 Gesa von Olshausen1,2*†
Gesa von Olshausen1,2*† Jonas Schwieler1,3Hamid Bastani1,3Tara Bourke1,3Ott Saluveer1,3Nikola Drca1,3Astrid Paul-Nordin1,3Emmanouil Charitakis1,3Fahd Asaad1,3Serkan Saygi1,3Yusuf Turkmen1,3Emma Svennberg1,3Finn Åkerström1,3Mats Jensen-Urstad1,3Frieder Braunschweig1,3
Jonas Schwieler1,3Hamid Bastani1,3Tara Bourke1,3Ott Saluveer1,3Nikola Drca1,3Astrid Paul-Nordin1,3Emmanouil Charitakis1,3Fahd Asaad1,3Serkan Saygi1,3Yusuf Turkmen1,3Emma Svennberg1,3Finn Åkerström1,3Mats Jensen-Urstad1,3Frieder Braunschweig1,3
- 1Department of Cardiology, Karolinska University Hospital, Stockholm, Sweden
- 2Medical Department I (Cardiology, Angiology, Pneumology), Klinikum Rechts der Isar, Technical University of Munich, Munich, Germany
- 3Heart and Lung Disease Unit, Department of Medicine, Karolinska Institutet, Stockholm, Sweden
Objective: This study aimed to examine the incidence of atrial fibrillation in patients with an accessory pathway (AP) and its association with transient ischemic attack (TIA)/stroke as well as mortality over long-term follow-up.
Methods: A total of 1,302 consecutive patients who underwent first-time ablation AP between 2005 and 2018 were included from the Karolinska Ablation Registry and followed up through the National Patient Registry and Cause of Death Registry.
Results: Patients were 41.7 ± 15.7 years old and 60.9% were men. New-onset or recurrence of atrial fibrillation occurred in 111 patients (8.5%) after a follow-up of up to 10 years (median 6.8 years; interquartile range 3.9–9.9 years). Multivariable analysis revealed that a history of atrial fibrillation, hyperlipidemia, a higher BMI, and older age were independently associated with new-onset or recurrence of atrial fibrillation during follow-up. All-cause mortality and TIA/stroke occurred in 35 patients (2.7%) and 28 patients (2.2%) after a follow-up of 10 years, respectively. Multivariable analysis revealed that the occurrence of atrial fibrillation during follow-up was independently associated with both outcomes.
Conclusion: In this large patient cohort with ablated APs, long-term follow-up revealed a high incidence of atrial fibrillation with 8.5%. Occurrence of atrial fibrillation during follow-up was independently associated with both all-cause mortality and TIA/stroke. Hence, closer monitoring for atrial fibrillation is advisable in patients with ablated APs, especially in those with a prior history of atrial fibrillation.
Introduction
Atrioventricular reentrant tachycardia (AVRT) is a common type of supraventricular tachycardia characterized by an accessory pathway (AP) that allows direct electrical conduction between the atria and ventricles. This AP allows formation of a reentrant circuit involving the AV-node and, thus, provides a substrate for recurrent episodes of rapid tachycardia. Most patients with APs have ventricular preexcitation with a characteristic delta wave in the resting 12-lead ECG during sinus rhythm, but in a substantial proportion preexcitation is absent (“concealed conduction”). Those with preexcitation and clinical AVRT are diagnosed with Wolff–Parkinson–White syndrome. More men than women are affected by APs (1).
Catheter ablation of AP has become the treatment of choice for symptomatic and recurrent AVRT with a high rate of success and few complications (2). Furthermore, invasive electrophysiology for risk assessment (and ablation if appropriate) is also recommended in asymptomatic patients with preexcitation who have a small but sizable risk of sudden death (3).
Among patients with AP, the incidence of atrial fibrillation has been reported ranging from 9%–24% (4–7) which is higher compared to the general adult population (around 3%) (8). In general, atrial fibrillation is associated with an increased risk of all-cause mortality and morbidity including stroke. In patients with an antegrade conduction over the AP, atrial fibrillation may lead to rapid ventricular response potentially degenerating into ventricular fibrillation causing cardiac arrest and death (9).
Therefore, assessing the risk of atrial fibrillation in patients with an AP is essential to provide early diagnosis and treatment. However, there is limited data from systematic analyses evaluating the incidence of atrial fibrillation in patients with an ablated AP in a large patient cohort with long-term follow-up. This study aimed to examine the incidence and risk factors of atrial fibrillation in patients with an ablated AP. Furthermore, the association of atrial fibrillation during follow-up with transient ischemic attack (TIA)/stroke and all-cause mortality was investigated.
Methods
Study protocol and setting
All patients who underwent electrophysiology procedures at Karolinska University Hospital from January 2005 to September 2018 were included in the analysis. Relevant patient characteristics and procedural details were prospectively gathered during the ablation procedure and documented in a computerized database.
The National Patient Registry and the Cause of Death Registry, managed by the Swedish Board of Health and Welfare, supplied data on the date and cause of death, additional baseline comorbidities and the cause-specific hospitalizations, defined based on ICD-10 codes. Each patient was uniquely identified using the personal identification number assigned to all permanent Swedish citizens, enabling the integration of data from various registries. The establishment of this analysis and the linkage of the aforementioned registries were approved by the Swedish Ethical Review Authority (etikprövningsmyndigheten; diarienummer: 2019-00086) and conducted in accordance with the Declaration of Helsinki. According to the approval for this study, individual patient consent was not required.
Study cohort and post-ablation follow-up
A cohort of patients undergoing AP ablation or electrophysiology procedure for risk assessment of AP was selected to ensure a reliable diagnosis of APs. Consecutive patients (≥18 years old at the time of index procedure) undergoing first-time catheter ablation of AP from 01 January 2005 to 30 September 2018 were enrolled. History of atrial fibrillation at baseline was defined as atrial fibrillation within 6 years prior to index procedure. Catheter ablations of AP were performed according to conventional and local standards, as described previously (10, 11). All patients were followed from the time of their index procedure until the date of death, emigration, or the end of the study (31st December 2018).
Study outcomes
Study outcomes were defined as new-onset or recurrence of atrial fibrillation, all-cause mortality and TIA/stroke. Atrial fibrillation and TIA/stroke were diagnosed during both inpatient and outpatient visits. The definitions of the variables used in this study are provided in Supplementary Table S1.
Statistical analysis
All continuous variables are presented as means ± standard deviation or medians with interquartile range (IQR). Categorical variables are reported as frequencies and percentages. Clinical outcomes were assessed over a ten-year period which was considered a meaningful duration for reflecting long-term follow-up. Univariate and multivariable backward logistic regression analyses were conducted to identify factors associated with the new onset or recurrence of atrial fibrillation, all-cause mortality, and hospitalization for TIA/stroke. The multivariable model included factors with a p-value <0.05 in the univariate analysis. Since all available AP patients were included, no sample size calculation was performed. All statistical tests and confidence intervals were two-sided, with a significance level of 0.05. Statistical analyses were performed using SPSS software, version 29 (IBM Corp., Armonk, New York).
Results
Baseline characteristics and index procedure details of patients undergoing first-time catheter ablation for AP
From January 1, 2005, to September 30, 2018, a total of 16,417 invasive electrophysiological procedures were performed in 12,247 patients. From this patient cohort, 1,302 distinct patients with APs met the inclusion criteria and were included in the analysis (Supplementary Figure S1). Their mean age was 41.7 ± 15.7 years and 793 patients (60.9%) were men. At baseline, 116 patients (8.9%) had a prior diagnosis of atrial fibrillation. Table 1 presents all baseline clinical characteristics of the study participants. Table 2 outlines the characteristics related to the index procedure.
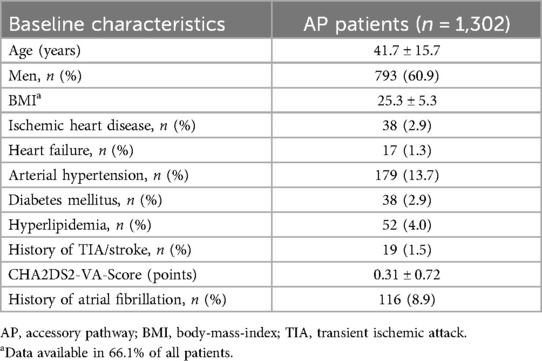
Table 1. Baseline characteristics of patients with catheter ablation for AP.
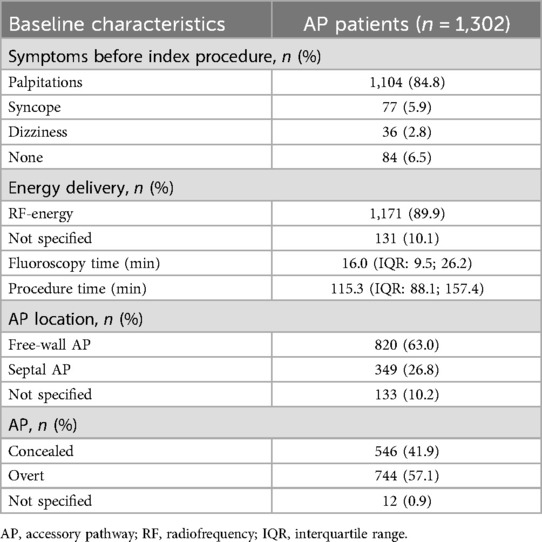
Table 2. Index procedure related characteristics of patients with catheter ablation for AP.
The mean duration of follow-up was 6.9 ± 3.7 years (median 6.8 years; interquartile range 3.9–9.9 years).
Outcomes: atrial fibrillation, all-cause mortality and TIA/stroke
New-onset or recurrence of atrial fibrillation occurred in 111 patients (8.5%) during follow-up of up to 10 years. The corresponding Kaplan–Meier-curve is presented in Figure 1. The mean period from AP ablation to diagnosis of new-onset or recurrence of atrial fibrillation was 1.8 ± 2.2 years. Excluding patients with a history of atrial fibrillation, new-onset of atrial fibrillation occurred in 54 patients (4.6%). Among patients with prior history of atrial fibrillation at baseline, recurrence of atrial fibrillation was observed in 57 patients (49.1%). History of atrial fibrillation, hyperlipidemia, a higher BMI and older age were independently associated with new-onset or recurrence of atrial fibrillation across the entire patient cohort in multivariable analysis (Supplementary Table S2). Table 3 and Supplementary Figure S2, supplementary, present the prevalence of atrial fibrillation based on age at the end of follow-up.
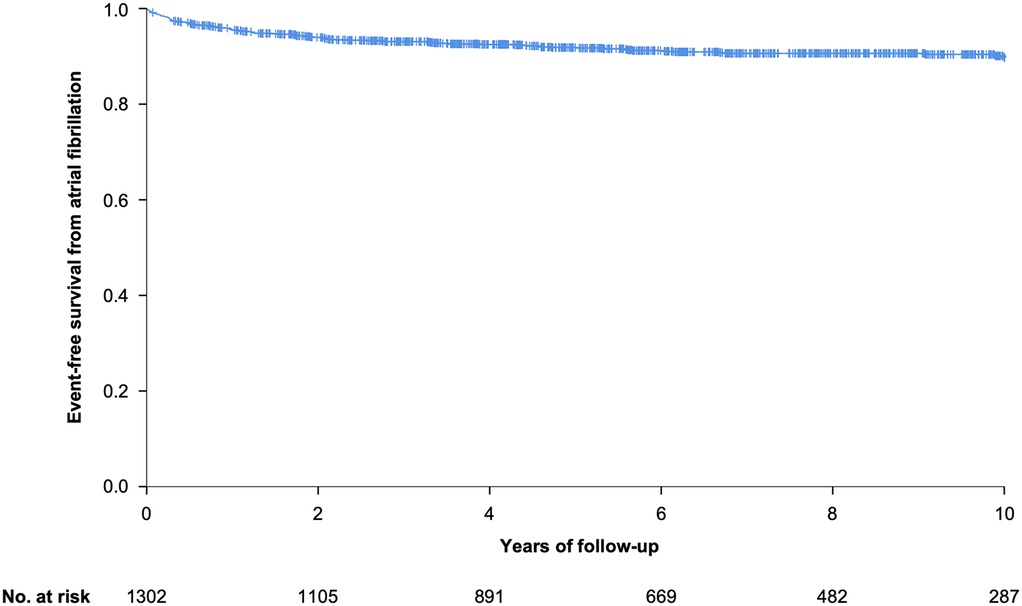
Figure 1. Kaplan–Meier analysis of event-free survival from atrial fibrillation after 10 year follow-up.
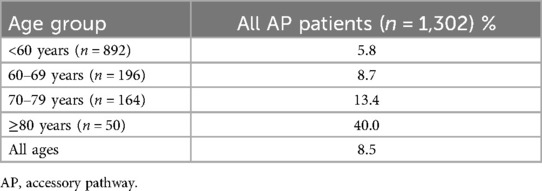
Table 3. Prevalence of atrial fibrillation according to age at the end of follow-up.
All-cause mortality occurred in 35 patients (2.7%) and cardiovascular mortality in 9 (0.7%) after a follow-up of 10 years. Diabetes mellitus, occurrence of atrial fibrillation during follow-up, arterial hypertension and older age were independently associated with all-cause mortality in multivariable analysis (Supplementary Table S3).
TIA/stroke occurred in 28 patients (2.2%) after a follow-up of 10 years. Occurrence of atrial fibrillation during follow-up, history of TIA/stroke and older age were independently associated with TIA/stroke in multivariable analysis (Supplementary Table S4).
Discussion
In this large patient cohort with ablated APs, long-term follow-up revealed a high incidence of atrial fibrillation with 8.5%. After adjusting for covariates, the occurrence of atrial fibrillation during follow-up continued to be independently associated with both all-cause mortality and TIA/stroke.
As far as we are aware, this is the largest patient cohort with ablated AP analyzed in terms of incidence of atrial fibrillation and its association with long-term outcome. The mean age with 41.7 ± 15.7 years at the time of AP ablation and higher proportion of male patients was comparable to previous studies (1, 6). The incidence of new-onset or recurrence of atrial fibrillation during follow-up was high with 8.5% compared to data from the general Swedish population (8) and at the lower range compared to previous data of AP patients (4–7). History of atrial fibrillation, hyperlipidemia, a higher BMI and older age remained independently associated with an increased risk of developing atrial fibrillation during follow-up, consistent with findings from previous studies (4, 7).
The prevalence of atrial fibrillation based on age at the end of follow-up increased with increasing age and was higher among all patient subgroups (<60 years: 5.8%; 60–69 years: 8.7%; 70–79 years: 13.4; ≥80 years: 40%) compared to Swedish general population-based data (<60 years: 0.6%; 60–69 years: 4.2%; 70–79 years: 9.7%; 80–89 years: 13.4%; ≥90 years: 9.0%) (8). Several mechanisms responsible for the genesis of atrial fibrillation in AP patients may be involved such as spontaneous degeneration of AVRT into atrial fibrillation, electrical properties of the AP, the effects of AP on atrial architecture, the intrinsic atrial muscle vulnerability (12, 13), the increased sympathetic activity and vagal withdrawal (14) and the influence of advancing age. Also the existence of a retrograde multiple or multifiber AP is related to atrial fibrillation inducibility (15). Several studies demonstrated a decrease of atrial fibrillation incidence after successful elimination of the AP, suggesting that the AP itself may play an important role in the initiation of atrial fibrillation at least in some patients (16). However, atrial fibrillation still occurs in other patients with AP even after successful ablation. This suggests that atrial vulnerability parameters can be modified through AP ablation in some patients while in others they persist despite ablation (15). In patients with recurrence of pre-existing atrial fibrillation, the natural course of atrial fibrillation also needs to be considered. In non-ablated populations, atrial fibrillation is known to progress over time - from paroxysmal to persistent forms, especially in the presence of structural heart disease or atrial remodeling (17). Thus, recurrence of atrial fibrillation in previously affected individuals may align with this course, and not necessarily be related to AP.
In the current study, nearly half the patients with history of atrial fibrillation had a recurrence of atrial fibrillation during follow-up after AP ablation (57 patients; 49.1%). The (retrospective) design of the current study does not allow to properly answer the question how and to which degree AP ablation impacts the occurrence of atrial fibrillation during follow-up. Nevertheless, due to the high rate of atrial fibrillation, continuation of anticoagulation therapy post AP ablation may be reconsidered in patients with prior atrial fibrillation and a relevant CHA2DS2-VA score.
Compared to our previous study of patients with atrioventricular nodal re-entrant tachycardia (AVNRT) (18), AP patients were younger, proportionally more male and had a lower comorbidity burden. This might explain the lower prevalence of atrial fibrillation at the end of follow-up in AP compared to AVNRT patients (but still being higher among all patient subgroups when compared to general population-based data).
As occurrence of atrial fibrillation during follow-up was independently associated with both all-cause mortality and TIA/stroke, closer clinical monitoring and follow-up in patients with ablated APs is advisable. This especially accounts for patients with prior atrial fibrillation underlining the importance of a close follow-up and a careful consideration before discontinuing anticoagulation in these patients.
Limitations
All data were collected at a single electrophysiology unit, and the results may vary compared to those from other centers.
Follow-up after ablation for atrial fibrillation did not involve intensive monitoring (such as regular Holter-ECG, transtelephonic monitoring, or implantable loop recorders) but was instead based on patient presentations during inpatient or outpatient visits. As a result, asymptomatic cases of atrial fibrillation may have been missed. However, our cohort reflects real-world data with practical clinical relevance.
A potential misclassification between AVRT and atrial fibrillation cannot be ruled out, meaning that an AVRT may have been (mis)classified as atrial fibrillation, particularly before AVRT ablation and when patients were followed up by non-cardiologists.
Energy delivery has not been specified in around 10% of the AP patients. According to documentation most of these patients have still been ablated. Few of these patients might have only received an electrophysiology procedure with AP diagnosis including risk assessment.
Primarily patients with ablated AP were analyzed. Therefore, the results may differ for patients with suspected but not ablated APs, as AP ablation itself may influence the incidence of atrial fibrillation during follow-up.
The administration of all types of treatments for atrial fibrillation, including both medical and ablative therapies, was not included in this study.
Conclusion
In this large patient cohort with ablated APs, long-term follow-up revealed a high incidence of atrial fibrillation with 8.5%. Occurrence of atrial fibrillation during follow-up was independently associated with both all-cause mortality and TIA/stroke. Hence, closer monitoring for atrial fibrillation is advisable in patients with ablated AP, especially in those with a prior history of atrial fibrillation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Swedish Ethical Review Authority (etikprövningsmyndigheten; diarienummer: 2019-00086). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
GvO: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. JS: Data curation, Formal analysis, Writing – review & editing. HB: Data curation, Formal analysis, Writing – review & editing. TB: Data curation, Formal analysis, Writing – review & editing. OS: Data curation, Formal analysis, Writing – review & editing. ND: Data curation, Formal analysis, Writing – review & editing, Validation. AP-N: Data curation, Formal analysis, Writing – review & editing. EC: Data curation, Formal analysis, Writing – review & editing. FA: Data curation, Formal analysis, Writing – review & editing. SS: Data curation, Formal analysis, Writing – review & editing. YT: Data curation, Formal analysis, Writing – review & editing. ES: Data curation, Formal analysis, Writing – review & editing. FÅ: Data curation, Formal analysis, Writing – review & editing. MJ-U: Data curation, Formal analysis, Writing – review & editing. FB: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing, Methodology, Project administration, Resources, Supervision.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This project was supported by the Deutsche Forschungsgemeinschaft to G.O. (OL 605/1-1).
Conflict of interest
GvO has received speaker fees from Astra Zeneca. ND has received consultancy fees from Biosense Webster and Medtronic. AP-N has received a speaker's fee from Johnson & Johnson. ES is supported by the Stockholm County Council (Clinical researcher appointment), the Swedish Research Council (DNR 2022-01466), the Swedish Heart and Lung foundation, CIMED, and has received institutional lecture fees from Abbott, Astra Zeneca, Bristol-Myers Squibb-Pfizer, Johnson & Johnson. FA is a consultant for Abbott and Johnson & Johnson. MJ-U has been consultant for Johnson & Johnson and Medtronic and has received research grants from Medtronic. FB has served as a committee member in trials sponsored by Medtronic and Biotronik. The employer of FB has been paid for industry related activities as chair or speaker. No payment has been directly transferred to FB because of these activities.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2025.1639305/full#supplementary-material
References
1. Porter MJ, Morton JB, Denman R, Lin AC, Tierney S, Santucci PA, et al. Influence of age and gender on the mechanism of supraventricular tachycardia. Heart Rhythm. (2004) 1(4):393–6. doi: 10.1016/j.hrthm.2004.05.007
2. Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomstrom-Lundqvist C, et al. 2019 ESC guidelines for the management of patients with supraventricular tachycardia. The task force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. (2020) 41(5):655–720. doi: 10.1093/eurheartj/ehz467
3. Jemtren A, Saygi S, Akerstrom F, Asaad F, Bourke T, Braunschweig F, et al. Risk assessment in patients with symptomatic and asymptomatic pre-excitation. Europace. (2024) 26(2):euae036. doi: 10.1093/europace/euae036
4. Borregaard R, Lukac P, Gerdes C, Moller D, Mortensen PT, Pedersen L, et al. Radiofrequency ablation of accessory pathways in patients with the Wolff-Parkinson-white syndrome: the long-term mortality and risk of atrial fibrillation. Europace. (2015) 17(1):117–22. doi: 10.1093/europace/euu176
5. Ozcan C, Strom JB, Newell JB, Mansour MC, Ruskin JN. Incidence and predictors of atrial fibrillation and its impact on long-term survival in patients with supraventricular arrhythmias. Europace. (2014) 16(10):1508–14. doi: 10.1093/europace/euu129
6. Dagres N, Clague JR, Lottkamp H, Hindricks G, Breithardt G, Borggrefe M. Impact of radiofrequency catheter ablation of accessory pathways on the frequency of atrial fibrillation during long-term follow-up; high recurrence rate of atrial fibrillation in patients older than 50 years of age. Eur Heart J. (2001) 22(5):423–7. doi: 10.1053/euhj.2000.2429
7. Oddsson H, Edvardsson N, Walfridsson H. Episodes of atrial fibrillation and atrial vulnerability after successful radiofrequency catheter ablation in patients with Wolff-Parkinson-white syndrome. Europace. (2002) 4(2):201–6. doi: 10.1053/eupc.2002.0223
8. Friberg L, Bergfeldt L. Atrial fibrillation prevalence revisited. J Intern Med. (2013) 274(5):461–8. doi: 10.1111/joim.12114
9. Van Gelder IC, Rienstra M, Bunting KV, Casado-Arroyo R, Caso V, Crijns H, et al. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European association for cardio-thoracic surgery (EACTS). Eur Heart J. (2024) 45(36)3314–414. doi: 10.1093/eurheartj/ehae176
10. Insulander P, Bastani H, Braunschweig F, Drca N, Gudmundsson K, Kenneback G, et al. Cryoablation of substrates adjacent to the atrioventricular node: acute and long-term safety of 1,303 ablation procedures. Europace. (2014) 16(2):271–6. doi: 10.1093/europace/eut215
11. Holmqvist F, Kesek M, Englund A, Blomstrom-Lundqvist C, Karlsson LO, Kenneback G, et al. A decade of catheter ablation of cardiac arrhythmias in Sweden: ablation practices and outcomes. Eur Heart J. (2019) 40(10):820–30. doi: 10.1093/eurheartj/ehy709
12. Konoe A, Fukatani M, Tanigawa M, Isomoto S, Kadena M, Sakamoto T, et al. Electrophysiological abnormalities of the atrial muscle in patients with manifest Wolff-Parkinson-white syndrome associated with paroxysmal atrial fibrillation. Pacing Clin Electrophysiol. (1992) 15(7):1040–52. doi: 10.1111/j.1540-8159.1992.tb03098.x
13. Zhang Y, Wang L. Atrial vulnerability is a major mechanism of paroxysmal atrial fibrillation in patients with Wolff-Parkinson-white syndrome. Med Hypotheses. (2006) 67(6):1345–7. doi: 10.1016/j.mehy.2006.02.053
14. Herweg B, Toosi B, Fisher JD, Ferrick KJ. Autonomic modulation and atrial fibrillation in the Wolff-Parkinson-white syndrome. Am J Cardiol. (2000) 85(10):1256–9. doi: 10.1016/S0002-9149(00)00741-4
15. Centurion OA. Atrial fibrillation in the Wolff-Parkinson-white syndrome. J Atr Fibrillation. (2011) 4(1):287. doi: 10.4022/jafib.287
16. Sharma AD, Klein GJ, Guiraudon GM, Milstein S. Atrial fibrillation in patients with Wolff-Parkinson-white syndrome: incidence after surgical ablation of the accessory pathway. Circulation. (1985) 72(1):161–9. doi: 10.1161/01.CIR.72.1.161
17. Calkins H, Hindricks G, Cappato R, Kim YH, Saad EB, Aguinaga L, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. (2017) 14(10):e275–444. doi: 10.1016/j.hrthm.2017.05.012
Keywords: accessory pathway, atrial fibrillation, catheter ablation, catheter ablation registry, recurrence
Citation: von Olshausen G, Schwieler J, Bastani H, Bourke T, Saluveer O, Drca N, Paul-Nordin A, Charitakis E, Asaad F, Saygi S, Turkmen Y, Svennberg E, Åkerström F, Jensen-Urstad M and Braunschweig F (2025) Incidence of atrial fibrillation and its association with long-term outcome in patients with an accessory pathway. Front. Cardiovasc. Med. 12:1639305. doi: 10.3389/fcvm.2025.1639305
Received: 1 June 2025; Accepted: 15 August 2025;
Published: 4 September 2025.
Edited by:
Konstantinos Athanasios Gatzoulis, National and Kapodistrian University of Athens, GreeceReviewed by:
Louisa O'Neill, AZ Sint-Jan Brugge-Oostende AV, BelgiumAnil Rajendra, Grandview Medical Center, United States
Copyright: © 2025 von Olshausen, Schwieler, Bastani, Bourke, Saluveer, Drca, Paul-Nordin, Charitakis, Asaad, Saygi, Turkmen, Svennberg, Åkerström, Jensen-Urstad and Braunschweig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gesa von Olshausen, Z2VzYS5vbHNoYXVzZW5AdHVtLmRl
†ORCID:
Gesa von Olshausen
orcid.org/0000-0001-8145-0414