 Jessica A. Reese
Jessica A. Reese Carla Guy1
Carla Guy1- 1Center for American Indian Health Research, Hudson College of Public Health, University of Oklahoma Health Sciences Center, Oklahoma City, OK, United States
- 2Department of Biostatistics and Epidemiology, Hudson College of Public Health, University of Oklahoma Health Sciences Center, Oklahoma City, OK, United States
Introduction: American Indians have higher rates of cardiovascular disease (CVD), likely due to disproportionate burden of diabetes and limited access to widespread CVD prevention programs such as Honoring the Gift of Heart Health (HGHH), a 10-week CVD risk factor awareness curriculum. Due to its length, HGHH may be difficult to complete; therefore, we aimed to evaluate a shortened CVD risk factor awareness program based on the HGHH educational materials for American Indians residing in southwest Oklahoma, entitled “The Amazing Race for Heart Health.”
Methods: We conducted an interventional study where each participant served as their own control (n = 61), with pre- and post-intervention measurements. We included American Indians from seven tribal nations in southwest Oklahoma. At two interventional meetings we used educational materials and activities from HGHH focusing on nutrition, cholesterol, diabetes, hypertension, physical activity, and heart attack warning signs. McNemar's test was used to determine the effectiveness of the intervention on raising CVD risk factor awareness.
Results: When comparing the pre- and post-survey responses, the percentage of correct responses either stayed the same or increased. Knowledge improved in 11/25 (44%, p < 0.05) domains including the difference between good and bad cholesterol and types of physical activity that can prevent CVD. When considering diabetes, knowledge increased regarding the interaction between diabetes and cholesterol in the association with CVD.
Discussion: These results demonstrate that the “Amazing Race for Heart Health,” a shortened CVD risk factor educational program based on the HGHH educational materials, was effective at increasing awareness regarding CVD risk factors.
Introduction
Cardiovascular disease (CVD) among American Indians was once thought to be low; however, results from the Strong Heart Study (SHS) have demonstrated that CVD in American Indians is higher than other United States (US) populations (1–3) and more likely to be fatal (1–4). Higher CVD prevalence and mortality in American Indian communities are likely due to disproportionate burden of diabetes, (5, 6) socioeconomic barriers to comprehensive cardiovascular care, (7) and limited access to widespread CVD prevention programs (8). Of the few programs that have been implemented in American Indian communities, many have focused health education on reducing body weight to achieve a proposed target to reduce the risk of diabetes and CVD (9, 10). In addition, most of these strategies have focused on American Indians with higher risks (i.e., metabolic syndrome), (9, 10) rather than the general American Indian populations residing in communities. Since culturally tailored CVD risk factor education is an integral component to intervention techniques for disease prevention, (11, 12) it is imperative that educational along with lifestyle interventions be expanded beyond weight control and be applicable on the community level (9, 10). Therefore, the proposed target for this study included education of additional CVD risk factors (beyond weight control), and implementation among a study population that was selected to be similar to the general population of American Indians residing in Southwest Oklahoma (i.e., not restricted to high risk groups). These proposed targets were based on focus group discussions with community members prior to developing the intervention.
To confront the high rates of CVD, (2, 13) potential interventions should be developed with direct community involvement (11, 12). Researchers, tribal nations, and community members must work collaboratively in decision-making process to develop a culturally relevant lifestyle intervention to reduce CVD risk (11, 14, 15). “Honoring the Gift of Heart Health” (HGHH) is a CVD risk factor education program developed by the National Heart, Lung, and Blood Institute for use in American Indian communities (16, 17). HGHH is unique because it incorporates a family-oriented approach for adopting heart health recommendations by emphasizing lifestyle changes for people of all ages (16). Although previous research indicates that HGHH has been effective, (18, 19) the full 10-week program may be difficult for participants to complete, due to working schedule conflicts, caring for family members, and other life priorities. Therefore, we aimed to work with American Indians residing in southwest Oklahoma to implement and evaluate a shortened CVD risk factor educational intervention program based on the HGHH materials.
Methods
Educational intervention development
To develop the shortened educational intervention based on HGHH materials, first we worked with the American Indian communities using a qualitative research design and a narrative inquiry approach, which has been previously described (20). Briefly, we conducted three focus group discussions, with 12 total participants. Two researchers transcribed the focus group audio recordings and conducted a content analysis to identify themes and patterns. American Indian participants provided recommendations regarding improving cultural responsiveness of the HGHH. On average, participants spent the highest percentage of time discussing themes related to nutrition (46%), followed by educational material format, risk factors, special groups, and new recommendations (20). This part of the project was the first step in working with American Indian communities to design a more effective and relevant educational intervention (11, 20). Next, we worked with a tribal liaison and other members of the community to incorporate the recommendations and to conduct the intervention in the communities.
Study population and recruiting
To determine if the intervention strategy was effective, we conducted a study where each participant served as their own control, with pre- and post-intervention survey measurements. We included American Indians from seven tribal communities that participated in the Strong Heart Study (SHS), which is a prospective cohort study of CVD in American Indians. Members of these tribal communities primarily reside in the rural areas of southwest Oklahoma; however, some reside in the urban areas of Oklahoma City. Throughout 2022, a tribal liaison (CG) and SHS field staff (HJ) used a snowball sampling approach to recruit participants for two separate interventional meetings. Tribal liaisons are important because they are tribal members that have leadership roles within the community. Therefore, they effectively communicate with the tribes and their members while respecting tribal sovereignty. Since the tribal liaison and the SHS field staff are members of the tribal communities, initial recruitment was based on their existing relationships within the community.
The first meeting included members of communities residing in Oklahoma City and was conducted at the University of Oklahoma Health Science Center. The second meeting included American Indian residents from SHS communities in rural areas and was conducted at the Wichita and Affiliated Tribes Community Center in Anadarko, Oklahoma. This study was approved by the participating tribes, University of Oklahoma Institutional Review Board, and the Oklahoma City Area Indian Health Service Institutional Review Board. We obtained written informed consent from each participant and community approval from the joint Southwest Oklahoma Intertribal Health Board.
Assessments
After obtaining individual informed consent, we asked the participants to complete a brief demographic survey, a heart disease risk factor assessment, and a heart disease risk factor knowledge survey (21). With the demographic survey, we collected age, gender, tribal affiliation, area of residence (urban or rural), and the highest attained level of education. The heart disease risk factor assessment contained self-reported CVD risk factors including current smoking behaviors, high blood pressure, high cholesterol, diabetes, being overweight or obese, being physically inactive, and having a family history of heart disease (17). Finally, we administered the heart disease risk factor knowledge survey. This survey was previously developed and validated and is a 25-item questionnaire that measures risk factor knowledge in people with diabetes (21). Although this questionnaire was not developed specifically for American Indians, it is relevant because of the high prevalence of diabetes in the American Indian communities that participate in the Strong Heart Study (22, 23). To determine if the intervention changed the participants' understanding of CVD risk factors, we administered the risk factor knowledge survey before and after the educational intervention.
Amazing race or heart health educational intervention
We delivered the intervention at two separate meetings. We began meetings with informal introductions, then we obtained individual informed consent and administered the assessments including the risk factor knowledge pre-survey. Next we delivered a 20 min educational power point presentation based on materials from the HGHH curriculum (16). We focused on HGHH topics that were interesting and relevant, based on comments during the focus groups that were previously conducted (17, 20). We presented information on the difference between saturated, unsaturated, and trans fats, describing what types of foods contain which types of fats. We then discussed how fat is related to blood cholesterol and the difference between low-density and high-density lipoproteins. Following the discussion on cholesterol, we discussed information on hypertension and hypertension medications. Then, we discussed diabetes, the amount of sugar in different types of food, and the relationship between sugar consumption and diabetes control. We defined diabetes, its symptoms, how it is related to heart disease, and the risk factors associated with diabetes. Then, we discussed some simple activities that participants can do to increase their physical activity, such as walking and gardening. Finally, we reviewed the heart attack warning signs presented in HGHH (16, 17).
To reinforce the information from the interactive presentation, we created the “Amazing Race for Heart Heath,” using activities and handouts from HGHH (17). During this part of the intervention, 6 groups of 5–6 people participated in an “scavenger hunt,” which lasted approximately 45 min. The participants performed the HGHH activities listed below:
1. Nutrition: We asked participants to choose the lower calorie food item from “Sally's Snack Choices.” In addition, we asked the participants to calculate the number of calories that Sally would save if she chose the lower calorie option.
2. Cholesterol: We asked participants to guess the amount of fat in various food items.
3. Diabetes: We asked participants to guess the amount of sugar in a big gulp, a bag of skittles, and a snickers bar. We had props including the actual candies and Styrofoam cup that would hold a big gulp. In addition, we had the amount of sugar contained in these items in a plastic bag.
4. Hypertension: We asked participants to list the four types of hypertension medications and how they work.
5. Physical activity: For this station, we asked the participants to complete the stretching exercises located in HGHH educator's manual. Then we asked them to walk a short distance.
6. Heart attack warning signs: Finally, we asked the participants to name the six heart attack warning signs located in HGHH educator's manual.
After successfully performing each of these activities, participants were given hints about where to go next. They also received handouts and materials to take home, based on HGHH educational materials. At the end of the race, we awarded study t-shirts to the group finishing first. Finally, we administered a post-survey to determine if they learned and retained the material (21).
Data analysis
We used descriptive statistics to summarize the population, calculating median and range for age and percents for all other variables. To assess CVD risk factor knowledge, we calculated the percent who correctly responded to each question on the pre- and post-surveys and used McNemar's test to determine if the responses on the surveys differed (24). We used SAS Software, version 9.4 for analyses (25).
Results
Study population demographics
We recruited 61 American Indian participants with a median age of 55 years (range = 23–88); 79% were female, 48% had ≥12 years of education, and 51% lived in rural Oklahoma. Regarding CVD risk factors, about one-half of the study population reported being overweight/obese (53%) or having hypertension (46%). Roughly one-third of the participants reported having high cholesterol (26%), diabetes (30%), physical inactivity (30%), or a family history of CVD (38%). Finally, 16% reported current smoking (Table 1).
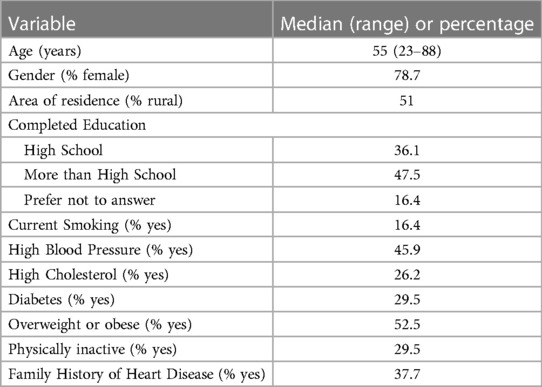
Table 1. Demographics and cardiovascular disease risk factors of American Indian study participants from southwestern Oklahoma (n = 61).
CVD risk factor knowledge
Since each participant served as their own control, we collected 122 observations from the pre- and post- CVD risk factor knowledge surveys. When comparing the pre- and post-surveys, the percentage of correct responses either increased or stayed the same. The participants had good baseline knowledge of several risk factors being associated with heart disease, including age (question 3), smoking (questions 4 and 5), high blood pressure (questions 6 and 7), being overweight (question 12), and having diabetes (questions 16–18, Table 2).
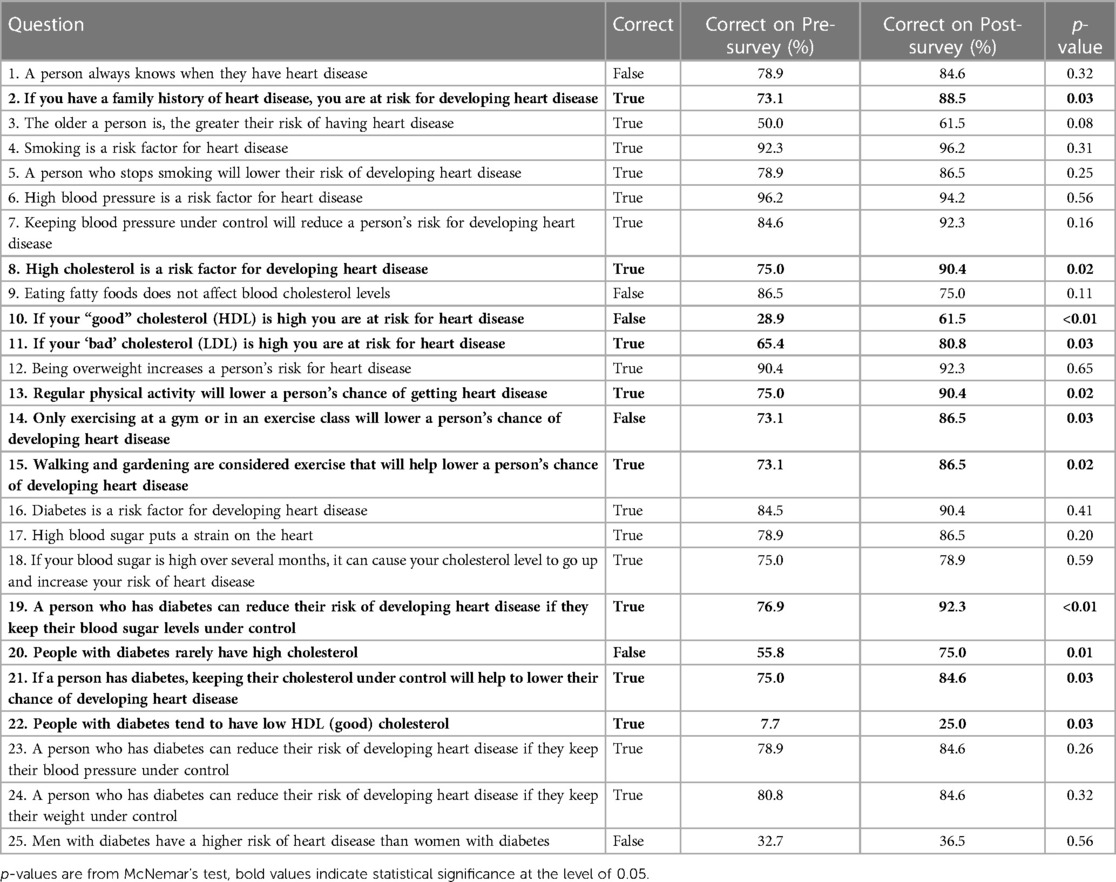
Table 2. Heart disease risk factor knowledge survey responses before and after an educational intervention for American Indians from communities that participate in the Strong Heart Study in southwest Oklahoma.
Heart disease risk factor knowledge improved in several domains, including family history of heart disease (question 2, p = 0.03), cholesterol (question 8, p = 0.02), and the difference between good and bad cholesterol (question 10, p = < 0.01 and question 11, p = 0.03). In addition, we observed improvements in knowledge regarding physical activity and the different types of physical activity that can prevent heart disease (questions 13–15, p-values all <0.05). When considering diabetes, knowledge increased regarding the association between blood glucose control and heart disease (question 19, p = < 0.01). Also, knowledge increased regarding the interaction between diabetes and cholesterol in the association with heart disease (questions 20–22, p-values all <0.05). On question 9, regarding the consumption of fatty foods and the effect on cholesterol, the percentage of correct responses decreased slightly from 86.5% to 75%, even though this material was covered in the presentation. However, this observation was not statistically significant (p = 0.11), indicating it could be due to chance. Finally, at baseline, only 33% correctly answered “false” to the question “Men with diabetes have a higher risk of heart disease than women with diabetes.” Since we did not focus on gender in our implementation program, the percentage of correct responses on this question did not increase on the post-survey (37%, p = 0.56).
Discussion
The results of this study demonstrate that the “Amazing Race for Heart Health,” a shortened CVD risk factor educational program based on the HGHH curriculum, was effective at increasing knowledge regarding CVD risk factors. When comparing the pre- and post-surveys, the percentage of correct responses either increased or stayed the same. Likely due to the educational efforts by the SHS in the past, the participants had good baseline knowledge of several risk factors being associated with CVD, including age, smoking, high blood pressure, being overweight, and having diabetes. This observation provides an opportunity for future research about the effect of previous SHS outreach and educational efforts. However, even with this good baseline knowledge, the educational intervention that we developed was effective at improving CVD risk factor knowledge in several domains, including family history of heart disease, cholesterol, physical inactivity, and the difference between good and bad cholesterol. When considering diabetes, knowledge increased regarding the association between blood glucose control and heart disease. Also, knowledge increased regarding the interaction between diabetes and cholesterol in the association with heart disease. These observations are similar to previous reports on the knowledge improvements for the full HGHH program (18, 19, 26).
Although the results of this project provide valuable information about a culturally relevant educational intervention, there are some limitations. The beliefs expressed by the American Indians participating in this project are limited to seven communities in southwest Oklahoma, and therefore may not be transferrable or generalizable to other tribal communities. In addition, this was pilot study with a relatively small sample size consisting of mainly women. Despite these potential limitations, this project provides valuable insights on an interventional approach to address CVD prevention within American Indian communities. With this first step in program enhancement, we hope the methods presented can be used to adapt this interventional program for a larger audience, other tribal communities, or other groups with similar levels of documented cardiometabolic risk factors.
These results illustrate the value of health promotion and educational initiatives. Based on study results, we recommend that focus groups or knowledge surveys be conducted before HGHH or other interventions are implemented to identify areas where specific populations may lack awareness, and then the intervention be adapted for specific communities. In addition, these results indicate the value of an interactive component to reinforce the didactic approaches. In the current study population, the following areas may deserve more effort, the association between CVD and family history of heart disease (question 2), age as a CVD risk factor (question 3), cholesterol and the different types of cholesterol (questions 8–11), physical inactivity (questions 13–15), diabetes control (question 19), the interaction of diabetes and cholesterol (questions 20–22), and gender in CVD risk (question 25). For example, on question 22, “People with diabetes tend to have low HDL (good) cholesterol,” the percentage of correct responses increased significantly from 7.7% to 25%, but the percentage post-intervention remained relatively low. Therefore, we may need to include more information on the difference between “good” and “bad” cholesterol and how it may affect patients with diabetes. Finally, to address the potential misconception that there are gender differences regarding CVD risk among people with diabetes (question 25), we want to emphasize that both men and women with diabetes have an elevated risk of CVD. In conclusion, “Amazing Race for Heart Health,” a shortened CVD risk factor educational program based on the HGHH educational materials, was effective at increasing awareness regarding CVD risk factors and may be applicable in future research with American Indians.
Data availability statement
The data were collected, analyzed, and reported under agreements made with the sovereign tribal nations that have partnered in this research, which preclude commonly accepted modes of data sharing. Requests to access the dataset from qualified researchers trained in responsible conduct of research may be sent to the Strong Heart Study Coordinating Center at https://strongheartstudy.org/. Requests will be reviewed by tribal research partners before data may be released. This policy is consistent with the “NIH Policy for Data Management and Sharing: Responsible Management and Sharing of American Indian/Alaska Native Participant Data (https://grants.nih.gov/grants/guide/notice-files/NOT-OD-22-214.html#:∼:text=NIH%20recognizes%20that%20conducting%20biomedical,Tribes%5Biii%5D%20and%20communities).
Ethics statement
The studies involving humans were approved by University of Oklahoma Health Sciences Center IRB, Oklahoma City Area Indian Health Service IRB. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JR: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. CG: Conceptualization, Investigation, Writing – review & editing. HJ: Investigation, Writing – review & editing. TA: Conceptualization, Project administration, Supervision, Writing – review & editing. EL: Conceptualization, Formal Analysis, Funding acquisition, Writing – review & editing. YZ: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This study was funded by the National Heart, Lung, and Blood Institute (NHLBI) through WESTAT, INC, under contract numbers HHSN268201700020B/75N92020F00001, with cost share from the Strong Heart Study (SHS). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication. The SHS has been funded in whole or in part with federal funds from the NHLBI, National Institute of Health, Department of Health and Human Services, under contract numbers 75N92019D00027, 75N92019D00028, 75N92019D00029, & 75N92019D00030. The study was previously supported by research grants: R01HL109315, R01HL109301, R01HL109284, R01HL109282, and R01HL109319 and by cooperative agreements: U01HL41642, U01HL41652, U01HL41654, U01HL65520, and U01HL65521.
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Indian Health Service (IHS). We would like to acknowledge Yashaswi Joshi for her contributions to study data entry and management.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Lee ET, Welty TK, Fabsitz R, Cowan LD, Le NA, Oopik AJ, et al. The strong heart study. A study of cardiovascular disease in American Indians: design and methods. Am J Epidemiol. (1990) 132(6):1141–55. doi: 10.1093/oxfordjournals.aje.a115757
2. Howard BV, Lee ET, Cowan LD, Devereux RB, Galloway JM, Go OT, et al. Rising tide of cardiovascular disease in American Indians: the strong heart study. Circulation. (1999) 99(18):2389–95. doi: 10.1161/01.CIR.99.18.2389
3. Lee ET, Howard BV, Wang W, Welty TK, Galloway JM, Best LG, et al. Prediction of coronary heart disease in a population with high prevalence of diabetes and albuminuria: the strong heart study. Circulation. (2006) 113(25):2897–905. doi: 10.1161/CIRCULATIONAHA.105.593178
4. Centers for Disease Control and Prevention (CDC). Disparities in premature deaths from heart disease–50 states and the district of Columbia, 2001. MMWR Morb Mortal Wkly Rep. (2004) 53(6):121–5. PMID: 1498136014981360
5. Lee ET, Welty TK, Cowan LD, Wang W, Rhoades DA, Devereux R, et al. Incidence of diabetes in American Indians of three geographic areas: the strong heart study. Diabetes Care. (2002) 25(1):49–54. doi: 10.2337/diacare.25.1.49
6. Lee ET, Howard BV, Go O, Savage PJ, Fabsitz RR, Robbins DC, et al. Prevalence of undiagnosed diabetes in three American Indian populations. A comparison of the 1997 American diabetes association diagnostic criteria and the 1985 world health organization diagnostic criteria: the strong heart study. Diabetes Care. (2000) 23(2):181–6. doi: 10.2337/diacare.23.2.181
7. Jernigan V, Lee ET, Yeh J, Fabsitz RR, Howard BV, Zhang Y. Abstract P373: health care access and usage patterns among native Americans: the strong heart study. Circulation. (2023) 147(Suppl_1):AP373–AP373. doi: 10.1161/circ.147.suppl_1.P373
8. Breathett K, Sims M, Gross M, Jackson EA, Jones EJ, Navas-Acien A, et al. Cardiovascular health in American Indians and Alaska natives: a scientific statement from the American heart association. Circulation. (2020) 141(25):e948–59. doi: 10.1161/CIR.0000000000000773
9. Lee ET, Jobe JB, Yeh J, Ali T, Rhoades ER, Knehans AW, et al. A cardiovascular risk reduction program for American Indians with metabolic syndrome: the balance study. J Prim Prev. (2012) 33(4):187–96. doi: 10.1007/s10935-012-0273-0
10. Lee ET, Begum M, Wang W, Blackett PR, Blevins KS, Stoddart M, et al. Type 2 diabetes and impaired fasting glucose in American Indians aged 5-40 years: the Cherokee diabetes study. Ann Epidemiol. (2004) 14(9):696–704. doi: 10.1016/j.annepidem.2003.10.013
11. Welty TK. Examples of successful community-based participatory research in American Indian communities. In: Solomon TGA, Randall LL, editors. Conducting health research with native American communities. Washington DC: American Public Health Association (2014). p. 157–170.
12. Jernigan VB. Community-based participatory research with native American communities: the chronic disease self-management program. Health Promot Pract. (2010) 11(6):888–99. doi: 10.1177/1524839909333374
13. Howard BV, Lee ET, Cowan LD, Fabsitz RR, Howard WJ, Oopik AJ, et al. Coronary heart disease prevalence and its relation to risk factors in American Indians. The strong heart study. Am J Epidemiol. (1995) 142(3):254–68. doi: 10.1093/oxfordjournals.aje.a117632
14. Noe TD, Manson SM, Croy C, McGough H, Henderson JA, Buchwald DS. The influence of community-based participatory research principles on the likelihood of participation in health research in American Indian communities. Ethn Dis. (2007) 17(1 Suppl 1):S6–14. PMID: 1759831117598311
15. Wallerstein NB, Duran B. Using community-based participatory research to address health disparities. Health Promot Pract. (2006) 7(3):312–23. doi: 10.1177/1524839906289376
16. U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute, Indian Health Service. Honoring the gift of heart health A heart health educator’s manual for American Indians. Washington, DC: National Institutes of Health (NIH) Publication (2006). No. 06-5218.
17. National Heart, Lung, and Blood Institute. Materials for the American Indian/Alaska Native Population. Available at: https://www.nhlbi.nih.gov/health/educational/healthdisp/health-education-materials/american-indian-alaska-native.htm (Published June, 2014. Accessed 2022).
18. Brega AG, Noe T, Loudhawk-Hedgepeth C, Jim DM, Morse B, Moore K, et al. Cardiovascular knowledge among urban American Indians and Alaska natives: first steps in addressing cardiovascular health. Prog Community Health Partnersh. (2011) 5(3):273–9. doi: 10.1353/cpr.2011.0042
19. Brega AG, Pratte KA, Jiang L, Mitchell CM, Stotz SA, Loudhawk-Hedgepeth C, et al. Impact of targeted health promotion on cardiovascular knowledge among American Indians and Alaska natives. Health Educ Res. (2013) 28(3):437–49. doi: 10.1093/her/cyt054
20. Eisele M, Reese J, Jones A, Zhang Y. Abstract P646: American Indian community stakeholders evaluate the cardiovascular health curriculum honoring the gift of heart health: the strong heart study. Circulation. (2023) 147(Suppl_1):AP646. doi: 10.1161/circ.147.suppl_1.P646
21. Wagner J, Lacey K, Chyun D, Abbott G. Development of a questionnaire to measure heart disease risk knowledge in people with diabetes: the heart disease fact questionnaire. Patient Educ Couns. (2005) 58(1):82–7. doi: 10.1016/j.pec.2004.07.004
22. Lee ET, Howard BV, Savage PJ, Cowan LD, Fabsitz RR, Oopik AJ, et al. Diabetes and impaired glucose tolerance in three American Indian populations aged 45–74 years. The strong heart study. Diabetes Care. (1995) 18(5):599–610. doi: 10.2337/diacare.18.5.599
23. Wang W, Zhang Y, Lee ET, Howard BV, Devereux RB, Cole SA, et al. Risk factors and prediction of stroke in a population with high prevalence of diabetes: the strong heart study. World J Cardiovasc Dis. (2017) 7(5):145–62. doi: 10.4236/wjcd.2017.75014
24. McNemar Q. Note on the sampling error of the difference between correlated proportions or percentages. Psychometrika. (1947) 12(2):153–7. doi: 10.1007/BF02295996
25. Statistical Analyis System (SAS) Software. Copyright © 2012. SAS Institute Inc., Cary, NC, USA. All rights reserved.
26. Moore K, Jiang L, Manson SM, Beals J, Henderson W, Pratte K, et al. Case management to reduce cardiovascular disease risk in American Indians and Alaska natives with diabetes: results from the special diabetes program for Indians healthy heart demonstration project. Am J Public Health. (2014) 104(11):e158–164. doi: 10.2105/AJPH.2014.302108
Keywords: cardiovascular disease, cardiovascular education, Strong Heart Study, American Indian, cardiovascular disease prevention, community health promotion
Citation: Reese JA, Guy C, Jay H, Ali T, Lee ET and Zhang Y (2023) A community health promotion project: Amazing Race for Heart Health. Front. Epidemiol. 3:1278672. doi: 10.3389/fepid.2023.1278672
Received: 16 August 2023; Accepted: 6 December 2023;
Published: 20 December 2023.
Edited by:
Theophilus I. Emeto, James Cook University, AustraliaReviewed by:
Jemma King, James Cook University, AustraliaHani Sabbour, Cleveland Clinic Abu Dhabi, United Arab Emirates
© 2023 Reese, Guy, Jay, Ali, Lee and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica A. Reese amVzc2ljYS1yZWVzZUBvdWhzYy5lZHU=