 Aneta Monika Gawlik1,2*
Aneta Monika Gawlik1,2* Elżbieta Berdej-Szczot2
Elżbieta Berdej-Szczot2 Iga Chmiel2
Iga Chmiel2 Miłosz Lorek1,2
Miłosz Lorek1,2 Aleksandra Antosz1,2
Aleksandra Antosz1,2 Małgorzata Firek-Pędras2Lesław Szydłowski3Kamila Maria Ludwikowska4Magdalena Okarska-Napierała5Natalia Dudek5Krzysztof Piwoński6
Małgorzata Firek-Pędras2Lesław Szydłowski3Kamila Maria Ludwikowska4Magdalena Okarska-Napierała5Natalia Dudek5Krzysztof Piwoński6 Aneta Afelt6,7Catherine Suski-Grabowski6
Aneta Afelt6,7Catherine Suski-Grabowski6 Miron Bartosz Kursa6Ernest Kuchar5Leszek Szenborn4
Miron Bartosz Kursa6Ernest Kuchar5Leszek Szenborn4 Teresa Jackowska8Jarosław Peregud-Pogorzelski9
Teresa Jackowska8Jarosław Peregud-Pogorzelski9 Artur Mazur10
Artur Mazur10- 1Department of Pediatrics and Pediatric Endocrinology, Faculty of Medical Sciences, Medical University of Silesia, Katowice, Poland
- 2Department of Pediatrics and Pediatric Endocrinology, John Paul II Upper Silesian Child Health Centre, Katowice, Poland
- 3Department of Pediatric Cardiology, Medical University of Silesia, Katowice, Poland
- 4Department of Pediatric Infectious Diseases, Wrocław Medical University, Wrocław, Poland
- 5Department of Pediatrics with Clinical Assessment Unit, Medical University of Warsaw, Warsaw, Poland
- 6Interdisciplinary Centre for Mathematical and Computational Modelling, University of Warsaw, Warsaw, Poland
- 7Espace-DEV, IRD - Institut de Recherche pour le Développement, Montpellier, France
- 8Department of Pediatrics, Medical Center of Postgraduate Education, Warsaw, Poland
- 9Department of Pediatrics and Pediatric Oncology, Pomeranian Medical University, Szczecin, Poland
- 10Department of Pediatrics, Pediatric Endocrinology and Diabetes, Medical College University of Rzeszów, Rzeszów, Poland
Background: A new disease entity called multisystem inflammatory syndrome in children (MIS-C) is a rare consequence of COVID-19 infection. The pathophysiology and risk factors of MIS-C are still unclear, and the clinical manifestation ranges from milder forms to cases needing intensive care unit treatment. Based on available data, obesity is linked to pro-inflammatory stimulation. Moreover, several studies showed that obesity could play a role in COVID-19 severity and its comorbidities among the adult and children’s populations. This study aimed to investigate the influence of overweightedness/obesity in childhood for the course of MIS-C in Poland.
Methods: This study presented data from the national MultiOrgan Inflammatory Syndromes COVID-19 Related Study (MOIS-CoR) collected between 4 March 2020 and 20 February 2021. Of the 371 patients that met the Polish MIS-C criteria, 306 were included for further analysis.
Results: Children who are obese (OB with body mass index (BMI) ≥95th percentile) and overweight (OV with BMI ≥85th percentile but <95th percentile) (28 and 49 patients, respectively) represented 25.1% (n=77) of all recruited patients. Complete recovery at the time of discharge presented in 93% of normal body weight (NW) participants and 90% of OV children (p>0.05). Among OB children, 76% recovered fully, which differed from the NW group (p=0.01). Calculated odds ratio (OR) of incomplete recovery for OB children was 4.2. Irrespective of body weight, there were no differences (p>0.05) in the length of hospitalization and the duration of symptoms (for OB, 13 and 16.5 days; for OV and NW, 10 and 14 days, respectively), as well as in the frequency of cardiovascular abnormalities, necessity of oxygen therapy (OB, 26.9%; OV, 23.9%; and NW, 20.7%), and intravenous immunoglobulin and glucocorticosteroid (GCS) treatment.
Conclusion: The higher risk of incomplete recovery and observed tendency toward a worsening course of MIS-C in patients with obesity suggest the need for further studies to confirm and understand our findings.
Introduction
In mid-April 2020, a few cases of uncommon multisystem inflammatory conditions emerged during the COVID-19 pandemic (1). This new disease entity, called, by the Royal College of Pediatrics and Child Health in the United Kingdom, pediatric inflammatory multisystem syndrome temporally associated with severe acute respiratory syndrome coronavirus 2 (PIMS-TS) (2), is described by the World Health Organization and the Centers for Disease Control and Prevention in Europe and the United States as the multisystem inflammatory syndrome in children (MIS-C) (3, 4). MIS-C is a rare consequence of COVID-19 infection and usually affects previously healthy children, rarely with comorbidities, after 4–8 weeks of COVID-19 infection (5).
The pathophysiology and risk factors of the disease are not yet clear, but they mostly included male sex, concomitance of asthma, diabetes mellitus, neurologic disorders, and other chronic disorders like obesity (5). Clinical manifestation ranges from milder forms to cases in need of intensive care unit treatment (6). Patients may present features characteristic of other inflammation entities such as Kawasaki disease (KD) (7, 8), atypical Kawasaki disease (aKD), toxic shock syndrome (TSS) (9, 10), or macrophage activation syndrome (MAS) (11). The abnormalities are usually observed among the cardiovascular, gastrointestinal, dermatological, hematological, neurological, and respiratory systems.
Based on available data, obesity, due to engaging inflammatory pathways and cytokine signaling cascades, may lead to chronic low-grade inflammation (12–14). Although the pathways correlating obesity with SARS-CoV-2 infection are still hypothetical (15, 16), several studies showed that obesity plays a role in COVID-19 severity among adult and children’s populations (5, 17–19).
Here, we analyzed data from the national MultiOrgan Inflammatory Syndromes COVID-19 Related Study (MOIS-CoR) to investigate the influence of overweightedness/obesity on the PIMS-TS/MIS-C course and final outcome.
Materials and methods
We analyzed the MOIS-CoR database containing data collected between 4 March 2020 and 20 February 2021. The database developments were adopted and described previously (20, 21). The data were collected using a special online form that was created and standardized by a multicenter group of experts from all over the country. The first Polish recommendation for MIS-C was established on April 2020. The criteria for PIMS/MIS-C and other clinical status definitions are presented in Tables 1, 2.

Table 1 The Polish inclusion criteria of PIMS/MIS-C (20).
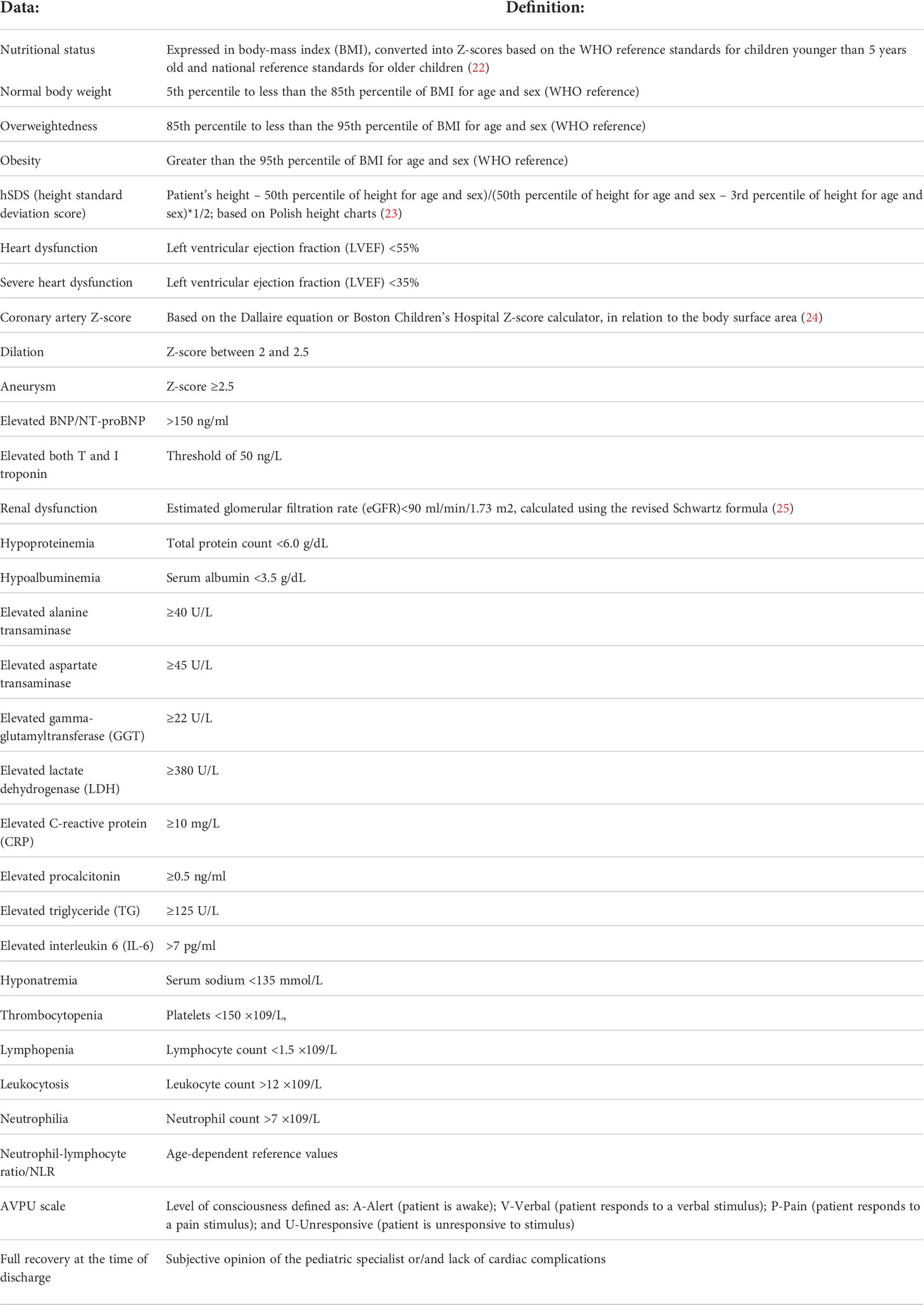
Table 2 Clinical and biochemical status definitions.
Statistical methods
All statistical analyses were performed using Statistica 13 PL software (StatSoft Inc., Tulsa, OK, USA). A p-value of <0.05 was considered significant. The Shapiro-Wilk test was utilized to verify the normality of distribution. To compare qualitative variables, the Chi2 test was utilized. Odds ratio was used for logistic regression. The comparisons between two parametric values were made by using the Student’s t-test or the Mann-Whitney U test for non-parametric distributions.
Results
Clinical phenotype
The MOIS-Cor Project included 437 patients. Our population, except for two Asian patients, was homogeneous, and comprised Caucasian children. Twelve patients did not fulfill the Polish PIMS criteria. Additionally, 54 cases were excluded due to lack of data. The Polish PIMS criteria were fulfilled by 371 patients. Moreover, to compare children with obesity/overweightedness to children with normal body weight, 22 underweight children were excluded. Of the 349 remaining patients, 43 were also excluded due to missing values in age, sex, height or weight. In further analyses, 306 patients were included. Two separate analyses were conducted: the first one included a study group (Obese/OB + Overweight/OV; n=77) vs. a control group (Normal Weight/NW; n=229), and the second encompassed all three groups: NW vs. OB vs. OV patients. The flowchart is presented in Figure 1.
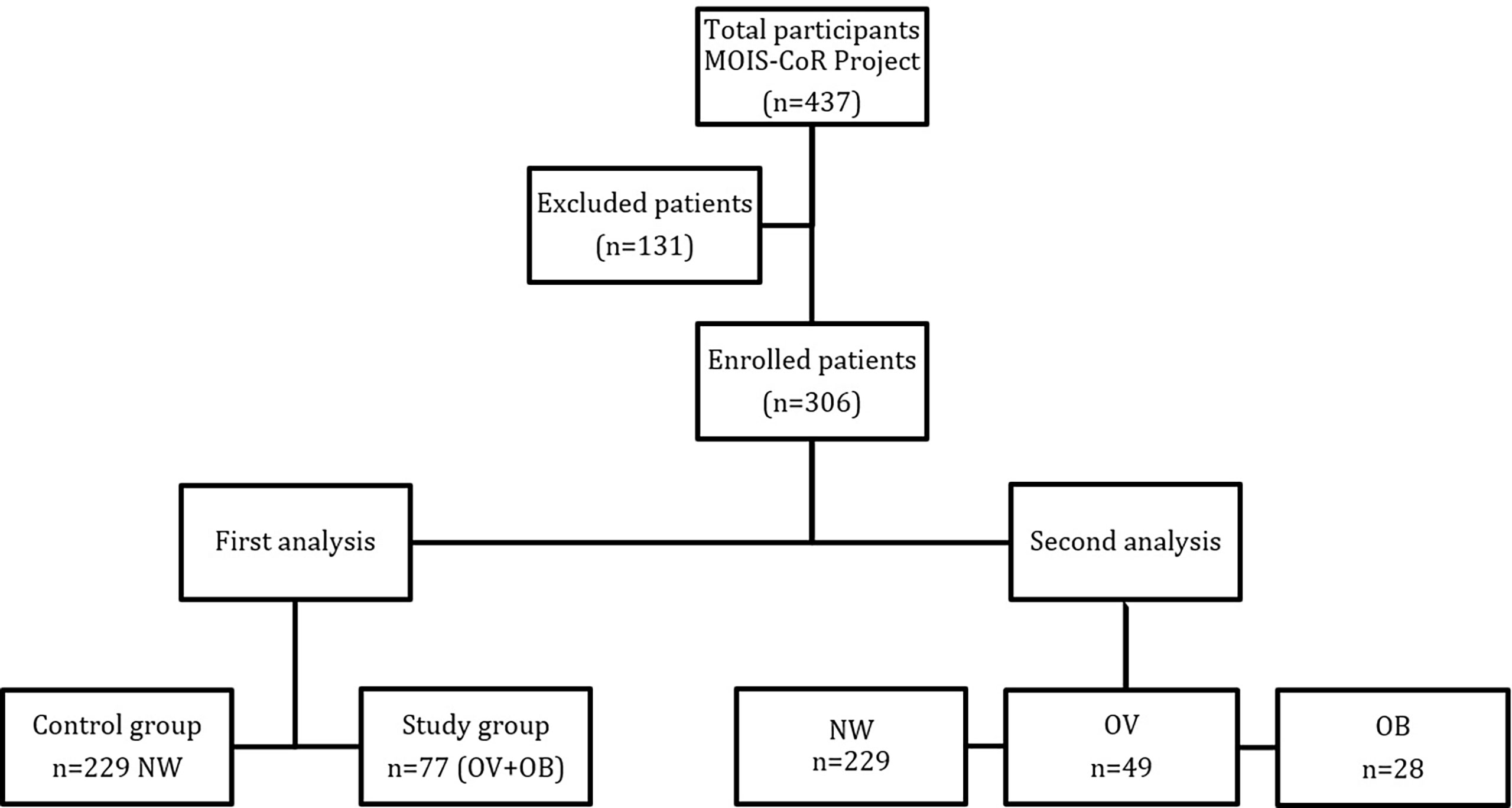
Figure 1 Flowchart of patients included in the MOIS-CoR study.
There were 229 NW, 28 OB, and 49 OV patients. They were 8.18 (95% CI: 7.6; 8.77), 8.55 (95% CI: 6.73; 10.38), and 8.47 (95% CI: 7.14; 9.81) years old, respectively. OB and OV children represented 25.1% (n=77) of all recruited patients. These groups did not differ in age, sex, and height as well as in the occurrence of other comorbidities (p>0.05) (Table 3).
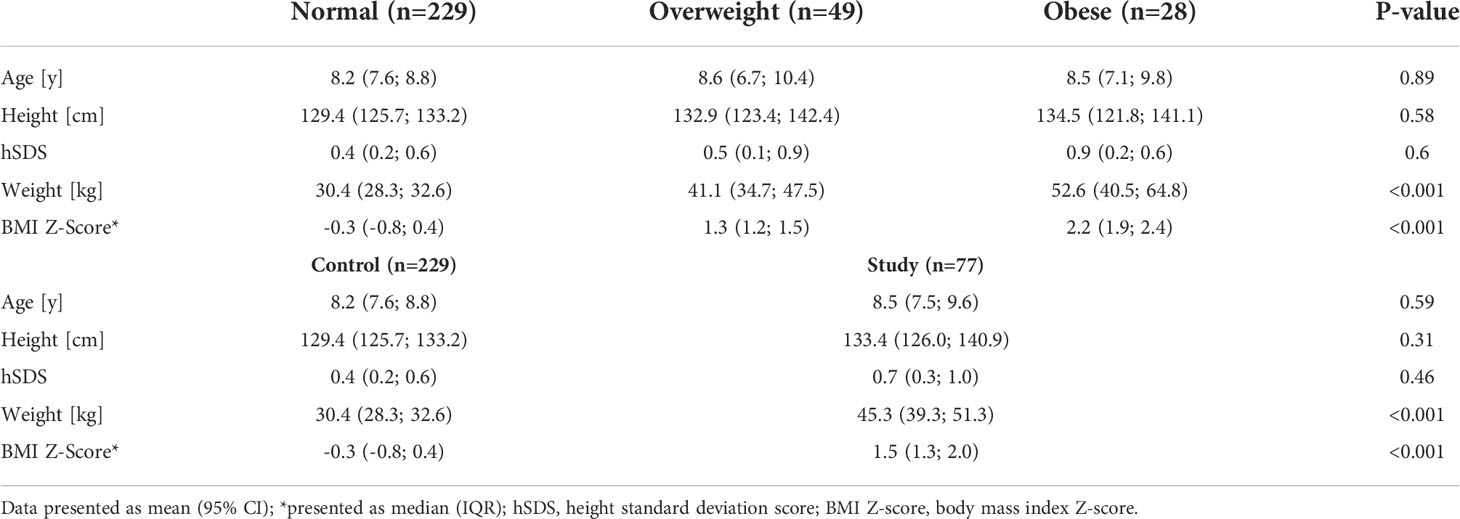
Table 3 Anthropometrical data of study subjects.
There were 5.6% (n=17/306) of patients categorized below “A” in the alert-verbal-pain-unresponsive (AVPU) scale at admission. In regard to body weight, n=2/49 (4.1%) were OV, n=15/214 (6.5%) were NW, and none was OB. During hospitalization, n=2/23 (7.1%) of OB children, n=6/44 (12.2%) of OV children, and n=37/207 (16.2%) of NW patients were described as below “A” in the AVPU scale.
Biochemical phenotype
Comparisons of laboratory tests results are presented in Tables 4, 5. Apart from interleukin 6 (IL-6) and total protein at admission, there was no difference between the study group (OV and OB) and the control group in inflammatory assays such as C-reactive protein (CRP), procalcitonin, leukocytosis, neutrophilia, lymphopenia, neutrophil–lymphocyte ratio (NLR), and albumins.
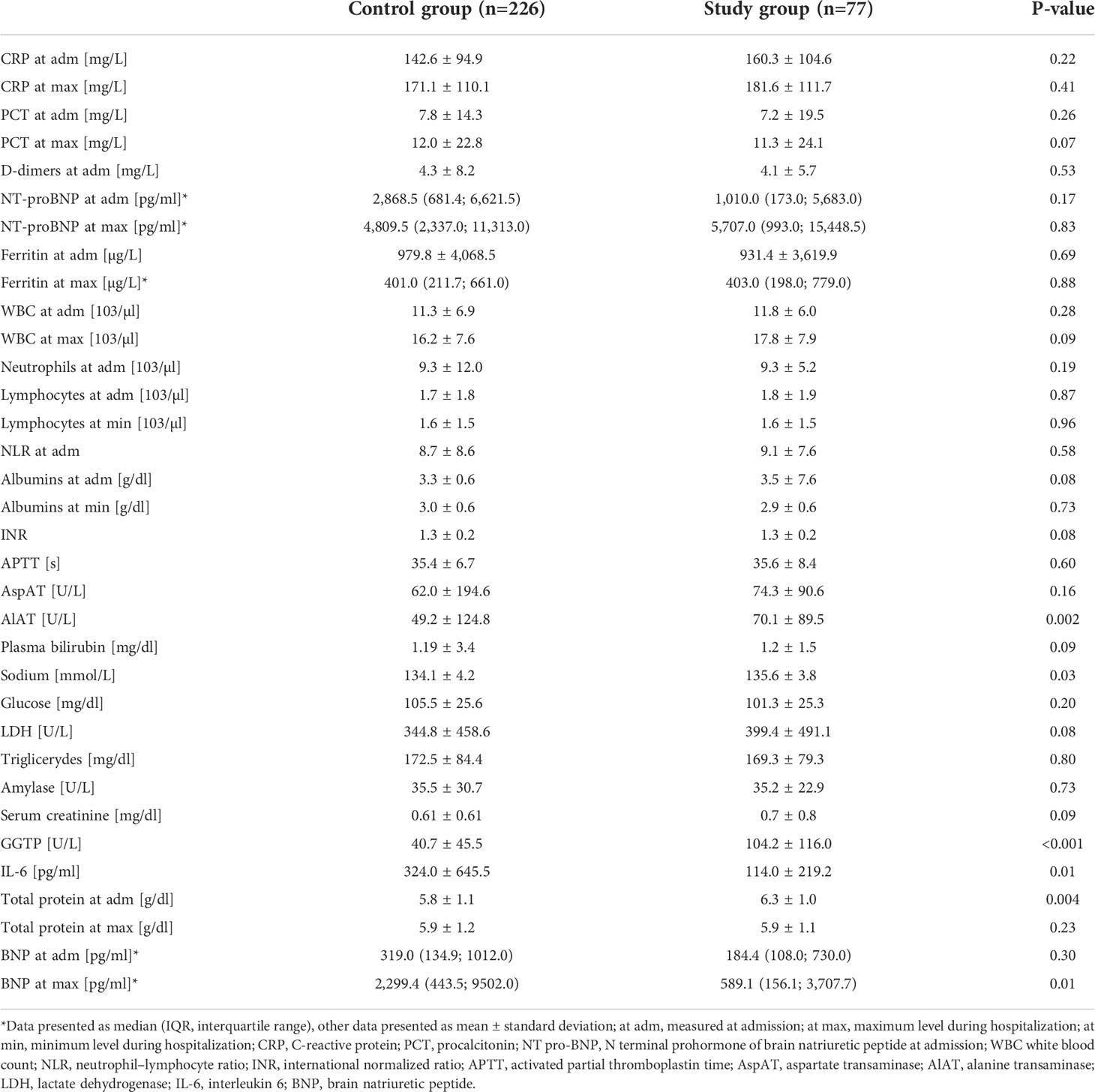
Table 4 Comparison of laboratory results between the control and study groups.
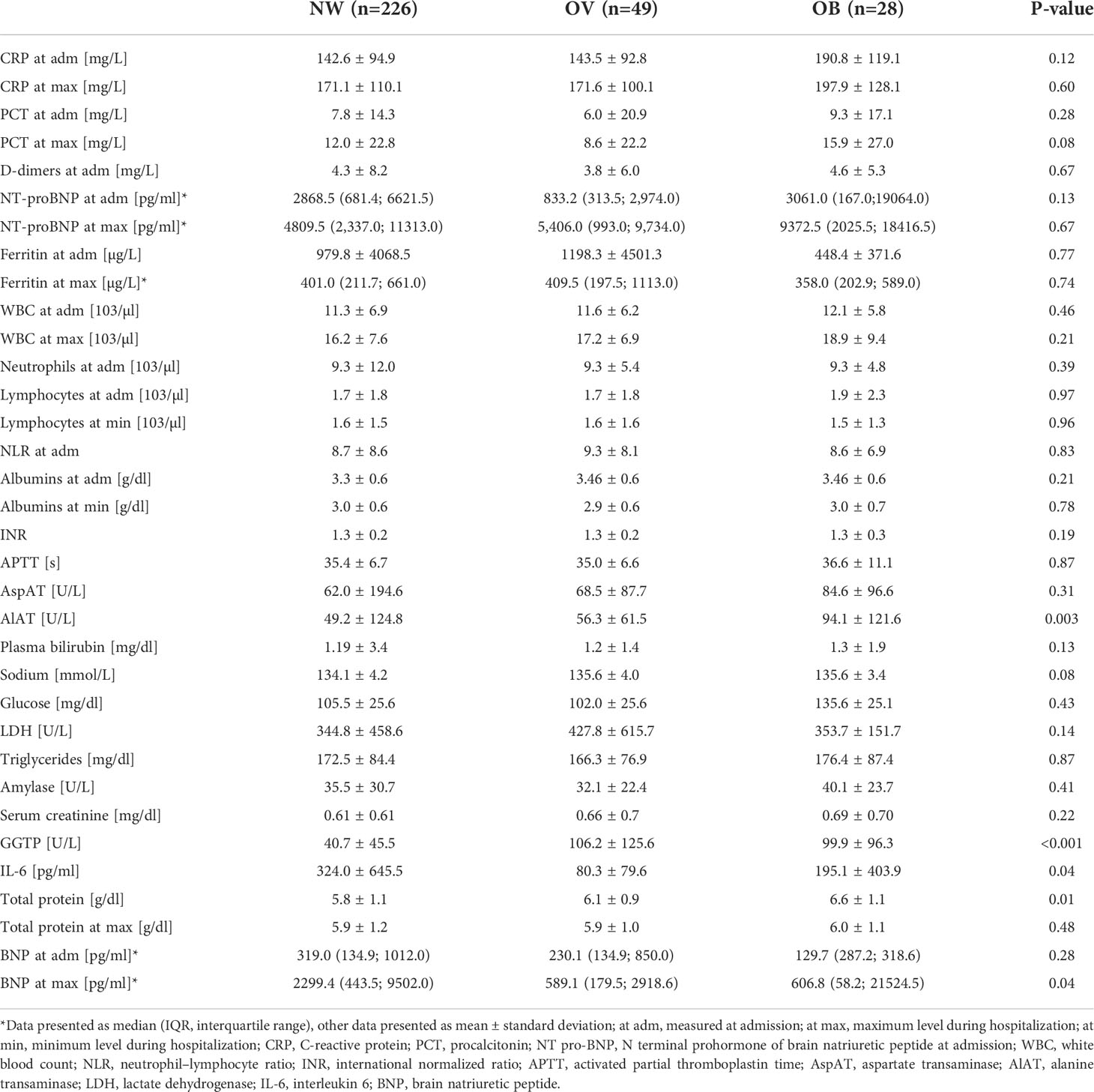
Table 5 Comparison of laboratory results between the NW, OV, and OB groups at admission.
There were significant differences between transaminases (AlAT, GGT) in the control/NW and the OB/OV groups, but no difference in the case of AspAT, LDH, and TG (Tables 4, 5).
Brain natriuretic peptide (BNP) level at admission did not differ between the control/NW and study/OB and OV; however, the BNP level at its maximum was higher in the control group (Tables 4, 5).
Cardiac phenotype/status
Those who had some echocardiographic abnormalities (decreased left ventricular ejection fraction (LVEF), coronary artery abnormalities (CAA) or pericardial effusion) were 40.6% (n=26/64) of the study/OB and OV patients and 29.4% (n=58/197) of the control/NW patients; however, there were no differences in particular cardiovascular abnormalities between groups (p>0.05). Those who developed cardiac disorders (p=>0.05) were 47.6% (n=10/21) of OB, 37.2% (n=16/43) of OV, and 29.4% (n=58/197) of NW patients. Among the study/OB and OV patients, 17.2% (n=11/64) were reported with decreased left ventricular ejection fraction during hospitalization, and 10.0% (n=5/50) maintained this condition. Pericardial effusion occurred in 9.4% (n=6/64) of the study/OB and OV patients, with two cases of arrhythmia and one case of myocarditis. There were 12.8% (n=5) of the study/OB and OV patients who developed vessel malformations (two cases of dilatation, one small aneurysm, one medium aneurysm, and one large aneurysm; see Table 6).
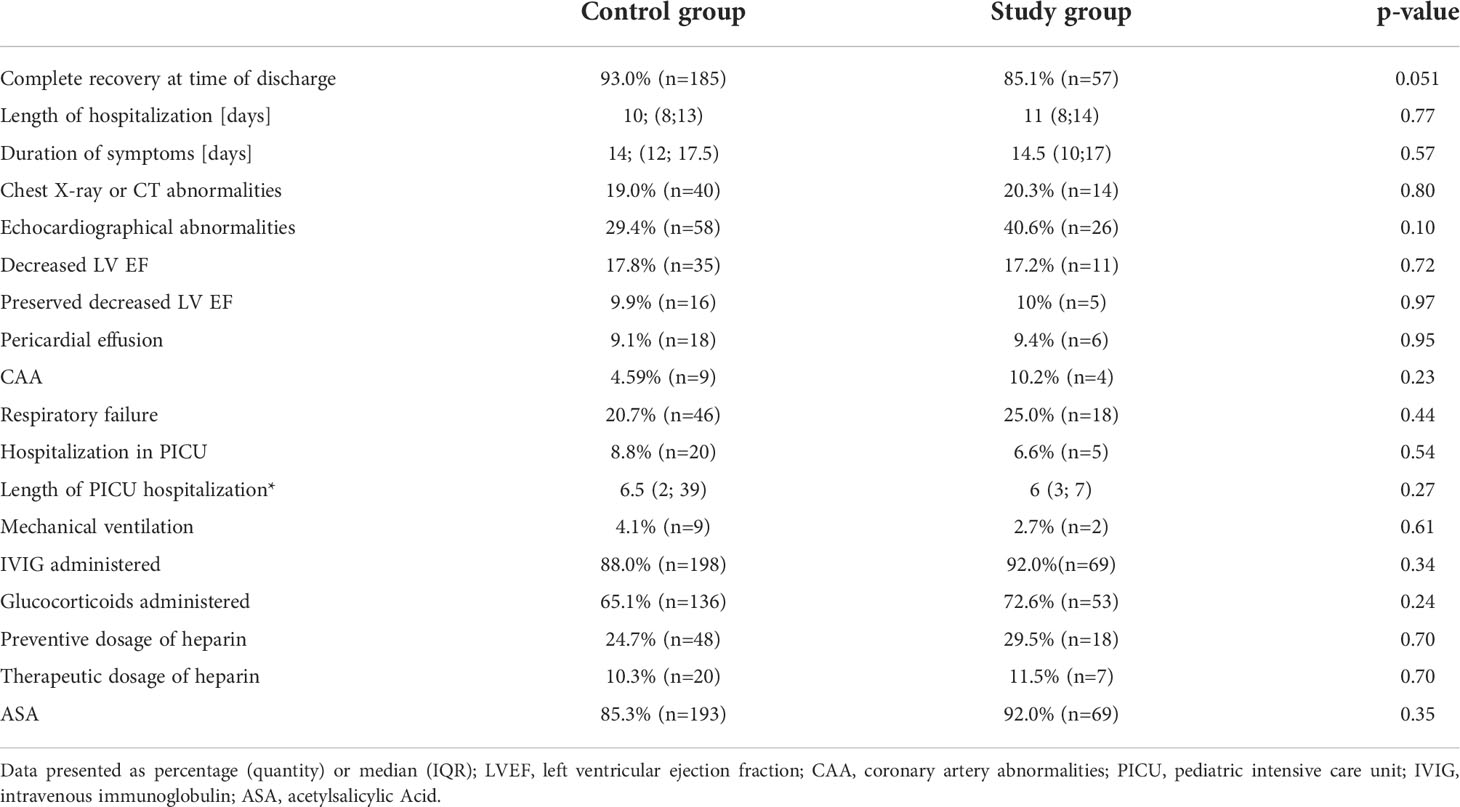
Table 6 Clinical findings of control and study groups.
A total of 34.0% (n=104/306) of patients developed hypotension during hospitalization; 10 (35.7% n=10/28) of the OB, 17 (34.7% n=17/49) of the OV, and 77 (33.6% n=77/229) of the NW groups (p>0.05).
Additional exam(s)
A total of 17.6% (n=54/306) of patients had detected X-ray or CT abnormalities at any time of hospitalization: In the OB group, it was 28.6% (n=8/28); in OV, 12.2% (n=6/38); and in NW, 17.5% (n=40/229). Only 75.9% (n=41/54) of all patients with chest imaging abnormalities recovered fully at the time of discharge. Two out of eight (25%) OB, one out of six (16.7%) OV, and three out of 40 (7.5%) NW children did not achieve full recovery.
Treatment
Oxygen supplementation was necessary in 25.0% (n=18) of cases in the study/OV and OB patients and in 20.7% (n=46) in the control/NW group (p>0.05). Oxygen therapy was required by 26.9% (n=7/26) of OB, 23.9% (n=11/46) of OV, and 20.7% (n=46/222) of NW patients (p>0.05). Among all participants, 5.7% (n=25) needed hospitalization at the pediatric intensive care unit (PICU); three of them were obese, and two were overweight. A total of 6.79% (n=11) of patients required mechanical ventilation, and two of them were from the study group. Of the mechanically ventilated patients, 72.7% (n=8/11) achieved full recovery. The median duration of hospitalization at the PICU was 6 days (interquartile range, IQR: 4-7), while the longest hospitalization at the PICU was 39 days. Among all patients who needed oxygen supplementation, 5.3% (n=3/53) did not achieve full recovery. All patients with obesity who were treated with oxygen reached full recovery at the time of discharge. Length of hospitalization was 13 (IQR: 10-16) days, and the symptoms lasted 17 (IQR: 15-26) days. A total of 53.1% (n=34/64) of the patients had diagnosed echocardiographic abnormalities. Intravenous immunoglobulin (IVIG) was administered to 87.3% of patients (n=267): 92.0% (n=69) of the study/OB and OV and 88.0% (n=198) of the control/NW patients (p>0.05). Glucocorticosteroids (GCSs) were administered in 72.6% (n=53) of the study/OB and OV patients and 65.1% (n=136) of the control/NW groups (p>0.05). A preventive dose of heparin s.c. was used in 29.5% (n=18) of the children in the study/OB and OV group and 24.7% (n=48) in the control/NW group (p>0.05). There were also no differences in the usage of a therapeutic dosage: 11.5% (n=7) and 10.3% (n=20) in the study and control groups, respectively. Acetylsalicylic acid (ASA) was administered to 85.6% (n=262) of the patients: 92.0% (n=69) of study patients and 85.8% (n=193) of normal body weight patients (p>0.05). There were no differences in the length of hospitalization and the duration of symptoms between the study and control groups (p>0.05). In the study group, the median length of hospitalization was 11 days (IQR: 8-14) and the symptoms lasted 14.5 days (IQR: 10-17). OB patients needed 13 (IQR: 9-16) days of hospitalization. OV patients and those with normal weight (NW) were equally hospitalized for 10 (IQR: 8-13) days. All three groups did not differ between each other (p>0.05). Symptoms lasted 16.5 (IQR: 12-19) days for the OB group, 14 (IQR: 11-17) days for the OV group, and 14 (IQR: 12-17) days for the NW group. There was no difference between groups (p>0.05). Data were not available on whether patients who did not recover after discharge were discharged to home or referred to another hospital unit.
Body weight did not differentiate the study group/OB and OV from the control group in regard to complete recovery at the time of discharge: 85.1% and 93.0%, respectively (p=0.06). However, only 76.0% (n=19/25) of OB children recovered fully and differed from the NW group (p=0.01; see Figure 2). Calculated odds ratio of incomplete recovery for OB children was 4.2 (95% CI: 1.4; 12.1) (Table 4). Among the OV children, 90% (n=38/42) recovered fully and this result did not differ compared to NW and OB children (p>0.05).
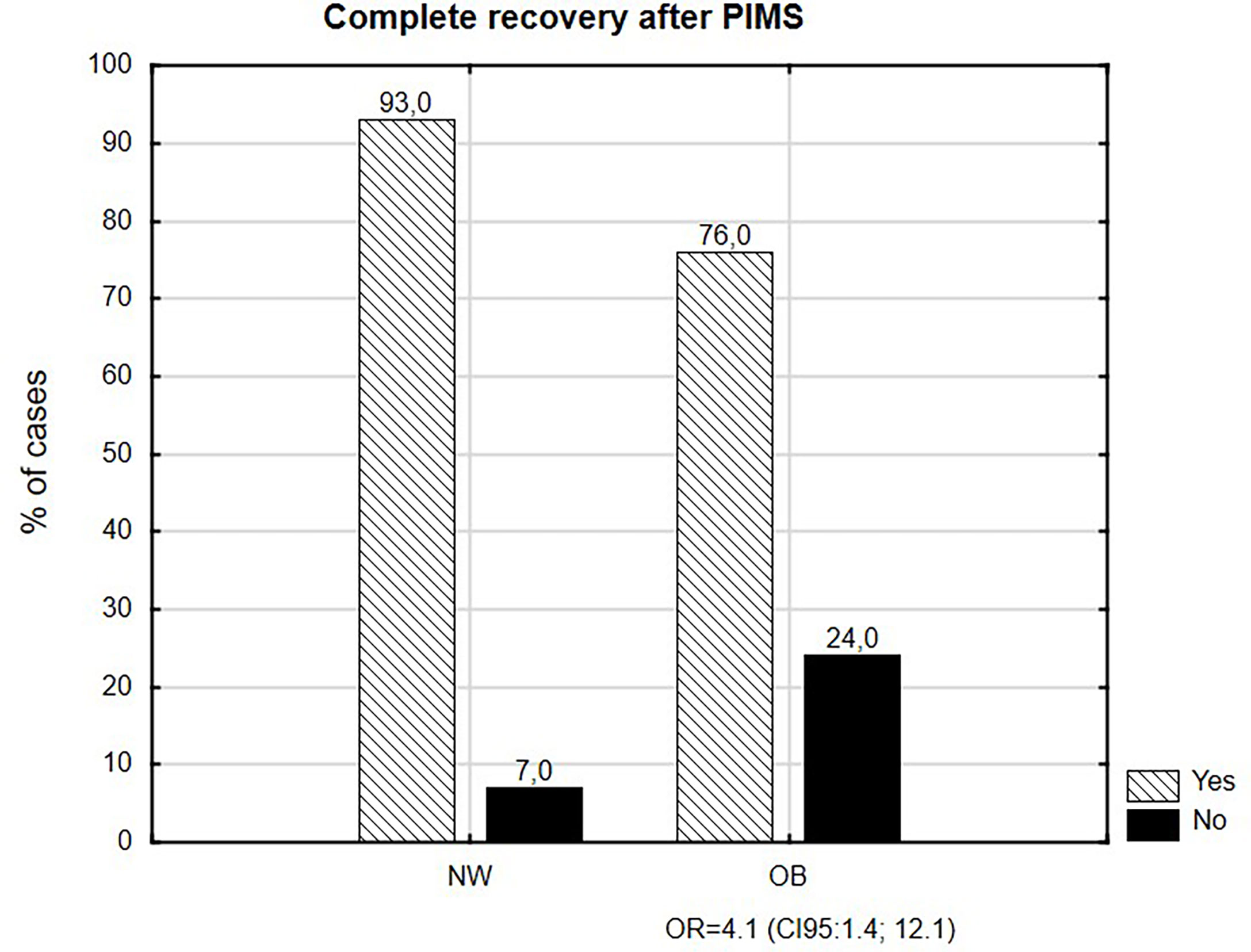
Figure 2 Complete recovery after PIMS.
Discussion
Pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV2, known as multisystem inflammatory syndrome in children (PIMS-TS/MIS-C), is a rare disorder, sometimes followed by extremely severe conditions and usually occurring in previously healthy children about 4–8 weeks after the onset of COVID-19 infection. According to available publications, obesity and its comorbidities have influence on the severity of COVID-19 infection among adult and pediatric populations (5, 17, 18, 26, 27) and might also be a risk factor for death, next to immunosupression, diabetes mellitus, chronic lung disease, and cardiac and neurological disorders (5). Possible pathways explaining this connection, such as overexpression of angiotensin 2 and increased production of inflammatory cytokines such as TNF-α, IL-1, and IL-6 by adipose tissue, are still not confirmed (27, 28).
In our article, we have analyzed the impact of obesity and overweightedness among Polish children on the severity and final outcome of PIMS-TS/MIS-C.
Studies from other countries mainly focused on describing the frequency of overweightedness and obesity among MIS-C/PIMS-TS populations (29–32). A systematic review in the US revealed a 50.8% rate of overweight or obese patients (vs. 25.1% in our study) among children with comorbidities, and indicated a need for further research among that group (30). Another study described the percentage of obesity to be higher, compared to our results (up to 26% vs. 9.1%) (29, 33). The lower prevalence might be a consequence of the demographic characteristic of Polish children. Depending on age and gender, the obesity rate in Polish adolescents and children is 13–14% (34). Secondly, the databases used were relatively wide-ranging (n=662, n=1080 patients included vs. n=306 in our research) and outlined the ethnic diversity among patients, such as a high prevalence of Hispanic and non-Hispanic black patients in contrast to the representation of Caucasian children in a homogeneous Polish population (20, 21, 29, 30, 33).
Moving to the laboratory results in our study group (OB/OV), we noticed the significant increase of transaminases (AlAT, GGT), which might be explained by liver diseases/non-alcoholic fatty liver disease (NAFLD) spectrum in children with obesity. On the other hand, there was no essential increase in inflammatory assays to support a hypothesis of chronic hepatitis.
Interestingly, the level of IL-6 differed significantly between groups (324 pg/ml for NWs vs. 80.3 pg/ml in OV and 195 pg/ml in OB). The level of interleukin 6, according to available research, increases both in MIS-C and obesity (4, 12, 27, 35). Because of that, we assumed multiplied elevation of IL-6, but our result was opposite to the hypothetical model. In this context, the mechanism of IL-6 elevation as well as higher maximal values of BNP in the control group with normal weight remained unknown and required further studies.
Moving forward in reference to a US surveillance study, obesity (up to 39% vs. 9.1% in obesity and 6.0% vs. 16.0% in overweightedness) was linked to decreased cardiac function (31), contrary to our findings that did not confirm a difference between the study and control groups in cases of cardiovascular abnormalities, including decreased left ventricular ejection fraction. This might be explained by a tendency toward a milder course of the disease in our population (20, 21); however, it demands further investigation.
The administration of intravenous immunoglobulins, steroids, heparin, and acetylsalicylic acid did not differ between groups and was similar to other studies (29, 30, 33) as well as the length of hospitalization. The tendency to a more frequent use of oxygen therapy was noticed in the groups with overweightedness and obesity.
Multicenter MOIS-CoR database analysis confirmed that obesity was less commonly predisposed to a complete recovery at the time of discharge after MIS-C diagnosis, compared to normal-weight patients (76% vs. 93%). Our findings showed that obesity increased the risk of incomplete recovery at the time of discharge by four times. To our best knowledge, this is the first report of an increased risk of incomplete recovery connected with a body mass index above the 95th percentile. This might suggest a tendency to worsen the course of MIS-C. To understand our findings, we need to continue and expand surveillance.
Study limitations
Although the MOIS-CoR project was created by a multicenter group of pediatric specialists, and the acquisition of the database was standardized, not all the data were collected from all the patients. Moreover, some patients were transferred between centers from low to high referentiality, and because of that, some parameters at admission might not reflect the values at the beginning of the disease. Lastly, the analyzed data, ‘recovery at the time of discharge’, depend on the subjective opinion of the pediatric specialist and/or lack of cardiac complications.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
This study was reviewed and approved by the Bioethics Committee at the Wrocław Medical University Poland (CWN UMW BW: 313/2020). All research was performed in accordance with relevant guidelines and regulations. The Bioethics Committee at Wroclaw Medical University granted waiver of informed consent, as only de-identified data were transmitted and analyzed.
Author contributions
Conceptualization: AG, EB-S, IC, and AM; methodology: AG, ML, EB-S, and IC; validation: AG and EB-S; formal analysis: AG and ML; investigation and resources: EB-S, MF-P, LSzy, KL, MO-N, ND, KP, AAn, AAf, CS-G, MK, EK, LSze, TJ, JP, and AM; data curation: AG; writing: original draft preparation, AG, EB-S, IC, and ML; visualization, ML and IC; supervision, AG and EB-S; project administration, AG. All authors approved the submitted version.
Funding
The costs of publication were sponsored by the Polish Paediatric Society.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Riphagen S, Gomez X, Gonzalez-Martinez C, Wilkinson N, Theocharis P. Hyperinflammatory shock in children during COVID-19 pandemic. In: , vol. 39510237) . London, England: Lancet (2020). p. 1607–8. doi: 10.1016/S0140-6736(20)31094-1
2. Health Policy Team. Guidance–paediatric multisystem inflammatory syndrome temporally associated with COVID-19. London, UK: Royal College of Paediatrics and Child Health. Available at: https://www.rcpch.ac.uk/resources/guidance-paediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19.
3. World Health Organization (WHO). Multisystem inflammatory syndrome in children and adolescents temporally related to COVID-19. Available at: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (Accessed May 15, 2020).
4. Centers for Disease Control and Prevention (CDC). Information for healthcare providers about multisystem inflammatory syndrome in children (MIS-c). Atlanta, GA, USA: CDC. Available at: https://www.cdc.gov/mis-c/hcp/.
5. McCormick DW, Richardson LC, Young PR, Viens LJ, Gould CV, Kimball A, et al. Deaths in children and adolescents associated with COVID-19 and MIS-c in the united states. Pediatrics (2021) 148(5):e2021052273. doi: 10.1542/peds.2021-052273
6. Davies P, Evans C, Kanthimathinathan HK, Lillie J, Brierley J, Waters G, et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health (2020) 4(9):669–77. doi: 10.1016/S2352-4642(20)30215-7
7. McCrindle BW, Rowley AH, Newburger JW, Burns JC, Bolger AF, Gewitz M, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American heart association. Circulation (2017) 135(17):e927–99. doi: 10.1161/CIR.0000000000000484
8. Pouletty M, Borocco C, Ouldali N, Caseris M, Basmaci R, Lachaume N, et al. Paediatric multisystem inflammatory syndrome temporally associated with SARS-CoV-2 mimicking Kawasaki disease (Kawa-COVID-19): a multicentre cohort. Ann rheumatic Dis (2020) 79(8):999–1006. doi: 10.1136/annrheumdis-2020-217960
9. Centers for Disease Control and Prevention (CDC). Streptococcal toxic shock syndrome (STSS) (Streptococcus pyogenes) 2010 case definition. Atlanta, GA, USA: CDC. Available at: https://ndc.services.cdc.gov/case-definitions/streptococcal-toxic-shock-syndrome-2010/.
10. Centers for Disease Control and Prevention (CDC). Toxic shock syndrome (Other than streptococcal) (TSS) 2011 case definition. Atlanta, GA, USA: CDC. Available at: https://wwwn.cdc.gov/nndss/conditions/toxic-shock-syndrome-other-than-streptococcal/case-definition/2011/.
11. Minoia F, Bovis F, Davì S, Horne A, Fischbach M, Frosch M, et al. Development and initial validation of the MS score for diagnosis of macrophage activation syndrome in systemic juvenile idiopathic arthritis. Ann rheumatic Dis (2019) 78(10):1357–62. doi: 10.1136/annrheumdis2019-215211
12. Gregor MF, Hotamisligil GS. Inflammatory mechanisms in obesity. Annu Rev Immunol (2011) 29:415–45. doi: 10.1146/annurev-immunol-031210-101322
13. Rodríguez-Hernández H, Simental-Mendía LE, Rodríguez-Ramírez G, Reyes-Romero MA. Obesity and inflammation: epidemiology, risk factors, and markers of inflammation. Int J Endocrinol (2013) 2013):678159. doi: 10.1155/2013/678159
14. Mraz M, Haluzik M. The role of adipose tissue immune cells in obesity and low-grade inflammation. J Endocrinol (2014) 222(3):R113–27. doi: 10.1530/JOE-14-0283
15. Ryan PM, Caplice NM. Is adipose tissue a reservoir for viral spread, immune activation, and cytokine amplification in coronavirus disease 2019? Obesity (2020) 28(7):1191–4. doi: 10.1002/oby.22843
16. De Groot CJ, Poitou Bernert C, Coupaye M, et al. Clinical management of patients with genetic obesity during COVID-19 pandemic: position paper of the ESE growth & genetic obesity COVID-19 study group and rare endo-ERN main thematic group on growth and obesity. Endocrine (2021) 71(3):653–62. doi: 10.1007/s12020-021-02619-y
17. Kass DA, Duggal P, Cingolani O. Obesity could shift severe COVID-19 disease to younger ages. Lancet (2020) 395(10236):1544–5. doi: 10.1016/S0140-6736(20)31024-2
18. Zachariah P, Johnson CL, Halabi KC, Ahn D, Sen AI, Fischer A, et al. Epidemiology, clinical features, and disease severity in patients with coronavirus disease 2019 (COVID-19) in a children's hospital in new York city, new York. JAMA Pediatr (2020) 174(10):e202430. doi: 10.1001/jamapediatrics.2020.2430
19. Tsankov BK, Allaire JM, Irvine MA, Lopez AA, Sauvé LJ, Vallance BA, et al. Severe COVID-19 infection and pediatric comorbidities: A systematic review and meta-analysis. Int J Infect Dis IJID Off Publ Int Soc Infect Dis (2021) 103:246–56. doi: 10.1016/j.ijid.2020.11.163
20. Ludwikowska KM, Okarska-Napierala M, Dudek N, Tracewski P, Kusa J, Piwonski KP, et al. Distinct characteristics of multisystem inflammatory syndrome in children in Poland. Sci Rep (2021) 11(1):23562. doi: 10.1038/s41598-021-02669-2
21. Okarska-Napierala M, Ludwikowska KM, Szenborn L, Dudek N, Mania A, Buda P, et al. Pediatric inflammatory multisystem syndrome (PIMS) did occur in Poland during months with low COVID-19 prevalence, preliminary results of a nationwide register. J Clin Med (2020) 9(11):3386. doi: 10.3390/jcm9113386
22. Body-mass index (BMI), converted into z-scores based on the WHO reference standards. Available at: https://www.who.int/toolkits/child-growth-standards/standards/body-mass-index-for-age-bmi-for-age.
23. Palczewska I, Nieźwiecka Z. Wskaźniki rozwoju somatycznego dzieci i młodzieży warszawskiej. Medycyna Wieku Rozwojowego (2001) 5(supl. 1):52, 113–114.
24. Boston Children's hospital z-score calculator. Available at: https://zscore.chboston.org/.
25. Schwartz GJ, Haycock GB, Edelmann CM Jr, Spitzer A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics. (1976) 58(2):259–63.
26. Tartof SY, Qian L, Hong V, Wei R, Nadjafi RF, Fischer H, et al. Obesity and mortality among patients diagnosed with COVID-19: Results from an integrated health care organization. Ann Internal Med (2020) 173(10):773–81. doi: 10.7326/M20-3742
27. Petrakis D, Margina D, Tsarouhas K, Tekos F, Stan M, Nikitovic D, et al. Obesity - a risk factor for increased COVID-19 prevalence, severity and lethality (Review). Mol Med Rep (2020) 22(1):9–19. doi: 10.3892/mmr.2020.11127
28. Physician information on childhood obesity in relation to COVID-19. Available at: https://www.eurospe.org/media/2311/espe-physicians-information-on-covid-19-and-obesity.pdf.
29. Abrams JY, Oster ME, Godfred-Cato SE, Bryant B, Datta SD, Campbell AP, et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-c) in the USA: a retrospective surveillance study. Lancet Child Adolesc Health (2021) 5(5):323–31. doi: 10.1016/S2352-4642(21)00050-X
30. Ahmed M, Advani S, Moreira A, Zoretic S, Martinez J, Chorath K, et al. Multisystem inflammatory syndrome in children: A systematic review. EClinicalMedicine (2020) 26:100527. doi: 10.1016/j.eclinm.2020.100527
31. Capone CA, Subramony A, Sweberg T, Schneider J, Shah S, Rubin L, et al. Characteristics, cardiac involvement, and outcomes of multisystem inflammatory syndrome of childhood associated with severe acute respiratory syndrome coronavirus 2 infection. J Pediatr (2020) 224:141–5. doi: 10.1016/j.jpeds.2020.06.044
32. Yasuhara J, Watanabe K, Takagi H, Sumitomo N, Kuno T. COVID-19 and multisystem inflammatory syndrome in children: A systematic review and meta-analysis. Pediatr pulmonology (2021) 56(5):837–48. doi: 10.1002/ppul.25245
33. Bautista-Rodriguez C, Sanchez-de-Toledo J, Clark BC, Herberg J, Bajolle F, Randanne PC, et al. Multisystem inflammatory syndrome in children: An international survey. Pediatrics (2021) 147(2):e2020024554. doi: 10.1542/peds.2020-024554
34. Kulaga Z, Grajda A, Gurzkowska B, Wojtylo MA, Gózdz M, Litwin MS. The prevalence of overweight and obesity among polish school- aged children and adolescents. Przegl Epidemiol. (2016) 70(4):641–51.
Keywords: obesity, childhood obesity, COVID-19, MIS-C, PIMS
Citation: Gawlik AM, Berdej-Szczot E, Chmiel I, Lorek M, Antosz A, Firek-Pędras M, Szydłowski L, Ludwikowska KM, Okarska-Napierała M, Dudek N, Piwoński K, Afelt A, Suski-Grabowski C, Kursa MB, Kuchar E, Szenborn L, Jackowska T, Peregud-Pogorzelski J and Mazur A (2022) A tendency to worse course of multisystem inflammatory syndrome in children with obesity: MultiOrgan Inflammatory Syndromes COVID-19 related study. Front. Endocrinol. 13:934373. doi: 10.3389/fendo.2022.934373
Received: 02 May 2022; Accepted: 03 August 2022;
Published: 26 September 2022.
Edited by:
Luca Busetto, Università degli Studi di Padova, ItalyReviewed by:
Beata Ewa Pyrżak, Medical University of Warsaw, PolandThomas Pixner, Salzkammergut Klinikum Vöcklabruck, Austria
Copyright © 2022 Gawlik, Berdej-Szczot, Chmiel, Lorek, Antosz, Firek-Pędras, Szydłowski, Ludwikowska, Okarska-Napierała, Dudek, Piwoński, Afelt, Suski-Grabowski, Kursa, Kuchar, Szenborn, Jackowska, Peregud-Pogorzelski and Mazur. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aneta Monika Gawlik, YWdhd2xpa0BtcC5wbA==; YWdhd2xpa0BzdW0uZWR1LnBs