 Pascale Coulombe1
Pascale Coulombe1 Maxime Robitaille-Fortin2Alexandra Nadeau1,3Christian Malo3,4
Maxime Robitaille-Fortin2Alexandra Nadeau1,3Christian Malo3,4 Pierre-Gilles Blanchard1,3,4Axel Benhamed3Marcel Émond1,3,4
Pierre-Gilles Blanchard1,3,4Axel Benhamed3Marcel Émond1,3,4 Eric Mercier1,3,4*
Eric Mercier1,3,4*- 1VITAM – Centre de Recherche en Santé Durable de l'Université Laval, Québec, QC, Canada
- 2Coopérative des Techniciens Ambulanciers de Québec (CTAQ), Québec, QC, Canada
- 3Axe Santé des Populations et Pratiques Optimales en Santé, Unité de Recherche en Traumatologie – Urgences – Soins Intensifs, Centre de Recherche du CHU de Québec – Université Laval, Québec, QC, Canada
- 4Département de Médecine Familiale et de Médecine d'urgence, Faculté de Médecine, Université Laval, Québec, QC, Canada
Objectives: Pelvic injuries can be life-threatening and are challenging to identify in the prehospital phase. This study aimed to assess how pelvic examination is performed by paramedics and to determine the accuracy of their clinical examination when identifying pelvic fractures.
Methods: This was a prospective cohort study of prehospital interventions including both real and simulated trauma patients between July and August 2022. Data collection for the injured patient was made by an observer who was paired with teams of two consenting paramedics. Data pertaining to the clinical assessment for potential pelvic injuries during all interventions with a trauma patient were collected. Additionally, data were collected during four simulated scenarios of patients with an open-book type pelvic fracture following high-energy trauma mechanisms.
Results: A total of 29 trauma-related clinical interventions were assessed. Most patients were female (n = 22, 75.9%) with a mean age of 69.8 (SD 22.2) years. Fall from standing was the main trauma mechanism (n = 21, 72.4%). During 72.4% (n = 21) of all trauma-related interventions, an assessment for pelvic injuries was performed, mostly by pelvic palpation (n = 19, 65.5%), inquiring about the presence of pain (n = 12, 41.4%), searching for deformation (n = 7, 24.1%), and/or assessing leg length (n = 8, 27.6%). No pelvic injury was suspected by the paramedics, but two patients (6.9%) had a pelvic fracture and two (6.9%) had a hip fracture. Simulated cases of high-velocity mechanisms with an open-book pelvic fracture were completed by 11 pairs of paramedics. Most did a clinical pelvic assessment (n = 8, 72.7%) using palpation. When asked after the simulation, nine pairs (81.8%) suspected a pelvic fracture.
Conclusion: Pelvic injuries are challenging to identify, and pelvic assessment on the field is not standardized among paramedics. Training is needed to increase awareness relative to pelvic injuries and to improve detection.
Introduction
Trauma affects all age groups and is one of the main causes of death and disability worldwide (1–4). An efficient continuum of care, starting with high-quality out-of-hospital care, is vital to improve outcomes in severely injured patients (5, 6). Notably, prehospital identification of patients with life-threatening injuries is critical for ensuring their direct transportation to major trauma centers with the required trauma care expertise (6–10). Pelvic injuries are associated with increased resource use, mortality, and morbidity (11–14). Identifying patients with pelvic trauma can be challenging in the prehospital field, contributing to undertriage (15–17). In our region, approximately one in four patients with a clinically important pelvic fracture is not transported directly to the major trauma center (18). Sensitivity of physical examination to identify pelvic injury is variable. It approaches 100% for conscious patients with an unstable fracture but is < 25% for patients with an altered level of consciousness (19). Furthermore, prehospital care for patients with a pelvic injury is limited. Pelvic circumferential compression devices (PCCDs) can be used as a temporary measure to restrict pelvic volume and reduce hemorrhage (11, 20). Their liberal and preventive application in the prehospital setting is the standard of care for severely injured patients in many countries, including most provinces across Canada (20, 21). However, in our province, PCCDs are not currently used in the prehospital setting. Before introducing them in our prehospital setting, it is important to understand how paramedics are assessing and identifying patients with pelvic trauma to improve detection (15–17). Hence, this study aimed to determine how pelvic examination is performed by paramedics and assess the accuracy of their clinical examination in identifying patients with a pelvic fracture.
Methods
Study design and setting
We performed a prospective cohort study. We collected data on the clinical assessment performed by paramedics during both real and simulated trauma cases between July and August 2022. In our regionalized trauma system, paramedics who have completed a 3-year training program are the sole professionals responsible for prehospital care. The interventions for trauma patients are limited to supraglottic airway device insertion, spinal motion restriction, limb immobilization, tourniquet, and wound packing (22).
Direct observations of patient encounters
Three observers (medical students) were paired with a team of two consenting paramedics and followed them during their whole shift. Prior to the study, the observers had a 1-h training session to explain the pelvic evaluation and how to detail their observations and ensure standardization. Paramedics were aware of the study objective. Overall, observations occurred during ~600 h, mostly during daytime hours and evenings. Data on the clinical assessments performed by the paramedics were collected using a standardized form during all trauma-related interventions on patients who were then transported to one of the five emergency departments (EDs) of the CHU de Québec. Hence, data pertaining to the mechanism of injury, pelvic examination (presence of pain, palpation, deformation, limb length, and others), mobilization device used (vacuum immobilizer mattress and/or a scoop), prehospital triage, and the paramedics' suspicion of a potential pelvic fracture were collected. In-hospital medical records of these patients were then reviewed to collect data relative to sex, age, pelvic imaging (X-ray and/or CT scan), diagnosis of pelvic fracture, and death.
Simulation observations
Four simulated trauma cases were co-created by a team of paramedics. Simulated cases were all adult trauma patients having sustained a high-energy trauma mechanism (car accident, motorcycle accident, fall from the third floor of a building, pedestrian struck; see Appendix 2). A manikin was used, and in each scenario, the simulated patient was unconscious and had an open-book pelvic fracture. Paramedics had to intervene with the manikin similarly as they would do during a regular encounter. The simulations were integrated into a continuous education process. Paramedics were asked to do the simulation during a regular clinical shift and had to consent to being observed by a medical student. Hence, during the simulation, two paramedics had to perform their clinical assessment and explain their reasoning and actions out loud in front of two instructors and the observer. They received some feedback from the instructors after the simulation. We collected data on the pelvic examination and the paramedics' level of suspicion of a pelvic fracture.
Statistical analysis
Categorical variables were presented using proportions and continuous variables were presented using means (SD). All analyses were performed using Excel (Microsoft Corporation, Redmond, WA, 2016).
Ethics approval
This project was approved by the research ethics board of the Centre de Recherche du CHU de Québec – Université Laval (2022-5994).
Results
Direct observations of patient encounters
During the study period, the observers collected data from 29 trauma-related interventions. The patients' mean age was 69.8 (SD 22.2) years, and 75.9% were female. The main mechanism of injury was fall from standing height (72.4%; Table 1).
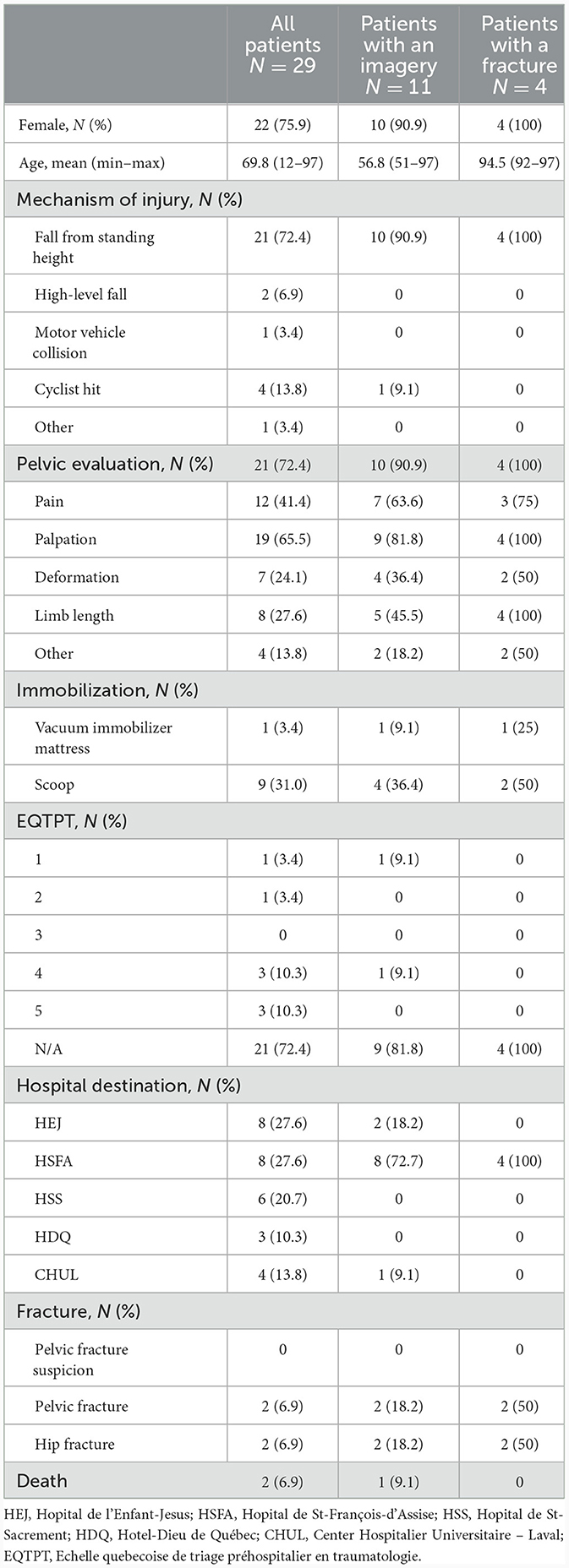
Table 1. Characteristics during direct encounters.
At least one assessment looking for a potential pelvic injury was conducted in the 21 (72.4%) interventions. Nineteen patients (65.5%) had pelvic palpation; deformation was verified for seven patients (24.1%) and eight patients (27.6%) for limb length. Twelve patients (41.4%) were asked about the presence of pelvic pain. Only pain was used for two patients (6.9%) and only palpation for three patients (10.3%). When asked directly after the intervention, no pelvic injury was suspected by the paramedics. The scoop was used for nine patients (31.0%), and only one patient (3.4%), who had a hip fracture, was placed in the vacuum immobilizer mattress. In the ED, 11 patients (37.9%) had a pelvic imaging. Overall, two patients (6.9%) had a pelvic fracture and two (6.9%) had a hip fracture. Visible deformation was seen for two of the four patients with a fracture (one hip fracture and one pelvic fracture), but no fracture was suspected by the paramedics. No pelvic surgery or angio-intervention was needed. Two patients died after their admission, and neither death was due to a pelvic fracture.
Simulation observations
Eleven pairs of paramedics were each subjected to one of the scenarios (Table 2). Pelvic evaluation was done during eight simulated cases (72.7%) via palpation only. Pain could not be used because all patients were unconscious. The scoop was used for five patients (45.5%), and the vacuum immobilizer mattress was used for 10 patients (90.9%). Special attention was paid to the straps at the pelvic level for two (18.2%) patients during the installation of the mattress. All the paramedics who did a pelvic examination suspected a pelvic fracture, plus another two who suspected the fracture at the end when they moved the patient (81.8%).
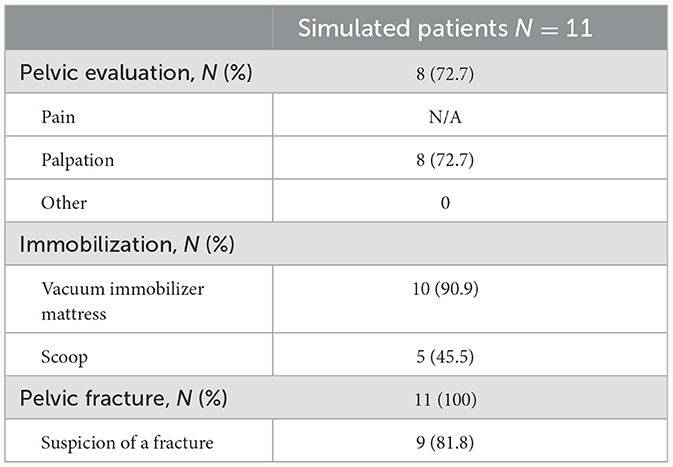
Table 2. Pelvic interventions during the simulations.
Discussion
This study illustrated the difficulties associated with the identification of pelvic fractures, both in the out-of-hospital field and during simulations. The pelvis was not systematically examined. The field cohort was relatively small and did not represent the most common causes of pelvic fracture with a majority of falls from standing height. The population also differed from the pelvic fracture population (18), with the majority being women and older individuals. However, even if the mechanisms of injury were not suggestive of a pelvic fracture, there were still some pelvic fractures not suspected despite a positive finding. Training is required to optimize the potential implementation of prehospital PCCDs, and then a continuous educational process is required to maintain the gains (23).
Regarding the simulations, which represented a population highly suggestive of a pelvic fracture, there were still improvements needed to identify potential pelvic fractures. Even if the mechanism of injury suggested a potentially unstable pelvic fracture, the pelvic region was not systematically examined. However, when the physical exam was done, all pelvic fractures were identified and were put in the vacuum immobilizer mattress, which is the only equipment used locally that may offer some sort of pelvic stabilization. However, there is no evidence in the literature regarding the mattress for pelvic fracture. According to protocols used in other Canadian provinces and other countries, all patients in the simulation would have pre-emptively received a PCCD (mechanism of injury suggestive and GCS < 14) (20, 21). The impact of using PCCDs in the out-of-hospital field on patient-important outcomes is unknown. The development of an evidence-based list of criteria to identify patients who would benefit from a prehospital PCCD would be useful to guide its potential implementation in our setting.
Prehospital triage is challenging, and poor sensitivity among trauma prehospital triage is common, especially in the geriatric population (24–26). Undertriage in identifying trauma patients who need specialized care is not specific to pelvic fractures, even if they are particularly difficult to assess (27). Correctly done, a pelvic examination is important for triage. Pelvic pain assessment for conscious patients can identify up to three-quarters of the fractures. However, deformation can only identify a third of fractures (19). It is important to conduct a diligent assessment aiming for a high sensitivity to avoid undertriage.
Limitations
The study has limitations. The number of observations was limited. The small sample size limited the potential to perform further analysis and make definitive conclusions relative to the accuracy of the pelvic physical examination in our context. Paramedics were not blinded to the objective of the observations. This knowledge probably increased their level of vigilance for potential pelvic injuries due to the Hawthorne effect (28). In addition, the evaluation of the physical examination was made by three different observers, and some actions may have been missed if they were not visible or not said out loud. For instance, there was no way to know if the deformation was evaluated if the paramedic did not comment on their actions. Finally, the study occurred during the summer when the environmental conditions were optimal for the paramedics. Assessments could vary depending on weather conditions.
Conclusion
Pelvic injuries are difficult to identify, especially in the prehospital context, which has its challenges. Pelvic evaluation for trauma patients is not standardized and varies depending on the paramedic. Training is needed to optimize clinical assessment, appropriately triage patients, and select those who would potentially benefit from prehospital PCCDs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Research Ethic Board of the Centre de Recherche du CHU de Quebec – Université Laval. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PC: Data curation, Formal analysis, Funding acquisition, Writing – original draft. MR-F: Conceptualization, Resources, Writing – review & editing. AN: Conceptualization, Formal analysis, Methodology, Project administration, Resources, Writing – original draft. CM: Conceptualization, Writing – review & editing. P-GB: Conceptualization, Writing – review & editing. AB: Conceptualization, Writing – review & editing. MÉ: Conceptualization, Writing – review & editing. EM: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Fonds de démarrage offert aux chercheurs FRQS – junior 1 de VITAM – Centre de recherche en santé durable. PC has received a scholarship from the Canadian Institutes of Health Research (CIHR), the Fonds de recherche du Québec-Santé (FRQS), and the Fond stratégique de développement de la recherche de VITAM – Centre de recherche en santé durable. The Coopérative des techniciens ambulanciers du Québec (CTAQ) – Quebec region, the participating paramedic company, also contributed financially to the project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/femer.2024.1346681/full#supplementary-material
References
1. Moore L, Champion H, O'Reilly G, Leppaniemi A, Cameron P, Palmer C, et al. Impact of trauma system structure on injury outcomes: a systematic review protocol. Syst Rev. (2017) 6:12. doi: 10.1186/s13643-017-0408-8
2. Moore L, Evans D, Hameed SM, Yanchar NL, Stelfox HT, Simons R, et al. Mortality in Canadian trauma systems: a multicenter cohort study. Ann Surg. (2017) 265:212–7. doi: 10.1097/SLA.0000000000001614
3. Benhamed A, Batomen B, Boucher V, Yadav K, Mercier E, Isaac CJ, et al. Epidemiology, injury pattern and outcome of older trauma patients: a 15-year study of level-I trauma centers. PLoS ONE. (2023) 18:e0280345. doi: 10.1371/journal.pone.0280345
4. Parachute. Potential Lost, Potential for Change: The Cost of Injury in Canada 2021. Vancouver, BC: Parachute (2021).
5. Dufresne P, Moore L, Tardif PA, Razek T, Omar M, Boutin A, et al. Impact of trauma centre designation level on outcomes following hemorrhagic shock: a multicentre cohort study. Can J Surg. (2017) 60:45–52. doi: 10.1503/cjs.009916
6. Sampalis JS, Denis R, Frechette P, Brown R, Fleiszer D, Mulder D. Direct transport to tertiary trauma centers versus transfer from lower level facilities: impact on mortality and morbidity among patients with major trauma. J Trauma. (1997) 43:288–95. discussion 95–6. doi: 10.1097/00005373-199708000-00014
7. Beck B, Smith K, Mercier E, Bernard S, Jones C, Meadley B, et al. Potentially preventable trauma deaths: a retrospective review. Injury. (2019) 50:1009–16. doi: 10.1016/j.injury.2019.03.003
8. Zhou Q, Rosengart MR, Billiar TR, Peitzman AB, Sperry JL, Brown JB. Factors associated with nontransfer in trauma patients meeting American college of surgeons' criteria for transfer at nontertiary centers. JAMA Surg. (2017) 152:369–76. doi: 10.1001/jamasurg.2016.4976
9. Cameron PA, Gabbe BJ, Cooper DJ, Walker T, Judson R, McNeil J, et al. statewide system of trauma care in Victoria: effect on patient survival. Med J Aust. (2008) 189:546–50. doi: 10.5694/j.1326-5377.2008.tb02176.x
10. Haas B, Gomez D, Zagorski B, Stukel TA, Rubenfeld GD, Nathens AB. Survival of the fittest: the hidden cost of undertriage of major trauma. J Am Coll Surg. (2010) 211:804–11. doi: 10.1016/j.jamcollsurg.2010.08.014
11. Perumal R, Dilip Chand Raja S, Sivakumar SP, Jayaramaraju D, Sen RK, Trikha V. Management of pelvic injuries in hemodynamically unstable polytrauma patients - Challenges and current updates. J Clin Orthop Trauma. (2021) 12:101–12. doi: 10.1016/j.jcot.2020.09.035
12. Giannoudis PV, Grotz MR, Tzioupis C, Dinopoulos H, Wells GE, Bouamra O, et al. Prevalence of pelvic fractures, associated injuries, and mortality: the United Kingdom perspective. J Trauma. (2007) 63:875–83. doi: 10.1097/01.ta.0000242259.67486.15
13. Pizanis A, Pohlemann T, Burkhardt M, Aghayev E, Holstein JH. Emergency stabilization of the pelvic ring: clinical comparison between three different techniques. Injury. (2013) 44:1760–4. doi: 10.1016/j.injury.2013.07.009
14. Grotz MR, Allami MK, Harwood P, Pape HC, Krettek C, Giannoudis PV. Open pelvic fractures: epidemiology, current concepts of management and outcome. Injury. (2005) 36:1–13. doi: 10.1016/j.injury.2004.05.029
15. Beck B, Smith K, Mercier E, Gabbe B, Bassed R, Mitra B, et al. Differences in the epidemiology of out-of-hospital and in-hospital trauma deaths. PLoS ONE. (2019) 14:e0217158. doi: 10.1371/journal.pone.0217158
16. Vaidya R, Roth M, Zarling B, Zhang S, Walsh C, Macsuga J, et al. Application of circumferential compression device (binder) in pelvic injuries: room for improvement. West J Emerg Med. (2016) 17:766–74. doi: 10.5811/westjem.2016.7.30057
17. Yong E, Vasireddy A, Pavitt A, Davies GE, Lockey DJ. Pre-hospital pelvic girdle injury: improving diagnostic accuracy in a physician-led trauma service. Injury. (2016) 47:383–8. doi: 10.1016/j.injury.2015.08.023
18. Coulombe P, Nadeau A, Malo C, Emond M, Isaac CJ, Mercier E. Identification and management of pelvic fracture during prehospital and emergency department care. CJEM. (2022) 24 (Suppl 1):S1–100. doi: 10.1007/s43678-022-00309-w
19. Shlamovitz GZ, Mower WR, Bergman J, Chuang KR, Crisp J, Hardy D, et al. How (un)useful is the pelvic ring stability examination in diagnosing mechanically unstable pelvic fractures in blunt trauma patients? J Trauma. (2009) 66:815–20. doi: 10.1097/TA.0b013e31817c96e1
20. Knops SP, Van Lieshout EM, Spanjersberg WR, Patka P, Schipper IB. Randomised clinical trial comparing pressure characteristics of pelvic circumferential compression devices in healthy volunteers. Injury. (2011) 42:1020–6. doi: 10.1016/j.injury.2010.09.011
21. Scott I, Porter K, Laird C, Greaves I, Bloch M. The prehospital management of pelvic fractures: initial consensus statement. Emerg Med J. (2013) 30:1070–2. doi: 10.1136/emermed-2013-203211
22. Dufour-Neyron H, Tanguay K, Nadeau A, Emond M, Harrisson J, Robert S, et al. Prehospital use of the esophageal tracheal combitube supraglottic airway device: a retrospective cohort study. J Emerg Med. (2022) 62:324–31. doi: 10.1016/j.jemermed.2021.11.005
23. Amiri H, Gholipour C, Mokhtarpour M, Shams Vahdati S, Hashemi Aghdam Y, Bakhshayeshi M. Two-day primary trauma care workshop: early and late evaluation of knowledge and practice. Eur J Emerg Med. (2013) 20:130–2. doi: 10.1097/MEJ.0b013e32835608c6
24. Beaumont-Boileau R, Nadeau A, Tardif PA, Malo C, Emond M, Moore L, et al. Performance of a provincial prehospital trauma triage protocol: a retrospective audit. Trauma. (2023). doi: 10.1177/14604086231156263
25. Coulombe P, Tardif PA, Nadeau A, Beaumont-Boileau R, Malo C, Emond M, et al. Accuracy of prehospital trauma triage to select older adults requiring urgent and specialized trauma care. J Surg Res. (2022) 275:281–90. doi: 10.1016/j.jss.2022.02.037
26. Fuller G, Pandor A, Essat M, Sabir L, Buckley-Woods H, Chatha H, et al. Diagnostic accuracy of prehospital triage tools for identifying major trauma in elderly injured patients: a systematic review. J Trauma Acute Care Surg. (2021) 90:403–12. doi: 10.1097/TA.0000000000003039
27. van Leent EAP, van Wageningen B, Sir O, Hermans E, Biert J. Clinical examination of the pelvic ring in the prehospital phase. Air Med J. (2019) 38:294–7. doi: 10.1016/j.amj.2019.04.004
Keywords: trauma, injury, prehospital/EMS, pelvic, fracture, triage
Citation: Coulombe P, Robitaille-Fortin M, Nadeau A, Malo C, Blanchard P-G, Benhamed A, Émond M and Mercier E (2024) Clinical assessment to identify pelvic injuries in the prehospital setting: a prospective cohort study. Front. Disaster Emerg. Med. 2:1346681. doi: 10.3389/femer.2024.1346681
Received: 29 November 2023; Accepted: 18 January 2024;
Published: 12 February 2024.
Edited by:
Robert Ehrman, Wayne State University, United StatesReviewed by:
Samad Shams Vahdati, Tabriz University of Medical Sciences, IranOzgur Karcioglu, University of Health Sciences, Türkiye
Copyright © 2024 Coulombe, Robitaille-Fortin, Nadeau, Malo, Blanchard, Benhamed, Émond and Mercier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eric Mercier, ZXJpYy5tZXJjaWVyQGZtZWQudWxhdmFsLmNh