 Andressa Karoline Pinto de Lima Ribeiro1,2Josilayne Patrícia Ramos Carvalho2,3
Andressa Karoline Pinto de Lima Ribeiro1,2Josilayne Patrícia Ramos Carvalho2,3 Natáli Valim Oliver Bento-Torres1,2,3*
Natáli Valim Oliver Bento-Torres1,2,3*- 1Graduate Program in Attention and Clinical Study in Diabetes, Institute of Medical Sciences, Federal University of Pará, Belém, Pará, Brazil
- 2Neurodegeneration and Infection Research Laboratory, João de Barros Barreto University Hospital, Federal University of Pará, Belém, Pará, Brazil
- 3Graduate Program in Human Movement Sciences, Institute of Health Sciences, Federal University of Pará, Belém, Brazil
Background: Type 2 diabetes mellitus (T2DM) is a leading cause of disability-adjusted life years (DALY). Physical exercise is an effective non-pharmacological intervention to promote glycaemic control in T2DM. However, the optimal exercise parameters for glycemic control in individuals with T2DM remain unclear.
Objective: This study aimed to analyze the relationship between physical training variables – frequency, intensity, type, duration, volume, and progression – and glycemic control in individuals with T2DM.
Methods: A rapid systematic literature review was conducted on PubMed and LILACS databases. The PICOT strategy was employed to define the inclusion criteria. Eligible studies had to assess the impact of exercise parameters (frequency, intensity, type, duration, volume, and progression) on glycemic control indicators, primarily glycosylated hemoglobin (HbA1c). Randomized and non-randomized clinical trials were included in the review. The methodological quality of each study was assessed using the PEDro scale (PROSPERO - CRD 42021262614).
Results: Out of 1188 papers initially identified, 18 reports met the inclusion criteria and were included in the analysis. A total of 1,228 participants with T2DM (1086 in exercise groups) were included in the selected studies. Among these studies, 16 (88.9%) were RCTs and 2 (11.1%) were nRCTs. The age of participants ranged from 43.1 and 68.9 years, and the average intervention duration was 16.8 weeks. Data on adherence to the intervention, adverse events, detailed intervention protocol, and its impacts on glycaemic control, lipid profile, blood pressure, anthropometric measures, medication, body composition, and physical fitness are reported.
Conclusion: The evidence supports the safety and effectiveness of physical exercises as non-pharmacological interventions for glycemic control. Aerobic, resistance and combined training interventions were associated with reductions in HbA1c and fasting glucose. The diversity of the physical exercise intervention protocols investigated in the studies included in this review is an important limitation to generalizing evidence-based practice. The call for action is mandatory to implement large-scale education programs on the prevention of diabetes and public health policies aimed to include well-planned and supervised exercise programs as an essential part of the primary prevention of type 2 diabetes.
Systematic Review Registration: PROSPERO, identifier (CRD42021262614).
1 Introduction
The prevalence of diabetes worldwide is rapidly increasing, with estimates suggesting a rise from 536.6 million adults (20–79 years) in 2021 to 783.2 million in 2045 (1). Type 2 diabetes mellitus (T2DM) is the third leading cause of increased disability-adjusted life years (DALY) among individuals aged 50 to 74 (2). Diabetes is associated with various complications such as blindness, kidney failure, heart attacks, stroke, and lower limb amputation. Furthermore, the age-standardized DALYs caused by T2DM in the Americas in 2019 were 29% greater than the global burden and increased by 27.4% from 1990 onwards (3). Diabetes is an economic burden, challenging public health policies worldwide. The direct costs associated with hospitalizations, outpatient procedures, and diabetes medications reached USD 966 billion in 2021 (1). Type 2 diabetes is responsible for an average of 5.4 quality-adjusted life-years (QALYs) lost and for limitations on occupational and daily activities (2, 4).
The treatment of T2DM requires physical exercise, a balanced diet, and medication (5). Well-planned, evidence-based, and supervised physical exercise is a cost-effective therapeutic strategy for managing T2DM, reducing insulin resistance, improving muscle glucose utilization, enhancing insulin sensitivity (6), and increasing QALY (7). Furthermore, exercise offers additional health benefits, including decreased cardiovascular disease risk, enhanced physical fitness, weight maintenance, and improved mental well-being and quality of life for individuals with diabetes (8–10).
Physical exercise should be tailored to meet the specific personal and clinical needs of each patient (11). An individualized exercise program is crucial for therapeutic success, although there are general guidelines (9, 12–16). Properly prescribed and executed physical exercise offers significant benefits to individuals with T2DM, serving as an effective tool for metabolic management and a non-pharmacological strategy for the prevention and treatment of T2DM in adults and older adults (9, 13). The dose of physical training, encompassing frequency, intensity, type, duration, volume, and progression of exercise, plays a pivotal role in determining the extent of the training response (5, 17–21).
Frequently, there is a lack of detailed information in papers regarding exercise training parameters to estimate the exercise dose-response, along with methodological differences between studies (22). This scenario limits our understanding of the role that frequency, intensity, type, duration, volume, and progression of the exercise play an effective glycemic control. Also, the lack of evidence-based information for the exercise professional compromises the individualized training protocols for individuals with T2DM. The primary objective of this study was to analyze the relationship between the variables of aerobic, resistance, and combined physical training and glycemic control in individuals with T2DM through a rapid systematic literature review.
2 Methods
We conducted a rapid literature review to investigate the effects of physical exercise interventions on glycemic control in adults with Type 2 Diabetes Mellitus (T2DM). We analyzed the exercise parameters of frequency, intensity, type, duration, volume, and progression. The review protocol was registered at PROSPERO (International Prospective Register of Systematic Reviews) under number CRD 42021262614. We followed the PRISMA Guideline (23) to report the results.
2.1 Eligibility criteria
We used the PICOT strategy to define the eligibility criteria. Population: Studies with Type 2 Diabetes Mellitus participants aged 45 years or older. Intervention: Physical exercise interventions, including aerobic, resistance, or combined exercises, with at least one modifiable variable in the individualized exercise prescription (frequency, intensity, type, duration, volume, or progression). Comparison: T2DM participants on different types of physical training or usual diabetes care. Outcome: The impact of modifiable exercise variables on glycosylated hemoglobin (HbA1c) and additionally on other glycemic control indicators. Type of Study: Randomized and non-randomized clinical trials. Only articles published in English or Portuguese, between 2012 and February 2023, were included.
Exclusion criteria: We excluded systematic reviews, meta-analyses, and observational studies. Studies that did not assess HbA1c, interventions exclusively based on education for an active lifestyle or mind-body therapies (except Pilates), unpublished studies, and gray literature were also excluded.
2.2 Information sources and search strategy
We conducted searches in the PubMed and LILACS databases. We used the following search strategy: (“Diabetes Mellitus Type 2” OR Diabetes OR DM2 OR “Diabetes Mellitus, Type 2”) AND (“Physical Exercise” OR “Circuit-based Exercise” OR “Resistance Training” OR “Aerobic Training” OR Exercise OR “Resistance Training” OR “Circuit-based Exercise”). The searches were conducted until February 2023.
2.3 Data selection
The study selection process consisted of four stages: Identification, screening by title and abstract, eligibility assessment, and inclusion. During the identification stage, we collected all papers found during the search process and searched for duplicates. At the screening stage, we analyzed the titles, abstracts, and keywords of the identified studies and excluded articles that did not meet the selection criteria. Two authors independently reviewed each record retrieved from the search, and articles that clearly did not meet the criteria were eliminated.
In the eligibility assessment stage, we conducted a full read of the articles to confirm their suitability for inclusion. Each article was independently read by two researchers, and any divergences regarding eligibility were discussed in a consensus meeting. Divergence occurred in only seven (8.86%) of the articles read in full, and two papers were included in the review after discussion (24, 25). We used the Zotero software for reference management.
2.4 Data collection process
Two authors independently extracted the following data, when available: authorship, publication date, study design details, sample size, age, sex proportion, inclusion criteria for participants, exercise variables (frequency, intensity, type, duration, volume, and progression), monitoring strategy, outcomes, follow-up time, and losses. If described, additional data such as diet, supervision, schedule, adherence, medication, and adverse effects were also collected.
Glycemic control through HbA1c measurement was considered the primary outcome of interest, with additional variables of interest including fasting and postprandial blood glucose, serum lipids and fractions, blood pressure, anthropometry/body composition, physical fitness, and medication changes.
2.5 Study risk of bias assessment
The methodological quality of each study was analyzed using the PEDro scale (Physiotherapy Evidence Database) (26). The assessment was based on the information described in each study. In case of doubt or missing information, the criterion was qualified as not meeting the PEDro scale recommendation. The final score on the PEDro scale is the sum of the number of criteria classified as satisfactory among criteria 2 to 11. Criterion 1, which assesses the study’s external validity, is not considered in the final score. Two independent researchers analyzed each clinical trial, and there was no disagreement on any evaluation item. For clinical trials indexed on PEDro, the database score was used (12, 24, 25, 27–35). PEDro score was not used as an exclusion criterion.
3 Results
3.1 Study selection
Initially, a total of 1188 records were identified, with no duplicates. After reviewing titles and abstracts, 79 articles were selected for full reading. Among these, 61 were excluded, and 18 articles met our inclusion criteria (12, 24, 25, 27–41). The detailed selection process and reasons for exclusion are described in Figure 1.
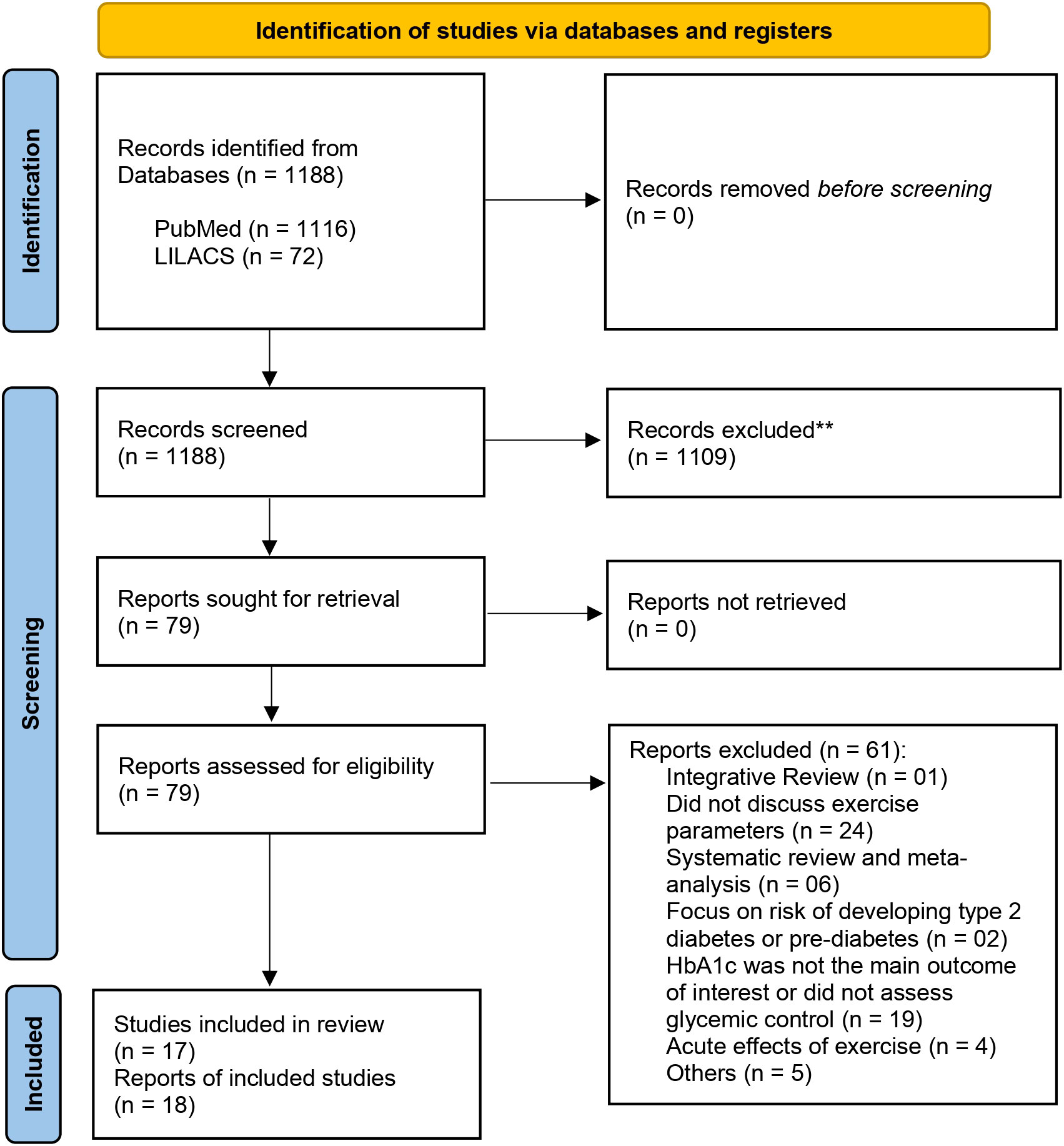
Figure 1 Flow diagram of studies selection and included in this review.
3.2 Characteristics of the included studies
A total of 1,228 participants with T2DM, aged between 43.1 and 68.9 years, were included in the studies. Among them, 1086 were allocated in exercise groups and 412 were allocated in non-exercised control groups. Sixteen of the included studies (88.9%) were randomized clinical trials, and 2 (11.1%) were non-randomized clinical trials, published between 2012 and 2022. The intervention length ranged from 10 to 52 weeks, with 66.67% of the interventions lasting between 12 and 16 weeks. Eight studies (44.4%) reported no adverse events during the intervention, four (22.2%) reported some minor events (such as back pain, tendinitis, hypoglycemia, or muscle injury), and six (33.3%) did not provide information on adverse events. The characteristics of the included studies are presented in Table 1.
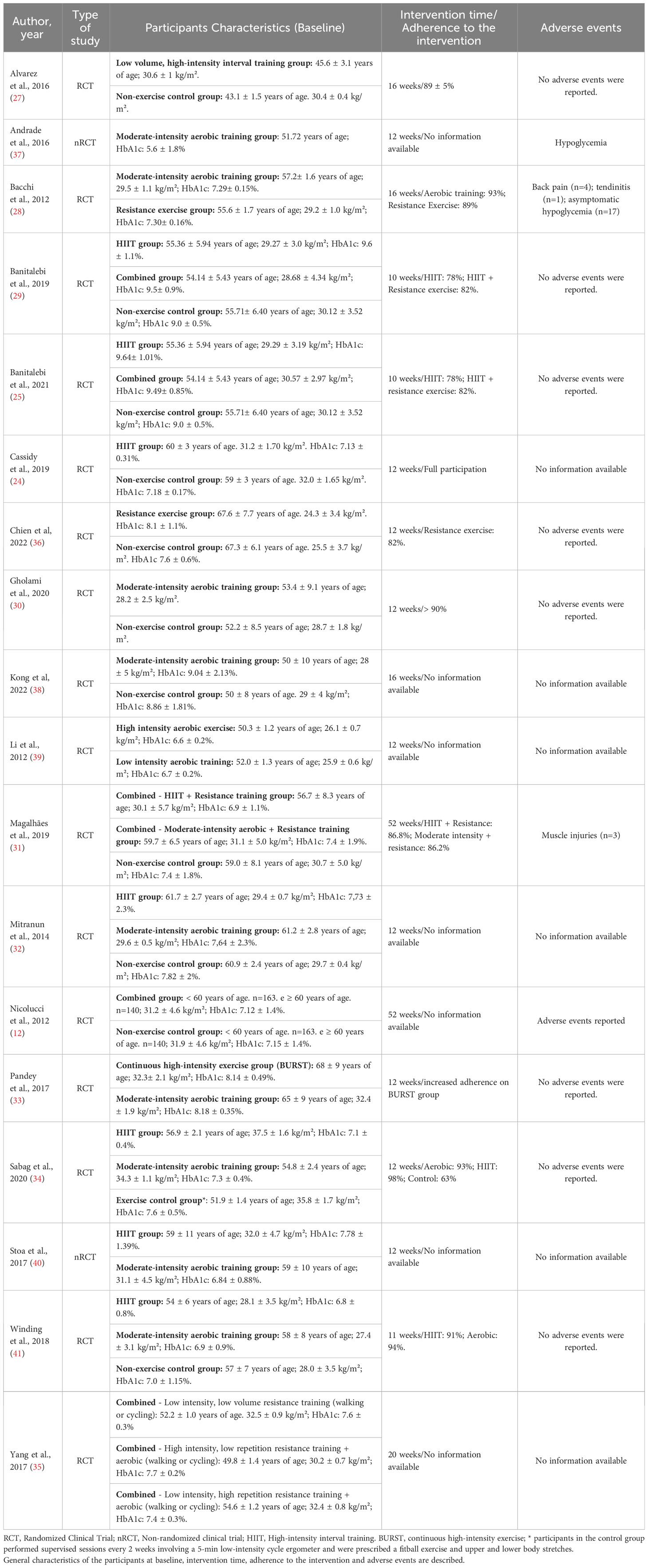
Table 1 Characteristics of clinical trials included in this review.
3.3 Risk of bias in studies
Four articles (22.2%) were considered to have a high risk of bias with scores below 5 on the PEDro scale (12, 24, 37, 40). Fourteen articles (77.8%) had moderate to high methodological quality, with scores ≥ 5 on the PEDro scale (25, 27–36, 38, 39, 41) (Table 2).
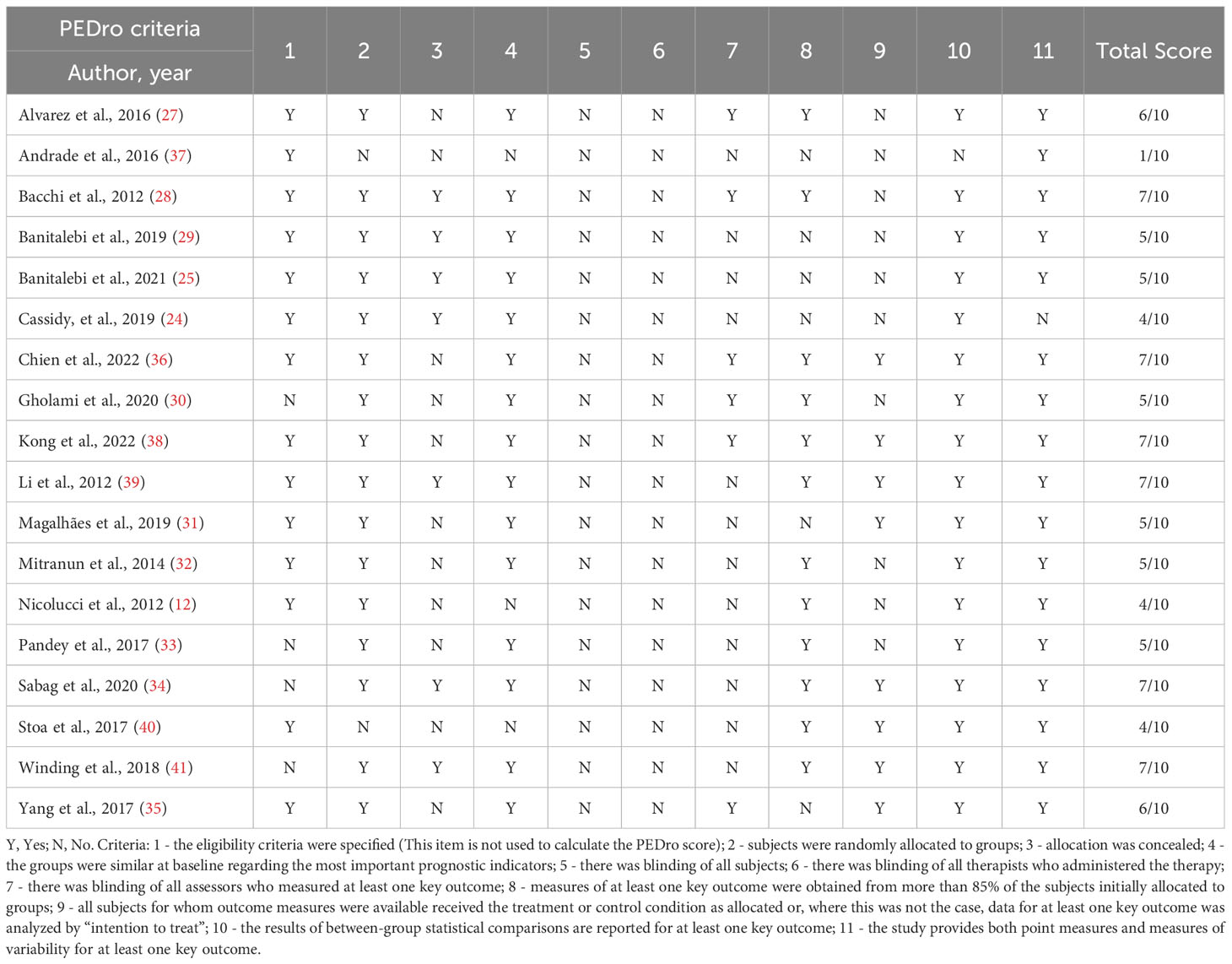
Table 2 Risk of bias assessment - PEDro Scale.
3.4 Characteristics of intervention protocols
Most articles reported the use of aerobic exercise as the primary intervention method. Ten studies utilized high-intensity interval training (HIIT) exercises, while ten used moderate-intensity exercises, primarily through ergometers such as treadmills and cycle ergometers. The duration of sessions varied from 15 to 90 minutes. Twelve papers (66.67%) reported to monitor exercise intensity: Nine used a heart rate monitor, two used a perceived exertion scale, and one used palpation of the carotid artery. In terms of frequency, eleven (78.6%) studies performed aerobic exercises three times a week, two (14.3%) studies five times a week, while one study reported performing three to five times a week without describing specific criteria (see Table 3).
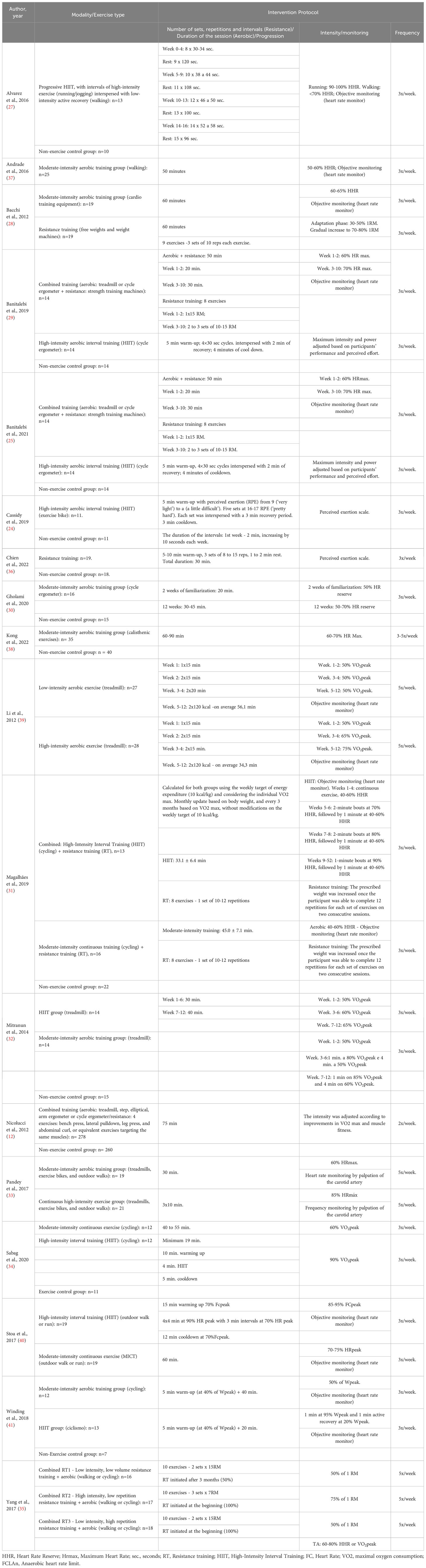
Table 3 Physical exercise protocols. Information on modality, type of exercise, duration, intensity, monitoring of intensity, frequency, and volume.
Resistance training as an exclusive modality was performed in two studies (10.52%). One study employed 60-minute high-intensity resistance training, three times a week, utilizing free weights and weightlifting machines (28). In the second study, participants performed 30-minute, home-based unsupervised, moderate-intensity exercises, following instructions from a booklet, three times a week (36).
Five papers (27.8%) reported combined training, which involved both aerobic and resistance exercises as a treatment approach, including low, moderate, and high-intensity interventions. The aerobic component of the training was performed through activities such as cycling, walking, or using ergometers, while the resistance component utilized weightlifting machines or free weights. The duration of sessions ranged between 20 and 75 minutes, twice to five times a week (12, 25, 29, 31, 35).
3.5 Impact of physical exercise intervention on glycemic control and other variables
HbA1c levels significantly decreased in the included reports, except for two of them (31, 39). Similar improvements in HbA1c levels were found after HIIT and combined training when compared to aerobic and resistance training (28). There are divergent results regarding the similar improvement induced in glycemic control after HIIT and moderate-intensity exercise (34) or combined exercise (25, 29) in contrast to the improvements achieved only after HIIT but not moderate-intensity aerobic training (32, 40, 41). Only one study compared high-intensity and moderate-intensity exercise and found that HbA1c levels were reduced in both groups, with a greater reduction after high-intensity training (33) (Table 4).
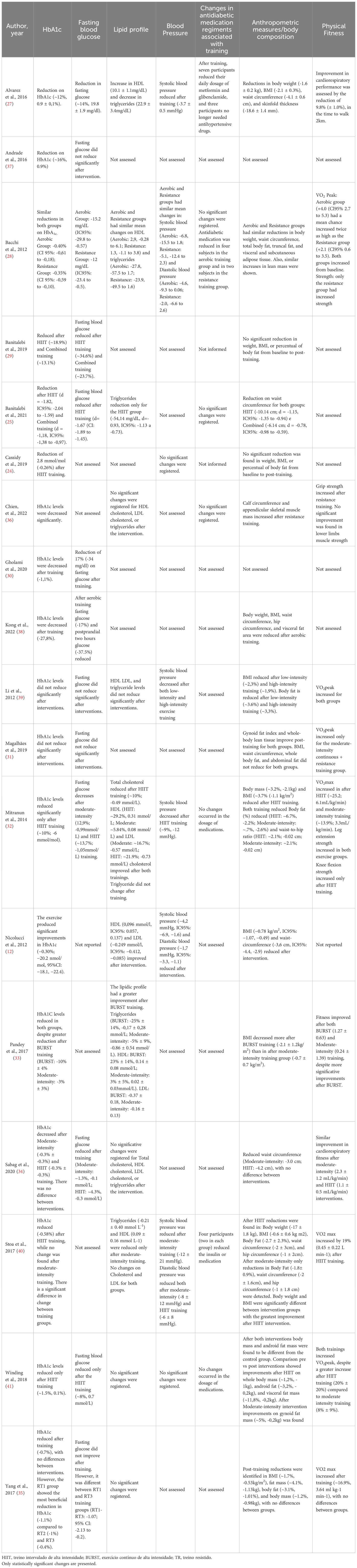
Table 4 Impact of physical exercise intervention protocols on glycemic control, lipid profile, blood pressure, anthropometric indicators, body composition, physical fitness, and medications in use.
A significant reduction in fasting blood glucose was reported after HIIT, moderate-intensity aerobic, resistance, or combined training (25, 27–30, 32, 34, 38, 41). Similar reductions in fasting blood glucose were reported when comparing aerobic and resistance training (28). Comparisons between HIIT and moderate-intensity or combined interventions show divergent results, with some studies showing similar improvements between intervention groups (29, 32), while others provide evidence to support that HIIT leads to superior results in reducing fasting glucose (25, 34, 41). Four studies reported non-significant results (31, 35, 37, 39).
HIIT induced improvements in blood pressure, anthropometric measures, body composition, and physical fitness (25, 27, 32, 34), but not under an unsupervised training program (24). HIIT had different impacts on the lipid profile, resulting in improvements (27, 32), but also no significant changes were reported (21, 26–28). Two studies found no significant changes in blood pressure (24, 41).
Only seven of the studies (38.9%) included in the present review assessed the impact of physical exercise interventions on the dosage of antidiabetic medication, reporting reductions in medication (27, 40), but also no exercise-induced modification in medication prescription (25, 28, 32, 36, 41).
Positive modifications in anthropometric measures, body composition, and physical fitness were described with similar results after the different intervention programs, most of them without clinically significant differences. HIIT and continuous high-intensity aerobic interventions showed superior improvements in aerobic fitness than moderate-intensity protocols. Coherently, aerobic training and muscular strength training were associated with improvements in cardiorespiratory fitness and muscular fitness, respectively.
4 Discussion
This study aimed to produce a literature synthesis, through a rapid review, on the effects of aerobic, resistance, and combined physical training variables on glycemic control in adults with type 2 Diabetes Mellitus. There is a strong body of evidence on the therapeutic effect of physical exercise on the prevention and treatment of T2DM (13, 16, 21, 42). However, previous studies have reported important heterogeneity in adherence rates and a low rate of patients with diabetes meeting the minimum amount of exercise recommended by guidelines (43, 44). The adaptation of physical exercise variables to the patient’s clinical needs, disease-specific symptoms, personal preferences, and time availability is important for long-term adherence to the exercise program (21, 43) and to an active lifestyle.
The studies included in the present review reported a significant reduction in HbA1c, regardless of the modality, duration, and frequency of exercise. However, regarding intensity one study investigated a low-intensity aerobic exercise and did not reach significant reductions in HbA1c, fasting glucose, or lipid profile (39). Other evidences found improved insulin sensitivity after an acute bout of low-intensity exercise, lasting for less than 24 hours (45) and also after a single low-intensity resistance training session (46). In this context, it is necessary to consider the importance of an active lifestyle and of even small amounts of exercise (8), and that low-intensity exercise may be an alternative for those patients at high risk for acute cardiovascular events, undergoing cardiac rehabilitation (21).
Superior effectiveness of HIIT for glycemic control was reported in the included studies in comparison to moderate-intensity (32, 40, 41) or combined training (25, 29, 32), except by one study that reported comparable effectiveness between HIIT and moderate-intensity training (34). Additionally, included studies that compared the metabolic benefits of HIIT to non-exercise control groups found improvements in HbA1c after interventions (24, 27, 32). These results add new and positive insight into previous inconclusive meta-analysis results in comparing HIIT vs moderate intensity exercise to reduce HbA1c levels (47), suggesting this modality as an efficient option for T2DM patients.
Only two reports from the same study (25, 29) compared a combined exercise program with another modality (HITT) and found the greatest percentual reduction after HIIT, despite a large effect size after both combined training or HITT on HbA1c reduction. This is in contradiction with previous studies showing that the greatest reduction in HbA1c is observed when using combined exercise compared to the other modalities alone (13, 48, 49). However, considering the limited information here available, it remains inconclusive if the combined training is more effective for glycemic control.
Resistance training comparably reduced HbA1c levels compared to aerobic exercise, with no statistical difference between the two groups (28), which supports previous findings (6, 29). However, a previous study (50) showed that while resistance exercise was effective and resulted in a -0.34% reduction in HbA1c with a large effect size, these reductions were not observed in individuals with a mean HbA1c level ≤ 7.5% (non-significant effect size), suggesting that a resistance exercise program alone may not effectively contribute to strict glycemic control in individuals with HBA1c values closer to the ideal range.
Previous results support that improvements in glycemic control induced by exercise are greater in individuals with higher HbA1c levels at baseline (51). We found mixed results on that, once the included studies that fail to find a reduction in HbA1c included participants within or near the recommended target of <7.0% for glycated hemoglobin baseline (31, 39, 40), but others got improvements after moderate-intensity, resistance, HIIT, and also combined training (12, 24, 28, 34, 37). In only one study with near to target patients HIIT, but not moderate-intensity exercise, promoted improvements in HbA1c (41). This result suggests that there are no preferential modalities to be indicated for patients with adequate glycemic control.
Not all the studies included in this review (30–32, 34, 36) meet the minimum of 150 minutes of moderate-intensity exercise per week or 75 minutes of combined moderate and high-intensity exercises, but all of them, except one (12) performed the minimum frequency recommended. The weekly frequency is an important factor to improve glycemic control and decrease cardiovascular risk in patients with T2DM (52). The recommendation that exercise should be performed with no more than 2 consecutive days between bouts of activity (13) is due to the transient exercise-induced sensitivity to insulin in individuals with T2D for up to 48 hours (21).
Structured exercise regimens exceeding 150 minutes per week have shown greater reductions in HbA1c levels compared to those with 150 minutes or less per week in individuals with type 2 diabetes (53). Two included papers from the same study (25, 29) were a shorter intervention (10 weeks) and found no positive impacts of the exercise on fasting glucose, lipidic profile, on medication dosage, and some measures of body composition. Moreover, the effects of physical exercise on HbA1c and BMI are found to be associated with interventions lengths, with an incremental decrease in HbA1c of 0.009 to 0.043% for each additional week of physical training, underscoring the importance of adherence to exercise for a sustained lifestyle change in achieving health improvements (41). However, a recent meta-analysis suggests that interventions longer than 12 weeks do not induce additional benefits on HbA1c (54). Taken together the results of the included studies reinforce the need for regularity and spacing between physical training sessions, but also the need for progression of the intervention intensity for adequate management and glycemic control (55).
Individuals with T2DM show a reduced maximal aerobic capacity which increases with disease duration. Although associations between poor glycemic control e reduced cardiorespiratory fitness had been established, the mechanisms are not fully understood (56). On the other hand, it is known that physical exercise may improve physical fitness in adults with diabetes (56). Cardiorespiratory fitness improvements were found in all studies included in the present review. As expected, the magnitude of the improvements was related to training modalities, with greater improvements due to aerobic and HIIT training, but also found after resistance and combined training, and in response to either interval, low-intensity, moderate- and high-intensity training (27, 28, 32–35, 39, 40). Divergent results were found showing improvements only after moderate-intensity or HIIT, but not both (31, 40). Greater improvement after HIIT or high-intensity continuous aerobic exercise vs Moderate-intensity was found (32, 33, 41). Strength was improved after resistance training (28, 32, 36) and also after HIIT and Moderate-intensity exercise in the lower limbs (32). Facing the diabetes-associated decline in fitness and the evidence of the improvement associated with aerobic capacity training and strength, it is mandatory its inclusion in exercise programs dedicated to individuals with diabetes.
Aerobic training interventions lead to improvements in cardiorespiratory fitness, with evidence of greater effectiveness of high-intensity interventions. Among the reviewed studies, only 50% reported objective monitoring of the exercise session by using heart rate monitors. By not monitoring heart rate, the accuracy of exercise intensity is reduced, and an important bias is added to the protocol analysis. High-intensity aerobic exercise has demonstrated superiority over moderate-intensity exercise in improving physical fitness measures such as VO2max and anthropometric indicators like body weight and BMI. The clinical implications of high-intensity aerobic exercise’s effectiveness in enhancing physical fitness are noteworthy, as VO2max serves as a predictor of cardiovascular risk, and its improvement is associated with decreased morbidity and mortality from cardiovascular diseases as well as a lower prevalence of diabetes (57)
We found that moderate-intensity and high-intensity exercises promoted reductions in HbA1C, but high-intensity seems to be more effective in regulating fasting glucose. In fact, only two studies did not report positive results on that variable. One of them (39) compared high vs low-intensity aerobic training in participants with baseline levels of HbA1C lower than 7.0% and overweight. The second one (31) compared HIIT + resistance training vs moderate-intensity + resistance training in obese participants with high MVPA at baseline, but did not control for modifications on medications and compliance with the program.
Improvements in fasting blood glucose levels, lipid profile, blood pressure, and changes in antidiabetic medication regiment are not consistently impacted by exercise modalities on the included studies. HIIT and moderate-intensity interventions most consistently showed positive impacts on fasting glucose levels and lipid profile. Some studies reported divergent results after combined training and no improvements after low-intensity aerobic training and resistance training. It is important to note that only one study was dedicated to investigating low-intensity and resistance training. Mixed results were found regarding modifications in the antidiabetic medication regiment associated with the physical training after HIIT, resistance training, and moderate intensity. Blood pressure reduced after HIIT, low intensity, moderate intensity, high intensity, resistance training, and combined training, but no significant changes after HIIT, moderate intensity were reported. These outcomes measures were not investigated in all included studies, as well, there are important differences in the intervention protocols. This heterogeneity limits the conclusion regarding those parameters. A core outcome set to be used in randomized controlled trials in type 2 diabetes was to provide greater uniformity and comparability between studies and, thus, generate information for clinical practice (58).
Participant adherence to the exercise intervention ranged from 78% to 93%, with no differences regarding modalities. The supervision of an exercise professional can improve exercise adherence and safety, particularly for physically inactive adults and individuals with chronic diseases initiating an exercise program, but individuals with T2DM show adequate adherence under different supervision regiment (43, 59, 60). An essential factor influencing participant adherence is the personal affinity with the chosen modality and the suitability of training to the personal routine, emphasizing the importance of respect for individual preferences in line with the principles of Evidence-Based Practice (50, 61).
Physical exercise is safe for individuals with T2DM. No adverse events or just minor events – including back pain, tendinitis, hypoglycemia, or muscle injuries – were described, and do not raise restrictions or contraindications for the practice of physical exercise by adults with type 2 diabetes. It is recognized that implementing screening protocols beyond routine diabetes care can mitigate the risk of exercise-induced adverse events in asymptomatic individuals with diabetes (15). However, precautions should be taken to avoid that the screening requirements do not lead to unnecessary barriers to initiating an exercise program (62), especially in individuals with limited or not covered by health insurance.
Randomized clinical trials are the gold standard in investigating dose-response, causal relationships, and efficacy of physical training interventions (22). The design of the exercise training clinical trials protocols needs to be detailed planned and reported, including frequency, intensity, type, duration, and progression. While the diversity of the intervention protocols included in this review is an important limitation to the evidence-based practice, its support the effectiveness and safety of the physical exercises, in different modalities and intensities, including HIIT, as non-pharmacological interventions for glycemic control in individuals with type 2 diabetes. The call for action is mandatory to implement large-scale education programs on the prevention of diabetes and public health policies aimed to include well-planned exercise programs as an essential part of the primary care for type 2 diabetes.
4.1 Study limitations
This review revealed great variety in the prescription of exercise protocols. Furthermore, a lack of sufficient information regarding the design of exercise interventions, particularly concerning the overall training volume, was observed. This limitation may prevent the assessment of adaptability and responsiveness to the performed exercises.
It is important to acknowledge other limitations, including the inclusion of non-randomized clinical trials and clinical trials with a high risk of bias. Additionally, the studies exhibited heterogeneity in exercise prescription variables, inadequate or non-existent descriptions of exercise progression, and a lack of supplementary information such as exercise adherence, timing, and adverse events.
At least, it is important to note that although our planned PICOT strategy included the population over 18 years of age, with no age limits, young adult, and older adult populations (≥ 65 years of age) are not significantly represented in the included studies. The studies included in this review have an average age group of 56.1 years old, within the minimum 43.1 and maximum of 68 years of age. In this scenario, it is recommended to take caution in extrapolating the information to older adults, especially over 70s, and young adults. Therefore, there is a gap in the literature regarding the impacts of physical exercise parameters as a nonpharmacological strategy for the treatment of people in these age groups with T2DM.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Author contributions
NB-T participated in the conception of the study, supervision, data analysis, interpretation of results, and writing. AR participated in the conception of the study, data extraction and analysis, interpretation of results, and writing. JC participated in the data extraction and analysis, interpretation of results, and writing. All authors contributed to the article and approved the submitted version.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. NVOB-T was supported by PROPESP/UFPA (PAPQ).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. International Diabetes Federation. IDF diabetes atlas (2021). Available at: www.diabetesatlas.org.
2. Vos T, Lim SS, Abbafati C, Abbas KM, Abbasi M, Abbasifard M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (2020) 396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9
3. Cousin E, Schmidt MI, Ong KL, Lozano R, Afshin A, Abushouk AI, et al. Burden of diabetes and hyperglycemia in adults in the Americas, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Diabetes Endocrinology. (2022) 10(9):655–67. doi: 10.1016/S2213-8587(22)00186-3
4. Diabetes State Burden Toolkit Technical Report. Centers for disease control and prevention (2016). Available at: https://nccd.cdc.gov/Toolkit/DiabetesBurden/YLL/QALY.
5. Riebe D, Ehrman JK, Liguori G, Magal M. ACSM’s guidelines for exercise testing and prescription. Tenth edition. Philadelphia, PA: American College of Sports Medicine’s guidelines for exercise testing and prescription. Philadelphia: Wolters Kluwer Health (2018).
6. Stanford KI, Goodyear LJ. Exercise and type 2 diabetes: molecular mechanisms regulating glucose uptake in skeletal muscle. Adv Physiol Education (2014) 38(4):308–14. doi: 10.1152/advan.00080.2014
7. Barbosa A, Whiting S, Ding D, Brito J, Mendes R. Economic evaluation of physical activity interventions for type 2 diabetes management: a systematic review. Eur J Public Health (2022) 32(Suppl 1):i56–66. doi: 10.1093/eurpub/ckac074
8. Colberg SR, Sigal RJ, Yardley JE, Riddell MC, Dunstan DW, Dempsey PC, et al. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care (2016) 39(11):2065–79. doi: 10.2337/dc16-1728
9. Sigal RJ, Armstrong MJ, Bacon SL, Boulé NG, Dasgupta K, Kenny GP, et al. Physical activity and diabetes. Can J Diabetes (2018) 42:S54–63. doi: 10.1016/j.jcjd.2017.10.008
10. Silva Júnior WS, Fioretti A, Vancea D, Macedo C, Zagury R, Bertoluci M, et al. Atividade física e exercício no pré-diabetes e DM2. Diretriz Oficial da Sociedade Brasileira de Diabetes (2022). doi: 10.29327/557753.2022-8
11. Doupis J, Karras K, Avramidis K. The role of individualized exercise prescription in type 2 diabetes mellitus management. touchREV Endocrinol (2021) 17(1):2–4. doi: 10.17925/EE.2021.17.1.2
12. Nicolucci A, Balducci S, Cardelli P, Cavallo S, Fallucca S, Bazuro A, et al. Relationship of exercise volume to improvements of quality of life with supervised exercise training in patients with type 2 diabetes in a randomised controlled trial: The Italian Diabetes and Exercise Study (IDES). Diabetologia (2012) 55(3):579–88. doi: 10.1007/s00125-011-2425-9
13. Kanaley JA, Colberg SR, Corcoran MH, Malin SK, Rodriguez NR, Crespo CJ, et al. Exercise/physical activity in individuals with type 2 diabetes: A consensus statement from the American college of sports medicine. Med Sci Sports Exerc. (2022) 54(2):353–68. doi: 10.1249/MSS.0000000000002800
14. U.S. Department of Health and Human Services. Physical activity guidelines for Americans. 2nd ed. Washington, DC: U.S (2018). p. 118. Available at: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf.
15. World Health Organization. Diagnosis and management of type 2 diabetes (HEARTS-D). Geneva: World Health Organization (2020). Available at: http://apps.who.int/iris.
16. Pereira WVC, Vancea DMM, De Andrade Oliveira R, De Freitas YGPC, Lamounier RN, Silva Júnior WS, et al. 2022: Position of Brazilian Diabetes Society on exercise recommendations for people with type 1 and type 2 diabetes. Diabetol Metab Syndr (2023) 15(1):2. doi: 10.1186/s13098-022-00945-3
17. MacDonald CS, Johansen MY, Nielsen SM, Christensen R, Hansen KB, Langberg H, et al. Dose-response effects of exercise on glucose-lowering medications for type 2 diabetes: A secondary analysis of a randomized clinical trial. Mayo Clin Proc (2020) 95(3):488–503. doi: 10.1016/j.mayocp.2019.09.005
18. Rhea MR, Alvar BA, Burkett LN, Ball SD. A meta-analysis to determine the dose response for strength development. Med Sci Sports Exerc (2003) 35(3):456–64. doi: 10.1249/01.MSS.0000053727.63505.D4
19. Peterson MD, Rhea MR, Alvar BA. Applications of the dose-response for muscular strength development: a review of meta-analytic efficacy and reliability for designing training prescription. J Strength Cond Res (2005) 19(4):950–8. doi: 10.1519/R-16874.1
20. Jayedi A, Emadi A, Shab-Bidar S. Dose-dependent effect of supervised aerobic exercise on hbA1c in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. Sports Med (2022) 52(8):1919–38. doi: 10.1007/s40279-022-01673-4
21. Zahalka SJ, Abushamat LA, Scalzo RL, Reusch JEB. The role of exercise in diabetes. Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, et al, editors. South Dartmouth (MA: MDText.com, Inc (2000). Available at: http://www.ncbi.nlm.nih.gov/books/NBK549946/. Endotext.
22. Hecksteden A, Faude O, Meyer T, Donath L. How to construct, conduct and analyze an exercise training study? Front Physiol (2018) 9:1007. doi: 10.3389/fphys.2018.01007
23. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 29:n71. doi: 10.1136/bmj.n71
24. Cassidy S, Vaidya V, Houghton D, Zalewski P, Seferovic JP, Hallsworth K, et al. Unsupervised high-intensity interval training improves glycaemic control but not cardiovascular autonomic function in type 2 diabetes patients: A randomised controlled trial. Diabetes Vasc Dis Res (2019) 16(1):69–76. doi: 10.1177/1479164118816223
25. Banitalebi E, Mardaniyan Ghahfarrokhi M, Faramarzi M, Earnest CP. Sprint interval training vs. combined aerobic + resistance training in overweight women with type 2 diabetes. J Sports Med Phys Fitness (2021) 61(5):1–13. doi: 10.23736/S0022-4707.20.11105-8
26. Shiwa SR, Costa LOP, Moser AD de L, Aguiar I de C, de Oliveira LVF. PEDro: a base de dados de evidências em fisioterapia. Fisioterapia em Movimento (2011) 24(3):523–33. doi: 10.1590/S0103-51502011000300017
27. Alvarez C, Ramirez-Campillo R, Martinez-Salazar C, Mancilla R, Flores-Opazo M, Cano-Montoya J, et al. Low-volume high-intensity interval training as a therapy for type 2 diabetes. Int J Sports Med (2016) 37(9):723–9. doi: 10.1055/s-0042-104935
28. Bacchi E, Negri C, Zanolin ME, Milanese C, Faccioli N, Trombetta M, et al. Metabolic effects of aerobic training and resistance training in type 2 diabetic subjects: A randomized controlled trial (the RAED2 study). Diabetes Care (2012) 35(4):676–82. doi: 10.2337/dc11-1655
29. Banitalebi E, Faramarzi M, Nasiri S, Mardaniyan M, Rabiee V. Effects of different exercise modalities on novel hepatic steatosis indices in overweight women with type 2 diabetes. Clin Mol Hepatol (2019) 25(3):294–304. doi: 10.3350/cmh.2018.0086
30. Gholami F, Nazari H, Alimi M. Cycle Training improves vascular function and neuropathic symptoms in patients with type 2 diabetes and peripheral neuropathy: A randomized controlled trial. Exp Gerontol (2020) 131:1–6. doi: 10.1016/j.exger.2019.110799
31. Magalhães JP, Júdice PB, Ribeiro R, Andrade R, Raposo J, Dores H, et al. Effectiveness of high-intensity interval training combined with resistance training versus continuous moderate-intensity training combined with resistance training in patients with type 2 diabetes: A one-year randomized controlled trial. Diabetes Obes Metab (2019) 21(3):550–9. doi: 10.1111/dom.13551
32. Mitranun W, Deerochanawong C, Tanaka H, Suksom D. Continuous vs interval training on glycemic control and macro- and microvascular reactivity in type 2 diabetic patients. Scandinavian J Med Sci Sports (2014) 24(2):1– 8. doi: 10.1111/sms.12112
33. Pandey A, Suskin N, Poirier P. The impact of burst exercise on cardiometabolic status of patients newly diagnosed with type 2 diabetes. Can J Cardiol (2017) 33(12):1645–51. doi: 10.1016/j.cjca.2017.09.019
34. Sabag A, Way KL, Sultana RN, Keating SE, Gerofi JA, Chuter VH, et al. The effect of a novel low-volume aerobic exercise intervention on liver fat in type 2 diabetes: A randomized controlled trial. Diabetes Care (2020) 43(10):2371–8. doi: 10.2337/dc19-2523
35. Yang P, Swardfager W, Fernandes D, Laredo S, Tomlinson G, Oh PI, et al. F inding the O ptimal volume and intensity of R esistance T raining E xercise for Type 2 Diabetes: The FORTE Study, a Randomized Trial. Diabetes Res Clin Practice (2017) 130:98–107. doi: 10.1016/j.diabres.2017.05.019
36. Chien YH, Tsai CJ, Wang DC, Chuang PH, Lin HT. Effects of 12-week progressive sandbag exercise training on glycemic control and muscle strength in patients with type 2 diabetes mellitus combined with possible sarcopenia. IJERPH (2022) 19(22):15009. doi: 10.3390/ijerph192215009
37. Andrade EA, Fett CA, Vieira Junior RC, Voltarelli FA. Exercício físico de moderada intensidade contribui para o controle de parâmetros glicêmicos e clearance de creatina em pessoas com Diabetes Mellitus tipo 2. R. bras. Ci. e Mov (2016) 24(1):118–26.
38. Kong N, Yang G, Wang L, Li Y. CALISTHENICS EXERCISES TO INTERVENE IN OBESITY AND DIABETES IN MIDDLE-AGED PEOPLE. Rev Bras Med Esporte. (2022) 28(2):85–8. doi: 10.1590/1517-8692202228022021_0457
39. Li J, Zhang W, Guo Q, Liu X, Zhang Q, Dong R, et al. Duration of exercise as a key determinant of improvement in insulin sensitivity in type 2 diabetes patients. Tohoku J Exp Med (2012) 227(4):289–96. doi: 10.1620/tjem.227.289
40. Støa EM, Meling S, Nyhus LK, Strømstad G, Mangerud KM, Helgerud J, et al. High-intensity aerobic interval training improves aerobic fitness and HbA1c among persons diagnosed with type 2 diabetes. Eur J Appl Physiol (2017) 117(3):455–67. doi: 10.1007/s00421-017-3540-1
41. Winding KM, Munch GW, Iepsen UW, Van Hall G, Pedersen BK, Mortensen SP. The effect on glycaemic control of low-volume high-intensity interval training versus endurance training in individuals with type 2 diabetes. Diabetes Obes Metab (2018) 20(5):1131–9. doi: 10.1111/dom.13198
42. Pfeifer LO, De Nardi AT, Da Silva LXN, Botton CE, Do Nascimento DM, Teodoro JL, et al. Association between physical exercise interventions participation and functional capacity in individuals with type 2 diabetes: A systematic review and meta-analysis of controlled trials. Sports Med - Open (2022) 8(1):34. doi: 10.1186/s40798-022-00422-1
43. Bullard T, Ji M, An R, Trinh L, Mackenzie M, Mullen SP. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: cancer, cardiovascular disease, and diabetes. BMC Public Health (2019) 19(1):636. doi: 10.1186/s12889-019-6877-z
44. Da Rocha RB, Silva CS, Cardoso VS. Self-care in adults with type 2 diabetes mellitus: A systematic review. CDR (2020) 16(6):598–607. doi: 10.2174/1573399815666190702161849
45. Newsom SA, Everett AC, Hinko A, Horowitz JF. A single session of low-intensity exercise is sufficient to enhance insulin sensitivity into the next day in obese adults. Diabetes Care (2013) 36(9):2516–22. doi: 10.2337/dc12-2606
46. da Cruz LC, Teixeira-Araujo AA, Passos Andrade KT, Rocha TCOG, Puga GM, Moreira SR. Low-intensity resistance exercise reduces hyperglycemia and enhances glucose control over 24 hours in women with type 2 diabetes. J Strength Cond Res (2019) 33(10):2826–35. doi: 10.1519/JSC.0000000000002410
47. Lora-Pozo I, Lucena-Anton D, Salazar A, Galán-Mercant A, Moral-Munoz JA. Anthropometric, cardiopulmonary and metabolic benefits of the high-intensity interval training versus moderate, low-intensity or control for type 2 diabetes: systematic review and meta-analysis. IJERPH (2019) 16(22):4524. doi: 10.3390/ijerph16224524
48. Church TS, Blair SN, Cocreham S, Johannsen N, Johnson W, Kramer K, et al. Effects of aerobic and resistance training on hemoglobin A1c levels in patients with type 2 diabetes: a randomized controlled trial. JAMA (2010) 304(20):2253–62. doi: 10.1001/jama.2010.1710
49. Pan B, Ge L, Xun Yq, Chen Yj, Gao Cy, Han X, et al. Exercise training modalities in patients with type 2 diabetes mellitus: a systematic review and network meta-analysis. Int J Behav Nutr Phys Act (2018) 15(1):72. doi: 10.1186/s12966-018-0703-3
50. Ishiguro H, Kodama S, Horikawa C, Fujihara K, Hirose AS, Hirasawa R, et al. In search of the ideal resistance training program to improve glycemic control and its indication for patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Sports Med (2016) 46(1):67–77. doi: 10.1007/s40279-015-0379-7
51. Sigal RJ, Kenny GP, Boulé NG, Wells GA, Prud’homme D, Fortier M, et al. Effects of aerobic training, resistance training, or both on glycemic control in type 2 diabetes. Ann Intern Med (2007) 147(6):357–69. doi: 10.7326/0003-4819-147-6-200709180-00005
52. Villafaina S, Collado-Mateo D, Fuentes JP, Merellano-Navarro E, Gusi N. Physical exercise improves heart rate variability in patients with type 2 diabetes: A systematic review. Curr Diabetes Rep (2017) 17(11):110. doi: 10.1007/s11892-017-0941-9
53. Grace A, Chan E, Giallauria F, Graham PL, Smart NA. Clinical outcomes and glycaemic responses to different aerobic exercise training intensities in type II diabetes: a systematic review and meta-analysis. Cardiovasc Diabetol (2017) 16(1):37. doi: 10.1186/s12933-017-0518-6
54. Wrench E, Rattley K, Lambert JE, Killick R, Hayes LD, Lauder RM, et al. There is no dose-response relationship between the amount of exercise and improvement in HbA1c in interventions over 12 weeks in patients with type 2 diabetes: a meta-analysis and meta-regression. Acta Diabetol (2022) 59(11):1399–415. doi: 10.1007/s00592-022-01918-8
55. do Nascimento Cândido G, Batalha APDB, da Silva Chaves GS, Pereira DS, Britto RR. Effects of exercise training parameters on cardiorespiratory fitness of individuals with type 2 diabetes mellitus: a systematic review and meta-analysis. J Diabetes Metab Disord (2023) 22(1):97–118. doi: 10.1007/s40200-023-01205-5
56. Nesti L, Pugliese NR, Sciuto P, Natali A. Type 2 diabetes and reduced exercise tolerance: a review of the literature through an integrated physiology approach. Cardiovasc Diabetol (2020) 19(1):134. s12933-020-01109–1. doi: 10.1186/s12933-020-01109-1
57. Boulé NG, Kenny GP, Haddad E, Wells GA, Sigal RJ. Meta-analysis of the effect of structured exercise training on cardiorespiratory fitness in Type 2 diabetes mellitus. Diabetologia (2003) 46(8):1071–81. doi: 10.1007/s00125-003-1160-2
58. Harman NL, Wilding JPH, Curry D, Harris J, Logue J, Pemberton RJ, et al. Selecting Core Outcomes for Randomised Effectiveness trials In Type 2 diabetes (SCORE-IT): a patient and healthcare professional consensus on a core outcome set for type 2 diabetes. BMJ Open Diabetes Res Care (2019) 7(1):e000700. doi: 10.1136/bmjdrc-2019-000700
59. World Health Organization. Classification of diabetes mellitus 2019. Geneva: World Health Organization (2019). Available at: http://apps.who.int/iris/.
60. Picard M, Tauveron I, Magdasy S, Benichou T, Bagheri R, Ugbolue UC, et al. Effect of exercise training on heart rate variability in type 2 diabetes mellitus patients: A systematic review and meta-analysis. Abdelbasset WK editor. PloS One (2021) 16(5):e0251863. doi: 10.1371/journal.pone.0251863
61. Akobeng AK. Principles of evidence based medicine. Arch Dis Childhood. (2005) 90(8):837–40. doi: 10.1136/adc.2005.071761
Keywords: diabetes mellitus, physical exercise, rehabilitation, glycemic control, primary health care, quality of life, physical fitness, Noncommunicable diseases
Citation: Ribeiro AKPdL, Carvalho JPR and Bento-Torres NVO (2023) Physical exercise as treatment for adults with type 2 diabetes: a rapid review. Front. Endocrinol. 14:1233906. doi: 10.3389/fendo.2023.1233906
Received: 02 June 2023; Accepted: 01 September 2023;
Published: 28 September 2023.
Edited by:
Åke Sjöholm, Gävle Hospital, SwedenReviewed by:
Alba Camacho-Cardenosa, University of Granada, SpainSudhanshu Kumar Bharti, Patna University, India
Copyright © 2023 Ribeiro, Carvalho and Bento-Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natáli Valim Oliver Bento-Torres, bmF0YWxpdmFsaW1AdWZwYS5icg==