 Celine Tabche1*
Celine Tabche1* Zeenah Atwan1
Zeenah Atwan1 Samar Al-Mutawakel2Noémie Andriamiseza2Maria Popovich2Ela Augustyniak1
Samar Al-Mutawakel2Noémie Andriamiseza2Maria Popovich2Ela Augustyniak1 Andrew Black3
Andrew Black3 Heini Utunen3
Heini Utunen3 Salman Rawaf1
Salman Rawaf1- 1WHO Collaborating Centre for Public Health Education and Training, Faculty of Medicine, Imperial College London, London, United Kingdom
- 2WHO Eastern Mediterranean Regional Office, Health Emergency Workforce, Cairo, Egypt
- 3WHO Health Emergencies (WHE), Geneva, Switzerland
Background: The Leadership in Emergencies (LIE) training programme, developed by WHO's Health Emergencies (WHE) Learning and Capacity Development Unit (LCD) and Eastern Mediterranean Region (EMR) Health Emergencies Department, aims to enhance emergency management and responders' technical and operational skills. WHO implemented a four-phase leadership programme to address leadership gaps in emergency response. This study evaluates its effectiveness using participant surveys and in-depth interviews.
Methods: A total of 207 participants completed the survey, with 10 providing qualitative insights through interviews. The WHO Research Ethics Review Committee approved the study. It assessed the application of non-technical skills, field-level public health expertise, project management in humanitarian settings, and leadership competencies.
Results: Participants frequently applied communication (35.7%), teamwork (36.7%), problem-solving (37.2%), and emotional intelligence (37.7%) skills. Field-level public health skills were frequently applied by 42.5%, and project management skills by 86.5%. Many reported career advancements, improved leadership, networking, stress management, and strategic thinking. The training was relevant, particularly simulation exercises, but challenges included balancing training with professional duties. Participants highlighted the need for structured follow-up. Future training should incorporate ongoing support mechanisms and emphasize simulation exercises and stakeholder engagement.
Conclusion: The findings highlight the necessity of ongoing evaluations, practical simulations, and continuous enhancement of training programmes.
Introduction
Leadership is defined as the influence displayed by an individual over others to achieve goals and make an organization more cohesive (1). Non-technical skills, including effective leadership, are critical in emergencies, characterized by rapid response, efficient coordination, evidence-based decision-making, solidarity through partnerships, and transparent public communication (2, 3). Resilient health system leadership is crucial for effective service management and continuous care delivery. This involves intersectoral collaboration, community involvement, and coordinated partnerships. Structured incident management teams play a key role in effective emergency leadership (4).
Collaborative efforts are vital in emergency responses, even within traditional intergovernmental frameworks (5). Interagency and facilitating interoperation work are essential to implementing leadership in a multi-team environment (3). Interagency lack of coordination remains a significant barrier to successful emergency leadership. This issue often arises from working with unfamiliar colleagues or collaborating under different, challenging circumstances (6).
Two key skill sets are crucial for effective leadership during emergencies. The first set includes fundamental strategic skills needed during stable times, such as having a clear vision and values, implementing strategic plans, and demonstrating communication, negotiation, and collaboration skills. The second set encompasses operational emergency-specific skills, such as analyzing new work environments, making swift decisions, and managing people adeptly in critical situations (7). The lack of specifying commands, such as who the coordinator is or who will achieve the task, was confusing and challenging. Relying on personal non-technical skills, such as building relationships and communications, was very challenging in organizations that are highly protective of their independence (3). Recent global crises, such as the COVID-19 pandemic and humanitarian emergencies in conflict zones, have underscored the crucial role of adaptive leadership in navigating complex and rapidly evolving situations.
Learning from different global experiences can provide valuable lessons for future emergencies. In Wuhan, China, where SARS-CoV-2 first emerged, strict lockdowns and public health measures were implemented in late January 2020, leading to a decline in daily cases. By the end of March 2020, no new cases were reported (8). Countries like Germany and New Zealand demonstrated effective leadership during the pandemic, with decisive decision-making and clear communication. A comparative analysis of 194 countries showed fewer COVID-19-related deaths in female-led nations after adjusting for demographic and economic factors (9, 10). In EMR, Jordan's leadership took proactive measures by suspending education, prohibiting religious gatherings, and closing borders as early as March 14, 2020 (11). Despite these examples, leadership remains a critical area for improvement in health education within the EMR region (12). At the operational level, leadership strengthening can be achieved by enhancing communication and management capacity. Furthermore, weaknesses in field leadership skills were highlighted in certain areas of the world due to the negative influence of the vertical interventions made by external partners during emergencies (13).
In May 2022, the WHO and partners adopted a roadmap to improve national workforce capacity for essential public health functions. It focuses on defining essential functions and services for specific contexts, advancing competency-based education, and assessing occupations contributing to these functions while forecasting workforce needs. In March 2024, a competency framework was published to enhance training programmes (14).
Success in regional emergency responses, including pandemics, hinges on highly coordinated efforts led by globally connected leaders with specialized skills and multi-sector leaders at national and sub-national levels. In the health sector, leadership is particularly challenging due to the complex interplay of politics, access, finance, and local actors in dynamic, rapidly evolving emergencies. Trust is crucial for combating misinformation, ensuring public adherence to health measures, and promoting international collaboration. The 2024 amendments to the International Health Regulations reflect a global commitment to prioritizing trust and collective wellbeing (15). A key lesson is that trust must be cultivated proactively, as efforts to build it during a crisis are often too late to ensure an effective response.
Addressing barriers in emergency leadership is crucial for medical leaders, especially in the EMR region, which faces geopolitical instability, under-resourced health systems, and frequent disease outbreaks. To strengthen leadership capacities, the WHO EMR Office (EMRO) implemented a four-phase training programme in collaboration with the WHO Learning and Capacity Development Unit for all WHO regions and countries worldwide. This blended training focused on advanced non-technical leadership skills, interregional coordination, public health in humanitarian settings, and project management in emergencies and included a practical field simulation (Figure 1). The LIE programme has so far trained over 500 participants from around the world. This study aims to analyse the impact of the LIE training programme on participants' leadership skills.
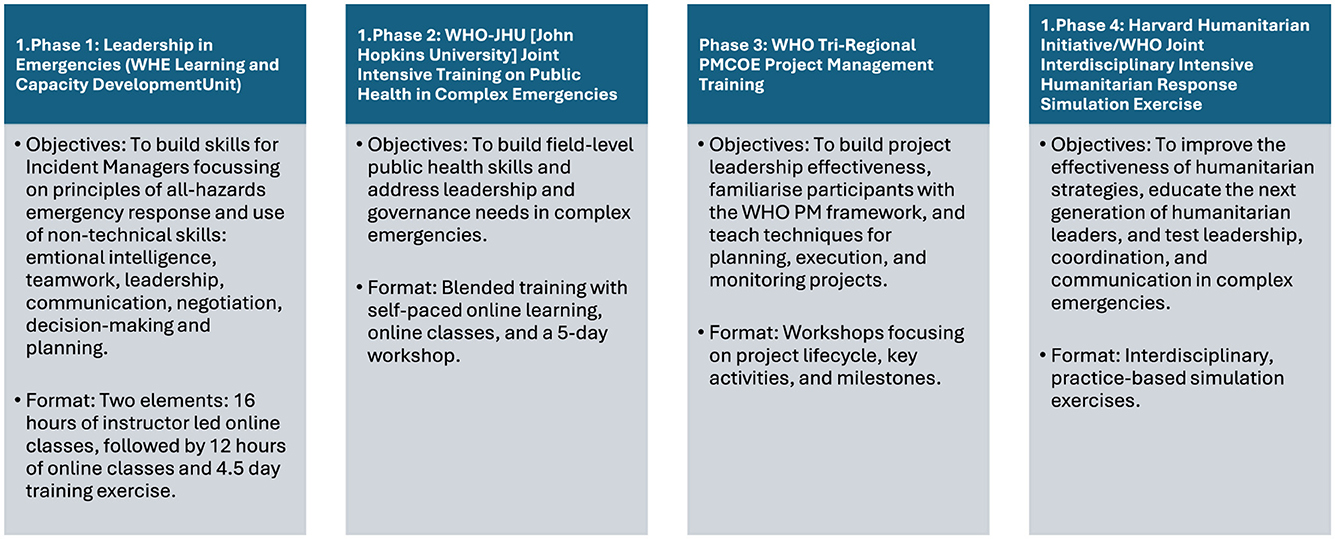
Figure 1. The WHO's four Leadership in Emergencies (LIE) training phases, objectives, and corresponding format.
Methods
The study was conducted to evaluate the WHO leadership in emergencies training. It consisted of two components: surveys and virtual interviews. The WHO Research Ethics Review Committee approved the study. All consent forms and ethical approval documents are available in Appendix 1. Informed consent was secured from all participants. The study involved 207 participants who completed a survey and interviews. The participants were diverse in terms of age, gender, and professional background, representing all parts of the world, ensuring a comprehensive evaluation of leadership in emergency exercises.
Survey
The survey included questions on demographic information (age and gender) and various aspects of the training programme, such as the application of non-technical skills (communication, teamwork, problem-solving, emotional intelligence), field-level public health skills, project management in humanitarian settings, and leadership, coordination, and communication during deployment (Appendix 2: Survey Questions). Participants rated the frequency of applying these skills and the impact of the training on their professional development.
Interviews
In-depth interviews were conducted to gather qualitative data on participants' experiences with the training programme. The interviews focused on themes such as the strengths of training, areas for improvement, collaboration and network feedback, and suggestions for future trainings (Appendix 3: Interview Questions). Saturation was assessed continuously during data collection, and no new themes emerged after the ninth interview, suggesting that thematic saturation was likely reached. Additionally, the participants were purposively sampled to capture a range of relevant professional roles and experiences, which strengthened the diversity of perspectives within the sample (16, 17). The themes for the interviews were informed by Kirkpatrick's model of training evaluation and findings from previous WHO-led leadership programmes, ensuring relevance to the programme's objectives (18).
Results
The survey and interview responses revealed important themes about leadership and non-technical skills in emergency preparedness, humanitarian settings, career advancement, and organizational changes from training. The findings focus on skill application, training impact, and career progression, supplemented by insights from interviews (Appendix 4: Key Survey Results Tables).
PART I: survey results
Participants' demography
The age group 35–44 had the highest participation at 35%, while the 25–34 group had the lowest at 6.8%. Male participants made up 49.8%, and 44.4% held a master's degree. About 66% completed two phases of leadership training, with 66% attending Phase I, 60.9% Phase II, and only 14% and 6% attending Phase III and IV, respectively.
Leadership skills
Participants were asked about the frequency of using non-technical skills in humanitarian and emergency response work. Communication skills were reported as “frequently” (34.3%) or “very frequently” (26.6%) applied by 60.9% of respondents, while 35.7% did not answer. Teamwork skills were noted by 36.2% as “very frequent” and 24.6% as “frequent,” with 36.7% not responding. Problem-solving skills were reported by 30.4% as “frequent” and 25.1% as “very frequent,” with 37.2% not responding. Emotional intelligence was applied “frequently” by 30.4% and “very frequently” by 23.7%, with 37.7% not providing a response.
In contrast, fewer participants indicated frequent application when asked about more field-specific public health and project management skills. Field-level public health skills were reported as “frequent” and “very frequent” by 16.9% and 26.1% of participants, respectively, while 43% did not respond. The application of project management in humanitarian settings was less common, with only 5.3% and 3.4% of participants indicating “frequent” and “very frequent” use, respectively, and 86.5% not answering this item. During deployment, the trainees highlighted the application of leadership, coordination, and communication skills at low percentages of 1.4% and 2.9%, respectively, with a significant majority (94.2%) not responding to this question.
Training impact
The training's impact on participants' skills and professional development was also assessed, with responses indicating significant improvements across various competencies. The programme “significantly” and “very significantly” improved participants' leadership non-technical skills at 30% and 31%, respectively. Networking skills, inside and outside their organizations, reported at 33.8% and 15.9% for “significant” and “very significant” improvement, respectively. Stress management and resilience under stressful conditions, with 46.9% reporting “significant” improvement and 14% reporting “very significant” improvement. Coordination and effectiveness skills improved by 35.3% and 23.2% of participants reporting “significant” and “very significant” enhancements, respectively.
Critical thinking and decision-making abilities were also “significantly” improved at 33.3%, with an additional 18.4% reporting “very significant” improvement. Written and verbal communication skills for conveying complex ideas were “significantly,” “moderately,” and “very significantly” improved by the training programme at 38.7%, 17.4%, and 7.7%, respectively. Negotiation skills with stakeholders showed “significant,” “moderate,” and “very significant” improvement in 33.3%, 15%, and 14% of participants, respectively, with more than 45% noting better collaboration with stakeholders.
Confidence in leading during emergencies was “frequently” or “very frequently” reported at 35.3% and 27.5%, respectively. Other improvements included awareness of organizational issues (43.5%), consideration of perspectives (51%), prioritization (52%), change implementation (49.3%), and encouragement of innovation (40.6%).
Most participants felt that the time spent training was “worth” the changes or developments they observed, with most ratings above 7 (from a scale of 1 to 10), indicating that participants perceived substantial value from the training. Almost all the participants were satisfied with the different degrees of leadership in the emergency training programmes, and more than 60% of the participants would recommend the course to other colleagues.
Career advancements
The training programme also improved various skills, including fostering innovation ecosystems, and inspiring a vision for the future, with reported improvements of 20.8% and 43%, respectively. Less than 10% of participants experienced career advancements such as promotions, recognition or awards, new job opportunities, or deployments, while more than 30% reported increased responsibilities. Specifically, 19 out of 207 participants reported being promoted after the training, and 68 participants indicated increased responsibilities within their organizations. Furthermore, 18 participants received recognition or awards, and 16 reported new job opportunities. Another 16 participants reported deployments post-training, highlighting the direct relevance of the skills gained to operational roles in emergency response.
Phase-specific benefits
When asked about the different phases of the training programme and their impact, most participants reported positive outcomes across several dimensions. In terms of organizational awareness, 90 participants (43.5%) felt more aware of current organizational and political issues, while 106 participants (51.2%) reported being better able to consider issues from others' perspectives. Regarding prioritization and communication, 109 participants (52.7%) felt they could better prioritize and communicate activities effectively. Improvements in change management were noted by 102 participants (49.3%), who reported being better equipped to work with key stakeholders to implement change management and transformation strategies. In the areas of innovation and strategic planning, 82 participants (39.6%) felt more capable of co-creating a strategic plan for their organization, and 84 participants (40.6%) felt better equipped to encourage innovation. Finally, in terms of long-term impact and vision, 89 participants (43%) reported being more able to recognize the long-term impact of their decisions and collaborations, and 69 participants (33.3%) felt they could better demonstrate an inspiring vision for the future.
Part II: interviews
The virtual interviews involved 10 participants, all of whom signed consent forms to ensure privacy and confidentiality. Their roles included emergency disaster manager, preparedness officer, and various positions with WHO related to health emergency preparedness. Attendance across the four phases varied, with 80% in Phase IV, 70% in Phase I, 60% in Phase II, and 50% in Phase III. A summary of key themes, findings, and quotes from the interviews can be found in Table 1.
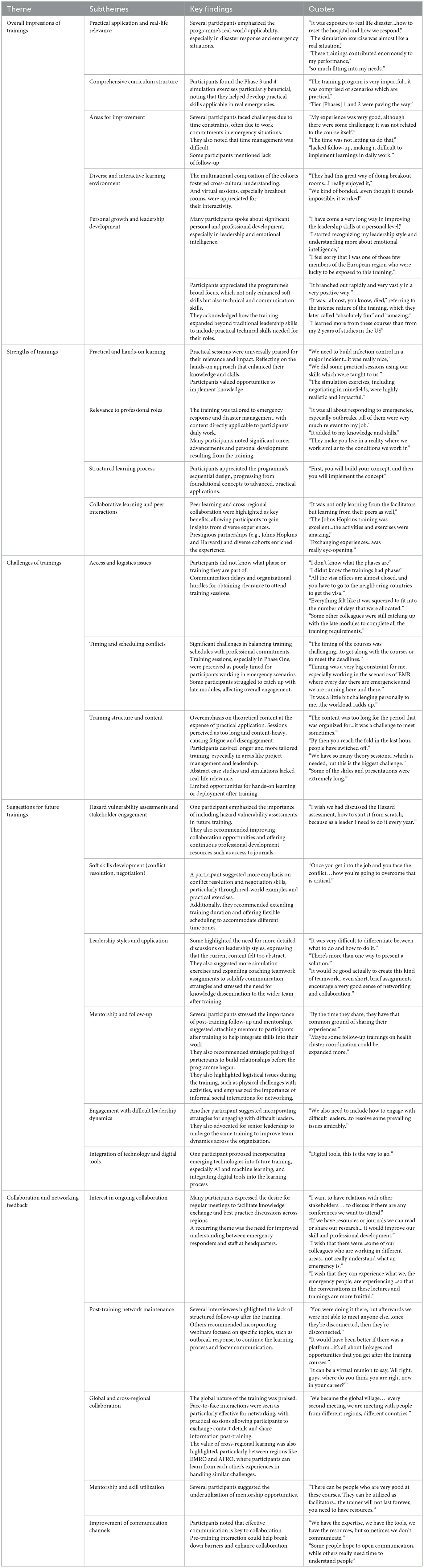
Table 1. Summary of the 10 interviews categorized into themes with key findings and quotes.
Overall impression of the trainings
The interview results provided insights into participants' experiences with the LIE training programme, highlighting its strengths and areas for improvement. Many praised its practical application, particularly in disaster response, due to realistic scenarios that allowed them to develop directly applicable skills. The curriculum's simulation exercises in Phases 3 and 4 were notably beneficial.
However, time constraints were a challenge for some, especially those with emergency work commitments, and a lack of mentoring opportunities post-training was noted. Despite these issues, the training fostered cross-cultural understanding through multiregional cohorts and valued interactive virtual sessions.
Participants reported significant personal growth in leadership and emotional intelligence, appreciating the programme's focus on both technical and non-technical skills. The structured learning process, progressing from foundational to advanced concepts, received positive feedback.
Strengths of the trainings
The programme's practical learning received high praise for its relevance to emergency response and disaster management roles. Many participants noted it contributed to their career advancement and personal growth. The chance for collaborative learning across regions was also highlighted as a key benefit, enhancing the experience with diverse perspectives.
Challenges of the trainings
However, there were challenges related to access and logistics, including communication delays and difficulties with obtaining senior management clearance to attend trainings. Additionally, balancing training schedules with professional commitments, particularly for those in emergency scenarios, was a significant challenge. Some participants felt that the training emphasized theoretical content too much at the expense of practical application. Sessions were occasionally seen as too long and content-heavy, leading to fatigue and disengagement.
Suggestions for future trainings
For future iterations of the training programme, participants suggested including hazard vulnerability assessments, which were included in Phase 1 of the training, and enhancing opportunities for stakeholder engagement. They also emphasized the need for more focus on conflict resolution, negotiation skills, and leadership styles, particularly through real-world examples and simulation exercises. Mentorship and follow-up were identified as critical areas for improvement, with participants suggesting that mentors be assigned to participants before the programme's start. Communication with the organizers needs to be enhanced since most participants did not know what the Phases of the training programme were. They also reported that these interviews were a good way to evaluate and hear their feedback about training programmes.
Collaboration and networking feedback
Participants suggested strategies for handling difficult leadership dynamics, emphasizing the importance of senior leaders participating in the same training to ensure a unified approach. They advocated for integrating emerging technologies like AI and digital tools into future sessions. Ongoing collaboration through topic-focused webinars was highlighted as valuable for continued learning. The global nature of the training was widely praised, with face-to-face interactions particularly valued for networking opportunities. Cross-regional collaboration was seen as a key benefit, and participants also suggested improving the utilization of mentorship opportunities to enhance collaboration.
Discussion
The results from the participants' perspectives indicate that all training phases enhanced leadership skills, particularly in non-technical and technical competencies, which are essential in emergencies. Training leaders in these areas is crucial, given the complex and high-stress environment of public health crises (14, 19). Interviewees highlighted the relevance of emergency-focused content, emphasizing the importance of timely decision-making. Delays in such decisions can significantly impact public health in situations like the COVID-19 pandemic, especially during exponential case growth (20). The findings align with existing studies on leadership training (21), which emphasizes the importance of practical simulations in enhancing emergency preparedness.
EMRO's Health Emergency Workforce initiative focuses on enhancing skills critical for swift decision-making and team coordination in emergencies. The programme also emphasizes stress management techniques to help responders maintain wellbeing and performance under pressure, highlighting the need for these competencies in training. Both surveyed and interviewed participants noted that their emotional intelligence and behavior, essential non-technical and technical skills for crisis leadership, had notably improved. Formal leadership training is often lacking in public health, with most learning adapted from other sectors, such as business and government (22). In particular, the programme enhanced communication skills, a fundamental competency in crisis leadership, supported by 10 best practices for crisis communication. These include pre-event planning, treating the public as informed partners, coordinating across agencies, and building credible partnerships (23). Enhancing participants' emotional intelligence aligns with the concept that compassionate leadership is both challenging and essential. Leaders lacking self-awareness often struggle with professional organization and emotional resilience (24).
A key gap identified was the lack of structured pre- and post-training mentorship. Participants were unclear about the training phases, suggesting a need for improved communication. Establishing formal mentorship frameworks and engaging stakeholders could enhance skill development. Furthermore, utilizing infographics to illustrate the phases and their respective objectives serves as a clear and concise communication strategy to address this challenge. Participants emphasized the importance of collaboration, referencing incidents like the World Trade Center disaster, which highlighted the necessity for coordinated efforts across agencies. Participants suggested integrating communication techniques into healthcare education to prepare future leaders (23).
The training's reported impact on career advancements, including promotions and increased responsibilities, indicates that such programmes can play a role in professional growth; however, even if it is the participants' perspective, it may not have been the sole reason. Organizations should consider integrating similar training modules to foster their staff's leadership development and career progression. Overall, the programmes fostered a range of competencies, such as advanced technical knowledge, strategic thinking and planning, critical analysis, emotional intelligence, negotiation and communication, which are critical for ensuring effective humanitarian response, organizational resilience, maintaining financial and employee stability (25).
The study's strengths include its combination of quantitative (survey) and qualitative (interviews) methods to assess the training programme's effectiveness from the participants' perspectives. It involved a diverse participant group comprising individuals of various ages, genders, and professional backgrounds, thereby enhancing the applicability of the findings to emergency responders. The in-depth interviews provided valuable insights into their experiences. This training has specific goals and was designed to address the needs of the WHO regions. It is delivered through the WHO EMRO and targets all emergency personnel in leadership roles who respond to emergency situations. This evaluation is also unique, as it is the first of its kind to assess participants' perspectives on the effectiveness of the training. According to the interviews, the inter-regional composition of the cohort facilitated the enrichment of knowledge and experience, an aspect identified as essential to sustain through ongoing communication platforms.
One of the limitations encountered during this study was the high non-response rate for key survey items, which reached around 35%. This lack of responses may be attributed to some survey participants not attending one of the training phases or finding certain aspects irrelevant to their experiences. Specifically, questions related to phases that some respondents did not participate in showed particularly high non-response rates, exceeding 90% for deployment-related questions and 86.5% for project management skills. Another limitation is that this type of training from the WHO is unique in its objectives, and this evaluation could have benefited from comparator evaluations of leadership programmes to assess its effectiveness.
Moreover, the reliance on self-reported survey data may introduce biases, such as social desirability. Future evaluations of these trainings should include pre- and post-competency assessments, as well as long-term follow-ups to assess the training's sustained impact on skills and career progression. Additionally, the small interview sample size may not fully represent the broader participant group, and future evaluations should consider interviewing a larger sample size to enhance generalisability and depth of analysis. Challenges in balancing training with professional duties were reported, impacting engagement and outcomes. While survey results indicated high satisfaction, some participants faced organizational barriers that hindered skill application. Future research should address these limitations by using observational methods and increasing participant recruitment.
Conclusion
In conclusion, participants reported that the leadership, technical, managerial, and deployment training empowered them with the confidence and ability to apply those skills effectively in real-life emergencies. By emphasizing practical applications, the programme enabled participants to translate theoretical knowledge into essential hands-on competencies for crisis management. This initiative has made a measurable impact on addressing leadership gaps in the WHO regions. To enhance the programme's impact, future phases should focus on fostering stakeholder engagement, emphasizing the need for continuous improvement through evaluations like this study, and ensuring clear communication. Strengthening leadership through targeted training is also essential for better emergency response and saving lives.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by WHO Research Ethics Review Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CT: Visualization, Software, Conceptualization, Validation, Investigation, Writing – original draft, Project administration, Formal analysis, Methodology, Writing – review & editing, Data curation. ZA: Validation, Formal analysis, Methodology, Data curation, Writing – review & editing, Writing – original draft. SA-M: Methodology, Writing – review & editing, Conceptualization. NA: Writing – review & editing, Data curation. MP: Data curation, Writing – review & editing. EA: Writing – review & editing. HU: Writing – review & editing. SR: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
SAl-M, NA, AB, HU, and MP work for the WHO Eastern Mediterranean Region (EMR) Office and WHO Headquarters, and they did not interfere with the data analysis or writing of the results of this manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/femer.2025.1599284/full#supplementary-material
References
1. Benmira S, Agboola M. Evolution of leadership theory. BMJ Leader. (2021) 5:3–5. doi: 10.1136/leader-2020-000296
2. Al Saidi AMO, Nur FA, Al-Mandhari AS, El Rabbat M, Hafeez A, Abubakar A. Decisive leadership is a necessity in the COVID-19 response. Lancet. (2020) 396:295–8. doi: 10.1016/S0140-6736(20)31493-8
3. Black A, Brown O, Utunen H, Gamhewage G, Gore J. Insights on public health professionals non-technical skills in an emergency response (multi-team system) environment. Front Psychol. (2022) 13:827367. doi: 10.3389/fpsyg.2022.827367
4. Njuguna C, Tola H, Maina BN, Magambo KN, Namukose S, Kamau S, et al. Roles of health system leadership under emergency in drought-affected districts in northeast Uganda: a mixed-method study. BMJ Open. (2024) 14:e080374. doi: 10.1136/bmjopen-2023-080374
5. Grisez Kweit M, Kweit RW. A tale of two disasters. Publius. (2006) 36:375–92. doi: 10.1093/publius/pjj023
6. Fos PJ, Honoré PA, Honoré RL. “Coordination of public health response: the role of leadership in responding to public health emergencies.” In: Science-Based Approaches to Respond to COVID and Other Public Health Threats. IntechOpen (2021). doi: 10.5772/intechopen.96304
7. Hershkovich O, Gilad D, Zimlichman E, Kreiss Y. Effective medical leadership in times of emergency: a perspective. Disaster Mil Med. (2016) 2:4. doi: 10.1186/s40696-016-0013-8
8. Tang JL, Li LM. Importance of public health tools in emerging infectious diseases. BMJ. (2021) 375:n2374. doi: 10.1136/bmj.n2374
9. Garikipati S, Kambhampati U. Leading the fight against the pandemic: does gender really matter? Fem Econ. (2021) 27:401–18. doi: 10.1080/13545701.2021.1874614
10. Forman R, Atun R, McKee M, Mossialos E. 12 lessons learned from the management of the coronavirus pandemic. Health Policy. (2020) 124:577–80. doi: 10.1016/j.healthpol.2020.05.008
11. Alsharaydeh I, Rawashdeh H, Saadeh N, Obeidat B, Obeidat N. Challenges and solutions for maternity and gynecology services during the COVID-19 crisis in Jordan. Int J Gynaecol Obstet. (2020) 150:159–62. doi: 10.1002/ijgo.13240
12. WHO EMRO. EMHJ. Medical education in the Eastern Mediterranean Region. (2015). Available online at: https://applications.emro.who.int/emhj/v21/09/EMHJ_2015_21_9_687.pdf?ua= (accessed January 14, 2025).
13. Bigirinama RN, Makali SL, Mothupi MC, Chiribagula CZ, St Louis P, Mwene-Batu PL, et al. Ensuring leadership at the operational level of a health system in protracted crisis context: a cross-sectional qualitative study covering 8 health districts in Eastern Democratic Republic of Congo. BMC Health Serv Res. (2023) 23:1–12. doi: 10.1186/s12913-023-10336-7
14. WHO Health Workforce. World Health Organization. Global Competency and Outcomes Framework for the Essential Public Health Functions. Available online at: https://www.who.int/publications/i/item/9789240091214 (accessed January 7, 2025).
15. Habibi R, Eccleston-Turner M, Burci GL. The 2024 amendments to the international health regulations: a new era for global health law in pandemic preparedness and response? SSRN Electronic Journal. (2024) 52. doi: 10.2139/ssrn.4962876
16. Hennink MM, Kaiser BN, Marconi VC. Code saturation versus meaning saturation: how many interviews are enough? Qual Health Res. (2016) 27:591. doi: 10.1177/1049732316665344
17. Guest G, Bunce A, Johnson L. How many interviews are enough? Field Methods. (2006) 18:59–82. doi: 10.1177/1525822X05279903
19. Larsen T, Beier-Holgersen R, Østergaard D, Dieckmann P. Training residents to lead emergency teams: a qualitative review of barriers, challenges and learning goals. Heliyon. (2018) 4:e01037. doi: 10.1016/j.heliyon.2018.e01037
20. Kerrissey MJ, Edmondson AC. HBR. What Good Leadership Looks Like During This Pandemic. (2020). Available online at: https://hbr.org/2020/04/what-good-leadership-looks-like-during-this-pandemic (accessed January 14, 2025).
21. Kayano R, Clarke Phd M, Gan C, Murray V, Chan E, El-Baba M, et al. Integration of simulation-based exercises and practical skills into a public health emergency management curriculum. Prehosp Disaster Med. (2023) 38:s26. doi: 10.1017/S1049023X23001097
22. Koh HK, Jacobson M. Fostering public health leadership. J Public Health. (2009) 31:199–201. doi: 10.1093/pubmed/fdp032
23. Bachmann C, Pettit J, Rosenbaum M. Developing communication curricula in healthcare education: an evidence-based guide. Patient Educ Couns. (2022) 105:2320–7. doi: 10.1016/j.pec.2021.11.016
24. Harrel E, Berland L, Jacobson J, Addiss DG. Compassionate leadership: essential for the future of tropical medicine and global health. Am J Trop Med Hyg. (2021) 105:1450–2. doi: 10.4269/ajtmh.21-0832
Keywords: training evaluation, emergency preparedness, leadership in emergencies, WHO training, leadership competencies, emergency response, pedagogy
Citation: Tabche C, Atwan Z, Al-Mutawakel S, Andriamiseza N, Popovich M, Augustyniak E, Black A, Utunen H and Rawaf S (2025) Evaluating the WHO leadership in emergencies training programme: participants' perspective. Front. Disaster Emerg. Med. 3:1599284. doi: 10.3389/femer.2025.1599284
Received: 24 March 2025; Accepted: 09 June 2025;
Published: 02 July 2025.
Edited by:
Ives Hubloue, Vrije University Brussels, BelgiumReviewed by:
Cara Taubman, Harlem Hospital Center, United StatesJamla Rizek, Adventures with Nurse Jamla, United States
Copyright © 2025 Tabche, Atwan, Al-Mutawakel, Andriamiseza, Popovich, Augustyniak, Black, Utunen and Rawaf. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Celine Tabche, Y2VsaW5lLnRhYmNoZUBpbXBlcmlhbC5hYy51aw==