 Carlos Muñoz-Bravo1,2*
Carlos Muñoz-Bravo1,2* Eva Soler-Iborte3
Eva Soler-Iborte3 Macarena Lozano-Lorca4,5Malak Kouiti4,6Carla González-Palacios Torres4
Macarena Lozano-Lorca4,5Malak Kouiti4,6Carla González-Palacios Torres4 Rocío Barrios-Rodríguez4,5,7José Juan Jiménez-Moleón4,5,7
Rocío Barrios-Rodríguez4,5,7José Juan Jiménez-Moleón4,5,7
- 1Department of Public Health and Psychiatry, School of Medicine, University of Málaga, Málaga, Spain
- 2Biomedical Research Institute of Malaga (IBIMA), Málaga, Spain
- 3Department of Public Health, Hospital Universitario San Cecilio, Spain Biohealth Research Institute in Granada (ibs.GRANADA), Granada, Spain
- 4Department of Preventive Medicine and Public Health, Universidad de Granada, Granada, Spain
- 5Instituto de Investigación Biosanitaria Ibs.GRANADA, Granada, Spain
- 6Laboratory of Health Sciences and Technologies, Higher Institute of Health Sciences, Hassan First University of Settat, Settat, Morocco
- 7Consortium for Biomedical Research in Epidemiology and Public Health (CIBERESP), Madrid, Spain
Background: Despite the fact that several studies have investigated the association between serum copper levels (S-Cu) and the risk of cardiovascular diseases, this relationship remains unclear. The aims of this study were to investigate the association between S-Cu and risk of major adverse cardiovascular events (MACE), including total stroke, ischemic stroke, hemorrhagic stroke, myocardial infarction and cardiovascular mortality, and identify potential sources of results heterogeneity.
Methods: We carried out a systematic review and meta-analysis. The selection criteria were: (1) Observational studies (cohort studies, case-control studies and hybrid studies); (2) Studies containing quantitative data about the relationship between S-Cu and risk of MACE; (3) Estimating association measures; and (4) Studies written in English, French or Spanish. Overall pooled Odds ratio (pOR) and 95% confidence intervals (95% CI) of MACE for the highest vs. lowest S-Cu category were calculated using random-effects models.
Results: Sixteen studies with a total of 41,322 participants were included in the meta-analysis: 10 prospective cohort studies, 5 nested case-control studies and 1 case-control study. Comparing highest vs. lowest category, high S-Cu levels were associated with total stroke (pOR: 1.49, 95% CI 1.22–1.82; I2 = 0%, p = 0.54), myocardial infarction (pOR: 1.31, 95% CI 1.17–1.46; I2 = 0.0%, p = 0.92) and cardiovascular mortality (pOR: 1.60, 95% CI 1.39–1.86; I2 = 0.0%, p = 0.54). Subgroup analysis showed that studies with a hybrid design had higher risks for cardiovascular mortality (pOR: 3.42, 95% CI 1.98–5.92) and ischemic stroke (pOR: 1.54, 95% CI 1.30–1.83).
Conclusion: High S-Cu levels were associated with an increased risk of total stroke, myocardial infarction and cardiovascular mortality. Hybrid studies seems to modify the strength of the association between S-Cu and the risk of cardiovascular mortality and ischemic stroke.
Systematic review registration: [https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022370782], identifier [CRD42022370782].
Introduction
Cardiovascular disease (CVD) is the leading cause of death and disability worldwide, making it a major public health problem. Despite the existing knowledge about this disease (1, 2), it is expected that around 45% of the American adult population will suffer some type of CVD in 2030 (3, 4). Worldwide, ischemic heart disease and stroke are the first and second causes of death and disability, respectively, in adults older than 50 years (2). It is estimated that around the world there are around 7.74 and 4.19 million incident cases of ischemic and hemorrhagic strokes, respectively. The influence of traditional risk factors on the pathophysiology of CVD has been well documented (5–8). However, the identification of new risk factors is a fundamental aspect in the understanding of new mechanisms associated with the development of CVD. In this sense, the relationship between metals, such as copper, and cardiovascular disease has been described, although the results are not always consistent.
In recent decades, there has been an increase in exposure to certain metal compounds. This has led to a growing interest in learning about the influence of these metals on CVD (9–13). Specifically, copper, despite having a fundamental role in cell metabolism, can also promote oxidation of immediate organic principles through the formation of reactive oxygen species (14–17). The determination of serum copper levels represents the most useful biomarker to know the status of this metal in the body (18).
The relationship between serum copper (S-Cu) levels and CVD has been previously analyzed (19–22). However, this relationship remains uncertain. To date, two meta-analyses (23, 24) have examined the relationship between S-Cu and CVD; however, both studies have shortcomings that limit the quality of the reported evidence, namely: (a) they do not study the association S-Cu and cardiovascular mortality; (b) when studying the S-Cu relationship and stroke, they do not differentiate between ischemic stroke and hemorrhagic stroke; and (c) they ignore potential sources of heterogeneity such as: the epidemiological design of the study, the quality of the study, the S-Cu exposure quantile, the year of publication of the study or the country where it is carried out.
The objectives of this meta-analysis were: (1) To assess the association between S-Cu levels and the risk of major adverse cardiovascular events (MACE), including total stroke, ischemic stroke, hemorrhagic stroke, myocardial infarction, and cardiovascular mortality; and (2) To identify possible sources of heterogeneity for the described association between S-Cu and MACE showed in previous studies.
Methods
This systematic review and meta-analysis was performed in accordance with the PRISMA statement standards (25). The protocol was previously registered in PROSPERO (CRD42022370782). The focused question was based on Participants/Population, Exposure, Comparator, and Outcome (PECO) strategy: (P) Men and women older than 18 years old; (E) High S-Cu levels; (C) Low S-Cu levels; (O) Total stroke, ischemic or hemorrhagic stroke, myocardial infarction, and cardiovascular mortality.
Data sources and search strategy
Initially, the search for the scientific literature was carried out through PubMed, Scopus and Web of Science for the period of time between January 1, 1980 and April 20, 2022. The search was kept active from April 21 to May 23, 2023 using the alert systems of each of the electronic platforms. The terms used were: “copper”, “serum copper”, “copper level”, “plasma copper”, “myocardial infarction”, “stroke”, “cardiovascular disease”, and “cardiovascular mortality”. Full information about the search strategy used is shown in Supplementary Table S1. A manual search was also carried out in the references of all the selected articles to ensure that eligible studies were not lost.
Study selection
The article selection criteria were defined a priori as follows: (1) longitudinal observational studies (cohort, case-control and hybrid studies); (2) studies that analyzed the relationship between S-Cu levels (as exposure of interest) and MACE risk (as outcome); (3) by estimating measures of association or to allow its calculation; and (4) studies written in English, French or Spanish. Exclusion criteria were: (a) studies that only looked at the relationship between copper intake and CVD risk; (b) studies that only measured the association of interest in terms of mean difference and standard deviation of copper levels; and (c) letters to the editor, editorials, book chapters, narrative and systematic reviews and trial protocols.
To select the relevant articles, the titles and abstracts were independently reviewed by two investigators (CM-B and ML-L). Duplicate articles were identified and removed. The full text of potentially eligible studies was also assessed by two reviewers (CM-B and ML-L). Disagreements regarding the selection of articles were resolved by a third researcher (JJ-M).
Data extraction
Two reviewers (CM-B and ML-L) independently extracted data from the included studies using a pre-designed form. The following data were recorded: first author and year of publication, country, study design, quantile of serum copper exposure (tertile, quartile or quintile), sample size, percentage of men, mean age of the participants, serum copper concentration in extreme categories, type of MACE, magnitude for effect measure and 95% CI, and the adjustment variables considered.
Quality assessment
The quality of the included studies was assessed using the Newcastle-Ottawa scale (26) (NOS) by two investigators (CM-B and ES-I) independently. This scale uses a star system (with a maximum of nine) to assess the quality of a study with respect to three dimensions: (1) selection of study groups, (2) comparability of study groups, and (3) determination of the exposure or outcome of interest for case-control or cohort studies. According to the NOS score, the selected articles were classified into: high (8–9 stars), medium (6–7), or low (5 or less) quality.
Statistical analysis
The measure of association and 95% confidence interval that estimated the MACE risk were extracted from each of the included studies when comparing the highest S-Cu level category against the lowest (reference category). The association measures of the multivariate models corresponded to those obtained with the model adjusted for the largest number of variables. To obtain the overall pOR, a random effects model was applied and weighted for the variability of the included studies. To assess the heterogeneity of results between the studies, forest plots were examined, and the Cochran Q test was used. I2 was estimated and heterogeneity was considered as low for values between 25% and 50%, moderate for 50%–75% and high for >75% (27). We explored heterogeneity by stratifying studies based on several potential variables that we assume might have produced the detected heterogeneity. These analyses were conducted considering the following variables: type of study design, sex of participants, country, S-Cu exposure quantile, as well as study quality.
A sensitivity analysis was performed, eliminating those studies that reported abnormally high association measures, to assess the influence of these values on the estimated risk. The possible presence of publication bias was examined by visual inspection of funnel plots. If asymmetry was observed suggestive of a probable publication bias, the Egger test was performed. All statistical tests were two-sided with an α level of 0.05. All statistical analyses were conducted using Stata 17.0 (Stata Corp).
Results
Identification and selection of studies
Figure 1 shows a detailed flowchart of the identification and selection of studies. Initially, 1,969 articles were identified as potentially relevant. Of these, 976 articles were eliminated for being duplicates, 939 for not being relevant after reviewing the title and abstract, and 42 after reading the full text. Subsequently, 2 articles found through manual consultation of the included articles' references and 2 through the alert systems activated in the different electronic search platforms used were added. Finally, a total of 16 studies were included in this systematic review and meta-analysis (20–22, 28–39).
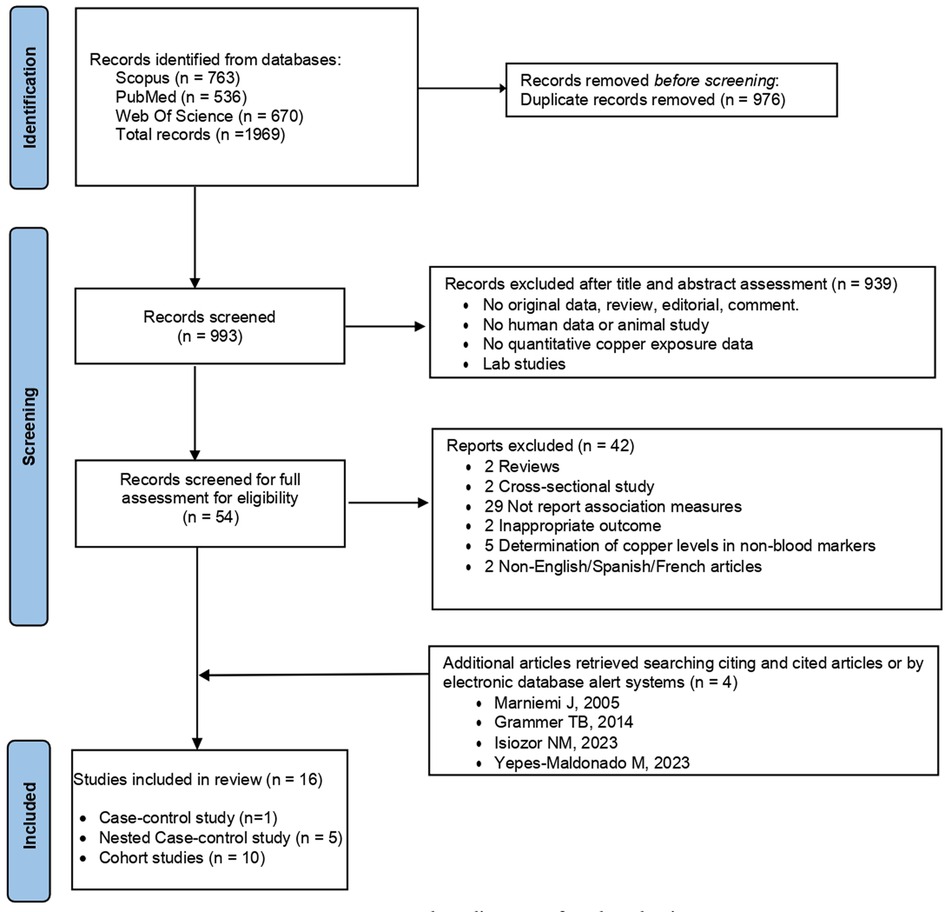
Figure 1. Flow diagram of study selection.
Characteristics of the included studies and quality assessment
The main characteristics of the included studies are shown in Table 1. A total of 41,322 participants were included in the 15 studies. The number of participants in the studies ranged from 186 to 6,155 people, with an age range from 15 to 99 years. The articles were published between 1988 and 2023. Of the total number of studies included, one study evaluated two different cardiovascular events as outcome variables (stroke and myocardial infarction) (21), while the remaining 15 evaluated a single type of cardiovascular event as the outcome variable. Of these, three articles distinguished between total, ischemic and hemorrhagic stroke (35, 37, 40), while one article considered only ischemic stroke (34).
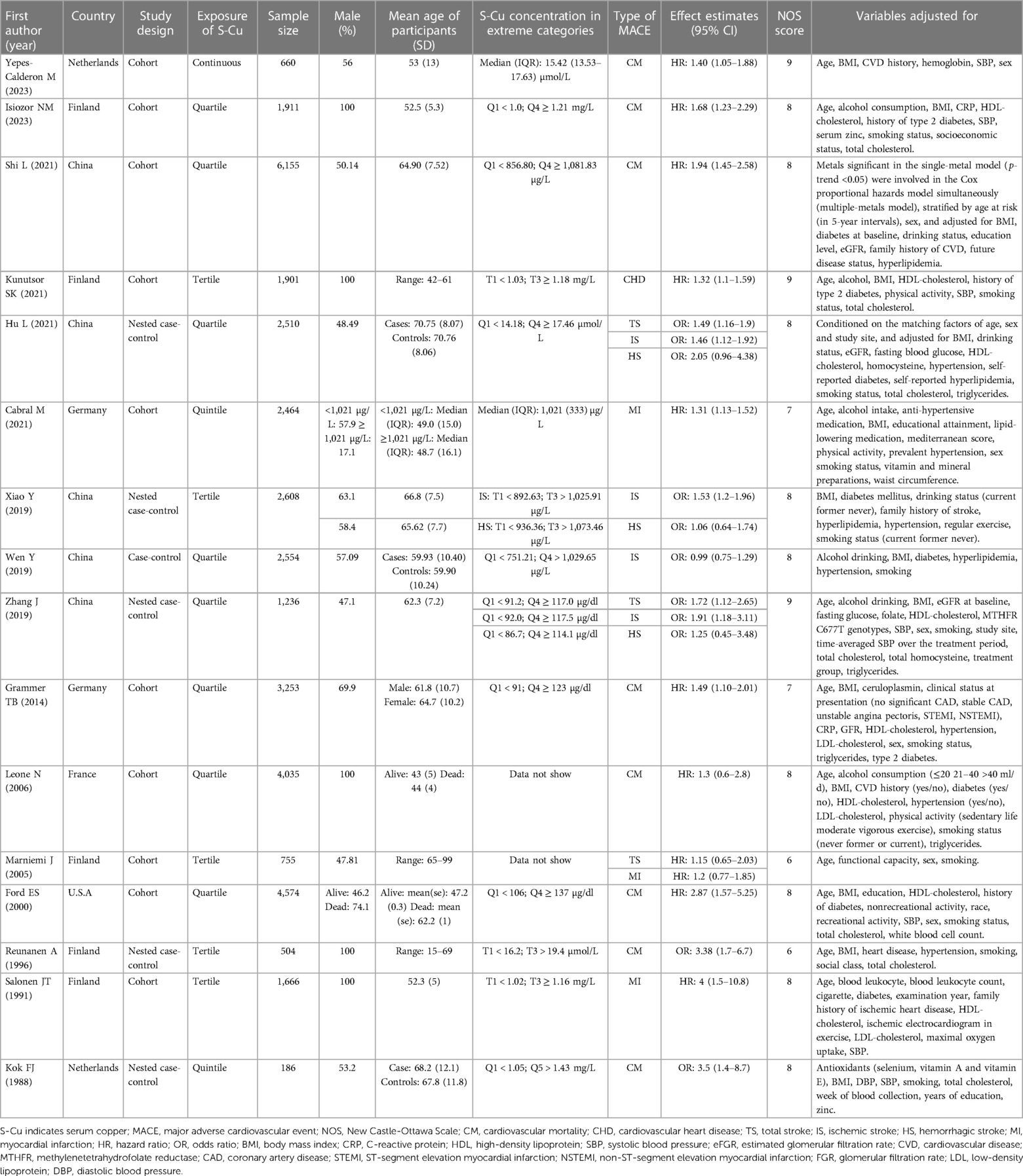
Table 1. Characteristics of the studies included in the systematic review and meta-analysis.
On the other hand, eight studies evaluated cardiovascular mortality as the main outcome (20, 22, 28, 30–32, 39) two the risk of myocardial infarction (29, 36), and one the risk of coronary artery disease (38). Regarding the geographical location, five studies were conducted in the Asian population (China) (22, 34, 35, 37, 40), ten in the European population [Finland (n = 5) (21, 29, 30, 38, 39), Germany (n = 2) (32, 36), France (n = 1) (31) and 1 Netherlands (n = 2) (28, 41)] and one in the American population (USA) (20). Regarding the sex of the participants, five studies included only men (29–31, 38, 39). Regarding the design, ten were from cohort studies (20–22, 29, 31, 32, 36, 38, 39) five nested case-control (28, 30, 35, 37, 40), and one case-control (34). Twelve of the fifteen articles included (75%) were assessed as high quality, the rest (25%) as medium quality (Supplementary Table S2).
Risk of stroke
The overall pOR of the association between S-Cu and the risk of total stroke, ischemic stroke, and hemorrhagic stroke was 1.49 (95% CI 1.22–1.82), 1.39 (95% CI 1.08–1.78) and 1.29 (95% CI 0.87–1.91), respectively (Figure 2). Significant heterogeneity was observed between studies for ischemic stroke (I2 = 69.3%, p = 0.04), with no heterogeneity being found for total stroke and hemorrhagic stroke. Visual inspection of funnel plots and Egger test revealed no evidence of publication bias (Supplementary Figures S1–S3).
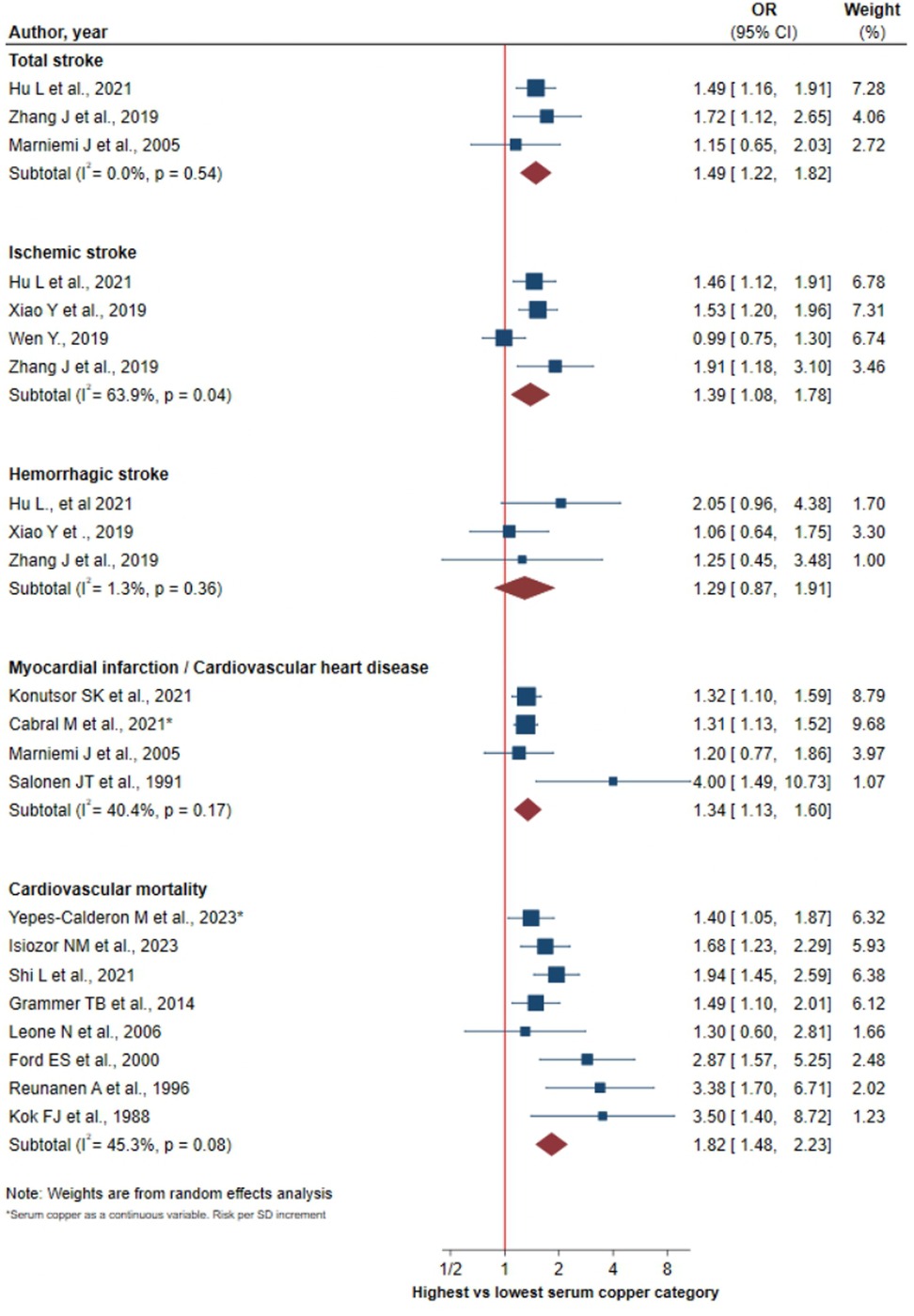
Figure 2. Forest plot of the association between serum copper levels and MACE.
Risk of myocardial infarction
A significant association was found between S-Cu levels and the risk of heart attack from myocardium/coronary disease (pOR: 1.34, 95% CI 1.13–1.60) with a medium-low heterogeneity among studies (I2 = 40.4%, p = 0.17) (Figure 2). Both the funnel plot and the Egger test (p = 0.1203) did not clearly show the existence of publication bias. Although the “abnormal” value belonging to the study by Salonen et al. (29) clearly impacted with the p value of the Egger's test not being superior (Supplementary Figures S4, S5).
Risk of cardiovascular mortality
S-Cu levels were positively associated with cardiovascular mortality risk (pOR: 1.82, 95% CI 1.48–2.23), showing medium-low heterogeneity among studies (I2 = 45.3%, p = 0.08) (Figure 2). The funnel plot showed a slight asymmetry corroborated by Egger's test (p = 0.039) (Supplementary Figure S6).
Sensitivity analysis and subgroup analysis
Of the sixteen studies included in the meta-analysis, the four studies published before from 2005 (20, 28–30) showed a particularly high magnitude of the effect measure, OR equal or higher than 2.87. Sensitivity analysis revealed a decreased risk of cardiovascular mortality, 1.60 (95% CI 1.39–1.86) vs. 1.82 for the total of the studies although the confidence intervals are overlapped. On the other hand, the risk of myocardial infarction was virtually unchanged, 1.31 (95% CI 1.17–1.46) (Figure 3). The previously observed heterogeneity for cardiovascular mortality risk was eliminated following this sensitivity analysis, as well as the disappearance of publication bias (Supplementary Figure S7).
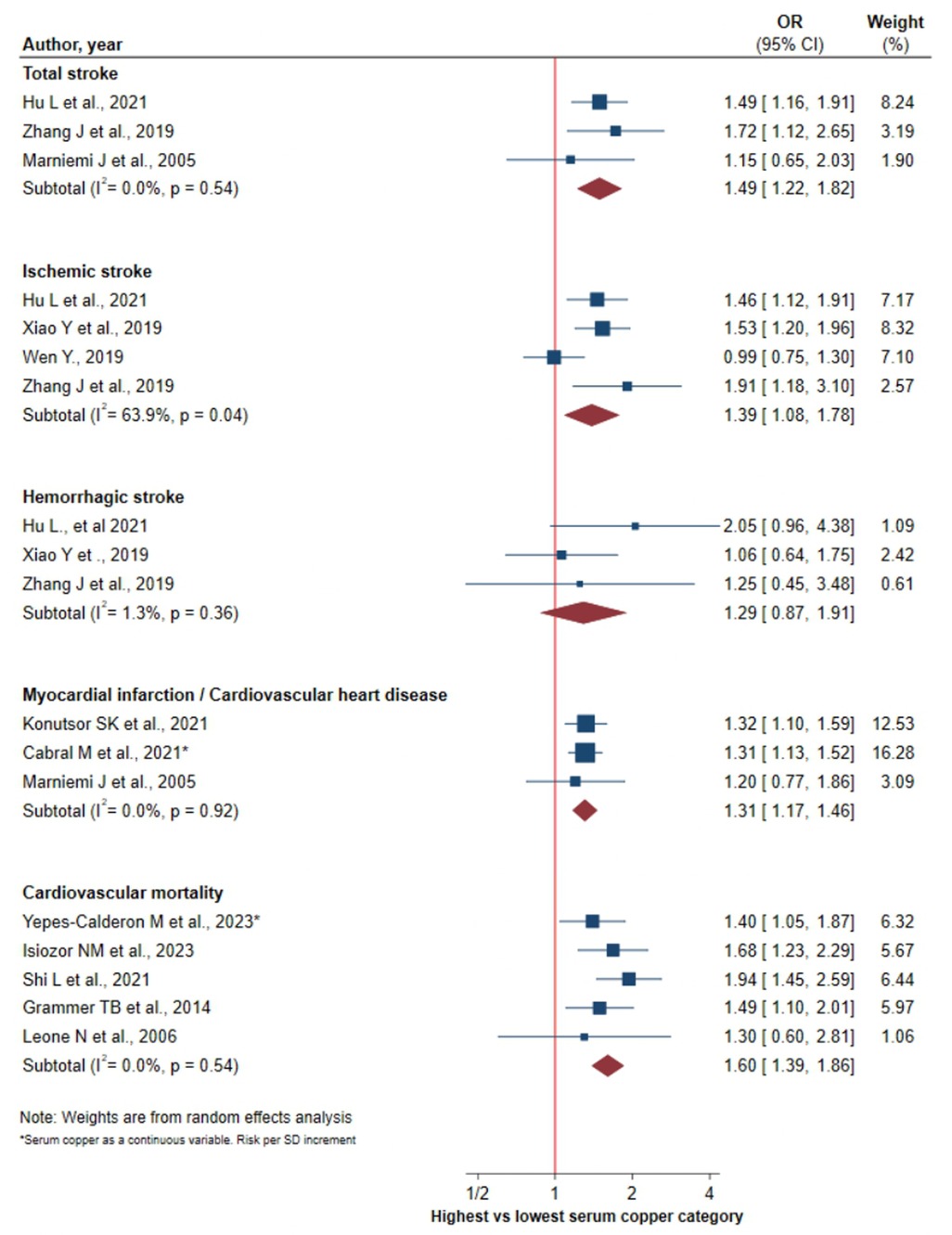
Figure 3. Forest plot of the association between serum copper levels and MACE without the studies before 2005.
Table 2 presents the subgroup analysis for cardiovascular mortality. The direct association observed between S-Cu and cardiovascular mortality is confirmed in most of the subgroups established according to the participants' sex, country, and S-Cu exposure quantile. However, in the analysis by study design, the risk of cardiovascular mortality was significantly higher in studies with a hybrid design compared to cohort studies (pOR: 3.42, 95% CI 1.98–5.92; I2 = 0%, p = 0.95 vs. pOR: 1.67, 95% CI 1.41–1.97; I2 = 22.9%, p = 0.26). In the analysis based on the quality of the studies, the association was significant for high quality studies (pOR: 1.80, 95% CI 1.44–2.25; I2 = 38.9%, p = 0.15), but not for medium quality (pOR: 2.11, 95% CI 0.96–4.67; I2 = 78.2%, p = 0.03). A greater strength of the association, relative to the overall pooled effect, was also observed in the studies conducted in Finland. For ischemic stroke, the subgroup analysis revealed a slightly increased risk in studies with a hybrid design compared with case-control studies (pOR: 1.54, 95% CI 1.30–1.83; I2 = 0%, p = 0.63 vs. pOR: 0.99, 95% CI 0.75–1.30) (Table 3). Regarding myocardial infarction, no source of heterogeneity was identified (Supplementary Table S3).
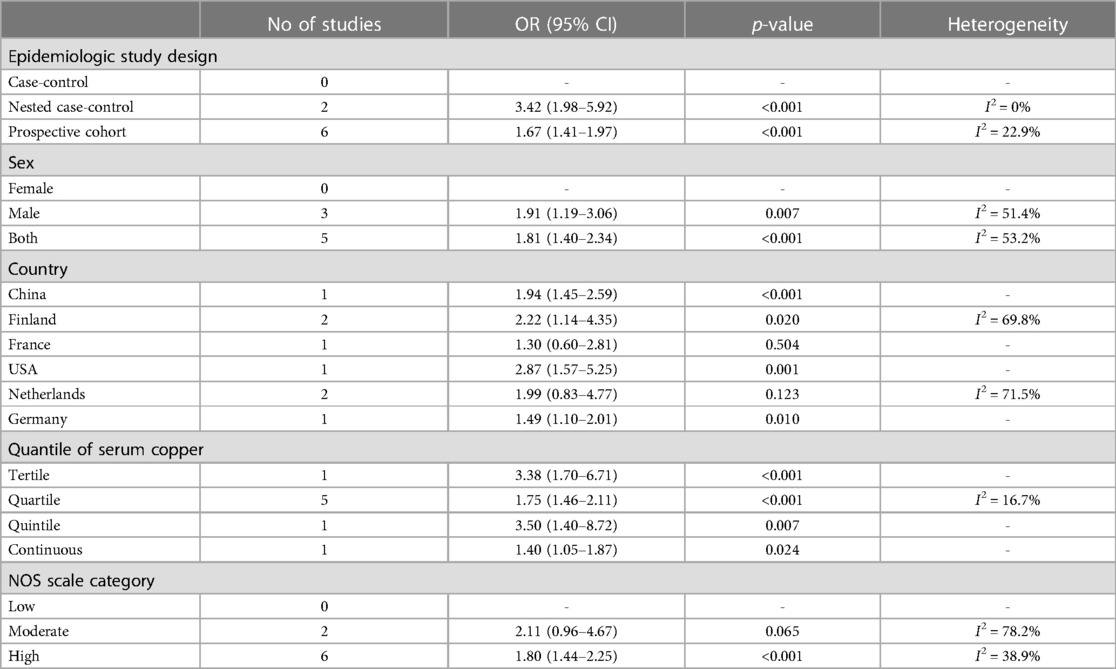
Table 2. Subgroup analysis of risk of cardiovascular mortality.
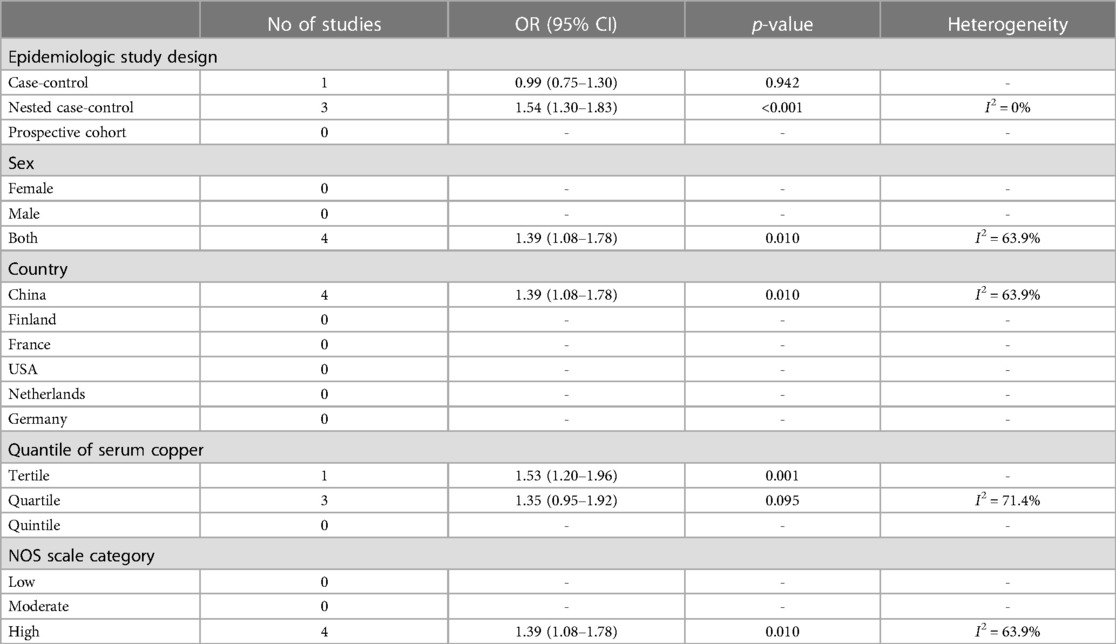
Table 3. Subgroup analysis of risk of ischemic stroke.
Discussion
To the best of our knowledge, this is the first meta-analysis that, in the context of studying the relationship between S-Cu and MACE, examines the relationship between S-Cu and cardiovascular mortality, as well as between S-Cu and stroke, distinguishing between ischemic stroke and hemorrhagic stroke. Within population reference values, a direct association was observed between S-Cu levels and the risk of total stroke, myocardial infarction and cardiovascular mortality. No association was found between S-Cu and hemorrhagic stroke or ischemic stroke. The observed heterogeneity for myocardial infarction and cardiovascular mortality disappeared after the influence analysis was performed in which studies reporting particularly high measures of association were removed. Finally, based on the subgroup analysis, our findings showed that studies with a hybrid design described higher risks for cardiovascular mortality and ischemic stroke.
Observational studies have previously analyzed the relationship between copper levels and CVD, obtaining contradictory results. This is observed in those studies where exposure to copper has been determined using serum concentration. Several of these studies suggest an increased risk of CVD associated with high levels of S-Cu (20, 22, 32, 38, 39), while other researchers have not found any such association (19, 21, 31, 34). Likewise, contradictory results have been reported in studies that analyzed the relationship between dietary consumption of copper and CVD (42–47).
Copper is an essential element for the organism that forms part of proteins with important biological functions, such as ceruloplasmin, superoxide dismutase, cytochrome c oxidase or lysyl oxidase (48). However, under certain circumstances it can also be harmful to the body, as it can favor the formation of reactive oxygen species through Fenton-type redox reactions (49, 50). It is through this mechanism that copper contributes to the development of the atherosclerotic process, which lays the foundation for cardiovascular disease (51–53). Other studies have indicated the involvement of copper in the pathophysiology of CVD, through the formation of the copper-homocysteine complex, favoring endothelial dysfunction (54, 55). Likewise, a positive association has been observed between S-Cu levels and acute phase proteins during the inflammatory process in the context of CVD (20, 31, 32, 56). Other investigations have reported an association between copper levels and an increased prevalence of certain cardiovascular risk factors such as hyperlipidemia (37, 52), hypertension or high fasting blood glucose, among others (37). High levels of S-Cu have also been related to patients with type 2 diabetes mellitus (43). In patients with Wilson's disease, characterised by excessively high copper levels due to a genetic disorder, cardiac disorders such as mild left ventricular hypertrophy, benign supraventricular tachycardias and extrasystolic beats have been reported, providing evidence that copper may be a risk factor for cardiovascular disease (57, 58).
Two previous meta-analyses have examined the relationship of copper levels on cardiovascular events, although they have limitations that should be considered. Bao's meta-analysis (23) focuses on analysing the relationship between copper levels and stroke, but does not differentiate between hemorrhagic and ischemic events. For its part, the Chowdhury's meta-analysis (24) gives estimates for which it does not assess the presence of heterogeneity, for example a pOR of 2.22 is given for coronary heart disease with an I2 of 66.7% and a p for heterogeneity of 0.3. Moreover, in the latter meta-analysis, stroke risk and stroke mortality are considered as if they were the same event. Limitations that cast doubt on the estimates made by both reviews on the relationship between copper and the different cardiovascular events.
We decided not to conduct a dose-response meta-analysis for the following reasons: (1) Not all studies classify serum copper levels in the same way. There are studies that work with tertiles, others with quartiles, one with quintiles. And there are even two studies that work with the variable continuously; (2) For those studies that use the same way of classifying blood copper exposure levels, the cut-off points are different and therefore we consider that they should not be used to analyse a dose-response gradient; (3) Moreover, some studies do not report the cut-off points for the different quantiles; (4) Not all studies give the median of serum copper for the different categories; and (5) To estimate a dose-response meta-analysis is convenient to know the number of cases by category. In this sense, some articles do not show the number of cases per quantile.
This study presents some limitations that must be considered in the interpretation of the results. First, our review was based solely on data from observational studies, an aspect that must be taken into account when assessing the level of causality. Second, although most of the articles estimated measures of association using multivariable regression models, the presence of residual confounding cannot be ruled out. In this sense, the lack of adjustment for other metals, such as zinc or other variables such as dietary pattern or total energy intake, could affect the independence of the association between S-Cu and MACE risk. Third, the restriction in the language may have limited the number of studies included in the meta-analysis; however, the number of articles published in languages other than those considered in this study is most likely very low.
The present meta-analysis also has several strengths. First, to the best of our knowledge, it is the first meta-analysis that, in the context of the study of the relationship between S-Cu and MACE, examines the relationship between S-Cu and cardiovascular mortality and between S-Cu and stroke, distinguishing between ischemic stroke and hemorrhagic stroke. Second, the type of study design has been identified as a source of heterogeneity, which has not been described to date, for cardiovascular mortality and ischemic stroke. Third, to control for confounding bias, the measures of association considered have been those from the maximum fit models. Finally, and to the best of our knowledge, these data provide the most complete information to date on the association between S-Cu and MACE risk.
Conclusion
We found a positive association between S-Cu levels and the risk of total stroke, myocardial infarction and cardiovascular mortality. No association was found for hemorrhagic stroke or ischemic stroke. The epidemiological design of the studies seems to modify the strength of the association between S-Cu and the risk of cardiovascular mortality and ischemic stroke. Monitoring of S-Cu levels, as an independent risk marker, could be an additional tool in the primary prevention of MACE.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
CM-B and ES-I: conceptualization, formal analysis, visualization, and writing—original draft. ML-L, MK, CG-P, and RB-R: writing—review and editing. JJ-M: conceptualization, resources, writing—review, editing and supervision. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2023.1217748/full#supplementary-material.
References
1. Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. (2017) 70:1–25. doi: 10.1016/j.jacc.2017.04.052
2. Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
3. Yin T, Zhu X, Xu D, Lin H, Lu X, Tang Y, et al. The association between dietary antioxidant micronutrients and cardiovascular disease in adults in the United States: a cross-sectional study. Front Nutr. (2022) 8:1–13. doi: 10.3389/fnut.2021.799095
4. Mensah GA, Roth GA, Fuster V. The global burden of cardiovascular diseases and risk factors: 2020 and beyond. J Am Coll Cardiol. (2019) 74:2529–32. doi: 10.1016/j.jacc.2019.10.009
5. Powell KL, Stephens SR, Stephens AS. Cardiovascular risk factor mediation of the effects of education and genetic risk score on cardiovascular disease: a prospective observational cohort study of the Framingham heart study. BMJ Open. (2021) 11:1–10. doi: 10.1136/bmjopen-2020-045210
6. Groenewegen A, Rutten FH, Mosterd A, Hoes AW. Epidemiology of heart failure. Eur J Heart Fail. (2020) 22:1342–56. doi: 10.1002/ejhf.1858
7. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics - 2018 update: a report from the American Heart Association. Circulation. (2018) 137:67–492. doi: 10.1161/CIR.0000000000000558
8. Xu J, Xu G, Fang J. Association between serum copper and stroke risk factors in adults: evidence from the national health and nutrition examination survey, 2011–2016. Biol Trace Elem Res. (2022) 200:1089–94. doi: 10.1007/s12011-021-02742-x
9. Lamas GA, Navas-Acien A, Mark DB, Lee KL. Heavy metals, cardiovascular disease, and the unexpected benefits of chelation therapy. J Am Coll Cardiol. (2016) 67:2411–8. doi: 10.1016/j.jacc.2016.02.066
10. Nasab H, Rajabi S, Eghbalian M, Malakootian M, Hashemi M, Mahmoudi-Moghaddam H. Association of as, pb, cr, and zn urinary heavy metals levels with predictive indicators of cardiovascular disease and obesity in children and adolescents. Chemosphere. (2022) 294:133664. doi: 10.1016/j.chemosphere.2022.133664
11. Carlsen HK, Andersson EM, Molnár P, Oudin A, Xu Y, Wichmann J, et al. Incident cardiovascular disease and long-term exposure to source-specific air pollutants in a Swedish cohort. Environ Res. (2022) 209. doi: 10.1016/j.envres.2022.112698
12. Nguyen HD, Oh H, Hoang NHM, Kim MS. Association between heavy metals, high-sensitivity C-reaction protein and 10-year risk of cardiovascular diseases among adult Korean population. Sci Rep. (2021) 11:1–14. doi: 10.1038/s41598-021-94158-9
13. Duan W, Xu C, Liu Q, Xu J, Weng Z, Zhang X, et al. Levels of a mixture of heavy metals in blood and urine and all-cause, cardiovascular disease and cancer mortality: a population-based cohort study. Environ Pollut. (2020) 263:114630. doi: 10.1016/j.envpol.2020.114630
14. Chen J, Jiang Y, Shi H, Peng Y, Fan X, Li C. The molecular mechanisms of copper metabolism and its roles in human diseases. Pflugers Arch. (2020) 472:1415–29. doi: 10.1007/s00424-020-02412-2
15. Uauy R, Olivares M, Gonzalez M. Essentiality of copper in humans. Am J Clin Nutr. (1998) 67:952–9. doi: 10.1093/ajcn/67.5.952S
16. Bost M, Houdart S, Oberli M, Kalonji E, Huneau JF, Margaritis I. Dietary copper and human health: current evidence and unresolved issues. J Trace Elem Med Biol. (2016) 35:107–15. doi: 10.1016/j.jtemb.2016.02.006
17. Fukai T, Ushio-Fukai M, Kaplan JH. Copper transporters and copper chaperones: roles in cardiovascular physiology and disease. Am J Physiol Cell Physiol. (2018) 315:186–201. doi: 10.1152/ajpcell.00132
18. Harvey LJ, Ashton K, Hooper L, Casgrain A, Fairweather-Tait SJ. Methods of assessment of copper status in humans: a systematic review. Am J Clin Nutr. (2009) 89:2009S–24S. doi: 10.3945/ajcn.2009.27230E
19. Karadas S, Sayin R, Aslan M, Gonullu H, Kati C, Dursun R, et al. Serum levels of trace elements and heavy metals in patients with acute hemorrhagic stroke. J Membr Biol. (2014) 247:175–80. doi: 10.1007/s00232-013-9621-0
20. Ford ES. Serum copper concentration and coronary heart disease among US adults. Am J Epidemiol. (2000) 151:1182–8. doi: 10.1093/oxfordjournals.aje.a010168
21. Marniemi J, Alanen E, Impivaara O, Seppänen R, Hakala P, Rajala T, et al. Dietary and serum vitamins and minerals as predictors of myocardial infarction and stroke in elderly subjects. Nutr Metab Cardiovasc Dis. (2005) 15:188–97. doi: 10.1016/j.numecd.2005.01.001
22. Shi L, Yuan Y, Xiao Y, Long P, Li W, Yu Y, et al. Associations of plasma metal concentrations with the risks of all-cause and cardiovascular disease mortality in Chinese adults. Environ Int. (2021) 157:106808. doi: 10.1016/j.envint.2021.106808
23. Bao QJ, Zhao K, Guo Y, Wu XT, Yang JC, Yang MF. Environmental toxic metal contaminants and risk of stroke: a systematic review and meta-analysis. Environ Sci Pollut Res Int. (2022) 29:32545–65. doi: 10.1007/s11356-022-18866-z
24. Chowdhury R, Ramond A, O’Keeffe LM, Shahzad S, Kunutsor SK, Muka T, et al. Environmental toxic metal contaminants and risk of cardiovascular disease: systematic review and meta-analysis. BMJ. (2018) 362:14–6. doi: 10.1136/bmj.k3310
25. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
26. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp (Accessed September 13, 2022).
27. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557. doi: 10.1136/BMJ.327.7414.557
28. Kok FJ, Van Duijn CM, Hofman A, Van Der Voet GB, De Wolff FA, Paays CHC, et al. Serum copper and zinc and the risk of death from cancer and cardiovascular disease. Am J Epidemiol. (1988) 128:352–9. doi: 10.1093/oxfordjournals.aje.a114975
29. Salonen JT, Salonen R, Korpela H, Suntioinen S, Tuomilehto J. Serum copper and the risk of acute myocardial infarction: a prospective population study in men in eastern Finland. Am J Epidemiol. (1991) 134:268–76. doi: 10.1093/oxfordjournals.aje.a116080
30. Reunanen A, Knekt P, Marniemi J, Mäki J, Maatela J, Aromaa A. Serum calcium, magnesium, copper and zinc and risk of cardiovascular death. Eur J Clin Nutr. (1996) 50:431–7.8862478
31. Leone N, Courbon D, Ducimetiere P, Zureik M. Zinc, copper, and magnesium and risks for all-cause, cancer, and cardiovascular mortality. Epidemiology. (2006) 17:308–14. doi: 10.1097/01.ede.0000209454.41466.b7
32. Grammer TB, Kleber ME, Silbernagel G, Pilz S, Scharnagl H, Lerchbaum E, et al. Copper, ceruloplasmin, and long-term cardiovascular and total mortality (the ludwigshafen risk and cardiovascular health study). Free Radic Res. (2014) 48:706–15. doi: 10.3109/10715762.2014.901510
33. Zhang J, Cao J, Zhang Y, Li H, Zhang H, Huo Y, et al. Baseline plasma zinc and risk of first stroke in hypertensive patients a nested case-control study. Stroke. (2019) 50:3255–8. doi: 10.1161/STROKEAHA.119.027003
34. Wen Y, Huang S, Zhang Y, Zhang H, Zhou L, Li D, et al. Associations of multiple plasma metals with the risk of ischemic stroke: a case-control study. Environ Int. (2019) 125:125–34. doi: 10.1016/j.envint.2018.12.037
35. Xiao Y, Yuan Y, Liu Y, Yu Y, Jia N, Zhou L, et al. Circulating multiple metals and incident stroke in Chinese adults: the dongfeng-tongji cohort. Stroke. (2019) 50:1661–8. doi: 10.1161/STROKEAHA.119.025060
36. Cabral M, Kuxhaus O, Eichelmann F, Kopp JF, Alker W, Hackler J, et al. Trace element profile and incidence of type 2 diabetes, cardiovascular disease and colorectal cancer: results from the EPIC-potsdam cohort study. Eur J Nutr. (2021) 60:3267–78. doi: 10.1007/s00394-021-02494-3
37. Hu L, Bi C, Lin T, Liu L, Song Y, Wang P, et al. Association between plasma copper levels and first stroke: a community-based nested case–control study. Nutr Neurosci. (2022) 25:1524–33. doi: 10.1080/1028415X.2021.1875299
38. Kunutsor SK, Dey RS, Laukkanen JA. Circulating serum copper is associated with atherosclerotic cardiovascular disease, but not venous thromboembolism: a prospective cohort study. Pulse. (2021) 9:109–15. doi: 10.1159/000519906
39. Isiozor NM, Kunutsor SK, Vogelsang DH, Isiozor I, Kauhanen J, Laukkanen JA. Serum copper and the risk of cardiovascular disease death in Finnish men. Nutr Metab Cardiovasc Dis. (2023) 33:151–7. doi: 10.1016/J.NUMECD.2022.09.024
40. Zhang J, Cao J, Zhang H, Jiang C, Lin T, Zhou Z, et al. Plasma copper and the risk of first stroke in hypertensive patients: a nested case-control study. Am J Clin Nutr. (2019) 110:212–20. doi: 10.1093/ajcn/nqz099
41. Yepes-Calderón M, Kremer D, Post A, Sotomayor CG, Seidel U, Huebbe P, et al. Plasma copper concentration is associated with cardiovascular mortality in male kidney transplant recipients. Antioxidants. (2023) 12:454. doi: 10.3390/ANTIOX12020454
42. Bates CJ, Hamer M, Mishra GD. Redox-modulatory vitamins and minerals that prospectively predict mortality in older British people: the national diet and nutrition survey of people aged 65 years and over. Br J Nutr. (2011) 105:123–32. doi: 10.1017/S0007114510003053
43. Eshak ES, Iso H, Yamagishi K, Maruyama K, Umesawa M, Tamakoshi A. Associations between copper and zinc intakes from diet and mortality from cardiovascular disease in a large population-based prospective cohort study. J Nutr Biochem. (2018) 56:126–32. doi: 10.1016/j.jnutbio.2018.02.008
44. Yang L, Chen X, Cheng H, Zhang L. Dietary copper intake and risk of stroke in adults: a case-control study based on national health and nutrition examination survey 2013–2018. Nutrients. (2022) 14:409. doi: 10.3390/nu14030409
45. Jones AA, DiSilvestro RA, Coleman M, Wagner TL. Copper supplementation of adult men: effects on blood copper enzyme activities and indicators of cardiovascular disease risk. Metab Clin Exp. (1997) 46:1380–3. doi: 10.1016/S0026-0495(97)90135-9
46. Dinicolantonio JJ, Mangan D, O’Keefe JH. Copper deficiency may be a leading cause of ischaemic heart disease. Open Heart. (2018) 5:e000784. doi: 10.1136/openhrt-2018-000784
47. Klevay LM. Symposium: trace element nutrition and human health cardiovascular disease from copper deficiency-a history 1. J Nutr. (2000) 130:489–92. doi: 10.1093/jn/130.2.489S
48. Linder MC, Hazegh-Azam M. Copper biochemistry and molecular biology. Am J Clin Nutr. (1996) 63:797S–811S. doi: 10.1093/ajcn/63.5.797
49. Burkitt MJ. A critical overview of the chemistry of copper-dependent low density lipoprotein oxidation: roles of lipid hydroperoxides, α-tocopherol, thiols, and ceruloplasmin. Arch Biochem Biophys. (2001) 394:117–35. doi: 10.1006/abbi.2001.2509
50. Jomova K, Valko M. Advances in metal-induced oxidative stress and human disease. Toxicology. (2011) 283:65–87. doi: 10.1016/j.tox.2011.03.001
51. Stadler N, Lindner RA, Davies MJ. Direct detection and quantification of transition metal ions in human atherosclerotic plaques: evidence for the presence of elevated levels of iron and copper. Arterioscler Thromb Vasc Biol. (2004) 24:949–54. doi: 10.1161/01.ATV.0000124892.90999.cb
52. Ari E, Kaya Y, Demir H, Asicioglu E, Keskin S. The correlation of serum trace elements and heavy metals with carotid artery atherosclerosis in maintenance hemodialysis patients. Biol Trace Elem Res. (2011) 144:351–9. doi: 10.1007/s12011-011-9103-0
53. Nakano E, Williamson MP, Williams NH, Powers HJ. Copper-mediated LDL oxidation by homocysteine and related compounds depends largely on copper ligation. Biochim Biophys Acta Mol Basis Dis. (2004) 1688:33–42. doi: 10.1016/j.bbadis.2003.10.005
54. Jiang Y, Wang LP, Dong XH, Cai J, Jiang GJ, Zhang C, et al. Trace amounts of copper in drinking water aggravate cerebral ischemic injury via impairing endothelial progenitor cells in mice. CNS Neurosci Ther. (2015) 21:677–80. doi: 10.1111/cns.12427
55. Kang YJ. Copper and homocysteine in cardiovascular diseases. Pharmacol Ther. (2011) 129:321–31. doi: 10.1016/j.pharmthera.2010.11.004
56. Skalny AV, Klimenko LL, Turna AA, Budanova MN, Baskakov IS, Savostina MS, et al. Serum trace elements are associated with hemostasis, lipid spectrum and inflammatory markers in men suffering from acute ischemic stroke. Metab Brain Dis. (2017) 32:779–88. doi: 10.1007/s11011-017-9967-6
57. Buksińska-Lisik M, Litwin T, Pasierski T, Członkowska A. Cardiac assessment in Wilson’s disease patients based on electrocardiography and echocardiography examination. Arch Med Sci. (2019) 15:857. doi: 10.5114/AOMS.2017.69728
Keywords: serum copper, cardiovascular disease, cardiovascular mortality, stroke, myocardial infarction, meta-analysis, major adverse cardiovascular events
Citation: Muñoz-Bravo C, Soler-Iborte E, Lozano-Lorca M, Kouiti M, González-Palacios Torres C, Barrios-Rodríguez R and Jiménez-Moleón JJ (2023) Serum copper levels and risk of major adverse cardiovascular events: a systematic review and meta-analysis. Front. Cardiovasc. Med. 10:1217748. doi: 10.3389/fcvm.2023.1217748
Received: 5 May 2023; Accepted: 14 June 2023;
Published: 27 June 2023.
Edited by:
Sorayya Kheirouri, Tabriz University of Medical Sciences, IranReviewed by:
Tommaso Filippini, University of Modena and Reggio Emilia, ItalyTomasz Litwin, Institute of Psychiatry and Neurology (IPiN), Poland
© 2023 Muñoz-Bravo, Soler-Iborte, Lozano-Lorca, Kouiti, González-Palacios Torres, Barrios-Rodríguez and Jiménez-Moleón. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Muñoz-Bravo Y2FybG9zbWJAdW1hLmVz