 Mays Altaraihi1*
Mays Altaraihi1* Thomas van Overeem Hansen1Eric Santoni-Rugiu2
Thomas van Overeem Hansen1Eric Santoni-Rugiu2 Maria Rossing3Åse Krogh Rasmussen4Anne-Marie Gerdes1
Maria Rossing3Åse Krogh Rasmussen4Anne-Marie Gerdes1 Karin Wadt1
Karin Wadt1- 1Department of Clinical Genetics, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 2Department of Pathology, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 3Center for Genomic Medicine, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 4Department of Endocrinology and Metabolism, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
Introduction: DICER1 syndrome encompasses a variety of benign and malignant manifestations including multinodular goitre, which is the most common manifestation among individuals carrying pathogenic DICER1 variants. This is the first study estimating the prevalence of pathogenic DICER1 variants in young individuals with multinodular goitre.
Methods: Danish individuals diagnosed with nodular goitre based on thyroidectomy samples in 2001-2016 with the age limit at time of operation being ≤ 25 years were offered germline DICER1 gene testing.
Results: Six of 46 individuals, 13% (CI [3.3;22.7], p <0.05), diagnosed with nodular goitre on the basis of thyroidectomy samples under the age of 25 years had pathogenic germline variants in DICER1. They were found in different pathoanatomical nodular goitre cohorts i.e. nodular goitre (n=2), colloid nodular goitre (n=3) and hyperplastic nodular goitre (n=1).
Conclusions: We recommend referral of patients thyroidectomised due to goitre aged <21 years and patients thyroidectomised due to goitre aged <25 years with a family history of goitre to genetic counselling. Patients of all ages thyroidectomised due to goitre, who are affected by another DICER1 manifestation should be referred to genetic counselling.
Introduction
DICER1 syndrome is a rare autosomal dominant disorder predisposing individuals to development of both benign and malignant neoplasms. The DICER1 gene encodes a ribonuclease involved in processing pre-microRNA (miRNA) to mature miRNA. Alterations in DICER1 lead to dysregulation of miRNA production, which is associated with different tumour types (1).
The hallmark tumours of the DICER1 syndrome are pleuropulmonary blastoma and Sertoli-Leydig cell tumour, which both are rare tumours. Most known families with pathogenic DICER1 variants have been identified through clinical findings of the hallmark tumours, which can cause ascertainment bias associated with the DICER1 syndrome.
Some of the other DICER1-related tumours include cystic nephroma, anaplastic renal sarcoma, Wilms tumour, differentiated thyroid carcinoma, gynandroblastoma, ciliary body medulloepithelioma, embryonal rhabdomyosarcoma and primary brain tumours such as pineoblastoma and pituitary blastoma.
However, the most common manifestation among pathogenic DICER1 variant carriers is multinodular goitre (MNG) diagnosed in young individuals. The cumulative incidence of thyroidectomy due to MNG is estimated to be 44% in women and 14% in men with DICER1 pathogenic variants by age 30 years in an American cohort (2). To date, no studies have investigated the prevalence of pathogenic variants in DICER1 in young individuals with MNG. Studies have tried to estimate the prevalence of germline DICER1 variants in women with SLCT, observing that it varies significantly from 0 to 88 % (3–9). One study has reported the frequency of germline pathogenic variants in DICER1 in children with pleuropulmonary blastoma (PPB) to be 70 % (10). Moreover, somatic pathogenic DICER1 variants were found in 10% (3 of 30) of papillary thyroid carcinomas belonging to individuals <18 years of age at time of diagnosis (11).
As MNG is one of the most common diseases of the thyroid gland and the most common manifestation associated with the DICER1 syndrome (12, 13), we have studied the prevalence of pathogenic germline DICER1 variants in a Danish cohort of young individuals operated for MNG.
Materials and Methods
Study Enrolment
Data on individuals with SNOMED diagnosis codes nodular goitre (M71602), colloid nodular goitre (M71622) or hyperplastic nodular goitre (M71642) were obtained from the National Pathology Data Bank. The data obtained were restricted to individuals acquiring the diagnosis codes from 2001-2016 nationally in Denmark. Only individuals with a histological diagnosis and prior partial or total thyroidectomy were included. No malignant histology was found. All the included patients were ≤ 25 years at time of thyroidectomy.
During a period of two years (2018 and 2019), letters of information and consent were sent to all meeting the inclusion criteria except individuals who had not reached the age of 18 years; individuals who had immigrated from Denmark; and individuals who registered non-disclosure of name and address (Figure 1). Letters were sent to 187 individuals, albeit only eighty individuals (43 %) responded to the letter. They received oral information about the study, and information about their medical records and family history were collected. Three individuals were excluded due to a pre-existing medical condition; one excluded patient had Graves’ disease, one had a pathogenic variant in the RET gene and one had an unspecified non-goitre thyroid disease. Subsequently, only 46 individuals (25 %) had blood sampling performed as agreed upon.
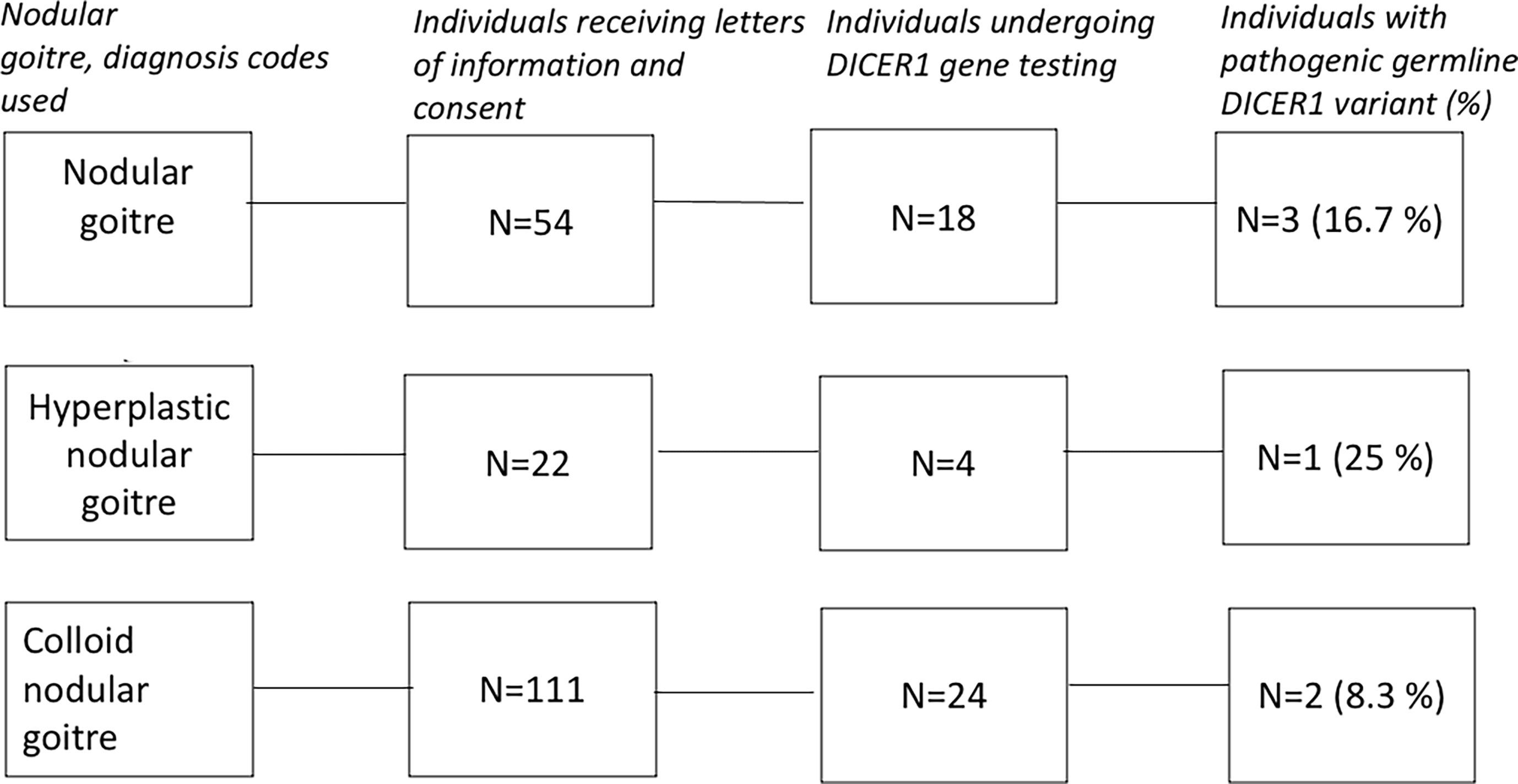
Figure 1 Schematic representation of the method used to obtain results.
DICER1 Gene Testing
Genomic DNA material was extracted from peripheral blood using standard protocols. Analysis of the coding regions and splice junctions (+/- 50 bp) of DICER1 was performed using Next Generation Sequencing (NGS) with Illumina platforms and CNV/MLPA analysis. DICER1 variants are numbered according to accession number NM_177438.2 using the nomenclature guidelines from the Human Genome Variation Society (https://varnomen.hgvs.org/).
The study was conducted according to the declaration of Helsinki and was approved by the Danish Data Protection Agency and Danish Regional Ethical Committee (H-17023400). Written informed consents were obtained from all participants.
Results
Six of 46 individuals, 13%, (CI [3.3;22.7], P <0.05) diagnosed with nodular goitre under the age of 25 years had pathogenic germline variants in DICER1. All of the 40 individuals without pathogenic variants of DICER1 had wild type alleles of the gene. Baseline characteristics of the overall nodular goitre cohort undertaking DICER1 gene testing is shown in Figure 1 and Table 1. The majority of participants undergoing DICER1 gene testing had a family history of goitre or thyroidectomies. In the nodular goitre cohort, three individuals had a pathogenic DICER1 variant (17%); in the colloid nodular goitre cohort, two individuals had pathogenic DICER1 variant (8%); and in the hyperplastic nodular goitre cohort, one individual had a pathogenic DICER1 variant (25%). The mean age at time of operation amongst individuals without pathogenic variants in DICER1 was 19.4 years, whilst the mean age amongst individuals with pathogenic variants in DICER1 was 15.3 years: Four of the six individuals found in the goitre cohorts carrying pathogenic DICER1 variants had their thyroid gland totally or partially removed at < 20 years of age, the remaining two were both 21 years of age at the time of thyroidectomy (Table 2). Furthermore, one third of the MNG individuals with variations in DICER1 had partial thyroidectomies – the rest had undergone total thyroidectomies. The indication for partial or total thyroidectomies was compressive symptoms due to the goitre.
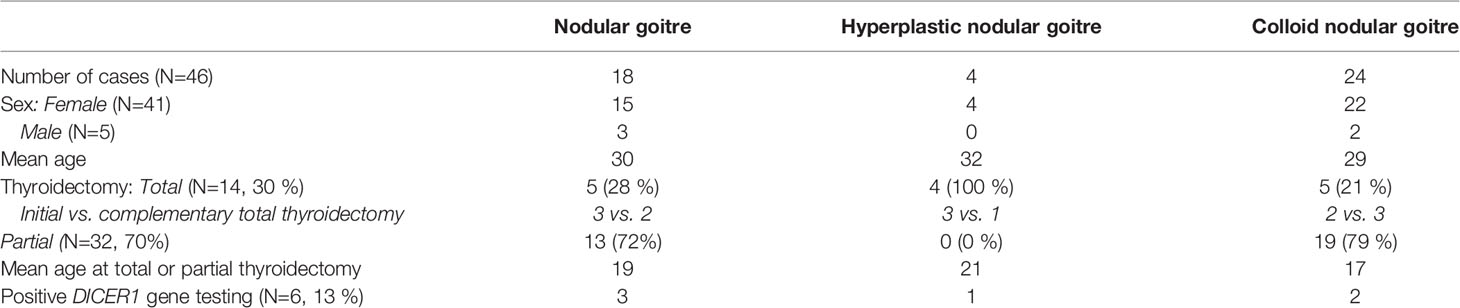
Table 1 Baseline characteristics of the goitre cohort.
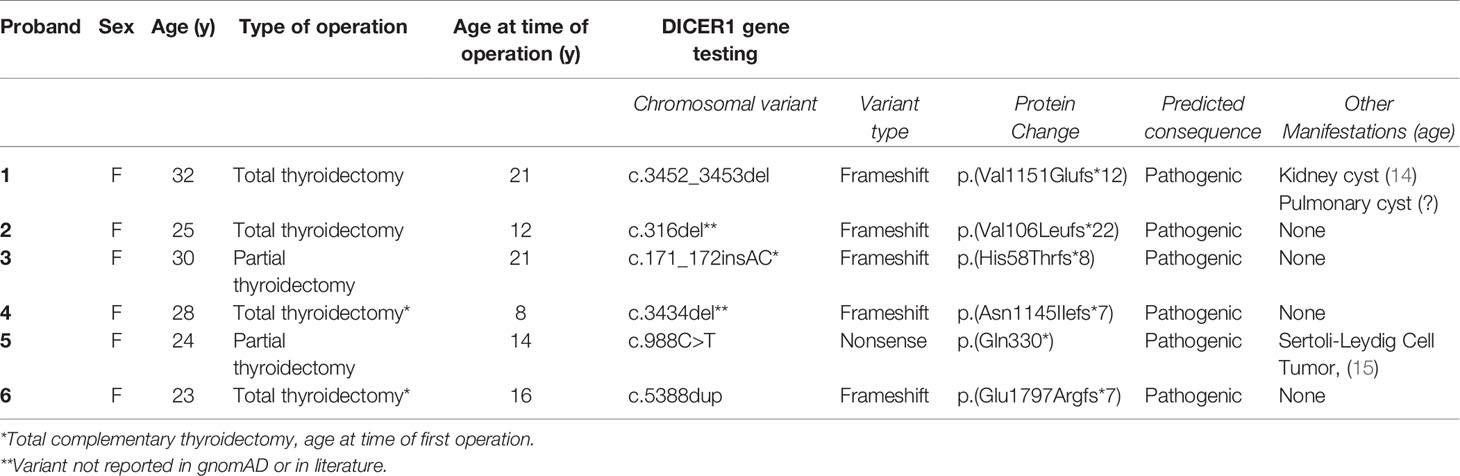
Table 2 Characteristics of DICER1 probands identified in the goitre cohort.
All six identified individuals with pathogenic DICER1 variants in the goitre cohort were females. Only one of the identified individuals with pathogenic DICER1 variants, proband 6, was already known with a germline de novo heterozygous frameshift, c.5388dup, p.(Glu1797Argfs*7) variant in DICER1 (Table 2). The newfound proband 1 and proband 4 had no family history of goitre or other DICER1 syndrome-related manifestations. The rest of the probands had a family history of relevant manifestations.
Three of the six individuals were carriers of pathogenic DICER1 variants not previously reported in gnomAD or in the literature: Proband 2 carried a frameshift variant, c.316del, p.(Val 106Leufs*22). Besides a total thyroidectomy performed at age 12, no other DICER1 syndrome-related manifestations were found at 25 years of age.
Proband 3 had a frameshift variant, c.171_172insAC, p. (His58Thrfs*8) in the DICER1 gene – other than undergoing a partial thyroidectomy at age 21, her medical records were unremarkable at age 30.
Another not previously described frameshift variant was detected in proband 4, c.3434del, p.(Asn11451IIefs*7). The individual was, apart from MNG resulting in total thyroidectomy at age 11, not affected by other DICER1 syndrome-related manifestations at 28 years of age.
Two of the six individuals had manifestations related to the DICER1 syndrome other than MNG: Proband 1, carrying a frameshift variant, c.3452_3453del, p.(Val1151Glufs*12), had a pulmonary cyst and a kidney cyst measuring 11 cm surgically removed at 25 years of age. Proband 5 carried a nonsense variant in DICER1, c.988C>T, p.(Gln330*). She had the thyroid gland partially removed at age 14 and was additionally diagnosed with Sertoli-Leydig cell tumour (SLCT) at age 17 (Table 2). All the six carriers were referred to examinations in accordance with the European surveillance protocol (16) - no new manifestations related to the DICER1 syndrome have been reported.
Discussion
To our knowledge, this is the first study estimating the prevalence of germline DICER1 pathogenic variants among young individuals operated for MNG in an age below 25 years, finding a prevalence of 13%. Although numbers are small and the data needs to be replicated in an independent dataset, the prevalence is surprisingly high. The estimated frequency of loss-of-function DICER1 variants in the general population is suggested to be ~ 1:10,600, which is a substantial higher number compared to the number of identified families with DICER1 syndrome (17). This is in line with data from our study.
Considering the prevalence being 13%, we recommend referring young individuals diagnosed with goitre in need of surgery aged <21 years to genetic counselling for DICER1 gene testing as the mean age at time of thyroidectomy amongst DICER1 patients in this study was 15.3 years, in which the oldest ones were 21 years. Similarly, we recommend genetic counselling to individuals diagnosed with MNG in need of surgery at age <25 years, if they have at least a family history of goitre. Furthermore, referral of individuals diagnosed with MNG in need of surgery, who are affected by another DICER1 manifestation should include all age groups. Parts of the recommendations are additionally supported by one study concluding that early onset MNG or multiple cases of MNG in a family should raise concerns of DICER1 alterations (18). Likewise, the recommendations might also apply to patients with MNG diagnosed with the support of fine needle aspiration or based on imaging (thyroid ultrasound or thyroid scintigraphy). However, as this study has explored MNG diagnosis based on histology, recommendations on DICER1 gene testing in patients with cytology-aided or imaging-based diagnosis of MNG without the need of surgery should rely on further studies.
The six carriers of DICER1 variants in the goitre cohort were discovered in different nodular goitre groups; nodular goitre, colloid nodular goitre, and hyperplastic nodular goitre. Different pathologists studied the different samples, which questions the consistency of the terminology use. However, this is in conjunction with the previously observed difficulty in histologically differentiation between papillary thyroid cancer and follicular thyroid cancer in DICER1 patients (15). Studies need to be conducted regarding the morphological features of nodular goitre in individuals harbouring DICER1 variants, and whether they - in case distinguishing hallmarks can be identified - may be suggestive of DICER1 syndrome.
Somatic mutational analyses of the nodular goitre tissue samples belonging to the six patients with DICER1 alterations were not performed. Khan et al. have reported that 84 % of thyroid nodules from 13 patients carrying germline DICER1 variations with MNG had somatic mutations in DICER1 hotspot amino acids (2). It could have been of great value if such analyses had been executed in this study, strengthening the published data regarding the unique two-hit-mechanism and the DICER1 syndrome.
The research recruitment rate has not been high as letters of information have been sent to 187 individuals, though only 80 individuals accepted to participate and in only 46 individuals DICER1 gene testing was performed. Almost all the participants who underwent genetic testing had a family history of goitre: This may have biased the study to a higher prevalence, assuming individuals without a family history were not interested in a study of genetics. Furthermore, most of the individuals contacted in this study were under the age of 30 years, which might also have contributed to the low participation rate, as the relevance of inherited diseases increases after having children.
All the identified DICER1 patients were females, which is to be expected as 89 % of the included individuals in the study were females. Overall, it is a well-known fact that goitre is more predominant in women (19). This is also consistent with a study based on an American cohort estimating that the incidence of thyroidectomy due to MNG is higher in women with DICER1 variations compared to men with DICER1 variations (2).
Total thyroidectomies were performed in four of six DICER1 patients found in the goitre cohort. Two of the four patients had initially undergone partial thyroidectomy, but, residual thyroid tissue was subsequently removed, as MNG had developed. This is in accordance with previous studies reporting that DICER1 patients undergoing partial thyroidectomy often need additional thyroid surgery (2). Furthermore, a study by Chernock et al. (20) demonstrated that poorly differentiated thyroid carcinomas in children and adolescents are strongly associated with DICER1 mutations and are highly aggressive, although in most cases differentiated thyroid carcinomas in DICER1 patients behave in an indolent manner (20). A genome-first approach study of the DICER1 observed that individuals harbouring putative LOF variants of DICER1 had a significantly stronger association with thyroid cancer and thyroidectomy compared to matched controls without DICER1 variations (21). These findings suggest considerations of early total thyroidectomy in a DICER1 patient - when goitre is detected - is relevant. However, it is also important to note that the risk of developing thyroid carcinomas secondarily to thyroid nodules has been suggested to be small (2, 22), and the cumulative incidence of thyroid cancer in carriers of DICER1 variants remains unknown (16, 20). Studies need to be done on whether to recommend total thyroidectomy in carriers of pathogenic germline DICER1 variants, when the diagnosis of a goitre is made, especially as the possible complications of the procedure can be postoperative hypocalcemia and recurrent laryngeal nerve paralysis (23).
Familial clustering of goitre is not uncommon in areas known to be without iodine deficiency, predominately showing an autosomal dominant inheritance pattern. Variations in the genes TG, TPO, NIS, PDS, PAX8, NKX2-1, NKX2-5, IYD, FOXE1, JAG1, DOUX2, DOUXA2 and TSH-R are associated with congenital hypothyroidism and/or nodular goitre (14, 24, 25). Pathogenic variants of the genes RGS12, GRPEL1, CLIC6 and WFS1 are suggested to be associated with an increased risk of nodular goitre, typically developing during the first decade of life – no other manifestations have been associated with the genes expect WFS1 (Wolfram syndrome), though the literature is very sparse (26, 27). A few cases of nodular goitre due to DICER1 alterations have been reported in the first decade of life in addition to proband 4 in this study (28), though the vast majority of cases are diagnosed in the second and third decades. Case reports show germline pathogenic variations in KEAP1 and NKX2-1 are also linked to nodular goitre diagnosed during the second decade of life (29, 30). Figure 2 shows a flowchart of age at nodular goitre diagnosis along with the putative causative genes. As this study has only addressed DICER1, we cannot recommend testing the other candidate genes in young individuals presenting with nodular goitre, especially as some of genes are not well-studied. Figure 2 only gives an overview of the genes presented in the literature connected to familial nodular goitre.
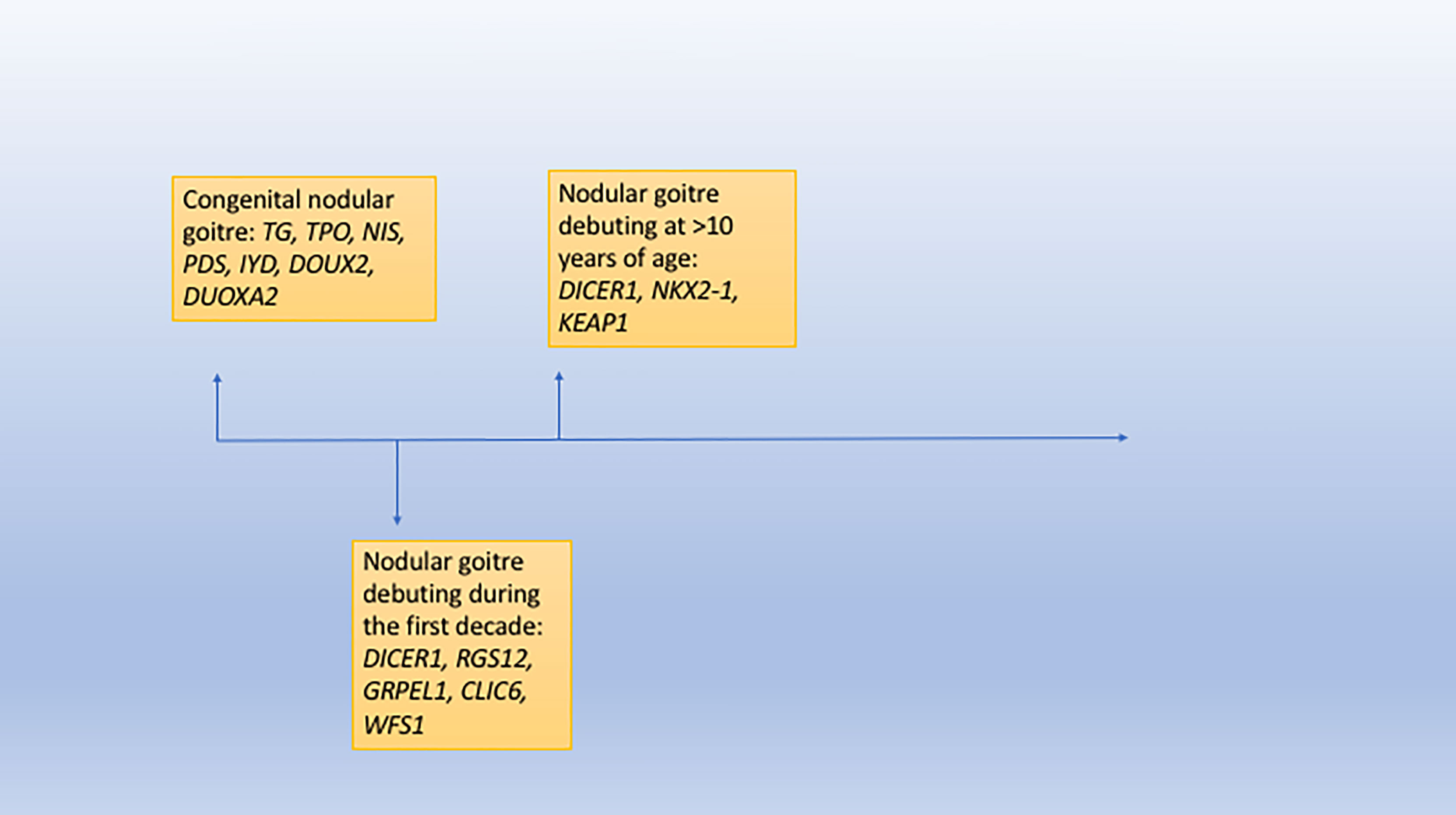
Figure 2 A flowchart showing age at nodular goitre diagnosis and the putative causative genes.
In conclusion, considering the estimated prevalence being 13%, we recommend referral of individuals with MNG in need of surgery aged <21 years to genetic counselling for DICER1 gene testing. Likewise, we recommend referral of individuals with MNG in need of surgery aged <25 years with a family history of goitre to genetic counselling for DICER1 gene testing. Individuals of all ages thyroidectomised due to goitre, who are also affected by another DICER1 syndrome-related manifestation should be referred to genetic counselling.
Data Availability Statement
All datasets presented in this study are included in the article.
Ethics Statement
The study was conducted according to the declaration of Helsinki and was approved by the Danish Data Protection Agency and Danish Regional Ethical Committee (H-17023400). Written informed consents were obtained from all participants. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
MA contributed to designing the research study, acquiring data, analysing data, and writing the original manuscript. TH contributed to acquiring data, analysing data, and revising the manuscript. ES-R contributed to analysing data and revising the manuscript. MR contributed to acquiring data. ÅR contributed to analysing data and revising the manuscript. A-MG contributed to designing the research study, acquiring data, and revising the manuscript. KW contributed to designing the research study, acquiring data, analysing data, and writing the original manuscript. All authors contributed to the article and approved the submitted version.
Funding
The Danish Cancer Society awarded author MA a research scholarship and author KW a research grant.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer KT declared a past collaboration with one of the authors KW to the handling editor.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all the included participants in this study and their families.
References
1. Kian R, Moradi S, Ghorbian S. Role of Components of MicroRNA Machinery in Carcinogenesis. Exp Oncol (2018) 40:2–9. doi: 10.31768/2312-8852.2018.40(1):2-9
2. Khan NE, Bauer AJ, Schultz KAP, Doros L, Decastro RM, Ling A, et al. Quantification of Thyroid Cancer and Multinodular Goiter Risk in the DICER1 Syndrome: A Family-Based Cohort Study. J Clin Endocrinol Metab (2017) 102(5):1614–22. doi: 10.1210/jc.2016-2954
3. Heravi-Moussavi A, Anglesio MS, Cheng S-WG, Senz J, Yang W, Prentice L, et al. Recurrent Somatic DICER1 Mutations in Nonepithelial Ovarian Cancers. N Engl J Med (2012) 366(3):234–42. doi: 10.1056/NEJMoa1102903
4. Witkowski L, Mattina J, Schönberger S, Murray MJ, Huntsman DG, Reis-Filho JS, et al. DICER1 Hotspot Mutations in Non-Epithelial Gonadal Tumours. Br J Cancer (2013) 109(10):2744–50. doi: 10.1038/bjc.2013.637
5. Kato N, Kusumi T, Kamataki A, Tsunoda R, Fukase M, Kurose A. DICER1 Hotspot Mutations in Ovarian Sertoli-Leydig Cell Tumors: A Potential Association With Androgenic Effects. Hum Pathol (2017) 59:41–7. doi: 10.1016/j.humpath.2016.09.005
6. Goulvent T, Ray-Coquard I, Borel S, Haddad V, Devouassoux-Shisheboran M, Vacher-Lavenu MC, et al. DICER1 and FOXL2 Mutations in Ovarian Sex Cord-Stromal Tumours: A GINECO Group Study. Histopathology (2016) 68(2):279–85. doi: 10.1111/his.12747
7. Conlon N, Schultheis AM, Piscuoglio S, Silva A, Guerra E, Tornos C, et al. A Survey of DICER1 Hotspot Mutations in Ovarian and Testicular Sex Cord-Stromal Tumors. Modern Pathol (2015) 28(12):1603–12. doi: 10.1038/modpathol.2015.115
8. Schultz KAP, Pacheco MC, Yang J, Williams GM, Messinger Y, Hill DA, et al. Ovarian Sex Cord-Stromal Tumors, Pleuropulmonary Blastoma and DICER1 Mutations: A Report From the International Pleuropulmonary Blastoma Registry. Gynecol Oncol (2011) 122(2):246–50. doi: 10.1016/j.ygyno.2011.03.024
9. de Kock L, Terzic T, McCluggage WG, Stewart CJR, Shaw P, Foulkes WD, et al. DICER1 Mutations Are Consistently Present in Moderately and Poorly Differentiated Sertoli-Leydig Cell Tumors. Am J Surg Pathol (2017) 41(9):1178–87. doi: 10.1097/PAS.0000000000000895
10. Hill DA, Brenneman M, Field A, Yang J, Williams G, Doros L, et al. Temporal Order of RNase IIIb and Loss-of-Function Mutations During Development Determines Phenotype in Pleuropulmonary Blastoma / DICER1 Syndrome: A Unique Variant of the Two-Hit Tumor Suppression Model. F1000Research (2018) 4:214. doi: 10.12688/f1000research.6746.2
11. Wasserman JD, Sabbaghian N, Fahiminiya S, Chami R, Mete O, Acker M, et al. DICER1 Mutations Are Frequent in Adolescent-Onset Papillary Thyroid Carcinoma. J Clin Endocrinol Metab (2018) 103(5):2009–15. doi: 10.1210/jc.2017-02698
12. Feingold KR, Anawalt B, Boyce A, Chrousos G, Dungan K, Grossman A, et al. Endotext. Feingold KR, Anawalt B, Boyce A, Chrousos G, Dungan K, Grossman A, et al, editors. South Dartmouth (MA): Endotext. MDText.com, Inc (2000). Available at: http://www.ncbi.nlm.nih.gov/pubmed/25905160.
13. Rio Frio T, Bahubeshi A, Kanellopoulou C, Hamel N, Niedziela M, Sabbaghian N, et al. DICER1 Mutations in Familial Multinodular Goiter With and Without Ovarian Sertoli-Leydig Cell Tumors. JAMA - J Am Med Assoc (2011) 305(1):68–77. doi: 10.1001/jama.2010.1910
14. Krohn K, Führer D, Bayer Y, Eszlinger M, Brauer V, Neumann S, et al. Molecular Pathogenesis of Euthyroid and Toxic Multinodular Goiter. Endocr Rev (2005) 26(4):504–24. doi: 10.1210/er.2004-0005
15. Gullo I, Batista R, Rodrigues-Pereira P, Soares P, Barroca H, do Bom-Sucesso M, et al. Multinodular Goiter Progression Toward Malignancy in a Case of DICER1 Syndrome. Am J Clin Pathol (2018) 149(5):379–86. doi: 10.1093/ajcp/aqy004
16. Bakhuizen JJ, Hanson H, Tuin Kvd, Lalloo F, Tischkowitz M, Wadt K, et al. Surveillance Recommendations for DICER1 Pathogenic Variant Carriers: A Report From the SIOPE Host Genome Working Group and CanGene-CanVar Clinical Guideline Working Group. Familial Cancer (2021) 1:1–12. doi: 10.1007/s10689-021-00264-y
17. Kim J, Field A, Schultz KAP, Hill DA, Stewart DR. The Prevalence of DICER1 Pathogenic Variation in Population Databases. Int J Cancer (2017) 141(10):2030–6. doi: 10.1002/ijc.30907
18. Oliver-Petit I, Bertozzi AI, Grunenwald S, Gambart M, Pigeon-Kerchiche P, Sadoul JL, et al. Multinodular Goitre Is a Gateway for Molecular Testing of DICER1 Syndrome. Clin Endocrinol (2019) 91(5):669–75. doi: 10.1111/cen.14074
19. Knudsen N, Laurberg P, Perrild H, Bülow I, Ovesen L, Jørgensen T. Risk Factors for Goiter and Thyroid Nodules. Thyroid (2002) 12(10):879–88. doi: 10.1089/105072502761016502
20. Chernock RD, Rivera B, Borrelli N, Hill DA, Fahiminiya S, Shah T, et al. Poorly Differentiated Thyroid Carcinoma of Childhood and Adolescence: A Distinct Entity Characterized by DICER1 Mutations. Modern Pathol (2020) 33(7):1264–74. doi: 10.1038/s41379-020-0458-7
21. Mirshahi UL, Kim J, Best AF, Chen ZE, Hu Y, Haley JS, et al. A Genome-First Approach to Characterize DICER1 Pathogenic Variant Prevalence, Penetrance, and Phenotype. JAMA Netw Open (2021) 4(2):e210112. doi: 10.1001/jamanetworkopen.2021.0112
22. van der Tuin K, de Kock L, Kamping EJ, Hannema SE, Pouwels M-JM, Niedziela M, et al. Clinical and Molecular Characteristics May Alter Treatment Strategies of Thyroid Malignancies in DICER1 Syndrome. J Clin Endocrinol Metab (2019) 104(2):277–84. doi: 10.1210/jc.2018-00774
23. Bhattacharyya N, Fried MP. Assessment of the Morbidity and Complications of Total Thyroidectomy. Arch Otolaryngol–Head Neck Surg (2002) 128(4):389–92. doi: 10.1001/archotol.128.4.389
24. Santos-Silva R, Rosário M, Grangeia A, Costa C, Castro-Correia C, Alonso I, et al. Genetic Analyses in a Cohort of Portuguese Pediatric Patients With Congenital Hypothyroidism. J Pediatr Endocrinol Metab (2019) 32(11):1265–73. doi: 10.1515/jpem-2019-0047/html
25. Denny JC, Crawford DC, Ritchie MD, Bielinski SJ, Basford MA, Bradford Y, et al. Variants Near FOXE1 Are Associated With Hypothyroidism and Other Thyroid Conditions: Using Electronic Medical Records for Genome- and Phenome-Wide Studies. Am J Hum Genet (2011) 89(4):529–42. doi: 10.1016/j.ajhg.2011.09.008
26. Yan J, Takahashi T, Ohura T, Adachi H, Takahashi I, Ogawa E, et al. Combined Linkage Analysis and Exome Sequencing Identifies Novel Genes for Familial Goiter. J Hum Genet (2013) 58(6):366–77. doi: 10.1038/jhg.2013.20
27. Hofmann S, Philbrook C, Gerbitz K-D, Bauer MF. Wolfram Syndrome: Structural and Functional Analyses of Mutant and Wild-Type Wolframin, the WFS1 Gene Product. Hum Mol Genet (2003) 12(16):2003–12. doi: 10.1093/hmg/ddg214
28. de Kock L, Sabbaghian N, Soglio DBD, Guillerman RP, Park BK, Chami R, et al. Exploring the Association Between DICER1 Mutations and Differentiated Thyroid Carcinoma. J Clin Endocrinol Metab (2014) 99(6):E1072–7. doi: 10.1210/jc.2013-4206
29. Teshiba R, Tajiri T, Sumitomo K, Masumoto K, Taguchi T, Yamamoto K. Identification of a KEAP1 Germline Mutation in a Family With Multinodular Goitre. PloS One (2013) 8(5):e65141. doi: 10.1371/journal.pone.0065141
Keywords: goitre, thyroidectomy, hereditary cancer, DICER1 syndrome, DICER1 mutation, goiter
Citation: Altaraihi M, Hansen TvO, Santoni-Rugiu E, Rossing M, Rasmussen ÅK, Gerdes A-M and Wadt K (2021) Prevalence of Pathogenic Germline DICER1 Variants in Young Individuals Thyroidectomised Due to Goitre – A National Danish Cohort. Front. Endocrinol. 12:727970. doi: 10.3389/fendo.2021.727970
Received: 20 June 2021; Accepted: 26 July 2021;
Published: 06 September 2021.
Edited by:
Leonidas H. Duntas, National University of Athens, GreeceReviewed by:
Karin Van Der Tuin, Leiden University Medical Center, NetherlandsYevgeniya Kushchayeva, University of South Florida, United States
Copyright © 2021 Altaraihi, Hansen, Santoni-Rugiu, Rossing, Rasmussen, Gerdes and Wadt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mays Altaraihi, bWF5cy5hbHRhcmFpaGlAcmVnaW9uaC5kaw==