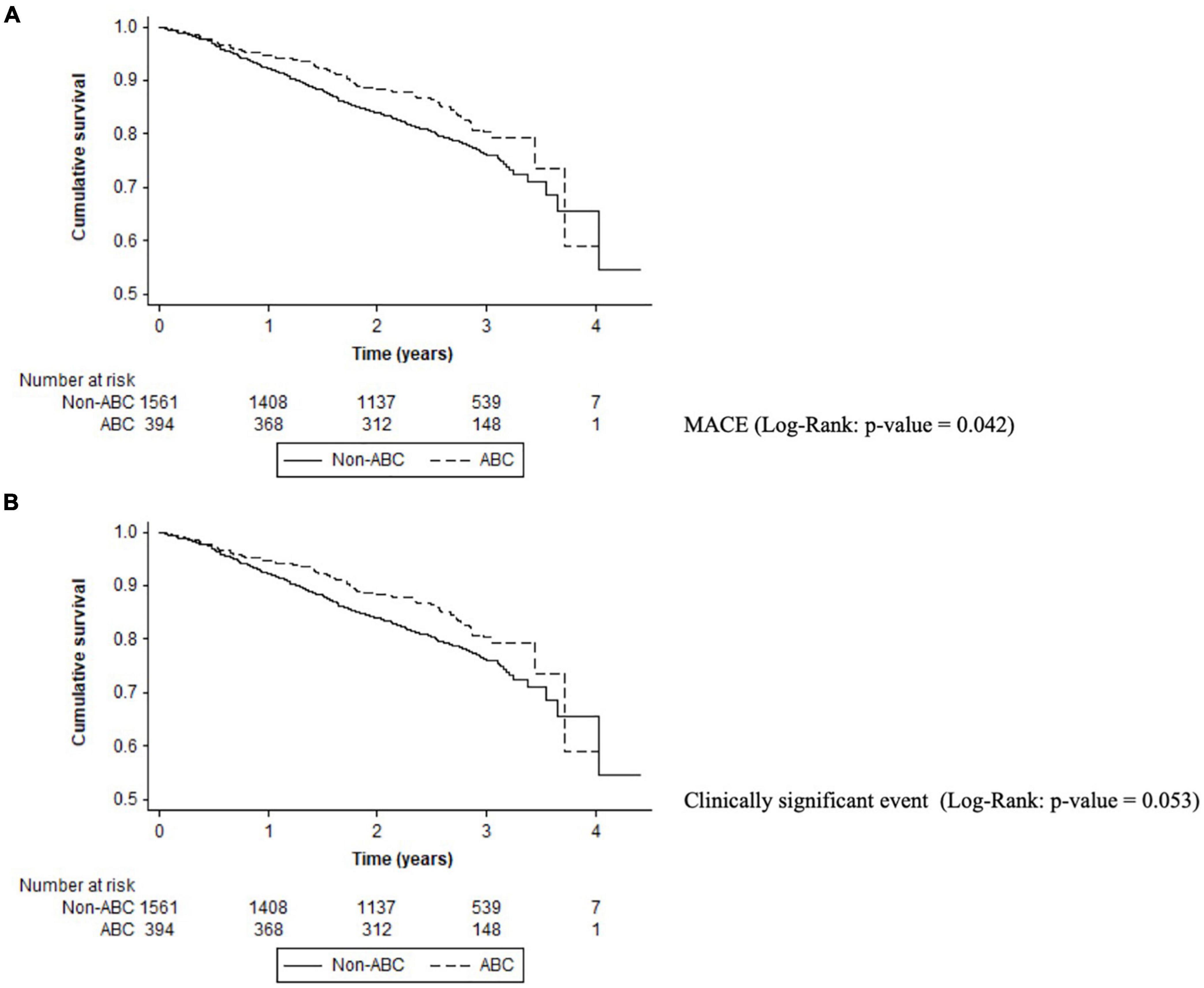
Figure 4. Kaplan–Meier curves for adverse events in the ABC pathway adherent group. (A) MACE (log-rank: p-value = 0.042). (B) Clinically significant event (log-rank: p-value = 0.053).
Discussion
In real-world anticoagulated AF patients from FANTASIIA registry, we observed a lack of adherence to integrated care management of AF following ABC pathway. The integrated ABC pathway adherent care is associated with a significant reduction in major cardiovascular events during long follow-up, although notable baseline differences between patients with and without ABC-adherent care are present. Control of symptomatology of AF, as assessed by EHRA functional class (B criterion), was associated with the most significant adverse event reductions.
Only 20.2% of the cohort were adherent to the ABC pathway, highlighting the low adherence to integrated care management. These data were consistent with observations from a recent systematic review by Romiti et al. (9) and the study by Pastori et al. (22) in the ATHERO-AF study where only 22.4% of patients were well managed according to the ABC pathway.
According to the “avoid stroke” (i.e., “A” criterion) with adequate oral anticoagulation, only 47% of patients were adherent. To reduce stroke, mortality, and adverse events in AF patients, good anticoagulation with high TTR with VKA or correct dose with DOAC is essential (23, 24). The VKAs have been shown to be highly effective for stroke prevention in AF, reducing the risk of stroke by 64% and all-cause death by 26% compared with control/placebo (25), but the effectiveness of VKA is dependent on the quality of anticoagulation control. Good quality anticoagulation (defined as TTR > 70%) is related with better outcomes during follow-up (26–28). In case of DOACs, those drugs have demonstrated similar or higher efficacy in thromboembolic prevention in AF patients with fixed dose and in the absence of drug monitoring (29–32). However, nearly one-third of patients may receive an inappropriate dose of DOAC in daily clinical practice, according to EHRA recommendations (33), increasing both thromboembolic and bleeding risks (34). Hence, management tools (classical education, smart technology, pill counts…) to improve oral anticoagulation adherence in AF patients involve patients, relatives, and health professionals (physicians, nursery, pharmacist…) (35). Education and counseling to explain the risks of non-adherence are needed to ensure optimal uptake in AF patients with both therapies, improving patient adherence and persistence with treatment (13, 36, 37).
In daily clinical practice, physicians often focus on oral anticoagulation or adverse events or observable risk factors but tend to forget the patient’s perspective, quality of life, and symptomatology related with AF (38). Different studies have analyzed the influence of AF symptoms on quality of life, with assessment tools to quantify the burden of this disease (39). However, the relationship between symptoms and adverse events is not widely analyzed in real-world patients.
In our study, we observed good control of AF symptoms with almost 90% of the sample in EHRA I-II status, and we showed the novel finding that the lack of control of symptoms (B criterion) was the strongest component of the ABC pathway related with adverse events. Such good control of AF symptoms was independently related with a significant reduction in stroke, all-cause mortality, cardiovascular mortality, and MACE. These results were slightly different from the results of ORBIT-AF registry (40) where there was lower quality of life and higher rates of hospitalization in symptomatic patients (EHRA > 2) but with no difference in mortality rates.
We also analyzed the influence of risk factors and comorbidities in AF patients according to an integrated care approach. Risk factor modification, healthy lifestyle, and interventions targeting underlying conditions have shown a reduction in AF burden and recurrence but with a multifaceted approach (12). This “C” criterion definition differs in previous studies, but in the FANTASIIA population, we have selected strict criteria as target control of comorbidities and risk factors according to the current clinical guidelines (Supplementary Figure 1). Hence, only 34.8% of AF patients had risk factors and comorbidities under control. Compared with ESC-EHRA EORP Atrial Fibrillation General Long-Term (AFGen LT) Registry population non-ABC adherent subgroup (41), our patients from FANTASIIA registry were more elderly, with a higher prevalence of cardiovascular or other concomitant diseases, highlighting the high-risk profile of our real-world AF patients. Non-adherence to C criterion had a higher risk, especially for cardiovascular outcomes (MACE, cardiovascular events, and acute myocardial infarction), compared with adherent patients. LaMori et al. (42) analyzed the comorbidity burden of AF patients and observed that almost all (98%) of the population had at least one additional comorbidity, 90% had cardiovascular comorbidities, and ≥ 63% of AF patients had four or more comorbidities in addition to AF, so the high multimorbidity disease burden carried beyond AF status. Indeed, Fauchier et al. (2) analyzed the causes of death in AF patients and only 7% were related with stroke accounting for the majority of deaths related with a cardiovascular cause(s).
In the FANTASIIA registry, only 20% of the AF population were ABC pathway adherent, highlighting the lack of adherence to holistic management of AF patients, despite the potential benefits from adherence to the ABC pathway (9). Stevens et al. (43) recently reviewed 12 clinical studies that focused on the ABC pathway and observed a wide range in the proportion of participants assessed as ABC pathway adherent in the included studies (7.0–43.8%) and near 37% in ATHERO-AF registry (18). In FANTASIIA registry, there was a reduction in MACE/composite outcome in those ABC adherent patients (by 36%) with similar results compared with ATHERO-AF cohort (18) or post-hoc AFFIRM trial analysis (44). The recent ESC-EHRA EORP AFGen Long Term registry (41) observed that ABC pathway adherence was associated with a significant lower risk for cardiovascular events, CV death, and all-cause death. Also, in our registry, we observed that the ABC pathway adherent patients had less cardiovascular events, MACE, and clinically significant events (that includes mortality) but no difference in all-cause mortality rates probably related to the small sample sizes of the subgroups.
Compliance with AF management plans, including advice on risk factors and lifestyle changes, simplifying assistance process and prescriptions, better patient education, nurse-led interventions, and close health support, may have a major impact on the burden of AF, improving decision-making, quality of life, and outcomes in AF patients (11, 45). Our study is one of the few based on a prospective cohort and provides more evidence for the use of ABC pathway as the integrated management of AF patients (both under VKA and DOAC), also highlighting the importance of the symptom management. Involving patients, relatives, and multidisciplinary health professionals in the decision-making process is crucial to facilitate truly integrated or holistic management of AF.
Strengths and Limitations
The limitations of the study are derived from its observational nature, as inclusion bias could not be completely eliminated, although it was minimized by the criterion of consecutive enrollment. However, differences in baseline risk factors characteristics were observed. Unfortunately, we cannot perform a direct comparison using propensity score matching to homogenize the baseline characteristics due to the sample size, so this should be considered a limitation of our study.
Other limitation was related to our use of the robust definition for ABC adherence leading to modest sample sizes of each subgroup with low adverse events and lack of statistical significance for comparison of outcomes, hence limiting the generalizability of the results. Although we have a large follow-up of AF patients, the ABC pathway compliance was calculated at baseline, and the variation of different components of the ABC pathway during the follow-up and the influence on outcomes are uncertain. Moreover, related with the predefined ratio in the protocol, 1:4 for DOACs and VKAs, we could not perform individual analysis to validate ABC pathway for DOAC vs. VKA or for each DOAC due to the small sample size, which is a limitation in the generalizability of the results in the DOAC group.
Regarding the difference between adherence to “A criterion” according to VKA or DOAC therapy, for VKA therapy the definition of good adherence according to TTR 70% is fully accepted in the original definition. However, regarding DOAC definition, there was no uniform approach in previous manuscripts. The most correct definition perhaps will be the assessment of taking DOAC therapy with pharmacy dispensing data from electronic health records, pill count, or laboratory control of DOACs. No studies have previously validated ABC pathway in this way in the DOAC group. However, FANTASIIA registry involves 50 centers in Spain, with different electronic and non-electronic pharmacy dispensing data, and it is not indicated as the laboratory control of DOAC to assess compliance. For that reason, we considered the correct dose of DOAC as an indirect indicator of correct adherence to A criteria, which is a small limitation in the DOAC group of ABC- pathway.
Otherwise, there are several strengths in the FANTASIIA registry, which is a cohort study with prospective long follow-up including a large number of patients with few losses to follow-up, and ≥90% of patients had follow-up data.
Conclusion
In real-world anticoagulated AF patients from FANTASIIA registry, we observed a lack of adherence to integrated care management of AF following the ABC pathway. AF managed according to the ABC pathway was associated with a significant reduction in adverse outcomes during long follow-up, suggesting the benefit of a holistic and integrated approach to AF management.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Clinical Research Ethics Committee at Hospital Universitario de San Juan (Spain) with the approval number 12/220 and by the Spanish Agency of Medicine and Health Products as a prospective follow-up post-authorization study with the approval number SEC-ACO-2012-01. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
ME-P and FM drafted the manuscript and writing–review and editing-lead. JM and DO performed the statistical analysis. MA, VB-M, and FM performed as conceptualization-lead, methodology-lead, and writing-review and editing-lead. GL performed the writing–review and editing-supporting. All authors made substantial contributions to the concept and design of the work, participated in the acquisition and interpretation of data, revised the manuscript for important intellectual content, approved the final version of the manuscript, and are able to take public responsibility for the full text of the article.
Funding
This study received funding from an unconditional grant from Pfizer/Bristol-Myers Squibb and grants from the Instituto de Salud Carlos III (Madrid)-FEDER (RD16/11/00420, RD12/0042/0068, RD12/0042/0010, RD12/0042/0069, and RD12/0042/0063). The authors are supported by RD12/0042/0049 (RETICS) from ISCIII, PI13/00513/FEDER from ISCIII, Fundación Séneca (19245/PI/14), and Instituto Murciano de Investigación Biosanitaria (IMIB16/AP/01/06).
Conflict of Interest
DO is employed by ODDS, SL.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.856222/full#supplementary-material
References
1. Burdett P, Lip GYH. Atrial fibrillation in the United Kingdom: predicting costs of an emerging epidemic recognising and forecasting the cost drivers of atrial fibrillation-related costs. Eur Heart J Qual Care Clin Outcomes. (2020) 8:187–94. doi: 10.1093/ehjqcco/qcaa093
2. Fauchier L, Villejoubert O, Clementy N, Bernard A, Pierre B, Angoulvant D, et al. Causes of death and influencing factors in patients with atrial fibrillation. Am J Med. (2016) 129:1278–87. doi: 10.1016/j.amjmed.2016.06.045
3. Gallagher C, Elliott AD, Wong CX, Rangnekar G, Middeldorp ME, Mahajan R, et al. Integrated care in atrial fibrillation: a systematic review and meta-analysis. Heart Br Card Soc. (2017) 103:1947–53. doi: 10.1136/heartjnl-2016-310952
4. Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. (1996) 74:511–44. doi: 10.2307/3350391
5. Lip GY, Ntaios G. Integrated Care for Stroke Management: Easy as ABC. Thromb Haemost. (2021) 122:316–9. doi: 10.1055/a-1632-1777
6. Field M, Kuduvalli M, Torella F, McKay V, Khalatbari A, Lip GYH. Integrated care systems and the aortovascular hub. Thromb Haemost. (2021) 122:177–80. doi: 10.1055/a-1591-8033
7. Dobler CC, Harb N, Maguire CA, Armour CL, Coleman C, Murad MH. Treatment burden should be included in clinical practice guidelines. BMJ. (2018) 363:k4065. doi: 10.1136/bmj.k4065
8. Potpara TS, Mihajlovic M, Zec N, Marinkovic M, Kovacevic V, Simic J, et al. Self-reported treatment burden in patients with atrial fibrillation: quantification, major determinants, and implications for integrated holistic management of the arrhythmia. Europace. (2020) 22:1788–97. doi: 10.1093/europace/euaa210
9. Romiti GF, Pastori D, Rivera-Caravaca JM, Ding WY, Gue YX, Menichelli D, et al. Adherence to the “atrial fibrillation better care” pathway in patients with atrial fibrillation: impact on clinical outcomes-a systematic review and meta-analysis of 285,000 patients. Thromb Haemost. (2021) 122:406–14. doi: 10.1055/a-1515-9630
10. Yoon M, Yang P-S, Jang E, Yu HT, Kim T-H, Uhm J-S, et al. Improved population-based clinical outcomes of patients with atrial fibrillation by compliance with the simple ABC (atrial fibrillation better care) pathway for integrated care management: a nationwide cohort study. Thromb Haemost. (2019) 119:1695–703. doi: 10.1055/s-0039-1693516
11. Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol. (2017) 14:627–8. doi: 10.1038/nrcardio.2017.153
12. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42:373–498.
13. Lip GYH, Lane DA, Potpara TS. Innovative strategies to improve adherence to non-Vitamin K antagonist oral anticoagulants for stroke prevention in atrial fibrillation. Eur Heart J. (2018) 39:1404–6. doi: 10.1093/eurheartj/ehx807
14. Bertomeu-González V, Anguita M, Moreno-Arribas J, Cequier Á, Muñiz J, Castillo-Castillo J, et al. Quality of anticoagulation with vitamin K antagonists. Clin Cardiol. (2015) 38:357–64. doi: 10.1002/clc.22397
15. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the national registry of atrial fibrillation. JAMA. (2001) 285:2864–70. doi: 10.1001/jama.285.22.2864
16. Lip GYH, Nieuwlaat R, Pisters R, Lane DA, Crijns HJGM. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. (2010) 137:263–72. doi: 10.1378/chest.09-1584
17. Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJGM, Lip GYH. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro heart survey. Chest. (2010) 138:1093–100. doi: 10.1378/chest.10-0134
18. Pastori D, Menichelli D, Violi F, Pignatelli P, Lip YH. The atrial fibrillation better Care (ABC) pathway and cardiac complications in atrial fibrillation: a potential sex-based difference. The ATHERO-AF study. Eur J Intern Med. (2021) 85:80–5. doi: 10.1016/j.ejim.2020.12.011
19. Steffel J, Collins R, Antz M, Cornu P, Desteghe L, Haeusler KG, et al. 2021 European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Europace. (2021) 23:1612–76.
20. Camm AJ, Lip GYH, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC GUIDELINES for the management of atrial fibrillation–developed with the special contribution of the European heart rhythm association. Eur Heart J. (2012) 14:1385–413.
21. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
22. Pastori D, Pignatelli P, Menichelli D, Violi F, Lip GYH. Integrated care management of patients with atrial fibrillation and risk of cardiovascular events: the ABC (atrial fibrillation better care) pathway in the ATHERO-AF study cohort. Mayo Clin Proc. (2019) 94:1261–7. doi: 10.1016/j.mayocp.2018.10.022
23. Hwang J, Han S, Bae H-J, Jun S-W, Choi S-W, Lee C-H, et al. NOAC adherence of patients with atrial fibrillation in the real world: dosing frequency matters? Thromb Haemost. (2020) 120:306–13. doi: 10.1055/s-0039-1697954
24. Sølvik UØ, Løkkebø E, Kristoffersen AH, Brodin E, Averina M, Sandberg S. Quality of warfarin therapy and quality of life are improved by self-management for two years. Thromb Haemost. (2019) 119:1632–41. doi: 10.1055/s-0039-1693703
25. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. (2007) 146:857–67. doi: 10.7326/0003-4819-146-12-200706190-00007
26. Esteve-Pastor MA, Rivera-Caravaca JM, Roldán-Rabadán I, Roldán V, Muñiz J, Raña-Míguez P, et al. Quality of oral anticoagulation with vitamin K antagonists in “real-world” patients with atrial fibrillation: a report from the prospective multicentre FANTASIIA registry. Europace. (2017) 20:1435–41. doi: 10.1093/europace/eux314
27. Prochaska JH, Hausner C, Nagler M, Göbel S, Eggebrecht L, Panova-Noeva M, et al. Subtherapeutic anticoagulation control under treatment with Vitamin K-antagonists-data from a specialized coagulation service. Thromb Haemost. (2019) 119:1347–57. doi: 10.1055/s-0039-1692175
28. Martín-Pérez M, Gaist D, de Abajo FJ, García Rodríguez LA. Predictors of over-anticoagulation in warfarin users in the UK general population: a nested case-control study in a primary health care database. Thromb Haemost. (2019) 119:66–76. doi: 10.1055/s-0038-1676519
29. Harenberg J, Beyer-Westendorf J, Crowther M, Douxfils J, Elalamy I, Verhamme P, et al. Accuracy of a rapid diagnostic test for the presence of direct oral factor Xa or thrombin inhibitors in urine-A multicenter trial. Thromb Haemost. (2020) 120:132–40. doi: 10.1055/s-0039-1700545
30. Douxfils J, Adcock DM, Bates SM, Favaloro EJ, Gouin-Thibault I, Guillermo C, et al. 2021 update of the international council for standardization in haematology recommendations for laboratory measurement of direct oral anticoagulants. Thromb Haemost. (2021) 121:1008–20. doi: 10.1055/a-1450-8178
31. Nelson AJ, Johnston BW, Waite AAC, Lemma G, Welters ID. A systematic review of anticoagulation strategies for patients with atrial fibrillation in critical care. Thromb Haemost. (2021) 121:1599–609. doi: 10.1055/a-1477-3760
32. Maji D, Opneja A, Suster MA, Bane KL, Wilson BM, Mohseni P, et al. Monitoring DOACs with a novel dielectric microsensor: a clinical study. Thromb Haemost. (2021) 121:58–69. doi: 10.1055/s-0040-1715589
33. Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, et al. The 2018 European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: executive summary. Eur Heart J. (2018) 39:1330–93.
34. Ruiz Ortiz M, Muñiz J, Raña Míguez P, Roldán I, Marín F, Asunción Esteve-Pastor M, et al. Inappropriate doses of direct oral anticoagulants in real-world clinical practice: prevalence and associated factors. A subanalysis of the FANTASIIA Registry. Europace. (2018) 20:1577–83. doi: 10.1093/europace/eux316
35. Pritchett RV, Bem D, Turner GM, Thomas GN, Clarke JL, Fellows R, et al. Improving the prescription of oral anticoagulants in atrial fibrillation: a systematic review. Thromb Haemost. (2019) 119:294–307. doi: 10.1055/s-0038-1676835
36. Clarkesmith DE, Pattison HM, Lip GYH, Lane DA. Educational intervention improves anticoagulation control in atrial fibrillation patients: the TREAT randomised trial. PLoS One. (2013) 8:e74037. doi: 10.1371/journal.pone.0074037
37. Clarkesmith DE, Lip GYH, Lane DA. Patients’ experiences of atrial fibrillation and non-vitamin K antagonist oral anticoagulants (NOACs), and their educational needs: A qualitative study. Thromb Res. (2017) 153:19–27. doi: 10.1016/j.thromres.2017.03.002
38. Wynn GJ, Todd DM, Webber M, Bonnett L, McShane J, Kirchhof P, et al. The European Heart Rhythm Association symptom classification for atrial fibrillation: validation and improvement through a simple modification. Europace. (2014) 16:965–72. doi: 10.1093/europace/eut395
39. Witassek F, Springer A, Adam L, Aeschbacher S, Beer JH, Blum S, et al. Health-related quality of life in patients with atrial fibrillation: the role of symptoms, comorbidities, and the type of atrial fibrillation. PLoS One. (2019) 14:e0226730. doi: 10.1371/journal.pone.0226730
40. Freeman JV, Simon DN, Go AS, Spertus J, Fonarow GC, Gersh BJ, et al. Association between atrial fibrillation symptoms, quality of life, and patient outcomes: results from the outcomes registry for better informed treatment of atrial fibrillation (ORBIT-AF). Circ Cardiovasc Qual Outcomes. (2015) 8:393–402. doi: 10.1161/CIRCOUTCOMES.114.001303
41. Proietti M, Lip GYH, Laroche C, Fauchier L, Marin F, Nabauer M, et al. Relation of outcomes to ABC (Atrial Fibrillation Better Care) pathway adherent care in European patients with atrial fibrillation: an analysis from the ESC-EHRA EORP atrial fibrillation general long-term (AFGen LT) Registry. Europace. (2021) 23:174–83. doi: 10.1093/europace/euaa274
42. LaMori JC, Mody SH, Gross HJ, daCosta DiBonaventura M, Patel AA, Schein JR, et al. Burden of comorbidities among patients with atrial fibrillation. Ther Adv Cardiovasc Dis. (2013) 7:53–62. doi: 10.1177/1753944712464101
43. Stevens D, Harrison SL, Kolamunnage-Dona R, Lip GYH, Lane DA. The Atrial Fibrillation Better Care pathway for managing atrial fibrillation: a review. Europace. (2021) 23:1511–27. doi: 10.1093/europace/euab092
44. Proietti M, Romiti GF, Olshansky B, Lane DA, Lip GYH. Improved outcomes by integrated care of anticoagulated patients with atrial fibrillation using the simple ABC (Atrial Fibrillation Better Care) Pathway. Am J Med. (2018) 131:1359–66.e6. doi: 10.1016/j.amjmed.2018.06.012
Keywords: atrial fibrillation, patient adherence, risk factors, ABC-pathway, integrated approach
Citation: Esteve-Pastor MA, Ruiz-Ortiz M, Muñiz J, Roldán-Rabadán I, Otero D, Cequier Á, Bertomeu-Martínez V, Badimón L, Anguita M, Lip GYH and Marín F (2022) Impact of Integrated Care Management on Clinical Outcomes in Atrial Fibrillation Patients: A Report From the FANTASIIA Registry. Front. Cardiovasc. Med. 9:856222. doi: 10.3389/fcvm.2022.856222
Received: 16 January 2022; Accepted: 05 April 2022;
Published: 02 May 2022.
Edited by:
Jonathan Douxfils, University of Namur, BelgiumReviewed by:
Job Harenberg, Heidelberg University, GermanyHåkan Wallen, Karolinska Institutet (KI), Sweden
Jordi Heijman, Maastricht University, Netherlands
Copyright © 2022 Esteve-Pastor, Ruiz-Ortiz, Muñiz, Roldán-Rabadán, Otero, Cequier, Bertomeu-Martínez, Badimón, Anguita, Lip and Marín. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco Marín, ZmNvbWFyaW5vQGhvdG1haWwuY29t
†These authors share senior authorship