 Rongrong Zhou1†
Rongrong Zhou1† Yashan Cui2†
Yashan Cui2† Yuehong Zhang1
Yuehong Zhang1 Jin De1Xuedong An1
Jin De1Xuedong An1 Yingying Duan3
Yingying Duan3 Yuqing Zhang1
Yuqing Zhang1 Xiaomin Kang2
Xiaomin Kang2 Fengmei Lian1*
Fengmei Lian1*- 1Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, China
- 2Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, China
- 3Beijing University of Chinese Medicine, Beijing, China
Objective: This study aimed at examining the long-term effects of non-pharmacological interventions on reducing the diabetes incidence among patients with prediabetes and chronic complications events among patients with hyperglycemia (pre-diabetes and diabetes) by performing a systematic review and meta-analysis of randomized controlled trials (RCTs).
Methods: PubMed, MEDLINE, EMBASE, the Cochrane Library, and the Web of Science Core Collection were searched for studies published between January 1990 and November 2021, looking for RCTs to evaluate the effects of non-pharmacological interventions on preventing the incidence of diabetes and chronic complications in comparison with medical therapy, placebo, or usual diabetes care. Two independent reviews extracted relevant data and quality assessment. Any discrepancies were resolved by a third reviewer.
Results: In total, 20 articles involved 16 RCTs (follow-up ranged from 2 to 30 years) were included. Pooled analysis of intervention studies demonstrated clearly that non-pharmacological interventions have a significant effect on reducing the diabetes events in patients with prediabetes (RR 0.62; 95% CI 0.54, 0.71). Pooled analysis of extended follow-up studies showed that non-pharmacological interventions could effectively reduce the diabetes incidence in patients with prediabetes (RR 0.78; 95% CI 0.63, 0.96). Meta-regression and subgroup analysis indicates that the diabetes incidence of the long-term group (duration > 3 years) was clearly reduced by 0.05% compared with the relatively short-term group (duration ≤ 3 years). The incidence of microvascular complications in patients with hyperglycemia was effectively lowered by non-pharmacological interventions (RR 0.60; 95% CI 0.43, 0.83).
Conclusion: Non-pharmacological interventions have a long-term effect on reducing the diabetes incidence among prediabetic patients and effectively preventing microvascular complications on hyperglycemia.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/.
Introduction
The condition of hyperglycemia is one of the most common chronic metabolic disorders, including prediabetes and diabetes. Prediabetic state is a high-risk group of diabetes and a potential risk factor for diabetes and cardiovascular disease, and impaired glucose tolerance (IGT) is more common than impaired fasting glucose (IFG) (1). According to the American Diabetes Association (ADA) expert group, up to 70% of patients with prediabetes will eventually develop diabetes (2). Without effective intervention, it will be more likely to worsen and develop into diabetes mellitus with macro- and microvascular conditions (3, 4). Diabetes complications, particularly macro- and microvascular diseases, are the leading cause of reduction in the quality of life of patients and increase in diabetic mortality. Previously large-scale meta-analyses have indicated that prediabetes is associated with an increased risk of cardiovascular diseases (5–8). Therefore, prevention of diabetes and its severe complications is urgently needed.
Currently, a growing number of clinics and patients pay more attention to non-pharmacological strategies due to the hypoglycemic agents having a limited role in the progression of diabetes and its complications (9). Different non-pharmacological strategies have been reported including lifestyle change, dietary modification, physical activity, and exercise with different intensity, with favorable and unfavorable records on diabetes and its complication prevention and development (10–12). Several large RCTs with a long-term follow-up such as Diabetes Prevention Program (DPP), the Finnish Diabetes Prevention Study, and Da Qing Diabetes Prevention have been reported, stating that adopting a healthy lifestyle would obtain long-term effects on preventing diabetes and its complications (13–15). Moreover, many recent systematic reviews have emphasized the important role in glycemic control and diabetes incidence (16–18). However, these systematic reviews only evaluated the effects on diabetes events among intervention studies, without assessing the effects of extended follow-up studies of intervention completed. In addition, few systematic reviews have reported the important role of non-pharmacological strategies in microvascular complications.
Therefore, it might be beneficial to conduct a systematic review and meta-analysis to whether comprehensive non-pharmacological interventions would be long-term effectiveness for preventing the diabetes and diabetes-related complications compared to other proposed treatments. The objective of this study, obtained by a comprehensive systematic review and meta-analysis of randomized controlled trials (RCTs), was to evaluate the long-term effects of non-pharmacological interventions on reducing the diabetes incidence in prediabetic patients and microvascular complications in patients with pre-diabetes and diabetes.
Materials and Methods
This systematic review and meta-analysis was performed according to the Cochrane Handbook for Systematic Reviews of Interventions (https://gdt.gradepro.org/app/handbook/handbook.html). Data were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Guidelines (19). The PRISMA checklist of this study is provided in Supplementary Table S1. The study was registered in the International prospective register of systematic reviews (CRD42021240826).
Data Sources and Search Strategy
The five databases including PubMed, MEDLINE, EMBASE, the Cochrane Library, and the Web of Science Core Collection were searched for eligible trials using the keywords “diabetes” or “hyperglycemia” or “Impaired glucose tolerance”; “Lifestyle intervention” or “physical activity” or “exercise”; “Macrovascular complications” or “Microvascular complications” or “diabetic nephropathy” or “Diabetic retinopathy” or “Diabetic peripheral neuropathy” or “Diabetic foot”; “diabetes incidence”. The initial search was performed in March 2021, and an updated search of five databases was performed in November 2021 using the same search terms. The search strategy for this study is provided in Supplementary Table S2.
Study Selection
To be included, studies had to be RCTs, which made direct comparisons of non-pharmacological interventions with medical therapy, placebo, usual care, or standard care; included RCTs had at least a 2-year duration of intervention; patients should be of any age with hyperglycemia (i.e., type 1 diabetes mellitus, type 2 diabetes mellitus, prediabetes, impaired glucose tolerance, impaired fasting blood glucose) and without chronic complications of diabetes; included RCTs reported at least one of the main outcomes of interest (i.e., diabetes incidence, cardiovascular complications, microvascular complications); and for the articles in the same study, the article with the longest follow-up duration was included. We excluded studies where both the intervention group and the control group were non-pharmacological interventions, non-RCTs, and publications without original data or with incomplete data. A second author (YC) confirmed that all articles that met the inclusion and exclusion criteria were included in the meta-analysis.
Data Extraction
Two independent investigators (RZ and (YC) used a standardized form to extract data from RCTs that met the inclusion/exclusion criteria, and any discrepancies were resolved by a third author (FL). The following relevant data from each article were extracted, including authors and year of publication; country; study design; study intervention and follow-up duration; patients’ data including type of hyperglycemia; intervention measures of treatment group and control group; diagnostic criteria of outcomes; and outcomes of diabetes incidence and chronic complications. When the outcomes were reported as the percentage of incidence, a conversion in number of diabetes and chronic complications has been made in order to conduct an analysis.
Data Synthesis and Analysis
The primary outcomes of this meta-analysis were the diabetes incidence among prediabetic patients and microvascular events in patients with hyperglycemia. The meta-analysis was carried out using Review Manager 5.4 (The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark).
Meta-analysis was performed using a random-effect model because of possible clinical heterogeneity. Data were pooled into relative risks (RRs) for dichotomous outcomes and RCTs with 95% CI. Heterogeneity was assessed using the I2 statistics, where I2<30% was considered as low heterogeneity, I2 values of 30–70 were considered as moderate heterogeneity, and I2>70% was considered as high heterogeneity.
Sensitivity analyses for the study quality and certain study characteristics (i.e., intervention duration, follow-up duration, and type of treatment measures) were performed through removing each individual trial. After recalculating pooled-effect estimates and heterogeneity, changing the significance of the effect or altering the effect size by 10% or more was considered influential. The meta-regression and subgroup analysis was used to examine the effect of follow-up duration on heterogeneity between the studies. We assessed publication bias by visual inspection of funnel plots for any outcomes>10 articles.
Quality Assessment
The Cochrane risk-of-bias tool was used to assess the RCT risk of bias. We assessed risk of bias in random sequence generation and allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. A sensitivity analysis was conducted to exclude the articles with relevant weaknesses in trial design or execution. The overall quality of the evidence was also assessed using Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group guidelines (20). The quality of each RCT was assessed blinding by two reviews (RZ and (YC), and disagreements were resolved by a third author (FL).
Results
Literature Search
The initial search assessed 4,495 publications. After the removal of duplicates, a total of 4,000 studies were selected and 3,936 publications were excluded by screening the titles and abstracts. Of the remaining 64 publications, 44 were excluded (Supplementary Table S3) because of study duration less than 2 years (7 publications), comparison of 2 treatments of non-pharmacological interventions (4 publications), unsuitable endpoints (11 publications), non-randomized study (9 publications), without original data (2 publication), unsuitable participants (5 publications), and articles being from the same trial and without the outcome of interest (6 publications). Finally, 20 suitable publications were included in the quantitative synthesis meta-analysis (Figure 1).
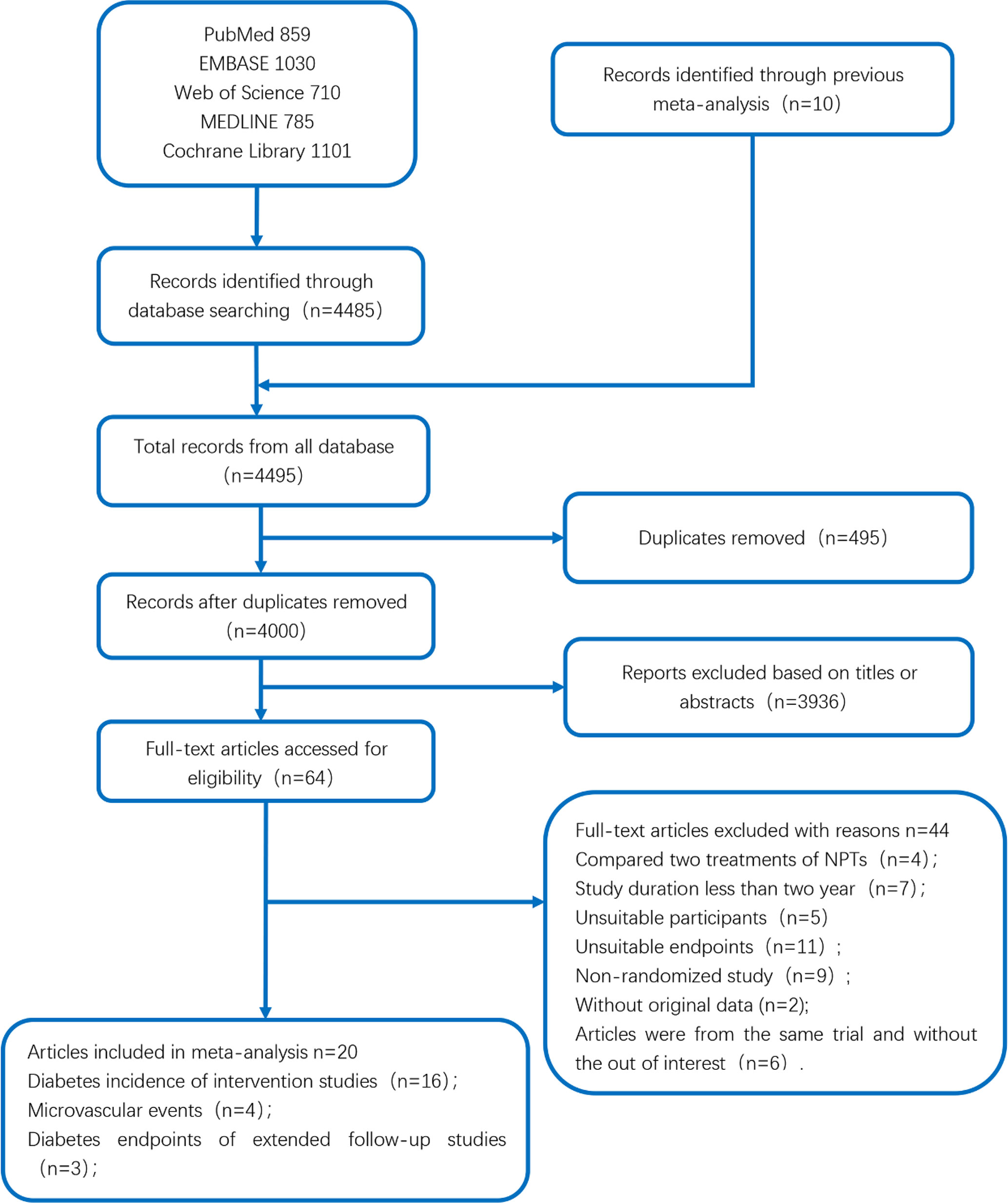
Figure 1 The flow diagram of search and selection process used for studies included in the meta-analysis.
Study Characteristics
The main characteristics of these eligible articles are shown in Table 1. We identified 20 articles (14, 21, 23–30, 32–38) and 16 RCTs used for the main analysis. The sample size ranged from 74 to 2,161. The length of total duration across all trials ranged from 2 to 20 years. The length of intervention ranged from 2 to 15 years, and the length of the extended follow-up ranged from 0 to 14 years. The 15 articles (21, 23, 25, 26, 28, 29, 32–39) reported the outcome of diabetes events among intervention studies, and the 3 articles (22, 24, 25) reported the outcome of diabetes events among extended follow-up studies of intervention completed. The 4 articles (14, 22, 27, 30) reported the outcome of microvascular complications. In these four articles, one article (30) reported the study conducted in patients with diabetes, the rest of which were conducted in prediabetic patients. The two articles (21, 22) reported on the Da Qing Diabetes Prevention Study, two (23, 24) on the Indian Prevention Study, and two (26, 27) on the American Diabetes Prevention Program. The primary outcome was change in the number of diabetes events in 15 articles and 3 extended follow-up studies, and microvascular complications in 4 articles.
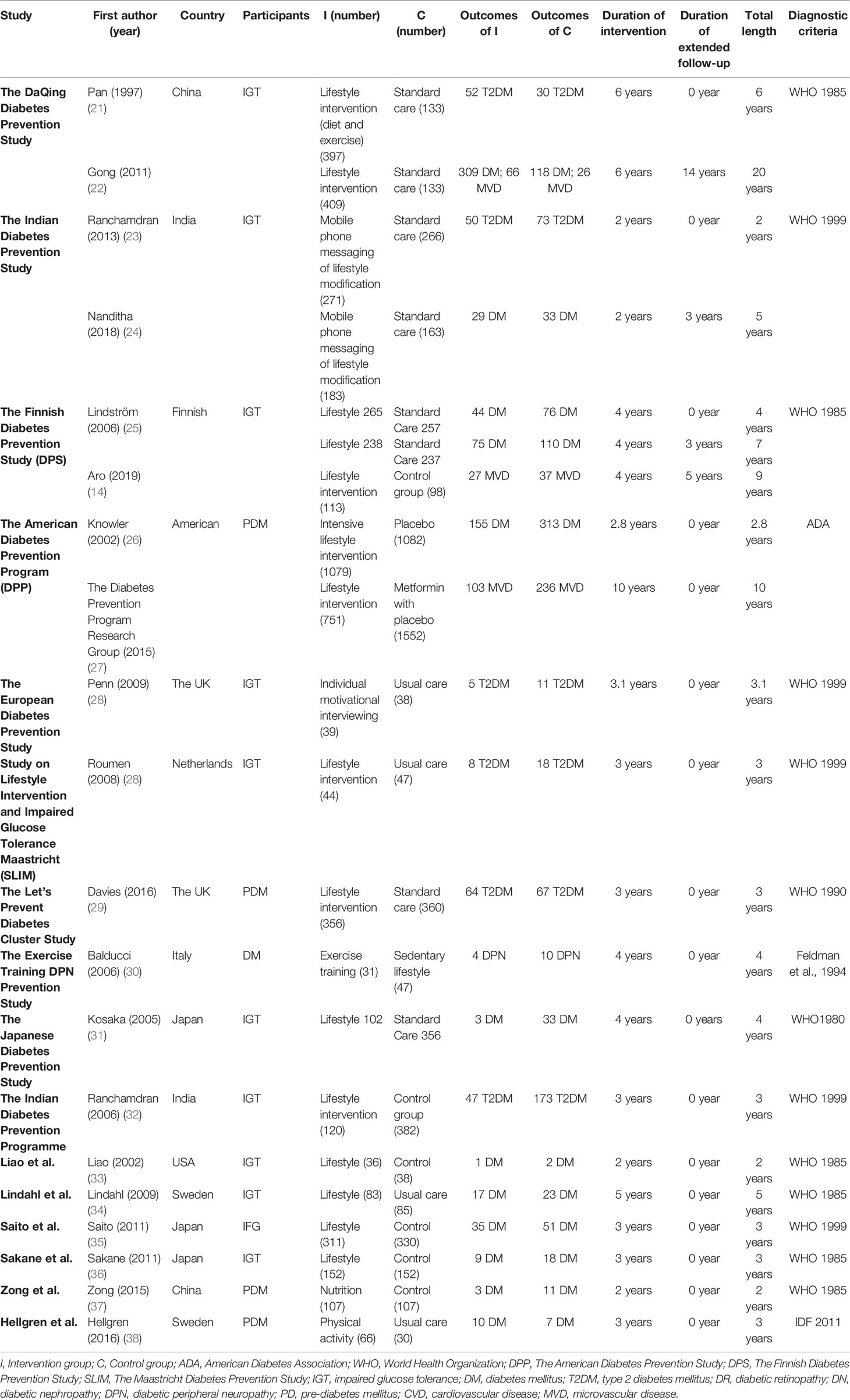
Table 1 The main characteristics of eligible articles included in the meta-analysis.
Long-Term Effects on the Prevention of Diabetes in Intervention Studies
This analysis selected the results of the study that reported the longest follow-up time of diabetes events in terms of the same RCT. In overall analysis of 15 studies, as Figure 2 shows, the non-pharmacological interventions led to a diabetes incidence decrease significantly greater than those of comparator groups (0.62; 95% CI 0.54 to 0.71, p < 0.00001), with low heterogeneity between studies (I2 = 29%, p = 0.14).
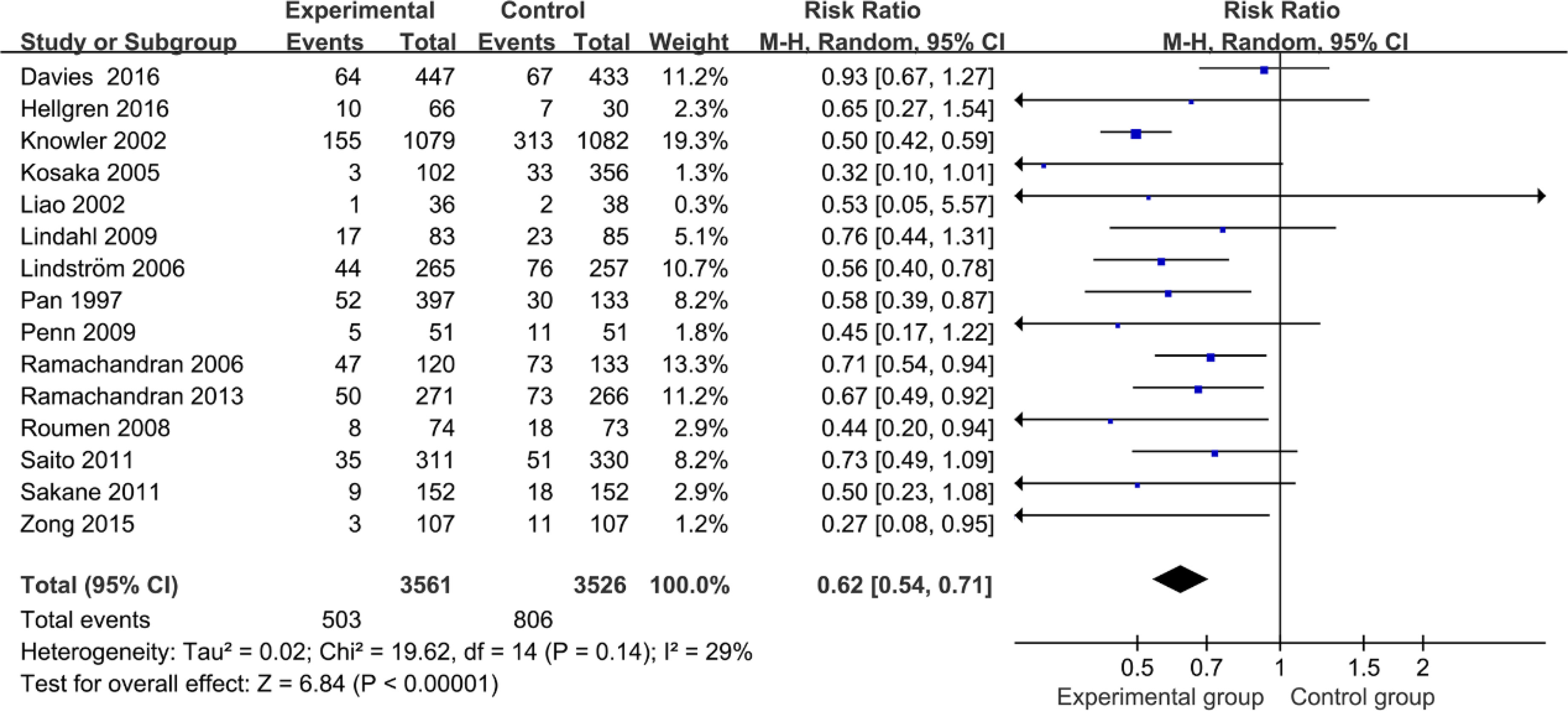
Figure 2 Forest plot of diabetes incidence in intervention studies.
Effects on Microvascular Complications
Figure 3 shows the long-term effect on lowering microvascular events among patients with hyperglycemia. Compared with usual care and medical treatment, those with non-pharmacological interventions among hyperglycemic individuals had a lower incidence of microvascular complications (0.60; 95% CI 0.43 to 0.83, p = 0.002); heterogeneity across articles was moderate with an I2 of 60% (p = 0.06). In sensitivity analysis, the heterogeneity of combined estimates did mark a change with the exclusion of Gong et al. or the DPP group (Table 2), indicating that the source of heterogeneity may be due to the great variation in the duration of follow-up (follow-up duration of Gong et al. was 20 years, and that of the DPP group was 15 years).
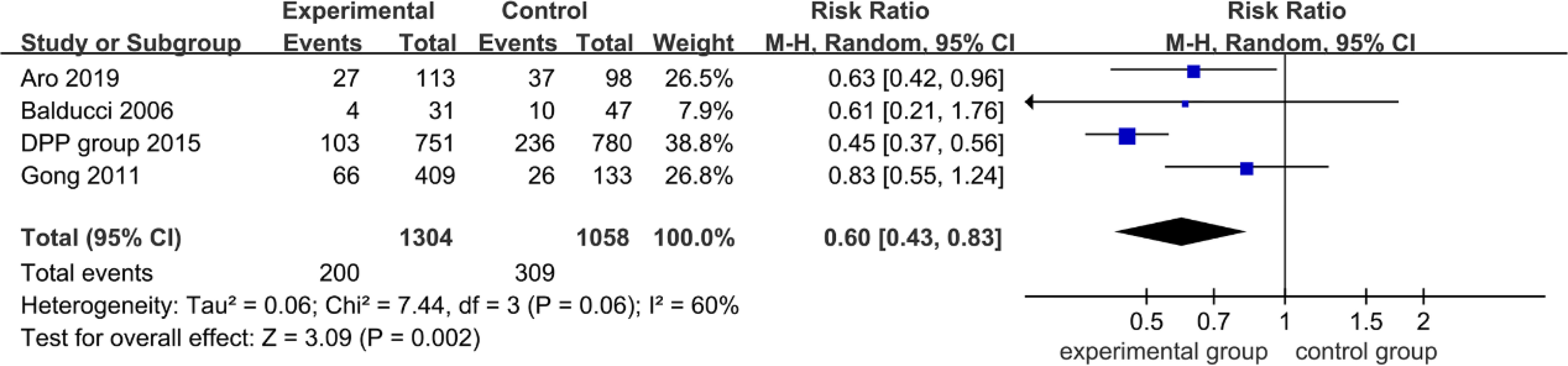
Figure 3 Forest plot of microvascular events.

Table 2 The sensitivity analysis outcomes of microvascular events.
Long-Term Effects on the Prevention of Diabetes in Extended Follow-Up Studies
The three articles (Gong et al.; Nanditha et al.; Lindström et al.) were reported with diabetes outcomes of extended follow-up of intervention completed. As Figure 4 shows, the overall diabetes incidence was clearly reduction (0.78; 95% CI 0.63 to 0.96, p = 0.07), with evidence of substantial heterogeneity (I2 = 62%, p = 0.0). It was indicated that the past non-pharmacological interventions still had a long-term legacy effect to lower diabetes incidence. However, the heterogeneity across articles was moderate with an I2 of 60%. In sensitivity analysis, the heterogeneity of combined estimates did mark a change with the exclusion of Gong et al. or Lindström et al. (Table 3), indicating that the source of heterogeneity may be due to the different participants (participants of Gong et al. and Lindström et al. were prediabetes, Nanditha et al. were diabetes).
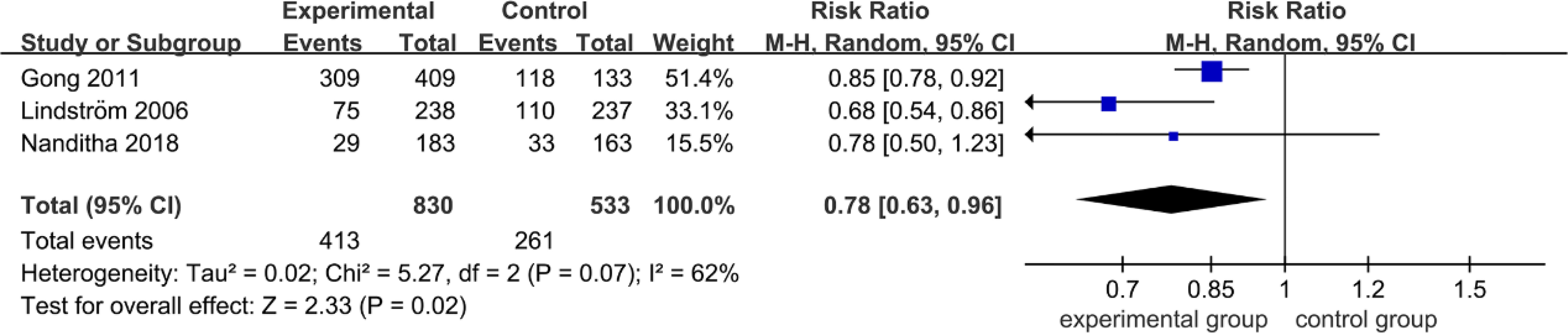
Figure 4 Forest plot of diabetes incidence in extended follow-up studies.

Table 3 The sensitivity analysis outcomes of diabetes incidence in extended follow-up studies.
Meta-Regression and Subgroup Analysis
Of the 21 articles, the 17 articles (the length of duration ranged from 2 to 6 years) were used to analyze the effect on diabetes prevention in intervention studies. To further evaluate the impact of duration on diabetes incidence, a random-effect meta-regression was conducted. The results of meta-regression analysis showed that duration (coefficient: -0.312, 95% CI: -0.457 to 0.166. p: 0.000) had a significant effect on prevention of diabetes. Based on the results of the meta-regression analysis, the subgroup analysis was performed for diabetes outcomes by follow-up duration (≤3 years, >3 years). As Figure 5 shows, the overall diabetes incidence was clearly reduced (0.62; 95% CI 0.54 to 0.71, p<0.01), with evidence of low heterogeneity (I2 = 29%, p = 0.14). Moreover, the diabetes incidence of the long-term duration group was clearly reduced by 0.05% compared with the relatively short-term-duration group.
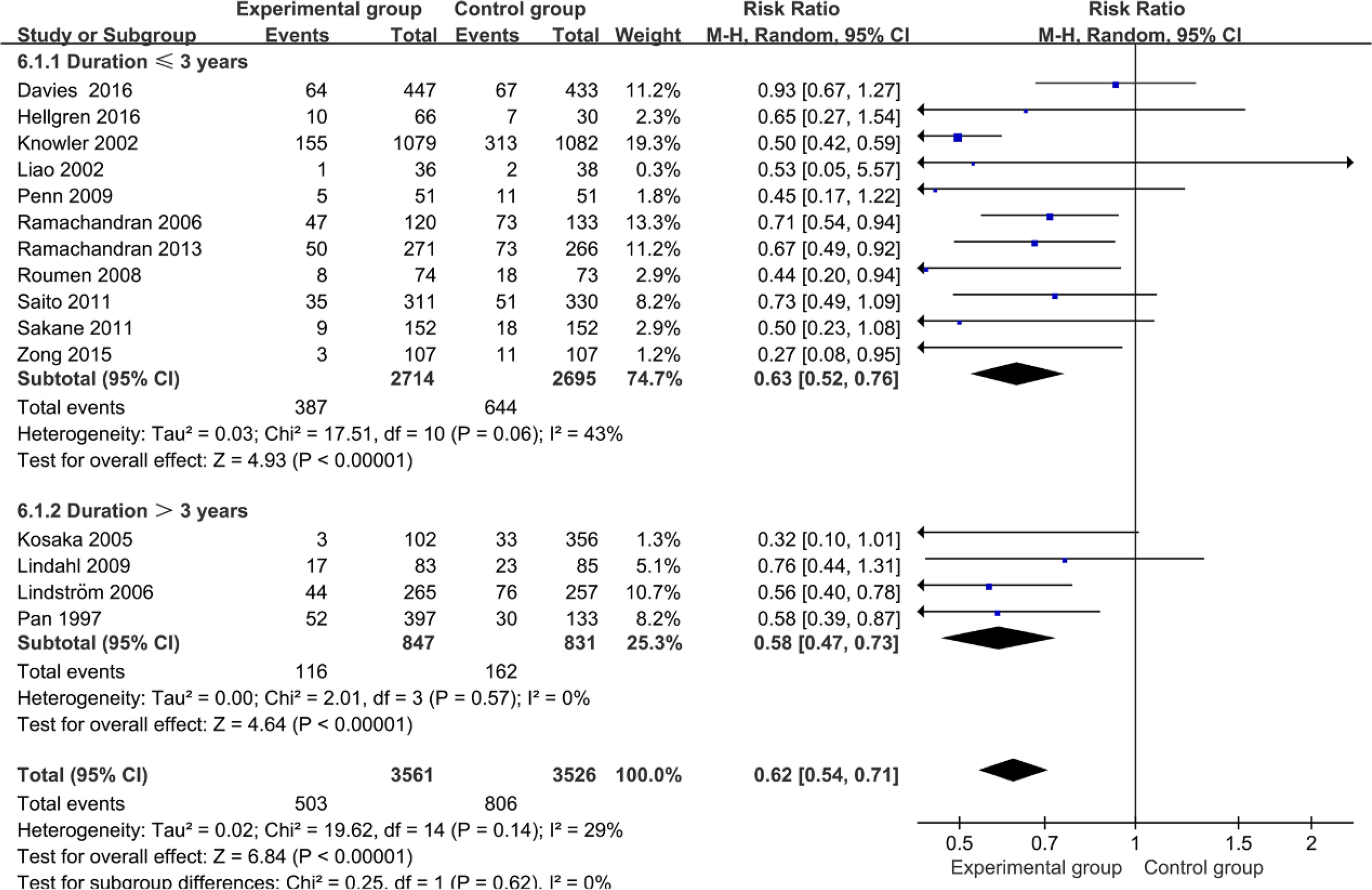
Figure 5 Forest plot of subgroup analysis of diabetes incidence in intervention studies.
Publication Bias
Publication bias was assessed for diabetes outcome of 15 intervention studies. Details of quality of bias assessment of the included studies are listed in Table 4, and the funnel plot of 15 articles is provided in Supplementary Table S4.
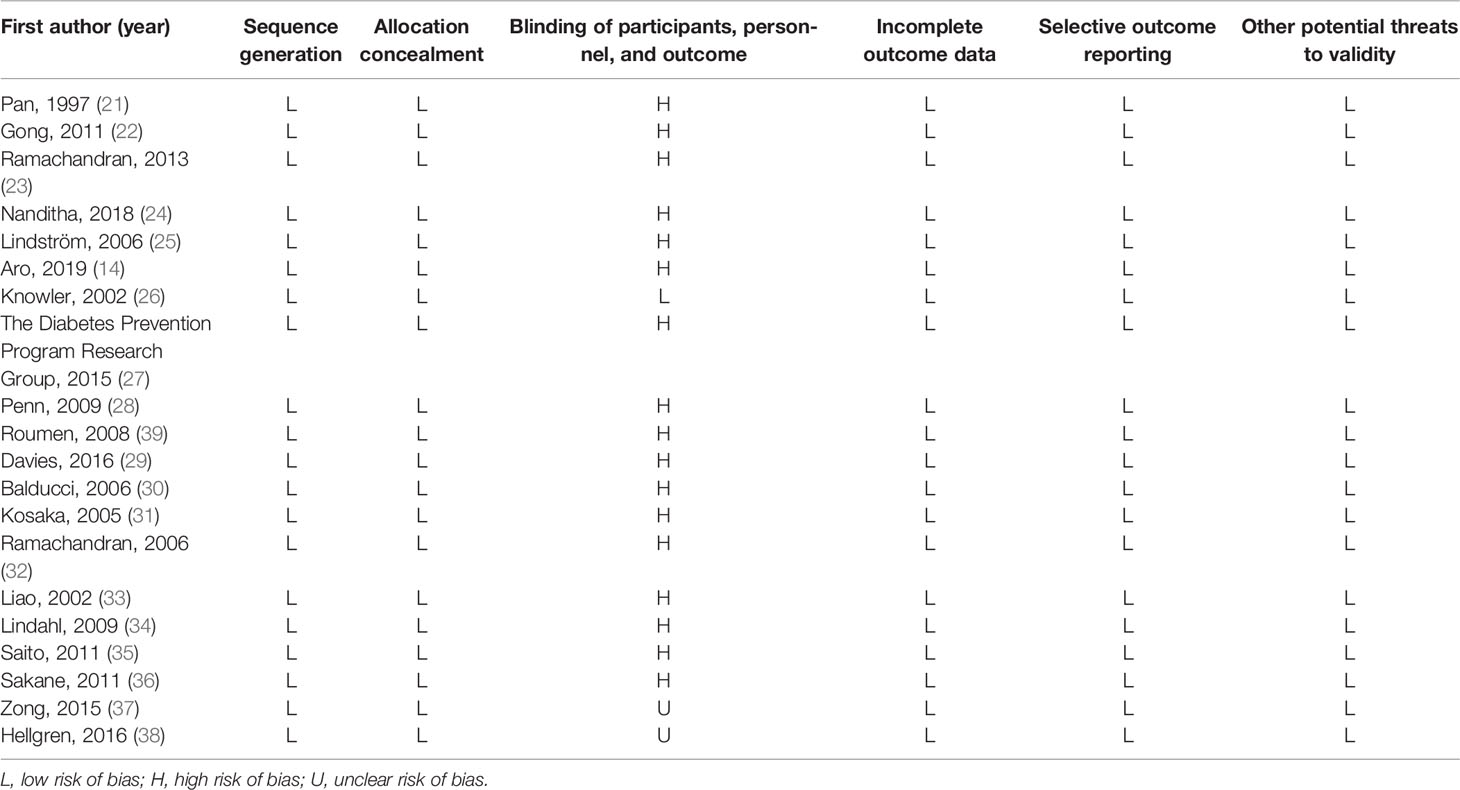
Table 4 Quality of bias assessment of the included studies according to Cochrane guidelines.
Discussion
In this systematic review and meta-analysis of 16 RCTs comparing non-pharmacological interventions with usual care, standard care, and medical therapy in prediabetes and diabetes, use of non-pharmacological interventions led to a long-term effect on reduction in the overall diabetes incidence and microvascular complications. Our forest plot of meta-analysis and sensitivity analysis demonstrated clearly that non-pharmacological interventions have such a reliable and long-term effect on the reduction in the microvascular complications among patients with hyperglycemia.
Our findings are consistent with several previous meta-analysis results which also indicated that the comprehensive non-pharmacological interventions showed significant effects on prevention of diabetes incidence and its risk of complications. Among them, lifestyle modification accounted for a large proportion, and previous meta-analysis studies have demonstrated a significant impact of lifestyle intervention on reduction of diabetes incidence and diabetes-related complications, as well as benefit in risk factors of cardiovascular disease (40–43). Moreover, several articles of meta-analysis show that physical activity and diet modification are also associated with a decrease in blood glucose and diabetes incidence (17, 44, 45). In addition, international guidelines recommended the year rate of diabetes incidence in diabetes prevention studies. In our meta-analysis, we have included that the follow-up duration of these studies was more than 2 years and even 20 years, and we not only analyzed the long-term effects of non-pharmacological therapies on diabetes incidence but also analyzed the efficacy of preventing microvascular events. Importantly, different intensities of intervention may affect the outcomes among participants. Low intensity of intervention may change the outcomes weakening the effects of interventions in these patients. However, with the increase of age, the intensity of intervention strategies and patients’ compliance may weaken as time goes by. We aimed to evaluate the relationship of un-pharmacotherapy with pharmacotherapy or placebo, and we did not evaluate the effects between different intensities of lifestyle intervention or physical activity in our analysis. The results of this pooled analysis show that non-pharmacological therapies (lifestyle intervention, physical activity, exercise, etc.) have a significant effect on the reduction in diabetes incidence in intervention studies and extended follow-up studies among prediabetic patients, and protection of diabetes from microvascular diseases. It is indicated that even a low intensity of intervention could lead to a significant effect and past interventions have had a very long-term effect and metabolic memory.
Some previous meta-analyses have reported relating outcomes of diabetic complications, such as the risk of cardiovascular events, and fewer systematic reviews have reported the chronic complications of diabetes in non-pharmacological studies. Since there are fewer studies that reported cardiovascular events in non-pharmacological studies, we have only analyzed the results of microvascular events. Originally, we have included RCTs of non-pharmacological-interventions in traditional Chinese medicine and bariatric surgeries. Compared with the medical therapies, bariatric and metabolic surgeries have been shown to be effective at preventing microvascular complications among patients with obesity and T2DM (46, 47). Bariatric and metabolic surgeries are not long-term interventions. Therefore, we updated the inclusion criteria and did not include surgery-related studies. In addition, bariatric and metabolic surgeries were invasive therapies through gastrectomy. Its necessity, safety, and postoperative complications should be carefully considered. Moreover, durations of non-pharmacological interventions of traditional Chinese medicine in diabetes prevention studies, such as acupuncture and Qigong, have been reported for less than 1 year, so we exclude them.
The strengths of this study include that it is a comprehensive non-pharmacological intervention (included RCTs more than 2 years and extended follow-up studies) that evaluates the effects on diabetes incidence and microvascular events. It was indicated that the past non-pharmacological interventions have had a long-term metabolic memory to prevent diabetes and its complications. This study has several limitations. First, regarding intervention strategies, only four intervention measures (lifestyle intervention, exercise, diet modification, and physical activity) met the inclusion criteria of this meta-analysis. Second is the variation in follow-up among the studies, ranging from 2 to 20 years. Last, due to the different treatment courses and different populations of patients, the heterogeneity remains relatively high among studies that evaluate the effect of reduction of diabetes incidence and microvascular complications.
Conclusion
Overall, non-pharmacological strategies implemented are promising approaches for preventing diabetes among prediabetic patients and microvascular complications among patients with hyperglycemia, with a long-term significant effect. More prospective randomized clinical trials and extended follow-up are needed to evaluate the non-pharmacological strategies on diabetes and microvascular events.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
FL conceived and designed the analysis. RZ and YC extracted the data and performed the analysis. RZ, YC, and YhZ wrote the paper and made the figures and tables. JD, XA, YD, YqZ, and XK provided the critical revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This work was funded by the 2015 Traditional Chinese Medicine Scientific Research (No. 201507001-11).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The research was conducted in the absence of any commercial or financial relationships.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.838224/full#supplementary-material
References
1. Grundy SM. Pre-Diabetes, Metabolic Syndrome, and Cardiovascular Risk. J Am Coll Cardiol (2012) 59(7):635–43. doi: 10.1016/j.jacc.2011.08.080
2. Tabák AG, Herder C, Rathmann W, Brunner EJ, Kivimäki M. Prediabetes: A High-Risk State for Diabetes Development. Lancet (2012) 379(9833):2279–90. doi: 10.1016/s0140-6736(12)60283-9
3. Abdul-Ghani M, DeFronzo RA, Jayyousi A. Prediabetes and Risk of Diabetes and Associated Complications: Impaired Fasting Glucose Versus Impaired Glucose Tolerance: Does It Matter? Curr Opin Clin Nutr Metab Care (2016) 19(5):394–9. doi: 10.1097/mco.0000000000000307
4. Wamil M, McMurray JJV, Scott CAB, Coleman RL, Sun Y, Standl E, et al. Predicting Heart Failure Events in Patients With Coronary Heart Disease and Impaired Glucose Tolerance: Insights From the Acarbose Cardiovascular Evaluation (ACE) Trial. Diabetes Res Clin Pract (2020) 170:108488. doi: 10.1016/j.diabres.2020.108488
5. Huang Y, Cai X, Mai W, Li M, Hu Y. Association Between Prediabetes and Risk of Cardiovascular Disease and All Cause Mortality: Systematic Review and Meta-Analysis. BMJ (2016) 355:i5953. doi: 10.1136/bmj.i5953
6. Cai X, Zhang Y, Li M, Wu JH, Mai L, Li J, et al. Association Between Prediabetes and Risk of All Cause Mortality and Cardiovascular Disease: Updated Meta-Analysis. BMJ (2020) 370:m2297. doi: 10.1136/bmj.m2297
7. Cai X, Liu X, Sun L, He Y, Zheng S, Zhang Y, et al. Prediabetes and the Risk of Heart Failure: A Meta-Analysis. Diabetes Obes Metab (2021) 23(8):1746–53. doi: 10.1111/dom.14388
8. Mai L, Wen W, Qiu M, Liu X, Sun L, Zheng H, et al. Association Between Prediabetes and Adverse Outcomes in Heart Failure. Diabetes Obes Metab (2021) 23(11):2476–83. doi: 10.1111/dom.14490
9. Smith-Marsh D. Pharmacological Strategies for Preventing Type 2 Diabetes in Patients With Impaired Glucose Tolerance. Drugs Today (Barc) (2013) 49(8):499–507. doi: 10.1358/dot.2013.49.8.2002839
10. Esefeld K, Kress S, Behrens M, Zimmer P, Stumvoll M, Thurm U, et al. Diabetes, Sports and Exercise. Exp Clin Endocrinol Diabetes (2020) 01:52–9. doi: 10.1055/a-1284-6097
11. Kriska AM, Rockette-Wagner B, Edelstein SL, Bray GA, Delahanty LM, Hoskin MA, et al. The Impact of Physical Activity on the Prevention of Type 2 Diabetes: Evidence and Lessons Learned From the Diabetes Prevention Program, a Long-Standing Clinical Trial Incorporating Subjective and Objective Activity Measures. Diabetes Care (2021) 44(1):43–9. doi: 10.2337/dc20-1129
12. Whelan ME, Denton F, Bourne CLA, Kingsnorth AP, Sherar LB, Orme MW, et al. A Digital Lifestyle Behaviour Change Intervention for the Prevention of Type 2 Diabetes: A Qualitative Study Exploring Intuitive Engagement With Real-Time Glucose and Physical Activity Feedback. BMC Public Health (2021) 21(1):130. doi: 10.1186/s12889-020-09740-z
13. Diabetes Prevention Program Research Group. The Diabetes Prevention Program (DPP): Description of Lifestyle Intervention. Diabetes Care (2002) 25(12):2165–71. doi: 10.2337/diacare.25.12.2165
14. Aro A, Kauppinen A, Kivinen N, Selander T, Kinnunen K, Tuomilehto J, et al. Life Style Intervention Improves Retinopathy Status-The Finnish Diabetes Prevention Study. Nutrients (2019) 11(7). doi: 10.3390/nu11071691
15. Chen Y, Zhang P, Wang J, Gong Q, An Y, Qian X, et al. Associations of Progression to Diabetes and Regression to Normal Glucose Tolerance With Development of Cardiovascular and Microvascular Disease Among People With Impaired Glucose Tolerance: A Secondary Analysis of the 30 Year Da Qing Diabetes Prevention Outcome Study. Diabetologia (2021) 64:1279–87. doi: 10.1007/s00125-021-05401-x
16. Bullard T, Ji M, An R, Trinh L, Mackenzie M, Mullen SP. A Systematic Review and Meta-Analysis of Adherence to Physical Activity Interventions Among Three Chronic Conditions: Cancer, Cardiovascular Disease, and Diabetes. BMC Public Health (2019) 19(1):636. doi: 10.1186/s12889-019-6877-z
17. Jenum AK, Brekke I, Mdala I, Muilwijk M, Ramachandran A, Kjøllesdal M, et al. Effects of Dietary and Physical Activity Interventions on the Risk of Type 2 Diabetes in South Asians: Meta-Analysis of Individual Participant Data From Randomised Controlled Trials. Diabetologia (2019) 62(8):1337–48. doi: 10.1007/s00125-019-4905-2
18. García-Molina L, Lewis-Mikhael AM, Riquelme-Gallego B, Cano-Ibáñez N, Oliveras-López MJ, Bueno-Cavanillas A. Improving Type 2 Diabetes Mellitus Glycaemic Control Through Lifestyle Modification Implementing Diet Intervention: A Systematic Review and Meta-Analysis. Eur J Nutr (2020) 59(4):1313–28. doi: 10.1007/s00394-019-02147-6
19. Knobloch K, Yoon U, Vogt PM. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement and Publication Bias. J Craniomaxillofac Surg (2011) 39(2):91–2. doi: 10.1016/j.jcms.2010.11.001
20. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev (2019) 10:Ed000142. doi: 10.1002/14651858.Ed000142
21. Pan XR, Li GW, Hu YH, Wang JX, Yang WY, An ZX, et al. Effects of Diet and Exercise in Preventing NIDDM in People With Impaired Glucose Tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care (1997) 20(4):537–44. doi: 10.2337/diacare.20.4.537
22. Gong Q, Gregg EW, Wang J, An Y, Zhang P, Yang W, et al. Long-Term Effects of a Randomised Trial of a 6-Year Lifestyle Intervention in Impaired Glucose Tolerance on Diabetes-Related Microvascular Complications: The China Da Qing Diabetes Prevention Outcome Study. Diabetologia (2011) 54(2):300–7. doi: 10.1007/s00125-010-1948-9
23. Ramachandran A, Snehalatha C, Ram J, Selvam S, Simon M, Nanditha A, et al. Effectiveness of Mobile Phone Messaging in Prevention of Type 2 Diabetes by Lifestyle Modification in Men in India: A Prospective, Parallel-Group, Randomised Controlled Trial. Lancet Diabetes Endocrinol (2013) 1(3):191–8. doi: 10.1016/s2213-8587(13)70067-6
24. Nanditha A, Snehalatha C, Raghavan A, Vinitha R, Satheesh K, Susairaj P, et al. The Post-Trial Analysis of the Indian SMS Diabetes Prevention Study Shows Persistent Beneficial Effects of Lifestyle Intervention. Diabetes Res Clin Pract (2018) 142:213–21. doi: 10.1016/j.diabres.2018.05.042
25. Lindström J, Ilanne-Parikka P, Peltonen M, Aunola S, Eriksson JG, Hemiö K, et al. Sustained Reduction in the Incidence of Type 2 Diabetes by Lifestyle Intervention: Follow-Up of the Finnish Diabetes Prevention Study. Lancet (2006) 368(9548):1673–9. doi: 10.1016/s0140-6736(06)69701-8
26. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the Incidence of Type 2 Diabetes With Lifestyle Intervention or Metformin. N Engl J Med (2002) 346(6):393–403. doi: 10.1056/NEJMoa012512
27. Diabetes Prevention Program Research Group. Long-Term Effects of Lifestyle Intervention or Metformin on Diabetes Development and Microvascular Complications Over 15-Year Follow-Up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol (2015) 3(11):866–75. doi: 10.1016/s2213-8587(15)00291-0
28. Penn L, White M, Oldroyd J, Walker M, Alberti KG, Mathers JC. Prevention of Type 2 Diabetes in Adults With Impaired Glucose Tolerance: The European Diabetes Prevention RCT in Newcastle Upon Tyne, UK. BMC Public Health (2009) 9:342. doi: 10.1186/1471-2458-9-342
29. Davies MJ, Gray LJ, Troughton J, Gray A, Tuomilehto J, Farooqi A, et al. A Community Based Primary Prevention Programme for Type 2 Diabetes Integrating Identification and Lifestyle Intervention for Prevention: The Let's Prevent Diabetes Cluster Randomised Controlled Trial. Prev Med (2016) 84:48–56. doi: 10.1016/j.ypmed.2015.12.012
30. Balducci S, Iacobellis G, Parisi L, Di Biase N, Calandriello E, Leonetti F, et al. Exercise Training can Modify the Natural History of Diabetic Peripheral Neuropathy. J Diabetes Complications (2006) 20(4):216–23. doi: 10.1016/j.jdiacomp.2005.07.005
31. Kosaka K, Noda M, Kuzuya T. Prevention of Type 2 Diabetes by Lifestyle Intervention: A Japanese Trial in IGT Males. Diabetes Res Clin Pract (2005) 67(2):152–62. doi: 10.1016/j.diabres.2004.06.010
32. Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V. The Indian Diabetes Prevention Programme Shows That Lifestyle Modification and Metformin Prevent Type 2 Diabetes in Asian Indian Subjects With Impaired Glucose Tolerance (IDPP-1). Diabetologia (2006) 49(2):289–97. doi: 10.1007/s00125-005-0097-z
33. Liao D, Asberry PJ, Shofer JB, Callahan H, Matthys C, Boyko EJ, et al. Improvement of BMI, Body Composition, and Body Fat Distribution With Lifestyle Modification in Japanese Americans With Impaired Glucose Tolerance. Diabetes Care (2002) 25(9):1504–10. doi: 10.2337/diacare.25.9.1504
34. Lindahl B, Nilssön TK, Borch-Johnsen K, Røder ME, Söderberg S, Widman L, et al. A Randomized Lifestyle Intervention With 5-Year Follow-Up in Subjects With Impaired Glucose Tolerance: Pronounced Short-Term Impact But Long-Term Adherence Problems. Scand J Public Health (2009) 37(4):434–42. doi: 10.1177/1403494808101373
35. Saito T, Watanabe M, Nishida J, Izumi T, Omura M, Takagi T, et al. Lifestyle Modification and Prevention of Type 2 Diabetes in Overweight Japanese With Impaired Fasting Glucose Levels: A Randomized Controlled Trial. Arch Intern Med (2011) 171(15):1352–60. doi: 10.1001/archinternmed.2011.275
36. Sakane N, Sato J, Tsushita K, Tsujii S, Kotani K, Tsuzaki K, et al. Prevention of Type 2 Diabetes in a Primary Healthcare Setting: Three-Year Results of Lifestyle Intervention in Japanese Subjects With Impaired Glucose Tolerance. BMC Public Health (2011) 11(1):40. doi: 10.1186/1471-2458-11-40
37. Zong Y, Duan P, Ding X, Si L, Liu J, Tu P. Effects of Lifestyle and Quantitative Nutrition Interventions on Individuals With Prediabetes. Zhonghua Yi Xue Za Zhi (2015) 95(40):3293–6.
38. Hellgren MI, Jansson PA, Wedel H, Lindblad U. A Lifestyle Intervention in Primary Care Prevents Deterioration of Insulin Resistance in Patients With Impaired Glucose Tolerance: A Randomised Controlled Trial. Scand J Public Health (2016) 44(7):718–25. doi: 10.1177/1403494816663539
39. Roumen C, Corpeleijn E, Feskens EJ, Mensink M, Saris WH, Blaak EE. Impact of 3-Year Lifestyle Intervention on Postprandial Glucose Metabolism: The SLIM Study. Diabetes Med (2008) 25(5):597–605. doi: 10.1111/j.1464-5491.2008.02417.x
40. Chen L, Pei JH, Kuang J, Chen HM, Chen Z, Li ZW, et al. Effect of Lifestyle Intervention in Patients With Type 2 Diabetes: A Meta-Analysis. Metabolism (2015) 64(2):338–47. doi: 10.1016/j.metabol.2014.10.018
41. Huang XL, Pan JH, Chen D, Chen J, Chen F, Hu TT. Efficacy of Lifestyle Interventions in Patients With Type 2 Diabetes: A Systematic Review and Meta-Analysis. Eur J Intern Med (2016) 27:37–47. doi: 10.1016/j.ejim.2015.11.016
42. Colpani V, Baena CP, Jaspers L, van Dijk GM, Farajzadegan Z, Dhana K, et al. Lifestyle Factors, Cardiovascular Disease and All-Cause Mortality in Middle-Aged and Elderly Women: A Systematic Review and Meta-Analysis. Eur J Epidemiol (2018) 33(9):831–45. doi: 10.1007/s10654-018-0374-z
43. Uusitupa M, Khan TA, Viguiliouk E, Kahleova H, Rivellese AA, Hermansen K, et al. Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients (2019) 11(11). doi: 10.3390/nu11112611
44. Mijatovic-Vukas J, Capling L, Cheng S, Stamatakis E, Louie J, Cheung NW, et al. Associations of Diet and Physical Activity With Risk for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients (2018) 10(6). doi: 10.3390/nu10060698
45. Doi SAR, Furuya-Kanamori L, Toft E, Musa OAH, Mohamed AM, Clark J, et al. Physical Activity in Pregnancy Prevents Gestational Diabetes: A Meta-Analysis. Diabetes Res Clin Pract (2020) 168:108371. doi: 10.1016/j.diabres.2020.108371
46. Yan G, Wang J, Zhang J, Gao K, Zhao Q, Xu X. Long-Term Outcomes of Macrovascular Diseases and Metabolic Indicators of Bariatric Surgery for Severe Obesity Type 2 Diabetes Patients With a Meta-Analysis. PLoS One (2019) 14(12):e0224828. doi: 10.1371/journal.pone.0224828
Keywords: randomized controlled trial, meta-analysis, diabetes incidence, long-term, complications, non-pharmacological intervention
Citation: Zhou R, Cui Y, Zhang Y, De J, An X, Duan Y, Zhang Y, Kang X and Lian F (2022) The Long-Term Effects of Non-Pharmacological Interventions on Diabetes and Chronic Complication Outcomes in Patients With Hyperglycemia: A Systematic Review and Meta-Analysis. Front. Endocrinol. 13:838224. doi: 10.3389/fendo.2022.838224
Received: 17 December 2021; Accepted: 10 February 2022;
Published: 18 March 2022.
Edited by:
Alok Raghav, Ganesh Shankar Vidyarthi Memorial Medical College, IndiaReviewed by:
Jamal Ahmad, Aligarh Muslim University, IndiaYuli Huang, Southern Medical University, China
Copyright © 2022 Zhou, Cui, Zhang, De, An, Duan, Zhang, Kang and Lian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fengmei Lian, Njk0Mzk3NjQ0QHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship