 Lilian de Souza D’Albuquerque Silva1
Lilian de Souza D’Albuquerque Silva1 Natércia Neves Marques de Queiroz1
Natércia Neves Marques de Queiroz1 Franciane Trindade Cunha de Melo1
Franciane Trindade Cunha de Melo1 João Felício Abrahão Neto1
João Felício Abrahão Neto1 Luísa Corrêa Janaú2
Luísa Corrêa Janaú2 Norberto Jorge Kzan de Souza Neto1
Norberto Jorge Kzan de Souza Neto1 Manuela Nascimento de Lemos1
Manuela Nascimento de Lemos1 Maria Clara Neres Iunes de Oliveira1
Maria Clara Neres Iunes de Oliveira1 Angélica Leite de Alcântara1
Angélica Leite de Alcântara1 Lorena Vilhena de Moraes1
Lorena Vilhena de Moraes1 Wanderson Maia da Silva1
Wanderson Maia da Silva1 Ícaro José Araújo de Souza1
Ícaro José Araújo de Souza1 Nivin Mazen Said1
Nivin Mazen Said1 Gabriela Nascimento de Lemos1
Gabriela Nascimento de Lemos1 Karem Miléo Felício1
Karem Miléo Felício1 Márcia Costa dos Santos1
Márcia Costa dos Santos1 Ana Regina Bastos Motta1
Ana Regina Bastos Motta1 Melissa de Sá Oliveira dos Reis1
Melissa de Sá Oliveira dos Reis1 Isabel Jane Campos Lobato1
Isabel Jane Campos Lobato1 Priscila Boaventura Barbosa de Figueiredo1
Priscila Boaventura Barbosa de Figueiredo1 Ana Carolina Contente Braga de Souza1
Ana Carolina Contente Braga de Souza1 Pedro Paulo Freire Piani1
Pedro Paulo Freire Piani1 João Soares Felício1*
João Soares Felício1*- 1Endocrinology Division, University Hospital João de Barros Barreto, Federal University of Pará, Belém, Brazil
- 2Department of Medicine, State University of Pará, Belém, Brazil
Background: Cardiovascular autonomic neuropathy (CAN) is associated with diabetes mellitus, increasing morbidity and mortality. Some cross-sectional studies associated CAN with low 25-hydroxyvitamin D levels. The aim of our study was to evaluate the effect of high-dose vitamin D (VD) supplementation on CAN in Type 1 Diabetes Mellitus (T1DM) patients.
Methods: We performed a prospective study with 23 patients diagnosed with T1DM and CAN. Subjects with VD levels <30 ng/ml received 10,000 IU/day; the ones with VD levels between 30–60 ng/ml were given 4,000 IU/day for 12 weeks.
Results: There was an improvement in CAN parameters related to resting heart rate variability, such as time domain parameters [Maximum RR interval (0.77 ± 0.11 vs 0.94 ± 0.51 s, p <0.05), Mean length of regular RR intervals (0.71 ± 0.10 vs 0.76 ± 0.09 s, p <0.05) and Standard deviation of all NN intervals (0.02 ± 0.01 vs 0.03 ± 0.02 s; p <0.01)] and frequency domain parameters [Low Frequency (1.9 ± 0.5 vs 2.5 ± 0.9 s, p < 0.001), Total Power (2.5 ± 0.4 vs 2.8 ± 0.6 s, p <0.05)]. In addition, there was a correlation between absolute VD level variation and posttreatment High Frequency (%), as well as among percent variation in VD level and end-of-study Low Frequency/High Frequency ratio (r=0.6, p<0.01; r= -0.5, p<0.05, respectively).
Conclusion: Our pilot study is the first to suggest a strong association between high-dose vitamin D supplementation and improved cardiovascular autonomic neuropathy in T1DM patients. It occurred without any variation in HbA1C, blood pressure levels, lipids, and insulin dose.
Clinical Trial Registration: http://www.isrctn.com/ISRCTN32601947, identifier ISRCTN32601947.
Background
Autonomic diabetic neuropathy is a degenerative condition that affects 16.7%–34.3% of DM patients (1, 2). It is related to time of disease and poor glycemic control and has multifactorial pathogenesis. Early diagnosis is a key factor to manage this condition, and slowing its progression by modifying risk factors is the prevalent therapeutic approach (3).
Cardiovascular autonomic neuropathy (CAN) is characterized by autonomic denervation of the cardiovascular system, causing hemodynamic changes and increasing morbidity and mortality in patients with diabetes (4, 5). It is often an underdiagnosed condition, as symptoms generally appear in late stages. Recently, several parameters of heart rate (HR) variability analyzed by software have shown good sensitivity and specificity for CAN diagnosis (6).
Few cross-sectional studies suggest an association between 25(OH)D level, presence and severity of peripheral neuropathies (7–11) and CAN (10, 12) in patients with diabetes (7–11). Nevertheless, there are no data available about the effect of high doses of VD supplementation on CAN in people with T1DM (13, 14). Molecular basis for this association is multifactorial; however, the inflammatory pathway and neurotrophin reduction might be involved in damage caused to peripheral and autonomic nerves (15, 16).
There are few therapeutics options for CAN currently. In this context, Vitamin D (VD) could be a potential option to be evaluated in patients with diabetes with CAN. Thus, the aim of this study is to evaluate the effects of high-dose VD supplementation on CAN parameters in patients with T1DM.
Methods
Study Design and Patients
We performed a prospective study to evaluate the effect of vitamin D supplementation on CAN in T1DM patients as part of a research protocol (ISRCTN32601947) that has already provided evidence on other aspects of VD supplementation outcomes (17–20).
A total of 68 subjects were recruited from the endocrinology ambulatory but only 23 had CAN diagnosis according to Toronto consensus (21) and were enrolled in this study to have their data analyzed before and after VD supplementation. Basal level of 25(OH)D was measured and those with value ≥ 30ng/dl received 4.000UI per day of cholecalciferol, while those with level < 30ng/dl were supplemented with 10.000UI/day, for 12 weeks (Figure 1).
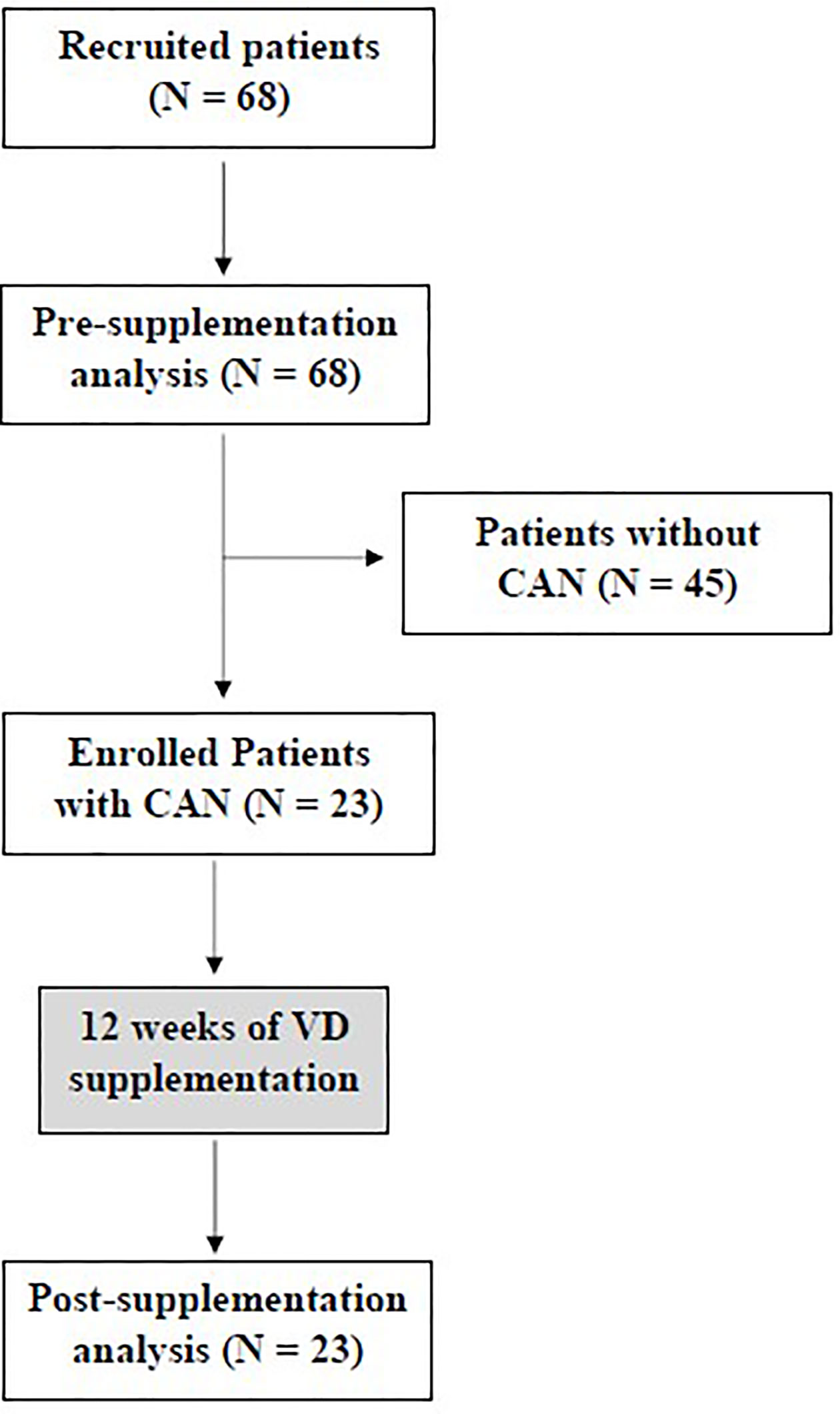
Figure 1 Design of the study.
This study was developed according to the Declaration of Helsinki and the Nuremberg Code and was approved by the University Hospital João de Barros Barreto ethics committee, reference number 0122.0.071.000-12. Signed consent was obtained from all patients.
Inclusion criteria consisted in: a) patients with T1DM diagnosis in at least a 1-year follow-up; b) age between 12 and 50 years in regular treatment with an endocrinologist; c) CAN diagnosis according to Toronto consensus (21); d) insulin therapy dose stability for at least 3 months before participating in the study; e) NPH, Glargine, Detemir, Aspart, Glulisin, Lispro, and Regular insulin were insulins allowed; f) patient in use of metformin could participate of the study as long as they were using the same dose for at least 3 months; g) compliance with diet and exercise regimen. Exclusion criteria included: history of a) hepatic diseases; b) bone metabolism disorders and previous VD or Calcium supplementation; c) abnormal serum creatinine levels d) anemias; e) pregnancy or breastfeeding women; f) uncontrolled hypo or hyperthyroidism and allergies to VD supplementation. There was no increase in activity or exercise in the intervention group. Those patients were previously instructed to maintain physical activity according to American Diabetes Association Guidelines (22) to participate in this trial.
Data Collection
Data collection occurred during scheduled visits, during pre-treatment (baseline) and post-treatment (end of study) phases. Analysis of medical records (demographics, pre-existent clinical conditions, insulin and other medications in use) and physical examination were carried out. Laboratory tests and CAN evaluation were performed before and after 12 weeks.
Serum 25(OH)D was measured quantitatively by the following kit: DiaSorin LIAISON 25-OH-Vitamin D TOTAL chemiluminescence immunoassay (DiaSorin, Stillwater, MN, USA) (23). DiaSorin LIAISON is one of the methods to evaluate 25(OH)D tested by DEQAS (Vitamin D External Quality Assessment Scheme), the largest specialist external quality assessment (proficiency testing) scheme for the vitamin D metabolites 25(OH)D and 1,25(OH)2D (24), and is also certified by Vitamin D Standardization-Certification Program (VDSCP). HbA1C was analyzed by high-performance liquid chromatography (HPLC). Fasting glucose, triglycerides, total cholesterol, low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C) were measured by colorimetry, as well as serum creatinine, which was used to calculate the glomerular filtration rate (GFR) using the Chronic Kidney Disease Epidemiology Collaboration equation (CKD-EPI) (25). Ultrasensitive C-reactive protein (PCR-US) was measured by nephelometry, with a detection limit of 0.01mg/dl.
CAN research was always made in the morning, with fasting capillary glycemia levels between 70–250 mg/dl. Subjects were instructed not to use alcohol, caffeine beverages and tobacco for at least 8 h before the test, and not to perform vigorous physical exercises 24 h before examination.
Parameters used to diagnose CAN were Very Low Frequency, Low Frequency, High Frequency, respiratory coefficient, 30/15 coefficient and Valsalva coefficient, as well as systolic blood pressure (SBP) reduction in orthostasis. Subjects were considered not to have CAN when presenting up to 1 abnormal parameter. The presence of two abnormal parameters was defined as criteria to diagnose incipient CAN; for established CAN, three parameters were necessary (21). Severe CAN was reported when patients presented orthostatic hypotension. All procedures were performed before and after vitamin D supplementation period.
CAN Evaluation
The VNS-MICRO software (Neurosoft, Ivanovo, Russia) was used to analyze data of seven heart rate variability (HRV) parameters: three of them in rest and four while performing maneuvers of vagal and sympathetic stimulations (26). The test begins with patients in supine positions and an electrocardiographic record for 300 s was performed. R waves are highlighted by the software and each regular RR interval is analyzed by a math algorithm and then expressed through an amplitude diagram of heart rate oscillation (HR fluctuations per second) versus HR in hertz. Total amplitude of HRV spectrum is distributed in three bands (Figure 2): 1) Very Low Frequency (VLF) component (0,01 to 0,04Hz), which is related to vasomotor tonus fluctuations linked to thermoregulation and sweating (sympathetic control); 2) Low Frequency (LF) component (0,4 to 0,15Hz), associated with baroreceptor reflex; and 3) High Frequency (HF) component (0,15 to 0,5Hz), related to parasympathetic control (vagus nerve). These represent frequency domain parameters, which also include Total Power (TP), a set of three combined spectral bands and LF/HF ratio, which reflects balance between sympathetic and parasympathetic systems.
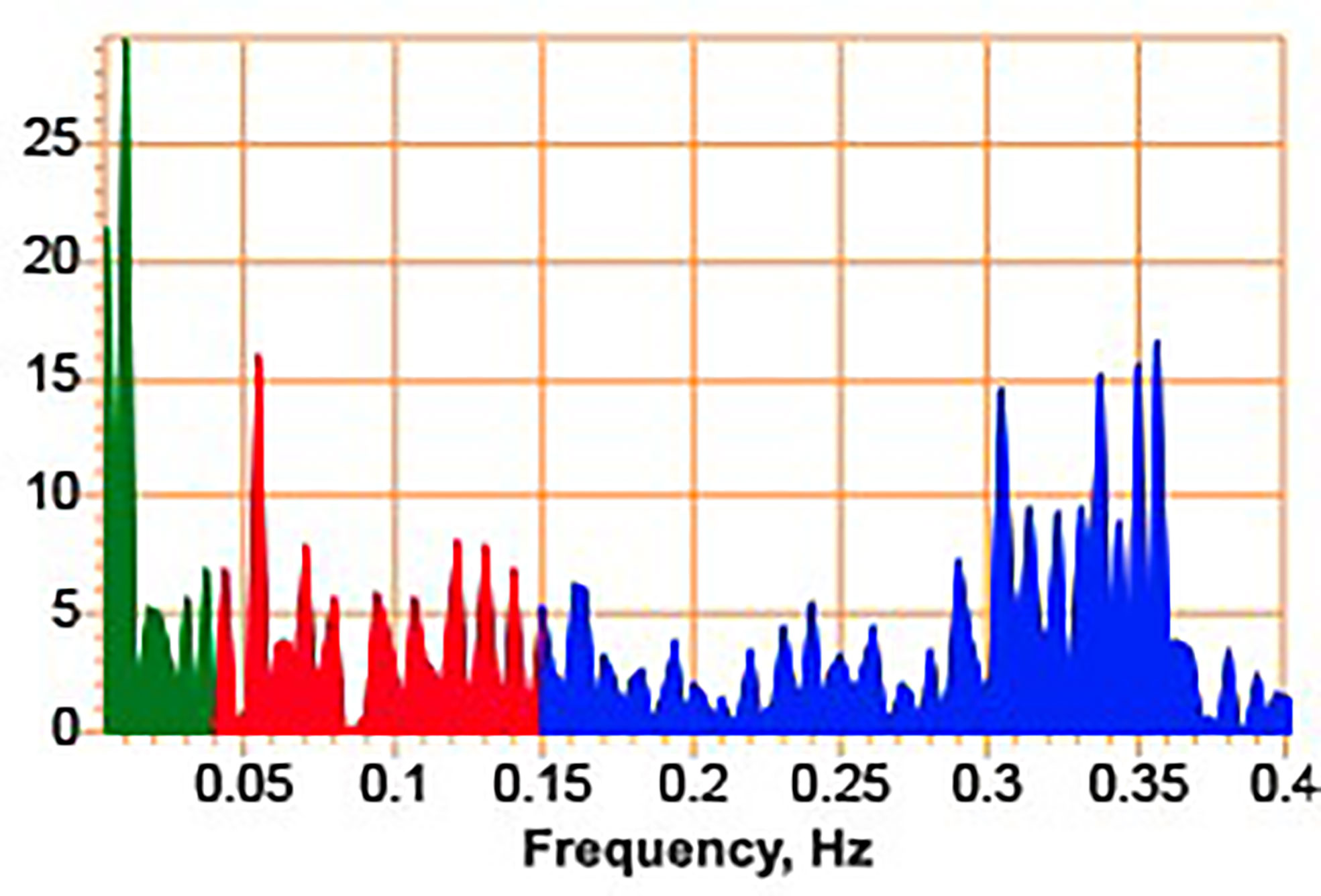
Figure 2 Spectrogram.
The stimulatory maneuvers used were deep breathing, Valsalva and orthostasis (blood pressure and HRV). In each test the relation between the largest and smallest RR interval is assessed and, then, a coefficient is obtained (27).
Beside seven diagnostic items, software provided another data about rest HRV called time domain parameters. Total Power (TP) is a set of three combined spectral bands, including: LF/HF ratio, which reflects balance between sympathetic and parasympathetic systems; RRmin (minimum RR interval), RRmax (maximum RR interval); RRNN (mean length of regular RR intervals); and SDNN (standard deviation of all NN intervals). Despite it is not a diagnostic criteria, it provides additional information in sympathetic and parasympathetic performance in heartbeat. The frequency domain parameters were expressed in logarithm with base 10.
Statistical Analysis
To compare variables before and after VD supplementation Wilcoxon and paired T test were applied, and Chi-square test was run for categorical variables.
To establish correlations between variables, Pearson’s or Spearman’s test was used. The level of statistical significance was set at p<0,05. Statistical analysis was performed using SigmaStat 3.5® (Jandel Scientific Corporation, Chicago, Illinois) e Statistical Package for Social Sciences (SPSS 22.0, Inc., Chicago, IL, USA).
Our sample size was calculated based on an expected difference of 0.01 in SDNN (SD=0.015) to achieve a power of 0.8 and alpha of <0.05, the sample size necessary was 20. In addition, the sample was enough to obtain the same power in all variables evaluated. 0.2 between means in TP (SD=0.3); 0.6 in LF (SD=0.4); 0.5 in HF (SD=0.7); 0.3 in VLF (SD=0.4); and 0.3 in Valsalva coefficient (SD=0.4). The sample size necessary was 20, 20, 18, 16, and 16, respectively.
Results
Baseline characteristics of all patients recruited and enrolled are described in Table 1. Table 2 presents clinical and laboratory features before and after vitamin D supplementation.
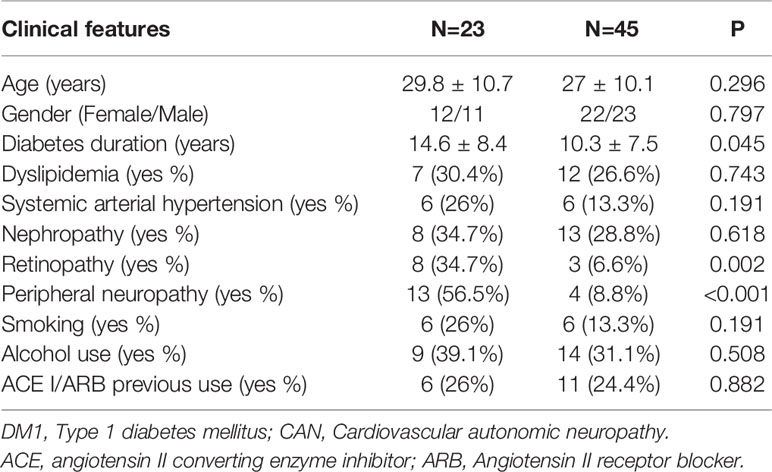
Table 1 Baseline characteristics of recruited and enrolled individuals with CAN (N=23) and without CAN (N=45).
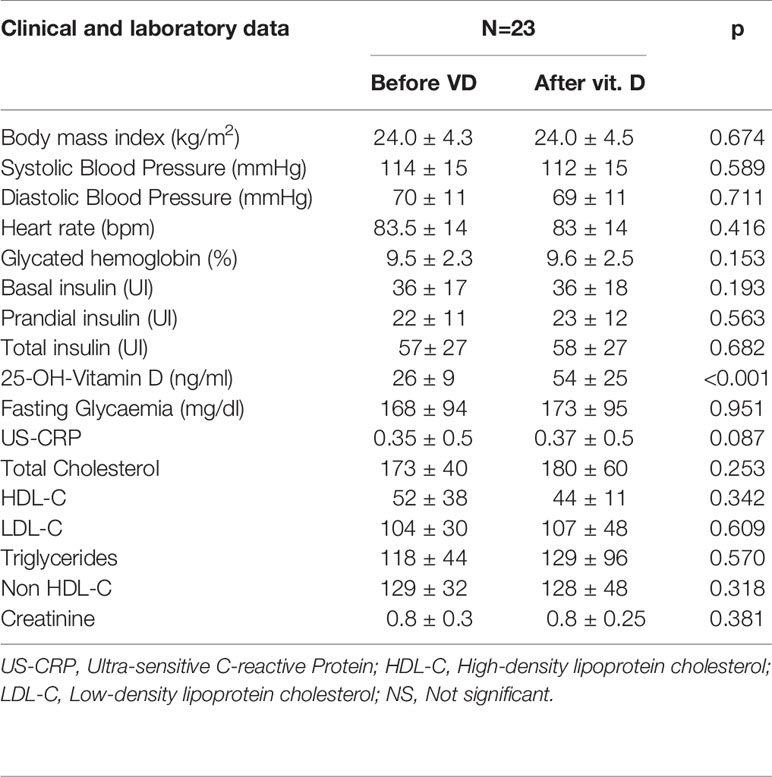
Table 2 Clinical and laboratory data of enrolled T1DM patients with CAN, before and after VD supplementation.
Cardiovascular Autonomic Neuropathy test results are described in Table 3. An improvement was observed in VLF, LF, HF, TP, as well as in RRmax, RRNN and SDNN, after VD supplementation. All time domain parameters are shown in Figure 3. These parameters are related to rest. The dynamic tests for heart rate variability (deep breathing, Valsalva, and orthostasis) and hypotension orthostatic were not different after vitamin D supplementation.
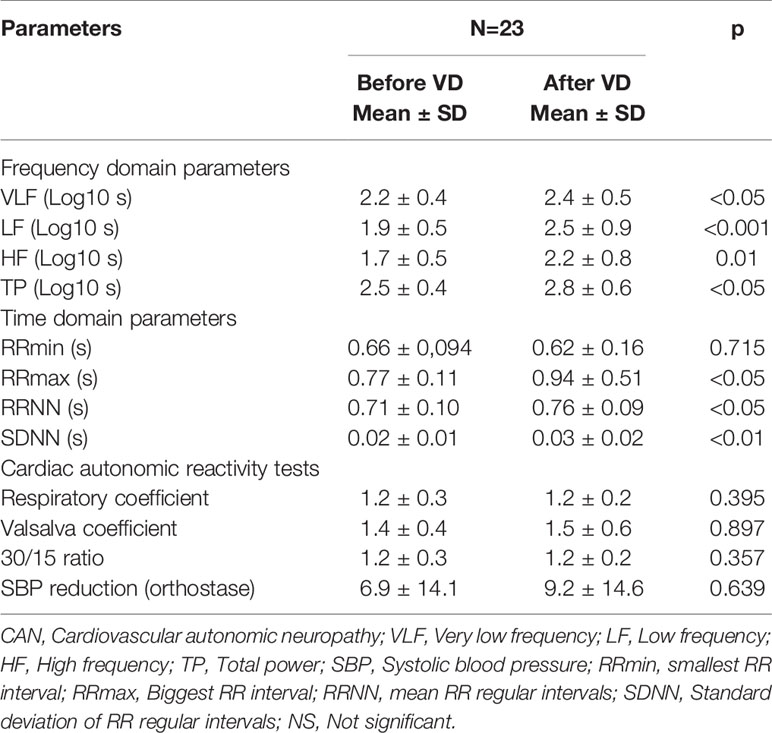
Table 3 CAN parameters before and after vitamin D supplementation in patients with T1DM.
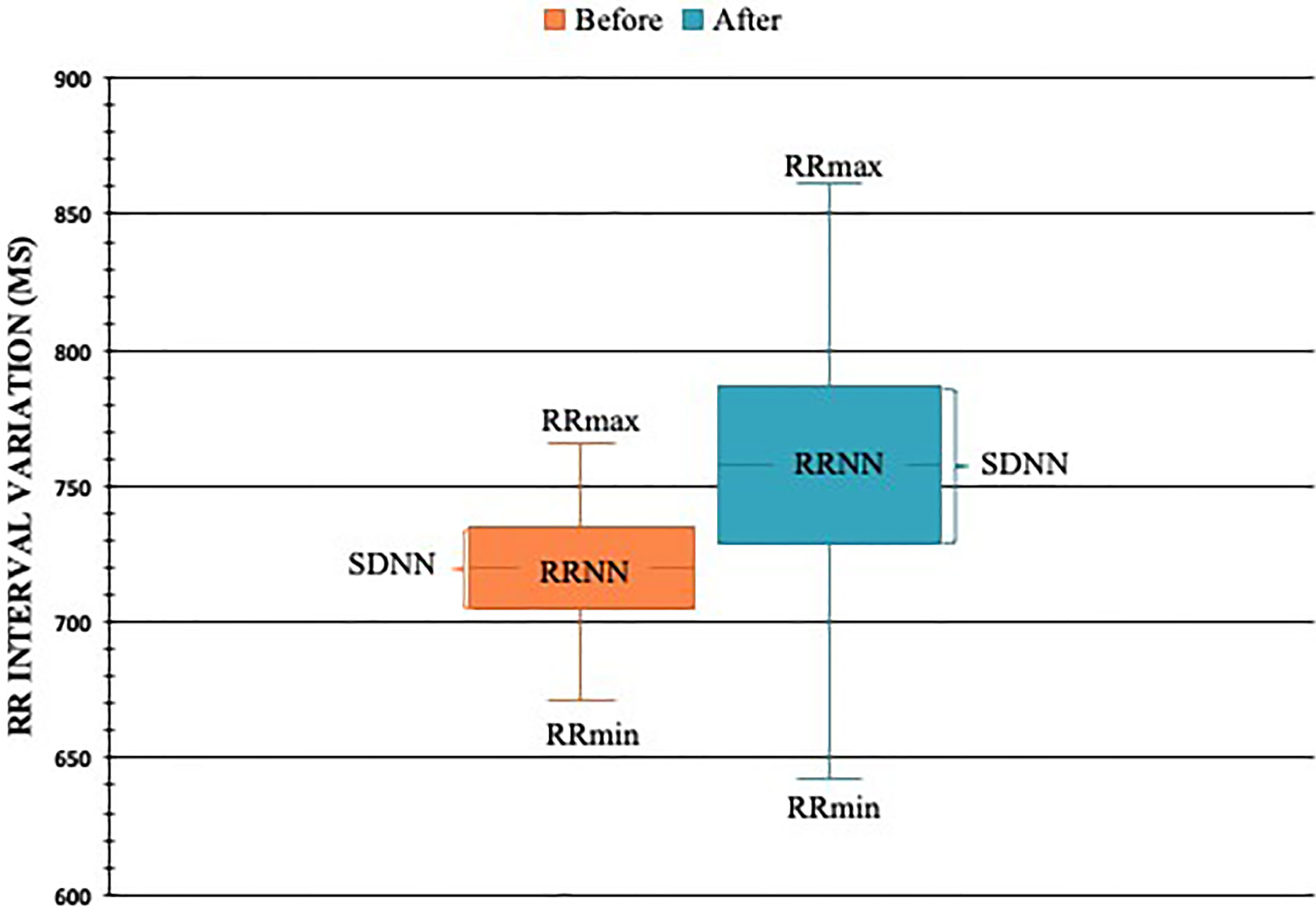
Figure 3 RR interval in milliseconds (ms) before and after VD supplementation in T1DM patients with CAN (N=23). * = p < 0.05. RRNN, mean of RR intervals at rest; SDNN, standard deviation of RR intervals; RRmin, minimum RR interval observed; RRmax, maximum RR interval observed.
When analyzing just CAN criteria, we noticed a reduction in the number of altered rest parameters (VLF, LF, and HF) after VD supplementation (Figure 4). However, the number of abnormal dynamic tests did not change after the treatment period (Figure 5).
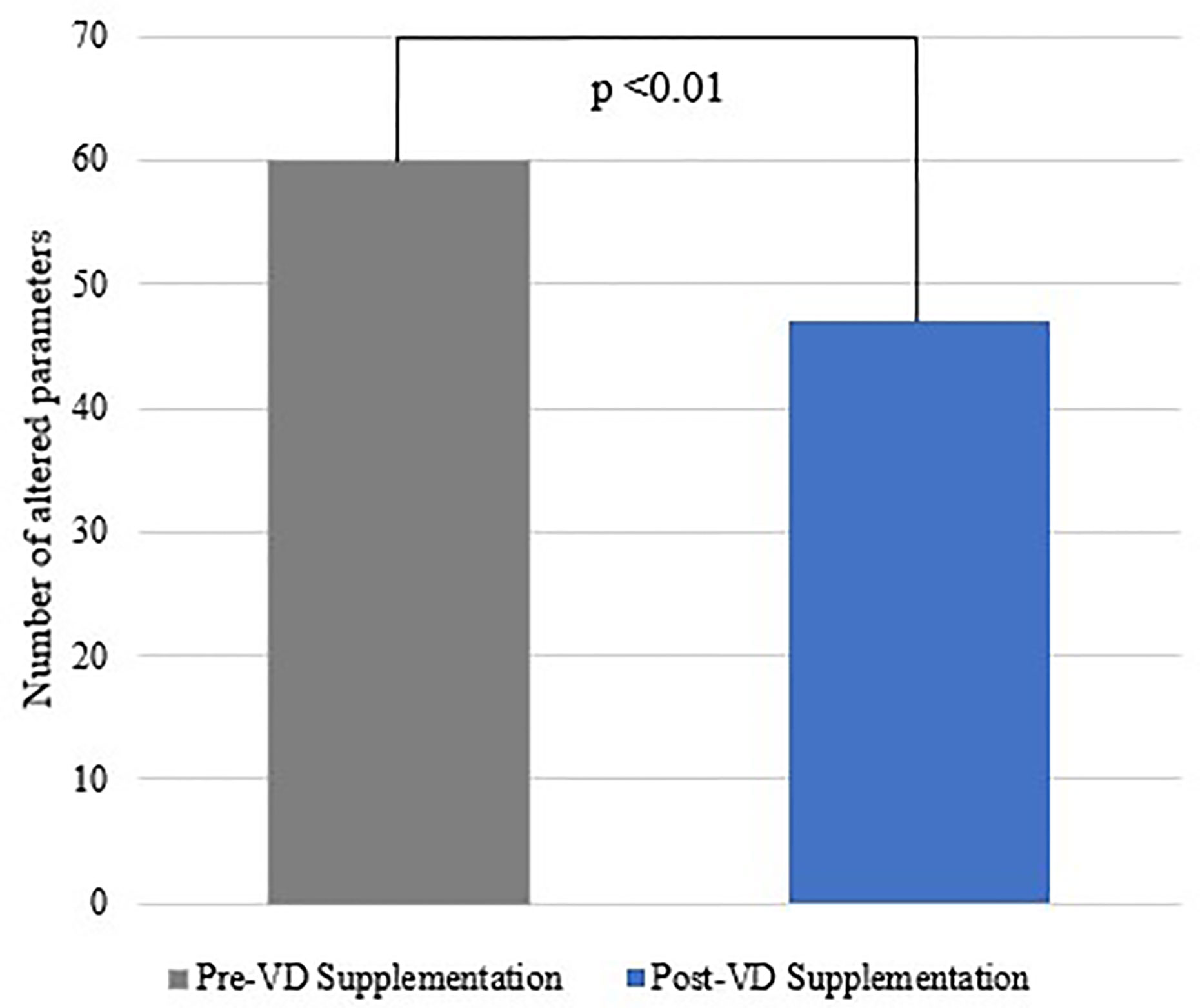
Figure 4 Number of altered frequency domain parameters before and after VD supplementation.
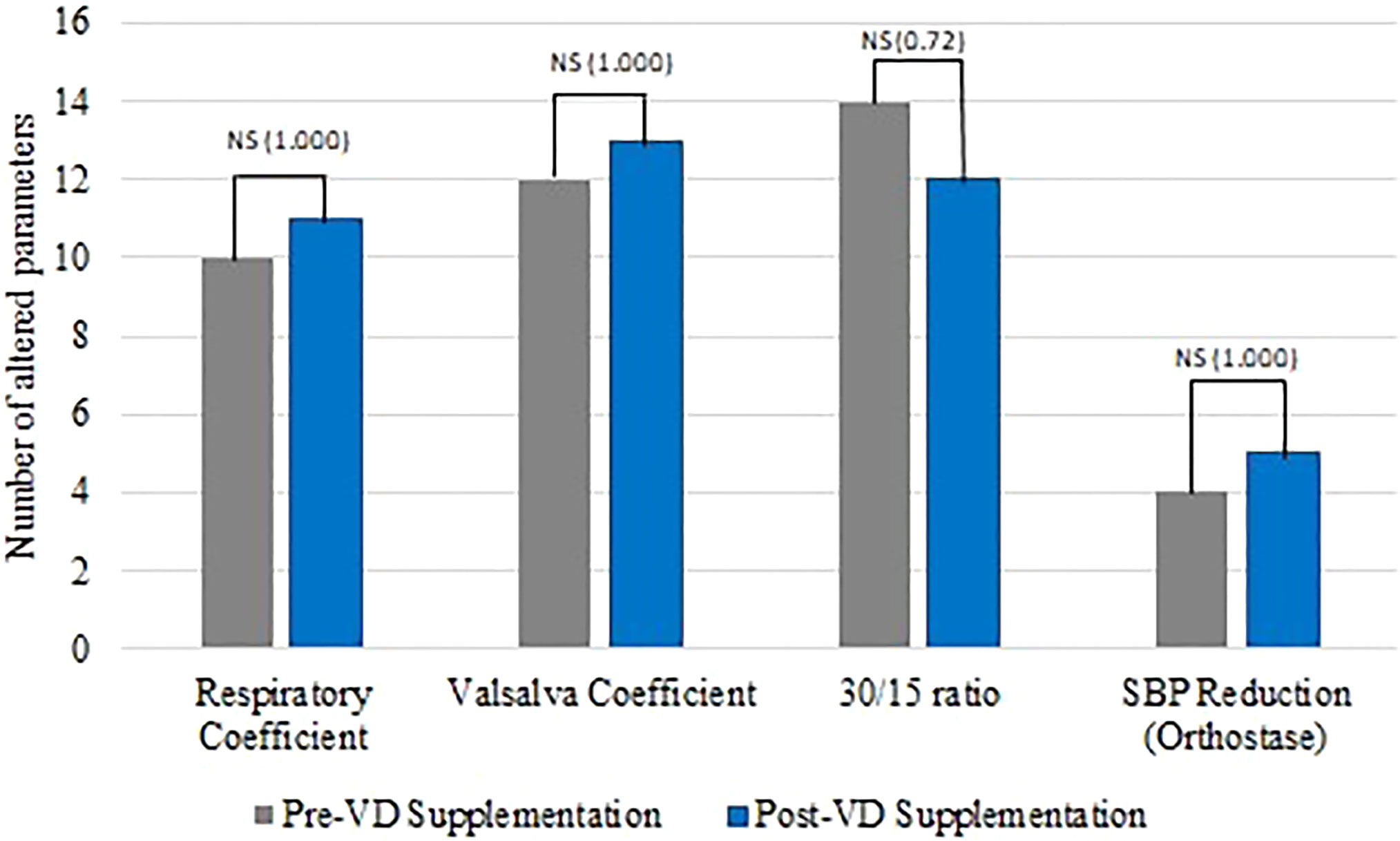
Figure 5 Number of abnormal dynamic tests before and after VD supplementation.
We found correlations between VD variations with percentage of HF and LF/HF ratio (Figures 6 and 7), suggesting a beneficial action of vitamin D in the parasympathetic via.
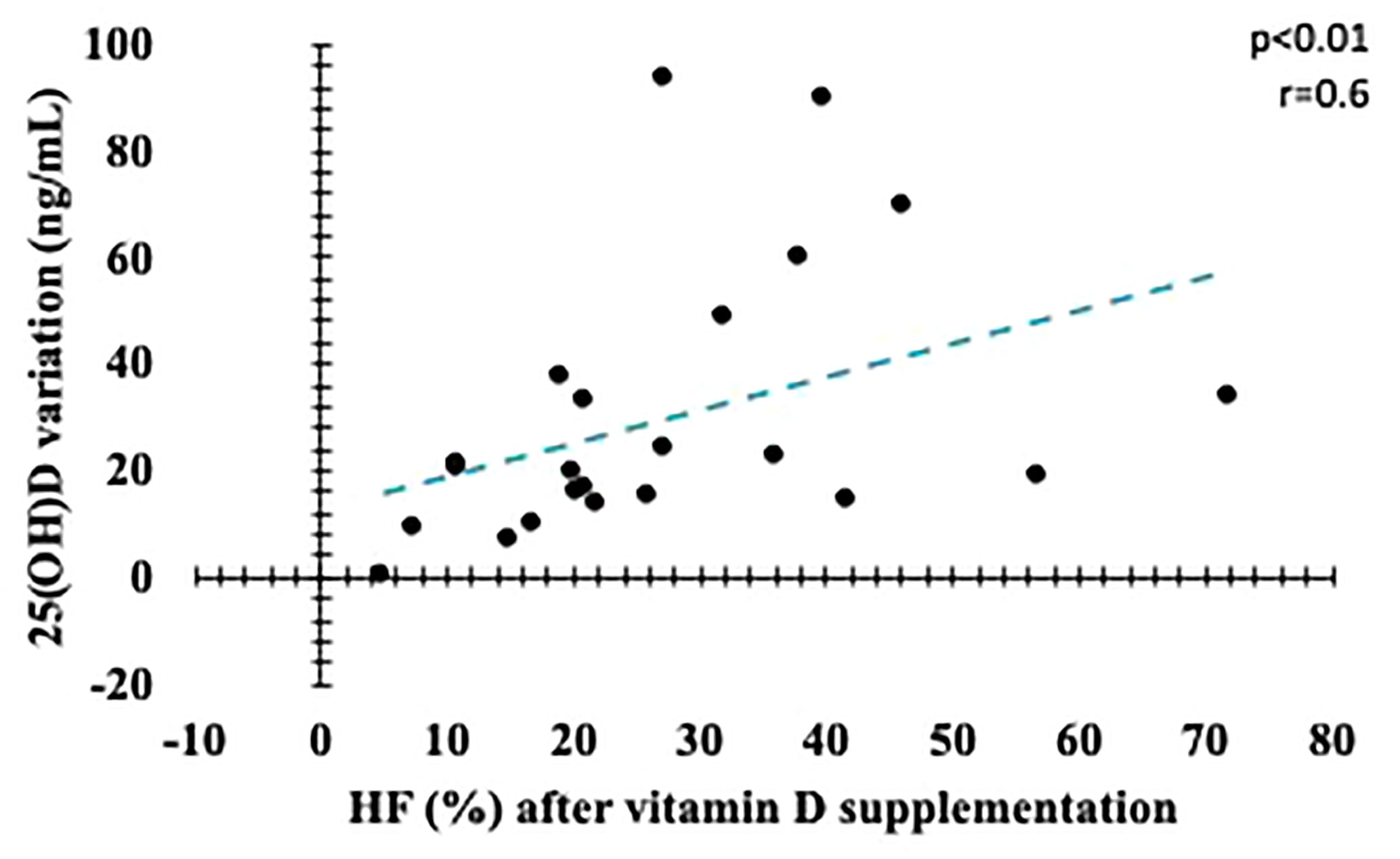
Figure 6 Correlation between variation in serum vitamin D levels and final HF (%). HF, High frequency.
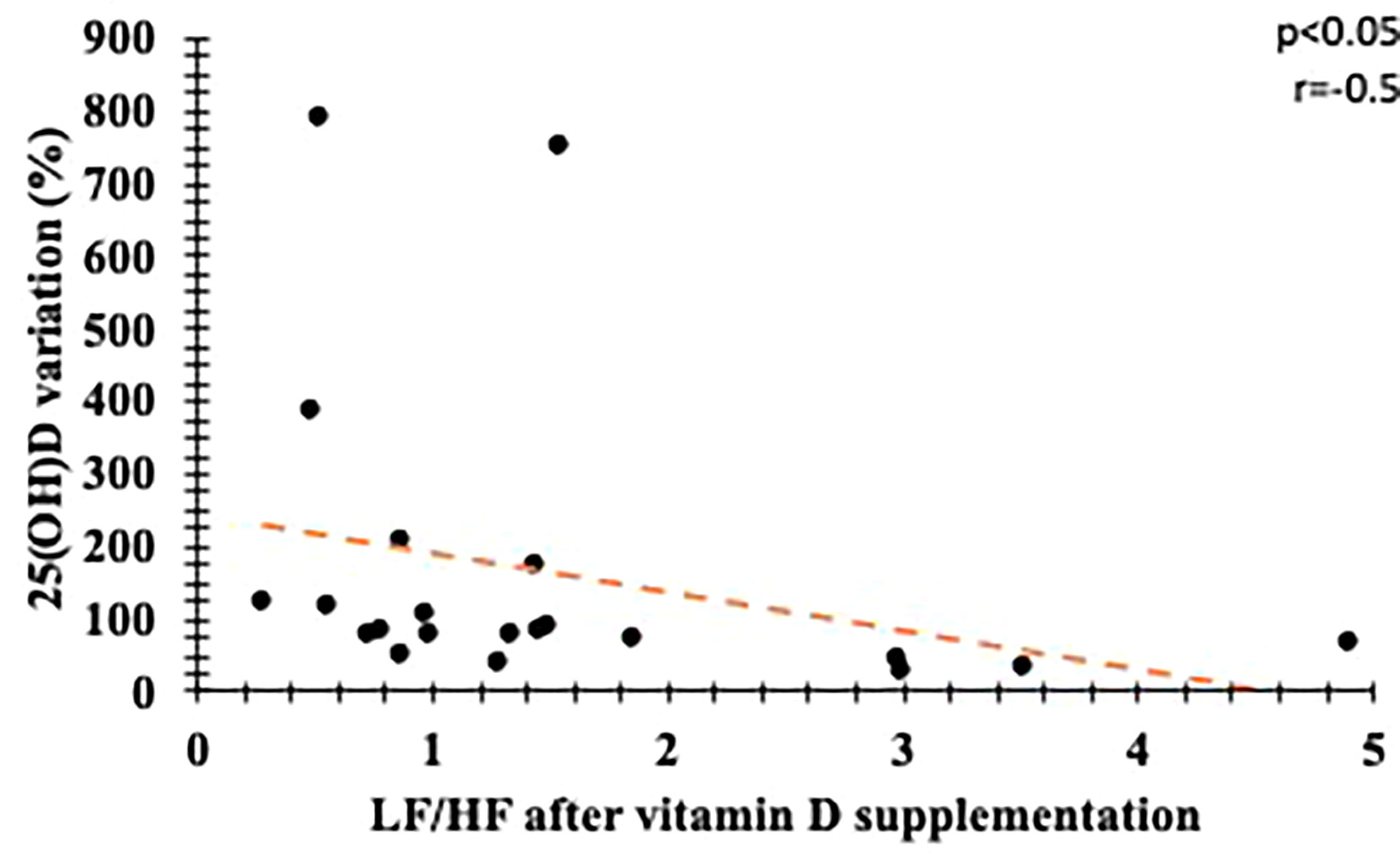
Figure 7 Correlation between percentage variation in serum vitamin D levels and final LF/HF. LF, Low frequency; HF, High frequency.
Discussion
Our study found a strong association between high-dose vitamin D supplementation and improvement in CAN parameters in patients with type 1 diabetes mellitus and autonomic neuropathy. There were no changes in HbA1C, blood pressure, lipid profile and insulin dose. In addition, we observed that percentage variation of serum VD level correlated with improvement in CAN rest parameters.
Resting heart rate variability was advocated by some authors as a sensitive and specific method for diagnosis of cardiovascular dysautonomia. Besides that, it is easier to be performed than dynamic tests and does not need patient collaboration (28–35). Takase et al. (28) found that a cut-off point <30ms in SDNN parameter has a sensitivity of 72% and specificity of 92% for CAN diagnosis in patients with type 2 diabetes, while Ziegler et al. (30) showed that HF index was more sensitive than functional tests to detect precocious autonomic disorder in patients with diabetes, using 0,892 as a cut-off. Likewise, Razainskaite-Virbichiene et al (36) demonstrated that in patients with T1DM, the parameters of time domain in supine position have a coefficient of variation <1.65, reflecting a sensitivity of 94.3% and specificity of 91.5% for the diagnosis of CAN. Additionally HRV variables were independent predictors for developing cardiovascular disease (CVD) in patients with T2DM (28, 30, 34, 36). These findings are in agreement with our results that showed improvement in rest HRV parameters in response to short interventional treatment, as opposed to dynamic tests that remained unchanged.
Some cross-sectional studies and a recent systematic review suggest an association between vitamin D serum level, presence and severity of peripheral neuropathies in patients with diabetes (7–11). In addition, Jung et al (10) and Da Silva et al. (12) showed an association between VD and rest parameters of CAN in this population. Alamdari et al. (37) found that increases of 2.5nmol/L in serum vitamin D correlated with a 2.2% and 3.4% reduction in the prevalence and severity of changes in nerve conduction velocity in people with type 2 diabetes. As far as we are aware, there are not recent publications on vitamin D supplementation effects in people with type 1 diabetes and CAN. The only available study (38) presented 13 healthy, non-diabetic volunteers who had low vitamin D serum level. They received VD supplementation for 28 days with the dose of 5.000 to 10.000UI/day and were submitted to stress with intravenous angiotensin II during 30 min before and after VD use. It was observed a reduction in LF/HF ratio and improvement in HF values. Nevertheless, there were differences in quantity and in profile of subjects, in comparison to our trial. Consequently, until this moment, scientific data about this issue are derived from experimental models and observational studies, which correlate hypovitaminosis D with presence and severity of CAN (7, 8, 10, 12). Therefore, we consider our study the first to evaluate the effect of high-dose VD supplementation in patients with type 1 diabetes with CAN.
There are several major factors associated with CAN onset and progression. For instance, poor glycemic control and variability seem to be enrolled in this complication, as intensive glycemic control reduced CAN incidence after 14 years of follow-up (7, 39, 40). In addition, renin-angiotensin-aldosterone (RAA) system has also been implicated in this pathogenesis, since there seems to be a potential benefit over CAN when the RAA system is blocked with ACE or ARB (41–44). Moreover, physical exercise might be a useful intervention, as endurance activity improves different CAN parameters and reduces compensatory hyperinsulinism, which could contribute to development of vagal autonomic neuropathy (30, 45). Finally, inflammatory and metabolic components seem to influence CAN development. Hansen et al. (7) shows that some inflammatory biomarkers are associated with elevation of HR and worsening of several variability indices. In our study, patients did not show change in glycemic control, insulin resistance (evaluated by dose of insulin used), lipid profile and PCR-US. In addition, there was no change in dose of ACE and ARB or in counseling regarding physical activity during study period. Therefore, the chance that any of these factors could have influenced our results is remote.
We have not evaluated genetic and epigenetic factors that could influence our results. It has been described that, among epigenetic factors, some miRNAs polymorphisms have been studied in this context. Presence of rs2910164 (G>C) MIR146A variant seems to have a beneficial effect in CAN, whereas the variant allele of rs895819 SNP in MIR27A was associated with a higher risk of developing this condition earlier. In addition, polymorphisms in vitamin D receptor (VDR) gene were described in association with type 1 and 2 diabetes mellitus, although there are no data about its correlation with diabetic neuropathy susceptibility (46). It is important to address these aspects in further studies.
A hypothesis that may explain improvement of NAC parameters in present study is action of VD in regulation of neurotrophin (47). This mechanism has been described in several neurological conditions (48) and the presence of VD receptors on neurons and glia cells (49) reinforce that proposition. Although the proper system of this relation are still unspecified, VD may also play an important role on γ-aminobutyric acid (GABA) and glutamatergic neurotransmission, along with suppressing oxidative stress and inhibiting inflammation, therefore, supplying neuroprotection (48).
The effect of vitamin D on diabetes microvascular complications has been studied for some authors (12, 50, 51). Encouraging data were described, particularly on diabetic kidney disease and peripheral neuropathy, though results are still not conclusive. Reports assessing the effect of vitamin D supplementation in CAN are not available, therefore there is an increasing necessity to evaluate if vitamin D has any effect on diabetes complications and whether this effect is dose-dependent.
Since it is a pilot study, our results are insufficient to clarify the real effect of vitamin D supplementation on cardiovascular neuropathy of these patients. Small number of participants, short period of VD supplementation and absence of a placebo-controlled group with CAN suggest that our results are limited in understanding the real utility of vitamin D as a therapeutic option for this complication. Prospective studies with this specific methodology are required to get this answer.
Conclusion
Our data suggest a strong association between high dose vitamin D supplementation and improvement of resting heart rate variability parameters in patients with type 1 diabetes and previous diagnosis of autonomic neuropathy. In addition, correlation between variation of serum vitamin D level and CAN parameters was observed.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by University Hospital Joao de Barros Barreto ethics committee. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript. LS, JF, KF, and NQ took part in conception and design of study. AM, PF, FM, MR, IL, MS, and AC were responsible for acquisition of data, while NMS, ÍS, WS, LJ, NJKS, and JA have done the analysis and interpretation of data. ML, MO, AA, LM, GL, and PP have drafted the manuscript together. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors thank Federal University of Pará, University Hospital João de Barros Barreto, Programa de Pós Graduação em Oncologia e Ciências Médicas and Programa de Pós-Graduação em Atenção e Estudo Clínico no Diabetes for their contribution to the research. This manuscript has been released as a pre-print at Institutional Repository of UFPA, Dissertations in Oncology and Medical Sciences (Master’s) collection—PPGOCM/NPO, (SILVA, 2018).
Abbreviations
25(OH)D, 25-hydroxyvitamin D; CAN, Cardiovascular autonomic neuropathy; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration equation; CVD, Cardiovascular Disease; DM, Diabetes Mellitus; GFR, Glomerular Filtration Rate; HbA1C, Glycated Hemoglobin; HDL-C, High-density lipoprotein cholesterol; HF, High frequency; HPLC, High-performance Liquid Chromatography; HR, Heart rate; HUJBB, Hospital Universitário João de Barros Barreto; HVR, Heart Rate Variability; HZ, Hertz; LDL-C, Low-density lipoprotein cholesterol; LF, Low frequency; PCR-US, Ultrasensitive C-reactive protein; RRmax, Maximum RR interval; RRmin, Minimum RR interval; RRNN, Mean length of regular RR intervals; SBP, Systolic blood pressure; SDNN, Standard deviation of all NN intervals.; T1DM, Type 1 Diabetes Mellitus; TP, Total power; VD, Vitamin D; VLF, Very low frequency.
References
1. Vinik AI, Maser RE, Mitchell BD, Freeman R. Diabetic Autonomic Neuropathy. Diabetes Care (2003) 26:1553–79. doi: 10.2337/diacare.26.5.1553
2. Freeman R. Diabetic autonomic neuropathy. In: Handbook of Clinical Neurology. Holland: Elsevier (2014). p. 63–79. doi: 10.1016/B978-0-444-53480-4.00006-0
3. Zakin E, Abrams R, Simpson DM. Diabetic Neuropathy. Semin Neurol (2019) 39:560–9. doi: 10.1055/s-0039-1688978
4. Vinik AI, Casellini C, Parson HK, Colberg SR, Nevoret M-L. Cardiac Autonomic Neuropathy in Diabetes: A Predictor of Cardiometabolic Events. Front Neurosci (2018) 12:591. doi: 10.3389/fnins.2018.00591
5. Dimitropoulos G. Cardiac autonomic neuropathy in patients with diabetes mellitus. WJD (2014) 5:17. doi: 10.4239/wjd.v5.i1.17
6. Spallone V. Blood Pressure Variability and Autonomic Dysfunction. Curr Diabetes Rep (2018) 18:137. doi: 10.1007/s11892-018-1108-z
7. Hansen CS, Fleischer J, Vistisen D, Ridderstråle M, Jensen JS, Jørgensen ME. High and low vitamin D level is associated with cardiovascular autonomic neuropathy in people with Type 1 and Type 2 diabetes. Diabetes Med (2017) 34:364–71. doi: 10.1111/dme.13269
8. Maser R, Lenhard M, Pohlig R. Vitamin D Insufficiency is Associated with Reduced Parasympathetic Nerve Fiber Function in Type 2 Diabetes. Endocrine Pract (2015) 21:174–81. doi: 10.4158/EP14332.OR
9. Zubair M, Malik A, Meerza D, Ahmad J. 25-Hydroxyvitamin D [25(OH)D] levels and diabetic foot ulcer: Is there any relationship? Diabetes Metab Syndrome: Clin Res Rev (2013) 7:148–53. doi: 10.1016/j.dsx.2013.06.008
10. Jung C-H, Jung S-H, Kim K-J, Kim B-Y, Kim C-H, Kang S-K, et al. The relationship between vitamin D status and cardiac autonomic neuropathy in patients with type 2 diabetes mellitus. Diabetes Vasc Dis Res (2015) 12:342–51. doi: 10.1177/1479164115588546
11. Yammine K, Wehbe R, Assi C. A systematic review on the efficacy of vitamin D supplementation on diabetic peripheral neuropathy. Clin Nutr (2020) 39:S0261561420300455. doi: 10.1016/j.clnu.2020.01.022
12. da Silva DD, Nunez LWP, da Silva Pinheiro DD, de Oliveira LL, Ladeira SS, de Queiroz NNM, et al. Vitamin D deficiency and cardiovascular autonomic neuropathy in patients with type 1 diabetes mellitus. Diabetol Metab Syndr (2015) 7:A44. doi: 10.1186/1758-5996-7-S1-A44
13. Karonova T, Stepanova A, Bystrova A, Jude EB. High-Dose Vitamin D Supplementation Improves Microcirculation and Reduces Inflammation in Diabetic Neuropathy Patients. Nutrients (2020) 12:2518. doi: 10.3390/nu12092518
14. Alam U, Petropoulos IN, Ponirakis G, Ferdousi M, Asghar O, Jeziorska M, et al. Vitamin D deficiency is associated with painful diabetic neuropathy. Diabetes Metab Res Rev (2020) e3361:1–8. doi: 10.1002/dmrr.3361
15. Chakhtoura M, Azar ST. The Role of Vitamin D Deficiency in the Incidence, Progression, and Complications of Type 1 Diabetes Mellitus. Int J Endocrinol (2013) 2013:1–10. doi: 10.1155/2013/148673
16. Riaz S, Malcangio M, Miller M, Tomlinson DR. A vitamin D 3 derivative (CB1093) induces nerve growth factor and prevents neurotrophic deficits in streptozotocin-diabetic rats. Diabetologia (1999) 42:1308–13. doi: 10.1007/s001250051443
17. Felício KM, de Souza ACCB, Neto JFA, de Melo FTC, Carvalho CT, Arbage TP, et al. Glycemic Variability and Insulin Needs in Patients with Type 1 Diabetes Mellitus Supplemented with Vitamin D: A Pilot Study Using Continuous Glucose Monitoring System. CDR (2018) 14:395–403. doi: 10.2174/1573399813666170616075013
18. de Queiroz NNM, de Melo FTC, Resende F de S, Janaú LC, de Souza Neto NJK, de Lemos MN, et al. High-dose Cholecalciferol Supplementation Reducing Morning Blood Pressure in Normotensive DM1 Patients. CDR (2020) 16. doi: 10.2174/1573399816999200729131508
19. Felício JS, Luz RM, de Melo FTC, de Souza Resende F, de Oliveira AF, Peixoto AS, et al. Vitamin D on Early Stages of Diabetic Kidney Disease: A Cross-sectional Study in Patients with Type 1 Diabetes Mellitus. Front Endocrinol (2016) 7(149):1–6. doi: 10.3389/fendo.2016.00149
20. Felício JS, de Oliveira AF, Peixoto AS, de Souza ACCB, Abrahão Neto JF, de Melo FTC, et al. Albuminuria Reduction after High Dose of Vitamin D in Patients with Type 1 Diabetes Mellitus: A Pilot Study. Front Endocrinol (2017) 8:199. doi: 10.3389/fendo.2017.00199
21. Spallone V, Ziegler D, Freeman R, Bernardi L, Frontoni S, Pop-Busui R, et al. Cardiovascular autonomic neuropathy in diabetes: clinical impact, assessment, diagnosis, and management: Diabetic Cardiovascular Autonomic Neuropathy in Clinical Practice. Diabetes Metab Res Rev (2011) 27:639–53. doi: 10.1002/dmrr.1239
22. Ameircan Diabetes Association. Improving Care and Promoting Health in Populations. Standards Med Care Diabetes 2020 Dia Care (2020) 43:S7–S13. doi: 10.2337/dc20-S001
23. DiaSorin. LIAISON 25 OH vitamin D TOTAL Assay [Brochure]. Stillwater, MN, USA: DiaSorin (2019). Available at: https://www.diasorin.com/en/node/8476.
24. DEQAS. Vitamin D External Quality Assessment Scheme. DEQAS Review 2016/2017. London, UK: DEQAS (2017). Available at: http://www.deqas.org/downloads/DEQAS%20Review%20October%202017.pdf.
25. Levey AS, Stevens LA, Schmid CH, Zhang Y(, Castro AF, Feldman HI, et al. A New Equation to Estimate Glomerular Filtration Rate. Ann Intern Med (2009) 150:604. doi: 10.7326/0003-4819-150-9-200905050-00006
26. Ewing DJ. Assessment of Cardiovascular Effects in Diabetic Autonomic Neuropathy and Prognostic Implications. Ann Intern Med (1980) 92:308. doi: 10.7326/0003-4819-92-2-308
27. Felício JS, Santos FM, de Souza ACC, Felício KM, Ribeiro AB, Zanella MT. Autonomic neuropathy tests correlate with left ventricular mass and cardiac diastolic function in normotensive patients with type 2 diabetes mellitus and without left ventricular hypertrophy. Exp Clin Cardiol (2010) 15:e5–9.
28. Takase B, Kurita A, Noritake M, Uehata A, Maruyama T, Nagayoshi H, et al. Heart rate variability in patients with diabetes mellitus, ischemic heart disease, and congestive heart failure. J Electrocardiol (1992) 25:79–88. doi: 10.1016/0022-0736(92)90112-D
29. Howorka K, Pumprla J, Schabmann A. Optimal parameters of short-term heart rate spectrogram for routine evaluation of diabetic cardiovascular autonomic neuropathy. J Autonomic Nerv System (1998) 69:164–72. doi: 10.1016/S0165-1838(98)00015-0
30. Ziegler D, Strom A, Bönhof G, Püttgen S, Bódis K, Burkart V, et al. Differential associations of lower cardiac vagal tone with insulin resistance and insulin secretion in recently diagnosed type 1 and type 2 diabetes. Metabolism (2018) 79:1–9. doi: 10.1016/j.metabol.2017.10.013
31. Balcıoğlu S, Arslan U, Türkoğlu S, Özdemir M, Çengel A. Heart Rate Variability and Heart Rate Turbulence in Patients With Type 2 Diabetes Mellitus With Versus Without Cardiac Autonomic Neuropathy. Am J Cardiol (2007) 100:890–3. doi: 10.1016/j.amjcard.2007.03.106
32. Khandoker AH, Jelinek HF, Palaniswami M. Identifying diabetic patients with cardiac autonomic neuropathy by heart rate complexity analysis. BioMed Eng Online (2009) 8:3. doi: 10.1186/1475-925X-8-3
33. Seyd P.T. A, Joseph PK, Jacob J. Automated Diagnosis of Diabetes Using Heart Rate Variability Signals. J Med Syst (2012) 36:1935–41. doi: 10.1007/s10916-011-9653-x
34. Cha S-A, Park Y-M, Yun J-S, Lee S-H, Ahn Y-B, Kim S-R, et al. Time- and frequency-domain measures of heart rate variability predict cardiovascular outcome in patients with type 2 diabetes. Diabetes Res Clin Pract (2018) 143:159–69. doi: 10.1016/j.diabres.2018.07.001
35. da Silva PZ, Schneider RH. The role of vitamin D in muscle strength among the elderly. Acta Fisiátrica (2016) 23:1–9. doi: 10.5935/0104-7795.20160019
36. Razanskaite-Virbickiene D, Danyte E, Mockeviciene G, Dobrovolskiene R, Verkauskiene R, Zalinkevicius R. Can coefficient of variation of time-domain analysis be valuable for detecting cardiovascular autonomic neuropathy in young patients with type 1 diabetes: a case control study. BMC Cardiovasc Disord (2017) 17:34. doi: 10.1186/s12872-016-0467-0
37. Alamdari A, Mozafari R, Tafakhori A, Faghihi-Kashani S, Hafezi-Nejad N, Sheikhbahaei S, et al. An inverse association between serum vitamin D levels with the presence and severity of impaired nerve conduction velocity and large fiber peripheral neuropathy in diabetic subjects. Neurol Sci (2015) 36:1121–6. doi: 10.1007/s10072-015-2207-0
38. Mann MC, Exner DV, Hemmelgarn BR, Turin TC, Sola DY, Ellis L, et al. Vitamin D supplementation is associated with improved modulation of cardiac autonomic tone in healthy humans. Int J Cardiol (2014) 172:506–8. doi: 10.1016/j.ijcard.2014.01.058
39. Pop-Busui R, Low PA, Waberski BH, Martin CL, Albers JW, Feldman EL, et al. Effects of Prior Intensive Insulin Therapy on Cardiac Autonomic Nervous System Function in Type 1 Diabetes Mellitus: The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Study (DCCT/EDIC). Circulation (2009) 119:2886–93. doi: 10.1161/CIRCULATIONAHA.108.837369
40. Fleischer J, Laugesen E, Cichosz SL, Hoeyem P, Dejgaard TF, Poulsen PL, et al. Continuous glucose monitoring adds information beyond HbA1c in well-controlled diabetes patients with early cardiovascular autonomic neuropathy. J Diabetes Complications (2017) 31:1389–93. doi: 10.1016/j.jdiacomp.2017.06.013
41. Malik RA, Williamson S, Abbott C, Carrington AL, Iqbal J, Schady W, et al. Effect of angiotensin-converting-enzyme (ACE) inhibitor trandolapril on human diabetic neuropathy: randomised double-blind controlled trial. Lancet (1998) 352:1978–81. doi: 10.1016/S0140-6736(98)02478-7
42. Gæde P, Vedel P, Larsen N, Jensen GVH, Parving H-H, Pedersen O. Multifactorial Intervention and Cardiovascular Disease in Patients with Type 2 Diabetes. N Engl J Med (2003) 348:383–93. doi: 10.1056/NEJMoa021778
43. Coppey LJ, Davidson EP, Rinehart TW, Gellett JS, Oltman CL, Lund DD, et al. ACE Inhibitor or Angiotensin II Receptor Antagonist Attenuates Diabetic Neuropathy in Streptozotocin-Induced Diabetic Rats. Diabetes (2006) 55:341–8. doi: 10.2337/diabetes.55.02.06.db05-0885
44. Didangelos T, Tziomalos K, Margaritidis C, Kontoninas Z, Stergiou I, Tsotoulidis S, et al. Efficacy of Administration of an Angiotensin Converting Enzyme Inhibitor for Two Years on Autonomic and Peripheral Neuropathy in Patients with Diabetes Mellitus. J Diabetes Res (2017) 2017:1–6. doi: 10.1155/2017/6719239
45. Röhling M, Strom A, Bönhof GJ, Roden M, Ziegler D. Cardiorespiratory Fitness and Cardiac Autonomic Function in Diabetes. Curr Diabetes Rep (2017) 17:125. doi: 10.1007/s11892-017-0959-z
46. da Silva MER, Mory D, Davini E. Marcadores genéticos e auto-imunes do diabetes melito tipo 1: da teoria para a prática. Arq Bras Endocrinol Metab (2008) 52:166–80. doi: 10.1590/S0004-27302008000200004
47. Peitl V, Silić A, Orlović I, Vidrih B, Crnković D, Karlović D. Vitamin D and Neurotrophin Levels and Their Impact on the Symptoms of Schizophrenia. Neuropsychobiology (2020) 79:179–85. doi: 10.1159/000504577
48. Moretti R, Morelli ME, Caruso P. Vitamin D in Neurological Diseases: A Rationale for a Pathogenic Impact. IJMS (2018) 19:2245. doi: 10.3390/ijms19082245
49. Lang F, Ma K, Leibrock C. 1, 25(OH)2D3 in Brain Function and Neuropsychiatric Disease. Neurosignals (2019) 27:40–9. doi: 10.33594/000000182
50. Manson JE, Brannon PM, Rosen CJ, Taylor CL. Vitamin D Deficiency — Is There Really a Pandemic? N Engl J Med (2016) 375:1817–20. doi: 10.1056/NEJMp1608005
Keywords: diabetes mellitus type 1, cardiovascular autonomic neuropathy, vitamin D, heart rate, autonomic nervous system
Citation: Silva LdSD’A, de Queiroz NNM, de Melo FTC, Abrahão Neto JF, Janaú LC, de Souza Neto NJK, de Lemos MN, de Oliveira MCNI, de Alcântara AL, de Moraes LV, da Silva WM, de Souza ÍJA, Said NM, de Lemos GN, Felício KM, Santos MCd, Motta ARB, dos Reis MdSO, Lobato IJC, de Figueiredo PBB, de Souza ACCB, Piani PPF and Felício JS (2020) Improvement in Cardiovascular Autonomic Neuropathy After High-Dose Vitamin D Supplementation in Patients With Type 1 Diabetes. Front. Endocrinol. 11:605681. doi: 10.3389/fendo.2020.605681
Received: 12 September 2020; Accepted: 21 October 2020;
Published: 19 November 2020.
Edited by:
Rayaz A. Malik, Weill Cornell Medicine-Qatar, QatarReviewed by:
Péter Kempler, Semmelweis University, HungaryUazman Alam, University of Liverpool, United Kingdom
Copyright © 2020 Silva, de Queiroz, de Melo, Abrahão Neto, Janaú, de Souza Neto, de Lemos, de Oliveira, de Alcântara, de Moraes, da Silva, de Souza, Said, de Lemos, Felício, Santos, Motta, dos Reis, Lobato, de Figueiredo, de Souza, Piani and Felício. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: João Soares Felício, ZmVsaWNpby5iZWxAdGVycmEuY29tLmJy