 Adriana Claudia Lopes Carvalho-Furtado1*
Adriana Claudia Lopes Carvalho-Furtado1* Daniela Mariano Carvalho-Louro2
Daniela Mariano Carvalho-Louro2 Neysa Aparecida Tinoco Regattieri3Marcelo Palmeira Rodrigues4
Neysa Aparecida Tinoco Regattieri3Marcelo Palmeira Rodrigues4 Maria Luiza Ricardo Nogueira Montenegro5André Metzker Ferro5Patrícia Souza Pirangi3
Maria Luiza Ricardo Nogueira Montenegro5André Metzker Ferro5Patrícia Souza Pirangi3 Luciana Ansaneli Naves6
Luciana Ansaneli Naves6- 1Endocrinology Unit, Instituto Hospital de Base, Brasília, Brazil
- 2Gastroenterology Unit, Instituto Hospital de Base, Brasília, Brazil
- 3Radiology Unit, Faculty of Medicine, University of Brasilia, Brasília, Brazil
- 4Pneumology Unity, Faculty of Medicine, University of Brasilia, Brasília, Brazil
- 5Faculty of Medicine, University of Brasilia, Brasília, Brazil
- 6Endocrinology Unit, Faculty of Medicine, University of Brasilia, Brasília, Brazil
Non-alcoholic fatty liver disease (NAFLD) is common in patients with growth hormone deficiency (GHD). Some noninvasive techniques have been used to quantify liver fat, such as the controlled attenuation parameter (CAP).
Objective: To evaluate CAP as a tool to identify liver steatosis and its relationship with different clinical and biochemical metabolic parameters in a group of patients with severe adult growth hormone deficiency (AGHD), and to compare the evolution of metabolic profiles after 6 months of human growth hormone (rhGH) replacement therapy in a subgroup of patients.
Methods: Cross-sectional observational study at baseline of naive rhGH multiple pituitary hormonal deficiency (MPHD) hypopituitarism patients. A 6-month intervention clinical trial in a selected group of a non-randomized, non-controlled cohort was also applied.
Results: Liver stiffness measurement (LSM) was normal in severe AGHD patients. CAP evaluation showed steatosis in 36.3% of baseline patients (8/22), associated with higher BMI, waist circumference, insulin, and alanine aminotransferase (ALT) levels. According to steatosis degree by CAP, child-onset growth hormone deficiency (CO-GHD) was graded as 68.75% (11/16) S0, 12.5% (2/16) S1, and 18.75% (3/16) S3, whereas AO-GHD was graded as 50% (3/6) S0, 16.66% (1/6) S2, and 33.33% S3. After 6 months of hrGH replacement, CAP measurements did not change significantly, neither on group without hepatic steatosis at baseline (194.4 ± 24.3 vs. 215.4 ± 51.3; p = 0.267) nor on the group with hepatic steatosis (297.2 ± 32.3 vs. 276.4 ± 27.8; p = 0.082). A significant improvement of body composition was observed only in the first group.
Conclusions: We have demonstrated the importance of CAP as a non-invasive tool in the liver steatosis identification on hypopituitary patients. This method may be an important indicator of the severity of metabolic disorders in MPHD patients. In our study, no liver health modification in LSM at baseline or after 6 months of rhGH replacement was found. Longer studies can help to establish the potential repercussions of growth hormone replacement therapy on liver steatosis.
Introduction
Significant metabolic changes are observed in AGHD, such as negative effects on lipoprotein metabolism, lean mass reduction, fat mass increase, and intra-abdominal fat, leading to an increased risk of cardiovascular events (1–3). Central obesity and altered lipid profiles give rise to the development of Metabolic Syndrome (MetS), which has insulin resistance as a key pathogenic mechanism (4).
NAFLD is used to define the accumulation of liver fat in a patient without a prior history of alcohol abuse. The higher concentration of lipids, especially triglycerides in hepatocytes, leads to the development of hepatic steatosis, defined as the accumulation of fatty tissue higher than 5% of liver weight (5, 6).
Hepatic steatosis is considered a reversible change but may progress to an inflammatory process (steatohepatitis) and to liver cirrhosis. In this case, it may lead to a higher risk of hepatocarcinoma (7, 8). In addition, NAFLD represents an isolated cardiovascular risk factor and is associated with an increased incidence of cardiovascular disease (9).
The high prevalence of hepatic steatosis on AGHD patients, confirmed by liver biopsy, reveals the presence of an increased risk of progression to non-alcoholic steatohepatitis (NASH) (10). Therefore, the GHD in the subgroup of patients with MPHD represents a high risk of NAFLD and progression to NASH and cirrhosis (7, 11).
An important non-invasive technique has been used in the hepatology field to identify liver fibrosis—FibroScan® Echosens (12). Transient elastography (TE) by FibroScan® has been widely used in the last decade as a fast, non-invasive, and reproducible method to evaluate the liver stiffness measurement (LSM) as a measure of the degree of liver fibrosis. TE measures low frequency (50 Hz) elastic shear wave velocity propagation through the liver. In this case, shear wave velocity is directly related to tissue stiffness, which is expressed in kiloPascals (kPa). Usual tissue stiffness ranges from 2.5 to 7.5 kPa. A normal values for healthy liver stiffness is estimated to be about 5.5 kPa (13, 14). An available tool in FibroScan®, validated on patients with chronic liver disease from many causes, has enabled the evaluation of hepatic steatosis using controlled attenuation parameter (CAP). This parameter is useful for estimating the attenuation of the propagation of ultrasonic waves signals through the liver, acquired simultaneously with LSM by the FibroScan® probe. CAP is measured in decibels per meter (dB/m), with typical values ranging from 100 to 400 dB/m. CAP analysis is effective in the diagnosis and quantification of hepatic steatosis, from absolute cut-off points, with 90% sensitivity (15–18). Recent studies have shown that transient elastography has the best performance on the diagnosis and exclusion of advanced hepatic fibrosis in NAFLD (19). There is no previous literature report on the use of Transient Elastography to identify liver disease on MPHD hypopituitary patients.
Objectives
The aim of this study is to evaluate the relationship of CAP with different clinical and biochemical metabolic parameters in a group of patients with severe AGHD. A secondary objective is to compare the evolution of metabolic profiles after 6 months of growth hormone replacement (rhGH) therapy in a selected group of patients.
Subjects and Methods
Study Design
This is a cross-sectional observational study at baseline of naive rhGH MPHD hypopituitarism patients and a 6-month intervention clinical trial in a selected group of a non-randomized, non-controlled cohort. Data were gathered and individuals were recruited from October 2016 thru October 2018 at the Endocrinology Unit of University Hospital of Brasilia, and at the Endocrinology Unit of Instituto Hospital de Base in Brasilia, located in the Federal District of Brazil.
Twenty-two patients were recruited at baseline and thirteen of them were enrolled in the intervention subgroup. From the intervention subgroup, patients who survived malignancies and those patients who did not agree to continue the study, were excluded from the group.
The study complied with the WMA Declaration of Helsinki and its amended versions on ethical principles for medical research involving human subjects and was approved by the Ethical Committee on Human Subject Research from the Fundação de Ensino e Pesquisa em Ciências da Saúde (FEPECS). All patients signed a proper informed consent before participating in the study.
Inclusion Criteria
Patients included in the study were adults, with periodical ambulatory follow-ups, presenting at least one of the following criteria: (i) confirmed MPHD diagnosis; (ii) GHD initiated and treated in infancy or with disability developed in adulthood, for at least 5 years without rhGH replacement. GH deficiency was defined by GH peak < 3 ng/dl in the insulin tolerance test and IGF-I concentration <-2SD. Patients with hypopituitarism secondary to treatment of functioning pituitary tumors (Cushing's disease, prolactinoma, acromegaly); and chronic use of supraphysiological doses of corticoids were also excluded.
Evaluation at Baseline
Variables considered were age, gender, signs, and symptoms at diagnosis. Also considered were comorbidities, anthropometric measurements, metabolic parameters (glucose, insulin, HOMA index, glycated hemoglobin, lipid metabolism, TGO, TGP, GGT) body composition by DXA, and hepatic evaluation by Fibroscan® with LSM and CAP measurement. All assessments were performed after night fasting.
Laboratory Analysis
Serum GH levels were measured by a two-site chemiluminescent immunometric assay (Immulite, 2000). Assay sensitivity was 0.01 ng/ml and the interassay coefficient of variation was <10%. Serum IGF-I was measured by a solid-phase enzyme labeled chemiluminescent immunometric assay with sample pretreatment on an onboard dilution step (Immulite, 2000). The manufacturer's normal range for age and gender was considered. Inter-assay coefficients of variation were <5%. Peptides were determined by chemiluminescent methods. Glucose, lipids, and transaminases were determined respectively by hexokinase and by IFCC without pyridoxal phosphate.
Body Composition by Dual Emission X-ray Absorptiometry (DEXA)
Body composition [including percent of fat body mass (FBM), truncal fat mass (TFM), lean body mass (LBM), and waist/hip ratio] was assessed by dual-emission X-ray absorptiometry (DXA, GE Healthcare, Lunar DPX NT, Diegem, Belgium) with participants in supine position (20).
FibroScan® Echosens, Paris, France
Transition Elastography (TE) was performed by a trained operator on the right lobe of the liver through the intercostal spaces with the patient lying in the dorsal decubitus position and with the right arm in maximal abduction. Ultrasound attenuation (CAP) was only calculated when the liver stiffness measurement (LSM) was valid in order to ensure an accurate attenuation. A reliable LSM was defined using the following 3 criteria: (i) at least 10 valid shots; (ii) a success rate (SR: the ratio of valid shots to the total number of shots) of at least 60%; and (iii) an interquartile range (IQR) of <30% of the median LSM (IQR/M\30%). The median value of 10 successful measurements was selected as the representative value. TE results were expressed as kilopascals (kPa) for LSM and as dB/m for CAP. LSM ranges from 2.5 to 7.5 kPa, and a healthy liver normal value is estimated to be 5.5 kPa (14, 21). The intensity of hepatic steatosis is graded by CAP according to published cut-offs bounds (for the M probe S0 <248; S1 = 248–267; S2 = 268–279; S3 ≥ 280 dB/m) (17).
Intervention Subgroup
Patients in the intervention subgroup started rhGH replacement therapy at a dose of 0.2 mg/day (0.6UI) for men and 0.3 mg/day (0.9UI) for women on oral estrogen therapy. They were evaluated monthly, with a dose increase of 0.1 mg/day rhGH until reaching IGF-1 concentrations between −1SD and +1SD for sex and age. After 6 months, with optimal concentrations of IGF-1 reached, the initial evaluations were repeated. The same radiological and biochemical parameters were evaluated at baseline and after 6 months of treatment.
The recombinant growth hormone used for treatment was Hormotrop®(4IU, Bergamo). Patients with MPHD who had survived malignancies were excluded from this group.
Statistical Analysis
The Kolmogorov-Smirnov and the Shapiro-Wilk tests were used to test the normality of the variables. The Pearson correlation test was used for normal variables, and the Spearman correlation test was used for non-normal variables. Student's t-test was used to analyze the significance of the variables with normal distribution, being expressed as media and standard deviation. The independent variables HOMA IR, IGF-I, insulin, triglycerides, truncal fat, ALT, and AST were considered non-normal and evaluated by the non-parametric Mann-Whitney test, being expressed as a median and interquartile interval. The Fisher exact test was used to test the association between two independent nominal variables.
Data analysis was performed using the independent variables before and 6 months after treatment with rhGH and was conducted using the T-test of paired samples for normal distribution variables and non-parametric tests of two independent samples for non-normal variables.
Results
Clinical Characteristics at Baseline
At baseline evaluation, the group of 22 patients presented a similar distribution between gender, and most of the patients had a diagnosis of GH deficiency in early childhood. Benign tumoral diseases were the most common etiology for hypopituitarism (36.4%), but inflammatory and malignant conditions were also observed. Half of the patients were submitted to a neurosurgical procedure. Six patients (27% of total) underwent previous adjuvant radiotherapy treatment of baseline pathology for more than 10 years (four patients with craniopharyngioma, one patient with medulloblastoma, and one patient with suprasellar dysgerminoma). ACTH deficiency was observed in 77% of the patients, treated by 5 mg of prednisone for more than 1 year (Table 1). From our sample, only one woman, 20 years old, had a normal gonadotropic axis. All hypogonadic patients (21/22) were under steroid replacement (estrogen/ progesterone or testosterone).
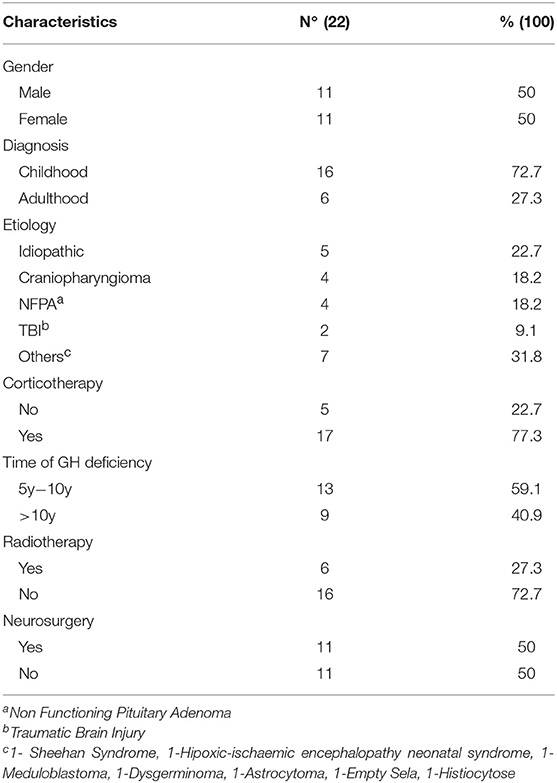
Table 1. Clinical aspects of baseline adult GHD patients.
Patients who presented adult-onset growth hormone deficiency (AO-GHD) had higher BMI, waist circumference, waist/hip ratio, and presented higher HOMA-IR and insulin levels. Body fat distribution assessed by DXA body composition did not differ between groups (Table 2).
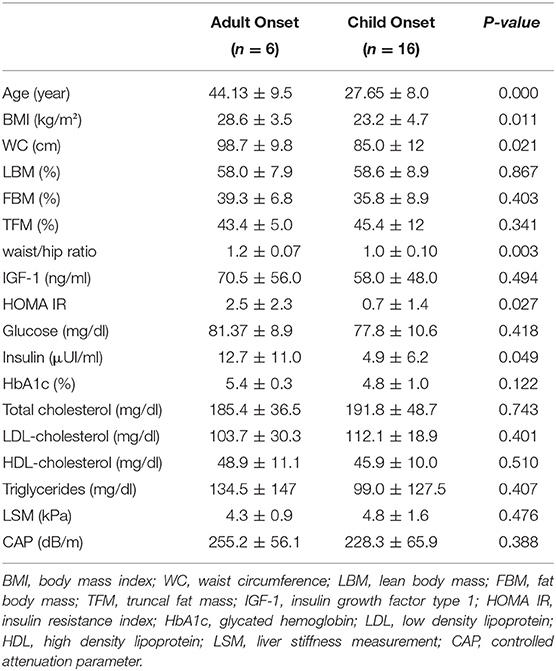
Table 2. Metabolic characteristics of baseline GHD patients according to deficiency onset phase.
Hepatic Evaluation by Elastography
Of the 23 patients submitted to FibroScan®, only one patient failed the method due to difficulty in acquiring valid measurements due to narrow intercostal spaces. The patient was excluded from the study. Considering FibroScan® results, LSM has not shown abnormalities or differences on GHD patients according to the deficiency onset phase, while absolute CAP values were higher in adult-onset patients but without statistical significance (Table 2). CAP evaluation showed hepatic steatosis in 36.3% of the patients (8/22), associated with higher BMI, waist circumference, insulin, and ALT. Lipid profile and body composition were not related to fatty liver disease identification by CAP (Table 3).
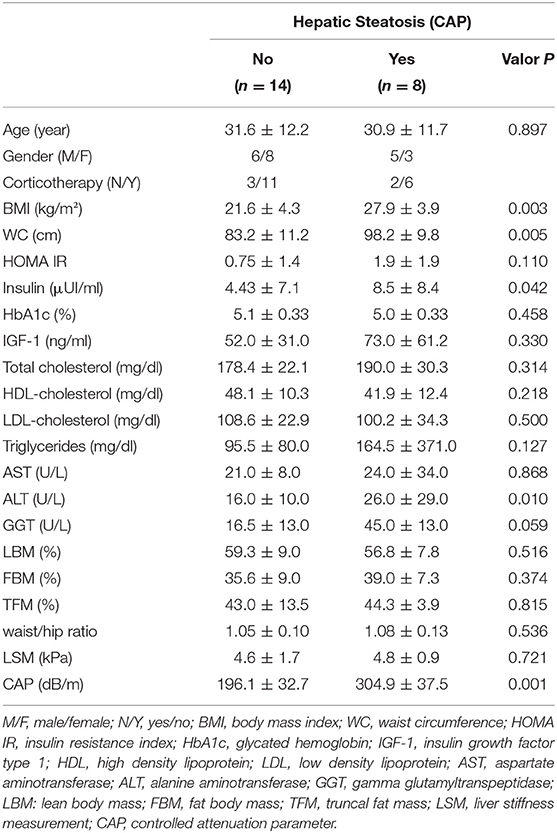
Table 3. Metabolic profile of baseline DGHA patients according to hepatic steatosis measured by CAP.
According to steatosis degree by CAP, child-onset growth hormone deficiency (CO-GHD) was graded as 68.75% (11/16) S0, 12.5% (2/16) S1, and 18.75% (3/16) S3, whereas AO-GHD was graded as 50% (3/6) S0, 16.66% (1/6) S2, and 33.33% S3 (Figure 1).
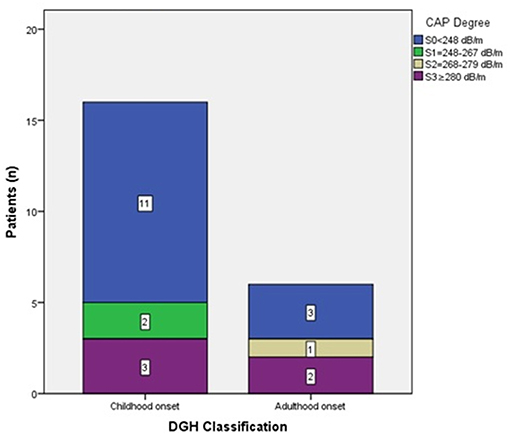
Figure 1. patients number according CAP degree.
In order to test the relationship between CAP and the independent variables of metabolic syndrome, the Spearman correlation was used (Figure 2). Moderately positive correlation results were found between CAP measurements with BMI (ρ = 0.621; p = 0.002), WC (ρ = 0.632; p = 0.002), HOMA IR (ρ = 0.447; p = 0.037), insulin (ρ = 0.515; p = 0.014), and triglycerides (ρ = 0.476; p = 0.025).
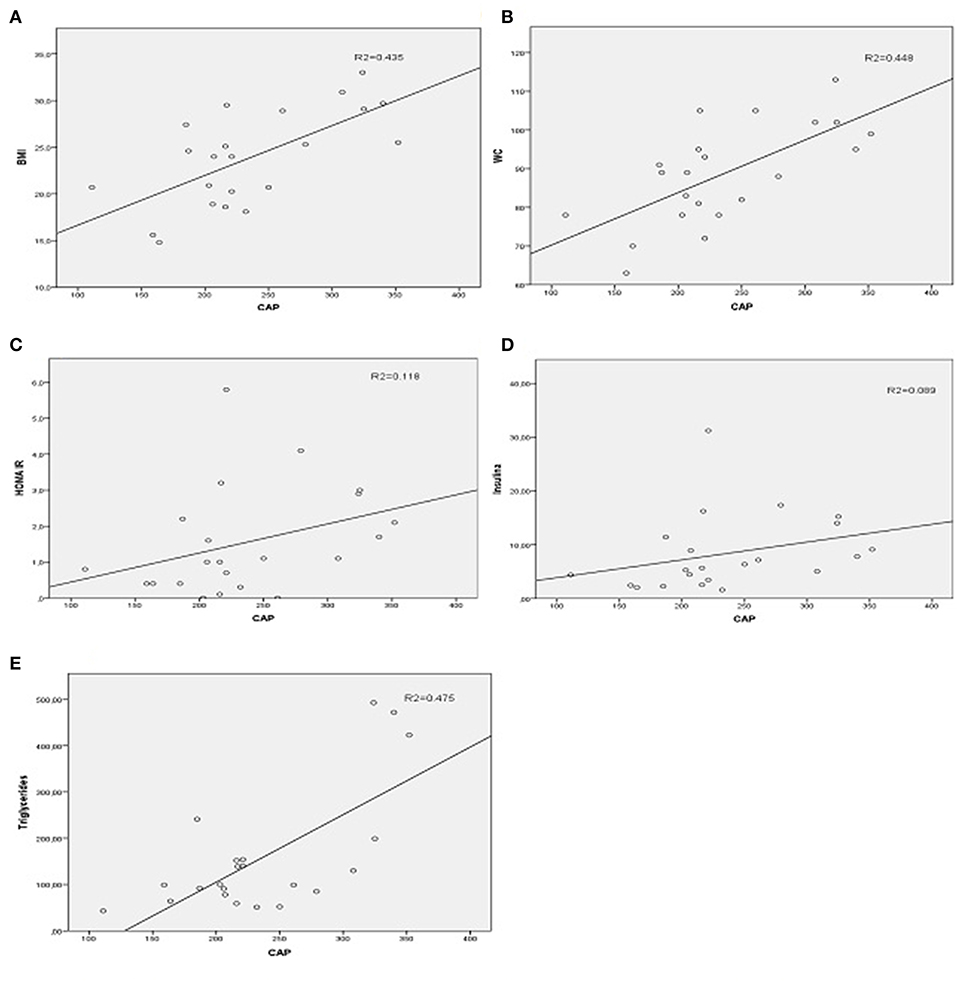
Figure 2. Spearman correlation graphics between CAP and metabolic parameters. (A) CAP, controlled attenuation parameter(dB/m) and BMI, body mass index (kg/m2). (B) CAP and WC, waist circumference (cm). (C) CAP and HOMA IR, homeostatic model assessment insulin resistance. (D) CAP and Insulin (μUI/ml). (E) CAP and Triglycerides (mg/dl).
Clinical Characteristics of Therapeutic Intervention Subgroup
Patients in the intervention subgroup started rhGH replacement therapy at a dose of 0.2 mg/day (0.6UI) for men and 0.3 mg/day (0.9UI) for women on oral estrogen therapy.
After 6 months of rhGH replacement therapy, the patients showed significant improvement in body composition, with a reduction of waist circumference and fat body distribution. A significant gain of lean body mass and reduction of fat body mass were also observed, and there was no change in BMI. However, a significant increase in blood glucose, insulin, and HOMA-IR index were observed. LSM and CAP measurements did not change significantly (Table 4).
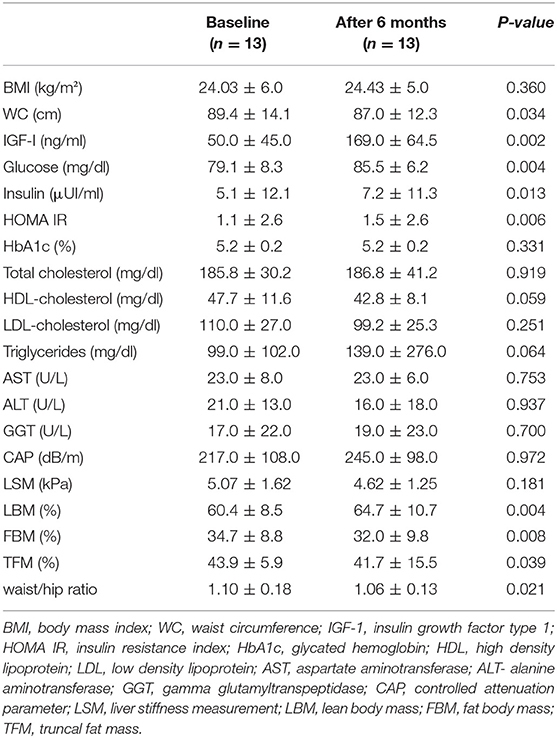
Table 4. Metabolic changes in the intervention group after 6 months of rhGH replacement therapy.
Intervention subgroup patients were divided according to the presence of hepatic steatosis measured by CAP, and a statistically significant improvement on body composition was observed only in patients without hepatic steatosis after 6 months of hrGH replacement therapy. CAP measurements did not change significantly, neither on the group without hepatic steatosis (194.4 ± 24.3 vs. 215.4 ± 51.3; p = 0.267) nor on the group with hepatic steatosis (297.2 ± 32.3 vs. 276.4 ± 27.8; p = 0.082), during 6 months of follow up. However, worsening absolute values of glucose, insulin, and HbA1c were found in the group with hepatic steatosis at baseline, despite the WC reduction (Table 5).
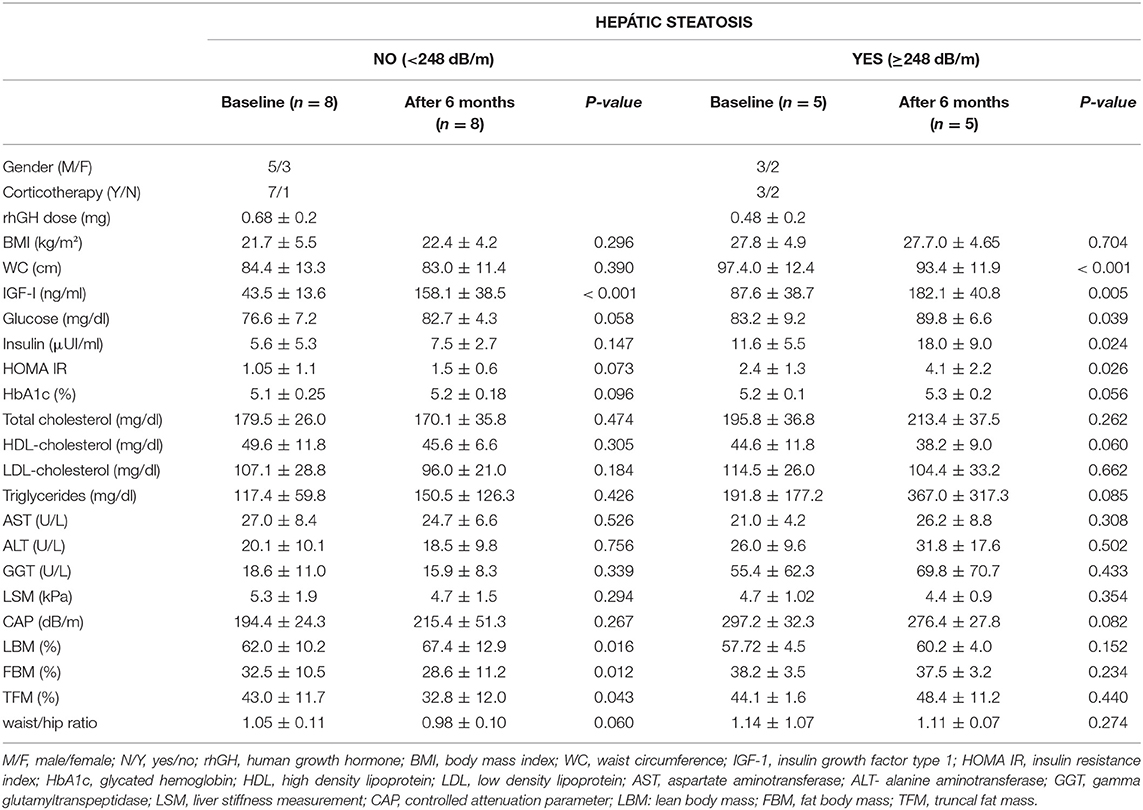
Table 5. Metabolic changes in the intervention group after 6 months of rhGH replacement therapy according to hepatic steatosis measured by CAP.
Discussion
Transient elastography by Fibroscan has been used as a fast, non-invasive, and reproducible method to evaluate liver fibrosis (13, 14). In addition to accurately evaluating LSM, TE is also capable of quantifying hepatic steatosis through a physical parameter (CAP), which is simultaneously acquired with LSM by the FibroScan probe and which estimates the liver attenuation levels (17, 18).
CAP is very efficient in detecting even low-grade steatosis, but neither the presence nor the severity of hepatic steatosis as measured by CAP predicts liver-related events, cancer, or CVE in the short period of time (15, 17).
The positive correlation observed between CAP and BMI, WC, and insulin resistance markers in the sample used in this study confirms the important role of this non-invasive tool in the identification of NAFLD on hypopituitarism patients. This represents an independent predictor of CVD (22, 23). This finding may be an alert for screening clinical features used to detect early risk of developing metabolic syndrome. Considering criteria based on insulin resistance, and supported by waist circumference data, MetS prevalence ranges between 10 and 84% worldwide, depending on the geographic region, urban or rural environment, individual demographic characteristics of the population studied (gender, age, racial, and ethnic origin), and the criteria used to define MetS (24).
At baseline, BMI was higher in adult-onset GH deficiency, but both groups presented a high percentage of fat mass, suggesting that there is a negative repercussion of GH deficiency in body composition (25). Greater alteration of insulin resistance clinical profiles, such as BMI, WC, waist/hip ratio, HOMA IR, and insulin, was observed in the group of patients with AO-GHD compared to the CO-GHD group. As the interval (years) without rhGH replacement therapy was similar between the groups, the differences found on clinical parameters may be related to genetic predisposition and to exposure to general factors such as eating behaviors, dietary factors contributing to insulin resistance, nutrient availability, and reduced or absent physical activity (26–28).
Furthermore, aging is truly important as an insulin resistance combined factor related to changes in body composition, insulin activity suppression by substrates such as free fatty acids (FFAs), and likely resistance to leptin (29–31). Thereby, as discussed by other authors, CO-GHD patients are more prone to accumulated metabolic risks because they have a higher time forward to hormonal deficiency exposure (32).
Moderated hypercholesterolemia due to an increase in low-density lipoprotein (LDL) cholesterol has been reported in patients with GHD (25). These data were not observed in the studied sample and could be explained in part by the replacement of rhGH in the group of patients with CO-GHD during childhood. The use of statins (data not shown) and the extreme individual lipid variations (mainly in the concentration of triglycerides) also contributed to these findings.
At baseline, the IGF1 showed no significant difference between groups, contrary to the literature reports (33–35), and may be related to the severity of pituitary deficiency present in both groups of MPHD patients.
A general overview of pathophysiological mechanisms that lead to insulin resistance in GHD patients gives them a higher risk of NAFLD development (23). The evaluation of hepatic steatosis by CAP of the considered sample confirmed the presence of risk factors such as for overweight, increased WC, and increased insulin levels as components of MetS hepatic manifestation (36, 37).
Liver biopsy remains the gold standard for the diagnosis of steatohepatitis and staging of fibrosis in patients with NAFLD, which is the strongest predictor for disease-specific mortality. Nevertheless, liver biopsy is invasive and associated with a low rate of complications such as pain and bleeding and restrains liver disease monitoring (14, 38). The current European Association for the Study of the Liver (EASL) guidelines for the management of NAFLD recommend TE as a non-invasive method for liver fibrosis assessment and monitoring (39). A recent study confirmed that transient elastography has the best non-invasive performance to evaluate liver fibrosis in NAFLD (19). In our series, no fibrosis changes were suggested by LSM, so a liver biopsy was not indicated in this cohort. In MPHD hypopituitary patients, complication and risks have increased such as hemorrhage, related to the use of corticosteroids, estrogens, and testosterone (11).
Patient with liver steatosis could also present a higher concentration of alanine aminotransferase with or without steatohepatitis. Although CAP measures reached statically significant transaminase differences, the absolute values were not higher than the reference values. These findings are in agreement with reports of normal transaminase in more than 70% of the patients with NAFLD (40).
Considering the metabolic findings hold up the development of NAFLD in the AO-GHD group, we observed a prevalence of severe steatosis on CO-GHD patients, highlighting the need for early diagnosis and intervention in this GHD group.
Intervention with rhGH in a selected group of patients with GHD resulted in a statistically significant effect on the corporal composition profiles, with an increase of lean mass and decrease of fat mass, truncal fat mass, and waist/hip ratio. This only occurred within the group of patients without hepatic steatosis at baseline. The lack of improvement in corporal composition in patients with steatotic liver may suggest a reduction of GH signaling in this condition, as recently described by Rufinatscha (41). On the other hand, this hypothesis could also suggest that the non-improvement of liver steatosis degree measured by CAP in our study could be related to reduced GH action on hepatic enzymes important to lipidic metabolism. This finding is in agreement with reports of non-improvement of steatosis with rhGH on GHD patients measured by other steatosis identification methods (37). This is in disagreement with the important role of GH and IGF-1 in the liver and the NAFLD improvement (42) and could be related to the short period of follow up in our study.
The worsening of the insulin resistance observed on the intervention group associated with steatosis by CAP could be transitory and followed by recovery of insulin sensitivity after therapy suspension, as has already been established (43, 44). At the same time, it was recently reported that the GH signaling in the liver could be diminished in patients with NAFLD, leading to hepatic insulin sensitivity and metabolic activity deterioration (41).
In conclusion, we have demonstrated the importance of CAP as a non-invasive tool in liver steatosis identification of hypopituitary patients. This method may be an important indicator of the severity of metabolic disorders in MPHD patients. In our study, no liver health modification in LSM at baseline and after 6 months of rhGH replacement was found. Further studies can help to establish the potential repercussion of growth hormone replacement therapy on liver steatosis.
Data Availability
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The study complied with the WMA Declaration of Helsinki and its amended versions on ethical principles for medical research involving human subjects and was approved by the Ethical Committee on Human Subject Research from Fundação de Ensino e Pesquisa em Ciências da Saúde (FEPECS). All patients signed a proper informed consent before participating in the study.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Funding
The recombinant growth hormone used in this study is part of the high-cost medicines distributed by SUS (Brazilian Health System), a program of the Brazilian Ministry of Health. This medication is distributed to every patient who is demonstrably growth hormone deficient. The project was submitted and accepted by the Research Support Center of the SABIN laboratory for clinical analyzes to support the performance of the laboratory tests.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the support of the Nucleus of Support on Research (Nucleo de Apoio a Pesquisa-NAP) from the Sabin Institute and the SABIN laboratory for performing the laboratory tests.
References
1. Colle M, Auzerie J. Discontinuation of growth hormone therapy in growth-hormone-deficient patients: assessment of body fat mass using bioelectrical impedance. Horm Res. (1993) 39:192–6. doi: 10.1159/000182734
2. Beshyah SA, Freemantle C, Thomas E, Rutherford O, Page B, Murphy M, et al. Abnormal body composition and reduced bone mass in growth hormone deficient hypopituitary adults. Clin Endocrinol. (1995) 42:179–89. doi: 10.1111/j.1365-2265.1995.tb01860.x
3. Johannsson G, Marin P, Lonn L, Ottosson M, Stenlof K, Bjorntorp P, et al. Growth hormone treatment of abdominally obese men reduces abdominal fat mass, improves glucose and lipoprotein metabolism, and reduces diastolic blood pressure. J Clin Endocrinol Metab. (1997) 82:727–34. doi: 10.1210/jc.82.3.727
4. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. (2005) 365:1415–28. doi: 10.1016/S0140-6736(05)66378-7
5. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. (2016) 65:1038–48. doi: 10.1016/j.metabol.2015.12.012
7. Chalasani N, Younossi Z, Lavine JE, Diehl AM, Brunt EM, Cusi K, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. (2012) 142:1592–609. doi: 10.1053/j.gastro.2012.04.001
8. White DL, Kanwal F, El–Serag HB. Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review. Clin Gastroenterol Hepatol. (2012) 10:1342–59. doi: 10.1016/j.cgh.2012.10.001
9. Edens MA, Kuipers F, Stolk RP. Non-alcoholic fatty liver disease is associated with cardiovascular disease risk markers. Obes Rev. (2009) 10:412–9. doi: 10.1111/j.1467-789X.2009.00594.x
10. Ichikawa T, Hamasaki K, Ishikawa H, Ejima E, Eguchi K, Nakao K. Non-alcoholic steatohepatitis and hepatic steatosis in patients with adult onset growth hormone deficiency. Gut. (2003) 52:914. doi: 10.1136/gut.52.6.914
11. Rinella ME, Sanyal AJ. Management of NAFLD: a stage-based approach. Nat Rev Gastroenterol Hepatol. (2016) 13:196–205. doi: 10.1038/nrgastro.2016.3
12. Karlas T, Petroff D, Sasso M, Fan JG, Mi YQ, de Ledinghen V, et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. J Hepatol. (2017) 66:1022–30. doi: 10.1016/j.jhep.2016.12.022
13. Castera L, Vilgrain V, Angulo P. Noninvasive evaluation of NAFLD. Nat Rev Gastroenterol Hepatol. (2013) 10:666–75. doi: 10.1038/nrgastro.2013.175
14. Kennedy P, Wagner M, Castera L, Hong CW, Johnson CL, Sirlin CB, et al. Quantitative elastography methods in liver disease: current evidence and future directions. Radiology. (2018) 286:738–63. doi: 10.1148/radiol.2018170601
15. de Ledinghen V, Vergniol J, Foucher J, Merrouche W, le Bail B. Non-invasive diagnosis of liver steatosis using controlled attenuation parameter (CAP) and transient elastography. Liver Int. (2012) 32:911–8. doi: 10.1111/j.1478-3231.2012.02820.x
16. Sasso M, Beaugrand M, de Ledinghen V, Douvin C, Marcellin P, Poupon R, et al. Controlled attenuation parameter (CAP): a novel VCTE guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: preliminary study and validation in a cohort of patients with chronic liver disease from various causes. Ultrasound Med Biol. (2010) 36:1825–35. doi: 10.1016/j.ultrasmedbio.2010.07.005
17. Liu K, Wong VW, Lau K, Liu SD, Tse YK, Yip TC, et al. Prognostic value of controlled attenuation parameter by transient elastography. Am J Gastroenterol. (2017) 112:1812–23. doi: 10.1038/ajg.2017.389
18. Tapper EB, Loomba R. Noninvasive imaging biomarker assessment of liver fibrosis by elastography in NAFLD. Nat Rev Gastroenterol Hepatol. (2018) 15:274–82. doi: 10.1038/nrgastro.2018.10
19. Tovo CV, Villela-Nogueira CA, Leite NC, Panke CL, Port GZ, Fernandes S, et al. Transient hepatic elastography has the best performance to evaluate liver fibrosis in non-alcoholic fatty liver disease (NAFLD). Ann Hepatol. (2019) 18:409–536.
20. Albanese CV, Diessel E, Genant HK. Clinical applications of body composition measurements using DXA. J Clin Densitom. (2003) 6:75–85. doi: 10.1385/JCD:6:2:75
21. Andrade P, Rodrigues S, Rodrigues-Pinto E, Gaspar R, Lopes J, Lopes S, et al. Diagnostic accuracy of controlled attenuation parameter for detecting hepatic steatosis in patients with chronic liver disease. GE Port J Gastroenterol. (2017) 24:161–8. doi: 10.1159/000453364
22. Mellinger JL, Pencina KM, Massaro JM, Hoffmann U, Seshadri S, Fox CS, et al. Hepatic steatosis and cardiovascular disease outcomes: an analysis of the Framingham Heart Study. J Hepatol. (2015) 63:470–6. doi: 10.1016/j.jhep.2015.02.045
23. Marino L, Jornayvaz FR. Endocrine causes of nonalcoholic fatty liver disease. World J Gastroenterol. (2015) 21:11053–76. doi: 10.3748/wjg.v21.i39.11053
24. Gluvic Z, Zaric B, Resanovic I, Obradovic M, Mitrovic A, Radak D, et al. Link between metabolic syndrome and insulin resistance. Curr Vasc Pharmacol. (2017) 15:30–9. doi: 10.2174/1570161114666161007164510
25. de Boer H, Blok GJ, Van der Veen EA. Clinical aspects of growth hormone deficiency in adults. Endocr Rev. (1995) 16:63–86. doi: 10.1210/er.16.1.63
26. Song YM, Lee K. Eating behavior and metabolic syndrome over time. Eat Weight Disord. (2019). doi: 10.1007/s40519-019-00640-9. [Epub ahead of print].
27. Schnack LL, Romani AMP. The metabolic syndrome and the relevance of nutrients for its onset. Recent Pat Biotechnol. (2017) 11:101–19. doi: 10.2174/1872208311666170227112013
28. Muller-Wieland D, Altenburg C, Becher H, Burchard J, Frisch A, Gebhard J, et al. Development of the metabolic syndrome: study design and baseline data of the lufthansa prevention study (LUPS), a prospective observational cohort survey. Exp Clin Endocrinol Diabetes. (2018). doi: 10.1055/a-0767-6361
29. Ferrannini E, Vichi S, Beck-Nielsen H, Laakso M, Paolisso G, Smith U. Insulin action and age. European Group for the Study of Insulin Resistance (EGIR). Diabetes. (1996) 45:947–53. doi: 10.2337/diabetes.45.7.947
30. Ma XH, Muzumdar R, Yang XM, Gabriely I, Berger R, Barzilai N. Aging is associated with resistance to effects of leptin on fat distribution and insulin action. J Gerontol A Biol Sci Med Sci. (2002) 57:B225–31. doi: 10.1093/gerona/57.6.B225
31. Kuk JL, Saunders TJ, Davidson LE, Ross R. Age-related changes in total and regional fat distribution. Ageing Res Rev. (2009) 8:339–48. doi: 10.1016/j.arr.2009.06.001
32. Attanasio AF, Mo D, Erfurth EM, Tan M, Ho KY, Kleinberg D, et al. Prevalence of metabolic syndrome in adult hypopituitary growth hormone (GH)-deficient patients before and after GH replacement. J Clin Endocrinol Metab. (2010) 95:74–81. doi: 10.1210/jc.2009-1326
33. Mukherjee A, Shalet SM. The value of IGF1 estimation in adults with GH deficiency. Eur J Endocrinol. (2009) 161(Suppl. 1):S33–9. doi: 10.1530/EJE-09-0247
34. Attanasio AF, Lamberts SW, Matranga AM, Birkett MA, Bates PC, Valk NK, et al. Adult growth hormone (GH)-deficient patients demonstrate heterogeneity between childhood onset and adult onset before and during human GH treatment. Adult Growth Hormone Deficiency Study Group. J Clin Endocrinol Metab. (1997) 82:82–8. doi: 10.1210/jc.82.1.82
35. Lissett CA, Jonsson P, Monson JP, Shalet SM. Determinants of IGF-I status in a large cohort of growth hormone-deficient (GHD) subjects: the role of timing of onset of GHD. Clin Endocrinol. (2003) 59:773–8. doi: 10.1046/j.1365-2265.2003.01884.x
36. Runchey SS, Boyko EJ, Ioannou GN, Utzschneider KM. Relationship between serum circulating insulin-like growth factor-1 and liver fat in the United States. J Gastroenterol Hepatol. (2014) 29:589–96. doi: 10.1111/jgh.12437
37. Meienberg F, Yee M, Johnston D, Cox J, Robinson S, Bell JD, et al. Liver fat in adults with GH deficiency: comparison to matched controls and the effect of GH replacement. Clin Endocrinol. (2016) 85:76–84. doi: 10.1111/cen.13042
38. Ekstedt M, Hagstrom H, Nasr P, Fredrikson M, Stal P, Kechagias S, et al. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology. (2015) 61:1547–54. doi: 10.1002/hep.27368
39. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J Hepatol. (2015) 63:237–64. doi: 10.1016/j.jhep.2015.04.006
40. Stefan N, Kantartzis K, Haring HU. Causes and metabolic consequences of Fatty liver. Endocr Rev. (2008) 29:939–60. doi: 10.1210/er.2008-0009
41. Rufinatscha K, Ress C, Folie S, Haas S, Salzmann K, Moser P, et al. Metabolic effects of reduced growth hormone action in fatty liver disease. Hepatol Int. (2018) 12:474–81. doi: 10.1007/s12072-018-9893-7
42. Takahashi Y. The role of growth hormone and insulin-like growth factor-I in the liver. Int J Mol Sci. (2017) 42:1447–60. doi: 10.3390/ijms18071447
43. Filipsson Nystrom H, Barbosa EJ, Nilsson AG, Norrman LL, Ragnarsson O, Johannsson G. Discontinuing long-term GH replacement therapy–a randomized, placebo-controlled crossover trial in adult GH deficiency. J Clin Endocrinol Metab. (2012) 97:3185–95. doi: 10.1210/jc.2012-2006
Keywords: transient elastography, controlled atenuation parameter, liver steatosis, metabolic syndrome, adult growth hormone deficiency (AGHD)
Citation: Carvalho-Furtado ACL, Carvalho-Louro DM, Regattieri NAT, Rodrigues MP, Montenegro MLRN, Ferro AM, Pirangi PS and Naves LA (2019) Transient Elastography and Controlled Attenuation Parameter (CAP) in the Assessment of Liver Steatosis in Severe Adult Growth Hormone Deficiency. Front. Endocrinol. 10:364. doi: 10.3389/fendo.2019.00364
Received: 18 March 2019; Accepted: 22 May 2019;
Published: 19 June 2019.
Edited by:
Monica Livia Gheorghiu, Carol Davila University of Medicine and Pharmacy, RomaniaReviewed by:
Grace L. H. Wong, The Chinese University of Hong Kong, ChinaNicoleta Baculescu, Carol Davila University of Medicine and Pharmacy, Romania
Dumitru Branisteanu, Grigore T. Popa University of Medicine and Pharmacy, Romania
Copyright © 2019 Carvalho-Furtado, Carvalho-Louro, Regattieri, Rodrigues, Montenegro, Ferro, Pirangi and Naves. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adriana Claudia Lopes Carvalho-Furtado, YWRyaWFuYWZ1cnRhZG9AdGVycmEuY29tLmJy