 Cem Demirel1†
Cem Demirel1† Pınar Özcan
Pınar Özcan Fırat Tülek
Fırat Tülek Hikmet Tunç Timur
Hikmet Tunç Timur Özge Pasin
Özge Pasin- 1Department of Obstetrics and Gynaecology, Acibadem University School of Medicine, Istanbul, Türkiye
- 2Department of Obstetrics and Gynaecology, Bezmialem University School of Medicine, Istanbul, Türkiye
- 3Department of Obstetrics and Gynecology, Dokuz Eylul University School of Medicine, Izmir, Türkiye
- 4Department of Biostatistics and Medical Informatics, Bezmialem University School of Medicine, Istanbul, Türkiye
Introduction: Concerning contemporary in-vitro fertilisation (IVF) practice, the use of frozen embryo transfer (FET) cycles has become more common than fresh transfers. Natural cycle (NC), programmed artificial cycle and mild stimulation cycle are primary endometrium preparation cycles. Monitoring serum progesterone levels in FET cycles are in the scope of current research focus. Low progesterone levels on the day of embryo transfer is presumed to negatively affect pregnancy outcomes, while progesterone supplementation may improve pregnancy rates. The purpose of our trial is to evaluate whether initiating subcutaneous (SC) progesterone supplementation on the day of embryo transfer when serum progesterone levels are below 10 ng/mL in tNC-FET will result in pregnancy rates comparable to those of patients with sufficient serum progesterone.
Methods: Retrospective single centre study was conducted between August 2022 and April 2023 with 181 tNC-FETs. Patients were separated into groups according to serum progesterone concentrations (≥10 ng/mL and <10 ng/mL) on embryo transfer (ET) day. S.c progesterone (25 mg) was given on the day of ET when serum progesterone was <10 ng/mL, continuing until the 10th gestational week. Blood samples for pregnancy tests were collected 12 days after ET. Outcome parameters were pregnancy rate, clinical pregnancy rate (CPR), miscarriage rate, multiple pregnancy rate, biochemical pregnancy, and ongoing pregnancy rate (OPR).
Results: About half (49.7%) had adequate progesterone concentrations (≥10ng/mL) on ET day. There was no significant difference between the groups regarding positive pregnancy test, OPR, multiple pregnancies, and miscarriage rates (57.8% versus 52.7%; 34.4% versus 29.7%, 1.1% versus 2.2%; 7.8% versus 5.5%; respectively, for progesterone concentrations on ET day ≥10 ng/mL and <10 ng/mL). With 55.2% of transfers leading to clinical pregnancy, significant differences emerged in biochemical pregnancy and CPR (3.3% vs 12.1%, P=0.02; 54.4% vs 40.7%, P=0.03, for ≥10 ng/mL and <10 ng/mL progesterone concentrations on ET day).
Discussion: This study indicates that nearly half of the tNC-FETs may need luteal phase support due to low progesterone. However, 25 mc sc progesterone rescued the luteal support and yielded similar OPR as compared to normal progesterone group. Further studies are needed for understanding optimal progesterone levels, supplementation effectiveness, and potential benefits of earlier supplementation in FETs.
Introduction
In today’s IVF practice, frozen embryo transfer (FET) cycles have started to override fresh transfers, owing to the improvements in vitrification techniques along with the added benefits of elimination of ovarian hyperstimulation syndrome (OHSS) and improved success rates in hyper-responders when freeze-all strategy is used. Increased utilisation of preimplantation genetic screening of embryos further augments the switch to frozen transfer cycles (1, 2). According to a United States nationwide database, FET cycles have recently become approximately 77.0% of all ETs (3). There are mainly three strategies utilised, each having further modifications within, for endometrium preparation during FET, namely natural cycle, programmed artificial cycle, and mild stimulation cycle FETs. Until very recently, there had been no clear-cut consensus yet for the optimal FET strategy, but the recent trend is more towards the use of a natural cycle (4–7). The reasons are primarily two folds, one being a higher ongoing pregnancy rate compared to artificial cycles due to a lower incidence of early pregnancy loss and the other one being the pregnancy complications like pregnancy induced hypertension and significant for gestational age fetuses that are unique to artificial cycles, most probably due to the absence of corpus luteum (8). Nowadays, the main research topic is focused on monitoring FET cycles best and finding out the confounding factors that may affect success rates. Monitorisation of serum progesterone levels is a central topic of interest in FET cycles, and it has been documented in various reports that serum progesterone levels below a certain threshold around the time of ET result in decreased odds for live birth rates. This has been verified in artificial FET cycles where serum progesterone levels lower than 8-10 ng/mL on the day or preceding day of ET are shown to adversely affect the live birth rates (9, 10). Rescue strategies in the form of adding 25 mg of supplemental subcutaneous (SC) progesterone are shown to restore live birth rates to those of patients with adequate serum progesterone levels in artificial FET cycles, to overcome the deleterious effect of the insufficient progesterone support of the endometrium (11, 12).
The corpus luteum (CL) is involved in a natural cycle FET. Nevertheless, progesterone production by CL in some cycles may be insufficient to provide adequate support for implantation and continuation of pregnancy. A very recent meta-analysis of randomised controlled trials for luteal phase support (LPS) in natural cycle FET (NC-FET) has shown that progesterone supplementation for LPS was associated with increased LBR and CPR in NC-FET cycles, giving additional evidence for the insufficiency of corpus luteum in some of the natural cycles (13). In the same meta-analysis, LPS improves LBR only in true NC-FET but not in modified NC-FET, where hCG used to trigger dominant follicles must act as LPS per se. A recent retrospective study has shown that patients with low serum progesterone (< 10 ng/mL) on the day before NC-FET have reduced live birth rates compared to those who have > 10 ng/mL progesterone (14). Of note, these NC-FET cases were not using any LPS, solely depending on progesterone production by CL. Since lower progesterone concentrations on ET day during natural cycles FET may negatively influence pregnancy outcomes, progesterone supplementation for the restoration of serum progesterone to adequate concentrations may be an opportunity to improve PRs (9, 14–16).
The purpose of our trial is to evaluate whether initiating SC progesterone supplementation on the day of embryo transfer when serum progesterone levels are below 10 ng/mL in tNC-FET will result in pregnancy rates comparable to those of patients with sufficient serum progesterone. In brief, to our knowledge, this is the first study to evaluate the feasibility of a rescue progesterone supplementation strategy in tNC-FET cases.
Materials and methods
This retrospective cohort study in a single centre was carried out at the IVF centre of Acibadem Ataşehir Hospital between August 2022 and April 2023. A total of 181 true natural cycles vitrified–warmed FETs (tNC-FET) were evaluated. The Ethical Committee of Bezmialem University approved the protocol of our study (Approval no. 2023/165). Exclusion criteria were patients with cycle cancellation due to lack of a viable embryo or who had Mullerian anomalies not corrected by surgery, such as bicornuate, unicornuate, or didelphic uterus, those with a history of recurrent miscarriage, and those with a presence of hydrosalpinx. Those who had corrected uterine anomalies such as uterine septum, submucosal fibroids, or endometrial polyps were not excluded.
The collected data consisted of demographic characteristics of the patients, including age at oocyte pick up (year), IVF indications (tubal, male, unexplained, diminishing ovarian reserve, ovulatory, mixed), serum LH concentration (IU/L) on the day of LH surge, serum progesterone concentration (ng/mL) on the day of LH surge and the day of embryo transfer, endometrial thickness (mm) on the day of embryo transfer, stage of transferred embryo (Day 3/blastocyst) and number of embryos transferred. Outcome parameters analysed are pregnancy rate, clinical pregnancy rate (CPR) (fetal heartbeat by transvaginal ultrasound), miscarriage rate (any clinical pregnancy lost before the 12th gestational week), multiple pregnancy rate, biochemical pregnancy, and ongoing pregnancy rate (OPR) (pregnancies beyond 12 weeks of pregnancy).
All women underwent a transvaginal ultrasound scan on the second or third day of menstruation to confirm the absence of any ovarian cyst or CL. The second control was scheduled on the eighth day of the cycle to evaluate the emergence of the dominant follicle by transvaginal ultrasonography. Endocrine monitoring with serum LH and progesterone measurements was initiated everyday at 9 am once the leading follicle attained a mean diameter of approximately 15 mm. An increase of at least 180% compared to the previous serum LH level was taken as consistent with LH surge. FETs were performed four days after the LH rise for day three embryos and six days after the blastocyst stage. Blood samples for serum progesterone concentrations were collected on ET day at 9 am for all patients. 25 mg of SC progesterone (Prolutex; IBSA, Switzerland) per day was initiated at 11 am in patients with serum progesterone concentrations <10 ng/mL on ET day. The blood samples for pregnancy tests were collected 12 days after ET. Progesterone supplementation was discontinued if there was no pregnancy. We hypothesized that patients with serum progesterone concentrations <10 ng/mL in tNC-FET on the day of embryo transfer may have insufficiency of corpus luteum. We would like to continue SC progesterone until the luteo-placental shift (10th weeks of pregnancy). Therefore, progesterone supplementation at the same dose was continued until the 10th gestational week for viable pregnancies. Serum analysis and hormone measurement, vitrification and warming procedure, and ET were performed as described in our previous study (17).
The data were analysed using SPSS Statistics for Windows, Version 26 (IBM Corp, Armonk, NY, USA). Data were reported as mean ± SD or number and percentage. The Pearson chi-squared test, Fisher’s exact and Fisher Freeman Halton tests were used to compare categorical variables. The Kolmogorov–Smirnov test was used to test the normal distribution of continuous variables. The homogeneity of variance was evaluated with Levene’s test. Student’s t-test was used to compare two independent groups regarding the means of normally distributed variables. The Mann–Whitney U-test was used to compare two independent groupsregardingf the means of non-normally distributed variables. P<0.05 was considered significant. As this is a retrospective study, no power analysis was performed prior to the study, and we included all women who underwent natural cycles FET during the period.
Results
A total of 181 tNC- FET were analysed. The mean age was 35.37 ± 4.72 in patients with serum progesterone concentrations ≥10 ng/mL on the day of ET and 35.35 ± 5.3 years in patients with serum progesterone concentrations <10 ng/ml on ET day. Overall, 49.7% (90/181) of patients had adequate serum progesterone concentrations on ET day (≥10 ng/mL). Patients with serum progesterone concentrations <10 ng/mL and ≥10 ng/mL were similar in terms of age at oocyte pick up, IVF indications, serum LH concentration on the day of LH surge, serum progesterone concentration on the day of LH surge, endometrial thickness on the day of embryo transfer and number of embryos transferred. (Table 1). There was a significant difference between groups regarding serum progesterone concentrations on ET day (14.63 ± 5.57 vs 7.29 ± 1.93 ng/mL; P < 0.001, respectively, for ≥10 ng/mL and <10 ng/mL serum progesterone concentration). There was a statistically significant difference in terms of the distribution of day three embryos and blastocysts in patients with serum progesterone concentrations ≥10 ng/mL and patients with <10 ng/mL on the day of ET. The number of day three embryo transfers was significantly higher in patients with serum progesterone concentrations <10 ng/mL on the day of ET (5.6% versus 18.7%; P =0.01). There was a statistically significant difference in serum progesterone concentrations between those undergoing day 3 and day 5 frozen thawed embryo transfers (7.99 ± 6.86 vs 11.34 ± 5.23 ng/mL; P<0.001, respectively, for day three and blastocyst stages). However, there was no significant difference between the patients in terms of clinical pregnancy rates according to the day of embryo transfer (2% versus 8.1%; P=0.31).
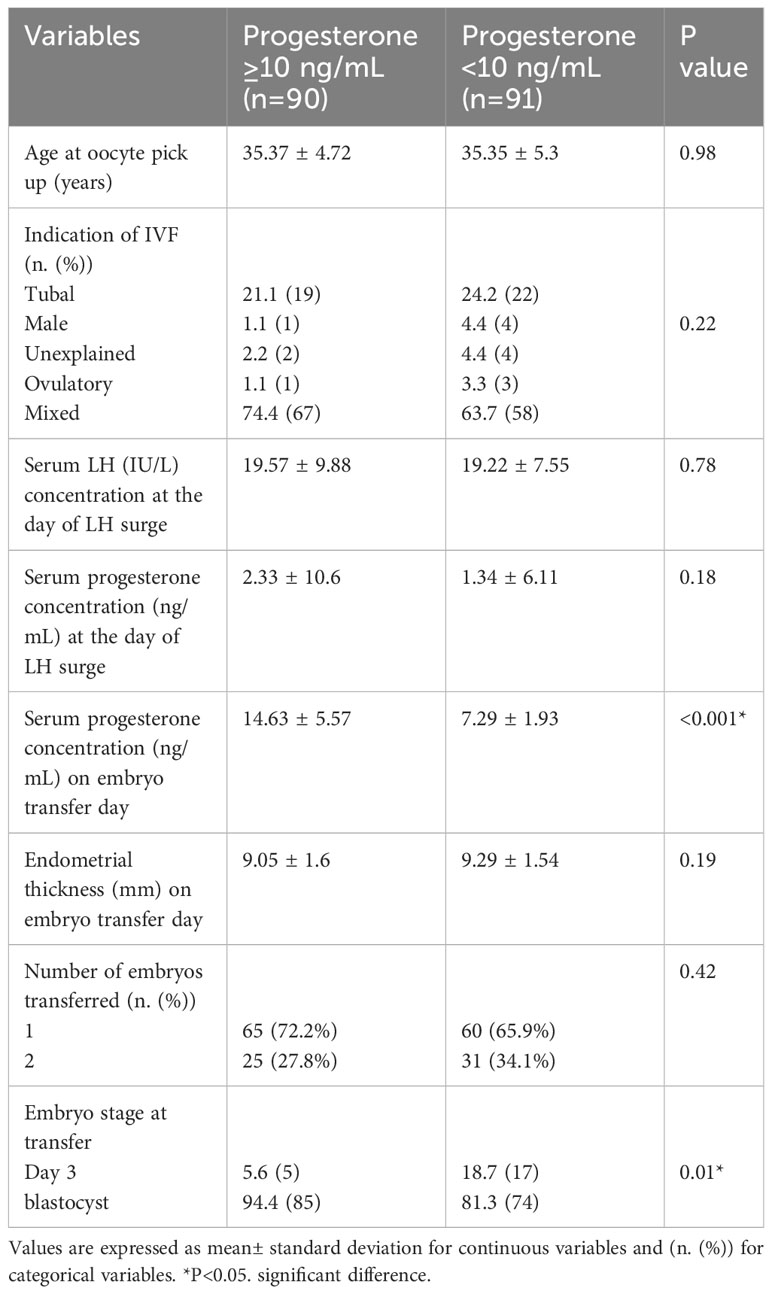
Table 1 The characteristics of patients.
Of all transfers, 55.2% (100/181) of all transfers resulted in a clinical pregnancy. There was no significant difference between the groups regarding positive pregnancy test, OPR, multiple pregnancies, and miscarriage rates (57.8% versus 52.7%; 34.4% versus 29.7%, 1.1% versus 2.2%; 7.8% versus 5.5%; respectively, for progesterone concentrations on ET day ≥10 ng/mL and <10 ng/mL). Biochemical pregnancy rates (3.3% versus 12.1%, P = 0.02) was lower and clinical pregnancy rates (54.4% versus 40.7%, P = 0.03) was higher in patients with ≥10 ng/mL P concentrations on the day of ET. Serum progesterone concentrations on ET day were evaluated by percentiles (<10%, 10–49%, 50–90%, and >90%). The threshold for <10%, 10– 49%, 50–90%, and >90% were 0–5.9 (11%), 5,9–9,96 (39.2%), 9.96–16.54 (39.8%) and >16.64 ng/mL (9.9%), respectively. However, the positive pregnancy test of serum progesterone percentiles on ET day was 8% in the <10% percentile, 40% in the 10–49% percentile, 39% in the 50–90% percentile, and 13% in the >90% percentile. The CPR of serum progesterone percentiles on ET day was 5.8% in the <10% percentile, 37.2% in the 10–49% percentile, 43% in the 50–90% percentile, and 14% in the >90% percentile. There was no significant difference between the patients in terms of CPR in all percentiles when evaluating separately according to the day of embryo transfer. The CPR of serum progesterone percentiles for day three embrio on ET day was 35.3% in the <10% percentile, 41.2% in the 10–49% percentile, 17.6% in the 50–90% percentile, and 5.9% in the >90% percentile (P=0.41). The CPR of serum progesterone percentiles for blastocyst stages on ET day was 9.4% in the <10% percentile, 37.5% in the 10–49% percentile, 46.9% in the 50–90% percentile, and 6.3% in the >90% percentile (P=0.14). 10 ng/mL was represented as the threshold of the 51st percentile in this study. A total of 78.5% of biochemical pregnancies were under the 50 percentile.
Discussion
The correlation between low serum progesterone levels around the timing of embryo transfer and decreased LBR has been demonstrated in artificial and natural frozen embryo transfer cycles (9, 10, 14). The necessity of exogenous luteal phase support has been debated in NC-FET cycles since there is a corpus luteum to produce endogenous progesterone. However, the adequacy of CL function is not absolute, and it has been shown in a recent study that low serum progesterone (<10 ng/mL) on the day before NC-FET has been associated with reduced live birth rates compared to cycles with ≥ 10 ng/mL progesterone (14). A recent meta-analysis to evaluate whether LPS is beneficial in NC-FET also supports the findings of this study, giving additional evidence for the insufficiency of the corpus luteum in some of the natural cycles. This meta-analysis showed that progesterone supplementation for LPS was associated with increased LBR and CPR in NC-FET cycles (13). Stavridis et al., have recently presented another meta-analysis. The results of this meta-analysis suggested that rescue progesterone in patients with lower serum progesterone levels results in similar CPR, OPR and LBRs to patients with sufficient progesterone levels in artificial FET (18).
The lower limit of serum progesterone concentration indicative of an adequate luteal phase in natural cycles is not yet clear. However, mid-luteal serum concentrations of about 10 ng/mL are mostly accepted as adequate progesterone production by the corpus luteum during a natural cycle (14, 19, 20). Therefore, we took 10 ng/mL as the threshold serum progesterone concentration on the ET day in our study. In our study, only 49.7% of patients who are undergoing an NC-FET reached the cutoff serum progesterone concentration (≥10 ng/mL) on ET day, but 50.3% of patients fell short of this range (<10 ng/mL). Therefore, nearly half the NC-FET cycles might have benefitted from some LPS. LPS might be routinely implemented one day after LH surge in a standard fashion or reserved for cases with low levels of serum progesterone around the time of embryo transfer/implantation. Meanwhile, the number of day three embryo transfers was significantly higher in patients with serum progesterone concentrations <10 ng/mL on the day of ET and serum progesterone concentrations on ET day were significantly lower in day three embryo transfers. Therefore, 10 ng/mL as the threshold concentration of serum progesterone on the day of ET may not be suitable for day three embryo transfers. The importance of endocrine monitoring in t-NC is still a matter of debate. A retrospective study including 610 patients underwent t-NC FET found a 28.4% incidence of serum P4 elevation before the LH surge but there was no significant difference in terms of OPR between patients with or without P4 elevation on the day of LH surge (32.5% vs 31.7%) (21). The results of subgroup analysis demonstrated that, not the level, but the duration of P4 exposure before the LH surge was associated with the lower pregnancy rates.
Our study is the first study in patients undergoing t-NC FET to evaluate the feasibility of the alternative approach, reserving the initiation of progesterone support when the serum levels of progesterone are below 10 ng/mL on the day of ET. If this approach had been practical, it might have rescued nearly half of the tNC-FET cycles with adequate serum progesterone concentrations from unnecessary progesterone supplementation.
The major finding of our study is that rescue protocol by adding SC progesterone is effective and as a result no significant difference could be shown in terms of OPR. At the same time, CPR in patients with low serum progesterone concentrations on ET day was lower despite LPS with sc progesterone supplementation. Our study has found that although pregnancy rates are similar, CPR is inferior in cycles with low serum progesterone despite the initiation of SC progesterone on ET day because of a higher incidence of biochemical pregnancies in this group. Therefore, SC progesterone supplementation can not sustain the essential luteal phase support when initiated on the day of ET if the endogenous CL function is inadequate. There are two possible explanations for this finding: Either we are too late to initiate luteal phase rescue, or the support dose/mode (sc) is inadequate. According to our best knowledge, our study is the first study to evaluate the effect of sc progesterone supplementation on PRs in tNC-FET based on serum progesterone level on ET day. Our previous study in programmed artificial FET cycles evaluated the effect of additional rescue. SC progesterone supplementation for restoring serum progesterone level in patients with low serum progesterone concentration on ET day, two days after the rescue treatment (17). However, in current study, we did not evaluate whether adequate serum progesterone level was reached with SC progesterone supplementation or not, due to its retrospective nature.
Bjuresten et al. reported an improvement in LBRs with 400 mg twice daily of vaginal progesterone in NC-FETs in their RCT, including 435 women (30% vs. 20%, P = 0.02), compared to those without supplementation (16). Likewise, in a prospective randomised controlled trial, Wanggren et al. evaluated the effect of LPS with 100 mg twice daily vaginal progesterone tablet in NC-FET cycles. They demonstrated the beneficial effect of vaginal progesterone supplementation on PRs (OR: 1.465, 95% CI 1.012–2.108, P=0.049), CPRs (OR: 1.497, 95% CI 1.024–2.188, P=0.043) and LBRs (OR:1.635, 95% CI 1.102–2.428, P=0.017) (22). In a retrospective cohort study including 228 consecutive patients who underwent NC-FET, Kim et al. reported improved LBR and reduced miscarriage rate with vaginal progesterone gel supplementation (23). Moreover, two recent meta-analyses strongly demonstrated the association between LPS with vaginal progesterone in NC-FET and higher LBRs (24, 25). In fact, according to our results, individualised rescue protocol using SC progesteron is effective since OPR is similar between groups. The primary difference was that we used an individualised LPS with SC progesterone by using serum progesterone levels on the day of ET. The optimal dosage of sc progesterone supplementation as LPS in tNC-FET has not been thoroughly studied, and further studies are needed on this aspect. Furthermore, in all those studies mentioned, vaginal progesterone as LPS was initiated before the transfer day, a RCT comparing rescue LPS with SC progesterone with no support is necessary to find out the exact role of this protocol.
We have previously mentioned a debate in the literature related to the beneficial effect of progesterone supplementation as LPS in tNC-FET. For tNC-FETs, it remains an open question about how to support the luteal phase, which dosages and agents to use, and the LPS’s efficacy for these selected agents in clinical practice. In this regard, our study may shed more light on our knowledge to affect the current practice for NC-FET.
There are few points related to the current study as limitations. The first limitation is that it is a retrospective study with a relatively small sample size and that we did not report LBRs. We do not think patients with low serum progesterone concentrations on ET day can be refrained from progesterone supplementation because of the well-documented strong relationship between adequate serum progesterone concentrations and successful implantation and pregnancy outcome. Furthermore, the design of our practice to add LPS rescue with SC 25 mg progesterone is a clinically proven mode of action in artificial FET cycles when serum progesterone levels are found in a suboptimal range for a successful outcome on the day of ET. The only difference was that this strategy was never validated in tNC-FET cases. We were expecting the same beneficial effect of this strategy in tNC-FET cases since we have an additional functioning CL in a natural cycle. The second limitation is that serum progesterone concentrations were not measured after starting progesterone supplementation to confirm the attainment of adequate levels with sc progesterone. The design of our study, SC progesterone supplementation as LPS in natural cycles FET based on serum progesterone level on ET day, might be considered as the strength of our study.
In conclusion, according to our results, almost half of the patients who undergo tNC-FET might need LPS because of low serum progesterone concentrations on ET day. The measurement of serum progesterone level on ET day may create the opportunity for progesterone supplementation for patients with low serum progesterone concentrations. On the other hand, daily 25 mg sc progesterone supplementation may achieve similar OPR. Starting luteal phase support earlier than the day of embryo transfer in all NC-FET cases may be a better clinical decision in this setting until cut-off levels of P on the day of ET in tNC-FET is established and the benefit of rescue protocol is proven by RCTs. Further well-designed randomised controlled trials with large samples of patients are needed to evaluate the cutoff level of serum progesterone, which determine the necessity of LPS and the effect of sc progesterone supplementation as LPS on LBR during NC-FET.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by The Ethical Committee of Bezmialem University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CD: Conceptualization, Methodology, Writing – review & editing. PÖ: Conceptualization, Formal Analysis, Methodology, Supervision, Writing – original draft. FT: Data curation, Formal Analysis, Methodology, Writing – original draft. HT: Data curation, Formal Analysis, Writing – review & editing. ÖP: Data curation, Formal Analysis, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Roque M, Haahr T, Geber S, Esteves SC, Humaidan P. Fresh versus elective frozen embryo transfer in IVF/ICSI cycles: a systematic review and meta-analysis of reproductive outcomes. Hum Reprod Update (2019) 25(1):2–14. doi: 10.1093/humupd/dmy033
2. Saket Z, Källén K, Lundin K, Magnusson Å, Bergh C. Cumulative live birth rate after IVF: trend over time and the impact of blastocyst culture and vitrification. Hum Reprod Open (2021) 2021(3):1–9. doi: 10.1093/hropen/hoab021
3. Department of Health U, Services Centers for Disease Control H. Assisted Reproductive Technology Fertility Clinic Success Rates Report (2018). Available at: http://www.cdc.gov/art/reports.
4. Ghobara T, Vandekerckhove P. Cycle regimens for frozen-thawed embryo transfer. Cochrane Database Syst Rev (2008) 1). doi: 10.1002/14651858.CD003414.pub2
5. Glujovsky D, Pesce R, Sueldo C, Quinteiro Retamar AM, Hart RJ, Ciapponi A. Endometrial preparation for women undergoing embryo transfer with frozen embryos or embryos derived from donor oocytes. Cochrane Database Syst Rev (2020) 10(10). doi: 10.1002/14651858.CD006359.pub3
6. Groenewoud ER, Cantineau AEP, Kollen BJ, Macklon NS, Cohlen BJ. What is the optimal means of preparing the endometrium in frozen-thawed embryo transfer cycles? A systematic review and meta-analysis. Hum Reprod Update (2013) 19(5):458–70. doi: 10.1093/humupd/dmt030
7. Groenewoud ER, Cohlen BJ, Al-Oraiby A, Brinkhuis EA, Broekmans FJM, De Bruin JP, et al. A randomized controlled, non-inferiority trial of modified natural versus artificial cycle for cryo-thawed embryo transfer. Hum Reprod (2016) 31(7):1483–92. doi: 10.1093/humrep/dew120
8. Wu H, Zhou P, Lin X, Wang S, Zhang S. Endometrial preparation for frozen-thawed embryo transfer cycles: a systematic review and network meta-analysis. J Assist Reprod Genet (2021) 38(8):1913–26. doi: 10.1007/s10815-021-02125-0
9. Gaggiotti-Marre S, Martinez F, Coll L, Garcia S, Álvarez M, Parriego M, et al. Low serum progesterone the day prior to frozen embryo transfer of euploid embryos is associated with significant reduction in live birth rates. Gynecol Endocrinol (2019) 35(5):439–42. doi: 10.1080/09513590.2018.1534952
10. Labarta E, Mariani G, Holtmann N, Celada P, Remohí J, Bosch E. Low serum progesterone on the day of embryo transfer is associated with a diminished ongoing pregnancy rate in oocyte donation cycles after artificial endometrial preparation: a prospective study. Hum Reprod (2017) 32(12):2437–42. doi: 10.1093/humrep/dex316
11. Álvarez M, Gaggiotti-Marre S, Martínez F, Coll L, García S, González-Foruria I, et al. Individualised luteal phase support in artificially prepared frozen embryo transfer cycles based on serum progesterone levels: a prospective cohort study. Hum Reprod (2021) 36(6):1552–60. doi: 10.1093/humrep/deab031
12. Labarta E, Mariani G, Rodríguez-Varela C, Bosch E. Individualized luteal phase support normalizes live birth rate in women with low progesterone levels on the day of embryo transfer in artificial endometrial preparation cycles. Fertil Steril (2022) 117(1):96–103. doi: 10.1016/j.fertnstert.2021.08.040
13. Jiang Y, Wang L, Shen H, Wang B, Wu J, Hu K, et al. The effect of progesterone supplementation for luteal phase support in natural cycle frozen embryo transfer: a systematic review and meta-analysis based on randomized controlled trials. Fertil Steril (2023) 119(4):597–605. doi: 10.1016/j.fertnstert.2022.12.035
14. Gaggiotti-Marre S, Alvarez M, González-Foruria I, Parriego M, Garcia S, Martínez F, et al. Low progesterone levels on the day before natural cycle frozen embryo transfer are negatively associated with live birth rates. Hum Reprod (2020) 35(7):1623–9. doi: 10.1093/humrep/deaa092
15. Montagut M, Santos-Ribeiro S, De Vos M, Polyzos NP, Drakopoulos P, Mackens S, et al. Frozen-thawed embryo transfers in natural cycles with spontaneous or induced ovulation: the search for the best protocol continues. Hum Reprod (2016) 31(12):2803–10. doi: 10.1093/humrep/dew263
16. Bjuresten K, Landgren BM, Hovatta O, Stavreus-Evers A. Luteal phase progesterone increases live birth rate after frozen embryo transfer. Fertil Steril (2011) 95(2):534–7. doi: 10.1016/j.fertnstert.2010.05.019
17. Ozcan P, Cetin C, Okten B, Tanoglu FB, Taha HS, Pasin O, et al. The importance of serum progesterone concentration at embryo transfer day and effect of rescue additional progesterone during programmed artificial frozen embryo transfer cycles. Reprod BioMed Online (2022) 45(4):785–92. doi: 10.1016/j.rbmo.2022.05.023
18. Stavridis K, Kastora SL, Triantafyllidou O, Mavrelos D, Vlahos N. Effectiveness of progesterone rescue in women presenting low circulating progesterone levels around the day of embryo transfer: a systematic review and meta-analysis. Fertil Steril (2023) 119(6):954–63. doi: 10.1016/j.fertnstert.2023.02.007
19. Hull MGR, Savage PE, Bromham DR, Ismail AA, Morris AF. The value of a single serum progesterone measurement in the midluteal phase as a criterion of a potentially fertile cycle (“ovulation”) derived form treated and untreated conception cycles. Fertil Steril (1982) 37(3):355–60. doi: 10.1016/S0015-0282(16)46095-4
20. Cédrin-Durnerin I, Isnard T, Mahdjoub S, Sonigo C, Seroka A, Comtet M, et al. Serum progesterone concentration and live birth rate in frozen-thawed embryo transfers with hormonally prepared endometrium. Reprod BioMed Online (2019) 38(3):472–80. doi: 10.1016/j.rbmo.2018.11.026
21. Lee VC, Li RH, Chai J, Yeung TW, Yeung WS, Ho PC, et al. Effect of preovulatory progesterone elevation and duration of progesterone elevation on the pregnancy rate of frozen-thawed embryo transfer in natural cycles. Fertil Steril (2014) 101(5):1288–93. doi: 10.1016/j.fertnstert.2014.01.040
22. Wånggren K, Dahlgren Granbom M, Iliadis SI, Gudmundsson J, Stavreus-Evers A. Progesterone supplementation in natural cycles improves live birth rates after embryo transfer of frozen-thawed embryos-a randomized controlled trial. Hum Reprod (2022) 37(10):2366–74. doi: 10.1093/humrep/deac181
23. Kim C-H, Lee Y-J, Lee K-H, Kwon S-K, Kim S-H, Chae H-D, et al. The effect of luteal phase progesterone supplementation on natural frozen-thawed embryo transfer cycles. Obstet Gynecol Sci (2014) 57, 291. doi: 10.5468/OGS.2014.57.4.291
24. Mizrachi Y, Horowitz E, Ganer Herman H, Farhi J, Raziel A, Weissman A. Should women receive luteal support following natural cycle frozen embryo transfer? A systematic review and meta-analysis. Hum Reprod Update (2021) 27(4):643–50. doi: 10.1093/humupd/dmab011
Keywords: luteal phase support, in-vitro fertilisation, progesterone, frozen embryo transfer, natural cycle
Citation: Demirel C, Özcan P, Tülek F, Timur HT and Pasin Ö (2023) Initiating luteal phase support with sc progesterone based on low serum progesterone on the transfer day in true natural cycle frozen embryo transfers. Front. Endocrinol. 14:1278042. doi: 10.3389/fendo.2023.1278042
Received: 15 August 2023; Accepted: 29 September 2023;
Published: 23 October 2023.
Edited by:
Emre Pabuccu, Ufuk University, TürkiyeReviewed by:
Meltem Sönmezer, Memorial Ankara Hospital, TürkiyeMehmet Erdemom, Gazi University, Türkiye
Copyright © 2023 Demirel, Özcan, Tülek, Timur and Pasin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pınar Özcan, ZHJwaW5hcm96Y2FuQGhvdG1haWwuY29t
†ORCID: Cem Demirel, orcid.org/0000-0002-6633-9651
Pınar Özcan, orcid.org/0000-0002-0306-6422
Fırat Tülek, orcid.org/0000-0003-1668-8746
Hikmet Tunç Timur, orcid.org/0000-0002-1250-8579
Özge Pasin, orcid.org/0000-0001-6530-0942