 Giovanni Monastra1
Giovanni Monastra1 Ivana Vucenik2
Ivana Vucenik2 Abdel Halim Harrath3Saleh H. Alwasel3
Abdel Halim Harrath3Saleh H. Alwasel3 Zdravko A. Kamenov4Antonio Simone Laganà5
Zdravko A. Kamenov4Antonio Simone Laganà5 Noemi Monti6
Noemi Monti6 Valeria Fedeli6
Valeria Fedeli6 Mariano Bizzarri6*
Mariano Bizzarri6*- 1Systems Biology Group Lab (SBGLab), Sapienza University, Rome, Italy
- 2Department of Medical and Research Technology, University of Maryland School of Medicine, Baltimore, MD, United States
- 3Department of Zoology, College of Science, King Saud University, Riyadh, Saudi Arabia
- 4Department of Internal Medicine, Medical University of Sofia, Sofia, Bulgaria
- 5Department of Obstetrics and Gynecology, “Filippo Del Ponte” Hospital, University of Insubria, Varese, Italy
- 6Department of Experimental Medicine, Systems Biology Group Lab, University Sapienza, Rome, Italy
A New Approaches in PCOS Treatment
Myo-Inositol (myo-Ins) and its phosphate derivatives—including inositol phosphates (InsPs), inositol pyrophosphates (IPPs) and phosphatidyl-inositol phosphate (PtdIns)—are credited to act as second messengers, which accumulate rapidly and transiently in response to external or endocrine signals, a phenomenon that allows signaling to be discrete and regulated (1, 2). Noticeably, inositol is involved in the transduction of several endocrine signals, including insulin (3, 4), thyroid hormones (5), gonadotropins (6), lipids with hormone-like activity (as prostaglandins) (7), and many other endocrine systems (8). Namely, in the last decade, a growing body of clinical and experimental research provided robust evidence about the efficiency of inositol in reversing a few clinical, metabolic, and endocrine features of the Polycystic Ovary Syndrome (PCOS). Myo-inositol, alone or in combination with its isomer D-Chiro-Inositol (D-Chiro-Ins), showed to exert a variable—albeit significant—effect in improving both symptoms and outcome in PCOS patients (9). Experimental and pilot clinical studies pointed out that a combination of both isomers could provide a reliable rationale for establishing a proper treatment strategy, as first suggested by Beemster’s seminal study (10, 11).
However, the proper formula—i.e., the respective percentage of myo-Ins and D-Chiro-Ins—is still a matter of debate. In several cases, no conclusive insights can be obtained from clinical trials based on unclear rational design, limited number of recruited patients and variable formula composition and dosage(s).
First, it is improper to compare clinical results from studies in which commercial nutraceutical formulas involve a wide range of concentrations (Table 1), with the myo-Ins/D-Chiro-Ins ratio varying implausibly from 0.4:1 to 104:1.
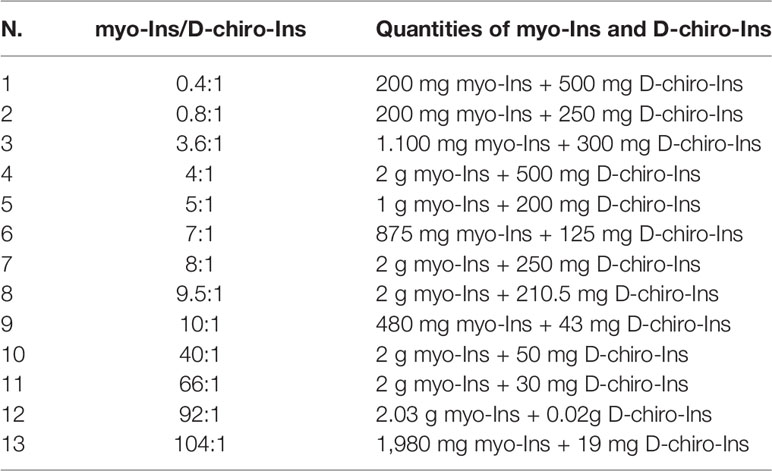
Table 1 Different myo-Ins/D-chiro-Ins ratios in commercial nutraceutical formulas.
Current commercial preparations also contain D-Chiro-Ins alone at concentrations reaching 600 mg that can be administered once or twice a day. Therefore, the daily dose of D-chiro-Ins, alone or with myo-Ins, ranges from low (less than 300 mg/die), medium (300–600 mg/die) and high (600–1,200 mg/die).
Inositols as Endocrine Modulators
No plausible hypothesis can justify these bizarre “compositions”, and consequently is not surprisingly that so different results have been gathered with nutraceutical supports deprived of any scientific evidence. We would also ask if it is ethical to permit that such “drugs”, while deceiving consumers, should invade the market, baffling both the Regulatory Agency’s control, as well as common sense. It is also regrettable that in some cases scientific journals have not felt the duty to inform correctly, by underestimating potential conflict of interest and biased methodological approaches (12), thus contributing to worsen the “epidemic” of controversial/irreproducible/biased results that plague current clinical research (13).
Second, several published reports (14) seems to ignore that myo-Ins and D-Chiro-Ins display opposite effects upon ovary and steroidogenesis, despite both improve insulin transduction and glucose utilization, through their inositolphosphoglycans (IPGs) derivatives (15). However important it may be, imbalance in glucose and insulin metabolism cannot explain by itself the overall history of PCOS pathogenesis.
Indeed, some evidence suggests that D-Chiro-Ins can directly regulate steroidogenic enzyme genes in human granulosa cells, reducing the mRNA expression of both aromatase and cytochrome P450 side-chain cleavage genes in a dose–response fashion (16). Furthermore, D-Chiro-Ins increases testosterone levels in theca cells from PCOS women (17). Those data should have suggested caution in treating PCOS women with high doses of D-Chiro-Ins. Indeed, despite the promising results obtained in a pivotal study (18), a subsequent investigation using high D-Chiro-Ins dosages was unable to confirm those preliminary results and was discontinued (19).
On the other hand, myo-Ins participates in the modulation of the FSH signaling, as suggested by clinical and experimental data. Indeed, upon myo-Ins treatment, LH/FSH ratio in plasma of PCOS women significantly decreases (20–22), while in vitro fertilization myo-Ins supplementation allows to significantly reduce the amount of recombinant FSH administered (6, 23). In turn, FSH stimulates aromatase synthesis, a critical step in androgen conversion to estrogens and in terminal follicle maturation (24). It is worth noting that downregulation of FSH and subsequent dramatic decrease in aromatase synthetized by granulosa cells constitute a hallmark of PCOS (25). Noticeably, while D-Chiro-Ins inhibits aromatase as previously recalled, myo-Ins seems to enhance aromatase synthesis in granulosa as well as in endocrine-responsive breast cancer, probably acting also through a direct genomic modulation, given that in breast cancer cell the observed increase in aromatase is independent from FSH stimulation (26). Moreover, myo-Ins can modulate steroidogenesis in the ovary by exerting complex effects upon cytoskeleton architecture (27). Therefore, it is not surprising that in physiological homeostatic conditions, the myo-Ins/D-Chiro-Ins ratio in ovarian tissues is kept within the range of 70–00:1, while in ovaries from PCOS women this ratio is pathologically decreased (28, 29). Conversely, high levels of D-Chiro-Ins show detrimental effects upon blastocyst quality (30). An appreciable step forward in understanding the tricky interplay in between myo-Ins and D-Chiro-Ins in modulating the ovarian physiology has been carried out by Bevilacqua et al. in a recent paper in which the effectiveness of different myo-Ins/D-Chiro-Ins formulas was experimentally addressed in PCOS mice (31). This study provided the first experimental evidence of the different efficacy exerted by various myo-Ins/D-Chiro-Ins ratios (5:1; 20:1; 40:1; 80:1) in restoring a normal phenotype. Mice treated daily with 420 mg/kg myo-Ins/D-Chiro-Ins in a 40:1 molar ratio made a fast and almost full recovery from PCOS signs and symptoms. On the contrary, the other myo-Ins/D-Chiro-Ins ratios were less effective or had even negative effects. In particular, the formulation with higher D-Chiro-Ins content proved to worsen the PCOS pathological features. Some clinical studies have recently confirmed these results in PCOS women (32), thus vindicating the keen insight first advanced by Unfer (33, 34).
Furthermore, administration of high concentrations of D-Chiro-Ins can have not only detrimental effects upon follicle functions but can also impair myo-Ins availability. A recent study by Garzon et al. showed that 1 g D-Chiro-Ins significantly reduces the intestinal absorption of 6 g myo-Ins (35). The same effect can be obtained by administering maltodextrin, sorbitol (36) or phlorizin (37), a non-transported competitive inhibitor of sodium-coupled sugar co-transporters. In the study by Garzon et al. (35), performed in female and male volunteers, the plasma myo-Ins/D-Chiro-Ins ratio was 6:1, which is strongly in favor of D-Chiro-Ins, when compared to the physiological value (40:1) (38).
This effect can be explained by hypothesizing a competitive action upon inositol transporter. In fact, SMIT2 transports myo-Ins with an average KM of 120–150 μM, with good agreement with plasma levels of myo-Ins (32.5 ± 1.5 μM, ranging from 26.8 to 43.0 μM) (39). D-Chiro-Ins is transported with an average KM of 110–130 μM, similar to myo-Ins; nevertheless, the average plasma concentration of D-Chiro-Ins is usually less than 100 nM and hence it is unlikely that it can interfere with myo-Ins absorption under normal conditions (40). Moreover, this observation implies that in the physiological setting SMIT2-based transport is only marginally committed in ensuring D-Chiro-Ins absorption, and D-Chiro-Ins could hardly impair myo-Ins uptake. However, when D-Chiro-Ins is administered at high dosage (i.e., ≥1 g), it could efficiently compete with myo-Ins for absorption at the gut level, thus decreasing the myo-Ins/D-Chiro-Ins ratio in plasma. Conversely, while pharmaceutical formulas in the physiological ratio of 40:1 are unlikely to impair myo-Ins uptake, other studies in which high D-Chiro-ins concentrations were used can significantly reduce myo-Ins bioavailability.
The unexpected competitive inhibition exerted by D-Chiro-Ins as well by other small sugar-like molecules may help explaining the phenomenon of the so-called “inositol resistance”—highlighted by several clinical trials—that could account for 30–40% of inositol failure in PCOS treatment (41). Resistance can be ascribed to insufficient inositol availability, as suggested by studies in which the intestinal absorption of inositols significantly increases in humans upon co-administration of α-lactalbumin that reversibly opens the tight junctions (42). Noticeably, the association of myo-Ins with α-lactalbumin demonstrated to be beneficial in restoring ovulation and in improving PCOS features by counteracting “inositol resistance” in a group of PCOS women (43). This study confirms how relevant could be achieving high plasma levels of myo-Ins in the therapeutic management of PCOS.
At the very beginning, studies on inositol in PCOS management were mostly influenced by metabolic considerations, given that D-Chiro-Ins is required to allow insulin transduction (44) It should be recalled that myo-Ins epimerization into D-Chiro-Ins is under the control of insulin, which tightly modulate the conversion rate according to the tissues needs (45). Noteworthy, both insulin resistance and diabetes type 2 have been associated with reduced availability of D-Chiro-Ins, suggesting that it should act as insulin second messenger and insulin-sensitizing agent (46).
The highest conversion rate of myo-Ins into D-Chiro-Ins is close to 9%, and was detected in liver and muscle, two important insulin sensitive areas, whereas in hearth and brain is less than 2% (47). Remarkably, in biological fluids the myo-Ins/D-Chiro-Ins ratio ranges from 40:1, in plasma, to 100:1 in follicular fluid (28). Differences in in the ratio values highlight that tissues display significant differential needs of both isomers. Insulin resistance can dramatically impair D-Chiro-Ins levels in many tissues, with resulting low intracellular levels of D-Chiro-Ins (48). Conversely, restoring D-Chiro-Ins levels proved to be beneficial in ameliorating diabetes-related metabolic features, and in reducing the insulin stimulation upon theca cells and, hence, the consequent insulin-dependent enhancement of androgenesis (49), given that insulin-dependent stimulation of ovarian epimerase will be appreciably tempered upon D-Chiro-Ins supplementation. However, D-Chiro-Ins administration exceeding the need to mitigate insulin secretion would likely impair ovary function by dramatically decreasing myo-Ins levels in the ovary, as demonstrated by Larner’s seminal paper (29). However, this “metabolic” model is biased by the assumption that PCOS pathogenesis mostly relies upon a metabolic “defect” (i.e., defective insulin transduction due to impaired availability of inositolphosphoglycans) and underestimates the steroidogenic effects directly triggered by myo-Ins and especially by D-Chiro-Ins. Exceeding doses of D-Chiro-Ins may indeed enhance androgenesis and hamper aromatase synthesis, as previously mentioned. Probably, the role of insulin resistance in underpinning PCOS pathogenesis has been too much emphasized since the first report in which a link was hypothesized in between PCOS and defects in insulin/glucose metabolism (50). Yet, the whole evidence related to D-Chiro-Ins is still scarce and should be urgently updated through focused investigations, namely by ascertaining the different evolution of PCOS associated with mixed insulin resistance compared to PCOS with exclusively muscular or exclusively hepatic insulin resistance (51).
The Right Formula
Overall, those data suggest that the choice of the respective concentrations of the two isomers should be carefully weighted and not left to improvisation. Namely, if the aim pursued is that of improving the ovary responsiveness to the FSH-Aromatase endocrine axis—as is the case in PCOS management—high dosages of D-Chiro-Ins should be avoided. After all, the fact that D-Chiro-Ins is usually excreted in urine in large amounts, showing a higher urinary D-Chiro-Ins/myo-Ins ratio, seems to suggest that kidney can selectively concentrates and then excretes D-Chiro-Ins in excess, which can be potentially harmful (47). Different D-Chiro-Ins dosages can be eventually conceived (and properly tested) in specific pathological conditions (anti-estrogenic treatments, diabetes)?, with the aim to primarily inhibit aromatase activity or foster insulin activity in non-ovarian tissues (52). However, it should be borne in mind that high dosages of D-Chiro-Ins should be avoided in PCOS patients. Instead, their administration can be useful if the therapeutic goal is to reduce aromatase activity and/or increase testosterone levels.
It is increasingly appreciated that PCOS may assume different clinical phenotypes and consequently proper assessment of the biochemical and medical features of each patho-phenotypes are required to adopt the best effective therapeutic strategy (53). Accordingly, it can be surmised that inositol-based treatments should be tailored for those specific clinical PCOS phenotypes for which a robust evidence has been provided.
Thereby, future studies are mandatory to ascertain the molecular basis of inositol activity upon ovarian cells and to investigate the beneficial effects of an appropriate myo-Ins/D-Chiro-Ins formula on larger cohorts of patients and on different PCOS phenotypes, besides promising results have been hitherto obtained with pharmacological formulas in which the myo-Ins/D-Chiro-Ins ratio is set at 40:1, according to the physiological plasma value (54). For now, empirical solutions, based on inappropriate pathogenic models and baseless statements, should be mandatorily avoided.
Author Contributions
GM, MB, IV, ZK, AH, SA and AL: conceptualization and writing. AH and SA: funding acquisition. NM and VF: supervision, revision and editing. All authors contributed to the article and approved the submitted version.
Funding
AH, SA, and MB extend their appreciation to the International Scientific Partnership program ISPP at King Saud University for funding this research work through ISPP-122.
Conflict of Interest
In the past, GM was employed as advisor by the company Lo.Li Pharma Co., Italy.
The authors declare that this study did not receive any funding from private companies. Supporting funds were only received from King Saud University. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Hughes AR, Horstman DA, Takemura H, Putney JW Jr. Inositol phosphate metabolism and signal transduction. Am Rev Respir Dis (1990) 141(3 Pt 2):S115–8. doi: 10.1164/ajrccm/141.3_Pt_2.S115
2. Chakraborty A, Kim S, Snyder SH. Inositol pyrophosphates as mammalian cell signals. Sci Signal (2011) 4(188):re1. doi: 10.1126/scisignal.2001958
3. Jones DR, Varela-Nieto I. Diabetes and the role of inositol-containing lipids in insulin signaling. Mol Med (1999) 5(8):505–14. doi: 10.1007/BF03401978
4. Larner J, Brautigan DL, Thorner MO. D-chiro-inositol glycans in insulin signaling and insulin resistance. Mol Med (2010) 16(11-12):543–52. doi: 10.2119/molmed.2010.00107
5. Benvenga S, Antonelli A. Inositol(s) in thyroid function, growth and autoimmunity. Rev Endocr Metab Disord (2016) 17(4):471–84. doi: 10.1007/s11154-016-9370-3
6. Lagana AS, Vitagliano A, Noventa M, Ambrosini G, D’Anna R. Myo-inositol supplementation reduces the amount of gonadotropins and length of ovarian stimulation in women undergoing IVF: a systematic review and meta-analysis of randomized controlled trials. Arch Gynecol Obstet (2018) 298(4):675–84. doi: 10.1007/s00404-018-4861-y
7. Sales KJ, Milne SA, Williams AR, Anderson RA, Jabbour HN. Expression, localization, and signaling of prostaglandin F2 alpha receptor in human endometrial adenocarcinoma: regulation of proliferation by activation of the epidermal growth factor receptor and mitogen-activated protein kinase signaling pathways. J Clin Endocrinol Metab (2004) 89(2):986–93. doi: 10.1210/jc.2003-031434
8. Catt KJ, Hunyady L, Balla T. Second messengers derived from inositol lipids. J Bioenerg Biomembr (1991) 23(1):7–27. doi: 10.1007/BF00768836
9. Lagana AS, Garzon S, Casarin J, Franchi M, Ghezzi F. Inositol in Polycystic Ovary Syndrome: Restoring Fertility through a Pathophysiology-Based Approach. Trends Endocrinol Metab (2018) 29(11):768–80. doi: 10.1016/j.tem.2018.09.001
10. Beemster P, Groenen P, Steegers-Theunissen R. Involvement of inositol in reproduction. Nutr Rev (2002) 60(3):80–7. doi: 10.1301/00296640260042748
11. Dinicola S, Chiu TT, Unfer V, Carlomagno G, Bizzarri M. The rationale of the myo-inositol and D-chiro-inositol combined treatment for polycystic ovary syndrome. J Clin Pharmacol (2014) 54(10):1079–92. doi: 10.1002/jcph.362
12. Laganà A, Aragona C. Effects of oral supplementation with Inositols in women with polycystic ovary syndrome undergoing in vitro fertilization: a long and windy road. Organisms (2019) 3(1):11–3. doi: 10.13133/2532-5876_5.3
13. Ioannidis JP. Why most published research findings are false. PloS Med (2005) 2(8):e124. doi: 10.1371/journal.pmed.0020124
14. Genazzani A. Inositols: reflections on how to choose the appropriate one for PCOS. Gynecol Endocrinol (2020) 36(12):1045–6. doi: 10.1080/09513590.2020.1846697
15. Paul C, Lagana AS, Maniglio P, Triolo O, Brady DM. Inositol’s and other nutraceuticals’ synergistic actions counteract insulin resistance in polycystic ovarian syndrome and metabolic syndrome: state-of-the-art and future perspectives. Gynecol Endocrinol (2016) 32(6):431–8. doi: 10.3109/09513590.2016.1144741
16. Sacchi S, Marinaro F, Tondelli D, Lui J, Xella S, Marsella T, et al. Modulation of gonadotrophin induced steroidogenic enzymes in granulosa cells by d-chiroinositol. Reprod Biol Endocrinol (2016) 14(1):52. doi: 10.1186/s12958-016-0189-2
17. Nestler JE, Jakubowicz DJ, de Vargas AF, Brik C, Quintero N, Medina F. Insulin stimulates testosterone biosynthesis by human thecal cells from women with polycystic ovary syndrome by activating its own receptor and using inositolglycan mediators as the signal transduction system. J Clin Endocrinol Metab (1998) 83(6):2001–5. doi: 10.1210/jcem.83.6.4886
18. Nestler JE, Jakubowicz DJ, Reamer P, Gunn RD, Allan G. Ovulatory and metabolic effects of D-chiro-inositol in the polycystic ovary syndrome. N Engl J Med (1999) 340(17):1314–20. doi: 10.1056/NEJM199904293401703
19. Cheang KI, Baillargeon JP, Essah PA, Ostlund RE Jr, Apridonize T, Islam L, et al. Insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator correlates with insulin sensitivity in women with polycystic ovary syndrome. Metabolism (2008) 57(10):1390–7. doi: 10.1016/j.metabol.2008.05.008
20. Pizzo A, Lagana AS, Barbaro L. Comparison between effects of myo-inositol and D-chiro-inositol on ovarian function and metabolic factors in women with PCOS. Gynecol Endocrinol (2014) 30(3):205–8. doi: 10.3109/09513590.2013.860120
21. Artini PG, Di Berardino OM, Papini F, Genazzani AD, Simi G, Ruggiero M, et al. Endocrine and clinical effects of myo-inositol administration in polycystic ovary syndrome. A randomized study. Gynecol Endocrinol (2013) 29(4):375–9. doi: 10.3109/09513590.2012.743020
22. Costantino D, Minozzi G, Minozzi E, Guaraldi C. Metabolic and hormonal effects of myo-inositol in women with polycystic ovary syndrome: a double-blind trial. Eur Rev Med Pharmacol Sci (2009) 13(2):105–10.
23. Emekci Ozay O, Ozay AC, Cagliyan E, Okyay RE, Gulekli B. Myo-inositol administration positively effects ovulation induction and intrauterine insemination in patients with polycystic ovary syndrome: a prospective, controlled, randomized trial. Gynecol Endocrinol (2017) 33(7):524–8. doi: 10.1080/09513590.2017.1296127
24. Stocco C. Tissue physiology and pathology of aromatase. Steroids. (2012) 77(1-2):27–35. doi: 10.1016/j.steroids.2011.10.013
25. Erickson GF, Hsueh AJ, Quigley ME, Rebar RW, Yen SS. Functional studies of aromatase activity in human granulosa cells from normal and polycystic ovaries. J Clin Endocrinol Metab (1979) 49(4):514–9. doi: 10.1210/jcem-49-4-514
26. Gambioli R, Forte G, Aragona C, Bevilacqua A, Bizzarri M, Unfer V. The use of D-chiro-Inositol in clinical practice. Eur Rev Med Pharmacol Sci (2021) 25(1):438–46. doi: 10.26355/eurrev_202101_24412
27. Bizzarri M, Cucina A, Dinicola S, Harrath AH, Alwasel SH, Unfer V, et al. Does myo-inositol effect on PCOS follicles involve cytoskeleton regulation? Med Hypotheses (2016) 91:1–5. doi: 10.1016/j.mehy.2016.03.014
28. Unfer V, Carlomagno G, Papaleo E, Vailati S, Candiani M, Baillargeon JP. Hyperinsulinemia Alters Myoinositol to d-chiroinositol Ratio in the Follicular Fluid of Patients With PCOS. Reprod Sci (2014) 21(7):854–8. doi: 10.1177/1933719113518985
29. Heimark D, McAllister J, Larner J. Decreased myo-inositol to chiro-inositol (M/C) ratios and increased M/C epimerase activity in PCOS theca cells demonstrate increased insulin sensitivity compared to controls. Endocr J (2014) 61(2):111–7. doi: 10.1507/endocrj.EJ13-0423
30. Ravanos K, Monastra G, Pavlidou T, Goudakou M, Prapas N. Can high levels of D-chiro-inositol in follicular fluid exert detrimental effects on blastocyst quality? Eur Rev Med Pharmacol Sci (2017) 21(23):5491–8. doi: 10.26355/eurrev_201712_13940
31. Bevilacqua A, Dragotto J, Giuliani A, Bizzarri M. Myo-inositol and D-chiro-inositol (40:1) reverse histological and functional features of polycystic ovary syndrome in a mouse model. J Cell Physiol (2019) 234(6):9387–98. doi: 10.1002/jcp.27623
32. Nordio M, Basciani S, Camajani E. The 40:1 myo-inositol/D-chiro-inositol plasma ratio is able to restore ovulation in PCOS patients: comparison with other ratios. Eur Rev Med Pharmacol Sci (2019) 23(12):5512–21. doi: 10.26355/eurrev_201906_18223
33. Carlomagno G, Unfer V, Roseff S. The D-chiro-inositol paradox in the ovary. Fertil Steril (2011) 95(8):2515–6. doi: 10.1016/j.fertnstert.2011.05.027
34. Nestler JE, Unfer V. Reflections on inositol(s) for PCOS therapy: steps toward success. Gynecol Endocrinol (2015) 31(7):501–5. doi: 10.3109/09513590.2015.1054802
35. Garzon S, Lagana AS, Monastra G. Risk of reduced intestinal absorption of myo-inositol caused by D-chiro-inositol or by glucose transporter inhibitors. Expert Opin Drug Metab Toxicol (2019) 15(9):697–703. doi: 10.1080/17425255.2019.1651839
36. Cammarata PR, Chen HQ, Yang J, Yorio T. Modulation of myo-[3H]inositol uptake by glucose and sorbitol in cultured bovine lens epithelial cells. II. Characterization of high- and low-affinity myo-inositol transport sites. Invest Ophthalmol Vis Sci (1992) 33(13):3572–80.
37. Coady MJ, Wallendorff B, Gagnon DG, Lapointe JY. Identification of a novel Na+/myo-inositol cotransporter. J Biol Chem (2002) 277(38):35219–24. doi: 10.1074/jbc.M204321200
38. Facchinetti F, Giulia D, Neri I. The Ratio of MI to DCI and Its Impact in the Treatment of Polycystic Ovary Syndrome: Experimental and Literature Evidences. Front Gynecol Endocrinol (2016) 3:103–9. doi: 10.1007/978-3-319-23865-4_13
39. Leung KY, Mills K, Burren KA, Copp AJ, Greene ND. Quantitative analysis of myo-inositol in urine, blood and nutritional supplements by high-performance liquid chromatography tandem mass spectrometry. J Chromatogr B Analyt Technol BioMed Life Sci (2011) 879(26):2759–63. doi: 10.1016/j.jchromb.2011.07.043
40. Ostlund RE Jr, McGill JB, Herskowitz I, Kipnis DM, Santiago JV. Sherman WR. D-chiro-inositol metabolism in diabetes mellitus. Proc Natl Acad Sci U.S.A. (1993) 90(21):9988–92. doi: 10.1073/pnas.90.21.9988
41. Kamenov Z, Kolarov G, Gateva A, Carlomagno G, Genazzani AD. Ovulation induction with myo-inositol alone and in combination with clomiphene citrate in polycystic ovarian syndrome patients with insulin resistance. Gynecol Endocrinol (2015) 31(2):131–5. doi: 10.3109/09513590.2014.964640
42. Monastra G, Sambuy Y, Ferruzza S, Ferrari D, Ranaldi G. Alpha-lactalbumin Effect on Myo-inositol Intestinal Absorption: In vivo and In vitro. Curr Drug Deliv (2018) 15(9):1305–11. doi: 10.2174/1567201815666180509102641
43. Montanino Oliva M, Buonomo G, Calcagno M, Unfer V. Effects of myo-inositol plus alpha-lactalbumin in myo-inositol-resistant PCOS women. J Ovarian Res (2018) 11(1):38. doi: 10.1186/s13048-018-0411-2
44. Larner J, Huang LC, Schwartz CF, Oswald AS, Shen TY, Kinter M, et al. Rat liver insulin mediator which stimulates pyruvate dehydrogenase phosphate contains galactosamine and D-chiroinositol. Biochem Biophys Res Commun (1988) 151(3):1416–26. doi: 10.1016/S0006-291X(88)80520-5
45. Bizzarri M, Fuso A, Dinicola S, Cucina A, Bevilacqua A. Pharmacodynamics and pharmacokinetics of inositol(s) in health and disease. Expert Opin Drug Metab Toxicol (2016) 12(10):1181–96. doi: 10.1080/17425255.2016.1206887
46. Larner J. D-chiro-inositol–its functional role in insulin action and its deficit in insulin resistance. Int J Exp Diabetes Res (2002) 3(1):47–60. doi: 10.1080/15604280212528
47. Pak Y, Huang LC, Lilley KJ, Larner J. In vivo conversion of [3H]myoinositol to [3H]chiroinositol in rat tissues. J Biol Chem (1992) 267(24):16904–10. doi: 10.1016/S0021-9258(18)41870-4
48. Asplin I, Galasko G, Larner J. chiro-inositol deficiency and insulin resistance: a comparison of the chiro-inositol- and the myo-inositol-containing insulin mediators isolated from urine, hemodialysate, and muscle of control and type II diabetic subjects. Proc Natl Acad Sci USA (1993) 90(13):5924–8. doi: 10.1073/pnas.90.13.5924
49. Baptiste CG, Battista MC, Trottier A, Baillargeon JP. Insulin and hyperandrogenism in women with polycystic ovary syndrome. J Steroid Biochem Mol Biol (2010) 122(1-3):42–52. doi: 10.1016/j.jsbmb.2009.12.010
50. Larner J, Craig JW. Urinary myo-inositol-to-chiro-inositol ratios and insulin resistance. Diabetes Care (1996) 19(1):76–8. doi: 10.2337/diacare.19.1.76
51. Yilmaz M, Bukan N, Ersoy R, Karakoç A, Yetkin I, Ayvaz G, et al. Glucose intolerance, insulin resistance and cardiovascular risk factors in first degree relatives of women with polycystic ovary syndrome. Hum Reprod (2005) 20:2414–20. doi: 10.1093/humrep/dei070
52. Lagana AS, Garzon S, Unfer V. New clinical targets of d-chiro-inositol: rationale and potential applications. Expert Opin Drug Metab Toxicol (2020) 16(8):703–10. doi: 10.1080/17425255.2020.1785429
53. Aversa A, La Vignera S, Rago R, Gambineri A, Nappi RE, Calogero AE, et al. Fundamental Concepts and Novel Aspects of Polycystic Ovarian Syndrome: Expert Consensus Resolutions. Front Endocrinol (Lausanne) (2020) 11:516. doi: 10.3389/fendo.2020.00516
Keywords: PCOS, myo-inositol, D-chiro inositol, metabolism, ovarian cells
Citation: Monastra G, Vucenik I, Harrath AH, Alwasel SH, Kamenov ZA, Laganà AS, Monti N, Fedeli V and Bizzarri M (2021) PCOS and Inositols: Controversial Results and Necessary Clarifications. Basic Differences Between D-Chiro and Myo-Inositol. Front. Endocrinol. 12:660381. doi: 10.3389/fendo.2021.660381
Received: 01 February 2021; Accepted: 04 March 2021;
Published: 06 April 2021.
Edited by:
Alberto Ferlin, University of Brescia, ItalyReviewed by:
Sandro La Vignera, University of Catania, ItalyAlessandra Gambineri, University of Bologna, Italy
Copyright © 2021 Monastra, Vucenik, Harrath, Alwasel, Kamenov, Laganà, Monti, Fedeli and Bizzarri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariano Bizzarri, bWFyaWFuby5iaXp6YXJyaUB1bmlyb21hMS5pdA==