 Lucio Vilar*
Lucio Vilar* José Luciano AlbuquerquePatrícia Sampaio GadelhaFrederico Rangel FilhoAline Maria C. SiqueiraMaíra Melo da FonsecaKaroline Frazão Viana
José Luciano AlbuquerquePatrícia Sampaio GadelhaFrederico Rangel FilhoAline Maria C. SiqueiraMaíra Melo da FonsecaKaroline Frazão Viana Barbara Sales Gomes
Barbara Sales Gomes Ruy Lyra
Ruy Lyra
- Division of Endocrinology, Hospital das Clínicas, Federal University of Pernambuco, Recife, Brazil
Successful discontinuation of cabergoline (CAB) treatment has been reported in 31–75% of prolactinomas patients treated for at least 2 years. In contrast, it is not well established whether CAB therapy can be successfully withdrawn after a failed first attempt. This prospective open trial was designed to address this topic and to try to identify possible predictor factors. Among 180 patients with prolactinomas on CAB therapy, the authors selected those who fulfilled very strict criteria, particularly additional CAB therapy for at least 2 years, normalization of serum prolactin (PRL) levels following CAB restart, no tumor remnant >10 mm, no previous pituitary radiotherapy or surgery; and current CAB dose ≤1.0 mg/week. Recurrence was defined as an increase of PRL levels above the upper limit of normal. A total of 34 patients (70.6% female) treated with CAB for 24–30 months were recruited. Ten patients (29.4%) remained without evidence of recurrence after 24–26 months of follow-up. Twenty-four patients (70.6%) recurred within 15 months (75% within 12 months) after drug withdrawal and ~80% were restarted CAB. Median time to recurrence was 10.5 months (range, 3–15). Despite overlapping values, non-recurring patients had significantly lower mean PRL levels before withdrawal. Moreover, the recurrence rate was lower in subjects without visible tumor on pituitary magnetic resonance imaging (MRI) than in those with small remnant tumor (60 vs. 79%), though the difference was not statistically significant (P = 0.20). No other characteristic could be identified as a predictor of successful CAB discontinuation. In conclusion, a second attempt of CAB withdrawal after two additional years of therapy may be successful, particularly in patients with lower PRL levels and no visible tumor on pituitary MRI. Close monitoring of PRL level is mandatory, especially within the first year after withdrawal, where most recurrences are detected.
Introduction
Prolactinomas are the most common pituitary tumors and account for about half of cases (1, 2). Their prevalence in the general population ranges from 6 to 50 per 100,000 (3, 4). Without appropriate treatment, prolactinomas may cause hypogonadism, infertility, bone loss, headaches, and visual fields defects from mass effect (5), as well as metabolic disorders (6). Based on their size, prolactinomas are classified into macro adenoma (>1 cm) or micro adenoma (<1 cm) (5). The mainstay of therapy involves the use of dopamine agonists (DA), even for patients with optic chiasm compression by large tumors (7, 8). Cabergoline (CAB) has been largely recommended as the first line agent, due to its better tolerability and higher efficacy in normalizing prolactin (PRL) levels and inducing tumor shrinkage, compared to bromocriptine (2, 5, 7, 8).
Studies of patients treated with CAB for microprolactinomas and macroprolactinomas have reported normalization of PRL levels in 75–90%, associated with an average decrease in tumor volume of 72–92% (9–11). In the Brazilian multicenter study on hyperprolactinemia, CAB therapy was able to induce significant tumor shrinkage and complete disappearance of tumor in 80 and 57.5% of patients, respectively (7).
A major drawback of DA therapy is the potential need to keep the medication indefinitely in many patients (2, 5). Indeed, despite the widespread use of DA for patients with prolactinomas and symptomatic idiopathic hyperprolactinemia for many decades, the optimal treatment strategy and duration of treatment is still not evident (12).
The 2011 Endocrine Society Clinical Practice Guideline recommends that, with careful clinical and biochemical follow-up, therapy may be tapered and perhaps discontinued in patients who have been treated with DA for at least 2 years, provided they no longer have elevated PRL levels, nor detectable tumor remnant on magnetic resonance imaging (MRI) (13). Accordingly, four recent studies (n = 292) have demonstrated that CAB therapy can be successfully discontinued, although hyperprolactinemia recurrence rates ranged from 25 to 69% (mean, 49%) (14–17).
On the other hand, it is not well established whether CAB therapy can be successfully withdrawn after a failed first attempt (18). This prospective study was conducted to address this topic and to try to identify possible predictor factors.
Subjects and Methods
Patients and Study Protocol
Among 180 patients with prolactinomas on CAB therapy routinely followed in the Division of Endocrinology, Hospital das Clínicas, Federal University of Pernambuco, Recife, Brazil, the authors selected those who fulfilled all of the following criteria: (1) recurrence of hyperprolactinemia after a first CAB withdrawal; (2) additional CAB therapy for at least 2 years; (3) normalization of serum PRL levels following CAB restart; (4) no tumor remnant ≥10 mm in its largest diameter on a recent (<6 months) MRI; (5) no previous pituitary radiotherapy or surgery; (6) no history of pregnancy over the past 3 years; (7) negative screening for macroprolactinemia; and (8) current CAB dose ≤1.0 mg/week.
After CAB withdrawal, the patients underwent clinical and hormonal (PRL levels) evaluation at 30 days and then every 3 months thereafter. Those patients who experienced disease recurrence, defined as an increase of PRL levels above the upper limit of normal (ULN) for gender, were removed from the study and restarted CAB at the same previous dose, according to the severity of their symptoms. They were also submitted to a pituitary MRI, aiming to detect any change in tumor remnant volume.
The study protocol was approved by our Local Ethics and Scientific Committees and all patients gave written informed consent.
Hormone Assays and Imaging Studies
Serum PRL was measured using a two-site chemiluminescent immunometric assay. The interassay coefficient of variation was <5%. Normal range was 1.2–29.9 ng/ml (25–634 μUI/ml) for women and 2.6–18.1 ng/ml (55–384 μUI/ml) for men.
The radiological study included the evaluation of the sellar region by MRI with axial, coronal, and sagittal slices in T1, pre- and post-gadolinium, and in T2. The MRI was evaluated by a skilled neuroradiologist.
Statistical Analysis
For comparison of categorical variables, the chi-squared test or the Fisher exact test were used where appropriate. A paired Student’s t-test was performed for the comparative analysis of quantitative variables. Results are expressed as percentages or mean values ± SD, unless otherwise stated. A stratified analysis was performed aiming at finding potential associations among clinical, imaging, and biochemical characteristics with outcome. Values of P < 0.05 were considered statistically significant. STATA version 10.0 and SPSS version 16.0 were used as statistical software.
Results
Characteristics of Patients
A total of 34 patients, 24 women and 10 men, fulfilled the selection criteria. Their individual baseline characteristics are shown in Table 1. At diagnosis, their mean age was 32.7 ± 4.53 years (range, 24(42; median, 32) and 11 (32.3%) had microadenomas. At withdrawal, their mean age was 41.35 ± 4.84 years (range, 31(52; median, 42) and they have been treated with CAB for 27.03 ± 2.02 months (range, 24(30; median, 27). The average weekly CAB dose at second withdrawal was 0.89 ± 0.20 mg (median, 1.0; range, 0.5(1.0) (Table 2).
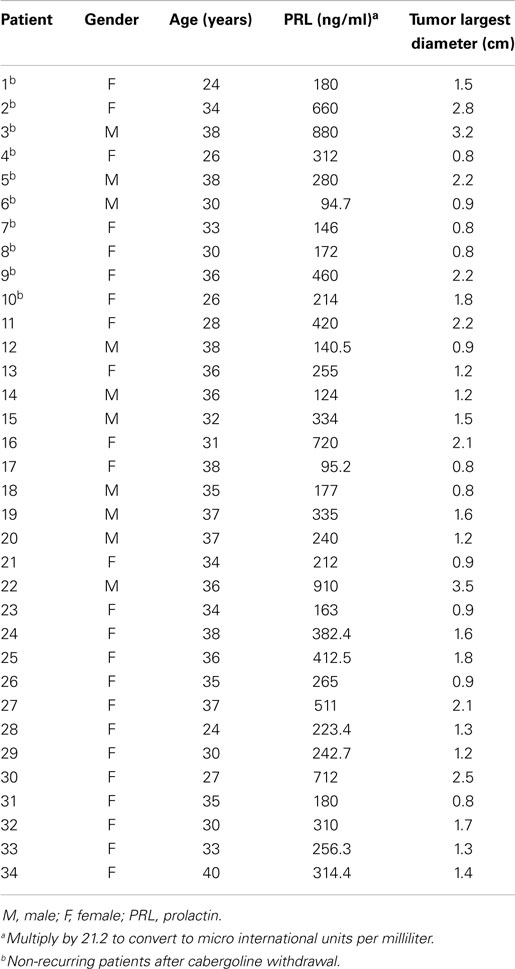
Table 1. Patients characteristics prior to the introduction of cabergoline therapy.
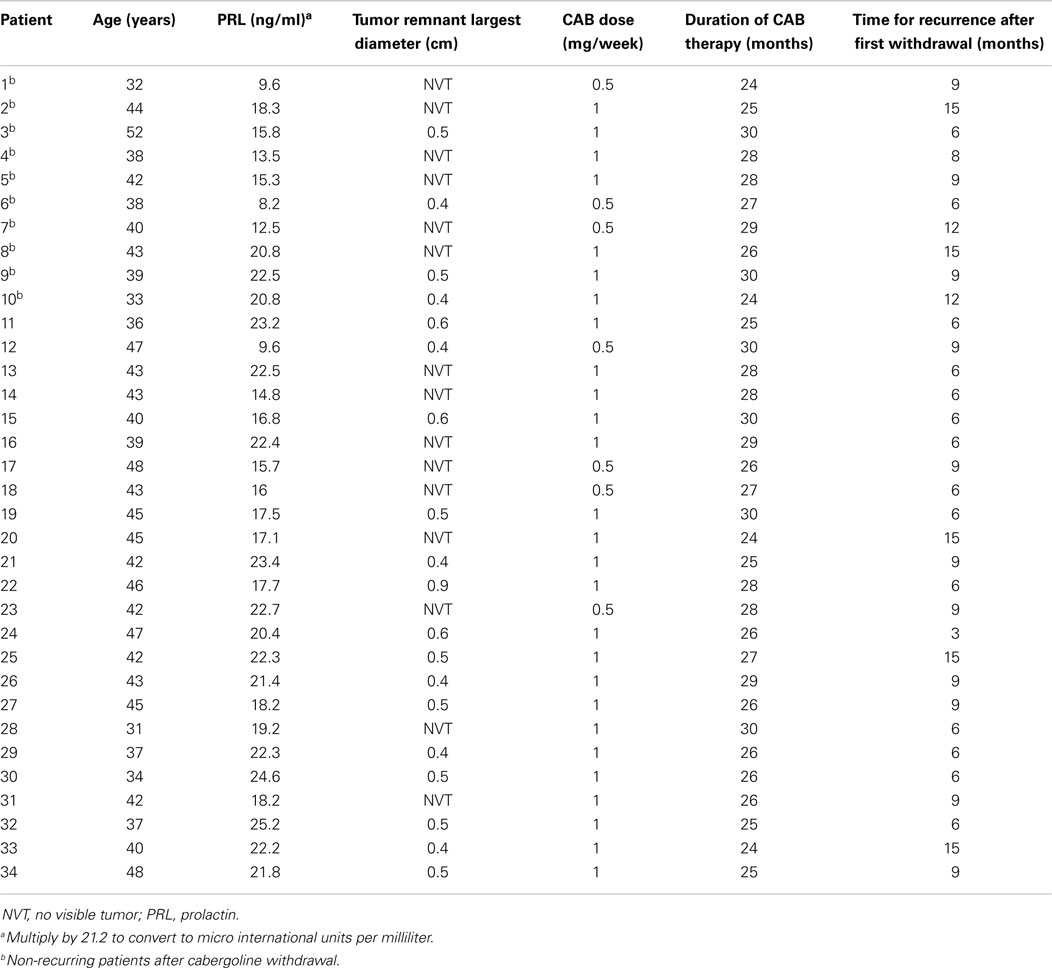
Table 2. Patients characteristics at cabergoline (CAB) therapy withdrawal.
Among the 146 patients not enrolled in the study, many presented with at least two exclusion criteria. The most prevalent were weekly CAB dosage >1 mg (60%), treatment duration <2 years (43%), tumor remnant >1 cm (16%), and concomitant macroprolactinemia (10%).
Responsiveness to Cabergoline Withdrawal
The median follow-up time was 12 months (ranging from 3 to 26 months). Overall, 24 out of 34 patients (70.6%) recurred within 15 months after CAB discontinuation (Figures 1 and 2). Eighteen patients (75%) did so within 12 months, 11 (45.8%) within 9 months, 7 (29.2%) within 6 months, and 2 (8.3%) within 3 months, respectively. Six patients (25%) relapsed after 12 months of follow-up (Figures 1 and 2). Median time to recurrence was 10.5 months. The follow-up for patients who recurred was considered complete at the time of recurrence. Noteworthy, none of the patients reached PRL levels above those found before CAB therapy introduction. Thus, mean PRL levels were significantly lower at the end of the follow-up (132.52 ± 48.3 vs. 366.88 ± 234.14 ng/ml, P < 0.01).
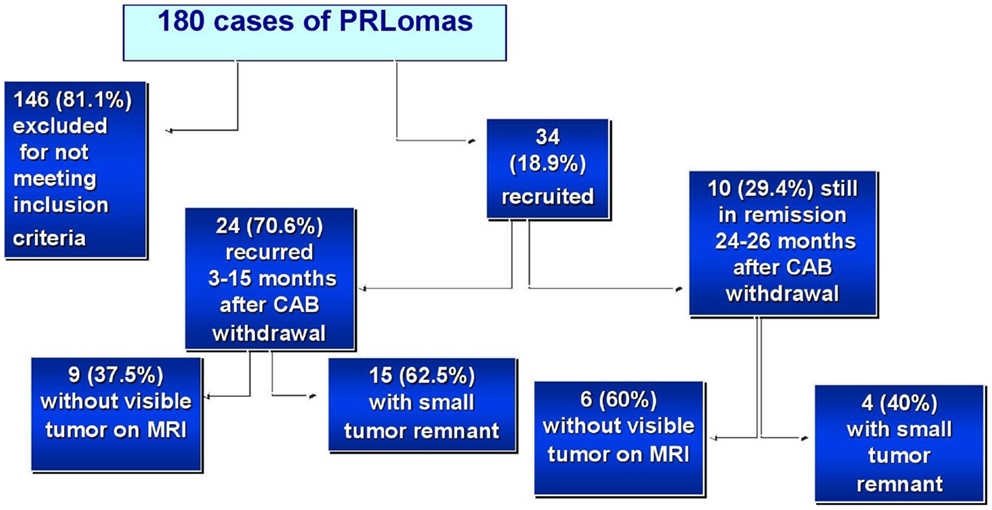
Figure 1. Characteristics and behavior of the patients with prolactinomas (PRLomas) who were evaluated.
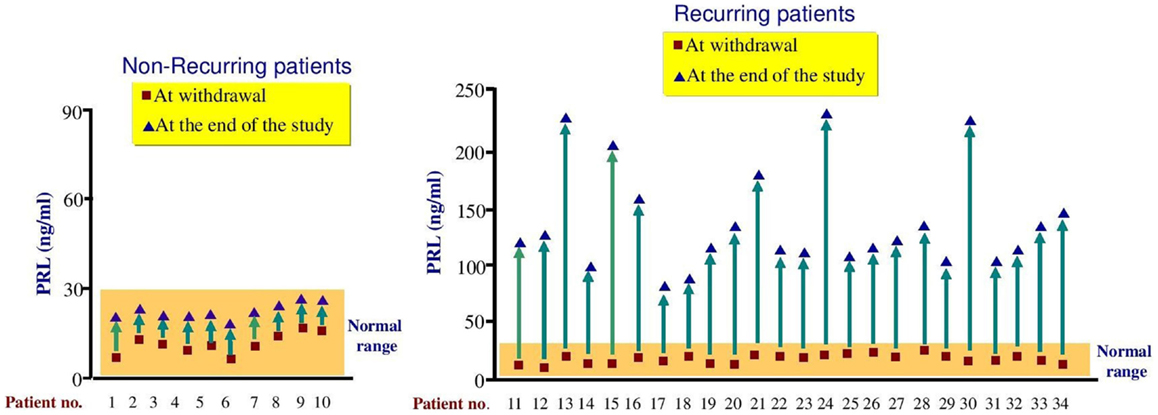
Figure 2. Comparison of PRL levels in non-recurring and recurring patients at withdrawal and at the end of the study. Recurrence was defined as PRL values above the upper limit of normal.
Among recurring female patients, four presented with amenorrhea, eight with amenorrhea and galactorrhea, whereas five remained asymptomatic. Concerning recurring male patients, all developed hypogonadism-related symptoms. None of the tumors enlarged in the patients experiencing recurrence. CAB was restarted in all symptomatic recurring patients.
A total of 10 patients (29.4%) remained without clinical and biochemical evidence of hyperprolactinemia recurrence after a median follow-up time of 24 months (range, 24–26 months). However, as shown in Figure 2, some increase in PRL levels was observed in all these patients, though they remained in the normal range.
Predictors of Responsiveness to Cabergoline Withdrawal
When recurring and non-recurring patients were compared, no significant difference was found concerning age, gender, CAB dose, and duration of CAB therapy before the second withdrawal (Table 3). Moreover, the proportion of patients with micro- (29.2 vs. 40%) and macroadenomas (70.8 vs. 60%) was similar in both groups (P = 0.40) (Table 3), and so was their initial tumor size (1.47 ± 0.65 vs. 1.7 ± 0.89 cm, P = 0.45) (Table 4). Likewise, the mean time of recurrence after first CAB withdrawal did not significantly differ (10.1 ± 3.28 vs. 8.0 ± 3.14 months; P = 0.66).
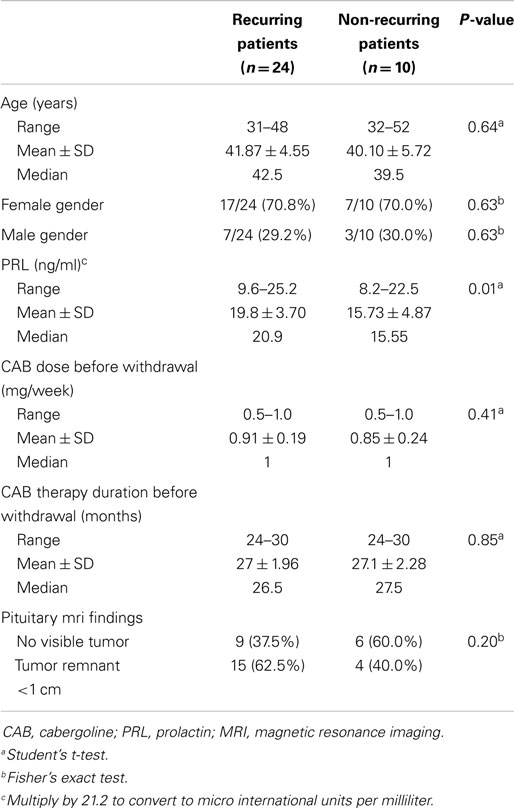
Table 3. Clinical, biochemical, and imaging characteristics in recurring and non-recurring patients at withdrawal.
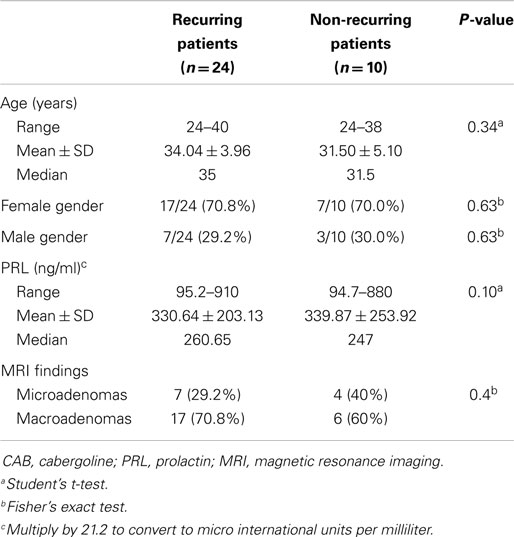
Table 4. Clinical, biochemical, and imaging characteristics in recurring and non-recurring patients at diagnosis.
By contrast, non-recurring patients had significantly lower mean PRL levels (15.73 ± 4.87 vs. 19.8 ± 3.70 ng/ml, respectively, P < 0.01) before second withdrawal (Table 3). Nevertheless, there was a high degree of overlap in PRL values in both groups (Table 3). Moreover, the recurrence rate was lower in subjects without visible tumor on pituitary MRI than in those with small remnant tumor (60 vs. 79%), though the difference was not statistically significant (P = 0.20).
Noteworthy, demographic, biochemical, and imaging features at the prolactinoma diagnosis did not significantly differ when patients who recurred and the ones who remained in remission were compared (Table 4).
Discussion
The optimal duration of therapy with DA for patients with prolactinomas or non-tumoral hyperprolactinemia remains controversial (12). There is however strong and growing evidence that discontinuation of dopamine agonist treatment may be successfully achieved in a selected group of patients treated for at least 2 years (14–17, 19, 20). A recent systematic review and meta-analysis has shown that the pooled proportion of patients with persisting normoprolactinemia after CAB withdrawal was 35% in a random effects model (21). In the series by Karlip et al. (15), which involved 46 patients, the overall recurrence was 54% and the median time to recurrence was 3 months (range, 1(18 months) (15).
In contrast, it is currently unknown how valid and how useful could be a second try to discontinue CAB administration in patients whose first withdrawal did not succeed. Presently, there are only data from a recent pilot prospective two-center study that evaluated 17 patients who had undertaken a second course of CAB treatment for at least 24 additional months (18). During a median follow-up of 6.1 months (ranging from 1 to 60 months) after CAB withdrawal, 11 patients (64.7%) recurred. The estimated overall recurrence rate was 44 events per 100 person-years. Moreover, the estimated cumulative hazard of recurrence was 40% at 6 months and 82% at 12 months (18).
We conducted a prospective trial to evaluate the outcome of a second attempt of CAB withdrawal in 34 patients who met strict selection criteria and have been treated with CAB for 24(30 months (median, 27 months). All patients presented with normal PRL levels, were given CAB doses (1 mg weekly, and had either no visible tumors or small tumor remnants (<1 cm) on MRI. We found that 10 patients (29.4%) were able to maintain normal PRL levels for up to 26 months following CAB withdrawal.
Concerning the 24 recurring subjects, all recurred within 15 months after CAB withdrawal, whereas 18 (75%) did so within 12 months. The median time to recurrence was 10.5 months. Similarly, in the study by Kwancharoen et al. (18), most of the recurrence (59%) also occurred within 1 year, whereas the median time to recurrence was 6 months. Likewise, Karlip et al. (15) had previously reported that 91% of the recurrences after the first withdrawal were observed within the first year of discontinuation. Thus, close clinical monitoring, especially within the first year after withdrawal, should be carried out in all patients in whom CAB therapy is discontinued.
According to previous studies, predictor factors for higher chance of successful CAB withdrawn include lower PRL levels, longer duration of treatment, tumor size (micro- > macroadenomas), previous pituitary radiotherapy or surgery, and pregnancy (5, 12, 13, 15, 16, 22). It has been shown that women with prolactinomas who became pregnant have a higher rate of remission than women without previous pregnancy (22, 23). Moreover, PRL levels are lower after delivery as compared to levels before conception and complete remission of hyperprolactinemia has been reported in 17–37% of women after pregnancy (23). For that reason, we did not include in our study women with history of pregnancy over the last 3 years.
Among our patients, a stratified analysis on clinical, pituitary imaging, and biochemical characteristics, at the beginning of the study and at CAB withdrawal, was unable to detect parameters that could quite accurately identify individuals most likely to respond to treatment discontinuation. However, non-recurring patients had significantly lower mean PRL levels at withdrawal. Furthermore, the recurrence rate was lower in patients without visible tumor remnant on pituitary MRI than in subjects with small tumor remnants (60 vs. 79%), though the difference was not statistically significant (P = 0.20). Accordingly, Hu et al. (21) reported that patients who received the lowest CAB dose and presented a significant reduction in tumor size before withdrawal were more likely to achieve the best success (P < 0.001). Likewise, in the series by Karlip et al. (15), size of tumor remnant prior to withdrawal predicted recurrence (18% increase in risk for each millimeter). By contrast, Kwancharoen et al. (18) could not depict any statistically significant clinical predictors of recurrence, but this may have been influenced by the small number of subjects enrolled in their trial (n = 17).
It was previously reported that a nadir PRL at the time of first withdrawal below 5.4 ng/ml was associated with a lower risk of recurrence (16). In our series, although mean PRL levels before withdrawal were lower in non-recurring subjects, individual PRL values in both groups greatly overlapped (8.2–22.5 vs. 9.6–25.2), as shown in Table 3.
Our study has some limitations. Notably, because of the small number of patients, some or most clinical predictors may not have reached statistically significance. It is also possible that some of the patients presently on remission may recur later on. However, recurrences beyond 2 years after CAB withdrawal have only seldom been reported (15–17, 24). In the largest series to date (n = 200), 63 patients (31.5%) had recurrent hyperprolactinemia, 56% during the first year, 33% during the second year, 11% during the third year, and none thereafter (P < 0.001) (16, 24).
As shown in Table 5, a combined analysis of our findings and those from the study by Kwancharoen et al. (18) would indicate that about 31% of a selected group of patients with prolactinomas treated with CAB for at least additional 24 months could benefit from a second drug discontinuation. In four recent previous studies, which involved 292 patients with micro- or macroprolactinomas, the mean recurrence rate after first CAB withdrawal was 49% [range, 25–69% (14–16)]. Therefore, the chance of achieving a successful second withdrawal seems to be similar to the first one. However, further studies with a greater number of patients and longer-term follow-up are clearly warranted.
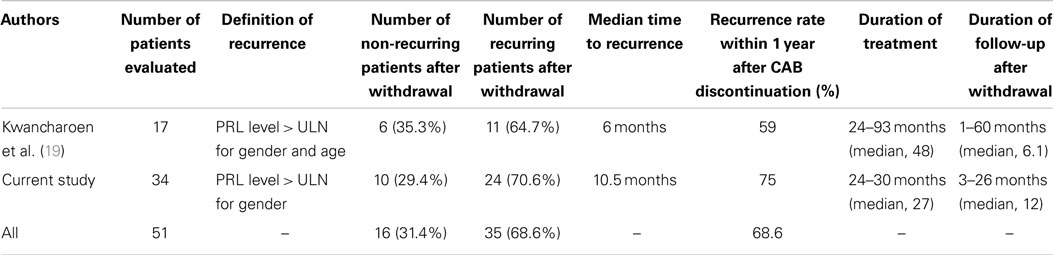
Table 5. Data from two studies specifically designed to evaluate the likelihood of successful second cabergoline (CAB) withdrawal after a failed first attempt in well-controlled patients with prolactinomas.
A likely explanation for the successful second withdrawal could be a longer exposure to CAB therapy and consequently to its antiproliferative and pro-apoptotic effects on pituitary tumor cells, described in several studies (25).
An additional advantage of CAB withdrawal would be to reduce the risk of fibrotic cardiac valvulopathy, which has been associated with the use of DA therapy (26–28), particularly with the higher dosage given to Parkinson’s disease patients (29, 30). However, most studies have not shown an increased prevalence of significant cardiac valve regurgitation in patients with pituitary diseases receiving CAB (13, 31–33).
In conclusion, the findings of the current study yield increasing awareness that a second trial of CAB discontinuation should be attempted in well-selected patients with prolactinomas who display normal PRL levels and tumor remnant <1 cm at low doses (≤1 mg/week). Although our patients have been treated for two or more years, the optimal length of therapy before attempting a second CAB withdrawal still needs to be established. Patients with lower PRL levels and no visible tumor on MRI seemed to be the most likely to benefit from this approach but it was also effective in subjects with small tumor remnants. It is essential however to closely follow-up these patients and reinstitute therapy promptly in symptomatic recurrent ones.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Vilar L, Fleseriu M, Bronstein MD. Challenges and pitfalls in the diagnosis of hyperprolactinemia. Arq Bras Endocrinol Metabol (2014) 58:9–22. doi: 10.1590/0004-2730000003002
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
2. Gillam MP, Molitch ME, Lombardi G, Colao A. Advances in the treatment of prolactinomas. Endocr Rev (2006) 27:485–534. doi:10.1210/er.2005-9998
3. Fernandez A, Karavitaki N, Wass JAH. Prevalence of pituitary adenomas: a community-based, cross-sectional study in Banbury (Oxfordshire, UK). Clin Endocrinol (Oxf) (2010) 72:377–82. doi:10.1111/j.1365-2265.2009.03667.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
4. Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A. High prevalence of pituitary adenomas: a crosssectional study in the province of Liege, Belgium. J Clin Endocrinol Metab (2006) 91:4769–75. doi:10.1210/jc.2006-1668
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
5. Colao A. Pituitary tumours: the prolactinoma. Best Pract Res Clin Endocrinol Metab (2009) 23:575–96. doi:10.1016/j.beem.2009.05.003
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
6. dos Santos Silva CM, Barbosa FR, Lima GA, Warszawski L, Fontes R, Domingues RC, et al. BMI and metabolic profile in patients with prolactinoma before and after treatment with dopamine agonists. Obesity (Silver Spring) (2011) 19:800–5. doi:10.1038/oby.2010.150
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
7. Vilar L, Freitas MC, Naves LA, Casulari LA, Azevedo M, Montenegro R Jr, et al. Diagnosis and management of hyperprolactinemia: results of a Brazilian multicenter study with 1234 patients. J Endocrinol Invest (2008) 31:436–44. doi:10.1007/BF03346388
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
8. Klibanski A. Clinical practice. Prolactinomas. N Engl J Med (2010) 362:1219–26. doi:10.1056/NEJMcp0912025
9. Verhelst J, Ab R, Maiter D, van den Bruel A, Vandeweghe M, Velkeniers B, et al. Cabergoline in the treatment of hyperprolactinaemia: a study in 455 patients. J Clin Endocrinol Metab (1999) 84:2518–22. doi:10.1210/jcem.84.7.5810
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
10. Ferrari C, Barbieri C, Caldara R, Mucci M, Codecasa F, Paracchi A, et al. Long-lasting prolactin-lowering effect of cabergoline, a new dopamine agonist, in hyperprolactinemic patients. J Clin Endocrinol Metab (1986) 63:941–5. doi:10.1210/jcem-63-4-941
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
11. Ferrari C, Paracchi C, Mattei AM, de Vincentiis S, D’Alberton A, Crosignani P. Cabergoline in the long-term therapy of hyperprolactinemic disorders. Acta Endocrinol (Copenh) (1992) 126:489–94.
12. Pereira AM. Update on the withdrawal of dopamine agonists in patients with hyperprolactinemia. Curr Opin Endocrinol Diabetes Obes (2011) 18:264–8. doi:10.1097/MED.0b013e328347c94a
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
13. Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, et al. Diagnosis and treatment of hyperprolactinemia: an endocrine society clinical practice guideline. J Clin Endocrinol Metab (2011) 96:273–88. doi:10.1210/jc.2010-1692
14. Anagnostis P, Adamidou F, Polyzos SA, Efstathiadou Z, Karathanassi E, Kita M. Long term follow-up of patients with prolactinomas and outcome of dopamine agonist withdrawal: a single center experience. Pituitary (2012) 15:25–9. doi:10.1007/s11102-011-0303-6
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
15. Kharlip J, Salvatori R, Yenokyan G, Wand GS. Recurrence of hyperprolactinemia after withdrawal of long-term cabergoline therapy. J Clin Endocrinol Metab (2009) 94:2428–36. doi:10.1210/jc.2008-2103
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
16. Colao A, Biswas M, Di Sarno A, Guerra E, Pivonello R, Cappabianca P, et al. Predictors of remission of hyperprolactinaemia after long-term withdrawal of cabergoline therapy. Clin Endocrinol (Oxf) (2007) 67:426–33. doi:10.1111/j.1365-2265.2007.02905.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
17. Biswas M, Smith J, Jadon D, McEwan P, Rees DA, Evans LM, et al. Long-term remission following withdrawal of dopamine agonist therapy in subjects with microprolactinomas. Clin Endocrinol (Oxf) (2005) 63:26–31. doi:10.1111/j.1365-2265.2005.02293.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
18. Kwancharoen R, Auriemma RS, Yenokyan G, Wand GS, Colao A, Salvatori R. Second attempt to withdraw cabergoline in prolactinomas: a pilot study. Pituitary (2014) 17:451–6. doi:10.1007/s11102-013-0525-x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
19. Vilar L, Naves LA, Casulari LA, Azevedo MF, Albuquerque JL, Serfaty FM, et al. Management of prolactinomas in Brazil: an electronic survey. Pituitary (2010) 13:199–206. doi:10.1007/s11102-010-0217-8
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
20. Dekkers OM, Lagro J, Burman P, Jørgensen JO, Romijn JA, Pereira AM. Recurrence of hyperprolactinemia after withdrawal of dopamine agonists: systematic review and metaanalysis. J Clin Endocrinol Metab (2010) 95:43–51. doi:10.1210/jc.2009-1238
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
21. Hu J, Zheng X, Zhang W, Yang H. Current drug withdrawal strategy in prolactinoma patients treated with cabergoline: a systematic review and meta-analysis. Pituitary (2014). doi:10.1007/s11102-014-0617-2
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
22. Bajwa SK, Bajwa SJ, Mohan P, Singh A. Management of prolactinoma with cabergoline treatment in a pregnant woman during her entire pregnancy. Indian J Endocrinol Metab (2011) 15(Suppl 3):S267–70. doi:10.4103/2230-8210.84883
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
23. Crosignani PG, Mattei AM, Scarduelli C, Cavioni V, Boracchi P. Is pregnancy the best treatment for hyperprolactinemia? Hum Reprod (1989) 4:910–2.
24. Colao A, Di Sarno A, Cappabianca P, Di Somma C, Pivonello R, Lombardi G. Withdrawal of long-term cabergoline therapy for tumoral and nontumoral hyperprolactinemia. N Engl J Med (2003) 349:2023–33. doi:10.1056/NEJMoa022657
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
25. Marazuela M, Ramos-Leví A, Sampedro-Núñez M, Bernabeu I. Cabergoline treatment in acromegaly: pros. Endocrine (2014) 46:215–9. doi:10.1007/s12020-014-0206-1
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
26. Colao A, Galderisi M, Di Sarno A, Pardo M, Gaccione M, D’Andrea M, et al. Increased prevalence of tricuspid regurgitation in patients with prolactinomas chronically treated with cabergoline. J Clin Endocrinol Metab (2008) 93:3777–84. doi:10.1210/jc.2007-1403
27. Elenkova A, Shabani R, Kalinov K, Zacharieva S. Increased prevalence of subclinical cardiac valve fibrosis in patients with prolactinomas on long-term bromocriptine and cabergoline treatment. Eur J Endocrinol (2012) 167:17–25. doi:10.1530/EJE-12-0121
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
28. Yedinak CG, McCartney S, Dillard TH, Wei KS, Fleseriu M. Case report: reversible cabergoline-associated cardiac valvulopathy post drug discontinuation. F1000Res (2014) 25(3):171. doi:10.12688/f1000research.3062.1
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
29. Peralta C, Wolf E, Alber H, Seppi K, Müller S, Bösch S, et al. Valvular heart disease in Parkinson’s disease vs. controls: an echocardiographic study. Mov Disord (2006) 21:1109–13. doi:10.1002/mds.20887
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
30. De Vecchis R, Esposito C, Ariano C. Cabergoline use and risk of fibrosis and insufficiency of cardiac valves. Meta-analysis of observational studies. Herz (2013) 38:868–80. doi:10.1007/s00059-013-3816-0
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
31. Auriemma RS, Pivonello R, Perone Y, Grasso LF, Ferreri L, Simeoli C, et al. Safety of long-term treatment with cabergoline on cardiac valve disease in patients with prolactinomas. Eur J Endocrinol (2013) 169:359–66. doi:10.1530/EJE-13-0231
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
32. Bogazzi F, Buralli S, Manetti L, Rafaelli V, Cigni T, Lombardi M, et al. Treatment with low doses of cabergoline is not associated with increased prevalence of cardiac valve regurgitation in patients with hyperprolactinaemia. Int J Clin Pract (2008) 62:1864–9. doi:10.1111/j.1742-1241.2008.01779.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
33. Drake WM, Stiles CE, Howlett TA, Toogood AA, Bevan JS, Steeds RP, et al. A cross-sectional study of the prevalence of cardiac valvular abnormalities in hyperprolactinemic patients treated with ergot-derived dopamine agonists. J Clin Endocrinol Metab (2014) 99:90–6. doi:10.1210/jc.2013-2254
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: cabergoline, dopamine agonists, prolactinoma, second withdrawal, recurrence
Citation: Vilar L, Albuquerque JL, Gadelha PS, Rangel Filho F, Siqueira AMC, da Fonseca MM, Viana KF, Gomes BS and Lyra R (2015) Second attempt of cabergoline withdrawal in patients with prolactinomas after a failed first attempt: is it worthwhile? Front. Endocrinol. 6:11. doi: 10.3389/fendo.2015.00011
Received: 26 November 2014; Accepted: 17 January 2015;
Published online: 04 February 2015.
Edited by:
Mônica Gadelha, Federal University of Rio de Janeiro, BrazilReviewed by:
Hidenori Fukuoka, Kobe University Hospital, JapanLeandro Kasuki, Federal University of Rio de Janeiro, Brazil
Copyright: © 2015 Vilar, Albuquerque, Gadelha, Rangel Filho, Siqueira, da Fonseca, Viana, Gomes and Lyra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucio Vilar, Rua Clovis Silveira Barros, 84/1202, Boa Vista, Recife (PE), CEP 50050-270, Brazil e-mail:bHZpbGFyZkBnbWFpbC5jb20=