 Martin Eichler1,2,3,4,5*
Martin Eichler1,2,3,4,5* Leopold Hentschel2,3,4,5
Leopold Hentschel2,3,4,5 Susanne Singer6Beate Hornemann2,3,4,5Stephan Richter1Christine Hofbauer2,3,4,5,7Peter Hohenberger8
Susanne Singer6Beate Hornemann2,3,4,5Stephan Richter1Christine Hofbauer2,3,4,5,7Peter Hohenberger8 Bernd Kasper9
Bernd Kasper9 Dimosthenis Andreou10,11Daniel Pink12,13
Dimosthenis Andreou10,11Daniel Pink12,13 Jens Jakob8,14
Jens Jakob8,14 Robert Grützmann15Stephen Fung16
Robert Grützmann15Stephen Fung16 Eva Wardelmann17Karin Arndt18Kerstin Hermes-Moll19Olaf Schoffer2,3,4,5,20Marius Fried21
Eva Wardelmann17Karin Arndt18Kerstin Hermes-Moll19Olaf Schoffer2,3,4,5,20Marius Fried21 Helena K. Jambor1,2,3,4,5Jürgen Weitz2,3,4,5,22Klaus-Dieter Schaser2,3,4,5,7
Helena K. Jambor1,2,3,4,5Jürgen Weitz2,3,4,5,22Klaus-Dieter Schaser2,3,4,5,7 Martin Bornhäuser1,2,3,4,5Jochen Schmitt2,3,4,5,20Markus K. Schuler1
Martin Bornhäuser1,2,3,4,5Jochen Schmitt2,3,4,5,20Markus K. Schuler1- 1Clinic and Polyclinic for Internal Medicine I, University Hospital Carl Gustav Carus, Technical University Dresden, Dresden, Germany
- 2National Center for Tumor Diseases Dresden (NCT/UCC), Dresden, Germany
- 3German Cancer Research Center (DKFZ), Heidelberg, Germany
- 4Faculty of Medicine and University Hospital Carl Gustav Carus, Technical University Dresden, Dresden, Germany
- 5Helmholtz-Center Dresden-Rossendorf (HZDR), Dresden, Germany
- 6Institute of Medical Biostatistics, Epidemiology and Informatics, University Medical Centre of Johannes Gutenberg University Mainz, Mainz, Germany
- 7University Center for Orthopedics and Trauma Surgery, Technical University Dresden, Dresden, Germany
- 8Division of Surgical Oncology & Thoracic Surgery, Mannheim University Medical Center, University of Heidelberg, Mannheim, Germany
- 9Sarcoma Unit, Mannheim Cancer Center, Mannheim University Medical Center, University of Heidelberg, Mannheim, Germany
- 10Department of General Orthopedics and Tumor Orthopedics, Münster University Hospital, Münster, Germany
- 11Department of Orthopedics and Trauma, Medical University of Graz, Graz, Austria
- 12Sarcoma Center Berlin-Brandenburg, Helios Hospital Bad Saarow, Bad Saarow, Germany
- 13Department of Internal Medicine C, University Hospital Greifswald, Greifswald, Germany
- 14Clinic for General, Visceral, and Pediatric Surgery, University Hospital Goettingen, Goettingen, Germany
- 15Clinic for Surgery, University Hospital Erlangen, Erlangen, Germany
- 16Clinic for General, Visceral, and Pediatric Surgery, University Hospital Dusseldorf, Dusseldorfn, Germany
- 17Gerhard-Domagk-Institute of Pathology, University Hospital Münster, Münster, Germany
- 18German Sarcoma Foundation, Woelfersheim, Germany
- 19Scientific Institute of Office-based Hematologists and Oncologists, Cologne, Germany
- 20Center for Evidence-based Healthcare, University Hospital Carl Gustav Carus, Technical University Dresden, Dresden, Germany
- 21Clinic and Polyclinic for Internal Medicine III/University Cancer Center Mainz, University Hospital Mainz, Mainz, Germany
- 22Department of Visceral, Thoracic and Vascular Surgery, University Hospital Carl Gustav Carus, Technical University Dresden, Dresden, Germany
Introduction: Sarcomas are rare cancers and very heterogeneous in their location, histological subtype, and treatment. Health-Related Quality of Life (HRQoL) of sarcoma patients has rarely been investigated in longitudinal studies.
Methods: Here, we assessed adult sarcoma patients and survivors between September 2017 and February 2020, and followed-up for one year in 39 study centers in Germany. Follow-up time points were 6 (t1) and 12 months (t2) after inclusion. We used a standardized, validated questionnaire (the European Organisation for Research and Treatment of Cancer Quality of Life Core Instrument (EORTC QLQ-C30) and explored predictors of HRQoL in two populations (all patients (Analysis 1), patients in ongoing complete remission (Analysis 2)) using generalized linear mixed models.
Results: In total we included up to 1111 patients at baseline (915 at t1, and 847 at t2), thereof 387 participants were in complete remission at baseline (334 at t1, and 200 at t2). When analyzing all patients, HRQoL differed with regard to tumor locations: patients with sarcoma in lower extremities reported lower HRQoL values than patients with sarcomas in the upper extremities. Treatment which included radiotherapy and/or systemic therapy was associated with lower HRQoL. For patients in complete remission, smoking was associated with worse HRQoL-outcomes. In both analyses, bone sarcomas were associated with the worst HRQoL values. Being female, in the age group 55-<65 years, having lower socioeconomic status, and comorbidities were all associated with a lower HRQoL, in both analyses.
Discussion: HRQoL increased partially over time since treatment and with sporting activities. HRQoL improved with time since treatment, although not in all domains, and was associated with lifestyle and socioeconomic factors. Bone sarcomas were the most affected subgroup. Methods to preserve and improve HRQoL should be developed for sarcoma patients.
1 Introduction
Sarcomas and gastrointestinal stromal tumors are a group of rare cancers, with about 7000 new cases per year in Germany (1) and an incidence of around 7 per 100,000 in Europe (2). The five-year relative survival in 2010–2016 was 65% for soft tissue sarcomas (STS), 60-79% for bone sarcomas, and 83% for gastrointestinal stromal tumors (GIST) (3). Sarcomas are heterogeneous tumors that include a large variety of over 100 histological subtypes (4), can occur anywhere in the body, and their therapy is based on complex and divergent treatment algorithms (5). Sarcomas are often diagnosed late due to their rarity and the unspecific symptoms they cause (6). Unplanned resections, a result of misdiagnosing the tumors as more common benign or even non-neoplastic lesions, with a negative influence on patient outcome are common (7, 8). Treatment at specialized centers is recommended by international guidelines and is associated with a prolonged survival (9–12).
Cancer patients rate their Health-Related Quality of Life (HRQoL) as an important aspect of their treatment and outcome, and improvement of HRQoL is at times preferred to the mere prolongation of live (13). The multidimensional construct HRQoL itself is a patient-reported outcome, that surveys physical, functional, social, and emotional well-being, as well as disease specific symptoms and restrictions (14).
Literature on HRQoL issues of sarcoma patients has improved over the last few years with two larger studies (15, 16) and a variety of reviews (17–19) published since 2019. Despite these developments, the heterogeneity and rareness of the disease, the variety of treatment pathways experienced by sarcoma patients, as well as the lack of a sarcoma specific measurement tool (20, 21) still leave questions unanswered.
The aim of this analysis was to explore factors associated with longitudinal HRQoL and specifically address lifestyle factors and HRQoL changes over time after the end of treatment. We examined both the predictors of the course of HRQoL in all sarcoma patients regardless of disease stage (Analysis 1) and the predictors of the course of HRQoL in patients in complete remission (Analysis 2).
2 Methods
The prospective PROSa cohort study (Burden and Medical Care of Sarcoma in Germany: Nationwide Cohort Study Focusing on Modifiable Determinants of Patient-Reported Outcome Measures in Sarcoma Patients; www.uniklinikum-dresden.de/prosastudie) was conducted nationwide in 39 study centers in Germany between September 2017 and May 2020 (NCT03521531; ClinicalTrials.gov). Of those, 8 were office-based practices, 22 hospitals of maximum care, and 9 other hospitals. Patients were approached at baseline as well as six (t1) and twelve months (t2) after baseline.
Eligible patients and survivors were asked to participate at the study centers during visits (treatment, diagnosis, aftercare) and sometimes by phone or letter. Participation required informed consent. The study was approved by the ethics committees of the Technical University of Dresden (IRB00001473, EK1790422017) and the participating centers (22). Baseline and follow-up data (t1, t2) were collected at the study coordination center at University Hospital Dresden. HRQoL data and socio-demographic data were sent by the participants to the study coordination center by mail or online. In case of non-participation in follow-up, a reminder was sent after 4 weeks. Clinical information was submitted to the study coordination center online by the study centers using case report forms. Data collection was performed using REDCap (23).
We included adult patients and survivors with histologically proven sarcoma of any entity (24). We excluded persons who were mentally or linguistically unable to complete questionnaires. For Analysis 1 (all patients) only participants with HRQoL data were included, for Analysis 2 (patients in ongoing complete remission), we excluded all patients not in complete remission, in current treatment, or with unknown disease status.
2.1 Instruments
HRQoL was measured using the European Organisation for Research and Treatment of Cancer Quality of Life Core Questionnaire (EORTC QLQ-C30) (25). This instrument measures global quality of life (global health), 5 functioning, and 9 symptom scales in values from 0 to 100. Higher scores indicate better quality of life for the functioning scales and higher symptom burden for the symptom scales. The relevance of the differences was evaluated using reference values from Cocks et al. (26). With these reference values, each scale difference can be classified as “trivial”, “small”, “medium” and “large”, defined as “Large: one representing unequivocal clinical relevance. Medium: likely to be clinically relevant but to a lesser extent. Small: subtle but nevertheless clinically relevant. Trivial: circumstances unlikely to have any clinical relevance or where there was no difference.” (26).
Socioeconomic status (SES) was assessed using the Winkler Index (27). The Winkler Index is a composite score which covers and quantifies three dimensions of SES: income, education and occupational prestige. On a scale of 3 to 21, a lower score means a lower SES.
The extent of sporting activities was measured using the German Exercise and Sport Questionnaire (“Bewegungs- und Sportfragebogen”) (28). This questionnaire assesses whether patients regularly exercised over the last 4 weeks and asks about the time spent doing so.
Alcohol consumption was grouped in 4 categories (none, weekly or less, regularly moderate (2-3 times a week of up to 4 drinks or 4 times or more a week up to 2 drinks), and regularly larger amounts (more than 4 drinks 2-3 times a week or more than 2 drinks 4 times or more a week.
For Analysis 1 (all patients), we used the patient reported socio-economic variable SES at baseline, as well as the lifestyle variables sporting activities at baseline, t1, and t2 (none, 1-<15 min per week, 15-<30 min per week, ≥30 min per week, unknown), smoking at baseline, t1, and t2 (never, former, actual, unknown), and alcohol consumption at baseline (never, weekly or less, regularly moderate, regularly larger amounts, unknown). From the medical records we collected age at baseline (18-<40, 40-<55, 55-<65, 65-<75, ≥75 years), gender (male, female)the disease characteristics sarcoma type (liposarcoma, fibroblastic/myofibroblastic/fibrohistiocytic sarcoma, GIST, unclassified sarcoma, leiomyosarcoma, bone sarcoma synovialsarcoma, others) and tumor location (abdomen/retroperitoneum, thorax, pelvis, lower limbs, upper limbs, other), comorbidities (cardiovascular, respiratory, diabetes, second cancer, kidney) at baseline (0, 1, 2, ≥3), disease status at baseline, t1, and t2 (complete remission, partial remission/stable disease, progression, unknown), time since treatment at baseline, t1, and t2 (in treatment, <0.5 year, 0.5-<1 year, 1-<2 years, 2-<5 years, ≥5 years, unknown), performed treatments at baseline, t1 and t2 (surgery alone, surgery + systemic therapy (ST), surgery + radiotherapy (RT), surgery + RT + ST, other). For Analysis 2 (patients in ongoing complete remission), we used the above-mentioned variables, except disease status at baseline.
2.2 Statistics
Continuous variables were evaluated by mean and standard deviation (SD). Categorical variables were presented with absolute and relative frequencies. We compared participants at all timepoints with those who were lost or did not send back the questionnaire during follow-up to estimate possible selection bias. An analysis of non-participants at baseline was reported elsewhere (16).
For both analyses, five pre-specified domains of the EORTC QLQ-C30 in which the most distinct differences were expected were examined for associated factors: global health, physical functioning, role functioning, pain, and fatigue. We used a generalized linear mixed model with patients as level 1 and timepoint of data collection (baseline, 6 months, 12 months) as level 2.
To avoid multicollinearity, correlations, and tolerance between the model variables were calculated before regression analyses. Correlations ≥ 0.7 and tolerance values ≤ 0.1 indicate strong multicollinearity.
For model variables with more than 5 missing cases, a category “unknown” was created. Imputation method for missing values in SES is described elsewhere (16).
Statistical analyses were performed with SPSS V.28 (IBM Corporation, Armonk, New York, USA).
3 Results
3.1 Description of the study population/analysis of follow-up non-participants and drop-outs
In total, 1309 sarcoma patients agreed to participate at baseline, 1030 were eligible at t1, and 969 at t2. Questions on global health were answered by 1106 (baseline), 909 (t1), and 845 (t2) patients. A number of 144 patients dropped out during the study period, 119 of them died. For the Analysis 2 of patients in ongoing complete remission, the general health data was available for 386 (baseline), 329 (t1), and 198 (t2) patients, respectively. See Figure 1 for a detailed flow-diagram.

Figure 1 Flow-Chart study population.
A full description of the variables used for Analysis 1 and Analysis 2 are presented in Table 1. At baseline, 51% of participants were men, the mean age was 57 years, and around 30% of patients were in treatment. For Analysis 2, 49% of analyzed patients were men, the mean age was 54 years.
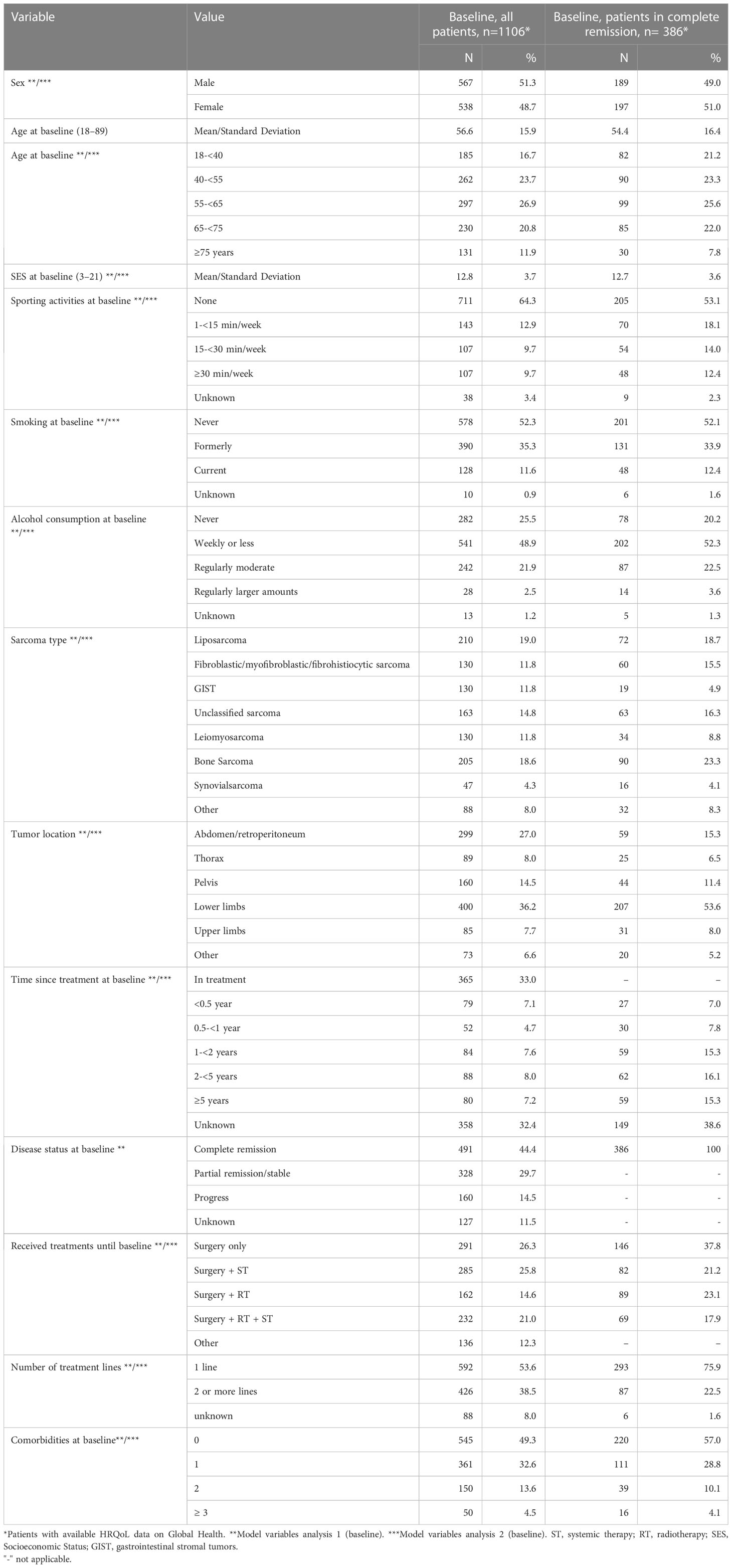
Table 1 Description of study populations.
The characteristics of patients surveyed, patients who declined responses, and patients who dropped out during follow-up, differed in parts (Table 2). While unadjusted HRQoL values between participants and non-participants were in a range of 2 points, non-participants were on average between 4 and 7 years younger than participants, and more often male than female. Large differences between deceased patients and participants were observed in HRQoL values (ranging from 14 to 20 points) and in gender (overall 50% and 51% of participants were female, among deceased patients this was only 37% and 39%).
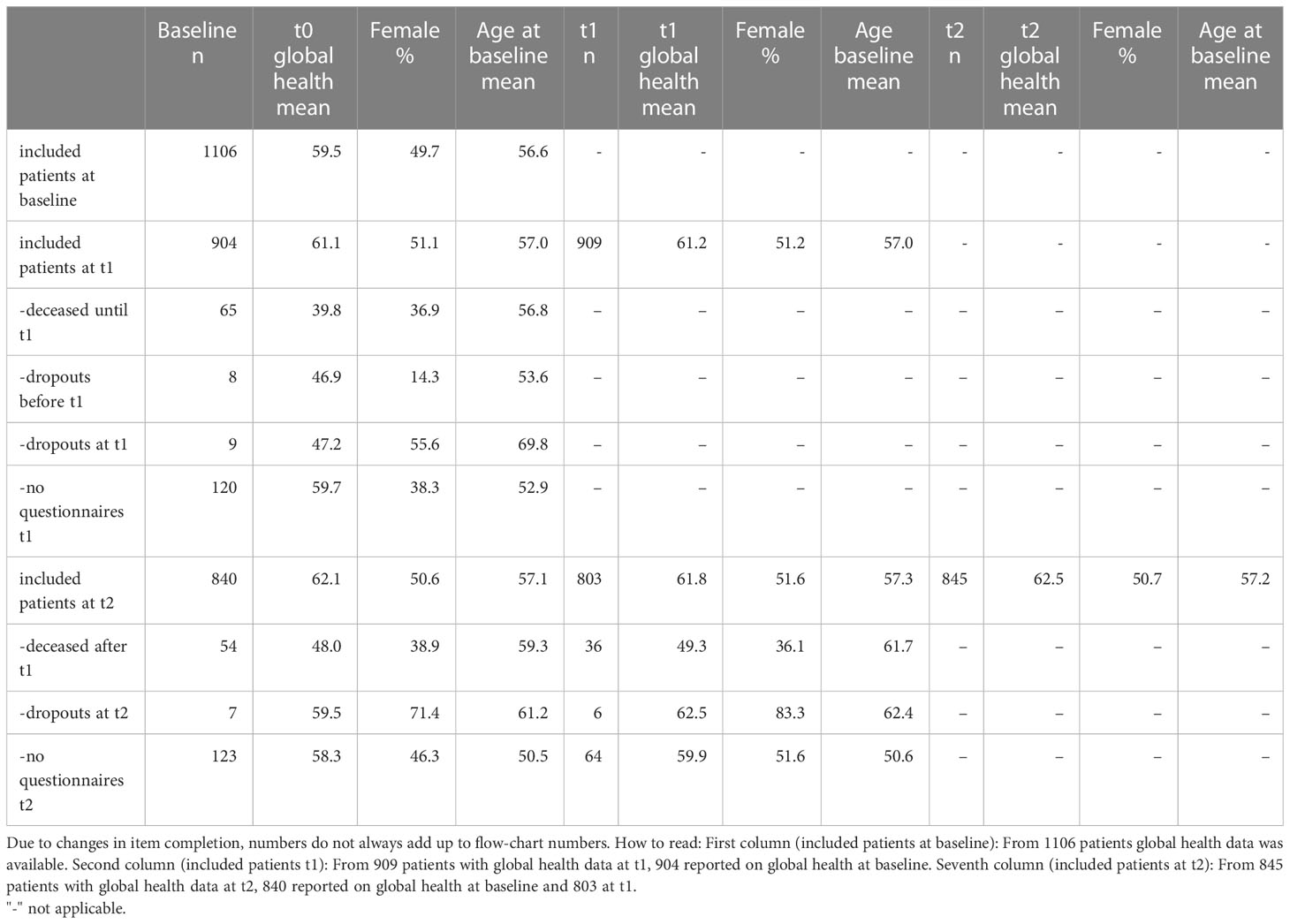
Table 2 Comparison of Global Health data, sex and age of analyzed (included) patients, unit non responders (no questionnaires) and patients lost to follow up during baseline, 6 months (t1) and 12 months (t2).
3.2 Analysis 1: factors associated with the course of HRQoL in all sarcoma patients
Data for Analysis 1 is summarized in Table 3, and includes non-standardized regression coefficients (B) indicating a B point increase or decrease in the respective scale. The HRQoL was mostly stable over the observed time, with significant, but trivial differences found in physical functioning, fatigue, and pain. In three domains woman were more strongly affected than men: differences were trivial for physical functioning and pain; small clinically relevant differences were found for fatigue. With younger patients (age: 18-<40 years) as reference value, we observed small but significant differences in all analyzed domains: the most affected groups were patients aged 55-<65 (global health, physical functioning, role functioning and fatigue) and those ≥75 (global health, physical functioning, fatigue, and pain). A 10-point increase in the socioeconomic status was associated with small and significant beneficial changes in global health, physical functioning, fatigue, and pain. Sporting activities were significantly associated with higher HRQoL in all HRQoL domains. Former smokers (comparison: those who never smoked) experienced lower HRQoL in three domains, but those differences were trivial. Compared to patients who consumed no alcohol at all, those with weekly or less consumption or those with a regular, but moderate consumption reported small clinically relevant better outcomes in all domains.
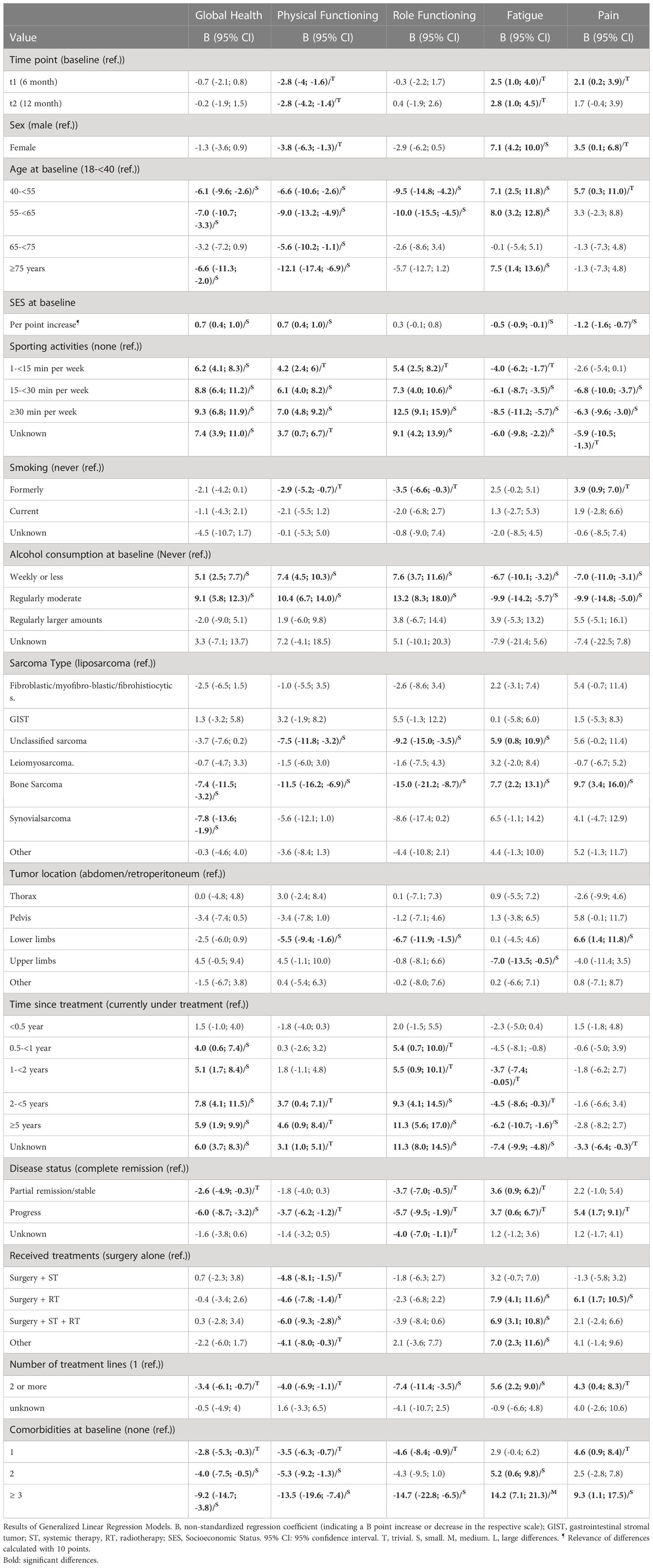
Table 3 Factors associated with HRQoL domains over time in German sarcoma patients (Analysis 1).
Using liposarcoma patients as reference group, bone sarcoma patients were the worst performing group. They showed small clinically relevant and significant differences in all analyzed domains. Patients with unclassified sarcomas experienced worse HRQoL in three (physical functioning, role functioning, fatigue), those with synovialsarcoma in one domain (global health). Patients with tumors located at the lower limbs (reference: abdominal/retroperitoneal sarcomas) reported lower physical and role functioning as well as higher pain. In contrast, patients with tumors located at the upper limbs reported better global health and less fatigue.
With respect to treatment status and time since treatment (reference: patients in treatment), an relevant improvement over time was observed in all domains except pain and physical functioning. Clinically relevant improvements over time were not uniform across domains. For global healtha small clinically relevant improvement was observed 6 months, for role functioning 2 years and for fatigue 5 years after treatment. Differences between patients in complete remission and partial remission/stable disease remained trivial. Patients with progressive disease showed small clinically relevant differences in global health. In comparison to patients treated with surgery alone, those treated additionally with systemic therapy (ST) + radiotherapy (RT) experienced worse physical functioning and more fatigue, and those treated additionally with RT worse fatigue and pain. Patients who received (at least) second line treatment were more affected than those in first line treatment. Small significant differences were observed in role functioning and fatigue. The number of comorbidities was also associated with lower HRQoL for patients with 3 or more comorbidities as the worst performing group over all 5 domains.
3.3 Analysis 2: factors associated with the course of HRQoL in patients in ongoing complete remission
Data for Analysis 2 is summarized in Table 4. HRQoL stayed largely stable over the observed period, with a significant, but trivial difference found in role functioning. Woman were in three domains more affected than men; significant small clinically relevant differences were found in global health, physical functioning, and fatigue. With younger patients (age: 18-<40 years) as reference, small to medium significant differences were found in all analyzed domains: the most affected groups were patients aged 55-<65 (all domains) and ≥75 (physical and role functioning, fatigue and pain). A 10-point increase in socioeconomic status showed small significant improvements in global health, physical functioning, and pain. Sporting activities were significantly associated with better HRQoL in all HRQoL domains. Current smokers (comparison: never smoked) experienced worse HRQoL in two domains (role functioning and fatigue), those differences were small. Compared to patients who consumed no alcohol at all, those with weekly or less consumption or those with a regular, but moderate consumption reported small clinically relevant better outcomes in all domains.
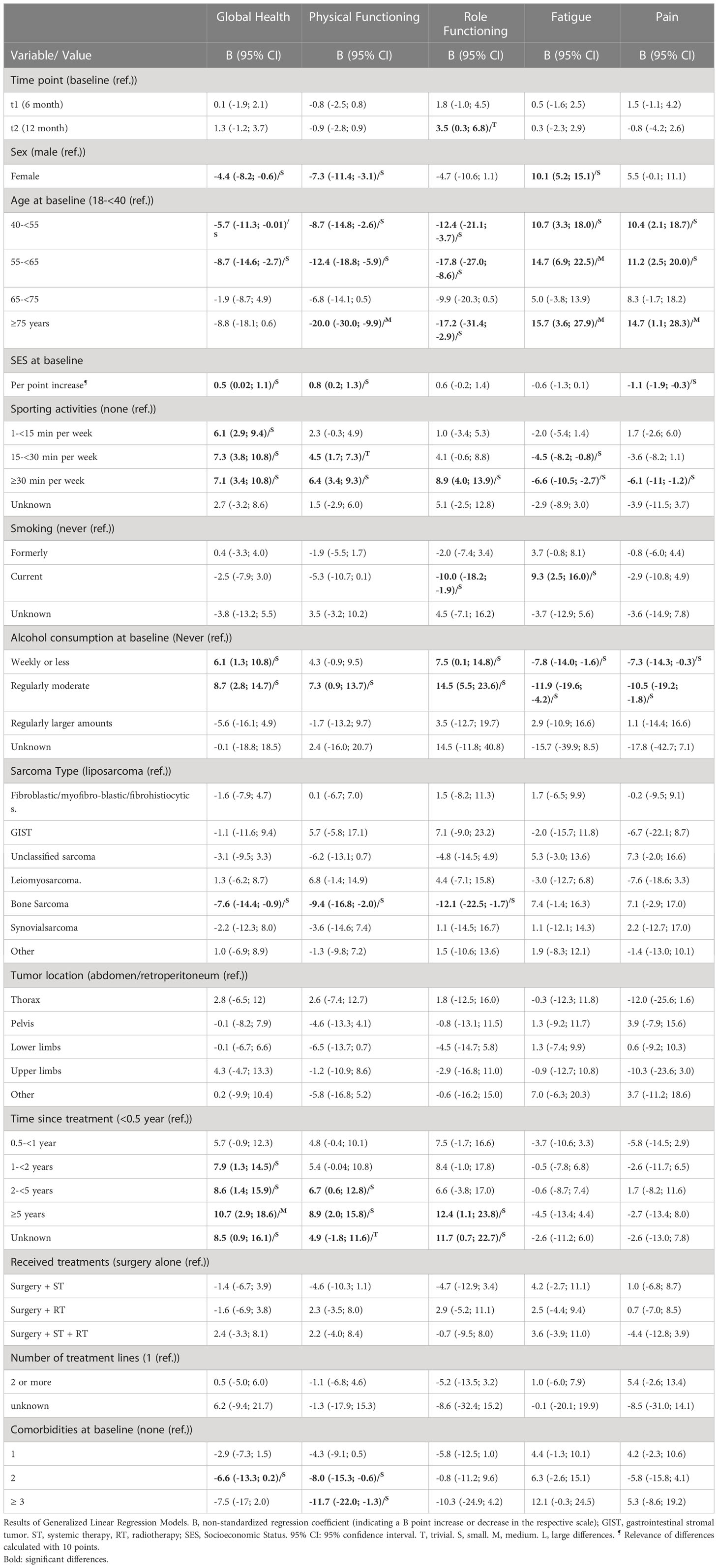
Table 4 Factors associated with HRQoL domains over time in German sarcoma patients in complete remission (analysis 2).
Compared to liposarcoma patients as reference, patients with bone sarcoma were the worst performing group. They showed small clinically relevant and significant differences in general health, physical and role functioning. Other differences did not reach significance. No significant differences were observed with regard to tumor location.
With respect to time since treatment (reference: up to 6 months after treatment) an improvement over time was observed in all domains except pain and fatigue. Improvement over time was not uniform across domains and took longest in role functioning, reaching clinical relevance in this domain 5 years after treatment. In global health, a small clinically relevant improvement was observed 12 months after treatment and a medium improvement after 5 years. In physical functioning a small clinically relevant improvement was observed 2 years after treatment.
No significant differences were observed for the received treatment or the number of treatment lines. The number of comorbidities was associated with lower HRQoL experiences in general health and physical functioning.
4 Discussion
4.1 Results in context
Our study extends previous quality of life research in oncology through the analysis of a large national sample of sarcoma patients with standardized follow-up over a 1-year period. As expected, in our heterogeneous population of sarcoma patients, differences were found between factors studied in both longitudinal analyses.
The observed differences between gender and age-groups in Analyses 1 and 2 are reported in almost all HRQoL studies in cancer populations (29). It is noteworthy that patients between 55-<65 years (in addition to those ≥75) represented the most restricted age group. This implies that reaching retirement age is accompanied by a temporary improvement in various quality-of-life domains, possibly associated with retirement itself, an aspect we previously reported in more detail for a cross sectional analysis of the data (16). Differences between women and men seemed to be larger in patients in complete remission compared to all patients. The association between HRQoL and SES was already observed in the aforementioned study, indicating that a holistic approach to health always should include the social-economic situation of patients.
To our knowledge, there is little sarcoma specific literature on the relation of HRQoL and the analyzed lifestyle factors sporting activities (30, 31), smoking, and alcohol consumption, even if the importance of maintaining physical activity is discussed (32–34). Sporting activities were in both analyses and across all domains associated with improved HRQoL. In the literature about cancers in general, this observation is well established (35, 36). However, our study design – even if longitudinal – does not allow causal conclusions, as it remains possible that a better HRQoL enables sporting activities and is not the result of it. This may be particularly obvious in the case of role functioning (fulfilling everyday tasks), which can conceptually include sporting activities. In the analysis of all patients, former smoking, but not current smoking, was associated with deteriorated HRQoL. It might be the case, that decreased HRQoL lead to smoking cessation. In the analysis of patients in complete remission, however, current smoking was associated with poorer HRQoL. This association is well established in the literature (37–39).
Moderate alcohol consumption was associated with an improvement in HRQoL compared to no consumption in both analyzed groups. This at first glance counterintuitive result is observed in other studies (40–42) and likely reflects the fact, when alcohol consumption is widespread and socially acceptable as is the case for Germany (43), many of those who do not consume alcohol (anymore) may be doing so because they are too ill or weak to drink alcohol. So here we might observe reverse causality, too.
Exploring the relation between time since treatment and analyzed HRQoL domains, a heterogenous picture was revealed. While in Analysis 1 (all patients), a rapid improvement over time was observed for general health, for role functioning, and fatigue clinically relevant improvements were observed only 2 resp. 5 years post treatment, while pain did not improve at all significantly and physical functioning not in a clinically relevant manner. In Analysis 2 (complete remission), HRQoL did not improve regarding pain and fatigue and improved at different times in general health, physical, and role functioning. This ambiguous picture is somewhat reflected in the literature, where for different populations some studies reported improvements 1 year after treatment (44, 45), while others reported more stable trajectories (46, 47). As the study population in the complete remission analysis is more homogenous than in the all-patients analysis, conclusions are probably easier to draw from the former one. Here, the stable trajectory in pain and fatigue raises the question, whether there is room for improvement especially in follow-up care (48, 49).
In Analysis 1, the heterogeneity of sarcoma patients was reflected in the analysis of subgroups and tumor location (15, 16). In Analysis 2, those differences did not remain statistically significant, which might be, at least partly a result of the smaller sample size. The exception are bone sarcoma patients, which were in both analyses stronger affected by functional impairments and lower general health than liposarcoma patients. Van Eck et al. reported that patients with sarcomas of the axial skeleton were the most affected group, a location that we did not document separately (15).
Patients treated with surgery alone had the lowest restrictions in terms of functional impairment and symptom burden in the all-patients analysis. Patients treated with surgery + ST + RT were most affected in all other domains, with the exception of pain, where patients with surgery + RT reported strongest symptoms. Interestingly, no differences were observed in the complete remission cohort. Winnette et al. reported increased burden after CT and RT, as well (50). Further, van Eck et al. compiled a comprehensive list of problems associated with specific treatments (15). Van Tine et al. observed a relatively rapid decline in HRQoL during doxorubicin-based treatment (51). An ongoing observational cohort study is investigating effects of CT on HRQoL (52).
As expected, progressive disease and the number of comorbidities were significantly and relevantly associated with most domains (53).
Overall, our research extends the existing knowledge on the HRQoL in sarcoma patients by providing a comprehensive and longitudinal analysis of a diverse national sample. Moreover, the inclusion of lifestyle factors, socio-economic status, the examination of time since treatment and disease-related factors add valuable insights to the current understanding of HRQoL in this patient population. We were thus able to capture a more holistic picture of the disease.
4.2 Strength and limitations
The PROSa study is one of the largest studies on HRQoL in sarcoma patients and survivors worldwide. Patients from 39 German hospitals and practices were included, representing a broad spectrum of sarcoma treating facilities and disciplines. We were able to follow patients for one year and thus to collect and analyze longitudinal data. The analysis has a limitation in the heterogenous patients collective. Despite being able to collect information about a relatively large number of patients, heterogeneity of the disease makes a subgroup analysis difficult. We were not able to compute interaction-analyses, especially on potential different HRQoL-trajectories in sarcoma subgroups (type, location, or treatment).
Although the present study has a longitudinal design, causal conclusions should be drawn cautiously. As discussed with respect to sporting activities, changes in HRQoL outcomes may have occurred before changes in independent variables. Unobserved or spurious confounding is also possible and the study is subject to selection bias. The majority of our patients were recruited in university hospitals and/or specialized centers and thus might not be representative for all sarcoma patients. In addition, we suspect a sick survivor bias, as healthy survivors have less frequent contact with our recruiting study centers. For Analysis 1, it should additionally be considered, that, as patients were in most cases recruited during hospital visits, the probability that the course of HRQoL over time is influenced by a subsequent treatment or worsening of disease is higher than in a sarcoma population recruited at a random timepoint. Our study population changed over the course of one-year, with younger patients and men being overrepresented in non-participants during follow-up, and there is the possibility that this influenced our results.
5 Conclusion
The heterogeneity of sarcomas regarding type, location, and treatment is reflected in the HRQoL outcomes in the analysis of all sarcoma patients, but only to a certain extent in the complete remission cohort. Bone sarcoma patients were in both analyses the most affected sarcoma type, while significant differences regarding location (patients with tumors located at the lower extremities performed worst and those with sarcomas at the upper extremities best) and treatment (having received radiotherapy and/or systemic therapy was associated with lower HRQoL in some domains) were only found in the analysis of all patients.
In both cohorts, sociodemographic factors like age, sex, and socioeconomic status were associated with HRQoL as well. Patients between 55-<65 years of age were the most affected group, indicating that certain life circumstances, like work, may increase the disease burden.
Lifestyle factors, especially sporting activities were strongly associated with HRQoL outcomes. Additionally, smokers had a higher probability of experiencing deteriorated HRQoL scores. It is thus important that clinicians are aware of these factors and take them into account and address them during treatment and follow-up. They should be considered in the development of supportive care programs.
Outcomes improved in both analyses over time since treatment, albeit in different patterns. Patients in ongoing complete remission improved over time in global health, physical, and role functioning. Such improvements were not observed for fatigue and pain. These findings can inform healthcare professionals and policymakers in developing targeted interventions and support services to enhance the well-being and overall quality of life for sarcoma patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics committees of the Technical University of Dresden. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
ME wrote the article and analyzed the data. ME, MS, and LH developed questionnaires and study design. JS and MS developed the conception of the study and supervised with MB the work throughout the whole study. EW supervised development of inclusion criteria. KA supervised the study from a patient’s perspective. ME and SS developed the statistical analysis plan for this paper. OS supervised statistical analysis. HJ did scientific editing and developed visualizations. SR, CH, PH, BK, DA, DP, JJ, RG, SF, KH-M, MF, JW, K-DS, and MS were responsible for the recruitment of patients or recruited patients directly. All authors have revised the manuscript critically and approved the published version.
Funding
The PROSa study was funded by the German Cancer Aid (No. 111713). ME, HJ, and MB received support by the German Cancer Aid, Mildred Scheel Early Career Center P2. The Article Processing Charges (APC) were funded by the joint publication funds of the TU Dresden, including Carl Gustav Carus Faculty of Medicine, and the SLUB Dresden as well as the Open Access Publication Funding of the DFG.
Conflict of interest
LH received fees from SERVIER, outside of this work. SS received lecture fees from Lilly, Pfizer and fees for consulting services from Content Ed Net, all outside of this work. SR - received fees for consulting services from Bayer, PharmaMar, Boehringer Ingelheim and fees for lectures PharmaMar, all outside of this work. DA received lecture fees from PharmaMar, outside of this work. DP received fees for consulting services from Lilly, PharmaMar, Roche and fees for lectures from Lilly, PharmaMar, all outside of this work. JJ received fees from Lilly and Boehringer Ingelheim, all outside of this work. SF received reimbursements for congress attendance fees from PharmaMar, all outside of this work. OS received consulting fees from Novartis outside of this work. JS received consulting fees from Novartis, Sanofi, ALK, and Lilly, all outside of this work. MS received research funding from PharmaMar and Novartis, all outside of this work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ressing M, Wardelmann E, Hohenberger P, Jakob J, Kasper B, Emrich K, et al. Strengthening health data on a rare and heterogeneous disease: sarcoma incidence and histological subtypes in Germany. BMC Public Health (2018) 18(1):235. doi: 10.1186/s12889-018-5131-4
2. Stiller CA, Trama A, Serraino D, Rossi S, Navarro C, Chirlaque MD, et al. Descriptive epidemiology of sarcomas in Europe: Report from the RARECARE project. Eur J Cancer (2013) 49(3):684–95. doi: 10.1016/j.ejca.2012.09.011
3. Survival Rates for Soft Tissue Sarcoma. Available at: https://www.cancer.org/cancer/soft-tissue-sarcoma/detection-diagnosis-staging/survival-rates.html.
4. Organisation mondiale de la santé, Centre international de recherche sur le cancer. Soft tissue and bone tumours. 5th ed. Geneva: OMS: World health organization classification of tumours (2020).
5. Gronchi A, Miah AB, Tos APD, Abecassis N, Bajpai J, Bauer S, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol (2021) 32(11):1348–65. doi: 10.1016/j.annonc.2021.07.006
6. Soomers V, Husson O, Young R, Desar I, van der Graaf W. The sarcoma diagnostic interval: a systematic review on length, contributing factors and patient outcomes. ESMO Open (2020) 5(1):e000592. doi: 10.1136/esmoopen-2019-000592
7. Traub F, Griffin AM, Wunder JS, Ferguson PC. Influence of unplanned excisions on the outcomes of patients with stage III extremity soft-tissue sarcoma: Outcome of Unplanned Excisions in STS. Cancer (2018) 124(19):3868–75. doi: 10.1002/cncr.31648
8. Kang S, Kim HS, Han I. Unplanned excision of extremity soft tissue sarcoma in korea: A nationwide study based on a claims registry. PloS One (2015) 10(8):e0134354. doi: 10.1371/journal.pone.0134354
9. Keung EZ, Chiang YJ, Cormier JN, Torres KE, Hunt KK, Feig BW, et al. Treatment at low-volume hospitals is associated with reduced short-term and long-term outcomes for patients with retroperitoneal sarcoma. Cancer (2018) 124(23):4495–503. doi: 10.1002/cncr.31699
10. Gutierrez JC, Perez EA, Moffat FL, Livingstone AS, Franceschi D, Koniaris LG. Should soft tissue sarcomas be treated at high-volume centers? An analysis of 4205 patients. Ann Surg (2007) 245(6):952–8. doi: 10.1097/01.sla.0000250438.04393.a8
11. Dangoor A, Seddon B, Gerrand C, Grimer R, Whelan J, Judson I. UK guidelines for the management of soft tissue sarcomas. Clin Sarcoma Res (2016) 6(1):20. doi: 10.1186/s13569-016-0060-4
12. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF. S3-Leitlinie Adulte Weichgewebesarkome, Langversion Version 1.0, 2021, AWMF-Registernummer: 032/044OL. Available at: https://www.leitlinienprogramm-onkologie.de/leitlinien/adulte-weichgewebesarkome.
13. Shrestha A, Martin C, Burton M, Walters S, Collins K, Wyld L. Quality of life versus length of life considerations in cancer patients: A systematic literature review. Psychooncology (2019) 28(7):1367–80. doi: 10.1002/pon.5054
14. Webster KA, Peipert JD, Lent LF, Bredle J, Cella D. The functional assessment of chronic illness therapy (FACIT) measurement system: guidance for use in research and clinical practice. In: Kassianos AP, editor. Handbook of Quality of Life in Cancer. Cham: Springer International Publishing (2022). p. 79–104. doi: 10.1007/978-3-030-84702-9_6
15. van Eck I, den Hollander D, Desar IME, Soomers VLMN, van de Sande MAJ, de Haan JJ, et al. Unraveling the heterogeneity of sarcoma survivors’ Health-related quality of life regarding primary sarcoma location: results from the SURVSARC study. Cancers (2020) 12(11):3083. doi: 10.3390/cancers12113083
16. Eichler M, Hentschel L, Richter S, Hohenberger P, Kasper B, Andreou D, et al. The health-related quality of life of sarcoma patients and survivors in Germany—Cross-sectional results of a nationwide observational study (PROSa). Cancers (2020) 12(12):3590. doi: 10.3390/cancers12123590
17. McDonough J, Eliott J, Neuhaus S, Reid J, Butow P. Health-related quality of life, psychosocial functioning, and unmet health needs in patients with sarcoma: A systematic review. Psycho-Oncology (2019) 28(4):653–64. doi: 10.1002/pon.5007
18. Almeida A, Martins T, Lima L. Patient-Reported Outcomes in Sarcoma: A scoping review. Eur J Oncol Nursing (2021) 50:101897. doi: 10.1016/j.ejon.2021.101897
19. den Hollander D, der Graaf WTAV, Fiore M, Kasper B, Singer S, Desar IME, et al. Unravelling the heterogeneity of soft tissue and bone sarcoma patients’ health-related quality of life: a systematic literature review with focus on tumour location. ESMO Open (2020) 5(5):1–39. doi: 10.1136/esmoopen-2020-000914
20. den Hollander D, Fiore M, Martin-Broto J, Kasper B, Casado Herraez A, Kulis D, et al. Incorporating the patient voice in sarcoma research: how can we assess health-related quality of life in this heterogeneous group of patients? A study protocol. Cancers (2020) 13(1):1. doi: 10.3390/cancers13010001
21. Husson O, den Hollander D, van der Graaf WTA. The complexity of assessing health-related quality of life among sarcoma patients. Qual Life Res (2020) 29(10):2613–4. doi: 10.1007/s11136-020-02561-y
22. Eichler M, Schmitt J, Schuler MK. Die Dauer von Ethikvoten in Deutschland am Beispiel einer nicht-interventionellen Beobachtungsstudie mit 44 teilnehmenden Zentren (PROSa). Z für Evidenz Fortbildung und Qualität im Gesundheitswesen (2019) 146:15–20. doi: 10.1016/j.zefq.2019.07.006
23. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Informatics (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
24. Eichler M, Andreou D, Golcher H, Hentschel L, Richter S, Hohenberger P, et al. Utilization of interdisciplinary tumor boards for sarcoma care in Germany: results from the PROSa study. ORT (2021) 44(6):301–12. doi: 10.1159/000516262
25. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
26. Cocks K, King MT, Velikova G, Martyn St-James M, Fayers PM, Brown JM. Evidence-based guidelines for determination of sample size and interpretation of the european organisation for the research and treatment of cancer quality of life questionnaire core 30. JCO (2011) 29(1):89–96. doi: 10.1200/JCO.2010.28.0107
27. Lampert T, Kroll LE, Müters S, Stolzenberg H. Messung des sozioökonomischen Status in der Studie “Gesundheit in Deutschland aktuell” (GEDA). Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz (2013) 56(1):131–43. doi: 10.1007/s00103-012-1583-3
28. Fuchs R, Klaperski S, Gerber M, Seelig H. Messung der Bewegungs- und Sportaktivität mit dem BSA-Fragebogen: Eine methodische Zwischenbilanz. Z für Gesundheitspsychol (2015) 23:60–76. doi: 10.1026/0943-8149/a000137
29. Schwarz R, Hinz A. Reference data for the quality of life questionnaire EORTC QLQ-C30 in the general German population. Eur J Cancer (2001) 37(11):1345–51. doi: 10.1016/S0959-8049(00)00447-0
30. Mason G, Aung L, Gall S, Meyers P, Butler R, Krug S, et al. Quality of life following amputation or limb preservation in patients with lower extremity bone sarcoma. Front Oncol (2013) 3:210. doi: 10.3389/fonc.2013.00210
31. Refaat Y, Gunnoe J, Hornicek FJ, Mankin HJ. Comparison of quality of life after amputation or limb salvage. Clin Orthopaedics Related Research® (2002) 397:298. doi: 10.1097/00003086-200204000-00034
32. Dewhurst S, Tigue R, Sandsund C, Mein G, Shaw C. Factors influencing people’s ability to maintain their activity levels during treatment for soft tissue sarcoma - A qualitative study. Physiother Theory Pract (2020) 36(8):923–32. doi: 10.1080/09593985.2018.1519622
33. Garcia MB, Ness KK, SChadler KL. Exercise and physical activity in patients with osteosarcoma and survivors. Adv Exp Med Biol (2020) 1257:193–207. doi: 10.1007/978-3-030-43032-0_16
34. Ranft A, Seidel C, Hoffmann C, Paulussen M, Warby AC, van den Berg H, et al. Quality of survivorship in a rare disease: clinicofunctional outcome and physical activity in an observational cohort study of 618 long-term survivors of ewing sarcoma. J Clin Oncol (2017) 35(15):1704–12. doi: 10.1200/JCO.2016.70.6226
35. Stout NL, Baima J, Swisher AK, Winters-Stone KM, Welsh J. A systematic review of exercise systematic reviews in the cancer literature (2005-2017). PM R (2017) 9(9S2):S347–84. doi: 10.1016/j.pmrj.2017.07.074
36. Posadzki P, Pieper D, Bajpai R, Makaruk H, Könsgen N, Neuhaus AL, et al. Exercise/physical activity and health outcomes: an overview of Cochrane systematic reviews. BMC Public Health (2020) 20(1):1724. doi: 10.1186/s12889-020-09855-3
37. Goldenberg M, Danovitch I, IsHak WW. Quality of life and smoking. Am J Addict (2014) 23(6):540–62. doi: 10.1111/j.1521-0391.2014.12148.x
38. Piper ME, Kenford S, Fiore MC, Baker TB. Smoking cessation and quality of life: changes in life satisfaction over 3 years following a quit attempt. Ann Behav Med (2012) 43(2):262–70. doi: 10.1007/s12160-011-9329-2
39. Underner M, Perriot J, Merson F, Peiffer G, Meurice JC. [Influence of tobacco smoking on quality of life in patients with lung cancer]. Rev Mal Respir (2015) 32(6):586–98. doi: 10.1016/j.rmr.2014.08.011
40. Eichler M, Keszte J, Meyer A, Danker H, Guntinas-Lichius O, Oeken J, et al. Tobacco and alcohol consumption after total laryngectomy and survival: A German multicenter prospective cohort study: Tobacco and alcohol consumption after laryngectomy. Head Neck (2016) 38(9):1324–9. doi: 10.1002/hed.24436
41. Révész D, Bours MJL, Wegdam JA, Keulen ETP, Breukink SO, Slooter GD, et al. Associations between alcohol consumption and anxiety, depression, and health-related quality of life in colorectal cancer survivors. J Cancer Surviv (2022) 16(5):988–97. doi: 10.1007/s11764-021-01090-y
42. Zhang FF, Hudson MM, Huang IC, Bhakta N, Ness KK, Brinkman TM, et al. Lifestyle factors and health-related quality of life in adult survivors of childhood cancer: A report from the St. Jude Lifetime Cohort Study Cancer (2018) 124(19):3918–23. doi: 10.1002/cncr.31647
43. Our World in Data. Alcohol consumption across the world today. Available at: https://ourworldindata.org/alcohol-consumption.
44. Sun YJ, Hu YJ, Jin D, Li JW, Yu B. Health-related quality of life after treatment for Malignant bone tumors: a follow-up study in China. Asian Pac J Cancer Prev (2012) 13(7):3099–102. doi: 10.7314/APJCP.2012.13.7.3099
45. Rivard JD, Puloski SS, Temple WJ, Fyfe A, Kwan M, Schachar N, et al. Quality of life, functional outcomes, and wound complications in patients with soft tissue sarcomas treated with preoperative chemoradiation: a prospective study. Ann Surg Oncol (2015) 22(9):2869–75. doi: 10.1245/s10434-015-4490-7
46. Paredes T, Pereira M, Moreira H, Simões MR, Canavarro MC. Quality of life of sarcoma patients from diagnosis to treatments: Predictors and longitudinal trajectories. Eur J Oncol Nursing (2011) 15(5):492–9. doi: 10.1016/j.ejon.2011.01.001
47. Davidson D, Barr RD, Riad S, Griffin AM, Chung PW, Catton CN, et al. Health-related quality of life following treatment for extremity soft tissue sarcoma: HRQL in Extremity Soft Tissue Sarcoma. J Surg Oncol (2016) 114(7):821–7. doi: 10.1002/jso.24424
48. Smith SR. Rehabilitation strategies and outcomes of the sarcoma patient. Phys Med Rehabil Clin N Am (2017) 28(1):171–80. doi: 10.1016/j.pmr.2016.08.008
49. Andrews CC, Siegel G, Smith S. Rehabilitation to improve the function and quality of life of soft tissue and bony sarcoma patients. Patient Relat Outcome Meas. (2019) 10:417–25. doi: 10.2147/PROM.S130183
50. Winnette R, Hess LM, Nicol SJ, Tai DF, Copley-Merriman C. The patient experience with soft tissue sarcoma: A systematic review of the literature. Patient (2017) 10(2):153–62. doi: 10.1007/s40271-016-0200-1
51. Van Tine BA, Krarup-Hansen A, Hess LM, Abdul Razak AR, Soldatenkova V, Wright J, et al. Quality of life of patients with soft tissue sarcoma treated with doxorubicin in the ANNOUNCE phase III clinical trial. Rare Tumors (2022) 14:20363613221100030. doi: 10.1177/20363613221100033
52. Younger E, Jones RL, Desar IME, Peckitt C, van der Graaf WTA, Husson O. Health-related quality Of Life In patients with advanced Soft TIssue sarcomas treated with Chemotherapy (The HOLISTIC study): protocol for an international observational cohort study. BMJ Open (2020) 10(6):e035171. doi: 10.1136/bmjopen-2019-035171
Keywords: sarcoma, GIST, health-related quality of life, patient reported outcomes, EORTC QLQ-C30, longitudinal observational cohort
Citation: Eichler M, Hentschel L, Singer S, Hornemann B, Richter S, Hofbauer C, Hohenberger P, Kasper B, Andreou D, Pink D, Jakob J, Grützmann R, Fung S, Wardelmann E, Arndt K, Hermes-Moll K, Schoffer O, Fried M, Jambor HK, Weitz J, Schaser K-D, Bornhäuser M, Schmitt J and Schuler MK (2023) Health related Quality of Life over time in German sarcoma patients. An analysis of associated factors - results of the PROSa study. Front. Endocrinol. 14:1166838. doi: 10.3389/fendo.2023.1166838
Received: 15 February 2023; Accepted: 01 August 2023;
Published: 29 August 2023.
Edited by:
Liam Chen, University of Minnesota, United StatesReviewed by:
Volker Arndt, German Cancer Research Center (DKFZ), GermanyNadia Ayub, Institute of Business Management, Pakistan
Copyright © 2023 Eichler, Hentschel, Singer, Hornemann, Richter, Hofbauer, Hohenberger, Kasper, Andreou, Pink, Jakob, Grützmann, Fung, Wardelmann, Arndt, Hermes-Moll, Schoffer, Fried, Jambor, Weitz, Schaser, Bornhäuser, Schmitt and Schuler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martin Eichler, bWFydGluLmVpY2hsZXJAdWtkZC5kZQ==