 Rauf Nouni-García1,2,3,4
Rauf Nouni-García1,2,3,4 Elisabeth Ramirez-Familia5
Elisabeth Ramirez-Familia5 Adriana López-Pineda3,4,5*Amanda Esquerdo-Arroyo4,5Álvaro Carbonell-Soliva5,6María Martínez-Muñóz5Antonio F. Compañ Rosique1
Adriana López-Pineda3,4,5*Amanda Esquerdo-Arroyo4,5Álvaro Carbonell-Soliva5,6María Martínez-Muñóz5Antonio F. Compañ Rosique1 Jose A. Quesada3,4,5
Jose A. Quesada3,4,5 Concepción Carratalá-Munuera3,4,5Vicente F. Gil-Guillén3,4,5
Concepción Carratalá-Munuera3,4,5Vicente F. Gil-Guillén3,4,5
- 1Pathology and Surgery Department, Medical School, University Miguel Hernández de Elche, Alicante, Spain
- 2Institute of Health and Biomedical Research of Alicante, General University Hospital of Alicante, Diagnostic Center, Alicante, Spain
- 3Network for Research on Chronicity, Primary Care and Health Promotion (RICAPPS), San Juan de Alicante, Spain
- 4Primary Care Research Center, Miguel Hernandez University, San Juan de Alicante, Spain
- 5Department of Clinical Medicine, University of Miguel Hernández Elche, Comunidad Valenciana, Spain
- 6Center for Research on Aging, Elche, Spain
Background: Aspirin (acetylsalicylic acid, ASA) is widely recommended for long-term secondary cardiovascular prevention (SCP), but its clinical effectiveness depends on patient adherence, which remains suboptimal. Understanding how adherence and persistence to ASA are measured is essential to improving outcomes. This systematic review aimed to identify the methods used to assess adherence and persistence to ASA in SCP and evaluate their validity indicators.
Methods: We systematically searched EMBASE, MEDLINE, and Scopus for studies published up to October 30, 2023, reporting methods for measuring adherence or persistence to ASA in adults undergoing secondary cardiovascular prevention. Two reviewers independently screened articles and extracted data on study characteristics, measurement methods, and validity indicators. The results were synthesized in tabular form according to method type (indirect or direct) and outcome assessed (adherence or persistence). Risk of bias was evaluated for studies that conducted validation analyses of the measurement methods.
Results: Forty studies were included, most conducted in the United States. Indirect methods predominated: self-report questionnaires (45%, n = 18) and pharmacy dispensing records (32.5%, n = 13) were the most common tools for assessing adherence. Direct methods, such as platelet function tests or biochemical assays, were less frequently used (25%, n = 10). For persistence, dispensing records were the most used method (70%, n = 7). No indirect method reported validation specifically for ASA adherence or persistence. Validity indicators were only partially available for some direct methods.
Conclusions: Adherence and persistence to ASA in SCP are primarily measured through indirect methods, with a lack of specific validation for ASA. There is a critical need to develop standardized, validated tools that integrate both direct and indirect measures and address gender-specific barriers to adherence.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42023470993, PROSPERO identifier CRD42023470993.
Background
Cardiovascular diseases (CVD) remain one of the leading causes of mortality worldwide. These diseases account for 19.7 million deaths annually across the globe, according to the World Health Organization, and it is expected that, due to population ageing, this number will continue to rise in the coming decades (1). In Spain, CVD was the second leading cause of death, with a mortality rate of 237.5 deaths per 100,000 inhabitants (26.5%), in 2023 (2). Effective secondary cardiovascular prevention (SCP), through lifestyle and pharmacological interventions, reduces mortality, prevents recurrent events, and improves quality of life (3). Among the recommended medications, acetylsalicylic acid (ASA), commonly referred to as aspirin, is an antiplatelet agent that works by inhibiting thromboxane A2 formation, thereby reducing platelet aggregation and preventing vascular obstruction due to clot formation (4). Long-term low-dose aspirin use has been shown to significantly reduce the risk of both fatal and non-fatal cardiovascular events, as well as the number of hospitalization days, in high-risk individuals undergoing SCP, regardless of age or sex (5–8). Its use is recommended with a Class I, Level A indication (7).
The effectiveness of aspirin therapy is closely linked to patient adherence. Medication adherence is defined as the extent to which a patient's medication-taking behavior corresponds with agreed recommendations from a healthcare professional. Despite its importance, only 50% of chronic patients in developed countries adhere to their treatment regimens, with even lower adherence rates reported in developing countries (9). Medication adherence is a multifactorial phenomenon determined by five interrelated domains: patient characteristics, social and family environment, disease characteristics, therapeutic regimen, and healthcare system conditions (10–15). Since the effectiveness of treatment depends not only on daily intake but also on maintaining therapy over time, another concept, persistence, has emerged in the context of medication adherence. Persistence is defined as the period between treatment initiation and the last dose taken before treatment discontinuation, or the proportion of days a patient continues the treatment over a given period (16). It is measured either as the proportion of days covered (PDC) by the medication or as the mean number of days until treatment discontinuation (17). In the case of ASA, a cohort study conducted in the Netherlands showed that the proportion of persistent users dropped from 77.3% after one year of follow-up to 27.5% after ten years (18). Lack of continuity compromises treatment effectiveness, preventing the expected benefits of the medication and increasing the risk of recurrence.
Adherence measurement methods can be classified as direct or indirect. Direct methods, such as directly observed therapy, therapeutic drug monitoring, and ingestible sensor systems, are objective, specific, and highly accurate but are often costly and impractical for routine clinical practice. Indirect methods include patient self-report questionnaires, pill counts, the proportion of days covered (PDC), the medication possession ratio (MPR), and medication event monitoring systems (MEMS), among others (19–21). Among these, self-report questionnaires are widely used due to their simplicity, practicality, and low cost; however, they have notable limitations, including subjectivity, recall bias, and response bias, as the information is provided by the patient. Commonly used questionnaires include the Haynes-Sackett Test, the Morisky-Green Test (22, 23), and the MMA-S 8 questionnaire (17, 24–26), the latter being one of the most commonly employed in clinical practice. Despite its validation in other populations and pathologies (27–29), the MMA-S 8 questionnaire has been used in unvalidated clinical settings, proving unsuitable for certain populations, such as patients with type 2 diabetes in Spain (30). Moreover, the results of the original MMA-S 8 study were recently retracted due to inconsistencies in its sensitivity and specificity values (26).
It is crucial for healthcare professionals to be familiar with validated tools for measuring adherence to ASA, given the severe consequences of non-adherence in chronic diseases such as CVD. Failure to identify non-adherence as the cause of poor disease control may result in a medication being incorrectly deemed ineffective. This can lead to unnecessary treatment intensification, unwarranted diagnostic tests, or even misinterpretation of clinical trial results when medication adherence is unknown (31). The objective of this systematic review was to identify the methods used in research to measure adherence and persistence to ASA in patients undergoing secondary cardiovascular prevention, as well as to assess the validity and accuracy of these methods.
Methods
The protocol for this systematic review was registered in PROSPERO (ID: CRD42023470993). The PRISMA guidelines and checklist (32) were followed to report the methodology and results. This study was approved by the Office of Responsible Research at Miguel Hernández University in Spain (TFG.GME.ALP.ERF.231213).
Eligibility criteria
Studies were eligible for this review if they reported measuring adherence and/or persistence to aspirin treatment in patients undergoing SCP and mentioned the specific measurement method used. Studies that assessed adherence or persistence to ASA alongside other medications were excluded. The study population included individuals aged 18 years or older undergoing SCP for conditions such as ischemic heart disease, acute myocardial infarction, stroke, cerebral hemorrhage, transient ischemic attack, renal failure, heart failure, peripheral artery disease, aortic dissection, or diabetic and hypertensive retinopathy, all treated with ASA. Eligible study designs encompassed observational (cross-sectional, case-control, and cohort) and experimental studies. Excluded were letters, editorials, clinical cases, reviews, opinion articles, conference abstracts, study protocols, and non-scientific studies, as well as those written in a non-Latin alphabet. There were no restrictions on the publication date.
Information sources and search strategy
The search was conducted in three databases: EMBASE, MEDLINE, and Scopus. All studies published from the inception of each database up to October 30, 2023, were included. No additional searches were performed.
The search strategy included key terms such as “Treatment Adherence and Compliance”, “Medication Adherence”, “Aspirin”, “Cardiovascular Diseases”, and “Acute Coronary Syndrome”, combining controlled vocabulary and free-text terms with Boolean operators. Filters were applied to restrict the results by study type and population age. Details of the search strategy for each database are provided in Supplementary Material 1.
Selection process
Articles retrieved from the database searches were exported to the Rayyan® platform. Duplicates were manually removed after automatic detection using Rayyan. Subsequently, the selection process was conducted by six independent reviewers, who divided the workload based on study type. Two pairs of reviewers screened the titles and abstracts of observational studies and experimental studies, respectively, during the first selection round. In the second round, the same pairs independently assessed the eligibility of the studies included in the first round by reviewing the full texts. Any discrepancies or conflicts in both rounds were resolved by a third reviewer assigned to each group. The reviewers responsible for study selection included researchers with experience in systematic reviews and expertise in cardiovascular prevention and adherence research, as well as two supervised student researcher. For studies without free full-text access, interlibrary loan requests were submitted to Miguel Hernández University. Studies that could not be retrieved were excluded.
Data extraction process
Data extraction from the finally included articles was performed by two researchers, with another researcher reviewing the extracted data for accuracy. The reviewers responsible for data extraction included researchers with experience in systematic reviews and expertise in cardiovascular prevention and adherence research. The extracted information included the principal author, year of publication, study location, study design, study population, and whether adherence, persistence, or both were measured. Adherence was defined as the extent to which a patient's medication-taking behavior corresponds with the prescribed dosage regimen, while persistence was defined as the duration of continuous medication use without interruption. These definitions follow the ABC taxonomy framework (16). Additional extracted data included sample size, study setting, methods used to measure adherence or persistence (type and description), criteria for classifying patients as adherent/persistent or non-adherent/non-persistent, validity indicators of the measurement methods (if available), and psychometric properties of the questionnaires (if available). Validity indicators were considered classical measures of method accuracy, such as sensitivity, specificity, positive predictive value, and negative predictive value. For self-report questionnaires, psychometric properties (e.g., internal consistency assessed through Cronbach's alpha, test–retest reliability, and construct validity) were extracted separately, recognizing their conceptual distinction from classical validity indicators.
Synthesis of results
A descriptive synthesis of the characteristics of the included studies was performed. Additionally, a narrative synthesis was conducted to describe separately the methods used to measure adherence and persistence, including a tabulation of the validity indicators for methods validated specifically for ASA and the psychometric properties of the questionnaires used. Due to the scarcity of studies providing validity indicators for measuring adherence and persistence to ASA, a meta-analysis could not be performed.
Risk of bias assessment
A formal risk of bias (RoB) assessment was not conducted for all included studies, as the primary objective of this systematic review was not to evaluate the effectiveness of interventions or the magnitude of adherence or persistence outcomes (which was the main objective of most included studies), but rather to identify and describe the methods used to measure adherence and persistence to aspirin (regardless of the studies’ primary aims) and to collect available information on their validation. In the majority of included studies, adherence or persistence was reported as a secondary outcome or a descriptive measure, and the studies did not aim to critically assess or validate the measurement tools used. In such cases, applying traditional RoB tools would primarily reflect the quality of the main research objective (e.g., intervention effectiveness, adherence or persistence outcome), not the reliability of the measurement method itself, which is not the focus of this review and may lead to misinterpretation regarding the quality of the adherence (or persistence) measurement methods themselves.
However, a risk of bias assessment was conducted for the subset of studies whose primary objective was to validate or evaluate a method for measuring adherence or persistence to aspirin, particularly those employing direct measurement approaches, such as platelet function tests or biochemical assays. In these cases, the quality of the study is directly relevant to the reliability of the reported validation indicators. The QUADAS-2 tool was used for diagnostic accuracy studies, and the COSMIN Risk of Bias checklist was applied to studies evaluating the psychometric properties of questionnaires.
Results
A total of 2,290 articles were identified through the search, and 1,925 titles and abstracts were screened after duplicate removal. Subsequently, the full texts of 123 studies were evaluated, resulting in the inclusion of 40 articles in the review. The main reason for exclusion was the absence of adherence (or persistence) measurements for ASA. Figure 1 presents the PRISMA flow diagram (32), which details the study selection process throughout the systematic review. Two studies by García Rodríguez et al. (33, 34), included in this review, were conducted with different objectives but focused on the same population. Both studies employed the same method to measure persistence and applied identical criteria to define non-persistence. As a result, they were combined and treated as a single outcome, with only one method extracted instead of two.
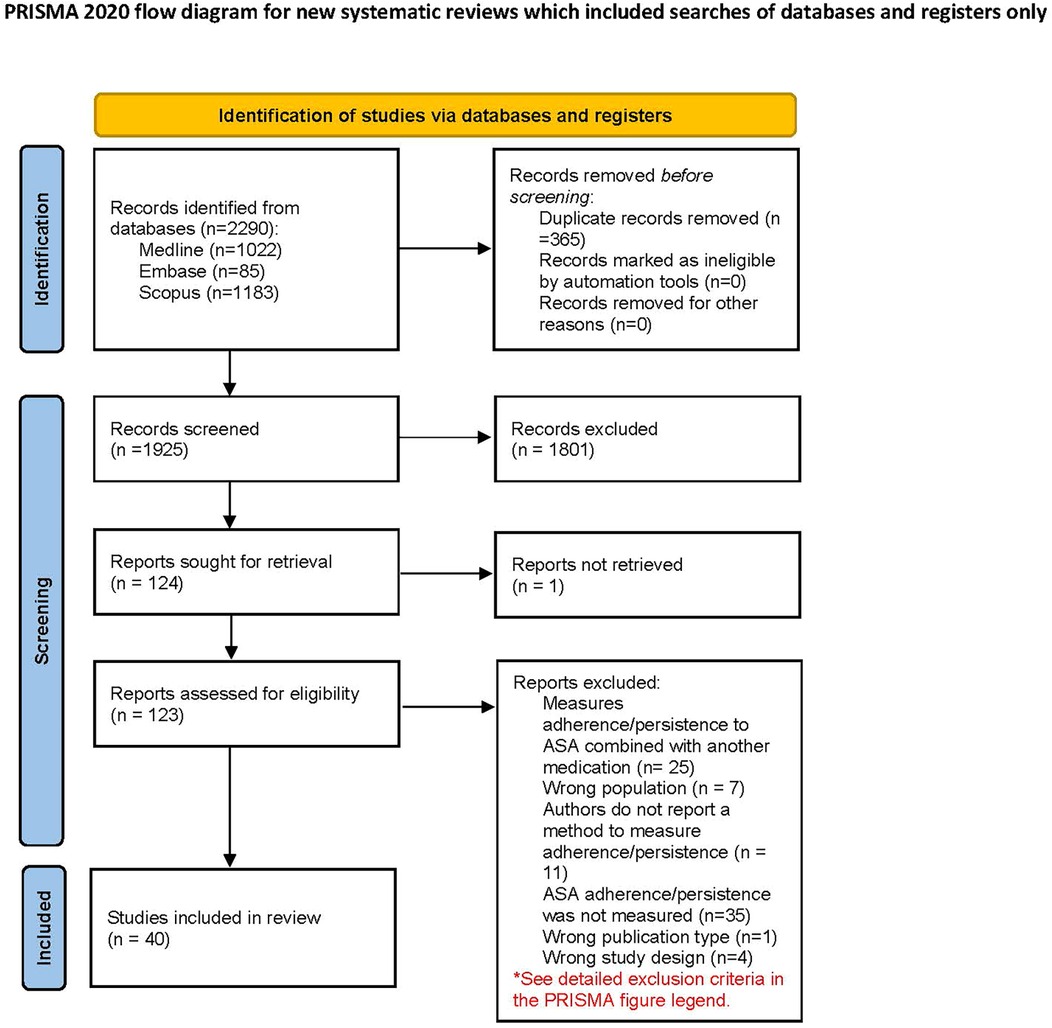
Figure 1. PRISMA flow diagram. *Reasons for exclusion included: combining ASA adherence with other medications (e.g., dual antiplatelet therapy), studies focused on non-SCP populations (e.g., primary prevention or non-cardiovascular conditions), lack of adherence measurement or unclear methodology (e.g., adherence mentioned but not described), and studies with designs not meeting inclusion criteria (e.g., case reports, narrative reviews). Adapted with permission from “PRISMA 2020 flow diagram template for systematic reviews” by Page et al., licensed under CC BY 4.0.
Characteristics of included studies
Table 1 shows the characteristics of the included articles, which were published between 2002 and 2023. Most of the studies were conducted in the United States (n = 15), followed by the United Kingdom (n = 4) and China (n = 3). Regarding study types, the majority were cohort studies (n = 22), followed by experimental studies (n = 13) and cross-sectional studies (n = 3). Sample sizes varied widely, ranging from 14 to 335,624 participants. Concerning the study setting, most were conducted in hospital settings (n = 15), while others were carried out in hospital-based outpatient follow-up settings (n = 9), outpatient-only settings (n = 8), and clinical research centers (n = 6). A large proportion of the articles (72.5%) focused on adherence (n = 29), whereas fewer studies measured persistence (5%, n = 2) or both adherence and persistence (22.5%, n = 9).
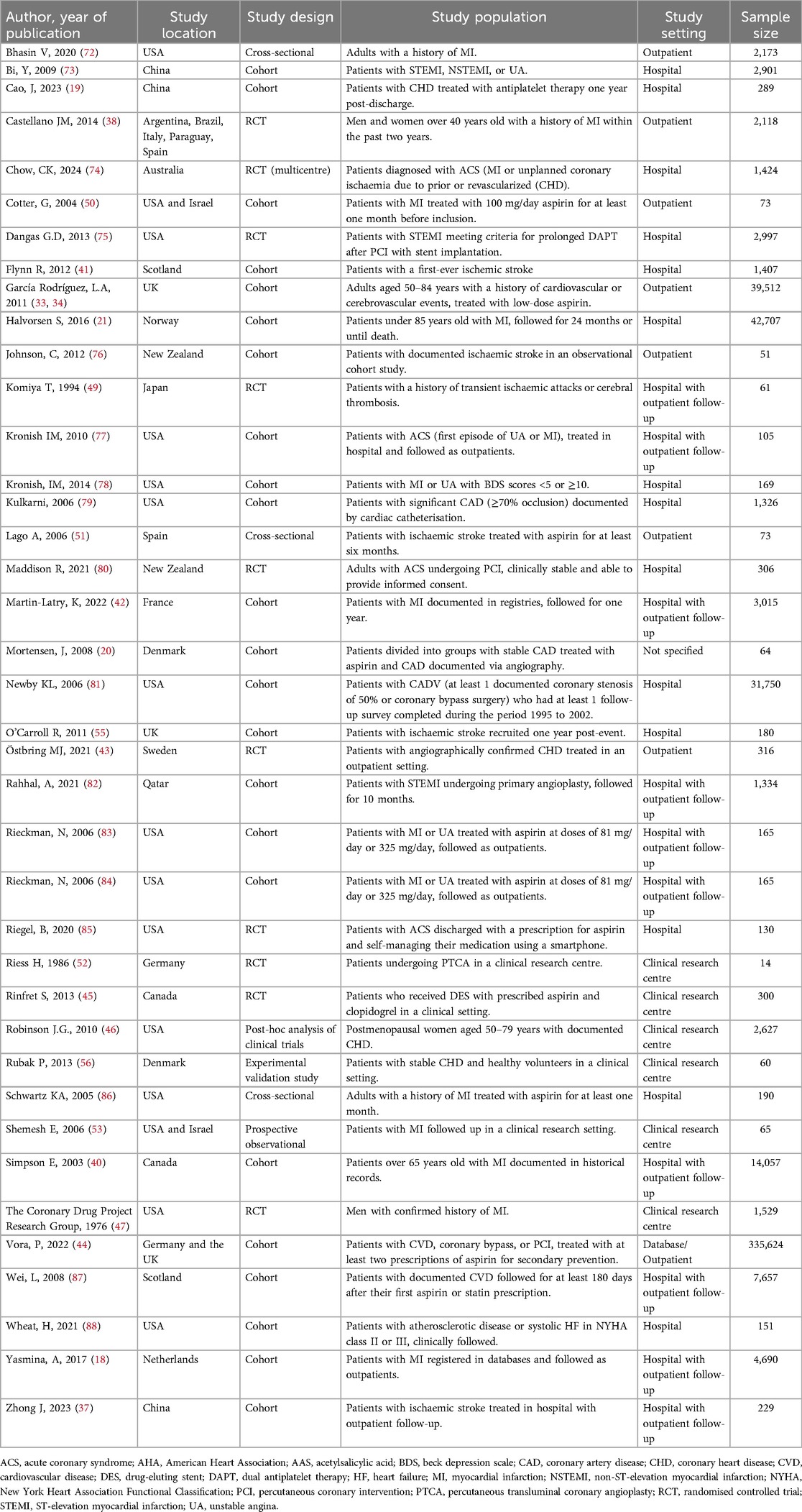
Table 1. Descriptive characteristics of included studies (n = 40).
Measurement methods identified
Indirect methods
Measurement of adherence
Table 2 shows the methods used to measure adherence to ASA in the reviewed studies, including definitions of adherent patients and validation information, if available. These methods, listed in descending order of frequency, included self-report tools (n = 18), medication dispensing records (n = 13), direct methods (n = 10) involving blood-based platelet function tests (n = 7) or ASA/metabolite detection (n = 3), MEMS (n = 6), and pill count methods (n = 7). Figure 2 illustrates the percentage of studies using each type and subtype of methods classified for measuring adherence to aspirin. The following sections describe each type of method in detail.
1. Self-report methods
• Direct patient-reported adherence assessment via medication recall and confirmation (in person or by phone): Patients were asked to list their medications. If their answers matched the prescribed medications at discharge, they were considered adherent. Alternatively, they were directly asked whether they were taking their medications as instructed.
• Morisky 8-item Adherence Scale (MMAS-8) (26): This scale consists of eight items, with a total score ranging from 0 to 8, where lower scores indicate higher adherence.
• Morisky 4-item Adherence Scale (MMAS-4, MAQ) (35): This scale consists of four items, with a total score ranging from 0 to 4, where lower scores indicate higher adherence.
• Medication Adherence Report Scale (MARS) (36): This is a five-item scale rated on a five-point scale from 1 (“very often”) to 5 (“never”). The total score ranges from 5 to 25, with higher scores indicating better adherence.
• Pill count via self-report (37): Patients were considered adherent if they took 100% of their prescribed pills. Partial adherence was defined as taking more than 75% but less than 100%, while severe non-adherence was defined as taking 75% or fewer of the prescribed pills.
2. Pill count methods
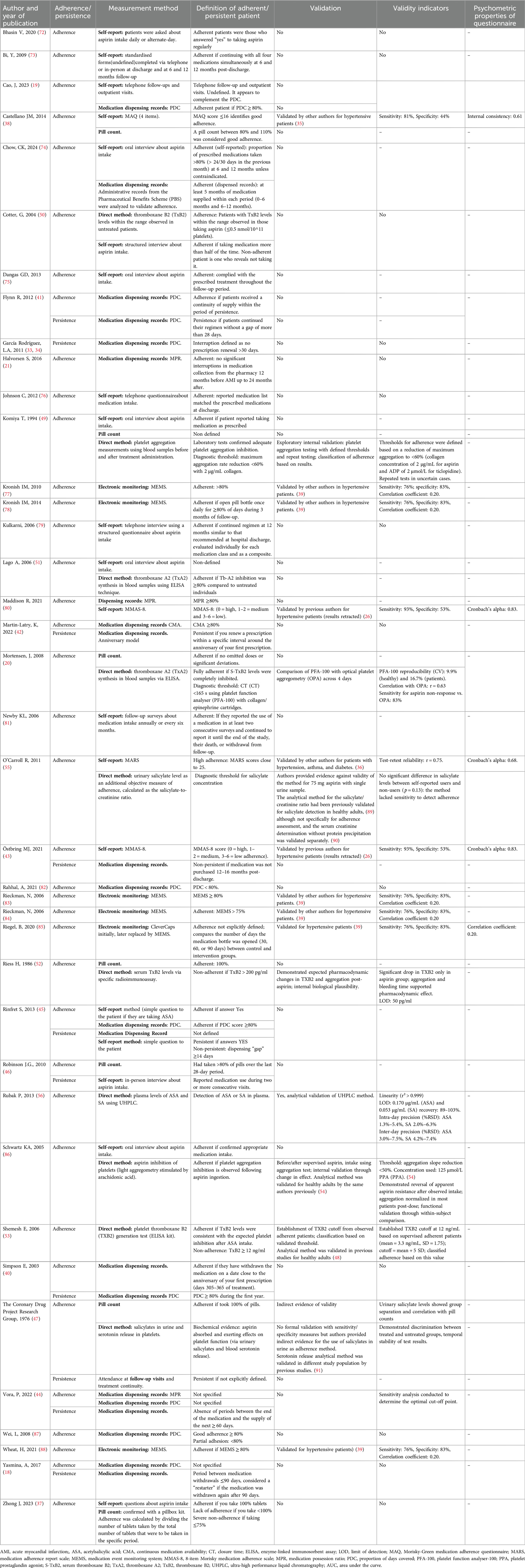
Table 2. Methods reported by studies for measuring adherence and/or persistence (n = 40).
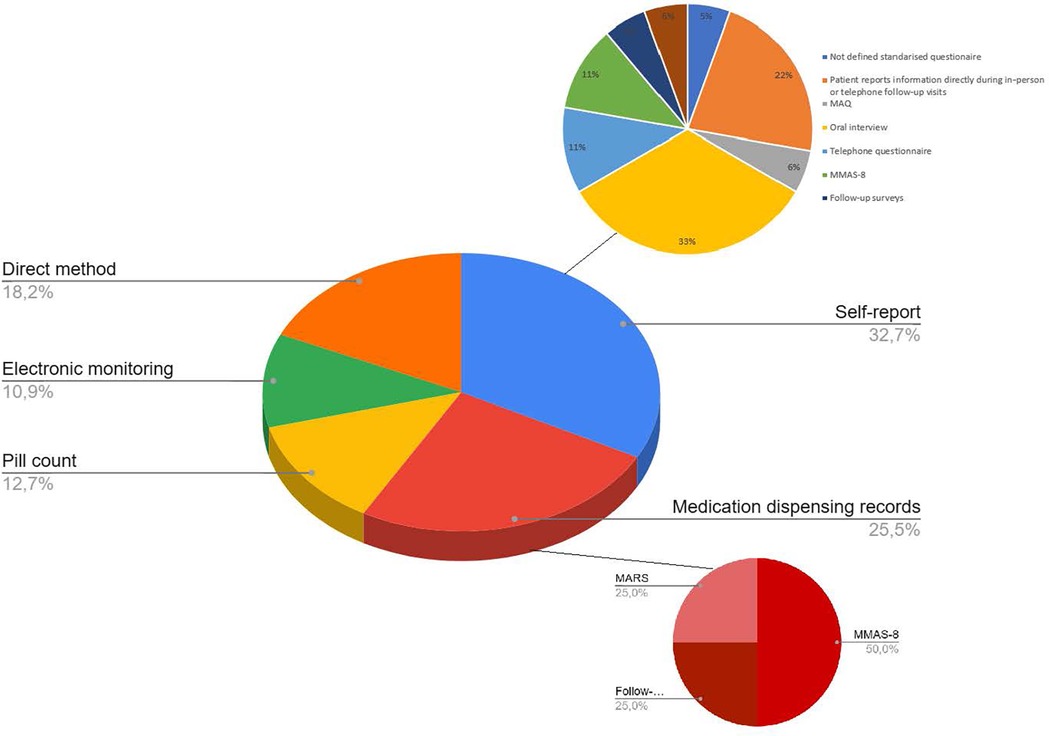
Figure 2. Pie chart illustrating the proportional distribution of aspirin adherence measurement methods reported in this review. MARS, Medication Adherence Rating Scale; MAQ, Medication Adherence Questionnaire; MMAS, Morisky Medication Adherence Scale.
In addition to self-reported pill counts, some studies employed pill count methods performed by healthcare professionals. Two studies (20, 38) defined patients as adherent if the pill count indicated they followed the prescribed ASA regimen without missed doses or significant deviations. In one of these studies (38), adherence was further defined as pill counts ranging from 80% to 110% of the prescribed doses.
3. Medication dispensing records
Among dispensing record methods, PDC (n = 8), MPR (n = 3), continuous multiple-interval measure of medication availability (n = 1) (CMA) were the most utilized metrics, with adherence thresholds generally set at PDC, MPR or CMA ≥ 80%. The anniversary model was also used (n = 1)
4. Electronic monitoring methods
Several studies employed electronic devices to measure adherence to ASA. Typically, patients were considered adherent if they took at least 80% of the prescribed doses during the monitoring period. The devices used included: MEMS or Clever Caps (39). These devices electronically record each time the medication container is opened, providing accurate data on the frequency and timing of medication access.
Measurement of persistence
Table 2 shows the methods used to assess persistence with ASA in the reviewed studies. Persistence was evaluated using various indirect methods, with medication dispensing records being the most frequently employed approach, used in 70% (n = 7) of studies. Within this category, methods such as the PDC, the Anniversary Model, and Defined Gap Periods were commonly utilised. Self-report methods were less common, appearing in 30% (n = 2) of studies, and typically relied on patient interviews or follow-up visit attendance to determine persistence (n = 1). Figure 3 illustrates the percentage distribution of studies by the methods used to measure ASA persistence, highlighting the predominance of dispensing record-based approaches. The following sections describe each method in detail.
1. Medication dispensing records
• PDC Record: One study (40) defined persistence as a PDC of 80% or higher during a one-year follow-up period. Other studies (33, 34) defined persistence based on dispensing interruptions, considering patients non-persistent if the gap exceeded 30 days. Another study (41) defined persistent patients if they continued their regimen without a gap of more than 28 days.
• Anniversary model (42): Patients were classified as persistent if they dispenseded their prescription within a specific time frame surrounding the anniversary of their first prescription.
• Defined gap periods (18, 43, 44): Persistence was measured by the absence of dispensing interruptions within specific periods, ranging from 60 to 90 days or within 12–16 months post-discharge.
2. Self-reported methods
• Self-report interview (45, 46): Patients confirmed that they were taking their medication as prescribed.
3. Indirect follow-up or monitoring method
• Follow-up visits and treatment continuity (47): Patients who attended follow-up visits and continued their treatment were considered persistent.
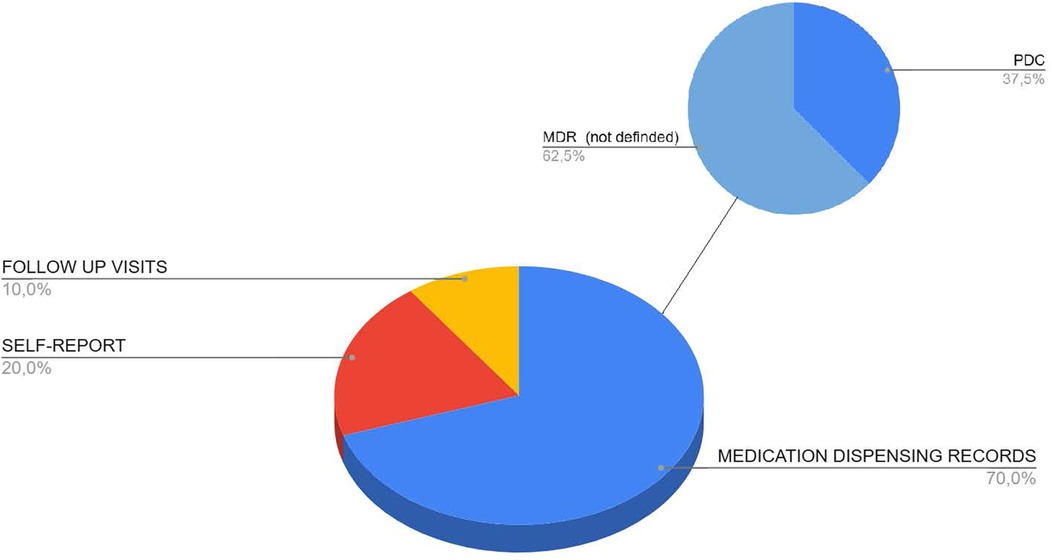
Figure 3. Pie chart illustrating the proportional distribution of aspirin persistence measurement methods reported in this review. MDR, Medication Dispensing Records; PDC, Proportion of Days Covered.
Direct methods
Measurement of adherence
Several reviewed studies employed direct methods to assess adherence to ASA, focusing on its best-characterised effect: the irreversible inhibition of cyclooxygenase-1 (COX-1) in platelets, which reduces thromboxane A2 synthesis (48). These methods included:
• Platelet aggregation tests using ADP and collagen as agonists (20, 49): Patients were considered adherent if they demonstrated a sufficient reduction in platelet aggregation (typically below 60%).
• Thromboxane B2 (TxB2) measurement (50–53): serves as a biomarker for the inhibition of thromboxane A2 synthesis. In patients who are adherent to treatment, low levels of TxB2 in plasma indicate effective inhibition of platelet aggregation.
• Platelet Function Analyzer-100 (PFA-100) (20): This device measures primary hemostatic function by assessing closure time (CT) in whole blood. Patients with adhesion disorders typically exhibit low CT values (below 165 s).
Other tests included optical aggregation tests for arachidonic acid and ADP responses, where adherence was indicated by aggregation responses below specific thresholds (20, 54). Three studies utilised urine (47, 55) or plasma (56) tests to detect ASA or its metabolites. With regard to studies measuring the presence of AAS metabolites in urine, one study (47) complemented the detection of urinary salicylates with blood analysis to evaluate serotonin release by platelets when stimulated with epinephrine. Aspirin impacts this function by inhibiting thromboxane A2 synthesis in platelets, thereby impairing their ability to respond to such stimulation. Another study (55) assessed salicylic acid levels adjusted for creatinine in urine samples to account for urinary volume. The only study (56) measuring plasma concentrations of ASA and SA employed ultra-high-performance liquid chromatography (UHPLC).
Validity indicators
None of the indirect methods used to measure adherence in the studies included in this review reported validity indicators specific to ASA adherence. Some methods, such as MEMS (39), the MMAS-8 (26) questionnaire (retracted), and the MMAS-4 (35), have validity indicators reported by previous authors, but these are for measuring adherence to other medications and in different populations. Table 2 presents the psychometric properties of these tools as reported in prior studies.
All direct methods are considered valid as they rely on established and validated analytical techniques to measure biological or chemical markers of ASA adherence. However, while some studies explicitly report validation data for the tests they employ, others do not provide this information. This inconsistency highlights the need for transparency in reporting validation processes to ensure reproducibility and reliability.
The methods used to measure ASA persistence lacked a formal validation process to ensure accuracy and consistency across different contexts. However, some authors conducted sensitivity analyses to justify the cut-off points for persistence, as seen in the study by Vora et al. (44), the sensitivity analysis confirmed that a 60-day cut-off for persistence and MPR calculations provided consistent estimates across different scenarios.
Additional tools related to adherence prediction
Although not a method for measuring adherence or persistence, one study¹⁹ developed a nomogram designed to predict the risk of non-adherence to antiplatelet therapy in patients with congenital heart disease one year after discharge. The nomogram did not directly measure medication intake but instead predicted the likelihood of non-adherence based on patient behavior and clinical factors, using PDC as the gold standard for classification. Since this tool predicts the risk of non-adherence rather than measuring adherence behavior, it has been presented separately from the methods used to assess adherence or persistence. It represents a complementary approach focused on early identification of patients at high risk of non-adherence to guide preventive interventions.
Risk of bias assessment
A risk of bias assessment was conducted for eight studies that provided empirical indicators of validity for methods used to assess adherence to aspirin, all of which involved direct measurement approaches such as platelet function tests or biochemical assays. The results of the RoB assessment, according to QUADAS-2 tool, are summarized in Table 3. Most studies were rated as having low risk of bias across all assessed domains. However, O'Carroll et al. (55) showed high risk in the index test and reference standard domains, due to the use of self-report as a comparator and the application of a urinary biomarker that failed to discriminate adherent from non-adherent patients. Shemesh et al. (53) was rated as moderate risk in patient selection due to limited information on recruitment methods. In several cases, the reference standard domain was marked as “not applicable”, as no external comparator was used.
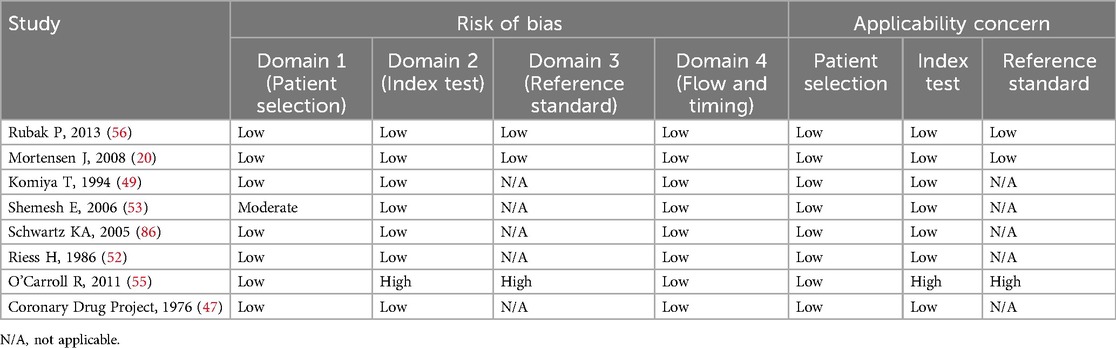
Table 3. Risk of bias and applicability concerns assessed using the QUADAS-2 tool in studies reporting validity indicators of adherence measurement methods (n = 8).
It should be acknowledged that only five of the included studies (20, 47, 53, 56) were specifically designed to validate aspirin adherence methods, using approaches such as comparison with established reference standards (e.g., UHPLC, PFA-100, or direct observation) or by defining biological cut-off points. The remaining three studies (49, 52, 55) were not designed as validation studies, although some provided indirect evidence on the usefulness or limitations of the methods applied, for example, O'Carroll et al. (55) found that urinary salicylate levels did not effectively distinguish between adherent and non-adherent patients.
Discussion
The results of this systematic review show that the methods used to measure adherence to ASA in SCP populations are primarily indirect. These methods include self-report techniques, such as questionnaires like MMAS-8 (26), MMAS-4 (35), and MARS (36), as well as standardised telephone or in-person surveys and self-report forms. Prescription and medication supply record reviews, mainly PDC and MPR, are also widely used, alongside electronic monitoring (e.g., MEMS), pill count methods, and direct methods measuring platelet activity or ASA/metabolite detection in blood or urine. In terms of persistence, most studies relied on medication dispensing records, particularly PDC and the anniversary model. Regarding the validity indicators of the methods used, none of the indirect methods had specific validation for measuring ASA adherence (or persistence).
Terminology
Terminology related to adherence and persistence is inconsistently used in the literature. Therefore, this review considered the terminology used in different studies (“adherence” or “persistence”) regardless of whether it strictly followed the definitions (57). Many studies use these terms interchangeably, even though adherence refers to the proportion of prescribed doses taken, while persistence refers to the continuous use of treatment without interruption. Additionally, terms like “compliance” and “concordance” have been used to define various aspects of medication use. However, “compliance” often carries a negative connotation of subordination to the prescriber (58, 59), and “concordance” is frequently misunderstood as synonymous with compliance (60–62). These inconsistencies hinder cross-study comparisons and make it difficult to draw definitive conclusions about the effectiveness of interventions aimed at improving adherence. Standardising terminology and measurement methods is essential to improve comparability and support evidence-based decision-making.
Indirect methods
Dispensing records are among the most widely used approaches for evaluating adherence and persistence. The most frequently used methods are PDC, followed by MPR and the anniversary model, with their evaluation often subject to the interpretation of study authors. PDC calculates the percentage of days a patient has the medication available during a given period, excluding oversupply from early dispensations. This metric is robust and widely accepted due to its consistency and positive association with clinical outcomes (63). In contrast, MPR calculates the proportion of time a patient has medication available but can exceed 100%, indicating oversupply. The main limitation of these methods is that they do not confirm whether the patient actually takes the medication. In this regard, Cao et al.'s predictive nomogram (19) demonstrates how these limitations can be overcome by integrating multiple clinical and social risk factors, allowing not only the measurement of adherence using PDC but also the prediction of the risk of non-adherence. This highlights the importance of combining quantitative metrics with predictive tools to design proactive intervention strategies aimed at evaluating and improving actual treatment adherence. Persistence is generally measured through dispensing records, particularly the PDC. Although PDC provides a general idea of adherence, it is not ideal for measuring persistence, as it does not guarantee continuous treatment without interruptions. Some studies have adapted PDC to measure persistence using interruption criteria (≥30, ≥60, or ≥90 days).
Self-report methods are simple and practical tools for evaluating adherence from the patient's perspective. However, their validity may be affected by recall bias or social desirability (64). The MMAS-8 (26) and its previous version, MMAS-4 (35), are among the most widely used questionnaires for chronic diseases, although they were originally developed and validated specifically for patients with hypertension. These questionnaires have been studied in numerous populations and contexts, yielding varied psychometric results. In some studies, the MMAS-8 has demonstrated good validity and reliability (27, 29), while in others, its internal consistency and predictive capacity have been limited (30), suggesting that its accuracy may depend on the context and specific population. Notably, the original Morisky study, which developed and validated the MMAS-8, has been retracted, raising questions about the instrument's validity and the integrity of its psychometric properties (26). This retraction, combined with the variability in performance across different patient populations, highlights significant limitations in the use of the MMAS-8 (26) and MMAS-4 (35) as adherence measurement tools. In light of these issues, alternative self-report instruments with stronger psychometric support, such as the MARS (36), should be considered. The MARS has demonstrated more consistent reliability and validity across various clinical contexts and has not been affected by concerns of scientific misconduct. Future research efforts should prioritize the use and further validation of such tools to ensure more accurate and trustworthy adherence assessments.
Telephone or in-person questionnaires are considered practical tools for assessing adherence. The direct patient-reported adherence assessment via medication recall and confirmation, in person or by phone, where patients are asked to list their medications and are considered adherent if their answers match the prescribed medications at discharge or are directly asked whether they are taking their medications as instructed, is widely used among the self-reported methods. However, their validity can be limited by reliance on patient honesty and accuracy, introducing potential information bias that could affect the accuracy of adherence measurements. Pill count through self-report is an indirect method used in some adherence studies, although its application in ASA evaluation is limited. It involves counting leftover pills in a container to infer adherence. While it is cost-effective, its validity is limited as it does not guarantee that the patient has taken the recorded doses.
Electronic monitoring devices like MEMS are regarded as a reference method for evaluating adherence, as they provide a detailed record of patient behavior. However, their validity is limited because they do not confirm whether the patient actually ingests the medication after opening the container. While they are useful approximations, they have significant limitations and are not recommended as the sole reference for assessing adherence (65).
Direct methods
Unlike other drugs, such as statins, where their concentration or that of their metabolites is measured in plasma or urine, (66) in the case of aspirin, due to its short half-life, direct methods instead evaluate its pharmacodynamic effect: the irreversible inhibition of platelet cyclooxygenase-1, which in turn inhibits thromboxane A2 synthesis. These methods aim to capture the functional consequences of this mechanism, including optical platelet aggregation tests, plasma thromboxane B2 (TxB2) measurement, PFA-100 tests, ADP and collagen-induced aggregation, and serotonin release induced by epinephrine in platelets (48). They offer an objective and personalised assessment of treatment effectiveness, helping to identify individual responses and detect adherence or resistance issues. However, most direct methods require invasive biological samples, which limits their routine clinical applicability. Moreover, costs and availability restrict their large-scale use outside of research or specific clinical settings.
Measurements of platelet aggregation effects in ASA-treated patients present various limitations, such as strict adherence thresholds that may misclassify patients. Biological variability, aspirin resistance, concurrent medications, health conditions, and irregular aspirin intake can all affect the results, complicating interpretation (20, 49, 67, 68). Cotter et al.'s study (50) suggests that many cases classified as biologically resistant to aspirin are actually due to non-adherence, highlighting the importance of assessing adherence before assuming biological resistance.
Three reviewed studies (47, 55, 56) utilised urine or plasma ASA/metabolite detection. One study (47) complemented salicylate detection with epinephrine-induced platelet serotonin release to assess platelet function. Urinary salicylate levels reflect recent aspirin intake but have limitations due to the short half-life of salicylates (69). Platelet function tests, however, provide a more enduring indicator of aspirin's therapeutic effect. In another study (55), salicylic acid levels adjusted for creatinine were measured in urine samples to control for urine volume. This method was ineffective at distinguishing between patients taking aspirin and those not taking it, likely due to aspirin's short half-life and low doses (75 mg). The only study (56) measuring plasma ASA and SA concentrations using UHPLC concluded that SA is a more sensitive marker due to its stability and longer half-life, but it also presents limitations, such as high interindividual variability and the risk of becoming undetectable after 24 hours at low doses.
Strengths and limitations of direct vs. indirect methods
Although both direct and indirect methods have been used to measure adherence, their applicability varies significantly depending on the context. Direct methods, such as platelet function tests and thromboxane B2 assays, offer objective measures of aspirin intake (adherence) but are costly, invasive, and require specialized laboratory infrastructure, limiting their use to research settings or specialized clinics. In contrast, indirect methods, such as dispensing records and self-reports, are used to assess both adherence and persistence, and are more feasible and widely adopted in routine clinical practice and large-scale studies, despite their susceptibility to information and recall bias. In settings with integrated electronic health systems, such as the United States, dispensing records are the predominant method due to their accessibility and linkage to clinical outcomes. In outpatient and resource-limited contexts, self-report questionnaires remain more common due to their low cost and ease of administration. Thus, the choice of measurement method is strongly influenced by feasibility, available infrastructure, and the specific objectives of each study.
Despite their widespread use, indirect methods such as dispensing records and self-reports have not been specifically validated for measuring adherence or persistence to aspirin, reflecting both pharmacological and methodological challenges. Ideally, validation would involve comparison against a gold standard such as the direct measurement of drug or metabolite levels. However, aspirin's short half-life, rapid metabolism into salicylate, and fast elimination, especially at low doses, make biochemical detection unreliable. Moreover, the pharmacodynamic effect of aspirin persists longer than its biochemical detectability, complicating direct validation. Although electronic monitoring systems (e.g., MEMS) could offer an alternative objective reference, no studies have systematically validated dispensing records for aspirin adherence using such technologies. This gap highlights the need for standardized validation protocols that combine dispensing data with objective measurements adapted to aspirin's pharmacological properties.
Validation gaps and methodological challenges
Although the number of studies providing validation data for adherence measurement methods was limited, the overall risk of bias among these studies was low. Most studies employed direct measurement techniques and were judged to have low risk of bias across the main QUADAS-2 domains. However, some concerns emerged, particularly regarding the absence of an independent reference standard in several studies and a high risk of bias in one study using a non-validated biomarker. These limitations highlight the need for more methodologically robust validation studies that include appropriate comparators and standardized evaluation criteria.
This study highlights the lack of validated ASA adherence measurement methods for SCP, emphasizing the urgent need to develop clinically applicable tools that incorporate gender perspectives. Although gender is a known independent predictor of non-adherence (70), most studies overlook gender disparities in adherence measurement. For example, women are 25% less likely to adhere to combined medication regimens after a myocardial infarction compared to men (71). Despite the critical influence of gender on adherence behaviors, none of the adherence measurement methods identified in this review explicitly accounted for gender differences in their design, validation, or application.
Current indirect methods, such as dispensing records and self-report questionnaires, typically fail to capture gender-specific barriers, including caregiving responsibilities, differential access to healthcare, and variations in perceptions of medication necessity. To improve the accuracy and equity of adherence measurement, future development of ASA adherence tools should combine dispensing records, self-reports, and direct methods, validated through comprehensive psychometric testing and explicitly incorporating gender-sensitive items and analytical strategies.
Proposed characteristics for optimal adherence and persistence assessment methods
To improve clinical management, methods for assessing adherence and persistence should meet several key criteria. They should be valid and reliable, ideally demonstrating high sensitivity and specificity to accurately distinguish between adherent and non-adherent patients. Feasibility is also essential: methods should be non-invasive, cost-effective, and easily applicable in routine clinical settings without imposing a significant burden on patients or healthcare providers. Additionally, they should be capable of assessing both adherence (execution of dosing) and persistence (continuation of therapy over time) separately, to provide a comprehensive picture of medication-taking behaviors.
Moreover, optimal methods should incorporate a patient-centered approach, considering individual barriers to adherence, including those related to gender, socioeconomic status, and healthcare access. Tools combining multiple data sources, such as pharmacy records, electronic monitoring, and validated self-report questionnaires, would offer a more accurate and holistic assessment. The development of predictive tools, capable of identifying patients at high risk of non-adherence before clinical deterioration occurs, should also be prioritized. These features would enhance the ability to implement timely and tailored interventions, ultimately improving treatment outcomes in secondary cardiovascular prevention.
Study limitations
This systematic review has some limitations. We restricted the search to studies published in languages using Latin alphabets, which likely had a minimal impact on the findings, as the majority of relevant studies were published in English. Additionally, the search was conducted in three major databases (EMBASE, MEDLINE, and Scopus), and grey literature as well as studies indexed exclusively in other sources were not included. Consequently, there is a possibility that some relevant studies may have been missed, although we believe this risk is limited given the broad coverage of the selected databases. Lastly, two of the reviewers involved in study selection were student researchers; however, their work was conducted under the supervision of experienced researchers, and all screenings were performed independently and verified through conflict resolution procedures to ensure the accuracy and consistency of the selection process.
Conclusions
The methods used to measure adherence to ASA in secondary cardiovascular prevention were primarily indirect, relying on the review of prescription and supply records, self-reporting methods, and electronic monitoring. To a lesser extent, pill count methods and direct approaches, such as blood-based platelet function tests—specifically platelet aggregation—were also employed. For measuring persistence, the methods utilised were based on medication dispensing records. Most indirect methods lacked specific validation indicators for measuring adherence to aspirin, highlighting the need for standardization and validation efforts tailored to this context.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
RN-G: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review & editing. ER-F: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AL-P: Conceptualization, Data curation, Project administration, Writing – original draft, Writing – review & editing. AE-A: Funding acquisition, Investigation, Resources, Writing – original draft, Writing – review & editing. ÁC-S: Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. MM-M: Investigation, Supervision, Validation, Writing – original draft, Writing – review & editing. AFCR: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. JAQ: Data curation, Project administration, Resources, Software, Visualization, Writing – original draft, Writing – review & editing. CC-M: Formal analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. VG-G: Conceptualization, Funding acquisition, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by the Health Research Projects—Strategic Action in Health (reference: PI20/01304) of the Spanish Fondo de Investigación Sanitaria—Instituto de Salud Carlos III, cofunded by the European Regional Development Fund/European Social Fund: A Way to Make Europe/Investing in Your Future and Spanish Ministry of Science and Innovation (MICINN) and Carlos III Health Institute (ISCIII)/European Regional Development Fund (ERDF), (RICAPPS: RD21/0016/0024). This funding source had no role in the design of the study, its execution and analyses, the interpretation of the data or the decision to submit results.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Generative AI tools were used in the preparation of this manuscript exclusively to enhance the clarity of writing and to assist in the review of the English translation.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1570331/full#supplementary-material
Abbreviations
ASA, acetylsalicylic acid (o Aspirin); CVD, cardiovascular diseases; MARS, medication adherence report scale; MEMS, medication event monitoring systems; MPR, medication possession ratio; PDC, proportion of days covered; SCP, secondary cardiovascular prevention; thromboxane B2, (TxB2); UHPLC, ultra-high-performance liquid chromatography.
References
1. Pan American Health Organization. WHO reveals leading causes of death and disability worldwide: 2000–2019. PAHO (2020). Available at: https://www.paho.org/en/news/9-12-2020-who-reveals-leading-causes-death-and-disability-worldwide-2000-2019 (Accessed April 03, 2025).
2. INE, National Institute of Statistics (INE). Mortality Statistics by Cause of Death. Madrid: INE (2023). Available at: https://www.ine.es/dyngs/Prensa/pEDCM2023.htm (Accessed January 20, 2025).
3. Rodriguez Artalejo F, Del Rey Calero J. Secondary prevention of cardiovascular disease is a priority but remains insufficient. Rev Esp Salud Publica. (1999) 73(4):441–3. https://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-5727199900040000110575932
4. Cañivano Petreñas L, García Yubero C. Aspirin resistance: prevalence, mechanisms of action, and association with thromboembolic events. A narrative review. Farm Hosp. (2010) 34(1):32–43. doi: 10.1016/j.farma.2009.08.002
5. Antiplatelet Trialists' Collaboration. Collaborative overview of randomised trials of antiplatelet therapy: prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Br Med J. (1994) 308(6921):81–106. doi: 10.1136/bmj.308.6921.81
6. Antithrombotic Trialists’ (ATT) Collaboration, Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. (2009) 373(9678):1849–60. doi: 10.1016/S0140-6736(09)60503-1
7. Orozco-Beltrán D, Brotons Cuixart C, Banegas Banegas JR, Gil Guillén VF, Cebrián Cuenca AM, Martín Rioboó E, et al. Recomendaciones preventivas cardiovasculares. Actualización PAPPS 2022. Aten Primaria. (2022) 54:102444. doi: 10.1016/j.aprim.2022.102444
8. Edney P, Jackson P, Burrell B, Lawton N, Leigh N, Lindsay McLellan P, et al. Secondary prevention of vascular disease by prolonged antiplatelet treatment. Br Med J (Clin Res Ed). (1988) 296(6618):320. doi: 10.1136/bmj.296.6618.320
9. World Health Organization. World health statistics 2023: monitoring health for the SDGs, Sustainable Development Goals. Geneva: World Health Organization (2023). Available at: https://cdn.who.int/media/docs/default-source/gho-documents/world-health-statistic-reports/2023/world-health-statistics-2023_20230519_.pdf (Accessed April 20, 2025).
10. Dilla T, Valladares A, Lizán L, Sacristán JA. Adherence and therapeutic persistence: causes, consequences, and strategies for improvement. Aten Primaria. (2009) 41(6):342–8. doi: 10.1016/j.aprim.2008.09.031
11. Solera G, Solera J, Tárraga L, Madrona F, Gálvez A, Tárraga P. Evaluation of pharmacist effectiveness in improving therapeutic adherence in patients with type 2 diabetes mellitus: a systematic review and meta-analysis. Med Gen Fam. (2018) 7(2):60–5. doi: 10.24038/mgyf.2018.029
12. Orueta Sánchez R. Strategies to improve therapeutic adherence in chronic conditions. Inf Ter Sist Nac Salud. (2005) 29(2):40–8. https://dialnet.unirioja.es/servlet/articulo?codigo=1217031
13. Conthe P, Márquez Contreras E, Aliaga Pérez A, Barragán García B, Fernández de Cano Martín MN, González Jurado M, et al. Treatment compliance in chronic illness: current situation and future perspectives. Rev Clin Esp (Barc). (2014) 214(6):336–44. doi: 10.1016/j.rce.2014.03.008
14. Gagnon MD, Waltermaurer E, Martin A, Friedenson C, Gayle E, Hauser DL. Patient beliefs have a greater impact than barriers on medication adherence in a community health center. J Am Board Fam Med. (2017) 30(3):331–6. doi: 10.3122/jabfm.2017.03.160129
15. Yap A, Thirumoorthy T, Kwan YH. Systematic review of the barriers affecting medication adherence in older adults. Geriatr Gerontol Int. (2016) 16(10):1093–101. doi: 10.1111/ggi.12616
16. Vrijens B, De Geest S, Hughes DA, Przemyslaw K, Demonceau J, Ruppar T, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. (2012) 73(5):691–705. doi: 10.1111/j.1365-2125.2012.04167.x
17. Orozco-Beltrán D, Carratalá-Munuera C, Gil-Guillén V. Improving adherence: one of the most effective actions to increase patient survival in secondary prevention. Rev Esp Cardiol Supl. (2015) 15(E):12–8. doi: 10.1016/s1131-3587(16)30004-
18. Yasmina A, de Boer A, Deneer VHM, Souverein PC, Klungel OH. Patterns of antiplatelet drug use after a first myocardial infarction during a 10-year period. Br J Clin Pharmacol. (2017) 83(3):632–41. doi: 10.1111/bcp.13139
19. Cao J, Zhang L, Zhou X. Constructing a prognostic tool for predicting the risk of non-adherence to antiplatelet therapy in discharged patients with coronary heart disease: a retrospective cohort study. PeerJ. (2023) 11:e15876. doi: 10.7717/peerj.15876
20. Mortensen J, Poulsen TS, Grove EL, Refsgaard J, Nielsen HL, Pedersen SB, et al. Monitoring aspirin therapy with the platelet function analyzer-100. Scand J Clin Lab Invest. (2008) 68(8):786–92. doi: 10.1080/00365510802262680
21. Halvorsen S, Jortveit J, Hasvold P, Thuresson M, Øie E. Initiation of and long-term adherence to secondary preventive drugs after acute myocardial infarction. BMC Cardiovasc Disord. (2016) 16(1):115. doi: 10.1186/s12872-016-0283-6
22. Fernández-Lázaro CI, García-González JM, Adams DP, Fernandez-Lazaro D, Mielgo-Ayuso J, Caballero-Garcia A, et al. Adherence to treatment and related factors among patients with chronic conditions in primary care: a cross-sectional study. BMC Fam Pract. (2019) 20(1):132. doi: 10.1186/s12875-019-1019-3
23. World Health Organization. Adherence to Long Term Therapies: Evidence for Action. Geneva: Ginebra (2003).
24. López-Romero LA, Romero-Guevara SL, Parra DI, Rojas-Sánchez LZ. Treatment adherence: concept and measurement. Rev Hacia Promoc Salud. (2016) 21:10. doi: 10.17151/hpsal.2016.21.1.10
25. Pagès-Puigdemont N, Valverde-Merino MI. Methods to measure therapeutic adherence. Ars Pharm. (2018) 59(3):163–72. doi: 10.30827/ars.v59i3.7387
26. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens (Greenwich). (2008) 10(5):348–54. doi: 10.1111/j.1751-7176.2008.07572.x Retraction in: J Clin Hypertens (Greenwich). 2023 Sep;25(9):889. Retraction in: J Clin Hypertens (Greenwich). 2023 Sep;25(9):890.18453793
27. Ali M, Kerr AJ, Lee M, Chan DZL. What is the statin possession ratio cut-off which identifies those at increased risk following acute coronary syndrome (ANZACS-QI 68)? Heart Lung Circ. (2023) 32(4):487–96. doi: 10.1016/j.hlc.2022.11.012
28. Allonen J, Niegarciminen MS, Lokki M, Parkkonen O, Vaara S, Perola M, et al. Mortality rate increases steeply with nonadherence to statin therapy in patients with acute coronary syndrome. Clin Cardiol. (2012) 35(11):E22–7. doi: 10.1002/clc.22056
29. Alsabbagh MW, Eurich D, Lix LM, Wilson TW, Blackburn DF. Does the association between adherence to statin medications and mortality depend on measurement approach? A retrospective cohort study. BMC Med Res Methodol. (2017) 17(1):66. doi: 10.1186/s12874-017-0339-z
30. Martinez-Perez P, Orozco-Beltrán D, Pomares-Gomez F, Hernández-Rizo JL, Borras-Gallen A, Gil-Guillen VF, et al. Validation and psychometric properties of the 8-item morisky medication adherence scale (MMAS-8) in type 2 diabetes patients in Spain. Aten Primaria. (2021) 53(2):101942. doi: 10.1016/j.aprim.2020.09.007
31. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. (2015) 2015:217047. doi: 10.1155/2015/217047
32. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
33. García Rodríguez LA, Cea Soriano L, Hill C, Johansson S. Increased risk of stroke after discontinuation of acetylsalicylic acid. Neurology. (2011) 76(8):740–6. doi: 10.1212/WNL.0b013e31820d62b5
34. Garcia Rodriguez LA, Cea-Soriano L, Martin-Merino E, Johansson S. Discontinuation of low dose aspirin and risk of myocardial infarction: case-control study in UK primary care. Br Med J. (2011) 343(jul19 1):d4094–d4094. doi: 10.1136/bmj.d4094
35. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. (1986) 24(1):67–74. doi: 10.1097/00005650-198601000-00007
37. Zhong J, Gao Y, Huang D, Hu Y, He Q, Diao L, et al. Analysis of antiplatelet therapy adherence in patients with ischemic cerebral stroke. Brain Behav. (2023) 13(5):e2982. doi: 10.1002/brb3.2982
38. Castellano JM, Sanz G, Peñalvo JL, Bansilal S, Fernández-Ortiz A, Alvarez L, et al. A polypill strategy to improve adherence: results from the FOCUS project. J Am Coll Cardiol. (2014) 64(20):2071–82. doi: 10.1016/j.jacc.2014.08.021
39. Hansen RA, Kim MM, Song L, Tu W, Wu J, Murray MD. Comparison of methods to assess medication adherence and classify nonadherence. Ann Pharmacother. (2009) 43(3):413–22. doi: 10.1345/aph.1L496
40. Simpson E, Beck C, Richard H, Eisenberg MJ, Pilote L. Drug prescriptions after acute myocardial infarction: dosage, compliance, and persistence. Am Heart J. (2003) 145(3):438–44. doi: 10.1067/mhj.2003.143
41. Flynn RW, MacDonald TM, Murray GD, MacWalter RS, Doney AS. Persistence, adherence and outcomes with antiplatelet regimens following cerebral infarction in the tayside stroke cohort. Cerebrovasc Dis. (2012) 33(2):190–7. doi: 10.1159/000331933
42. Martin-Latry K, Latry P, Berges C, Coste P, Douard H, Pucheu Y, et al. One-year care pathway after acute myocardial infarction in 2018: prescription, medical care and medication adherence, using a French health insurance reimbursement database. Arch Cardiovasc Dis. (2022) 115(2):78–86. doi: 10.1016/j.acvd.2021.12.003
43. Östbring MJ, Eriksson T, Petersson G, Hellström L. Effects of a pharmaceutical care intervention on clinical outcomes and patient adherence in coronary heart disease: the MIMeRiC randomized controlled trial. BMC Cardiovasc Disord. (2021) 21(1):367. doi: 10.1186/s12872-021-02178-0
44. Vora P, Soriano-Gabarró M, Russell B, Morgan Stewart H. Long-term adherence and persistence to low-dose aspirin for the prevention of cardiovascular disease: a population-based cohort study. Int J Clin Pract. (2022) 2022:7786174. doi: 10.1155/2022/7786174
45. Rinfret S, Rodés-Cabau J, Bagur R, Déry JP, Dorais M, Larose E, et al. Telephone contact to improve adherence to dual antiplatelet therapy after drug-eluting stent implantation. Heart. (2013) 99(8):562–9. doi: 10.1136/heartjnl-2012-303004
46. Robinson JG, Wallace R, Safford MM, Pettinger M, Cochrane B, Ko MG, et al. Another treatment gap: restarting secondary prevention medications: the Women’s Health initiative. J Clin Lipidol. (2010) 4(1):36–45. doi: 10.1016/j.jacl.2009.12.006
47. Aspirin in coronary heart disease. The coronary drug project research group. Circulation. (1980) 62(6 Pt 2):V59–62.7002353
48. Patrono C, Ciabattoni G, Pinca E, Pugliese F, Castrucci G, De Salvo A, et al. Low dose aspirin and inhibition of thromboxane B2 production in healthy subjects. Thromb Res. (1980) 17(3-4):317–27. doi: 10.1016/0049-3848(80)90066-3
49. Komiya T, Kudo M, Urabe T, Mizuno Y. Compliance with antiplatelet therapy in patients with ischemic cerebrovascular disease. Assessment by platelet aggregation testing. Stroke. (1994) 25(12):2337–42. doi: 10.1161/01.str.25.12.2337
50. Cotter G, Shemesh E, Zehavi M, Dinur I, Rudnick A, Milo O, et al. Lack of aspirin effect: aspirin resistance or resistance to taking aspirin? Am Heart J. (2004) 147(2):293–300. doi: 10.1016/j.ahj.2003.07.011
51. Lago A, Tembl JI, Pareja A, Ponz A, Ferrer JM, Vallés J, et al. Adherence to aspirin in secondary prevention of ischemic stroke. Cerebrovascular Diseases. (2006) 21(5–6):353–6. doi: 10.1159/000091542
52. Riess H, Höfling B, von Arnim T, Hiller E. Thromboxane receptor blockade versus cyclooxigenase inhibition: antiplatelet effects in patients. Thromb Res. (1986) 42(2):235–45. doi: 10.1016/0049-3848(86)90299-9
53. Shemesh E, Koren-Michowitz M, Yehuda R, Milo-Cotter O, Murdock E, Vered Z, et al. Symptoms of posttraumatic stress disorder in patients who have had a myocardial infarction. Psychosomatics. (2006) 47(3):231–9. doi: 10.1176/appi.psy.47.3.231
54. Schwartz KA, Schwartz DE, Pittsley RA, Mantz SL, Ens G, Sami A, et al. A new method for measuring inhibition of platelet function by nonsteroidal antiinflammatory drugs. J Lab Clin Med. (2002) 139(4):227–33. doi: 10.1067/mlc.2002.121855
55. O'Carroll R, Whittaker J, Hamilton B, Johnston M, Sudlow C, Dennis M. Predictors of adherence to secondary preventive medication in stroke patients. Ann Behav Med. (2011) 41(3):383–90. doi: 10.1007/s12160-010-9257-6
56. Rubak P, Hardlei TF, Würtz M, Kristensen SD, Hvas AM. Low-dose acetylsalicylic acid therapy monitored with ultra high performance liquid chromatography. Clin Biochem. (2013) 46(12):988–92. doi: 10.1016/j.clinbiochem.2013.04.007
57. Haynes RB, McDonald H, Garg AX, Montague P. Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev. (2002) (2):CD000011. doi: 10.1002/14651858.CD000011 Update in: Cochrane Database Syst Rev. (2005) (4):CD000011.12076376
58. López San Román A. Adhesión al tratamiento, adherencia al tratamiento o cumplimiento del tratamiento? [treatment adhesion, treatment adherence or treatment compliance?]. Rev Clin Esp. (2006) 206(8):414. doi: 10.1157/13090520
59. Haynes RB. A critical review of the “determinants” of patient compliance with therapeutic regimens. In: Sackett DL, Haynes RD, editors. Compliance with Therapeutic Regimens. Baltimore: Johns Hopkins University Press (1979). p. 24–40.
60. Marinker M. From Compliance to Concordance: Achieving Shared Goals in Medicine Taking. London: Royal Pharmaceutical Society; Merck, Sharp, and Dohme (1997).
61. Bissonette JM. Adherence: a concept analysis. J Adv Nurs. (2008) 63(6):634–43. doi: 10.1111/j.1365-2648.2008.04745.x
62. Snowden A, Martin C, Mathers B, Donell A. Concordance: a concept analysis. J Adv Nurs. (2014) 70(1):46–59. doi: 10.1111/jan.12147
63. Raebel MA, Schmittdiel J, Karter AJ, Konieczny JL, Steiner JF. Standardizing terminology and definitions of medication adherence and persistence in research employing electronic databases. Med Care. (2013) 51(8 Suppl 3):S11–21. doi: 10.1097/MLR.0b013e31829b1d2a
64. Sjölander M, Eriksson M, Glader EL. Inequalities in medication adherence to statin treatment after stroke: a nationwide observational study. Eur Stroke J. (2016) 1(2):101–7. doi: 10.1177/2396987316646026
65. Anghel LA, Farcas AM, Oprean RN. An overview of the common methods used to measure treatment adherence. Med Pharm Rep. (2019) 92(2):117–22. doi: 10.15386/mpr-1201
66. Kristiansen O, Vethe NT, Fagerland MW, Bergan S, Munkhaugen J, Husebye E. A novel direct method to determine adherence to atorvastatin therapy in patients with coronary heart disease. Br J Clin Pharmacol. (2019) 85(12):2878–85. doi: 10.1111/bcp.14122
67. Han YL. Aspirin resistance in coronary heart disease: current understandings and strategies. J Transl Int Med. (2016) 4(1):7–10. doi: 10.1515/jtim-2016-0002
68. Mărginean A, Bănescu C, Scridon A, Dobreanu M. Anti-platelet therapy resistance—concept, mechanisms and platelet function tests in intensive care facilities. J Crit Care Med (Targu Mures). (2016) 2(1):6–15. doi: 10.1515/jccm-2015-0021
69. Hutt AJ, Caldwell J, Smith RL. The metabolism of aspirin in man: a population study. Xenobiotica. (1986) 16(3):239–49. doi: 10.3109/00498258609043527
70. Venditti V, Bleve E, Morano S, Filardi T. Gender-related factors in medication adherence for metabolic and cardiovascular health. Metabolites. (2023) 13(10):1087. doi: 10.3390/metabo13101087
71. Soldati S, Di Martino M, Castagno D, Davoli M, Fusco D. In-hospital myocardial infarction and adherence to evidence-based drug therapies: a real-world evaluation. BMJ Open. 2021;11(2):e042878. doi: 10.1136/bmjopen-2020-042878
72. Bhasin V, Mehta A, Skopicki HA, Parikh PB. Predictors of aspirin nonadherence in adults with prior myocardial infarction. Crit Pathw Cardiol. (2020) 19(3):115–8. doi: 10.1097/HPC.0000000000000218
73. Bi Y, Gao R, Patel A, Su S, Gao W, Hu D, et al. Evidence-based medication use among Chinese patients with acute coronary syndromes at the time of hospital discharge and 1 year after hospitalization: results from the clinical pathways for acute coronary syndromes in China (CPACS) study. Am Heart J. (2009) 157(3):509–516.e1. doi: 10.1016/j.ahj.2008.09.026
74. Chow CK, Klimis H, Thiagalingam A, Redfern J, Hillis GS, Brieger D, et al. Text messages to improve medication adherence and secondary prevention after acute coronary syndrome: the TEXTMEDS randomized clinical trial. Circulation. (2022) 145(19):1443–55. doi: 10.1161/CIRCULATIONAHA.121.056161
75. Dangas GD, Claessen BE, Mehran R, Xu K, Stone GW. Stent thrombosis after primary angioplasty for STEMI in relation to non-adherence to dual antiplatelet therapy over time: results of the HORIZONS-AMI trial. EuroIntervention. (2013) 8(9):1033–9. doi: 10.4244/EIJV8I9A159
76. Johnson C, Lane H, Barber PA, Charleston A. Medication compliance in ischaemic stroke patients. Intern Med J. (2012) 42(4):e47–52. doi: 10.1111/j.1445-5994.2010.02209.x
77. Kronish IM, Rieckmann N, Shimbo D, Burg M, Davidson KW. Aspirin adherence, aspirin dosage, and C-reactive protein in the first 3 months after acute coronary syndrome. Am J Cardiol. (2010) 106(8):1090–4. doi: 10.1016/j.amjcard.2010.06.018
78. Kronish IM, Rieckmann N, Burg MM, Alcántara C, Davidson KW. The psychosocial context impacts medication adherence after acute coronary syndrome. Ann Behav Med. (2014) 47(2):158–64. doi: 10.1007/s12160-013-9544-0
79. Kulkarni SP, Alexander KP, Lytle B, Heiss G, Peterson ED. Long-term adherence with cardiovascular drug regimens. Am Heart J. (2006) 151(1):185–91. doi: 10.1016/j.ahj.2005.02.038
80. Maddison R, Jiang Y, Stewart R, Scott T, Kerr A, Whittaker R, et al. An intervention to improve medication adherence in people with heart disease (Text4HeartII): randomized controlled trial. JMIR Mhealth Uhealth. (2021) 9(6):e24952. doi: 10.2196/24952
81. Newby LK, Bhapkar MV, White HD, Moliterno DJ, LaPointe NM, Kandzari DE, et al. Aspirin use post-acute coronary syndromes: intolerance, bleeding and discontinuation. J Thromb Thrombolysis. (2003) 16(3):119–28. doi: 10.1023/B:THRO.0000024050.78728.35
82. Rahhal A, Mahfouz A, Khir F, Okleh N, Aljundi AH, AlKhalaila O, et al. Medications adherence post-primary percutaneous coronary intervention in acute myocardial infarction: a population-based cohort study. J Clin Pharm Ther. (2021) 46(3):772–9. doi: 10.1111/jcpt.13348
83. Rieckmann N, Kronish IM, Haas D, Gerin W, Chaplin WF, Burg MM, et al. Persistent depressive symptoms lower aspirin adherence after acute coronary syndromes. Am Heart J. (2006) 152(5):922–7. doi: 10.1016/j.ahj.2006.05.014
84. Rieckmann N, Gerin W, Kronish IM, Burg MM, Chaplin WF, Kong G, et al. Course of depressive symptoms and medication adherence after acute coronary syndromes. J Am Coll Cardiol. (2006) 48(11):2218–22. doi: 10.1016/j.jacc.2006.07.063
85. Riegel B, Stephens-Shields A, Jaskowiak-Barr A, Daus M, Kimmel SE. A behavioral economics-based telehealth intervention to improve aspirin adherence following hospitalization for acute coronary syndrome. Pharmacoepidemiol Drug Saf. (2020) 29(5):513–7. doi: 10.1002/pds.4988
86. Schwartz KA, Schwartz DE, Ghosheh K, Reeves MJ, Barber K, DeFranco A. Compliance as a critical consideration in patients who appear to be resistant to aspirin after healing of myocardial infarction. Am J Cardiol. (2005) 95(8):973–5. doi: 10.1016/j.amjcard.2004.12.038
87. Wei L, Fahey T, MacDonald TM. Adherence to statin or aspirin or both in patients with established cardiovascular disease: exploring healthy behaviour vs. drug effects and 10-year follow-up of outcome. Br J Clin Pharmacol. (2008) 66(1):110–6. doi: 10.1111/j.1365-2125.2008.03212.x
88. Wheat HL, Irani E, Hughes J, Josephson R, Dolanksy MA. Insights from monitoring aspirin adherence: a medication adherence cascade tool. Patient Prefer Adherence. (2021) 15:1639–46. doi: 10.2147/PPA.S315296
89. Baxter GJ, Lawrence JR, Graham AB, Wiles D, Paterson JR. Identification and determination of salicylic acid and salicyluric acid in urine of people not taking salicylate drugs. Ann Clin Biochem. (2002) 39(Pt 1):50–5. doi: 10.1258/0004563021901739
90. Bartels H, Böhmer M, Heierli C. Serum kreatinibestimmung ohne enteiweissen [Serum creatinine determination without protein precipitation]. Clin Chim Acta. (1972) 37:193–7. doi: 10.1016/0009-8981(72)90432-9
Keywords: aspirin, cardiovascular disease, secondary prevention, medication adherence, platelet function tests
Citation: Nouni-García R, Ramirez-Familia E, López-Pineda A, Esquerdo-Arroyo A, Carbonell-Soliva Á, Martínez-Muñóz M, Compañ Rosique AF, Quesada JA, Carratalá-Munuera C and Gil-Guillén VF (2025) Methods and validity indicators for measuring adherence and persistence to aspirin in secondary cardiovascular prevention: a systematic review. Front. Cardiovasc. Med. 12:1570331. doi: 10.3389/fcvm.2025.1570331
Received: 17 February 2025; Accepted: 7 May 2025;
Published: 26 May 2025.
Edited by:
Piero Pollesello, Orion Corporation, FinlandReviewed by:
Elena Grossini, University of Eastern Piedmont, ItalyHector A. Cabrera-Fuentes, Imam Abdulrahman bin Faisal University, Saudi Arabia
Copyright: © 2025 Nouni-García, Ramirez-Familia, López-Pineda, Esquerdo-Arroyo, Carbonell-Soliva, Martínez-Muñóz, Compañ Rosique, Quesada, Carratalá-Munuera and Gil-Guillén. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriana López-Pineda, YWRyaWFuYS5sb3BlenBAdW1oLmVz