 Claire Briet1,2*
Claire Briet1,2* Karine Braun1Michel Lefranc3,4Patrick Toussaint3,4Bernard Boudailliez1,4Hélène Bony1
Karine Braun1Michel Lefranc3,4Patrick Toussaint3,4Bernard Boudailliez1,4Hélène Bony1- 1Department of Pediatrics, University Medical Center, Amiens, France
- 2Department of Endocrinology, Diabetology and Nutrition, Institut MITOVASC, INSERM U1083, Angers University, University Medical Center, Angers, France
- 3Department of Neurosurgery, University Medical Center, Amiens, France
- 4Department of Medicine, University of Picardie Jules Verne, Amiens, France
Objective: The aim of this study was to evaluate the frequency of hypopituitarism following TBI in a cohort of children who had been hospitalized for mild TBI and to identify the predictive factors for this deficiency.
Design: A prospective study was conducted on children between 2 and 16 years of age who had been hospitalized for mild TBI according to the Glasgow Coma Scale between September 2009 and June 2013. Clinical parameters, basal pituitary hormone assessment at 0, 6, and 12 months, as well as a dynamic testing (insulin tolerance test) 12 months after TBI were performed.
Results: The study included 109 children, the median age was 8.5 years. Patients were examined 6 months (n = 99) and 12 months (n = 96) after TBI. Somatotropic deficiency (defined by a GH peak <20 mUI/l in two tests, an IGF-1 <-1SDS and a delta height <0SDS) were confirmed in 2 cases. One case of gonadotrophic deficiency occurred 1 year after TBI among 13 pubertal children. No cases of precocious puberty, 5 cases of low prolactin level, no cases of corticotropic insufficiency (cortisol peak <500 nmol/l) and no cases diabetes insipidus were recorded.
Conclusion: Pituitary insufficiency was present 1year after mild TBI in about 7% of children. Based on our results, we suggest testing children after mild TBI in case of clinical abnormalities. i.e., for GH axis, IGF-1, which should be assessed in children with a delta height <0 SDS, 6 to 12 months after TBI, and a dynamic GH testing (preferentially by an ITT) should be performed in case of IGF-1 <-1SDS, with a GH threshold at 20 mUI/L. However, if a systematic pituitary assessment is not required for mild TBI, physicians should monitor children 1 year after mild TBI with particular attention to growth and weight gain.
Introduction
Traumatic brain injury (TBI) is a serious public health concern. Indeed, it is the principal cause of mortality and disability in children and young adults (1). Considering that the survival rate of children is higher than that of adults following severe TBI, studying TBI consequences is of interest (2). Indeed, mild TBI represents 80% of total TBI in children (1). In the last 15 years, retrospective studies have shown that pituitary deficiency is very common in children after TBI, but the frequency varies widely among studies (from 0.8 to 90% of children) (3–13).In these studies, GH deficiency (GHD) is the most common pituitary defect, but the diagnosis is based on biological data only. In the KIMS database (Pfizer International Metabolic Database reporting a follow up of patients under GH treatment), TBI accounted for 4% of GHD treated during childhood (14).
The prevalence of a pituitary deficiency after TBI in children cannot be reliably determined from the few published prospective studies, because of the small number of patients and partial information on the proportion of mild to moderate TBI (Table 1). The largest prospective study, including 87 children, focused on severe TBI (20). It interesting to note that almost all studies have concluded that TBI severity is not predictive of a pituitary deficiency (15, 20). Therefore, we focused our study on mild TBI.
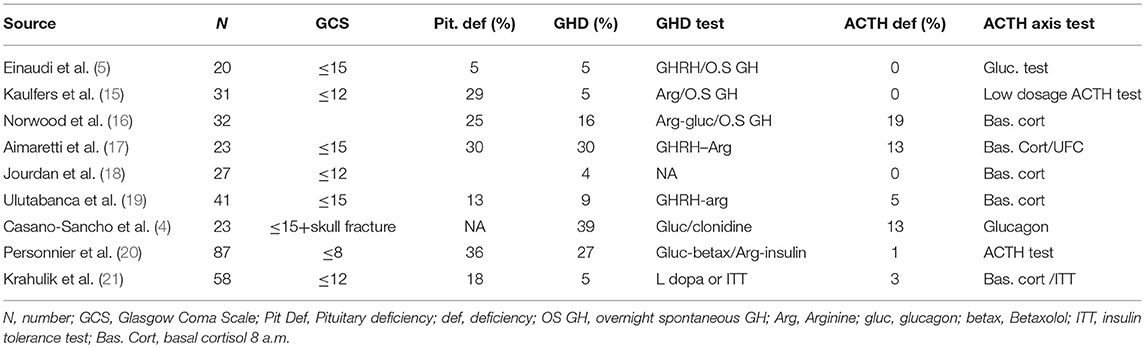
Table 1. Prospective pediatric studies assessing pituitary deficiency 1 year after TBI.
Here, we report the results of a large prospective study on 109 children (2–16 years) who had been hospitalized for mild TBI. The primary objective was to evaluate the prevalence of pituitary deficiencies in this cohort. The secondary objective was to determine predictive parameters of endocrine deficiency.
Subjects and Methods
Subjects
Inclusion criteria were age between 2 and 16 years old and admission to the Neurosurgery Unit of the University Hospital of Amiens (France) for medical supervision between September 2009 and November 2013 for TBI. The criteria for hospitalization in Neurosurgery after TBI in children in our hospital were: having experienced two episodes of vomiting, headaches, loss of consciousness, Glasgow Coma Scale <15, or neurological symptoms. The patients who met the criteria, agreed to participate in the clinical trial and came to the hospital for at least one evaluation (6 or 12 months after TBI) were included. Written and informed consent was obtained from the parents of all participants. Exclusion criteria were: children with a history of endocrine disease or TBI, or children who lived more than 150 km from our hospital.
The study protocol was approved by the French Ethics Committee (Comité de Protection des Personnes-2008-A00268-47), and the French General Direction of Health.
Study Design
The Glasgow Coma Scale (GCS) was used to rank TBI as mild (GCS>12) (22, 23). Clinical parameters (height, weight, pubertal stage), were assessed at diagnosis and 6 and 12 months after TBI. Baseline pituitary function (IGF-I, FSH-LH, estradiol for girls, testosterone for boys, TSH-FT4, PRL, cortisol-ACTH, plasmatic osmolarity, and urinary osmolarity) was assessed at diagnosis and 6 and 12 months after TBI. Bone age was assessed at diagnosis and at 12 months. At 12 months, an insulin tolerance test (ITT) was performed for somatotropic and corticotropic axis assessment, given that it is considered the “gold standard” with fewer false positive results (24).
After overnight fasting, intravenous insulin (0.075 UI per kilogram for body weight below 15 kg, otherwise 0.1 units per kilogram) was administered to patients and samples were taken for blood glucose, cortisol and growth hormone (GH) measurement at 0, 15, 30, 45, 60, 90, and 120 min after injection.
In the event of a seizure at the time of TBI, an arginine test was performed for somatotropic evaluation, as well as a synacthen test (250 μg IV with cortisol dosage at −30, 30, and 60 min) for corticotropic evaluation.
Dynamic testing of the corticotropic and somatotropic axis was performed 12 months after TBI. Therefore, the prevalence of pituitary hormone deficiencies is reported only at 12 months.
Hormonal Assessment
GH, IGF-1, FT4 were assessed by radioimmunoassay (CisBio International for GH and IGF-1, Beckman-Coulter for FT4) with a sensitivity of 0.03 mUI/ml, 2 ng/ml, and 0.5 pmol/l, respectively. Cortisol was assessed using a Beckman Access kit with a sensitivity of 1.1 nmol/l. ACTH, prolactin, LH and FSH were assessed with immunoradiometric assays (Beckman Coulter) with a sensitivity of 1.2 pg/ml, 0.5 ng/ml, 0.2 UI/ml, 0.2 UI/ml, respectively. Estradiol was assessed with E2—Coatria, CisBio International with a sensitivity of 4 pg/ml.
Inter/intra-assay coefficients of variation were 4.5%/1.7% for GH, 3.8%/3.8% for IGF-1, 7.5%/8.3% for FT4, 7.9%/6.7% for cortisol, 9.6%/9.1% for ACTH, 8%/2.8% for prolactin, 4.9%/3.9% for estradiol, 15%/14.8% for testosterone, 3.7%/6.7% for LH, and 6.3%/2.6% for FSH.
The pediatric normal values published in the literature were used to diagnose pituitary dysfunction:
– Diabetes insipidus was suspected in cases of nocturnal drinking combined with low morning urine osmolarity (<300 mmol/kg) (25, 26).
– Hypocortisolism was defined as a peak of cortisol <500 nmol/l with documented hypoglycemia (blood glucose <2.2 mmol/l (27–29).
– Thyrotropin insufficiency as FT4 level below the normal range (from <11.96 to 14.29 pmol/l according to age) and normal or low TSH level (normal value from 0.57–5.51 to 0.5–4.9 mUI/l according to age) (30, 31).
– Hypogonadotropic hypogonadism was diagnosed
◦ in pubertal girls: by secondary amenorrhea or alteration of menses regularity (from regular menses to irregular menses) after age of 13 and low estradiol levels with low FSH and LH levels (<1 and 0.4 mUI/l, respectively (32),
◦ in pubertal boys: with complete puberty (genital and pubertal stage 5) by erectile dysfunction (lack of spontaneous morning erection) after the age of 15 and a testosterone below 10.4 nmol/l (3 ng/ml) with low FSH (< 1.2 mUI/l) and LH (2.4 mUI/l) (32, 33).
Hypogonadotropic hypogonadism was not evaluable in prepubertal children, for these children, signs of precocious puberty were investigated: acceleration of height velocity, advanced bone age, and enlargement of mammary gland before 8 years of age for girls or increased testes volume (> 25 × 20 mm or 4 ml) before 9 years for boys (30, 34).
– The somatotropic axis was evaluated by an ITT with documented hypoglycemia (blood glucose <2.2 mmol/l) (35, 36). In the event of GH peak <20 mUI/l, a second test was performed (arginine test) within the following 3 months. The arginine test was performed with a 30-min IV perfusion of arginine 0.5 g/kg (maximum 25 g), with blood samples every 15 min from 30 to 90 min. IGF-1 was expressed in standard deviation for age, sex, and pubertal stage (SDS). We explored the consequences of 3 definitions of GHD according to various criteria:
◦ Level 1: biochemical GHD defined by two GH peaks <20 mUI/L in response to stimulation tests. Two stimulation tests are used because of the low specificity of dynamic testing (37). The cut off used for GHD treatment in children in France is 20 mUI/l (6.7 μg/l) which is approved in the literature (38, 39). However, if there is a consensus for GHD diagnosis in adults with a GH peak after ITT <3 μg/l (9 mUI/l) and 6 μg/l (18 mUI/) in the transition period, there is no consensus for GH cut-off after ITT in children (16, 19),
◦ Level 2: biochemical GHD + low IGF-1: two GH peaks <20 mUI/L in response to stimulation tests and IGF-1 <- 1 SDS, as recommended by the GH Research Society as a way of counterbalancing the low specificity of GH stimulation tests, especially in obese children and because most children with GHD have an IGF-1 below−1 SDS as described in the literature (40–43),
◦ Level 3: biochemical GHD + low IGF-1 + growth deficiency: two GH peaks <20 mUI/L in response to stimulation tests, an IGF-1 <-1 SDS and a decrease in height velocity (delta height < 0 SDS). We used these stringent criteria for GHD diagnosis as a way of avoiding any false positive diagnoses of GHD and because GHD had a deficiency on growth in children.
We presented the results for the three levels of GHD mainly for the discussion of GHD frequency according to these levels and comparison with previous studies. However, for the diagnosis of GHD in our cohort, the most stringent criteria (GHD level 3) were adopted.
– Hyperprolactinemia was defined by PRL above 20 ng/ml, hypoprolactinemia was defined by a PRL below 3 ng/ml.
– Bone age was assessed through an X-ray of the left hand, finger and wrist and was calculated by the same pediatrician according to the Greulich and Pyle atlas at M0 and M12.
TBI Severity
Mild TBI is defined by a CGS > 12 and was further characterized as complicated or uncomplicated mild TBI, according to the presence or absence of CT-Scan abnormalities such as a depressed skull fracture or other trauma-related intracranial abnormalities (e.g., hemorrhage, contusion, and edema) (44).
Statistical Analysis
The sample size calculation required was one hundred and twenty patients, comparing those who have one or more pituitary deficiency to those without, to ensure a statistical power of 80% for an odd ratio of 1.5 to 2.5 (prevalence of one or more pituitary deficiencies at around 20% according to the literature review) with 10% lost to follow up.
Data were expressed as median, range and percentage of abnormal responses compared to normative cut-off levels.
Statistical analysis in various groups was performed using the Wilcoxon rank-sum test. The percentages were compared using the chi-squared test, with Fisher correction.
The predictive factor for developing a pituitary deficiency was calculated using logistic regression analysis including age, sex, initial presentation (GCS score, vomiting, scan abnormalities, loss of consciousness), pubertal status and BMI, adjusted with prealbumin levels as a marker of malnourishment which can modify GH response to stimulation tests and IGF-1 levels. We excluded children with previous TBI and endocrine disorders as potential confounders. In the same way, we excluded children under 2 years of age to avoid shaken baby syndrome.
A two-tailed p value < 0.05 was considered statistically significant. The statistical analysis was performed using GraphPad Prism version 4 software for Windows (GraphPad Software, San Diego, California, USA) and with Statistical Analysis System version 9.2 software for Windows for the logistic regression analysis (SAS Software, L9.2G, North Carolina, USA).
Results
Patients
Of the 139 children admitted to the Neurosurgery Unit between September 2009 and June 2013, 30 were excluded: 1 had a history of precocious puberty, 6 lived too far from the university hospital to participate in the follow-up, 14 parents declined to participate, and 9 children did not return for a 6-month and 12-month evaluation (Supplemental Figure 1).
The characteristics of the 109 patients included are summarized in Table 2. The median age was 8.5 years, and 73% were at pubertal stage 1 at M0. Ninety-Nine and Ninety-Six patients were evaluated at Six and Twelve months, respectively. The median height of the total group was 0.53 SDS (−1.9 to 3.2), median weight 0.03 SDS (−1.7 to 6.2) and median BMI −0.49 SDS (−2.8 to 10).
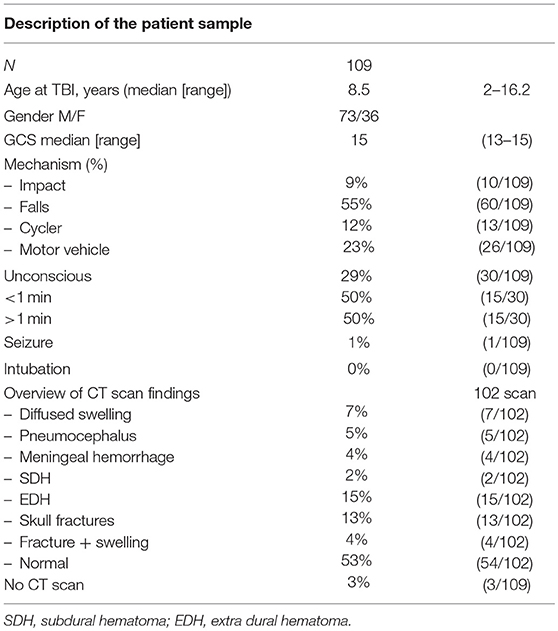
Table 2. Demographics, injury characteristics and imaging results of the 109 patients at M0 (102 CT scan realized).
Endocrine Evaluation
Somatotropic Axis
One year after TBI, 10 out of 96 children had GHD level 1 (two tests with GH peak <20 mUI/l). Among these 10 children, 3 had IGF-1 <-1 SDS and were labeled GHD level 2. Among them, 2 had delta height <0 SDS between M0 and M12 (GHD level 3). Between the two patients, one had a GH peak <10 mUI/l. No IGF-1 below−2 SDS was found in children with GHD regardless of the level. The median height of children with GHD was 0.53 SDS (−0.27 to 1.8) and the median BMI 0.28 SDS (−0.18 to 3.6). For the complete description of children with GHD level 1, 2, and 3 see Table 3.
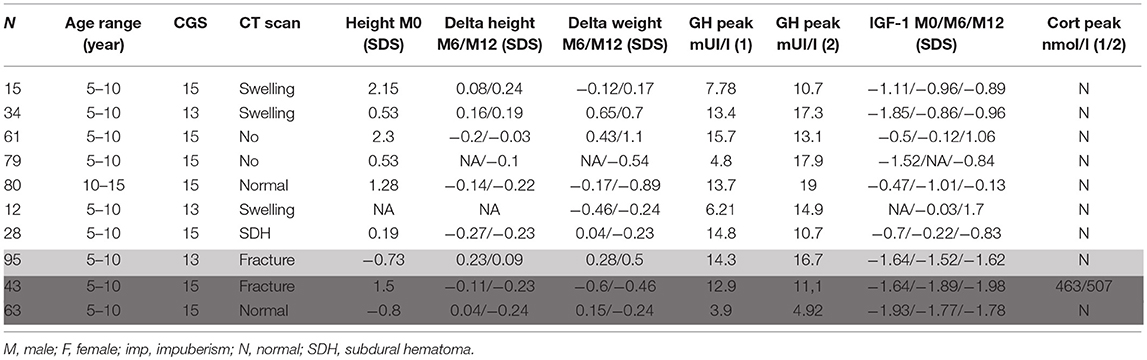
Table 3. Auxological and hormonal data of patients with two stimulated GH peaks below 20 mUI/l (GHD level 1 in white), with two peaks below 20 mUI/l and IGF-1 <-1SDS (GHD level 2 in light gray) and with the previous criteria and delta height <0 (GHD level 3 dark gray).
By targeting children with a growth deficiency at M12 (with a delta height below 0 SDS), 63 children would have been selected. Among them 24 had an IGF-1 < −1SDS. Among the 24 children, 2 children had a GH peak after two stimulation tests < 20 mUI/l (GHD level 3). This strategy for screening children after TBI would have 100% sensibility and 34.4% specificity.
Corticotropic Axis
The ITT revealed 28 corticotropic deficiencies, according to the 500 nmol/l threshold, among the 96 children tested. An ACTH stimulation test was performed on 18 children within 3 months, none had a cortisol peak <500 nmol/l.
Thyrotropin, Axis
Upon first investigation, immediately after TBI, there were 12 cases of thyrotropin deficiency among 109 patients; all of whom recovered at 6 months (Figure 1). A subclinical hypothyroidism (elevated TSH and normal FT3 and FT4) was found in one case at M0 and 2 cases at M12.
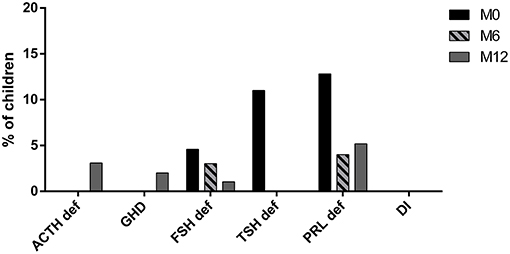
Figure 1. Pituitary evaluation at traumatism (M0), 6 months (M6) and 12 months (M12) after TBI. (PRL def, prolactin deficiency; TSH def, TSH deficiency; FSH def, gonadotropin deficiency; DI, diabetes insipidus; GHD, GH deficiency; ACTH def, ACTH deficiency).
Gonadotropin, Prolactin Axis and Posterior Pituitary Evaluation
At M0, 14 of 109 children had a prolactin deficit (10 had recovered at 6 months and 1 new deficiency was diagnosed at 12 months). Out of 10 children who were pubertal at presentation, 5 had a gonadotropin deficiency (3 recovered at 6 months and 1 recovered at 12 months). At 12 months, one case of gonadotropin deficiency persisted among 13 late adolescents. There were no cases of precocious puberty among 62 prepubertal children. Morning urine osmolarity was low in one child who began drinking during the night, but the suspicion of DI was not confirmed by the total urinary volume (less than 50 ml/kg) (Figure 1).
To summarize the hormonal results, at 12 months, 7 out of the 96 children (7.2%) tested had one or more pituitary deficiencies except for the gonadotropic axis which was evaluated according to age. Comparison of the demographic, clinical, biochemical and radiological data in these patients highlighted no differences between patients with a normal pituitary function and patients with pituitary deficiencies in terms of age, gender, CT scan abnormalities, unconsciousness at presentation, weight gain, delta height gain, CGS.
Influence of TBI Severity
In our study, pituitary deficiency occurred even in mild TBI with a CGS score at 15 (Figure 2).
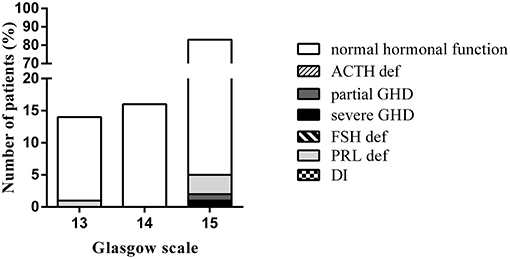
Figure 2. Comparison of pituitary function at 12 months, according to the Glasgow Coma Scale. (DI, diabetes insipidus; FSH def, gonadotropin deficiency; PRL def, prolactin deficiency; ACTH def, ACTH deficiency; GHD, Growth hormone deficiency).
When splitting the cohort into two subgroups: complicated or uncomplicated mild TBI, according to the presence or absence of CT-Scan abnormalities, there were no differences between the two subgroups (Figure 3).
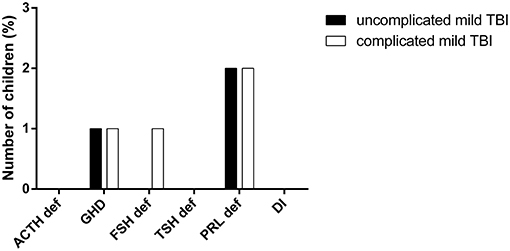
Figure 3. Comparison of hormonal deficiencies in complicated or uncomplicated mild TBI. (PRL def, prolactin deficiency; TSH def, TSH deficiency, FSH def, gonadotropin deficiency, DI, diabetes insipidus, GHD, GH deficiency, ACTH def, ACTH deficiency).
Predictive Factors
Clinical and biological parameters at M0 (vomiting, GCS, scan abnormalities, loss of consciousness, pubertal status, BMI, age, hormonal level at TBI) were not predictive of pituitary insufficiency.
Discussion
We prospectively assessed pituitary hormonal deficiency in a cohort of children and adolescents who had been hospitalized for mild TBI.
Twelve months after TBI, we found that 7.2% of patients suffered from pituitary deficiencies which is much less than previous prospective studies (Table 1) have recorded. These differences can be explained by the stimulation test used (ITT), which is more sensitive, and by the stringent criteria used to define pituitary deficiency (GHD level 3 and cortisol peak <500 nmol/l after two stimulation tests). We choose a cut-off for the GH peak of 20 mUI/l (6.7 μg/l) as recommended by the GH research society and as used in France for GH treatment (40). GHD, as assessed by a GH peak below 20 mUI/l following two consecutive stimulation tests, an IGF-1 <-1SDS and a delta height <0SDS (GHD level 3) was present in 2 children who were treated. In the literature, GHD is the most frequent pituitary deficiency, but the definition does not include the growth defect in most published research. Furthermore, the cut off values for GH peak and the stimulation tests were often different (45, 46).
A GHD level 1 or 2 with normal growth following TBI in children is common in the literature. Considering GHD when only a hormonal deficiency has an impact on growth, the percentage of children with a diagnosis of GHD falls from 10 to 2% in our study, and from 39 to 3.8%, 5 to 0% or 30 to 2% in the series reported by Casano Sancho et al., Kaulfers et al., Personnier et al., respectively (4, 15, 20). By combining a low level of IGF-1 and a GH peak below 20 mUI/l, as recommended by the GH Research Society (47), 3 children fulfilled the criteria for GHD in our study (48). Given that many children had a high BMI in our cohort, which leads to physiologically low GH peaks in response to stimulation, the addition of a low IGF-1 as a criterion of GHD could be a discriminant in this subpopulation. However, the discrepancy between two dynamic tests can reach 50% and children with normal growth can have a low GH peak following a GH stimulation test (from 44 to 61% for children Tanner 1 and 2, respectively), IGF-1 measurement has a high variability and a GHD with normal IGF-1 is possible (24, 37, 49). It is therefore difficult to define GHD after TBI: should it be determined by dynamic testing alone, or by the combination of dynamic testing, basal IGF-1 and/or with a decreased delta height? This is an important point as in adults, the lack of impaired growth as criterion for GHD, may partially explain the differences in GHD frequencies after TBI between children and adults (50).
Bellone et al. recommend the evaluation of height velocity and basal hormonal testing at 6 and 12 months after TBI and performing dynamic testing only on children with impaired height velocity (<25e percentile) (6). With regard to our results, we recommend monitoring height velocity at 0, 6, and 12 months after TBI, and measuring IGF-1 in children with a delta height <0 SDS 6 or 12 months after TBI. In case of IGF-1 <-1 SDS, a dynamic testing should be proposed, preferably an ITT in absence of contraindication with a threshold of GH at 20 mUI/l. With this strategy, 63 children would have been selected and tested for IGF-1. Among them 24 children with an IGF-1 < −1SDS would have been tested for GH secretion. Among the 24 children, 2 children with GHD would have been diagnosed.
In our study the incidence of cortisol deficiency was 29% with a threshold of 500 nmol/l, which was not confirmed following a second test. Three children had a second cortisol peak between 500 and 550 nmol/l. In the literature, the frequency of cortisol deficiencies after TBI is variable (0 to 19%), mainly because different stimulation tests and variable cut off's are used (summarized in Table 1).
In contrast to other studies, we did not observe any precocious or delayed puberty, probably due to the mean age of the cohort (with a majority of Tanner 1 children) and the short follow-up (5, 9, 15). A gonadotrophic deficiency was diagnosed in one girl with an impaired cycle, low estradiol and low FSH-LH. There were only 13 pubertal children at 12 months, it is therefore difficult to draw any conclusions on the frequency of abnormalities for this axis. A prolonged follow-up should provide further information.
In our study, pituitary deficiency is not correlated with a lower GCS at TBI, as in some prospective studies (15, 20). TBI severity is commonly evaluated with GCS, even if it is not the optimal score (51). Therefore, we tried to complement the GCS score for mild TBI by including the TDM result (complicated and uncomplicated mild TBI). However, this classification did not change the predictive value of TBI severity.
Various blood biomarkers of TBI severity were recently proposed and correlated with injury severity and outcome: Ubiquitin C-terminal Hydrolase-L1 and Glial Fibrillary Acidic Protein, Interleukin 10, neuron specific enolase, neurogranin, metallothionein, S100B, tau, estrone. These could help to assess TBI severity at diagnosis more effectively (52–57).
In this longitudinal study, we did not find any new deficit between 6 and 12 months except for prolactin deficiency which is difficult to define in prepubertal children. Nevertheless, further evaluation should be interesting in this cohort 3 years after TBI, especially regarding putative gonadotropic deficiencies, or precocious puberty.
The strength of this study is its large number of children, and its use of the insulin tolerance test which is the gold reference test and the most suitable test after TBI (3, 58). The absence of a control group (for ethical reasons), appears to be a limitation, but the tests used here have been largely accepted in the general pediatric population. This study sheds lights on several problems in endocrinology: the fragility of hormonal testing, the threshold in endocrinology, and the difficulties in diagnosing GHD in patients after TBI, particularly in adulthood where the growth parameter is lacking.
Conclusion
This study calls the attention to endocrine dysfunction after TBI, even for mild TBI. In this study, we could stress the value of a delta height < 0 SDS is a warning, which should lead to an IGF-1 measurement, and dynamic testing in case of IGF <-1 SDS. The basic care of children should include the assessment of growth and weight with particular attention to the year following mild TBI.
Data Availability
All datasets generated for this study are included in the manuscript and/or the supplementary files.
Author Contributions
CB, KB, and ML contributed to the recruitment and follow up. CB, KB, PT, BB, and HB contributed to the redaction of the manuscript.
Funding
This study received financial support from Ipsen and a Defi–TC grant from the French Endocrine Society.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors take full responsibility for the content and would like to thank Luigi di Nicola (Ipsen employee) for his support throughout the entire duration of the project.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2019.00149/full#supplementary-material
References
1. Dewan MC, Mummareddy N, Wellons JC III, Bonfield CM. Epidemiology of global pediatric traumatic brain injury: qualitative review. World Neurosurg. (2016) 91:497–509.e1. doi: 10.1016/j.wneu.2016.03.045
2. Emami P, Czorlich P, Fritzsche FS, Westphal M, Rueger JM, Lefering R, et al. Impact of Glasgow Coma Scale score and pupil parameters on mortality rate and outcome in pediatric and adult severe traumatic brain injury: a retrospective, multicenter cohort study. J Neurosurg. (2016) 126:760–7. doi: 10.3171/2016.1.JNS152385
3. Heather NL, Jefferies C, Hofman PL, Derraik JG, Brennan C, Kelly P, et al. Permanent hypopituitarism is rare after structural traumatic brain injury in early childhood. J Clin Endocrinol Metab. (2012) 97:599–604. doi: 10.1210/jc.2011-2284
4. Casano-Sancho P, Suarez L, Ibanez L, Garcia-Fructuoso G, Medina J, Febrer A. Pituitary dysfunction after traumatic brain injury in children: is there a need for ongoing endocrine assessment? Clin Endocrinol. (2013) 79:853–8. doi: 10.1111/cen.12237
5. Einaudi S, Matarazzo P, Peretta P, Grossetti R, Giordano F, Altare F, et al. Hypothalamo-hypophysial dysfunction after traumatic brain injury in children and adolescents: a preliminary retrospective and prospective study. J Pediatr Endocrinol Metab. (2006) 19:691–703. doi: 10.1515/JPEM.2006.19.5.691
6. Bellone S, Einaudi S, Caputo M, Prodam F, Busti A, Belcastro S, et al. Measurement of height velocity is an useful marker for monitoring pituitary function in patients who had traumatic brain injury. Pituitary. (2013) 16:499–506. doi: 10.1007/s11102-012-0446-0
7. Auble BA, Bollepalli S, Makoroff K, Weis T, Khoury J, Colliers T, et al. Hypopituitarism in pediatric survivors of inflicted traumatic brain injury. J Neurotrauma. (2014) 31:321–6. doi: 10.1089/neu.2013.2916
8. Khadr SN, Crofton PM, Jones PA, Wardhaugh B, Roach J, Drake AJ, et al. Evaluation of pituitary function after traumatic brain injury in childhood. Clin Endocrinol. (2010) 73:637–43. doi: 10.1111/j.1365-2265.2010.03857.x
9. Moon RJ, Sutton T, Wilson PM, Kirkham FJ, Davies JH. Pituitary function at long-term follow-up of childhood traumatic brain injury. J Neurotrauma. (2010) 27:1827–35. doi: 10.1089/neu.2010.1408
10. Poomthavorn P, Maixner W, Zacharin M. Pituitary function in paediatric survivors of severe traumatic brain injury. Arch Dis Child. (2008) 93:133–7. doi: 10.1136/adc.2007.121137
11. Salomon-Estebanez MA, Grau G, Vela A, Rodriguez A, Morteruel E, Castano L, et al. Is routine endocrine evaluation necessary after paediatric traumatic brain injury? J Endocrinol Invest. (2014) 37:143–8. doi: 10.1007/s40618-013-0020-2
12. Niederland T, Makovi H, Gal V, Andreka B, Abraham CS, Kovacs J. Abnormalities of pituitary function after traumatic brain injury in children. J Neurotrauma. (2007) 24:119–27. doi: 10.1089/neu.2005.369ER
13. Casano-Sancho P. Pituitary dysfunction after traumatic brain injury: are there definitive data in children? Arch Dis child. (2017) 102:572–7. doi: 10.1136/archdischild-2016-311609
14. Kreitschmann-Andermahr I, Poll EM, Reineke A, Gilsbach JM, Brabant G, Buchfelder M, et al. Growth hormone deficient patients after traumatic brain injury–baseline characteristics and benefits after growth hormone replacement–an analysis of the German KIMS database. Growth Horm IGF Res. (2008) 18:472–8. doi: 10.1016/j.ghir.2008.08.007
15. Kaulfers AM, Backeljauw PF, Reifschneider K, Blum S, Michaud L, Weiss M, et a. Endocrine dysfunction following traumatic brain injury in children. J Pediatrics. (2010) 157:894–9. doi: 10.1016/j.jpeds.2010.07.004
16. Norwood KW, Deboer MD, Gurka MJ, Kuperminc MN, Rogol AD, Blackman JA, et al. Traumatic brain injury in children and adolescents: surveillance for pituitary dysfunction. Clin Pediatrics. (2010) 49:1044–9. doi: 10.1177/0009922810376234
17. Aimaretti G, Ambrosio MR, Di Somma C, Gasperi M, Cannavo S, Scaroni C, et al. Hypopituitarism induced by traumatic brain injury in the transition phase. J Endocrinol Invest. (2005) 28:984–9. doi: 10.1007/BF03345336
18. Jourdan C, Brugel D, Hubeaux K, Toure H, Laurent-Vannier A, Chevignard M. Weight gain after childhood traumatic brain injury: a matter of concern. Dev Med Child Neurol. (2012) 54:624–8. doi: 10.1111/j.1469-8749.2012.04291.x
19. Ulutabanca H, Hatipoglu N, Tanriverdi F, Gokoglu A, Keskin M, Selcuklu A, et al. Prospective investigation of anterior pituitary function in the acute phase and 12 months after pediatric traumatic brain injury. Childs Nerv Syst. (2014) 30:1021–8. doi: 10.1007/s00381-013-2334-y
20. Personnier C, Crosnier H, Meyer P, Chevignard M, Flechtner I, Boddaert N, et al. Prevalence of pituitary dysfunction after severe traumatic brain injury in children and adolescents: a large prospective study. J Clin Endocrinol Metab. (2014) 99:2052–60. doi: 10.1210/jc.2013-4129
21. Krahulik D, Aleksijevic D, Smolka V, Klaskova E, Venhacova P, Vaverka M, et al. Prospective study of hypothalamo-hypophyseal dysfunction in children and adolescents following traumatic brain injury. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. (2017) 161:80–5. doi: 10.5507/bp.2016.047
22. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. (1974) 2:81–4. doi: 10.1016/S0140-6736(74)91639-0
23. Borgialli DA, Mahajan P, Hoyle JD Jr., Powell EC, Nadel FM, Tunik MG, et al. Performance of the Pediatric glasgow coma scale score in the evaluation of children with blunt head trauma. Acad Emerg Med. (2016) 23:878–84. doi: 10.1111/acem.13014.
24. Kokshoorn NE, Wassenaar MJ, Biermasz NR, Roelfsema F, Smit JW, Romijn JA, et al. Hypopituitarism following traumatic brain injury: prevalence is affected by the use of different dynamic tests and different normal values. Eur J Endocrinol. (2010) 162:11–8. doi: 10.1530/EJE-09-0601
25. Fenske W, Allolio B. Clinical review: current state and future perspectives in the diagnosis of diabetes insipidus: a clinical review. J Clin Endocrinol Metab. (2012) 97:3426–37. doi: 10.1210/jc.2012-1981
26. Lamberts SW, de Herder WW, van der Lely AJ. Pituitary insufficiency. Lancet. (1998) 352:127–34. doi: 10.1016/S0140-6736(98)85043-5
27. Maghnie M, Uga E, Temporini F, Di Iorgi N, Secco A, Tinelli C, et al. Evaluation of adrenal function in patients with growth hormone deficiency and hypothalamic-pituitary disorders: comparison between insulin-induced hypoglycemia, low-dose ACTH, standard ACTH and CRH stimulation tests. Eur J Endocrinol. (2005) 152:735–41. doi: 10.1530/eje.1.01911
28. Dickstein G. The assessment of the hypothalamo-pituitary-adrenal axis in pituitary disease: are there short cuts? J Endocrinol Invest. (2003) 26:25–30.
29. Gonzalbez J, Villabona C, Ramon J, Navarro MA, Gimenez O, Ricart W, et al. Establishment of reference values for standard dose short synacthen test (250 microgram), low dose short synacthen test (1 microgram) and insulin tolerance test for assessment of the hypothalamo-pituitary-adrenal axis in normal subjects. Clin Endocrinol. (2000) 53:199–204. doi: 10.1046/j.1365-2265.2000.01028.x
30. Petersenn S, Quabbe HJ, Schofl C, Stalla GK, von Werder K, Buchfelder M. The rational use of pituitary stimulation tests. Dtsch Arztebl Int. (2010) 107:437–43. doi: 10.3238/arztebl.2010.0437
31. Lem AJ, de Rijke YB, van Toor H, de Ridder MA, Visser TJ, Hokken-Koelega AC. Serum thyroid hormone levels in healthy children from birth to adulthood and in short children born small for gestational age. J Clin Endocrinol Metab. (2012) 97:3170–8. doi: 10.1210/jc.2012-1759
32. Resende EA, Lara BH, Reis JD, Ferreira BP, Pereira GA, Borges MF. Assessment of basal and gonadotropin-releasing hormone-stimulated gonadotropins by immunochemiluminometric and immunofluorometric assays in normal children. J Clin Endocrinol Metab. (2007) 92:1424–9. doi: 10.1210/jc.2006-1569
33. Khairullah A, Klein LC, Ingle SM, May MT, Whetzel CA, Susman EJ, et al. Testosterone trajectories and reference ranges in a large longitudinal sample of male adolescents. PLoS ONE. (2014) 9:e108838. doi: 10.1371/journal.pone.0108838
34. Carel JC, Eugster EA, Rogol A, Ghizzoni L, Palmert MR; ESPE-LWPES GnRH Analogs Consensus Conference Group, et al. Consensus statement on the use of gonadotropin-releasing hormone analogs in children. Pediatrics. (2009) 123:e752–62. doi: 10.1542/peds.2008-1783
35. Juul A, Bernasconi S, Clayton PE, Kiess W, DeMuinck-Keizer Schrama S, Drugs and Therapeutics Committee of the European Society for Paediatric Endocrinology (ESPE). European audit of current practice in diagnosis and treatment of childhood growth hormone deficiency. Horm Res. (2002) 58:233–41. doi: 10.1159/000066265
36. Cohen P, Rogol AD, Deal CL, Saenger P, Reiter EO, Ross JL, et al. Consensus statement on the diagnosis and treatment of children with idiopathic short stature: a summary of the Growth Hormone Research Society, the Lawson Wilkins Pediatric Endocrine Society, and the European Society for Paediatric Endocrinology Workshop. J Clin Endocrinol Metab. (2008) 93:4210–7. doi: 10.1210/jc.2008-0509
37. Marin G, Domene HM, Barnes KM, Blackwell BJ, Cassorla FG, Cutler GB Jr. The effects of estrogen priming and puberty on the growth hormone response to standardized treadmill exercise and arginine-insulin in normal girls and boys. J Clin Endocrinol Metab. (1994) 79:537–41.
38. Ghigo E, Bellone J, Aimaretti G, Bellone S, Loche S, Cappa M, et al. Reliability of provocative tests to assess growth hormone secretory status. Study in 472 normally growing children. J Clin Endocrinol Metab. (1996) 81:3323–7.
39. Wagner IV, Paetzold C, Gausche R, Vogel M, Koerner A, Thiery J, et al. Clinical evidence-based cutoff limits for GH stimulation tests in children with a backup of results with reference to mass spectrometry. Eur J Endocrinol. (2014) 171:389–97. doi: 10.1530/EJE-14-0165
40. Ho KK, 2007 GH Deficiency Consensus Workshop Participants. Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: a statement of the GH Research Society in association with the European Society for Pediatric Endocrinology, Lawson Wilkins Society, European Society of Endocrinology, Japan Endocrine Society, and Endocrine Society of Australia. Eur J Endocrinol. (2007) 157:695–700. doi: 10.1530/EJE-07-0631
41. Martinez AS, Domene HM, Ropelato MG, Jasper HG, Pennisi PA, Escobar ME, et al. Estrogen priming effect on growth hormone (GH) provocative test: a useful tool for the diagnosis of GH deficiency. J Clin Endocrinol Metab. (2000) 85:4168–72. doi: 10.1210/jc.85.11.4168
42. Mauras N, Walton P, Nicar M, Welch S, Rogol AD. Growth hormone stimulation testing in both short and normal statured children: use of an immunofunctional assay. Pediatr Res. (2000) 48:614–8. doi: 10.1203/00006450-200011000-00010
43. Williams T, Berelowitz M, Joffe SN, Thorner MO, Rivier J, Vale W, et al. Impaired growth hormone responses to growth hormone-releasing factor in obesity. A pituitary defect reversed with weight reduction. N Engl J Med. (1984) 311:1403–7. doi: 10.1056/NEJM198411293112203
44. Williams DH, Levin HS, Eisenberg HM. Mild head injury classification. Neurosurgery. (1990) 27:422–8. doi: 10.1227/00006123-199009000-00014
45. Reifschneider K, Auble BA, Rose SR. Update of endocrine dysfunction following pediatric traumatic brain injury. J Clin Med. (2015) 4:1536–60. doi: 10.3390/jcm4081536
46. Rose SR, Auble BA. Endocrine changes after pediatric traumatic brain injury. Pituitary. (2012) 15:267–75. doi: 10.1007/s11102-011-0360-x
47. Grimberg A, DiVall SA, Polychronakos C, Allen DB, Cohen LE, Quintos JB, et al. Guidelines for growth hormone and insulin-like growth factor-I treatment in children and adolescents: growth hormone deficiency, idiopathic short stature, and primary insulin-like growth factor-I deficiency. Horm Res Paediatr. (2016) 86:361–97. doi: 10.1159/000452150
48. Growth Hormone Research Society. Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH Research Society. GH Research Society. J Clin Endocrinol Metab. (2000) 85:3990–3. doi: 10.1210/jcem.85.11.6984
49. Chanson P, Arnoux A, Mavromati M, Brailly-Tabard S, Massart C, Young J, et al. Reference values for insulin-like growth factor I (IGF-I) serum concentrations: comparison of six immunoassays. J Clin Endocrinol Metab. (2016) 101:3450–8. doi: 10.1210/jc.2016-1257
50. Schneider HJ, Kreitschmann-Andermahr I, Ghigo E, Stalla GK, Agha A. Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review. JAMA. (2007) 298:1429–38. doi: 10.1001/jama.298.12.1429
51. Harrison DA, Prabhu G, Grieve R, Harvey SE, Sadique MZ, Gomes M, et al. Risk Adjustment In Neurocritical care (RAIN)–prospective validation of risk prediction models for adult patients with acute traumatic brain injury to use to evaluate the optimum location and comparative costs of neurocritical care: a cohort study. Health Technol Assess. (2013) 17:vii-viii, 1–350. doi: 10.3310/hta17230
52. Mondello S, Kobeissy F, Vestri A, Hayes RL, Kochanek PM, Berger RP. Serum concentrations of ubiquitin C-terminal hydrolase-L1 and glial fibrillary acidic protein after pediatric traumatic brain injury. Sci Rep. (2016) 6:28203. doi: 10.1038/srep28203
53. O'Connell B, Kelly AM, Mockler D, Oresic M, Denvir K, Farrell G, et al. Use of blood biomarkers in the assessment of sports-related concussion-a systematic review in the context of their biological significance. Clin J Sport Med. (2017) 28:561–71. doi: 10.1097/JSM.0000000000000478
54. Peacock WF IV, Van Meter TE, Mirshahi N, Ferber K, Gerwien R, Rao V, et al. Derivation of a three biomarker panel to improve diagnosis in patients with mild traumatic brain injury. Front Neurol. (2017) 8:641. doi: 10.3389/fneur.2017.00641
55. Lagerstedt L, Egea-Guerrero JJ, Rodriguez-Rodriguez A, Bustamante A, Montaner J, El Rahal A, et al. Early measurement of interleukin-10 predicts the absence of CT scan lesions in mild traumatic brain injury. PLoS ONE. (2018) 13:e0193278. doi: 10.1371/journal.pone.0193278
56. Rakholia MV, Kumar RG, Oh BM, Ranganathan PR, Berga S, Kochanek PM, et al. Systemic estrone production and injury induced sex hormone steroidogenesis after severe traumatic brain injury: a prognostic indicator of TBI-related mortality. J Neurotrauma. (2018) doi: 10.1089/neu.2018.5782. [Epub ahead of print].
57. Gill J, Mustapic M, Diaz-Arrastia R, Lange R, Gulyani S, Diehl T, et al. Higher exosomal tau, amyloid-beta 42 and IL-10 are associated with mild TBIs and chronic symptoms in military personnel. Brain Inj. (2018) 32:1277–84. doi: 10.1080/02699052.2018.1471738
58. Klose M, Stochholm K, Janukonyte J, Lehman Christensen L, Frystyk J, Andersen M, et al. Prevalence of posttraumatic growth hormone deficiency is highly dependent on the diagnostic set-up: results from The Danish National Study on Posttraumatic Hypopituitarism. J Clin Endocrinol Metab. (2014) 99:101–10. doi: 10.1210/jc.2013-2397
Keywords: traumatic brain injury, pituitary function, pediatric, hypopituitarism, growth hormone deficiency
Citation: Briet C, Braun K, Lefranc M, Toussaint P, Boudailliez B and Bony H (2019) Should We Assess Pituitary Function in Children After a Mild Traumatic Brain Injury? A Prospective Study. Front. Endocrinol. 10:149. doi: 10.3389/fendo.2019.00149
Received: 19 November 2018; Accepted: 20 February 2019;
Published: 19 March 2019.
Edited by:
Margaret Cristina Da Silva Boguszewski, Universidade Federal do Paraná, BrazilReviewed by:
Roberto Lanes, Hospital de Clinicas Caracas, VenezuelaRodolfo A. Rey, Center for Endocrinology Research Dr. César Bergadá (CEDIE), Argentina
Copyright © 2019 Briet, Braun, Lefranc, Toussaint, Boudailliez and Bony. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Claire Briet, Y2xhaXJlLmJyaWV0QGNodS1hbmdlcnMuZnI=