 Joan Gil1,2,3†
Joan Gil1,2,3† Montserrat Marques-Pamies1,4†
Montserrat Marques-Pamies1,4† Elena Valassi1,2,3Guillermo Serra5Isabel Salinas6Gemma Xifra7
Elena Valassi1,2,3Guillermo Serra5Isabel Salinas6Gemma Xifra7 Paula Casano-Sancho8
Paula Casano-Sancho8 Cristina Carrato9
Cristina Carrato9 Betina Biagetti10
Betina Biagetti10 Gemma Sesmilo11Jennifer Marcos-Ruiz1Helena Rodriguez-Lloveras1Anna Rueda-Pujol1Anna Aulinas2,3Alberto Blanco12Cristina Hostalot12Andreu Simó-Servat13
Gemma Sesmilo11Jennifer Marcos-Ruiz1Helena Rodriguez-Lloveras1Anna Rueda-Pujol1Anna Aulinas2,3Alberto Blanco12Cristina Hostalot12Andreu Simó-Servat13 Fernando Muñoz14Marta Rico14Javier Ibáñez-Domínguez15Esteban Cordero16
Fernando Muñoz14Marta Rico14Javier Ibáñez-Domínguez15Esteban Cordero16 Susan M. Webb2,3
Susan M. Webb2,3 Mireia Jordà1Manel Puig-Domingo1,3,4*
Mireia Jordà1Manel Puig-Domingo1,3,4*- 1Endocrine Research Unit, Germans Trias i Pujol Research Institute (IGTP), Badalona, Spain
- 2Department of Endocrinology, Research Center for Pituitary Diseases, Hospital Sant Pau, IIB-SPau, Department of Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain
- 3Centro de Investigación en Red de Enfermedades Raras, CIBERER, Unit 747, Instituto de Salud Carlos III, Madrid, Spain
- 4Department of Endocrinology, Hospital Municipal de Badalona, Badalona, Catalonia, Spain
- 5Department of Endocrinology, Son Espases University Hospital, Palma de Mallorca, Spain
- 6Department of Endocrinology and Nutrition, Germans Trias i Pujol University Hospital, Badalona, Spain
- 7Department of Endocrinology, Josep Trueta University Hospital, Girona, Spain
- 8Centro de Investigación en Red de Diabetes y Enfermedades Metabólicas Asociadas (CIBERDEM), Pediatric Endocrinology Unit, Institut de Recerca SJS 39-57, Hospital Sant Joan de Déu, University of Barcelona, Esplugues, Spain
- 9Department of Pathology, Germans Trias i Pujol University Hospital, Badalona, Spain
- 10Department of Endocrinology, University Hospital Vall d’Hebron, Barcelona, Spain
- 11Department of Endocrinology, Dexeus University Hospital, Barcelona, Spain
- 12Department of Neurosurgery, Germans Trias i Pujol University Hospital, Badalona, Spain
- 13Department of Endocrinology, Hospital Universitari Mútua de Terrassa, Terrassa, Spain
- 14Department of Neurosurgery, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
- 15Department of Neurosurgery, Son Espases University Hospital, Palma de Mallorca, Spain
- 16Department of Neurosurgery, University Hospital Vall d’Hebron, Barcelona, Spain
Introduction: Different medical therapies have been developed for pituitary adenomas. However, Non-Functioning Pituitary Neuroendocrine Tumors (NF-PitNET) have shown little response to them. Furthermore, epithelial-mesenchymal transition (EMT) has been linked to resistance to medical treatment in a significant number of tumors, including pituitary adenomas.
Methods: We aimed to evaluate the expression of EMT-related markers in 72 NF-PitNET and 16 non-tumoral pituitaries. To further explore the potential usefulness of medical treatment for NF-PitNET we assessed the expression of somatostatin receptors and dopamine-associated genes.
Results: We found that SNAI1, SNAI2, Vimentin, KLK10, PEBP1, Ki-67 and SSTR2 were associated with invasive NF-PitNET. Furthermore, we found that the EMT phenomenon was more common in NF-PitNET than in GH-secreting pituitary tumors. Interestingly, PEBP1 was overexpressed in recurrent NF-PitNET, and could predict growth recurrence with 100% sensitivity but only 43% specificity. In parallel with previously reported studies, SSTR3 is highly expressed in our NF-PitNET cohort. However, SSTR3 expression is highly heterogeneous among the different histological variants of NF-PitNET with very low levels in silent corticotroph adenomas.
Conclusion: NF-PitNET showed an enhanced EMT phenomenon. SSTR3 targeting could be a good therapeutic candidate in NF-PitNET except for silent corticotroph adenomas, which express very low levels of this receptor. In addition, PEBP1 could be an informative biomarker of tumor regrowth, useful for predictive medicine in NF-PitNET.
1 Introduction
Non-Functioning Pituitary Neuroendocrine Tumors (NF-PitNET) are defined as pituitary tumors that do not secrete biologically active hormones depicting specific hormonal symptoms. These neoplasms are the most common pituitary tumors in humans and when they come to medical attention, it is usually due to a mass effect and/or hypopituitarism (1–3). Histologically, NF-PitNET comprise a heterogeneous group of tumors arising from different pituitary cell lineages (4). The new WHO Classification of Pituitary Tumors 2022 divides NF-PitNET according to the cell of origin; however, it does not contain specific molecular information linked to treatment response prediction (5–7).
Nowadays, transsphenoidal surgery is the first-line treatment for most of these patients, whereas medical therapy -mostly temozolomide in aggressive tumors- and irradiation are reserved for patients that are not good surgical candidates or that have undergone unsuccessful surgery (5, 8). The recurrence rate of NF-PitNET in patients who underwent complete surgical resection is 20-25% at 10 years, while it rises up to 50-60% in case of partial removal (9, 10).
Therefore, there is a need to identify molecular targets in NF-PitNETs that clarify their biological behavior leading to the development of a more specific medical treatment. The current available targeted medical treatments for pituitary tumors are first and second generation somatostatin receptor ligands (SRLs), dopamine receptor D2 agonists (DA) and the alkylating agent temozolomide, usually reserved for very aggressive tumors (11, 12). Tumor shrinkage during therapy with either DA or SRLs has been previously reported in a variable percentage of NF-PitNET cases; however, response of NF-PitNET to medical treatment is still considered poor, insufficiently understood and nowadays unpredictable. Tumor reduction has only been observed in 12% of patients after octreotide treatment and in 28% of patients treated with DA therapy (13). Some authors suggested that SRLs treatment in NF-PitNET could only be useful for the stabilization of tumor growth without any significant effect on tumor shrinkage (14). Other authors have provided evidence favoring DA use when there is post-surgical residual tumor (15), independently of any other characteristic of the case.
Epithelial–mesenchymal transition (EMT) is a process that restructures the cell from an epithelial to a mesenchymal phenotype driven by a network of transcription factors (16). This process produces changes in post-translational regulation mechanisms and gene expression, leading to the loss of cell polarity and epithelial characteristics and the acquisition of increased migratory and invasive properties. EMT is not a binary process, and distinct intermediate cellular states have been reported (17). Epithelial-Mesenchymal Transition (EMT) has been linked to both the clinical course of NF-PitNET (18, 19) and resistance to medical therapy in pituitary tumors (20–23). Despite not being fully understood, several mechanisms have been described to explain the association of EMT and the lack of response to therapy in PitNETs. It has been proposed that EMT could disrupt alternative splicing in GH-secreting tumors (21) and that this is associated with a lack of response to somatostatin receptor ligands (23, 24). Another possible explanation is the involvement of the cytoskeleton, in particular, the actin binding protein filamin A that regulates localization, expression and signaling of SSTR2 and DRD2 in some PitNETs (25–29). Moreover, β-Arrestin 2 mediates the downstream effects of DRD2 in NF-PitNETs (30). The aim of our study is to elucidate the molecular landscape of NF-PitNETs for EMT-associated genes and genes related to the response to medical therapy with SRLs and DAs.
2 Materials and methods
2.1 Patients
This retrospective study enrolled 72 adult patients with NF-PitNET from 26 tertiary centers from all over Spain who underwent pituitary surgery and had tissue availability from 2014 to 2020. NF-PitNET was diagnosed by magnetic resonance image (MRI) of the sella turcica with a tumor visualized, in the absence of symptoms suggesting hormone hypersecretion and a biochemical confirmation of normal or hyposecretion of pituitary hormones. All tumors underwent surgical treatment. Furthermore, the pathologist selected a surplus of tumor to be embedded in RNAlater (Invitrogen, Carlsbad, CA, USA) for research purposes. All the tumors were naïve to medical treatment and radiotherapy. NF-PitNET invasiveness and size were established according to the preoperative MRI following the conceptual classification by Raverot (31). Tumor recurrence was considered when a new tumor image was detected in patients with no apparent postsurgical remnants or when a regrowth of a known remnant tumor was of sufficient clinical entity that required a second surgical intervention. The minimum surveillance time for considering a recurrence was 2 years, with a median of 5.32 ± 2.05 years for a total number of 58 patients. The clinical and neuropathogical characteristics of the cohort are described in Table 1. Sixteen non-tumoral pituitary samples from autopsies (8 samples) and organ donors (8 samples) were also analyzed as a non-pathological condition reference (mean age: 62.4 years ± 10.9; 37.5% females).
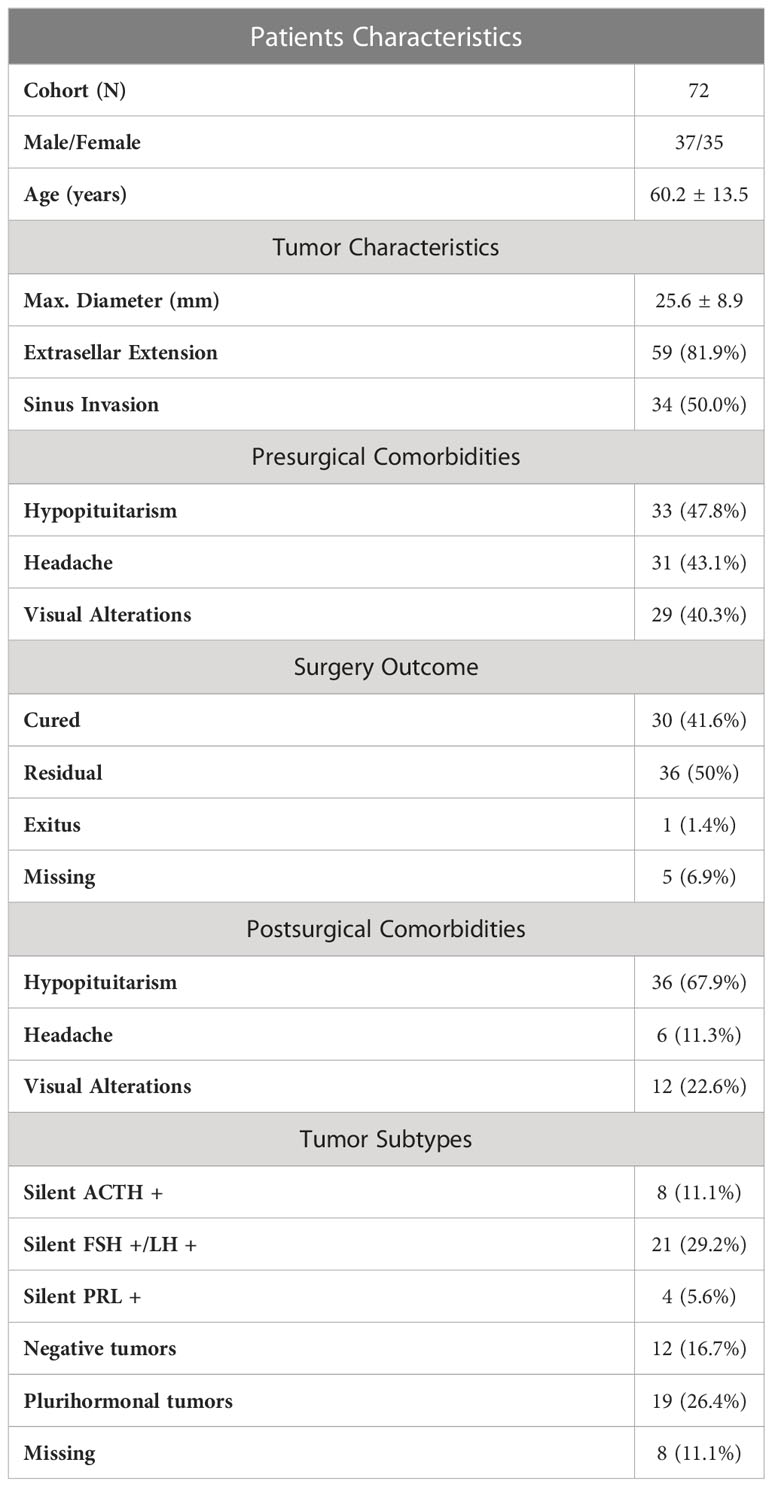
Table 1 Description of the cohort.
The molecular data of the GH-secreting adenomas used was obtained from our previous paper where the cohort is fully described (23). Briefly, a total of 57 (32 women) acromegaly patients from the REMAH cohort who underwent pituitary surgery and had tissue availability was used. Mean age was 45.74 ± 12.35, 82% of the tumors were macroadenomas, 68% presented extrasellar extension, with a mean tumor diameter of 19.49 ± 10.03.
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and implemented and reported in accordance with the International Conference on Harmonized Tripartite Guideline for Good Clinical Practice. The study was approved by the Germans Trias i Pujol Hospital Ethical Committee for Clinical Research (Ref.: EO-11-080 http://www.ceicgermanstrias.cat/index.html). The protocol and informed consent forms were approved by the institutional review board of the participating centers, independent ethics committee, and/or research ethics board of each study site. All patients provided written informed consent to participate in the study.
2.2 Immunohistochemical analysis
Formalin-fixed paraffin-embedded tumor samples were used for anterior pituitary hormone expression assessment. Growth hormone (GH), prolactin (PRL), thyroid-stimulating hormone (TSH), adrenocorticotropic hormone (ACTH), luteinizing hormone (LH) and follicle-stimulating hormone (FSH) expression were all tested with the corresponding antibodies, following local protocols for diagnostic assessment. Hematoxylin-eosin and reticulin staining, as well as cytokeratin, Ki-67, α-subunit and p53 immunolabeling, were also carried out in most of the cases as part of the standard pathological evaluation. Plurihormonal tumors were defined as tumors that showed immunoreactivity for more than one hormone that cannot be explained by normal cytophysiology or developmental mechanisms. We considered negative tumors those that did not express positivity for any of the hormones.
2.3 RNA isolation and reverse transcription
Representative fragments of the fresh tumor were selected by a pathologist and embedded in RNAlater (Invitrogen, Carlsbad, CA, USA) for 24 h, after which the samples were frozen at −80°C. Total RNA was isolated from pituitary adenomas using AllPrep DNA/RNA/miRNA Universal Kit (Qiagen, Hilden, Germany). We removed contaminating genomic DNA from RNA by treating samples with RNAse-free DNAse twice: the first time during the extraction of RNA following the manufacturer’s protocol and the second time, before the retrotranscription, for which ezDNase Enzyme (Invitrogen, Carlsbad, CA, USA) was used. The quantity and purity of DNA and RNA were measured using a NanoDrop™ 1000 spectrophotometer (RRID : SCR_016517, Thermo Fisher Scientific, Waltham, MA, USA). Integrity of the RNA was checked by agarose gel electrophoresis.
Five hundred nanograms of total RNA were reverse transcribed using SuperScript IV reverse transcriptase (Invitrogen, Carlsbad, California, USA), and random hexamers in a final volume of 20 uL according to the manufacturer’s protocol.
2.4 Quantitative polymerase chain reaction
Gene expression was quantified using Taqman assays (Applied Biosystems, Fosters City, California, USA). The genes analyzed were Somatostatin Receptor Subtype 2 (SSTR2, Hs00990356_m1), Somatostatin Receptor Subtype 3 (SSTR3, Hs00265633_s1), Somatostatin Receptor subtype 5 (SSTR5, Hs00990408_s1), short Dopamine Receptor D2 (DRD2) Isoform (Hs01014210_m1), long DRD2 Isoform (Hs01024460_m1), Arrestin Beta 1 (ARRB1, Hs00930516_m1), Pleiomorphic Adenoma Gene-Like 1 (PLAGL1, Hs00414677_m1), Raf Kinase Inhibitory Protein (RKIP/PEBP1, Hs01110783_g1), E-cadherin (CDH1, Hs01023894_m1), Ki-67 (MKI67, Hs01032443_m1), Ghrelin and Obestatin Prepropeptide (GHRL, Hs01074053_m1), Aryl Hydrocarbon Receptor Interacting Protein (AIP, Hs00610222_m1), Snail Family Transcriptional Repressor 1 (SNAI1, Hs00195591_m1), Snail Family Transcriptional Repressor 2 (SNAI2, Hs00950344_m1), Epithelial Splicing Regulatory Protein 1 (ESRP1, Hs00214472_m1), RAR Related Orphan Receptor C (RORC, Hs01076112_m1), N-Cadherin (CDH2, Hs00983056_m1), Twist Family bHLH Transcription Factor 1 (TWIST1, Hs00361186_m1) and Vimentin (VIM, Hs00958111_m1); furthermore, a custom assay was ordered for Intron 1 Ghrelin In1-GHRL (AJ89KWC). We tested six reference genes to normalize gene expression: Hypoxanthine Phosphoribosyltransferase 1 (HPRT1, Hs99999909_m1), Proteasome 26S Subunit ATPase 4 (PSMC4, Hs00197826_m1), Glucuronidase Beta (GUSB, Hs00939627_m1), TATA-Box Binding Protein (TBP, Hs00427621_m1), Mitochondrial Ribosomal Protein L19 (MRPL19, Hs01040217_m1) and Phosphoglycerate Kinase 1 (PGK1, Hs00943178_g1), and selected the last three reference genes based on their stability in our samples according to Chainy software (available on: http://maplab.imppc.org/chainy/) (32).
Quantitative polymerase chain reactions (qPCR) were carried out in a 7900HT Fast Real-Time PCR System (RRID : SCR_018060; Applied Biosystems, Fosters City, California, USA). We used TaqMan Gene Expression Master Mix (Applied Biosystems, Fosters City, California, USA), and the amplification reactions were performed in triplicate for each sample in a final volume of 10 uL in 384-well plates. To minimize the inter-assay variation, all the genes, including the reference genes, for each sample were analyzed in the same plate. To quantify relative gene expression we calculated a normalization factor for each sample based on the geometric mean of the selected reference genes, according to geNorm (RRID : SCR_006763, https://genorm.cmgg.be/) algorithms (33).
2.5 Statistical analysis
Descriptive results were expressed as mean ± standard deviation. Unsupervised hierarchical clustering was used to investigate the potential identification of patient’s response subgroups, based on their molecular expression profile. Differences between groups were compared using analysis of variance (Student’s t-test, Wilcoxon signed-rank test and Kruskal-Wallis analysis of variance as appropriate). Samples from all groups within an experiment were processed at the same time. The P values were two-sided, and statistical significance was considered when P < 0.05. All statistical analyses were performed using R version 4.2.1 (R Project for Statistical Computing, RRID : SCR_001905). Unsupervised hierarchical clustering was performed using the R package pheatmap (Pretty Heatmaps, https://CRAN.R-project.org/package=pheatmap). The graphical representation was done using package ggplot 2 (RRID : SCR_014601, Whickham https://CRAN.R-project.org/package=ggplot2) and the P values were added using the ggpubr package (‘ggplot2’ Based Publication Ready Plots, https://CRAN.R-project.org/package=ggpubr).
3 Results
3.1 Clinical description of the NF-PitNET cohort
We analyzed 72 patients with NF-PitNETs, 37 men and 35 women. The mean age was 60.3 years ± 13.5 and the mean follow-up was 915.7 ± 696.4 days. During follow-up, 6 patients with tumor remnants presented a recurrence after a mean of 759.8 days and 3 patients without visible remnants after surgery presented a recurrence after a mean of 783 days. Based on MRI, maximal tumor diameter did not show significant differences in tumors with or without extrasellar extension (p=0.22). However, maximal tumor diameter showed differences among tumors with sinus invasion (mean: 28.3 mm) and tumors without (mean: 23.3 mm) (p=0.02). The proportion of patients presenting headache and visual alterations fell after surgery (43.1% to 11.3%, and 40.3% to 22.6%, respectively in intrasellar and extrasellar tumors) while the proportion of patients presenting hypopituitarism increased after surgery (from 47.8% to 67.9%) (Table 1).
3.2 Association of EMT markers with clinical variables in NF-PitNETs
We analyzed the gene expression of different EMT-related markers and their relationship with clinical features of NF-PitNETs (Table 2). We found that SNAI1 and vimentin expression was associated with invasive tumors (p=0.049 and p=0.039, respectively) while E-cadherin expression was associated with non-invasive intrasellar tumors (p=0.047). Moreover, vimentin and SNAI1 overexpression showed an association with tumors presenting, respectively, headache and hypopituitarism before surgery (p=0.050 and p=0.048).
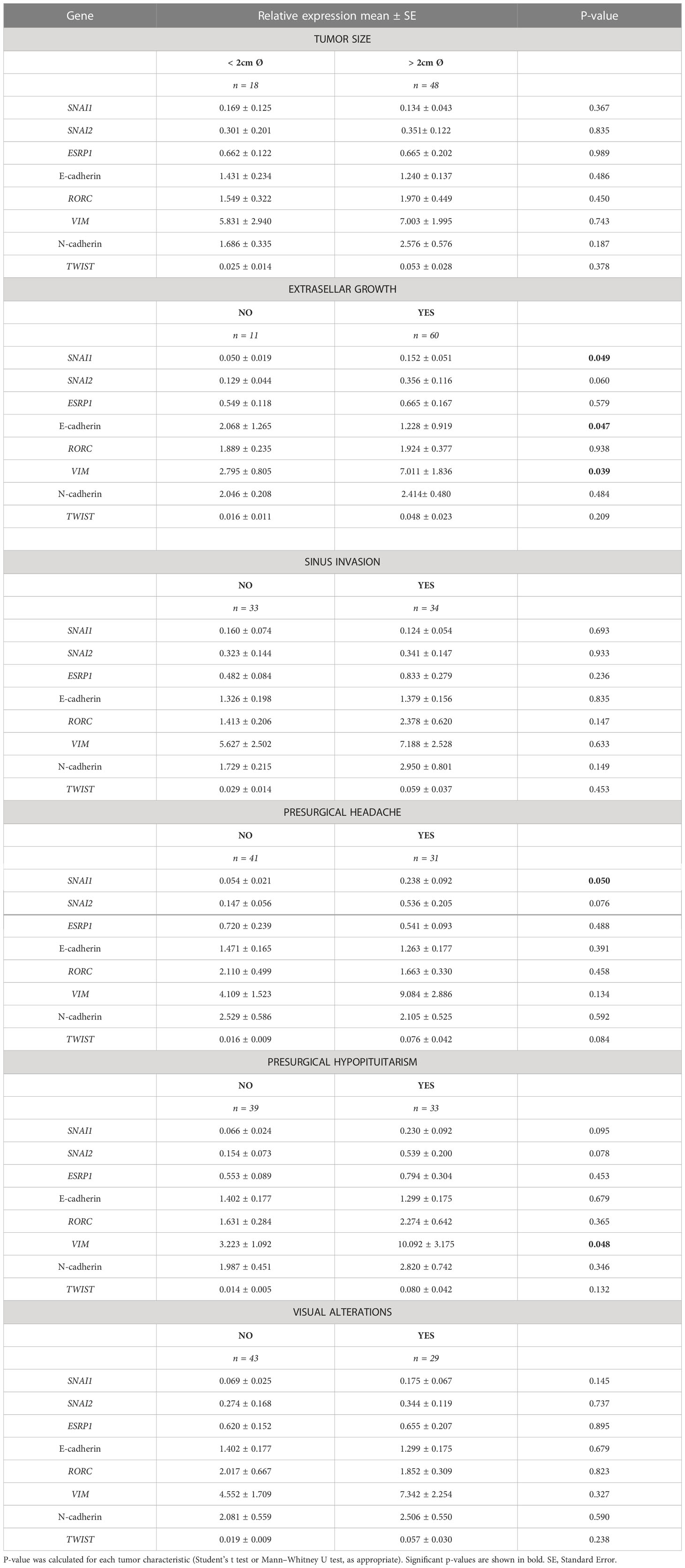
Table 2 Association between the relative expression of each EMT marker and different tumor characteristics.
3.3 NF-PitNETs showed a more mesenchymal expression profile than GH-secreting tumors
We recently reported that most GH-secreting pituitary tumors showed a hybrid and variable EMT expression profile rather than a clear binarial epithelial or mesenchymal phenotype (23). Taking these data into account, we compared the expression of EMT-related markers in GH-secreting tumors, NF-PitNETs and normal pituitaries. Unsupervised hierarchical clustering analysis revealed multiple EMT transition states, with normal pituitaries forming a subcluster associated with high levels of the epithelial marker E-cadherin while NF-PitNETs and GH-secreting tumors were mixed in several different subclusters. Interestingly, a cluster associated with a mesenchymal expression profile was found in 1 GH-secreting adenoma and 6 NF-PitNETs (Figure 1). This result showed that 12.5% of NF-PitNETs harbored an expression profile compatible with an advanced EMT transformation compared to 3.6% of GH-secreting tumors.
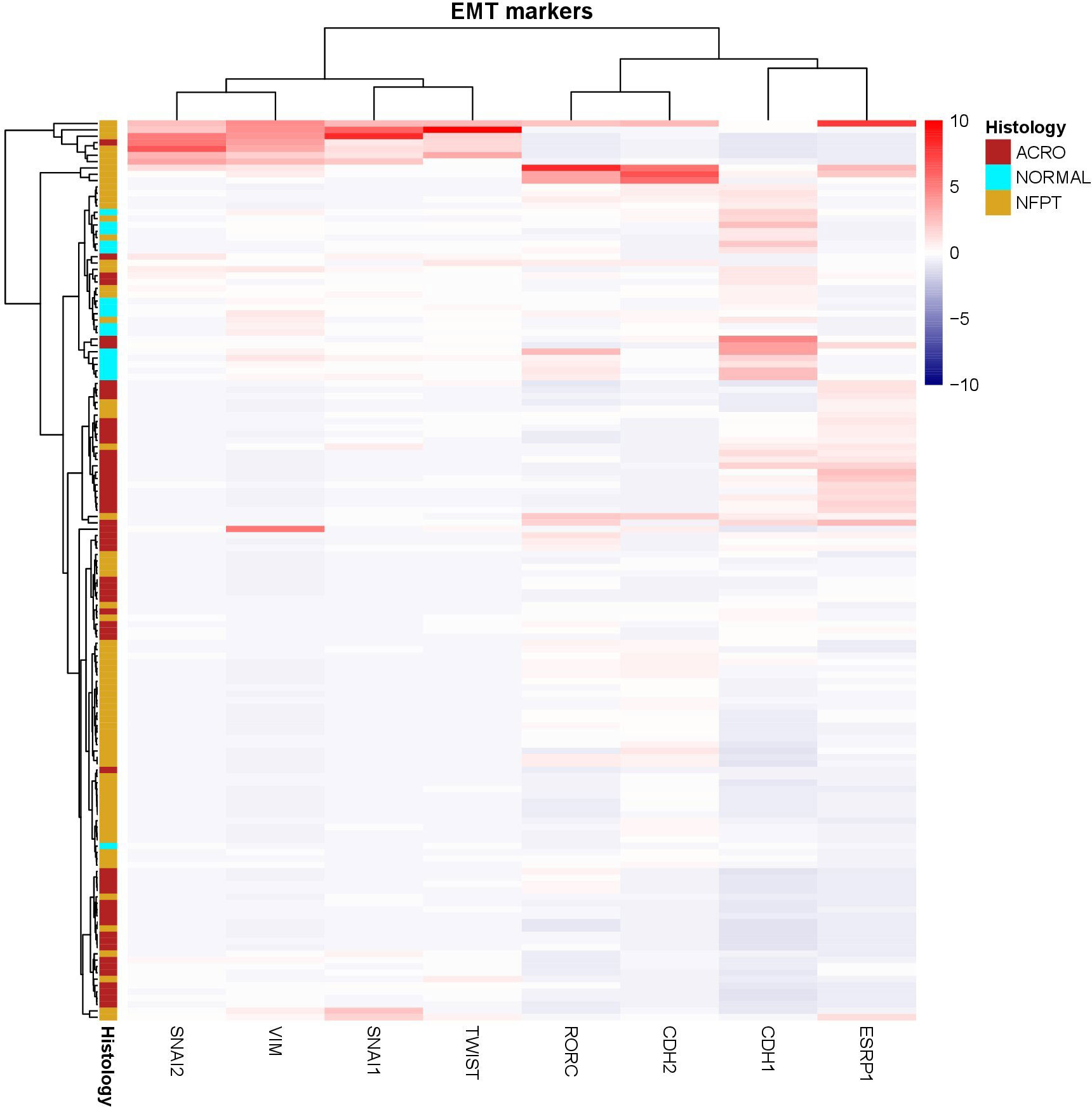
Figure 1 Dendrogram and unsupervised hierarchical clustering heatmap of the EMT-related genes in NF-PitNETs (NFPT), somatotropinomas (ACRO) and healthy pituitary tissue (NORMAL) using Ward’s minimum variance method and Minkowski distance.
3.4 Association of SRLs and dopaminergic response markers with clinical variables in NF-PitNETs: PEBP1 as a predictor of recurrence
We also analyzed the expression of SRLs response biomarkers in NF-PitNETs. In those patients in which clinical information was available, gene expression was correlated with clinical parameters (Table 3). Tumor size showed a negative association with the DRD2 long isoform (Pearson’s r = -0.25, p = 0.05). Extrasellar extension was related to SSTR2, PEBP1, Ki-67 and KLK10 (p = 0.031, p=0.033, p =0.042 and p = 0.008, respectively).
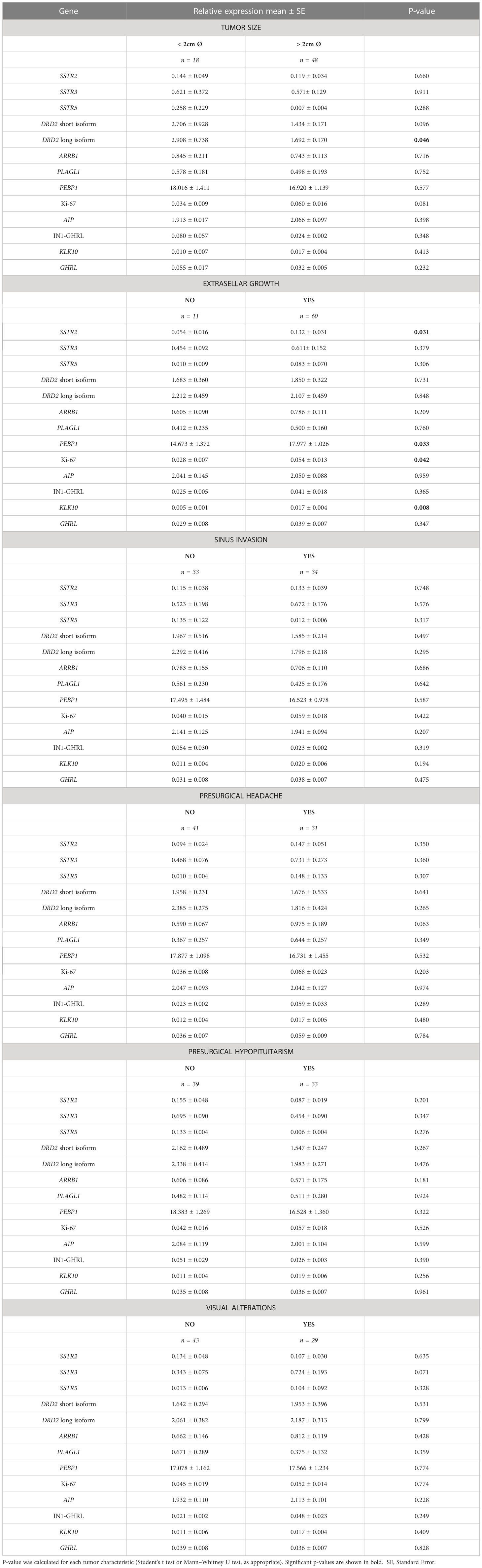
Table 3 Association between the relative expression of each SRLs response marker and different tumor characteristics.
Differences were found also in SRLs biomarkers between NF-PitNETs, GH-secreting pituitary adenomas and non-tumoral pituitaries. GH-secreting tumors showed higher levels of SSTR2 and SSTR5, whereas SSTR3 was more expressed in NF-PitNETs (Figures 2A–C). ARRB1 levels were higher in normal tissue (Figure 2D). On the other hand, NF-PitNETs seem to be characterized by high levels of KLK10 and PLAGL1 (Figures 2E, F). Finally, non-tumoral tissue presented high levels of E-cadherin and DRD2 (Figures 2G–I).
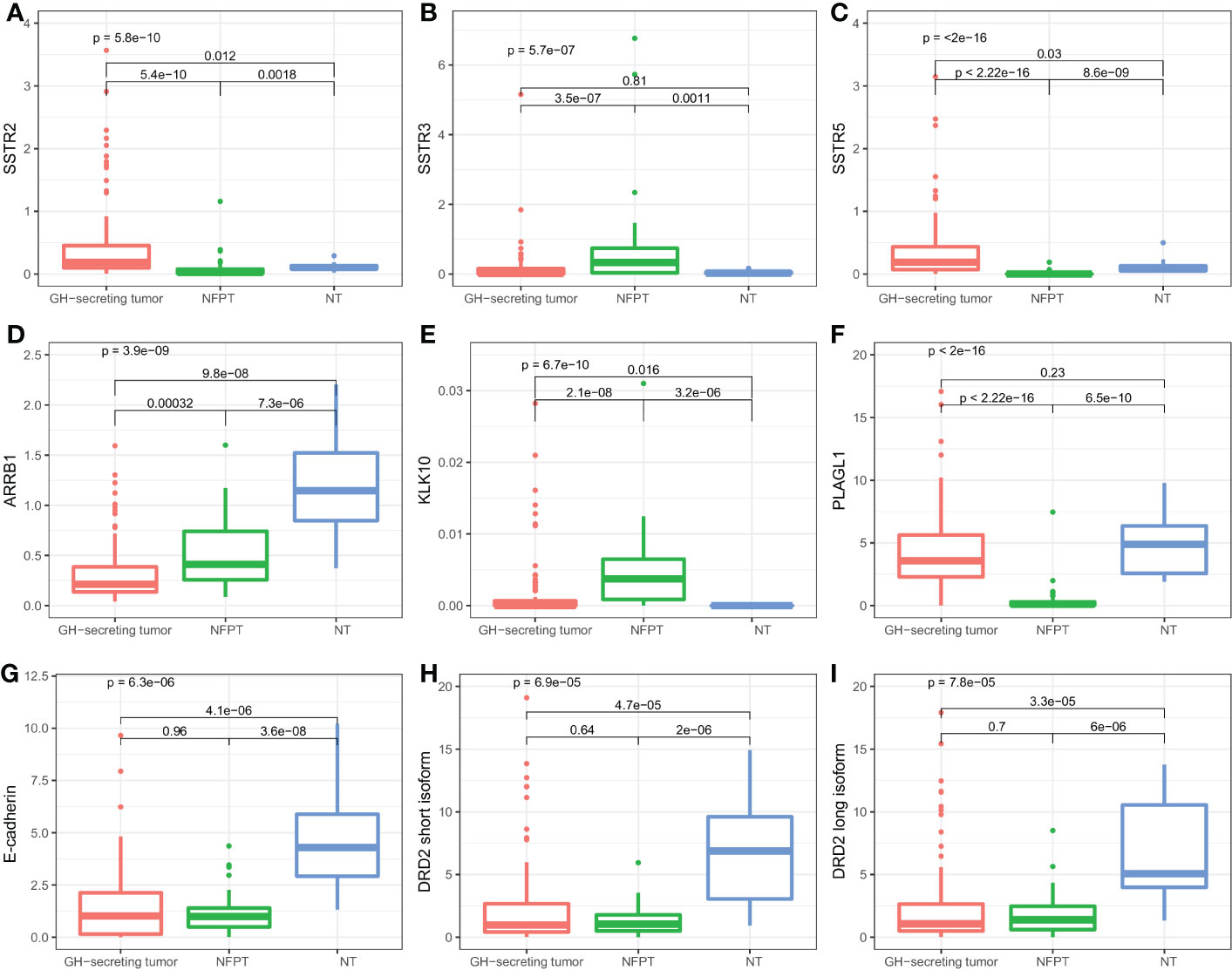
Figure 2 Boxplots of SRL-related genes according to the different histological samples. Relative expression of SSTR2 (A), SSTR3 (B), SSTR5 (C), ARRB1 (D), KLK10 (E), PLAGL1 (F), E-cadherin (G), DRD2 short (H) and long (I) isoform. NT, Normal tissue.
Furthermore, we wanted to investigate if some of these genes could be used to predict patient’s outcome. We investigated the ability of these markers in predicting recurrence in NF-PitNETs (Table 4), and found that only PEBP1 showed a difference between tumors that recurred and tumors that did not (p=0.036) (Figure 3A). When performing a binomial logistic regression, PEBP1 showed an AUC of 69.9%, for a cut-off of 14.0, with a sensitivity of 100% and a specificity of 42.6% (Figure 3B).

Table 4 Association between the relative expression of each gene and the development of a recurrence.
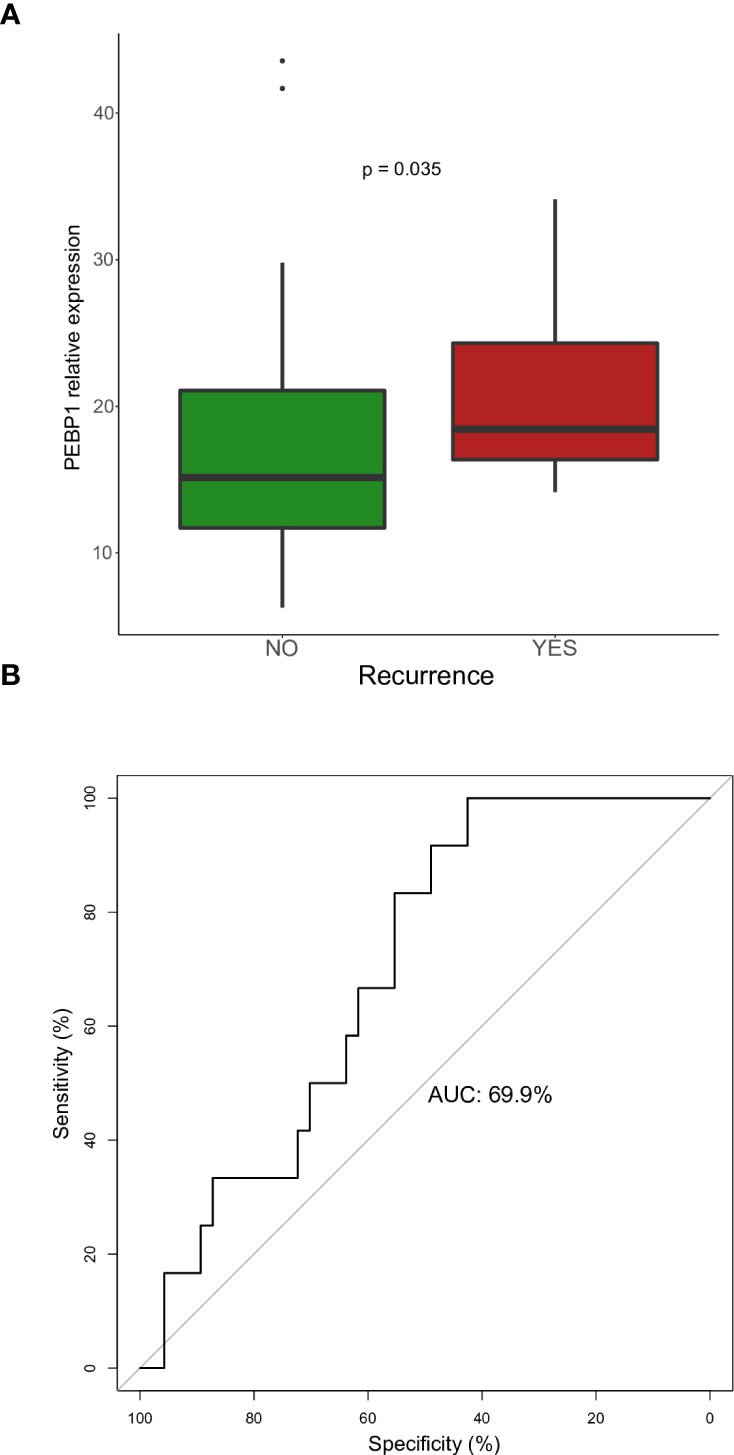
Figure 3 (A) Relative expression of PEBP1 in NF-PitNETs in tumors that recurred vs. tumors that did not. (B) ROC curve for predicting recurrence using ARRB1 expression in NF-PitNETs.
3.5 Relative expression of drug receptors: DRD2 is the most expressed receptor both in GH-secreting tumors and NF-PitNETs
We wanted to compare relative quantities of drug receptor expression in both NF-PitNETs and GH-secreting tumors. In NF-PitNETs the more prevalent receptor was DRD2, followed by SSTR3, while SSTR2 and SSTR5 presented a low expression (Figure 4A). In the case of GH-secreting tumors DRD2 was also the most quantitatively expressed, SSTR2 and SSTR5 were expressed at the same level as the SSTR3 in NF-PitNETs, while SSTR3 showed a very low expression level (Figure 4B).
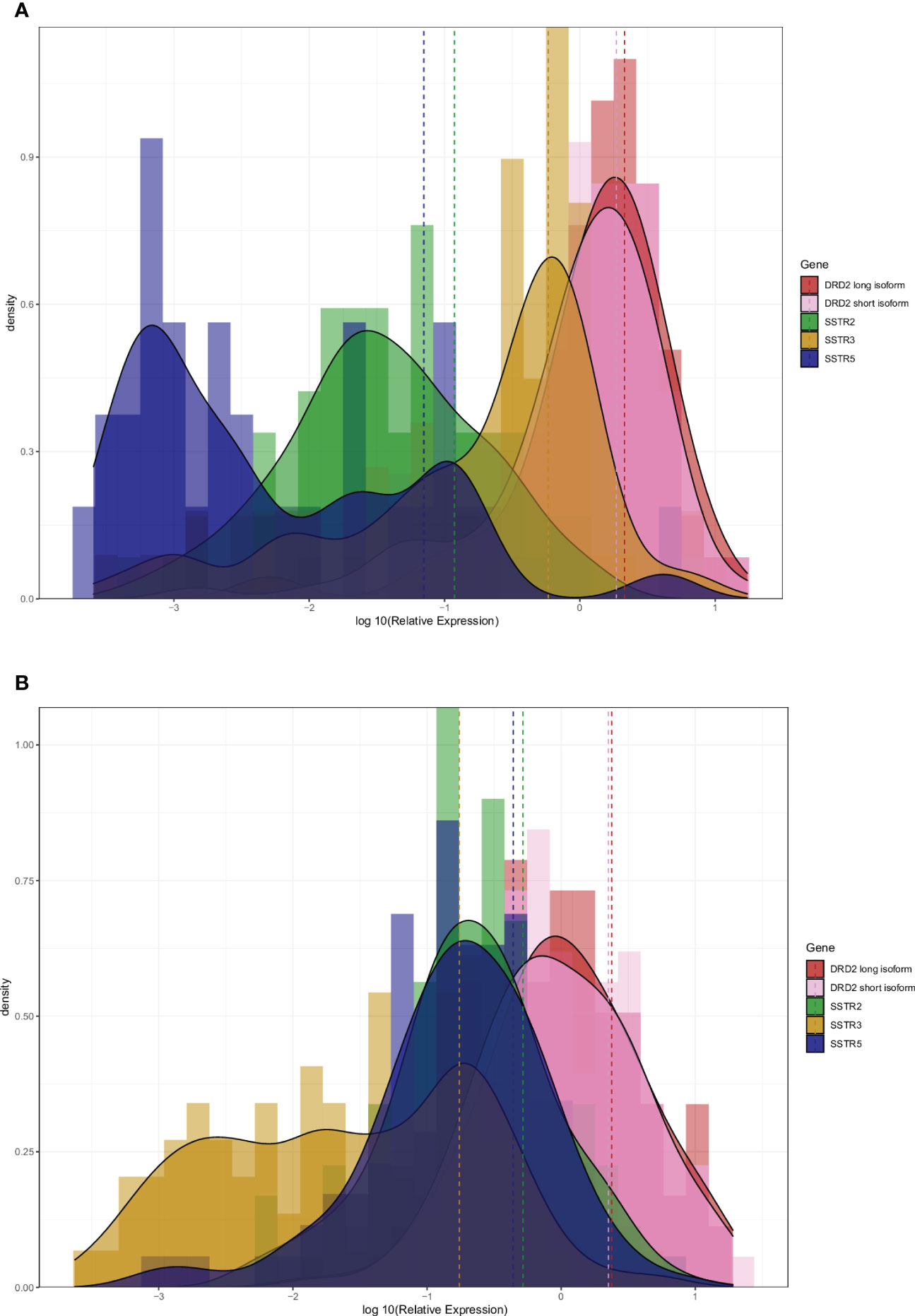
Figure 4 Histogram and density plot of the log10 relative expression of DRD2 long and short isoform, SSTR2, SSTR3 and SSTR5 in NF-PitNETs (A) and GH-secreting pituitary neuroendocrine tumors (B). Dashed line showed the mean expression of each gene.
3.6 Specific expression profile associated with NF-PitNET cell subtype: low levels of SSTR3 and ARRB1 in silent corticotroph adenomas
We correlated levels of EMT and SRL response gene expression with immunohistochemical characteristics of NF-PitNETs (Table 5). We found differences in SSTR3 comparing ACTH-expressing NF-PitNETs versus FSH/LH-positive, plurihormonal NF-PitNETs and negative tumors (p = 0.001, p = 0.005 and p = 0.004, respectively) (Figure 5A). We also found differences in ARRB1 comparing ACTH-expressing NF-PitNETs versus FSH/LH-positive and negative cell tumors (p=0.005 and p=0.012, respectively) (Figure 5B).

Table 5 Analysis of differences between the relative expression of each gene and the positive immunostaining for pituitary hormones.
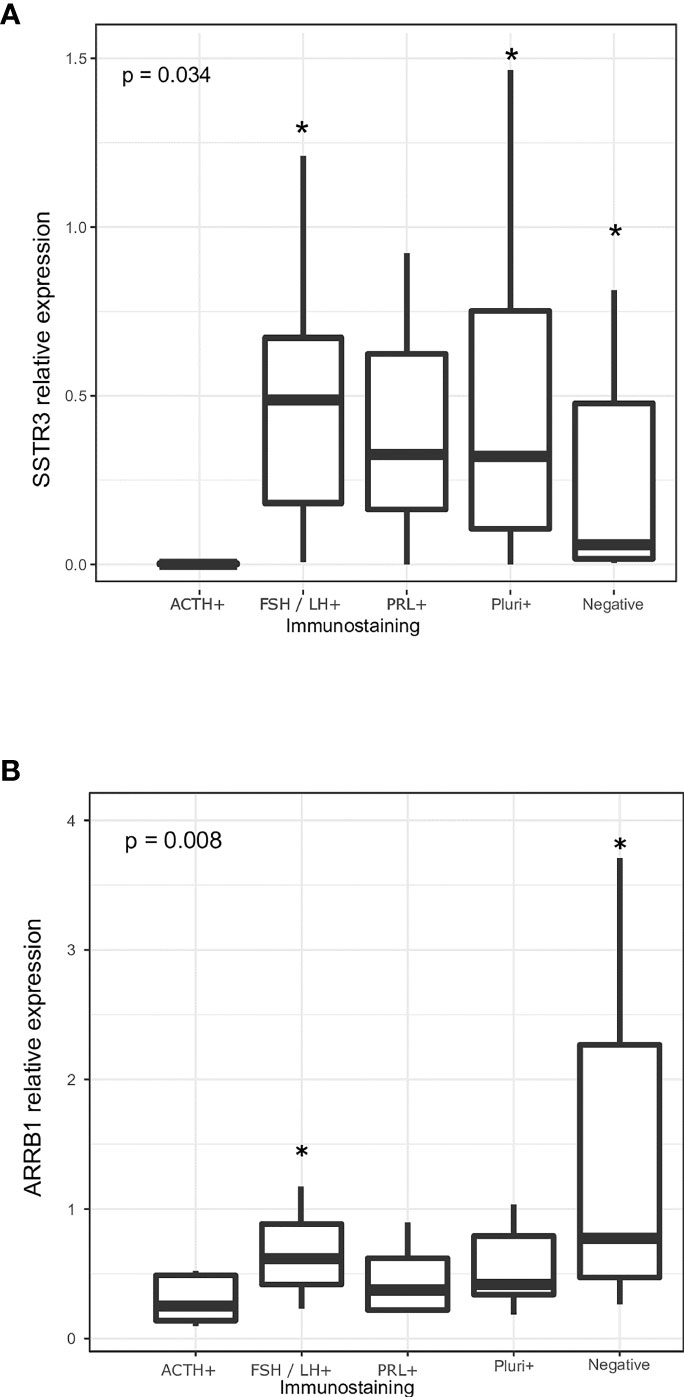
Figure 5 (A) Relative expression of SSTR3 according to the immunohistochemical expression of the pituitary hormones. (B) Relative expression of ARRB1 according to the immunohistochemical expression of the pituitary hormones. P-values for the different group comparisons regarding SSTR3 expression: ACTH+ vs. FSH/LH-+ (p=0.001), ACTH+ vs. PRL+ (p=0.418), ACTH+ vs. plurihormonal NF-PitNETs (p=0.005), ACTH+ vs. negative tumors (p=0.004), FSH/LH+ vs. PRL+ (p=0.418), FSH/LH+ vs. plurihormonal NF-PitNETs (p=0.429), FSH/LH+ vs. negative tumors (p=0.603), PRL+ vs. plurihormonal NF-PitNETs (p=1), PRL+ vs. negative tumors (p=0.795) and plurihormonal NF-PitNETs vs. negative tumors (p=0.787). P-values for the different group comparisons regarding ARRB1 expression: ACTH+ vs. FSH/LH-+ (p=0.005), ACTH+ vs. PRL+ (p=0.509), ACTH+ vs. plurihormonal NF-PitNETs (p=0.152), ACTH+ vs. negative tumors (p=0.012), FSH/LH+ vs. PRL+ (p=0.119), FSH/LH+ vs. plurihormonal NF-PitNETs (p=0.085), FSH/LH+ vs. negative tumors (p=0.147), PRL+ vs. plurihormonal NF-PitNETs (p=0.535), PRL+ vs. negative tumors (p=0.051) and plurihormonal NF-PitNETs vs. negative tumors (p=0.026). * indicates the subtypes of NF-PitNETs that showed significant differences compared to ACTH+ NF-PitNETs.
4 Discussion
NF-PitNET is a very unspecific tumor class in which by definition, no clinically detectable hypersecretory pituitary tumors are included. Its main clinical feature is the mass effect upon the surrounding anatomical sellar structures. In the present work we aimed to explore the molecular knowledge of this tumor class and confirmed its very heterogeneous nature. Regarding tumors with extrasellar growth, we found that both EMT and SRL response genes presented differential expression compared to non-invasive tumors. It has already been described that EMT genes correlate with invasive pituitary tumors as well as with angiogenesis and extracellular matrix degrading genes (34). However, we also found that SSTR2 and PEBP1 were associated to extrasellar growth in some NF-PitNETs that, as far as we know, has not been previously reported.
The measurement of DA receptor and SRL response genes in NF-PitNETs provides interesting information that could be useful in the case that a pharmacological treatment is considered in this type of pituitary tumors (35); thus, it would be recommendable to perform such studies rather than initiating a blind course of treatment with unpredictable results. In the present study, we found a striking NF-PitNET subtype clustering by using the expression of a few genes. Our results indicate the existence of substantial differences in the SRLs biomarkers’ landscape when NF-PitNETs are compared with somatotropinomas, the latter being an archetype of medically treated pituitary tumors. We believe that this is a relevant finding, since usually the detection of differences in clustering between different types of pituitary tumors requires genome-wide data (36).
Furthermore, the present work can shed light on the controversy over the quantitative analysis of dopamine receptors, somatostatin receptor subtypes and downstream effectors in NF-PitNETs (14, 35, 37, 38).
Another interesting finding of the present study, probably the one of most clinical relevance for its application in personalized medicine, is the association of EMT-markers with local growth in NF-PitNETs. Although this association has been previously reported (18, 39–41), we could observe that the EMT phenomenon is more present in the NF-PitNETs compared to somatotropinomas. Furthermore, EMT has been described as a cause of resistance to medical treatment in pituitary tumors, in particular to SRLs (20); thus, the evaluation of these biomarkers in NF-PitNETs would seem highly recommendable in case of considering medical treatment.
The absence of SSTR2, SSTR5 and PLAGL1 has also been proposed by other groups as an explanation for the lack of response to SRLs in NF-PitNETs (35, 37). Furthermore, regarding SSTRs, SSTR3 ligands could be a very interesting druggable target in NF-PitNETs and its pharmacologic activation may be of potential benefits regarding the prevention of tumor regrowth, since SSTR3 inhibits cell cycle dynamics and promotes apoptosis. A recent experimental study has demonstrated that SSTR3 monoligands activate signaling mechanisms that reduce NF-PitNET cell viability and inhibit pituitary tumor growth in animal models expressing SSTR3, suggesting that it could be an efficacious treatment for NF-PitNETs (42).
When comparing the relative expression of the drug receptors, we found that DRD2 was the most expressed receptor in both NF-PitNETs and GH-secreting tumors. However, dopaminergic agents are only useful in 30% of tumors in attaining a clinically significant volume reduction (13), while in GH-secreting pituitary tumors, SRLs induce tumor shrinkage in more than 50% of the cases (43, 44). If we assume that the effects of the drugs are correlated with the expression of their target receptors, we would expect beneficial results from targeting SSTR3 in NF-PitNETs at least at similar levels as observed when targeting SSTR2 in acromegaly. However, if according to our results SSTR3 could be an interesting target for most NF-PitNETs, silent corticotroph tumors should be excluded for such a treatment, because of the low receptor levels they express, and therefore no positive results of SRLs treatment would be expectable in this tumor subtype. This is an important issue in order to identify those tumors presenting a worse prognosis, as is the case for this corticotrophic subtype (45). However, the assumption that the effects of drugs are correlated with the levels of expression of their target receptors is too naïve. The presence of target receptors for both DA and SRLs that act via the MAPK pathway are a sine quanon requirement for a positive therapy outcome. However, the precise molecular mechanisms and the modulatory effect of different transcription factors, intermediate effectors and even cytoskeleton proteins are still not clear (46). The assumption that the presence of more target receptors means more drug efficacy is not so straightforward (47).
Moreover, we found an association between KLK10 expression in NF-PitNETs and extrasellar extension. KLK10 is a gene encoding for a serine protease, member of the tissue kallikrein proteins (KLKs) (48). KLKs are widely recognized as cancer biomarkers (49) and are considered interesting targets for the development of novel drugs (50). KLK10 has been involved in the development of many cancers, such as ovarian (51), breast (52), prostate (53) and thyroid (54) cancers, although the specific role of KLK10 in tumorigenesis is not yet sufficiently defined. Regarding human pituitary tumors, KLK10 has been found to be consistently expressed in prolactinomas, thyrotropinomas, somatotrophinomas and corticotroph adenomas (55, 56). KLK10 could thus be an interesting target for NF-PitNETs, but currently more studies on its pathophysiologic and mechanistic implications should be performed, either silencing or overexpressing its gene in order to clearly define its implications in tumor growth as well as its potential therapeutic use.
Finally, we also found that recurrent tumors expressed higher levels of PEBP1. PEBP1, also known as RKIP, is considered a metastasis suppressor gene (45, 57). In addition, it has been linked to poor response to SRLs in acromegaly (58). We found that PEBP1 is a potential biomarker for predicting recurrence, due to its high sensitivity, although its low specificity may limit its usefulness in clinical practice. Thus, with the current lack of robust biomarkers for implementation of predictive medicine in NF-PitNETs, PEBP1 may be a first step to classify a subgroup of these tumors requiring a more careful follow-up. A validation study of this and the other biomarkers presented in the present work is required. Moreover, drugs specifically designed to target KLK10 and PEBP1 would be welcome, and would be useful for pituitary tumors currently lacking an efficient medical treatment.
In summary, the lack of response to SRLs and DA in NF-PitNETs could be partly explained by a more common EMT phenomenon in this subset of pituitary tumors than in functioning ones (20). Moreover, despite the fact that SSTR3 could be a good therapeutic target, it will presumably not be effective in silent corticotroph tumors. The absence of validated prognostic markers or a prognostic classification for NF-PitNETs limits the evaluation of medical strategies for these lesions. Different pathological markers have been suggested so far, including those of the present study. Their prognostic value should be prospectively confirmed in a large multicenter study which would help to build the instrument to implement precision medicine also for NF-PitNETs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Germans Trias i Pujol Hospital Ethical Committee for Clinical Research (Ref.: EO-11-080 http://www.ceicgermanstrias.cat/index.html). The patients/participants provided their written informed consent to participate in this study.
Author contributions
JG, MM-P, MJ and MP-D contributed to conception and design of the study. MM-P organized the database. JG performed the statistical analysis, performed the experiments and wrote the first draft of the manuscript. BB, MJ and MP-D wrote sections of the manuscript. The remaining authors provided patients and clinical information to the study and critically discussed the results. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the Instituto de Salud Carlos III (PMP15/00027, co-funded by the European Union-ERDF; and PMP22/00021, funded by the European Union -NextGenerationEU); and Novartis through the REMAH (Registro Español Molecular de Adenomas Hipofisarios) consortium of the SEEN (Sociedad Española de Endocrinología y Nutrición). Novartis was not involved in the study design, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
We want to acknowledge the efforts of the REMAH community.
Conflict of interest
MP-D, EV, GuS, IS, GX, PC-S, BB, GeS, SW declare to have received funds from Novartis, Ipsen, and Pfizer as lecturers.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Melmed S. Pituitary tumors. Endocrinol Metab Clin North Am (2015) 44:1–9. doi: 10.1016/j.ecl.2014.11.004
2. Ntali G, Wass JA. Epidemiology, clinical presentation and diagnosis of non-functioning pituitary adenomas. Pituitary (2018) 21:111–8. doi: 10.1007/s11102-018-0869-3
3. Daly AF, Rixhon M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A. High prevalence of pituitary adenomas: A cross-sectional study in the province of liege, Belgium. J Clin Endocrinol Metab (2006) 91:4769–75. doi: 10.1210/jc.2006-1668
4. Lopes MBS. The 2017 world health organization classification of tumors of the pituitary gland: a summary. Acta Neuropathol (2017) 134:521–35. doi: 10.1007/s00401-017-1769-8
5. Even-Zohar N, Greenman Y. Management of NFAs: Medical treatment. Pituitary (2018) 21:168–75. doi: 10.1007/s11102-018-0865-7
6. Drummond J, Roncaroli F, Grossman AB, Korbonits M. Clinical and pathological aspects of silent pituitary adenomas. J Clin Endocrinol Metab (2018) 104:2473–89. doi: 10.1210/jc.2018-00688
7. Asa SL, Mete O, Perry A, Osamura RY. Overview of the 2022 WHO classification of pituitary tumors. Endocr Pathol (2022) 33:6–26. doi: 10.1007/s12022-022-09703-7
8. Chanson P, Raverot G, Castinetti F, Cortet-Rudelli C, Galland F, Salenave S. French Endocrinology society non-functioning pituitary adenoma work-group. management of clinically non-functioning pituitary adenoma. Ann Endocrinol (Paris) (2015) 76:239–47. doi: 10.1016/j.ando.2015.04.002
9. Delgado-López PD, Pi-Barrio J, Dueñas-Polo MT, Pascual-Llorente M, Gordón-Bolaños MC. Recurrent non-functioning pituitary adenomas: A review on the new pathological classification, management guidelines and treatment options. Clin Transl Oncol (2018) 20:1233–45. doi: 10.1007/s12094-018-1868-6
10. Levy MJ, Robertson IJ, Khalk N, Vitello S, Reddy N, Bhake R, et al. Long-term follow up of a large prospective cohort of patients with non-functioning pituitary adenomas: the outcome of a conservative management policy. Clin Endocrinol (Oxf) (2018) 89:354–9. doi: 10.1111/cen.13791
11. Heaney AP, Melmed S. Molecular targets in pituitary tumours. Nat Rev Cancer (2004) 4:285–95. doi: 10.1038/nrc1320
12. Lamberts SWJ, Hofland LJ. Future treatment strategies of aggressive pituitary tumors. Pituitary (2009) 12:261–4. doi: 10.1007/s11102-008-0154-y
13. Colao A, Di Somma C, Pivonello R, Faggiano A, Lombardi G, Savastano S. Medical therapy for clinically non-functioning pituitary adenomas. Endocr Relat Cancer (2008) 15:905–15. doi: 10.1677/ERC-08-0181
14. Fusco A, Giampietro A, Bianchi A, Cimino V, Lugli F, Piacentini S, et al. Treatment with octreotide LAR in clinically non-functioning pituitary adenoma: results from a case-control study. Pituitary (2012) 15:571–8. doi: 10.1007/s11102-011-0370-8
15. Greenman Y, Cooper O, Yaish I, Robenshtok E, Sagiv N, Jonas-Kimchi T, et al. Treatment of clinically nonfunctioning pituitary adenomas with dopamine agonists. Eur J Endocrinol (2016) 175:63–72. doi: 10.1530/EJE-16-0206
16. Yang J, Antin P, Berx G, Blanpain C, Brabletz T, Bronner M, et al. Guidelines and definitions for research on epithelial–mesenchymal transition. Nat Rev Mol Cell Biol (2020) 21:341–52. doi: 10.1038/s41580-020-0237-9
17. Grigore A, Jolly M, Jia D, Farach-Carson M, Levine H. Tumor budding: The name is EMT. J Clin Med (2016) 5:51. doi: 10.3390/jcm5050051
18. Jia W, Zhu J, Martin TA, Jiang A, Sanders AJ, Jiang WG. Epithelial-mesenchymal transition (EMT) markers in human pituitary adenomas indicate a clinical course. Anticancer Res (2015) 35:2635–43.
19. Marques P, Barry S, Carlsen E, Collier D, Ronaldson A, Awad S, et al. Chemokines modulate the tumour microenvironment in pituitary neuroendocrine tumours. Acta Neuropathol Commun (2019) 7:172. doi: 10.1186/s40478-019-0830-3
20. Gil J, Jordà M, Soldevila B, Puig-Domingo M. Epithelial–mesenchymal transition in the resistance to somatostatin receptor ligands in acromegaly. Front Endocrinol (Lausanne) (2021) 12:646210. doi: 10.3389/fendo.2021.646210
21. Lekva T, Berg JP, Fougner SL, Olstad OK, Ueland T, Bollerslev J. Gene expression profiling identifies ESRP1 as a potential regulator of epithelial mesenchymal transition in somatotroph adenomas from a large cohort of patients with acromegaly. J Clin Endocrinol Metab (2012) 97:E1506–14. doi: 10.1210/jc.2012-1760
22. Lekva T, Berg JP, Heck A, Lyngvi Fougner S, Olstad OK, Ringstad G, et al. Attenuated RORC expression in the presence of EMT progression in somatotroph adenomas following treatment with somatostatin analogs is associated with poor clinical recovery. PloS One (2013) 8:e66927. doi: 10.1371/journal.pone.0066927
23. Gil J, Marques-Pamies M, Valassi E, García-Martínez A, Serra G, Hostalot C, et al. Implications of heterogeneity of epithelial-mesenchymal states in acromegaly therapeutic pharmacologic response. Biomedicines (2022) 10:460. doi: 10.3390/biomedicines10020460
24. Puig-Domingo M, Gil J, Sampedro Nuñez M, Jordà M, Webb SM, Serra G, et al. Molecular profiling for acromegaly treatment: A validation study. Endocr Relat Cancer (2020) 27:357–89. doi: 10.1530/ERC-18-0565
25. Treppiedi D, Mangili F, Giardino E, Catalano R, Locatelli M, Lania AG, et al. Cytoskeleton protein filamin a is required for efficient somatostatin receptor type 2 internalization and recycling through Rab5 and Rab4 sorting endosomes in tumor somatotroph cells. Neuroendocrinology (2020) 110:642–52. doi: 10.1159/000503791
26. Mantovani G, Treppiedi D, Giardino E, Catalano R, Mangili F, Vercesi P, et al. Cytoskeleton actin-binding proteins in clinical behavior of pituitary tumors. Endocr Relat Cancer (2019) 26:R95–R108. doi: 10.1530/ERC-18-0442
27. Peverelli E, Mantovani G, Vitali E, Elli FM, Olgiati L, Ferrero S, et al. Filamin-a is essential for dopamine D2 receptor expression and signaling in tumorous lactotrophs. J Clin Endocrinol Metab (2012) 97:967–77. doi: 10.1210/jc.2011-2902
28. Caccavelli L, Morange-Ramos I, Kordon C, Jaquet P, Enjalbert A. Alteration of gα subunits mRNA levels in bromocriptine resistant prolactinomas. J Neuroendocrinol (1996) 8:737–46. doi: 10.1046/j.1365-2826.1996.04902.x
29. Mangili F, Treppiedi D, Catalano R, Marra G, Di Muro G, Spada A, et al. Mantovani g. a novel mechanism regulating dopamine receptor type 2 signal transduction in pituitary tumoral cells: The role of cAMP/PKA-induced filamin a phosphorylation. Front Endocrinol (Lausanne) (2021) 11:611752. doi: 10.3389/fendo.2020.611752
30. Mangili F, Giardino E, Treppiedi D, Barbieri AM, Catalano R, Locatelli M, et al. Beta-arrestin 2 is required for dopamine receptor type 2 inhibitory effects on AKT phosphorylation and cell proliferation in pituitary tumors. Neuroendocrinology (2021) 111:568–79. doi: 10.1159/000509219
31. Raverot G, Jouanneau E, Trouillas J. MANAGEMENT OF ENDOCRINE DISEASE: Clinicopathological classification and molecular markers of pituitary tumours for personalized therapeutic strategies. Eur J Endocrinol (2014) 170:R121–32. doi: 10.1530/EJE-13-1031
32. Mallona I, Díez-Villanueva A, Martín B, Peinado MA. Chainy: an universal tool for standardized relative quantification in real-time PCR. Bioinformatics (2017) 33:1411–3. doi: 10.1093/bioinformatics/btw839
33. Vandesompele J, De Preter K, Pattyn F, Poppe B, Van Roy N, De Paepe A, et al. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol (2002) 3:RESEARCH0034. doi: 10.1186/gb-2002-3-7-research0034
34. Yang Q, Li X. Molecular network basis of invasive pituitary adenoma: A review. Front Endocrinol (Lausanne) (2019) 10:7. doi: 10.3389/fendo.2019.00007
35. Vieria Neto L, Wildemberg LE, Colli LM, Kasuki L, Marques NV, Moraes AB, et al. ZAC1 and SSTR2 are downregulated in non-functioning pituitary adenomas but not in somatotropinomas. PloS One (2013) 8:e77406. doi: 10.1371/journal.pone.0077406
36. Salomon MP, Wang X, Marzese DM, Hsu SC, Nelson N, Zhang X, et al. The epigenomic landscape of pituitary adenomas reveals specific alterations and differentiates among acromegaly, cushing’s disease and endocrine-inactive subtypes. Clin Cancer Res (2018) 24:4126–36. doi: 10.1158/1078-0432.CCR-17-2206
37. Taboada GF, Luque RM, Bastos W, Guimarães RFC, Marcondes JB, Chimelli LMC, et al. Quantitative analysis of somatostatin receptor subtype (SSTR1-5) gene expression levels in somatotropinomas and non-functioning pituitary adenomas. Eur J Endocrinol (2007) 156:65–74. doi: 10.1530/eje.1.02313
38. Kiseljak-Vassiliades K, Xu M, Mills TS, Smith EE, Silveira LJ, Lillehei KO, et al. Differential somatostatin receptor (SSTR) 1-5 expression and downstream effectors in histologic subtypes of growth hormone pituitary tumors. Mol Cell Endocrinol (2015) 417:73–83. doi: 10.1016/j.mce.2015.09.016
39. Chauvet N, Romanò N, Meunier A-C, Galibert E, Fontanaud P, Mathieu M-N, et al. Combining cadherin expression with molecular markers discriminates invasiveness in growth hormone and prolactin pituitary adenomas. J Neuroendocrinol (2016) 28. doi: 10.1111/jne.12352
40. Zhou K, Jin H, Luo Y. Expression and significance of e-cadherin and β-catenins in pituitary adenoma. Int J Surg Pathol (2013) 21:363–7. doi: 10.1177/1066896912471850
41. Mendes GA, Haag T, Trott G, Rech CGSL, Ferreira NP, Oliveira MC, et al. Expression of e-cadherin, Slug and NCAM and its relationship to tumor invasiveness in patients with acromegaly. Braz J Med Biol Res (2018) 51. doi: 10.1590/1414-431x20176808
42. Vázquez-Borrego MC, Gupta V, Ibáñez-Costa A, Gahete MD, Venegas-Moreno E, Toledano-Delgado Á, et al. A somatostatin receptor subtype-3 (SST 3 ) peptide agonist shows antitumor effects in experimental models of nonfunctioning pituitary tumors. Clin Cancer Res (2020) 26:957–69. doi: 10.1158/1078-0432.CCR-19-2154
43. Giustina A, Mazziotti G, Torri V, Spinello M, Floriani I, Melmed S. Meta-analysis on the effects of octreotide on tumor mass in acromegaly. PloS One (2012) 7:e36411. doi: 10.1371/journal.pone.0036411
44. Caron PJ, Bevan JS, Petersenn S, Flanagan D, Tabarin A, Prévost G, et al. Tumor shrinkage with lanreotide autogel 120 mg as primary therapy in acromegaly: Results of a prospective multicenter clinical trial. J Clin Endocrinol Metab (2014) 99:1282–90. doi: 10.1210/jc.2013-3318
45. Ben-Shlomo A, Cooper O. Silent corticotroph adenomas. Pituitary (2018) 21:183–93. doi: 10.1007/s11102-018-0864-8
46. Peverelli E, Treppiedi D, Giardino E, Vitali E, Lania AG, Mantovani G. Dopamine and somatostatin analogues resistance of pituitary tumors: Focus on cytoskeleton involvement. Front Endocrinol (Lausanne) (2015) 6:187. doi: 10.3389/fendo.2015.00187
47. Gatto F, Arvigo M, Ferone D. Somatostatin receptor expression and patients’ response to targeted medical treatment in pituitary tumors: Evidences and controversies. J Endocrinol Invest (2020) 43:1543–53. doi: 10.1007/s40618-020-01335-0
48. Yousef GM, Diamandis EP. The new human tissue kallikrein gene family: structure, function, and association to disease. Endocr Rev (2001) 22:184–204. doi: 10.1210/edrv.22.2.0424
49. Borgoño CA, Diamandis EP. The emerging roles of human tissue kallikreins in cancer. Nat Rev Cancer (2004) 4:876–90. doi: 10.1038/nrc1474
50. Prassas I, Eissa A, Poda G, Diamandis EP. Unleashing the therapeutic potential of human kallikrein-related serine proteases. Nat Rev Drug Discov (2015) 14:183–202. doi: 10.1038/nrd4534
51. Dong Y, Loessner D, Irving-Rodgers H, Obermair A, Nicklin JL, Clements JA. Metastasis of ovarian cancer is mediated by kallikrein related peptidases. Clin Exp Metastasis (2014) 31:135–47. doi: 10.1007/s10585-013-9615-4
52. Kioulafa M, Kaklamanis L, Stathopoulos E, Mavroudis D, Georgoulias V, Lianidou ES. Kallikrein 10 (KLK10) methylation as a novel prognostic biomarker in early breast cancer. Ann Oncol Off J Eur Soc Med Oncol (2009) 20:1020–5. doi: 10.1093/annonc/mdn733
53. Hu J, Lei H, Fei X, Liang S, Xu H, Qin D, et al. NES1/KLK10 gene represses proliferation, enhances apoptosis and down-regulates glucose metabolism of PC3 prostate cancer cells. Sci Rep (2015) 5:17426. doi: 10.1038/srep17426
54. Buj R, Mallona I, Díez-Villanueva A, Zafon C, Mate JL, Roca M, et al. Kallikreins stepwise scoring reveals three subtypes of papillary thyroid cancer with prognostic implications. Thyroid (2018) 28:601–12. doi: 10.1089/thy.2017.0501
55. Rotondo F, Di Ieva A, Kovacs K, Cusimano MD, Syro LV, Diamandis EP, et al. Human kallikrein 10 in surgically removed human pituitary adenomas. Hormones (Athens) (2014) 14:272–9. doi: 10.14310/horm.2002.1558
56. Di Meo A, Rotondo F, Kovacs K, Cusimano MD, Syro LV, Di Ieva A, et al. Human kallikrein 10 expression in surgically removed human pituitary corticotroph adenomas: An immunohistochemical study. Appl Immunohistochem Mol Morphol AIMM (2015) 23:433–7. doi: 10.1097/PAI.0000000000000108
57. Escara-Wilke J, Yeung K, Keller ET. Raf kinase inhibitor protein (RKIP) in cancer. Cancer Metastasis Rev (2012) 31:615–20. doi: 10.1007/s10555-012-9365-9
Keywords: Epithelial-mesenchymal transition, non-functioning pituitary adenomas, somatostatin receptor ligands, dopamine agonists, somatostatin analogs
Citation: Gil J, Marques-Pamies M, Valassi E, Serra G, Salinas I, Xifra G, Casano-Sancho P, Carrato C, Biagetti B, Sesmilo G, Marcos-Ruiz J, Rodriguez-Lloveras H, Rueda-Pujol A, Aulinas A, Blanco A, Hostalot C, Simó-Servat A, Muñoz F, Rico M, Ibáñez-Domínguez J, Cordero E, Webb SM, Jordà M and Puig-Domingo M (2023) Molecular characterization of epithelial-mesenchymal transition and medical treatment related-genes in non-functioning pituitary neuroendocrine tumors. Front. Endocrinol. 14:1129213. doi: 10.3389/fendo.2023.1129213
Received: 21 December 2022; Accepted: 23 February 2023;
Published: 22 March 2023.
Edited by:
Murat Aydin Sav, Yeditepe University, TürkiyeReviewed by:
Donatella Treppiedi, University of Milan, ItalyAndrea Lania, Humanitas University, Italy
Copyright © 2023 Gil, Marques-Pamies, Valassi, Serra, Salinas, Xifra, Casano-Sancho, Carrato, Biagetti, Sesmilo, Marcos-Ruiz, Rodriguez-Lloveras, Rueda-Pujol, Aulinas, Blanco, Hostalot, Simó-Servat, Muñoz, Rico, Ibáñez-Domínguez, Cordero, Webb, Jordà and Puig-Domingo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manel Puig-Domingo, bXB1aWdkQGlndHAuY2F0
†These authors share first authorship